Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Poor Knowledge and Suboptimal Practice Regarding Postmenopausal Osteoporosis Prevention Among Chinese Postmenopausal Women: A Structural Equation Model Analysis
Authors Chen Y, Chen F, Ying R, Ai L, Dai F, Zhang Q ![]()
Received 30 January 2026
Accepted for publication 22 May 2026
Published 9 July 2026 Volume 2026:19 600126
DOI https://doi.org/10.2147/JMDH.S600126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jagdish Khubchandani
Yiqing Chen, Fuhua Chen, Ruixue Ying, Liya Ai, Fang Dai, Qiu Zhang
Department of Endocrinology, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China
Correspondence: Fang Dai, Email [email protected] Qiu Zhang, Email [email protected]
Background: This study aimed to investigate the knowledge, attitude, and practice (KAP) of postmenopausal women toward postmenopausal osteoporosis (PMOP).
Methods: A cross-sectional study was conducted between March and July 2024 at the First Affiliated Hospital of Anhui Medical University among postmenopausal women, using a self-administered questionnaire. KAP scores ≥ 70% were defined as adequate levels based on previous literature. Structural equation modeling (SEM) was constructed based on the KAP theoretical framework to examine the relationships among knowledge, attitude, and practice.
Results: A total of 466 valid questionnaires were analyzed, with a validity rate of 97.69%. The mean knowledge, attitude, and practice scores were 14.08 ± 7.90 (range: 0– 30), 24.45 ± 2.43 (range: 7– 35), and 16.42 ± 3.96 (range: 5– 25), respectively. Multivariate logistic regression analysis revealed that knowledge was negatively associated with practice (OR = 0.936, 95% CI: [0.910– 0.962], P < 0.001). Additionally, education level (OR = 1.752, 95% CI: [1.110– 2.766], P = 0.016) and marital status (OR = 0.392, 95% CI: [0.167– 0.917], P = 0.031) were independently associated with better practice. The structural equation model results indicated that knowledge was significantly associated with attitude (β = 0.481, 95% CI: 0.402– 0.570, P = 0.009), and was negatively associated with practice (β = − 0.324, 95% CI: − 0.460– 0.199, P = 0.011).
Conclusion: Postmenopausal women showed poor PMOP knowledge and prevention practices, with a notable knowledge–practice gap. Higher knowledge levels were associated with poorer preventive practices, suggesting that knowledge alone may not translate into appropriate health behaviors. Targeted interventions addressing both awareness and behavioral barriers are needed.
Keywords: knowledge, attitude and practice, postmenopausal osteoporosis, postmenopausal women, cross-sectional study
Introduction
Osteoporosis (OP) is an osteometabolic disorder and silent killer characterized by impaired bone matrix mineralization, leading to a decrease in bone mass, micro-architectural deterioration of bone tissue, and predisposition to fracture.1 OP is a disease of aging. In countries with serious aging society, such as China, its prevalence is gradually increasing. A 2019 survey2 analyzed data from 75,321 adults in seven research centers in Northeast, North, East, and Southwest China. The study found that the age-standardized prevalence of OP in men and women aged 50 and above was 6.46% and 29.13% respectively. It is estimated that there are currently 10.9 million men and 49.3 million women in China suffering from OP. By 2050, it’s predicted that OP will affect 7.46% of Chinese men and 39.19% of women aged 50 and above.3 Osteoporotic fracture leads to increased mortality and disability rates, consuming huge medical expenses and resources, and causing great burden on families and society. Therefore, it has become a serious chronic disease that threatens the health of Chinese citizens.4
Among the common causes of OP, postmenopausal OP (PMOP) caused by estrogen deficiency has the highest incidence rate.5 Despite its high incidence and significant hazards, most women are only familiar with the disease’s name and lack an understanding of the dangers it poses as well as the importance of early diagnosis and treatment. Therefore, most PMOP patients often delay the treatment opportunity, resulting in increased risk of fracture and significantly reduced quality of life.
The Knowledge, Attitude, and Practice (KAP) survey serves as a valuable diagnostic research tool, shedding light on a group’s understanding, beliefs, and behaviors concerning a specific subject. In the context of health literacy, it is grounded in the premise that knowledge is a catalyst for shaping attitudes, which in turn influence behaviors.6–8 Despite the well-documented health implications of OP, it becomes apparent that postmenopausal women may exhibit deficiencies in their awareness, attitudes, and practices related to this condition. This gap in knowledge and understanding could result in a lack of timely preventive actions, such as maintaining appropriate nutrition, engaging in moderate exercise, and seeking essential medical guidance. While previous KAP studies have explored healthcare workers and men,9,10 there is a conspicuous absence of KAP studies concerning postmenopausal women. In addition, existing studies on postmenopausal women are often limited by small or region-specific samples and variability in measurement tools, which may affect the comparability and generalizability of findings. Additionally, the existing research on PMOP and bone health in postmenopausal women remains limited in scope and comprehensiveness.11 Although the KAP framework is widely used to assess health-related behaviors, its traditional linear assumption that knowledge leads to attitudes and subsequently to behavior has been increasingly questioned. In this study, we adopted the KAP framework as a guiding structure while further exploring the relationships among its components using structural equation modeling to capture more complex pathways. Therefore, this study aimed to investigate the KAP of postmenopausal women toward PMOP and to examine the relationships among knowledge, attitude, and practice using structural equation modeling. We hypothesized that knowledge would influence practice both directly and indirectly through attitude, thereby providing a more comprehensive understanding of the pathways underlying preventive behaviors.
Materials And Methods
Study Design and Participants
This cross-sectional study was conducted between March 2024 and July 2024 at the First Affiliated Hospital of Anhui Medical University. The participants were postmenopausal women primarily recruited from the hospital’s health examination center and nearby community health centers. To ensure broad participation, flyers were posted in multiple community health centers to invite eligible individuals who were interested in joining the study. Inclusion criteria were: 1) Age ≥ 40 years and a minimum of 12 months since the occurrence of natural menopause; 2) Demonstrated literacy skills sufficient to independently complete the questionnaire; 3) Willing participation, as confirmed by the provision of signed informed consent. Exclusion criteria were: 1) Individuals with a personal history of mental illness or a documented family history of mental illness. The study received ethical approval from the Committee on Medical Ethics of the First Affiliated Hospital of Anhui Medical University (Approval No. 2024–01-67), and informed consent was obtained from the participants.
Questionnaire Introduction
The questionnaire design was informed by the consensus of leading Chinese experts specializing in the prevention and treatment of OP in perimenopausal and postmenopausal women, along with insights from relevant research articles.11–13 Following the initial design, the questionnaire underwent two rounds of expert consultation. In the first round, it was reviewed and modified by two endocrinology experts, each boasting over 30 years of experience. The second round involved feedback from one endocrinology expert with over 30 years of experience and one epidemiology expert with over 20 years of experience. To ensure the questionnaire’s reliability, a random sample of 99 individuals was selected for testing, resulting in a Cronbach’s α coefficient of 0.895, indicating a commendable level of internal consistency.
The final questionnaire comprised four sections: demographic information, knowledge dimension, attitude dimension, and practice dimension. The knowledge dimension encompassed 15 questions, with scores of 2, 1, and 0 allocated for complete understanding, partial understanding, and lack of clarity, respectively, resulting in a possible score range of 0–30 points. This scoring approach was adopted to capture varying levels of understanding beyond a simple correct/incorrect dichotomy, allowing for more nuanced assessment of participants’ knowledge. “Partial understanding” was defined as recognizing the general concept but lacking complete or accurate details. The attitude dimension encompassed 7 questions, employing a five-point Likert scale. Positive attitude questions were rated from 5 points (strongly agree) to 1 point (strongly disagree), while negative attitude questions (1st, 3rd, and 6th questions) were reverse-scored, yielding a score range of 7–35 points. The practice dimension evaluated the frequency of various preventive measures in daily life. There are a total of 11 questions in the practice dimension. Among them, 5 questions adopt a 5-point Likert scale, ranging from “never” (1 point) to “every day” (5 points), with a total score ranging from 5 to 25. These items were included in the composite practice score as they reflect the frequency of core preventive behaviors. The remaining 6 questions (eg, exercise type, duration of exercise, duration of sun exposure, and information sources) were analyzed descriptively because they represent qualitative or contextual aspects of behavior that are not directly comparable on a unified frequency scale. KAP scores exceeding 70% were considered indicative of sufficient knowledge and positive attitudes and practices, based on previously published KAP studies using similar cut-off criteria 14. Although this threshold has been widely applied across different health-related KAP studies, its applicability to osteoporosis-related populations should be interpreted with caution.14
The questionnaire was developed using the Questionnaire Star platform (https://www.wjx.cn), with an electronic QR code generated for distribution. It was disseminated through popular social media platforms (eg, Weibo, WeChat) and posted at the entrances of participating health examination centers and community health centers. Additionally, paper-based questionnaires were administered by on-site staff to broaden participation and minimize selection bias.
Participants were recruited through random sampling during their visits to these centers. Trained research assistants explained the study purpose and procedures to voluntary participants. For electronic responses, participants accessed the questionnaire by scanning the QR code and were required to log in via a social media account (one response per unique ID). All questions were mandatory to ensure completeness, and submissions with missing items were prohibited. Paper questionnaires were distributed in person, with research assistants verifying responses for duplicates or errors.
Quality Control
To uphold data reliability, a dedicated team of physicians and healthcare professionals provided assistance during questionnaire completion. Two trained research assistants independently evaluated the integrity, internal consistency, and validity of all responses. Questionnaires completed in less than 120 seconds or containing logical inconsistencies (eg, conflicting answers) were excluded. Prior to analysis, cross-checks between electronic and paper submissions were performed to identify and remove duplicate entries.
Sample Size Calculation
Drawing from prior literature, the awareness rate of OP in postmenopausal women stands at 51%,15 accompanied by a 95% confidence interval and a permissible error of 5%. Consequently, the calculated sample size was determined to be 384. To account for potential participant attrition, a 10% dropout rate was considered, leading to a finalized minimum sample size of 422. In addition, considering the requirements of structural equation modeling, the sample size was deemed adequate based on the commonly recommended criterion of at least 10–20 participants per observed variable, ensuring sufficient statistical power and model stability.
Statistical Analysis
Statistical analysis was conducted using SPSS 22.0 (IBM Corp., Armonk, N.Y., USA). Continuous variables were described using mean ± standard deviation (SD), and between-group comparisons were performed using t-tests or analysis of variance (ANOVA). Categorical data were expressed as n (%) and analyzed using the chi-square test. Pearson correlation analysis was employed to assess the correlations between knowledge, attitude, and practice scores. Univariate variables with P<0.05 were enrolled in multivariate regression. In regression analyses, knowledge, attitude, and practice scores were treated as continuous variables when included as independent variables. For logistic regression analysis, knowledge, attitude, and practice scores were dichotomized using the 70% threshold, with scores ≥70% defined as adequate/positive and scores <70% defined as inadequate/negative. The relationships among knowledge, attitude, and practice were assessed using a path analysis model (structural equation model, SEM). The hypothesized paths were constructed based on the KAP theoretical framework and relevant literature, with knowledge specified to be associated with attitude and practice, while attitude was modeled as a potential mediator between knowledge and practice. Model fit was evaluated using root mean square error of approximation (RMSEA), incremental fit index (IFI), Tucker-Lewis index (TLI), and comparative fit index (CFI). Two-sided p<0.05 were considered statistically significant in this study.
Results
Demographic Characteristics
Initially, 477 questionnaires were collected for this study. After excluding 4 cases with response times less than 120 seconds, 2 cases with disagreements regarding informed consent, and 4 cases with logical errors, 466 valid responses remained, resulting in a validity rate of 97.69%. Among these participants, 254 (54.51%) were under the age of 60, 212 (45.49%) were aged 60 years and above, 390 (83.69%) resided in urban areas, 76 (16.31%) resided in rural or suburban areas, 291 (62.45%) were retired, and 168 (36.05%) had been in menopause for five years and above. 148 (31.76%) had been in menopause for 5–10 years, and 150 (32.19%) had been in menopause for more than 10 years. Additionally, 95 (20.39%) had been diagnosed with osteoporosis, 398 (85.41%) had no history of osteoporotic fractures, 30 (6.44%) had a history of osteoporotic fractures, and 406 (87.12%) had not undergone PMOP treatment (Table 1).
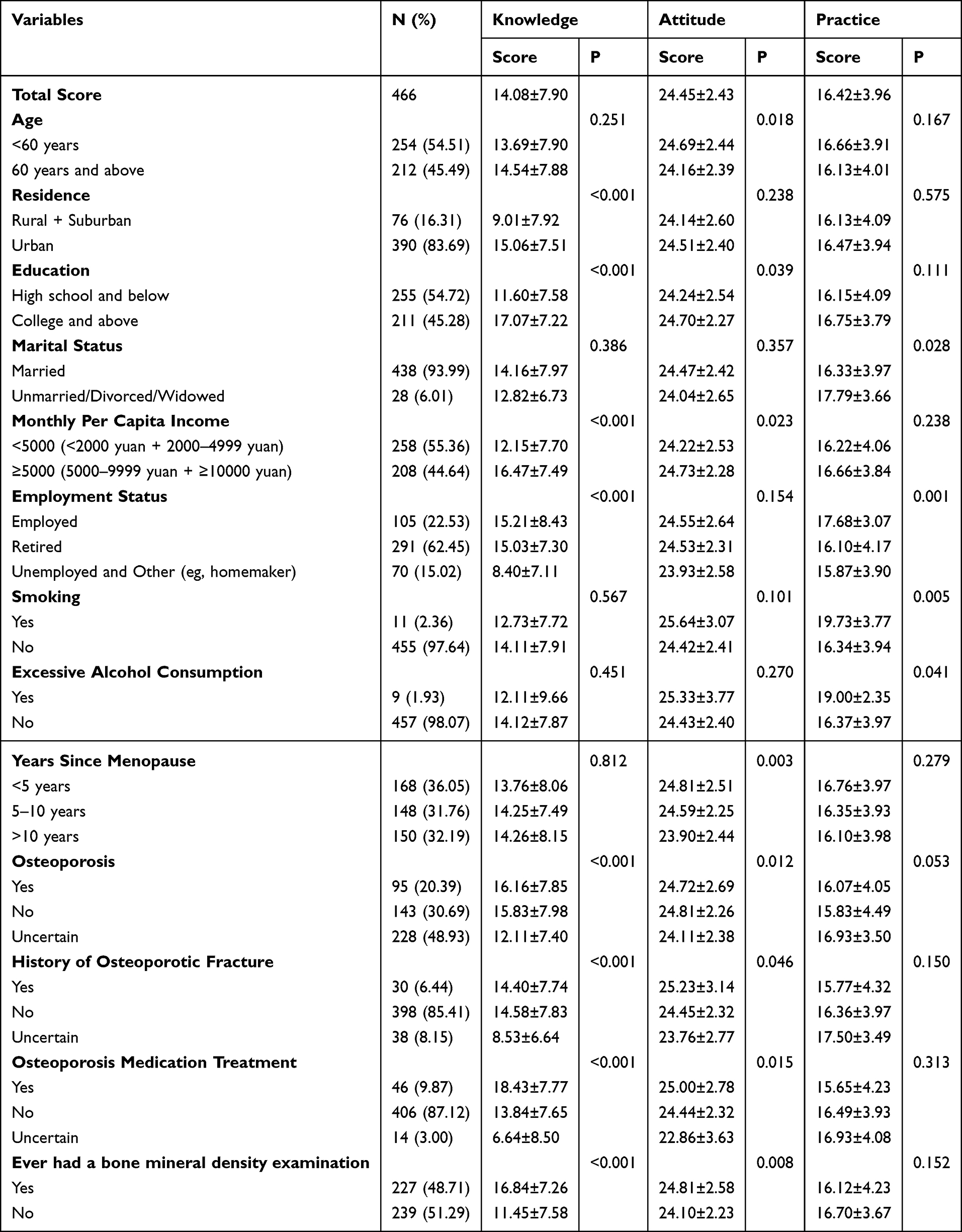 |
Table 1 Demographic Characteristic and Knowledge, Attitude, Practice Scores |
Knowledge, Attitude and Practice Dimensions
The mean knowledge, attitude and practice scores were 14.08 ± 7.90 (possible range: 0–30), 24.45 ± 2.43 (possible range: 7–35) and 16.42±3.96 (possible range: 5–25). Knowledge, attitude, and practice scores varied among postmenopausal women with different education levels (P < 0.001 and P = 0.039), monthly per capita income (P < 0.001 and P = 0.023), history of osteoporotic fractures (P < 0.001 and P = 0.046), and whether they had undergone osteoporosis medication treatment (P < 0.001 and P = 0.015). Furthermore, differences in residence (P < 0.001) and employment status (P < 0.001 and P = 0.001) were associated with significant differences in knowledge, attitude, and practice scores among postmenopausal women. Finally, variations in age (P = 0.018) and the duration of menopause (P = 0.003) were linked to differing attitude scores (Table 1).
The distribution of knowledge dimensions revealed that the three questions with the highest number of participants choosing the “Understand” option were “Do you understand that regular outdoor sunlight exposure can help prevent osteoporosis?” (K7) with 62.23%, “Do you understand that supplementing calcium and vitamin D can help prevent osteoporosis?” (K8) with 56.44%, and “Do you understand that moderate exercise can help prevent osteoporosis?” (K9) with 53.65%. On the contrary, the three questions with the highest number of participants choosing the “Unclear” option were “Do you understand the adverse effects associated with estrogen therapy?” (K12) with 65.45%, “Do you understand that women within 10 years of menopause can use estrogen therapy to prevent postmenopausal osteoporosis?” (K11) with 63.09%, and “Do you understand that smoking may lead to osteoporosis?” (K6) with 58.58% (Supplementary Table 1).
A significant majority of respondents (76.61%) expressed concern about the potential development of postmenopausal osteoporosis and osteoporotic fractures (A1), with 25.75% strongly agreeing and 50.86% agreeing. Additionally, a substantial percentage (71.67%) believed that BMD examination should be conducted regularly after the age of 40, regardless of menopausal status (A2), with 16.31% strongly agreeing and 55.36% agreeing. In contrast, a noteworthy proportion (42.70%) of participants believed that postmenopausal osteoporosis would not pose a threat to their life (A3), with 3.86% strongly agreeing and 38.84% agreeing. On the topic of comorbidities, a notable majority (77.89%) agreed that having other chronic conditions, such as diabetes and rheumatoid arthritis, can contribute to or exacerbate osteoporosis (A4), with 10.94% strongly agreeing and 66.95% agreeing. The majority of respondents (89.05%) believed that postmenopausal osteoporosis is both preventable and treatable (A5), with 13.73% strongly agreeing and 75.32% agreeing. Additionally, a significant proportion (74.25%) felt that one should not wait until a fracture occurs to undergo osteoporosis screening (A6), with 13.73% strongly agreeing and 60.52% agreeing. Finally, a substantial majority (84.34%) emphasized the importance of proactively educating themselves about postmenopausal osteoporosis (A7), with 19.96% strongly agreeing and 64.38% agreeing (Supplementary Table 2).
Postmenopausal women have diverse practices. 17.38% never drink milk, while 30.90% consume it 1–2 days per week (P1), and 23.39% drink it every day. 56.44% of respondents never consume strong tea or coffee (P2), while 19.96% drink it 1–2 days per week, and 12.45% drink it every day. In terms of supplementation, 50.64% never take calcium supplements (P9), while 21.89% take them 1–2 days per week, and 13.30% take them every day. 68.03% never take vitamin D (P10), and 13.52% take it 1–2 days per week. On the topic of exercise, 13.52% never exercise (P4), while 29.18% engage in exercise 3–4 days per week, and 24.25% exercise every day. 48.28% of participants exercise for 30 minutes to 1 hour each time (P5). Additionally, 13.95% never sunbathe (P6), 35.62% get sun exposure 1–2 days per week, and 63.52% spend less than 30 minutes in the sun each time (P7). As for the sources of osteoporosis-related knowledge, 65.24% of participants receive education from healthcare professionals (P10), 45.06% obtain information from the internet and social media, and 38.20% acquire it from television, newspapers, and other media (Supplementary Table 3).
Multivariate Logistic Regression Analysis
Multivariate logistic regression analysis revealed that having an education level of college or above (OR = 1.978, 95% CI: [1.147–3.410], P = 0.014) and receiving osteoporosis medication treatment (OR = 2.597, 95% CI: [1.161–5.810], P = 0.020) were independently associated with knowledge. Additionally, lacking awareness of their PMOP condition (OR = 0.455, 95% CI: [0.261–0.795], P = 0.006) was found to be negatively associated with knowledge. Lacking awareness of their PMOP condition (OR = 0.573, 95% CI: [0.368–0.893], P = 0.014) was independently associated with attitude. Knowledge was independently and negatively associated with practice (OR = 0.936, 95% CI: [0.910–0.962], P < 0.001), while education level (college and above) (OR = 1.752, 95% CI: [1.110–2.766], P = 0.016), marital status (married) (OR = 0.392, 95% CI: [0.167–0.917], P = 0.031), and employment status (retired) (OR = 0.582, 95% CI: [0.361–0.939], P = 0.027) or unemployed/other (OR = 0.442, 95% CI: [0.217–0.900], P = 0.024) were independently associated with practice (Tables 2–4). Attitude was not included in the multivariate model for practice due to its non-significant association in univariate analysis (P = 0.861).
 |
Table 2 Univariate and Multivariate Logistic Regression Analysis of Knowledge |
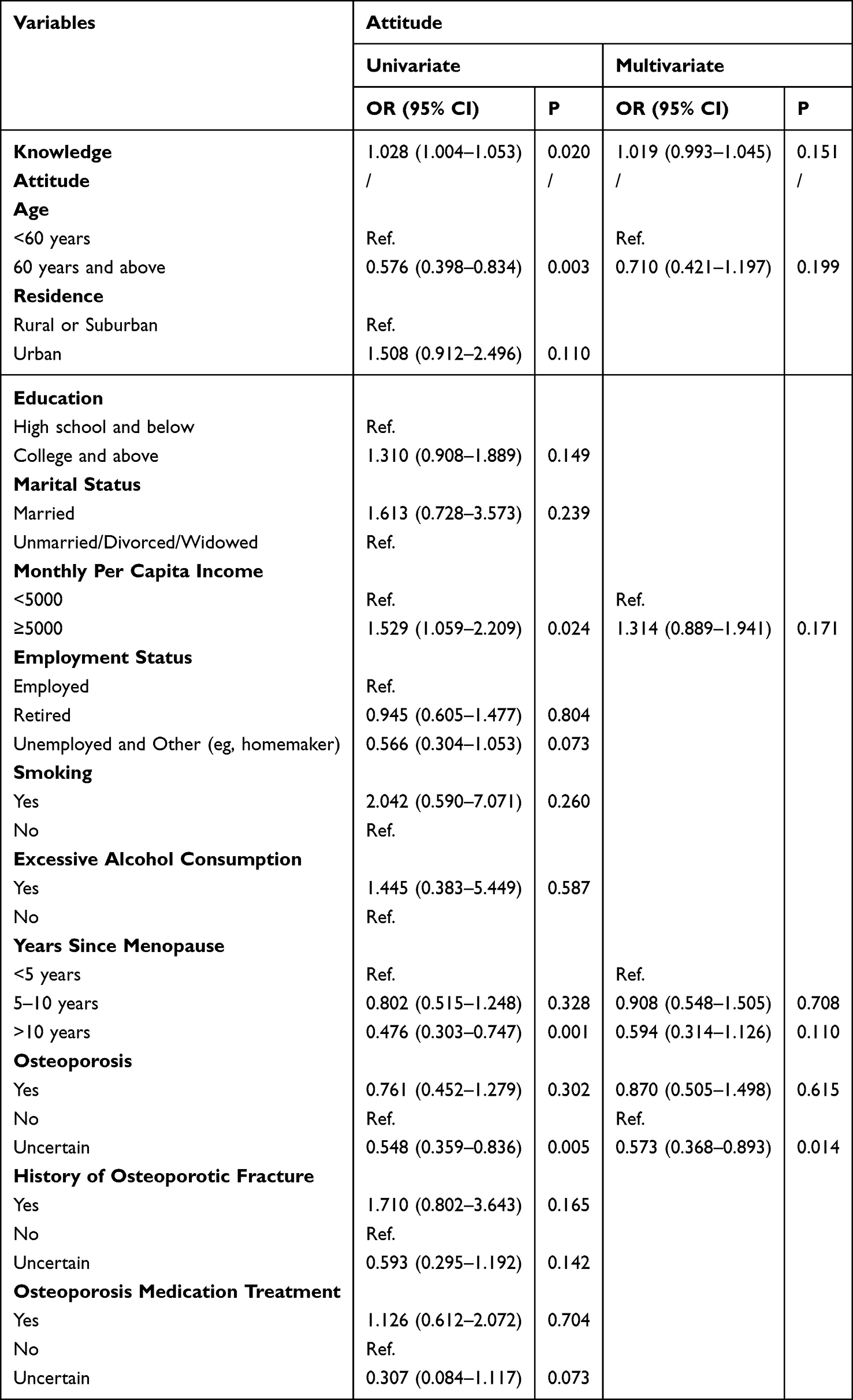 |
Table 3 Univariate and Multivariate Logistic Regression Analysis of Attitude |
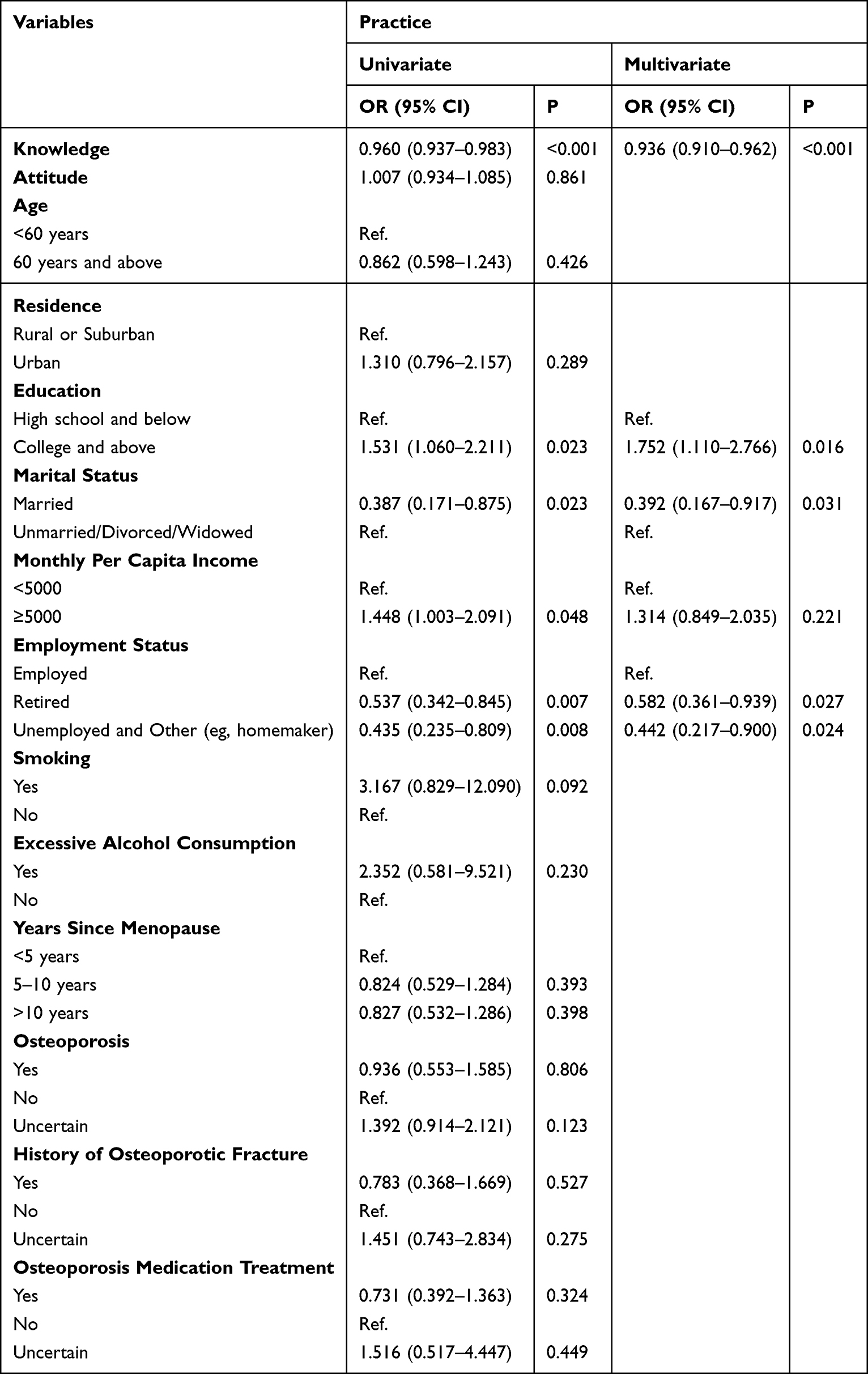 |
Table 4 Univariate and Multivariate Logistic Regression Analysis of Practice |
Correlation Analysis
Correlation analysis showed that knowledge was positively associated with attitude (r = 0.185, P < 0.001) but negatively associated with practice (r = −0.209, P < 0.001), while attitude showed no significant association with practice (r = 0.002, P = 0.963) (Supplementary Table 4).
SEM
The model fit indices for the SEM indicated an acceptable model fit, as evidenced by the following results: the CMIN/DF value was 2.802; the RMSEA was 0.062, indicating a good fit (<0.08); the IFI, TLI, and CFI values were 0.890, 0.876, and 0.889, respectively, exceeding the threshold of 0.8. Although slightly below the conventional 0.90 criterion, these values are considered acceptable for exploratory models (Supplementary Table 5). The SEM results indicated that knowledge was significantly associated with attitude (β = 0.481, 95% CI: 0.402–0.570, P = 0.009), and was negatively associated with practice (β = −0.324, 95% CI: −0.460–0.199, P = 0.011) (Table 5 and Figure 1).
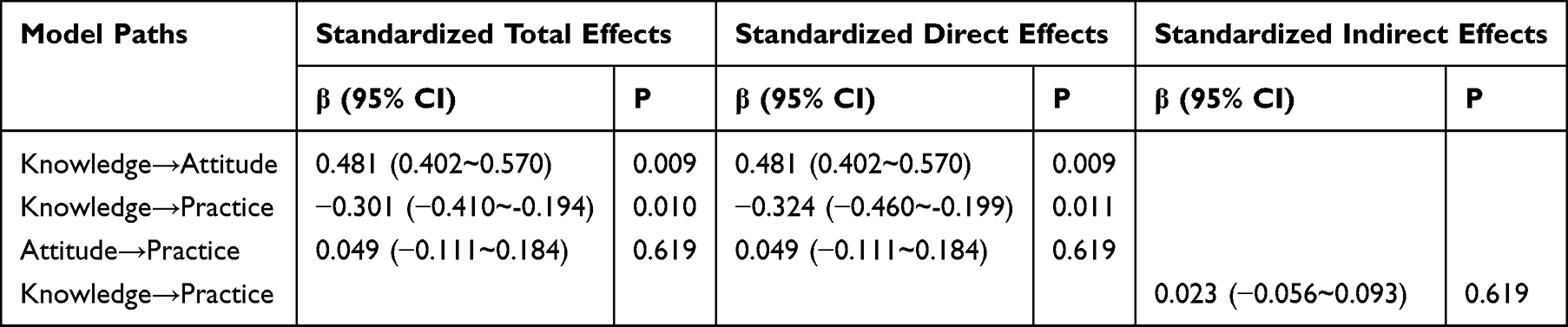 |
Table 5 Direct and Indirect Effects of Bootstrap Test |
 |
Figure 1 Path Analysis Model with standardized path coefficients. |
Discussion
Main Finding of This Study
The findings suggest women had inadequate knowledge, moderate attitudes, and inactive practices toward PMOP. Notably, knowledge was negatively associated with practice across multiple analyses, including multivariate logistic regression, correlation analysis, and SEM, indicating that higher knowledge levels were linked to less favorable preventive behaviors. This unexpected pattern suggests that knowledge alone may not translate into appropriate practice and highlights a potential disconnect between awareness and behavior. Possible explanations may include perceived barriers to implementation, lack of access to resources, or insufficient translation of knowledge into actionable skills. These findings emphasize that improving knowledge alone may be insufficient, and more comprehensive strategies addressing behavioral, psychological, and contextual factors are needed.
What is Already Known on This Topic
The present study indicated that postmenopausal women exhibit insufficient knowledge and moderate attitudes regarding PMOP, which poses a significant challenge to clinical practice and public health. To enhance clinical practice in the context of OP management and prevention, it is imperative to implement targeted educational interventions that focus on improving knowledge and fostering positive attitudes among this population.16,17 Healthcare professionals, particularly those specializing in women’s health and geriatrics, play a pivotal role in disseminating information, conducting regular screenings, and promoting awareness of PMOP, its risk factors, and preventive measures.18,19 Furthermore, public health campaigns and community-based initiatives are essential to raise awareness and provide accessible resources to empower postmenopausal women with the knowledge and attitudes necessary for effective PMOP management and prevention.20,21 Compared with studies conducted in other regions, including the Middle East, Southeast Asia, and Europe, variations in awareness levels and preventive practices may be influenced by differences in healthcare systems, access to screening, and cultural attitudes toward osteoporosis management. These international differences further highlight the need for context-specific strategies in China.
The study discerned significant variations in knowledge and attitude scores among postmenopausal women, with educational levels, monthly per capita income, OP status, history of osteoporotic fractures, and PMOP medication treatment playing pivotal roles. Moreover, disparities related to residence and employment status were associated with varying knowledge scores. Notably, age and the duration of menopause were linked to differing attitude scores. Multivariate logistic regression analysis further underscored the independent influence of higher education and PMOP medication treatment on knowledge, while the lack of awareness about one’s PMOP condition was independently associated with knowledge and attitude scores. These findings underscore the multifaceted determinants of knowledge and attitudes among postmenopausal women, highlighting the need for targeted interventions and educational initiatives that consider these diverse factors to enhance clinical practice, particularly in the context of PMOP management and prevention.22,23
What This Study Adds
The distribution of knowledge among participants underscores significant deficiencies in understanding various aspects of PMOP. Notably, a substantial proportion of participants (48.93%) reported being uncertain about their osteoporosis status, which may reflect limited diagnostic awareness and insufficient access to screening services among postmenopausal women. In particular, awareness of estrogen therapy-related knowledge was notably low, with only 13.30% of participants reporting clear understanding. Given the important role of estrogen in the prevention and management of postmenopausal osteoporosis, this finding highlights a critical gap between clinical recommendations and patient awareness. These findings necessitate a focused approach to enhance clinical practice and promote better PMOP management and prevention. Initiatives should include comprehensive education campaigns addressing the root causes of these knowledge gaps, with particular emphasis on estrogen therapy, fracture risk awareness, and appropriate screening strategies.18,24 By addressing the specific areas of misunderstanding identified in the study, healthcare providers and public health practitioners can deliver tailored interventions. These interventions should emphasize the importance of understanding the impact of estrogen deficiency on OP, the role of family history as a risk factor that necessitates more vigilant screening, and the influence of lifestyle factors. Preventive measures such as calcium and vitamin D supplementation, regular exercise, and Bone Mineral Density (BMD) examination should be highlighted to effectively manage and reduce the risk of postmenopausal OP.25,26 Moreover, a clear discrepancy was observed between knowledge and behavior. Although a relatively high proportion of participants were aware of the benefits of sunlight exposure, actual practices remained suboptimal, with many participants reporting limited or no sun exposure. This inconsistency further supports the existence of a knowledge–practice gap identified in this study. In addition, addressing the potential benefits and risks of estrogen therapy, as well as the consequences of osteoporotic fractures, should be a fundamental component of these educational programs.17,27
The distribution of attitudes highlights various gaps and misconceptions in the perception of PMOP, warranting targeted efforts to improve clinical practice in this context. Notably, 42.70% of participants agreed or strongly agreed that PMOP would not threaten their life, reflecting a potentially dangerous misconception that may reduce the perceived urgency of prevention and early intervention. To address these deficiencies, there is a critical need for comprehensive and tailored educational initiatives focusing on altering attitudes and beliefs regarding PMOP, combined with behavioral support strategies to facilitate the translation of attitudes into actual preventive practices. Healthcare providers and public health practitioners can play a pivotal role in promoting increased awareness of the risks associated with PMOP, emphasizing the importance of regular BMD examination regardless of menopausal status for women over 40 years old and dispelling the misconception that PMOP poses no threat to life.28,29 The significance of comorbidities as risk factors for PMOP and the potential for prevention and treatment must also be underlined. Furthermore, it is vital to advocate for proactive education and the importance of PMOP prevention measures.18
The distribution of practices among postmenopausal women reveals several areas of concern and room for enhancement in clinical practice. These findings also suggest the presence of a subgroup with relatively higher knowledge but suboptimal practices, highlighting the need for clinicians to identify and provide targeted support for individuals with a knowledge–behavior gap. Notably, a discrepancy was observed between calcium supplementation behavior and osteoporosis medication treatment. While a high proportion of participants reported never taking calcium supplements, only a small percentage received formal osteoporosis treatment, which may reflect differences between general dietary supplementation behaviors and clinically prescribed pharmacological treatments. Addressing these deficiencies necessitates targeted strategies to promote better practices related to PMOP prevention and management. Promoting a more active lifestyle and engaging in regular exercise, specifically weight-bearing and balance-enhancing activities, should be encouraged as part of daily routines.30–32 Although most participants reported engaging in aerobic exercise, the adoption of strength and balance training, both critical for osteoporosis prevention, was notably low. This imbalance in exercise patterns may partially explain why knowledge does not translate into optimal preventive practices. Additionally, it is crucial to educate women about the benefits of sun exposure for vitamin D synthesis. These initiatives should also consider women’s preferences for information sources, utilizing both traditional and modern channels, such as television, newspapers, magazines, the internet, and social media. In conjunction with public health campaigns and educational interventions, these approaches can help bridge the knowledge-practice gap and ultimately improve clinical practice in PMOP prevention and management.33,34
The correlation and SEM results reveal a complex relationship between knowledge, attitude, and practice in postmenopausal PMOP. The positive correlation between knowledge and attitude aligns with existing literature, confirming that increased knowledge leads to more favorable attitudes toward prevention.35,36 However, the weak and non-significant association between attitude and practice (β = 0.049, P = 0.619) suggests that while individuals may hold positive attitudes, these may not necessarily translate into preventive actions. Furthermore, the negative association between knowledge and practice points to a disconnect between awareness and action, suggesting that other factors, such as accessibility, perceived barriers, or insufficient behavioral support, may influence the adoption of preventive measures.37 This finding may also reflect that individuals with greater knowledge are more aware of the complexity of prevention, potential treatment limitations, or their own risk status, which may lead them to report their behaviors more cautiously. In addition, it is possible that women with higher knowledge levels may already have poorer bone health, previous symptoms, or greater perceived vulnerability, which could increase their awareness while simultaneously limiting their ability or motivation to engage in preventive behaviors. Another possible explanation is that greater awareness of osteoporosis-related risks may, in some individuals, induce worry or avoidance rather than proactive behavioral change. Therefore, the observed negative association should be interpreted cautiously and may reflect the combined influence of psychological, behavioral, and unmeasured clinical factors. These findings emphasize the need for multifaceted interventions that enhance both knowledge and the practical implementation of preventive strategies. Importantly, the negative association between knowledge and practice suggests that traditional education-based approaches alone may be insufficient. Behavioral change strategies, such as motivational interviewing, goal-setting, and reinforcement-based interventions, may be necessary to bridge the gap between knowledge and action.
Limitations of This Study
This study has several limitations. First, its cross-sectional design precludes the establishment of causal relationships; therefore, all observed relationships should be interpreted as associations rather than causal effects. Second, the use of self-administered questionnaires may introduce response bias, and the single-center setting may limit the generalizability of the findings. In addition, the reliance on self-reported data may result in recall bias and social desirability bias, as participants may provide answers they perceive as socially acceptable rather than reflecting their true attitudes and practices. Furthermore, the small number of participants reporting smoking or excessive alcohol consumption may have limited the reliability of subgroup comparisons for these variables. The recruitment of participants from health examination centers and nearby communities may also introduce sampling bias, as women with extremely poor health status or those less engaged in healthcare services may be underrepresented. Moreover, although the questionnaire demonstrated good internal consistency, its validity was not formally assessed. Certain items (eg, those related to estrogen therapy) may also be influenced by cultural and clinical practice patterns in China, where hormone replacement therapy is less commonly utilized. Finally, although the SEM demonstrated acceptable model fit, the indices were marginal, and the possibility of unmeasured confounding factors cannot be excluded.
Conclusion
In conclusion, this study highlights a gap in knowledge and suboptimal practices regarding PMOP among postmenopausal women, despite a moderate attitude toward the condition. Notably, higher knowledge levels were associated with poorer preventive practices, suggesting that knowledge alone may not be sufficient to promote appropriate health behaviors. Therefore, interventions should not only focus on improving awareness but also address behavioral, perceptual, and practical barriers to effectively translate knowledge into action, thereby improving osteoporosis prevention practices.
Abbreviations
KAP, Knowledge, attitude, and practice; PMOP, Postmenopausal osteoporosis; OP, Osteoporosis; BMD, Bone mineral density; SEM, Structural equation model; RMSEA, Root mean square error of approximation; IFI, Incremental fit index; TLI, Tucker-Lewis index; CFI, Comparative fit index.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The study received ethical approval from the Committee on Medical Ethics of the First Affiliated Hospital of Anhui Medical University (Approval No. 2024-01-67), and informed consent was obtained from the participants. The study was carried out in accordance with the applicable guidelines and regulations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Research Project for the Returned Overseas Chinese Scholars, Anhui Province Human Resources and Social Security bureau (2020LCX003), Research Project for the Advanced Returned Overseas Chinese Scholars, Ministry of Human Resources and Social Security of the People’s Republic of China, and Anhui Provincial Natural Science Foundation, Science and Technology Department of Anhui Province (2208085QH242); 2020 Youth Science Fund Training Program Project of the National Natural Science Foundation, the First Affliated Hospital of Anhui Medical University (2020kj15).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Goroll AH, Mulley AG. Primary Care Medicine: Office Evaluation and Management of the Adult Patient.
2. Zeng Q, Li N, Wang Q, et al. The prevalence of osteoporosis in China, a nationwide, multicenter DXA survey. J Bone Miner Res. 2019;34(10):1789–15. doi:10.1002/jbmr.3757
3. Cui Z, Meng X, Feng H, et al. Estimation and projection about the standardized prevalence of osteoporosis in mainland China. Arch Osteoporosis. 2019;15(1):2. doi:10.1007/s11657-019-0670-6
4. Cooper C. Epidemiology of osteoporosis. Osteoporosis Int. 1999;9(Suppl 2):S2–8. doi:10.1007/PL00004156
5. Shu J, Li J, Fu Y, et al. Association of ESR1 polymorphism rs2234693 and rs9340799 with postmenopausal osteoporosis in a Chinese population. BMC Musculoskelet Disord. 2020;21(1):346. doi:10.1186/s12891-020-03359-2
6. Khalid A, Haque S, Alvi S, et al. Promoting health literacy about cancer screening among Muslim immigrants in Canada: perspectives of Imams on the role they can play in community. J Prim Care Community Health. 2022;13:21501319211063051. doi:10.1177/21501319211063051
7. Koni A, Taha S, Daifallah A, et al. A cross-sectional evaluation of knowledge, attitudes, practices, and perceived challenges among Palestinian pharmacists regarding COVID-19. SAGE Open Med. 2022;10:20503121211069278. doi:10.1177/20503121211069278
8. Shubayr MA, Kruger E, Tennant M. Oral health providers’ views of oral health promotion in Jazan, Saudi Arabia: a qualitative study. BMC Health Serv Res. 2023;23(1):214. doi:10.1186/s12913-023-09170-8
9. Elwakil W, El Gaafary M, El Miedany Y. Screening and management of osteoporosis: a survey of knowledge, attitude, and practice among healthcare professionals in Egypt-a study by the Egyptian Academy of Bone Health. Osteoporosis Int. 2023;35:93–103. doi:10.1007/s00198-023-06914-4
10. Lo SST, Kok WM. Osteoporosis knowledge, health beliefs, and self-efficacy in Hong Kong Chinese men. Arch Osteoporosis. 2022;17(1):60. doi:10.1007/s11657-022-01104-x
11. Tabor E, Kuźniewicz R, Zagórski P, Martela K, Pluskiewicz W. The relationship of knowledge of osteoporosis and bone health in postmenopausal women in Silesia osteo active study. J Clin Densitom. 2018;21(1):98–104. doi:10.1016/j.jocd.2016.08.005
12. El Hage C, Hallit S, Akel M, Dagher E. Osteoporosis awareness and health beliefs among Lebanese women aged 40 years and above. Osteoporosis Int. 2019;30(4):771–786. doi:10.1007/s00198-019-04901-2
13. Lai PS, Chua SS, Chan SP, Low WY. The validity and reliability of the Malaysian osteoporosis knowledge tool in postmenopausal women. Maturitas. 2008;60(2):122–130. doi:10.1016/j.maturitas.2008.04.006
14. Lee F, Suryohusodo AA. Knowledge, attitude, and practice assessment toward COVID-19 among communities in East Nusa Tenggara, Indonesia: a cross-sectional study. Front Public Health. 2022;10:957630. doi:10.3389/fpubh.2022.957630
15. Okumus M, Ceceli E, Tasbas O, Kocaoglu S, Akdogan S, Borman P. Educational status and knowledge level of pre- and postmenopausal women about osteoporosis and risk factors: a cross-sectional study in a group of Turkish female subjects. J Back Musculoskelet Rehabil. 2013;26(3):337–343. doi:10.3233/BMR-130389
16. Kang J, Zhu X, Kan Y, Zhuang S. Application of the knowledge, attitude, and practice model combined with motivational interviewing for health education in female patients with systemic lupus erythematosus. Medicine. 2023;102(12):e33338. doi:10.1097/MD.0000000000033338
17. Soen S, Arai Y, Matsuda S, Emori K, Ikezaki T, Osawa M. A 3-year postmarketing study on the safety and effectiveness of once-monthly risedronate in Japanese patients with osteoporosis. Osteoporos Sarcopenia. 2020;6(4):191–198. doi:10.1016/j.afos.2020.11.002
18. Albrecht BM, Stalling I, Foettinger L, Recke C, Bammann K. Adherence to lifestyle recommendations for bone health in older adults with and without osteoporosis: cross-sectional results of the OUTDOOR ACTIVE study. Nutrients. 2022;14(12):2463. doi:10.3390/nu14122463
19. Courtalin M, Verkindt H, Oukhouya Daoud N, et al. An evaluation of the implementation of the European Calcified Tissue Society recommendations on the prevention and treatment of osteoporosis secondary to bariatric surgery. Nutrients. 2023;15(4):1007. doi:10.3390/nu15041007
20. Evensen E, Skeie G, Wilsgaard T, et al. How is adolescent bone mass and density influenced by early life body size and growth? The Tromsø study: fit futures-a longitudinal cohort study from Norway. JBMR Plus. 2018;2(5):268–280. doi:10.1002/jbm4.10049
21. Li H, Wu W, He X, et al. Applying vibration in early postmenopausal osteoporosis promotes osteogenic differentiation of bone marrow-derived mesenchymal stem cells and suppresses postmenopausal osteoporosis progression. Biosci Rep. 2019;39(9). doi:10.1042/BSR20191011
22. Ma YC, Jiang JL, Lin YC. The outcome-present state test model of clinical reasoning to promote critical thinking in psychiatric nursing practice among nursing students: a mixed research study. Healthcare. 2023;11(4).
23. Park H, Cho H. Effects of a self-directed clinical practicum on self-confidence and satisfaction with clinical practicum among south Korean nursing students: a mixed-methods study. Int J Environ Res Public Health. 2022;19(9).
24. Xia N, Cai Y, Wang W, et al. Association of bone-related biomarkers with femoral neck bone strength. BMC Musculoskelet Disord. 2022;23(1):482. doi:10.1186/s12891-022-05427-1
25. Bi X, Liu F, Zhang X, et al. Vitamin D and calcium supplementation reverses Tenofovir-caused bone mineral density loss in people taking ART or PrEP: a systematic review and meta-analysis. Front Nutr. 2022;9:749948. doi:10.3389/fnut.2022.749948
26. Mortensen C, Tetens I, Kristensen M, Snitkjaer P, Beck AM. Adherence and barriers to the vitamin D and calcium supplement recommendation at Danish nursing homes: a cross-sectional study. BMC Geriatr. 2022;22(1):27. doi:10.1186/s12877-021-02719-4
27. Harahap IA, Suliburska J. Probiotics and isoflavones as a promising therapeutic for calcium status and bone health: a narrative review. Foods. 2021;10(11):2685. doi:10.3390/foods10112685
28. Panithanang B, Srithongklang W, Kompor P, et al. The effect of health behavior modification program for liver fluke prevention among the Risk Group in Rural Communities, Thailand. Asian Pac J Cancer Prev. 2018;19(9):2673–2680. doi:10.22034/APJCP.2018.19.9.2673
29. Shaikh BT, Laghari AK, Durrani S, Chaudhry A, Ali N. Supporting tuberculosis program in active contact tracing: a case study from Pakistan. Infect Dis Poverty. 2022;11(1):42. doi:10.1186/s40249-022-00965-1
30. Cullen M, Cadogan C, George S, et al. Key stakeholders’ views, experiences and expectations of patient and public involvement in healthcare professions’ education: a qualitative study. BMC Med Educ. 2022;22(1):305. doi:10.1186/s12909-022-03373-z
31. Johansen H, Grøndahl VA, Helgesen AK. Palliative care in home health care services and hospitals - the role of the resource nurse, a qualitative study. BMC Palliat Care. 2022;21(1):64. doi:10.1186/s12904-022-00956-x
32. Ohashi C, Akiguchi S, Ohira M. Development of a remote health monitoring system to prevent frailty in elderly home-care patients with COPD. Sensors. 2022;22(7):2670. doi:10.3390/s22072670
33. Garefino VE, Milton SL. Influence of sunlight on Vitamin D and health status in Green (Chelonia mydas) Sea Turtles with Fibropapillomatosis. Animals. 2022;12(4). doi:10.3390/ani12040488
34. Silvestro D, Villette C, Delecolle J, et al. Vitamin D(5) in Arabidopsis thaliana. Sci Rep. 2018;8(1):16348. doi:10.1038/s41598-018-34775-z
35. Khanal S, Rajbanshi M, Rana A, et al. Knowledge, attitude, and practice regarding the prevention of osteoporosis among middle and old-aged women of Kirtipur Municipality, Nepal. PLoS One. 2024;19(10):e0312738. doi:10.1371/journal.pone.0312738
36. Saltık H, Öztürk F, Emiroğlu C, Hekimoğlu B, Aypak C. Knowledge, attitude, and behavior levels of postmenopausal women about osteoporosis. J Bone Metab. 2023;30(4):347–354. doi:10.11005/jbm.2023.30.4.347
37. Barber K, Charles A. Barriers to accessing effective treatment and support for menopausal symptoms: a qualitative study capturing the behaviours, beliefs and experiences of key stakeholders. Patient Prefer Adherence. 2023;17:2971–2980. doi:10.2147/PPA.S430203
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nursing Students’ Knowledge, Attitude, and Practice Regarding Disaster Preparedness: A Cross-Sectional Study
Mohamed NA, Abdel-Aziz HR, Elsehrawy MG
Risk Management and Healthcare Policy 2023, 16:2427-2437
Published Date: 14 November 2023
Knowledge, Attitudes, and Practices Among Patients with Systemic Lupus Erythematosus Toward Disease Management and Biologic Therapy
Liu X, Song Y, Wan L, Du R
Journal of Multidisciplinary Healthcare 2024, 17:937-947
Published Date: 2 March 2024
Knowledge, Attitudes and Practices Towards Psoriasis Among Patients and Their Family Members
Zhang X, Du H, Liu X, Liu L, Zhang T
Clinical, Cosmetic and Investigational Dermatology 2024, 17:769-782
Published Date: 3 April 2024
Knowledge, Attitude and Practice of Radiologists Regarding Artificial Intelligence in Medical Imaging
Huang W, Li Y, Bao Z, Ye J, Xia W, Lv Y, Lu J, Wang C, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:3109-3119
Published Date: 4 July 2024
Knowledge, Attitudes, and Practices Among Community Populations Toward Long COVID in China
He N, Tunala S, Wu R, Zhao C, Wuren T, Hushuud C
International Journal of General Medicine 2024, 17:4455-4463
Published Date: 1 October 2024