Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Plasminogen Activator Inhibitor-1 4G/5G (rs1799889) Polymorphism in Chinese Patients with Diabetes Mellitus and Hypertension
Authors Wang Z, Chen J ![]() , Song J, Kong L, Wang X, Xu T
, Song J, Kong L, Wang X, Xu T ![]() , Lin S, Dou Y
, Lin S, Dou Y
Received 1 March 2023
Accepted for publication 18 April 2023
Published 22 April 2023 Volume 2023:16 Pages 1133—1147
DOI https://doi.org/10.2147/DMSO.S410682
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Ziran Wang,1 Jintu Chen,2 Jingjing Song,3 Lingjun Kong,1 Xuanzhi Wang,4 Tengda Xu,5 Songbai Lin,5 Yaling Dou1
1Department of Clinical Laboratory, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 2Department of Clinical Laboratory, Quanzhou First Hospital Affiliated to Fujian Medical University, Quanzhou, Fujian, People’s Republic of China; 3Department of Clinical Laboratory, Anhui Provincial Maternal and Child Health Hospital, Hefei, Anhui, People’s Republic of China; 4Department of Medical Laboratory, North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China; 5Department of Health Management, Peking Union Medical College Hospital, Beijing, People’s Republic of China
Correspondence: Yaling Dou, Department of Clinical Laboratory, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing, 100730, People’s Republic of China, Email [email protected]
Objective: To determine the plasminogen activator inhibitor-1 (PAI-1) 4G/5G (rs1799889) genotype of the subjects in a robust detection method and to explore the association of the PAI-1 4G/5G polymorphism with susceptibility to diabetes mellitus (DM) and hypertension (HTN) as well as clinical characteristics.
Methods: This study recruited 208 patients (68 patients were diagnosed with DM, 70 patients with HTN and 70 patients with DM combined with HTN) and 132 healthy controls (HC). A subset of the population was selected to evaluate the accuracy of the Real-time PCR (RT-PCR) method for detecting PAI-1 4G/5G polymorphism by using the sequencing method as the gold standard. Furthermore, the association of the PAI-1 4G/5G polymorphism with genetic susceptibility to DM and HTN was explored. Moreover, variations in clinical characteristics among individuals with various PAI-1 genotypes were also analyzed in the DM group, the HTN group and the DM+HTN group.
Results: There was a high concordance between the RT-PCR method and the sequencing method in determining the PAI-1 4G/5G polymorphism. No association was observed between the PAI-1 4G/5G polymorphism and susceptibility to DM, HTN and DM+HTN, respectively. There were no statistical differences in all study indicators among individuals that carrying various genotypes in the HC group. There were several variations in clinical characteristics among individuals harboring different PAI-1 4G/5G genotypes in the DM group, the HTN group and the DM+HTN group.
Conclusion: The RT-PCR method can accurately identify the PAI-1 4G/5G genotype in different individuals. The PAI-1 4G/5G polymorphism may not be associated with genetic susceptibility to DM, HTN and DM+HTN, but differences in clinical characteristics among individuals with various genotypes may provide a reference for disease assessment and personalized treatment of patients.
Keywords: diabetes mellitus, hypertension, plasminogen activator inhibitor-1, gene polymorphism
Introduction
Diabetes mellitus (DM) is a group of metabolic syndromes characterized by disorders of glucose metabolism, including type 1 DM, type 2 DM, gestational DM, and specific types of DM due to other causes. DM is closely associated with abnormal cardiac electrophysiological signal conduction and arrhythmias, whereby it triggers sudden cardiac death (SCD) as a leading cause of death.1 Besides, DM may cause a variety of complications, including retinopathy, nephropathy, and peripheral neuropathy; long-term hyperglycemia-induced microvascular changes can eventually lead to multiple organ damage, dysfunction and even failure.2 In China, the prevalence of DM has risen dramatically from less than 1% in the 1980s to 9–12% in recent years.3 Notably, in a cross-sectional nationally representative survey in 2018, the estimated prevalence of DM reached 12.4%, within more than 60% of adults with DM were unaware of their condition.4 Hypertension (HTN) is a cardiovascular syndrome with elevated arterial pressure in the body circulation, and can be divided into essential HTN and secondary HTN. HTN is identified as a source of abnormal myocardial structural remodeling and myocardial dysfunction, which might further lead to left heart hypertrophy and heart failure.5 Moreover, HTN is a leading contributor to cardiovascular disease (CVD) and mortality. It was reported that over 10 million people dying from elevated blood pressure in 2019.6 In a population-based screening study (China PEACE Million Persons Project) comprising 1,738,886 adults, 777,282 participants (44.7%) had HTN, only 44.7% of whom were aware of the diagnosis, 30.1% were taking prescribed antihypertensive medications and only 7.2% had achieved control.7 In many cases, DM and HTN often appear together, significantly increasing the risk of cardiovascular-related death. Based on the huge population of China, DM and HTN pose a huge disease burden on society.
The etiology of DM and HTN is diverse and complex, with a combination of genetic factors (eg, family history, genetic susceptibility), environmental factors (eg, obesity, smoking, infections, drugs), dietary factors (eg, high glucose diet, high fat diet), psychological factors (eg, stress, agitation), and immune factors (eg, autoantibodies). Among these, genetic factors may not be negligible. In recent years, single nucleotide polymorphisms (SNPs) have been considered to be closely associated with disease susceptibility and have gradually drawn attention.8 In addition to this, SNPs have also been shown to be closely related to drug responsiveness and the safety of therapy.9 On this basis, it would be beneficial to analyze the variations in genetic susceptibility and clinical features of individuals carrying different genotypes to better understand the role of SNPs in the pathogenesis of disease.
As a member of the serpin superfamily, plasminogen activator inhibitor-1 (PAI-1) plays an indispensable role in the fibrinolytic system as it maintains plasminogen/plasmin homeostasis by inhibiting the activation of tissue-type and urokinase-type plasminogen.10 Notably, hypo-fibrinolysis status is a pivotal abnormality in DM. It is strongly associated with unfavorable vascular outcomes, with PAI-1 expression levels often elevated in patients with DM and insulin resistance.11 Furthermore, overproduction of PAI-1 has been proven to be associated with endothelial dysfunction, which increases the risk of HTN.12 Thus, PAI-1 may be a driver in the pathogenic process of DM and HTN. With the development of sequencing technology, the genetic polymorphisms of PAI-1 have gradually been unveiled. Among these, the guanine (G) insertion/deletion (5G or 4G) polymorphism at position 675 in the promoter region of the PAI-1 gene (rs1799889) was more common.13 Insertion/deletion polymorphism is currently being identified and investigated in numerous genes, such as angiotensin-converting enzyme (ACE) gene14 and interleukin-1A 3’untranslated region.15 For the PAI-1 gene, a five-guanine nucleotide bundle at position 675 in the promoter region, called the 5G allele, is considered the major allele, while deletion of one G nucleotide results in the 4G allele. The PAI-1 4G/5G polymorphism has been reported to be connected with susceptibility to several diseases, such as venous thrombosis,16 ischemic stroke,17 diabetic nephropathy,18 cancers,19 and systemic lupus erythematosus.20 Nevertheless, the relevance of the PAI-1 4G/5G polymorphism to DM and HTN susceptibility as well as clinical characteristics is still not fully elucidated, especially in Chinese patients.
In this study, we aimed to determine the PAI-1 4G/5G genotype of the subjects in a robust detection method and to explore the association of the PAI-1 4G/5G polymorphism with susceptibility to DM and HTN as well as clinical characteristics.
Materials and Methods
Study Population
This study recruited 208 patients (68 patients were diagnosed with DM, 70 patients with HTN and 70 patients with DM combined with HTN) and 132 healthy controls (HC) at Peking Union Medical College Hospital (PUMCH), Chinese Academy of Medical Sciences from July 2019 to July 2022. The diagnosis of DM was made by the physicians with reference to World Health Organization (WHO) criteria21 based on the patients’ family history, symptoms and laboratory findings. Briefly, the main laboratory criteria were: fasting plasma glucose ≥7.0 mmol/L and/or 2-hour plasma glucose ≥11.1 mmol/L. The diagnosis of hypertension was determined by the physicians according to the Chinese guidelines for the management of hypertension,22 with the main criteria being systolic blood pressure (SBP) ≥ 140 mmHg and/or diastolic blood pressure (DBP) ≥ 90 mmHg. The DM group was defined as the cohort with the diagnosis of DM but not HTN. The HTN group was the cohort with the diagnosis of HTN but not DM, and the DM+HT group was defined as the cohort suffering from both DM and HTN. Meanwhile, healthy individuals with normal blood pressure and no abnormal laboratory test results were included in this study as HC. Each subject was enrolled only once by using the unique identification code.
Study Design
The overall design of this study was presented in Figure 1. The first stage was methodological evaluation, which a subset of the population was selected to evaluate the accuracy of the Real-time PCR (RT-PCR) method for detecting PAI-1 4G/5G polymorphisms by using the sequencing method as the gold standard. The second stage was the disease susceptibility analysis, where five genetic models were used to explore the association of the PAI-1 4G/5G polymorphism with DM and HTN. The last stage was clinical profile analysis, where differences in clinical characteristics were compared among individuals carrying various genotypes.
 |
Figure 1 The overall design of this study. Abbreviations: HC, healthy controls; DM, diabetes mellitus; HTN, hypertension; PAI-1, plasminogen activator inhibitor-1; RT-PCR, real-time PCR. |
Genotyping
EDTA-anticoagulated whole blood samples were collected from all subjects and the DNA was subsequently extracted by using the Blood Genome Extraction Kit (Tianlong Technology Co. LTD, China). The PAI-1 4G/5G genotype of each subject was determined by using the TaqMan-MGB RT-PCR detection kit (Wuhan HealthCare Biotechnology Co. LTD, China) according to the instruction. PCR reactions and data analysis were performed in the Applied Biosystems (ABI) 7500 Real-time System (ABI Inc. CA, United States) instrument and matching software. The VIC, FAM and ROX channels were used to capture the amplification fluorescence signals of 5G allele, 4G allele and β-actin (internal control), respectively. The primer and probe sequences of PAI-1 were as follows: forward primer 5′-GCC AGA CAA GGT TGT TGA CACA-3′; reverse primer 5′-GAG GAC TCT TGG TCT TTC CCT CAT −3′; 5G allele probe 5′-VIC-CTG ACT CCC CCA CGTG-MGB-NFQ-3′; 4G allele probe 5′-FAM-CTG ACT CCC CAC GTGT-MGB-NFQ-3′. The primer and probe sequences of β-actin were as follows: forward primer 5′-TGA AGA TCC TCA CCG AGC G-3′; reverse primer 5′-GGC AGC TCG TAG CTC TTC TC-3′; probe 5′-ROX-ACC ACC ACG GCC GAG CGG -BHQ-3′. In addition, sanger sequencing was also performed as the gold standard to determine the genotypes in the ABI Real-time Prism 3730XL Sequence Detection System (ABI Inc. CA, United States) in accordance with the corresponding protocol.
Clinical Data Collection
Laboratory results, physical examination findings and medical records of all subjects were obtained through the laboratory information system (LIS) and hospital information system (HIS) of PUMCH. The SBP and DBP could be available in the HIS system. White blood cell counts (WBC), red blood cell counts (RBC), hemoglobin (Hb), lymphocyte counts (L), neutrophil counts (N), platelet counts (PLT) were measured with XN-9100 (Sysmex Corporation, Japan). Neutrophil-to-lymphocyte ratio (NLR) was calculated by dividing the absolute neutrophil counts by the absolute lymphocyte counts, whilst platelet-to-lymphocyte ratio (PLR) was calculated by dividing the platelet counts by the absolute lymphocyte counts. Hemoglobin A1c (HbA1c) was measured using the D-100 hemoglobin testing system (Bio-Rad, USA). Serum glucose (Glu), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C) were measured with Beckman AU 5800 (Beckman Coulter, USA).
Statistical Analysis
General information and clinical data of subjects were collected and managed using Excel 2019 (Microsoft, USA). Statistical analysis was conducted using R Project (version 4.2.0) and RStudio (Open-Source Edition) software. The concordance between sequencing method and RT-PCR method was tested using the kappa test. The Hardy-Weinberg equilibrium (HWE) test was used to evaluate the distribution of genotypes. Logistic regression and logistic regression adjusted for age and sex were used to explore the association of the PAI-1 4G/5G polymorphism with the risk of DM and HTN. When comparing differences in clinical characteristics among various groups, the Wilcoxon or t-test was applied for analysis of continuous data while the chi-square test or Fisher’s exact probability for analysis of categorical data. P<0.05 was regarded as statistically significant.
Results
Basic Characteristics of Enrolled Population
A total of 132 HC and 208 patients (68 DM, 70 HTN, 70 DM+HTN) were enrolled in this study. The baseline characteristics of the participants were presented in Table 1. Compared to the HC group, the DM group had higher age, male ratio, SBP, DBP, HbA1c, WBC, L, N, RBC, Hb, Glu and TG while lower PLR, HDL-C (P<0.05). When compared to the HC group, the HTN group had higher age, male ratio, SBP, DBP, HbA1c, WBC, L, N, Glu, TC, TG and LDL-C as well as lower PLR, HDL-C (P<0.05). The DM + HTN group had higher age, male ratio, SBP, DBP, HbA1c, WBC, L, N, RBC, Hb, Glu, TG along with lower HDL-C in comparison to the HC group (P<0.05).
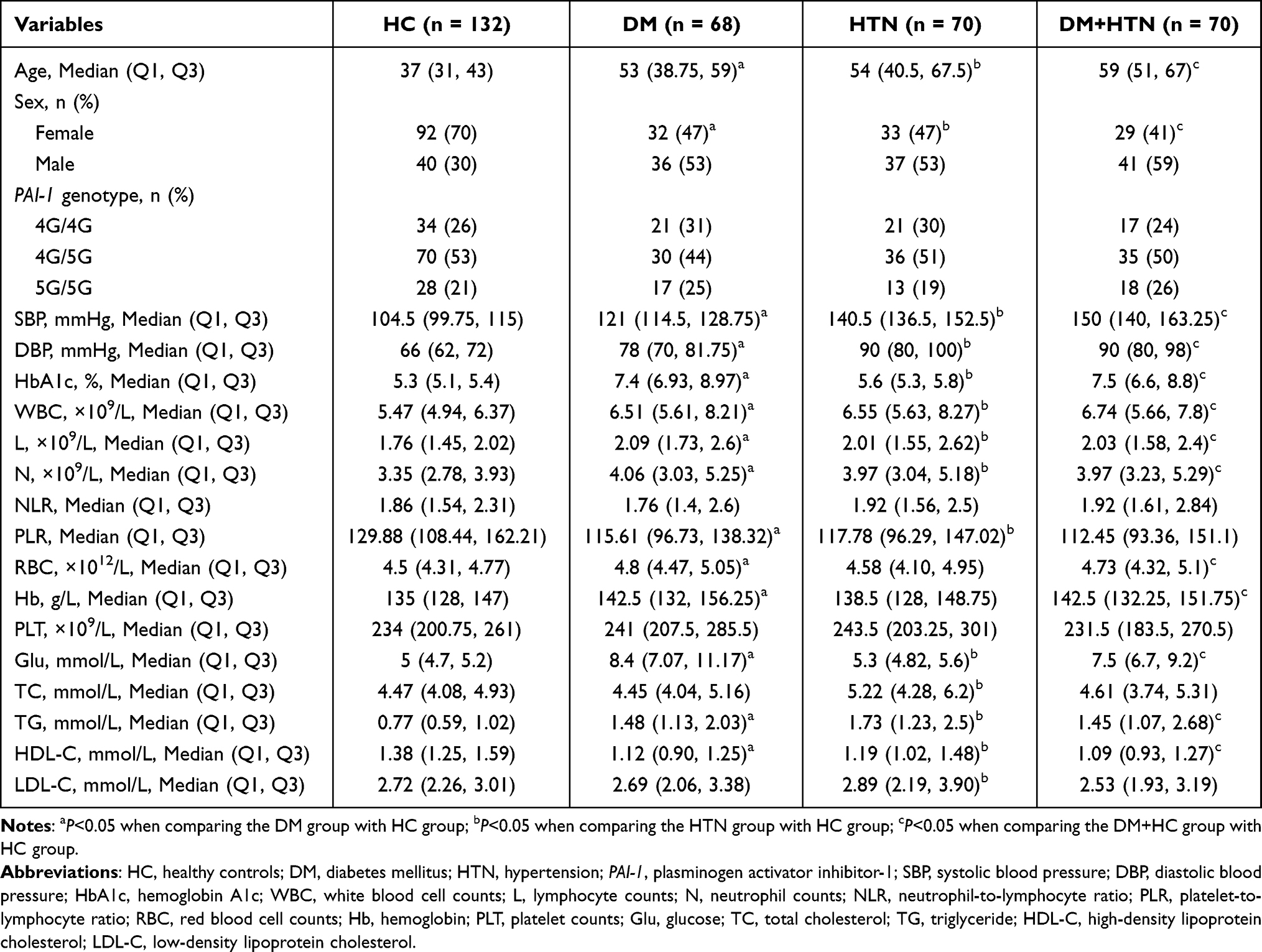 |
Table 1 The Baseline Characteristics of the Participants in This Study |
Methodological Evaluation of the PAI-1 4G/5G Polymorphism
A subgroup of the population (17 DM, 60 HTN, 46 DM+HTN and 60 HC) was selected for methodological evaluation of the PAI-1 4G/5G polymorphism detection. The accuracy of the RT-PCR method for detecting the PAI-1 4G/5G polymorphism was assessed using the sequencing method as the gold standard. The results showed a high concordance between the RT-PCR method and the sequencing method in the diverse groups (Table 2).
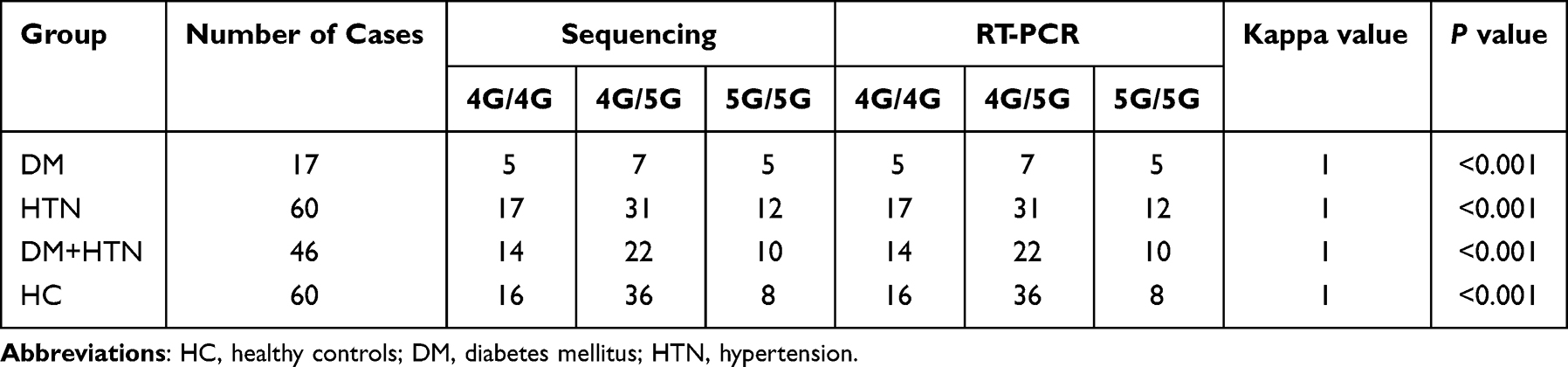 |
Table 2 Detection of the Genotypes of PAI-1 4G/5G by the Sequencing Method and the RT-PCR Method |
PAI-1 4G/5G Genotypes Distribution
As the RT-PCR method exhibited excellent agreement with the sequencing method in methodological evaluation, we used the RT-PCR method to determine the PAI-1 4G/5G genotypes of all participants in this study. As depicted in Table 1, in the HC group, 34 individuals were 4G/4G genotypes, 70 were 4G/5G genotypes and 28 were 5G/5G genotypes. Specifically, 21 individuals in the DM group harbored the 4G/4G genotypes, 30 harbored the 4G/5G genotypes and 17 harbored the 5G/5G genotypes whereas 21 individuals in the HTN group harbored the 4G/4G genotypes, 36 harbored the 4G/5G genotypes and 13 harbored the 5G/5G genotypes. For the DM+HTN group, 17 individuals carried the 4G/4G genotypes, 35 carried the 4G/5G genotypes and 18 carried the 5G/5G genotypes. The HWE test revealed that the 4G/5G genotype frequencies of PAI-1 were in accordance with the genetic equilibrium law (P>0.05, Table 3).
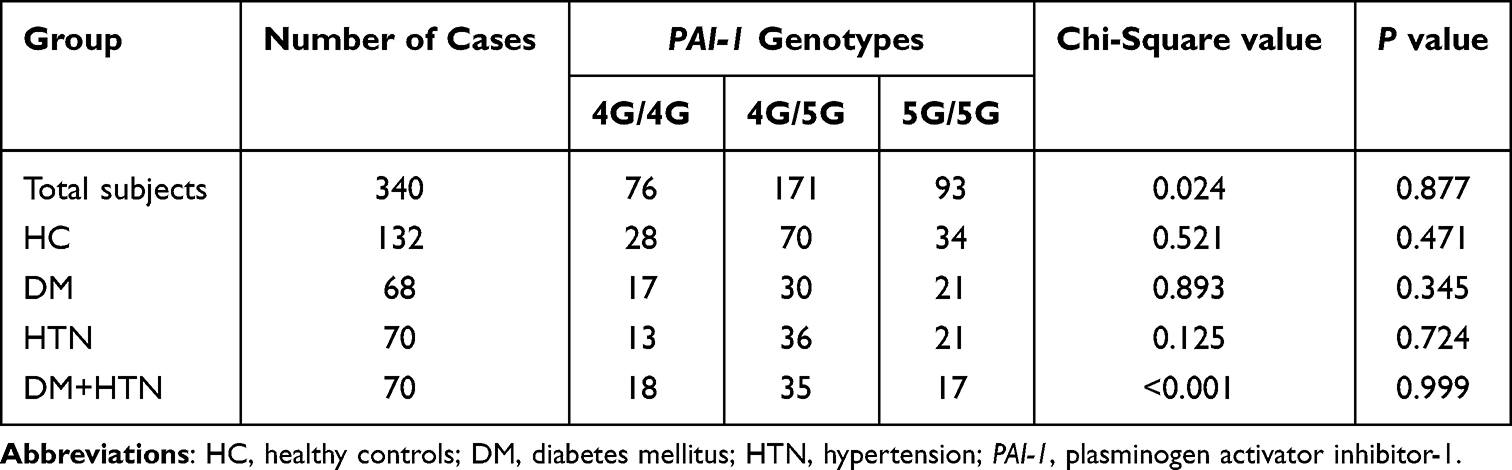 |
Table 3 Results of the Hardy-Weinberg Equilibrium (HWE) Test for Different Groups |
PAI-1 4G/5G Polymorphism and Diseases Susceptibility
To explore the association of the PAI-1 4G/5G polymorphism with DM and HTN susceptibility, five different genetic models (allele, genotype, dominant, recessive, additive) were applied. As shown in Tables 4–6, no association was observed between the PAI-1 4G/5G polymorphism and susceptibility to DM, HTN and DM+HTN, respectively. After adjusting for age and sex, the association of the PAI-1 4G/5G polymorphism with DM, HTN and DM+HTN susceptibility remained absent.
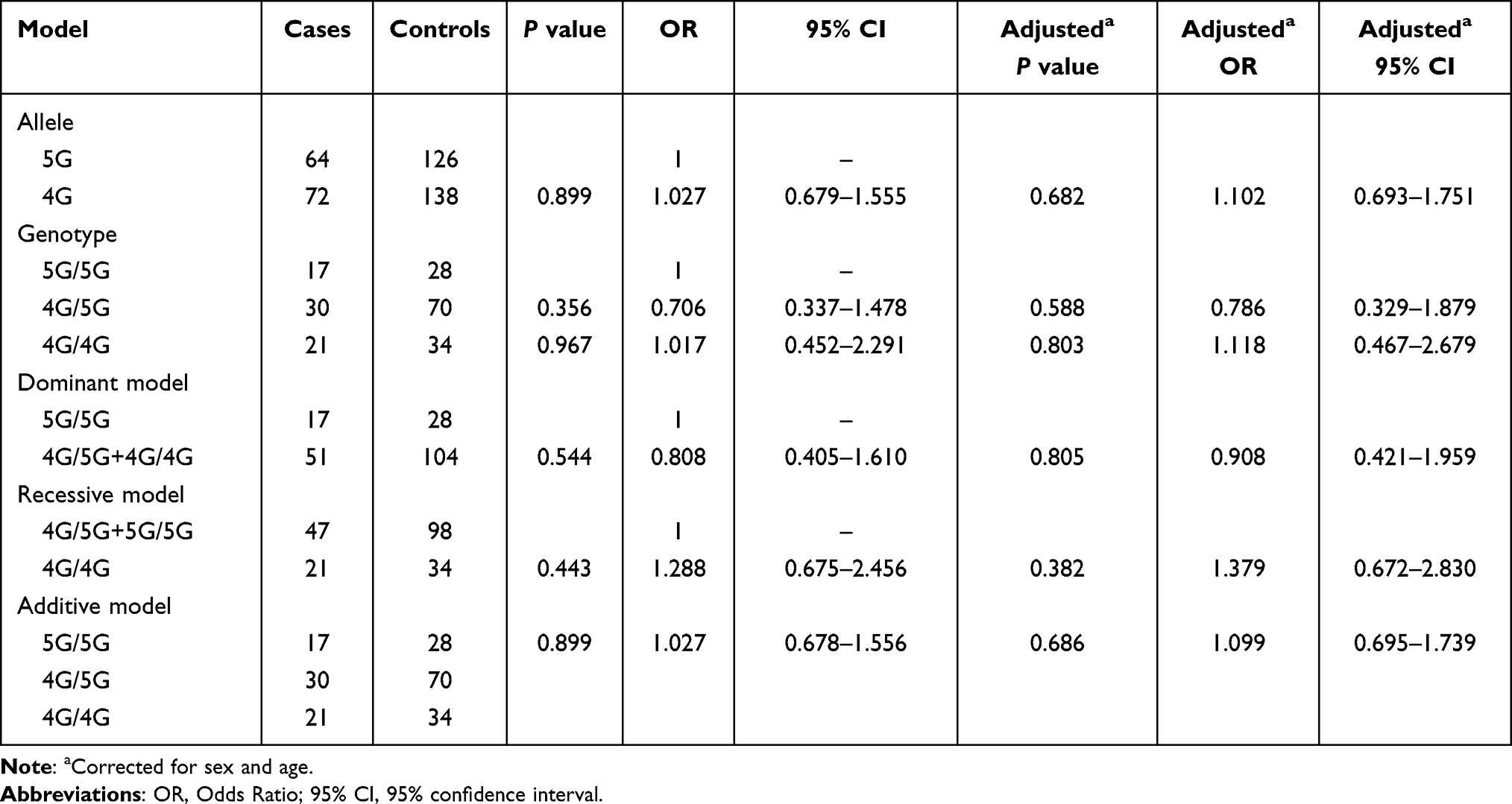 |
Table 4 Analysis of the Association Between the PAI-1 4G/5G Polymorphism and DM Risk |
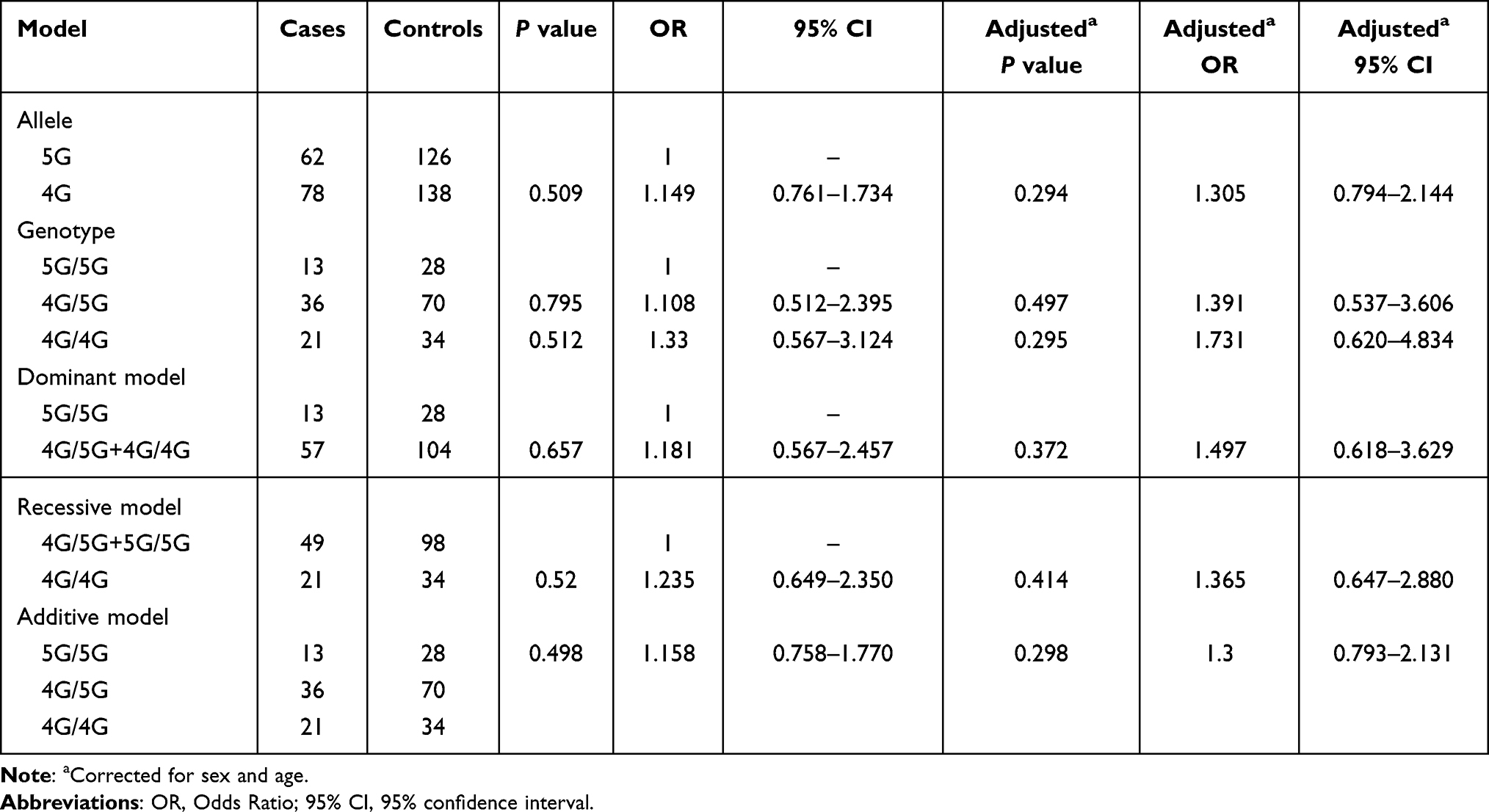 |
Table 5 Analysis of the Association Between the PAI-1 4G/5G Polymorphism and HTN Risk |
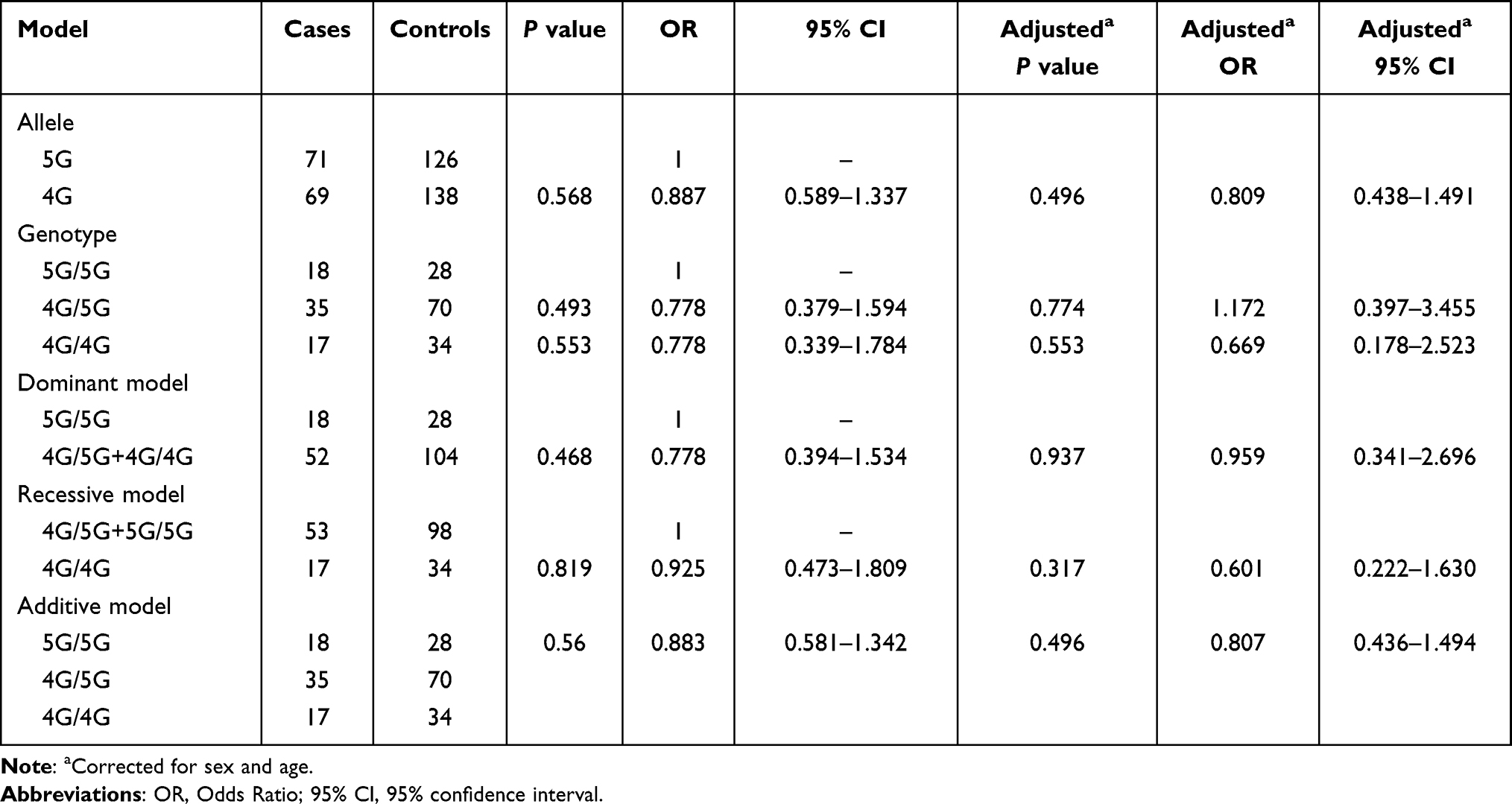 |
Table 6 Analysis of the Association Between the PAI-1 4G/5G Polymorphism and DM+HTN Risk |
Clinical Profile Analysis of PAI-1 Genotypes
To better understand the clinical impact of the PAI-1 4G/5G polymorphism, we compared differences in the clinical characteristics of individuals carrying various genotypes in different cohorts. As illustrated in Figure 2, there were no statistical differences in all study indicators among individuals carrying the 4G/4G, 4G/5G and 5G/5G genotypes in the HC group. For the DM group, individuals carrying the 5G/5G genotype had lower L compared to 4G/5G, while comparisons of other indicators were not statistically significant (Figure 3). In the HTN group, individuals with the 5G/5G genotype had higher RBC and Hb than individuals with the 4G/5G genotype (Figure 4). Considering the inherent variations in RBC and Hb across age and sex, the above differences persisted after correcting for age and sex. Meanwhile, in the HTN group, individuals carrying the 4G/5G and 5G/5G genotypes had higher HbA1c compared to the 4G/4G genotype whilst the 5G/5G individuals had higher Glu compared to the 4G/4G individuals. For the DM+HTN group, individuals carrying the 4G/5G and 4G/4G genotypes had higher WBC and N when compared to the 5G/5G genotype (Figure 5). Furthermore, compared to the 4G/4G genotype, individuals carrying the 4G/5G genotype had lower LDL-C while individuals carrying the 5G/5G genotype had lower TG.
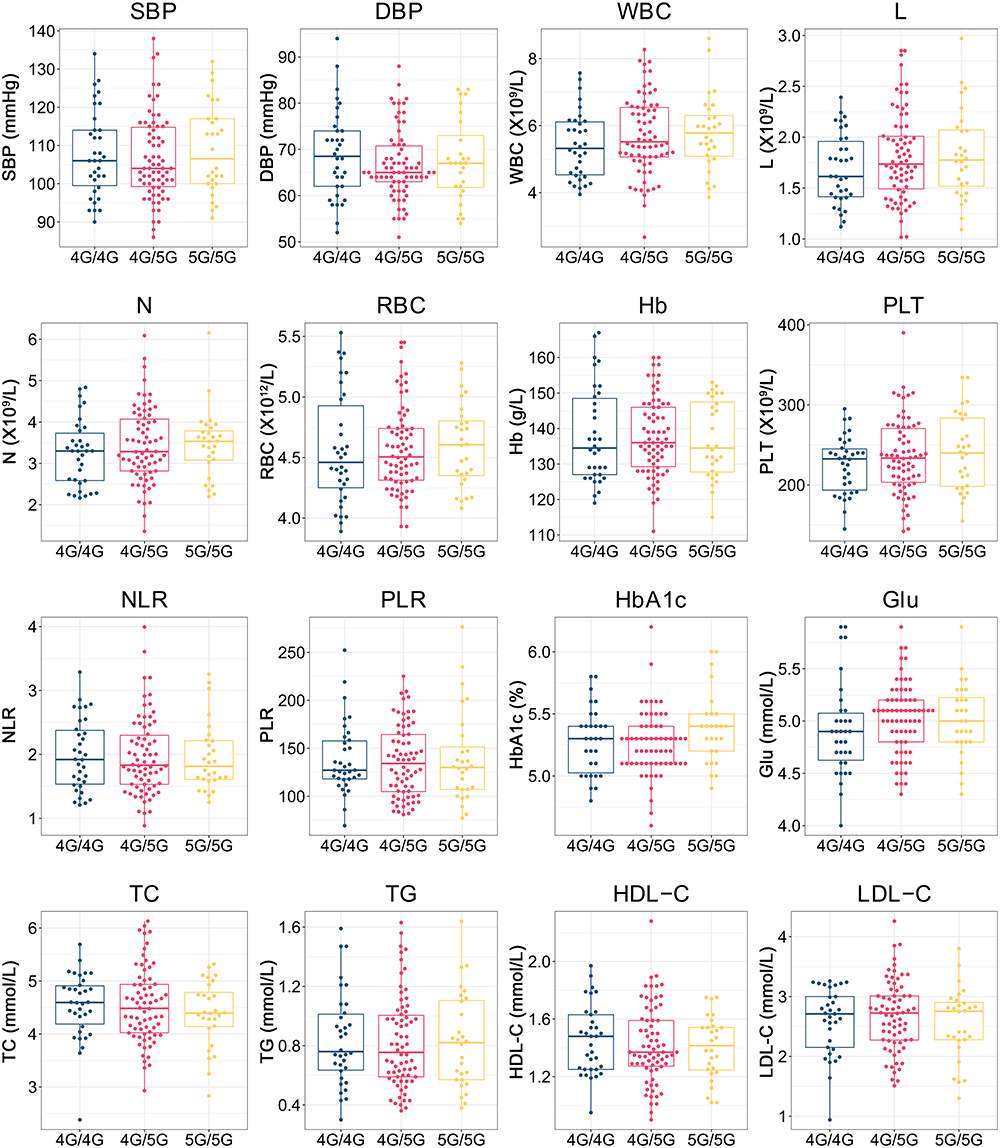 |
Figure 2 Differences in clinical characteristics of individuals carrying various PAI-1 genotypes in the HC cohort. Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure; HbA1c, hemoglobin A1c; WBC, white blood cell counts; L, lymphocyte counts; N, neutrophil counts; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; RBC, red blood cell counts; Hb, hemoglobin; PLT, platelet counts; Glu, glucose; TC, total cholesterol; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol. |
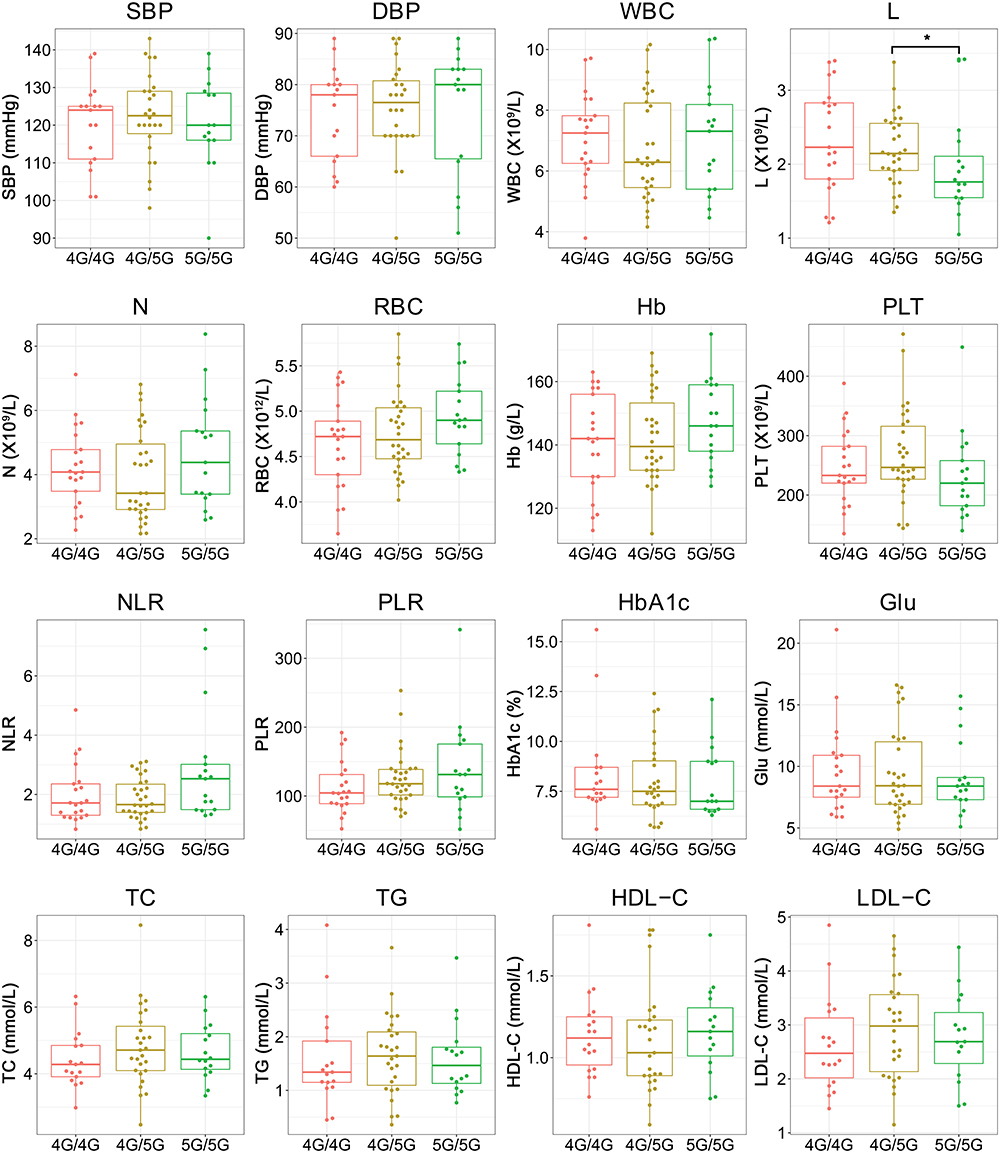 |
Figure 3 Differences in clinical characteristics of individuals carrying various PAI-1 genotypes in the DM cohort. *P<0.05. Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure; HbA1c, hemoglobin A1c; WBC, white blood cell counts; L, lymphocyte counts; N, neutrophil counts; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; RBC, red blood cell counts; Hb, hemoglobin; PLT, platelet counts; Glu, glucose; TC, total cholesterol; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol. |
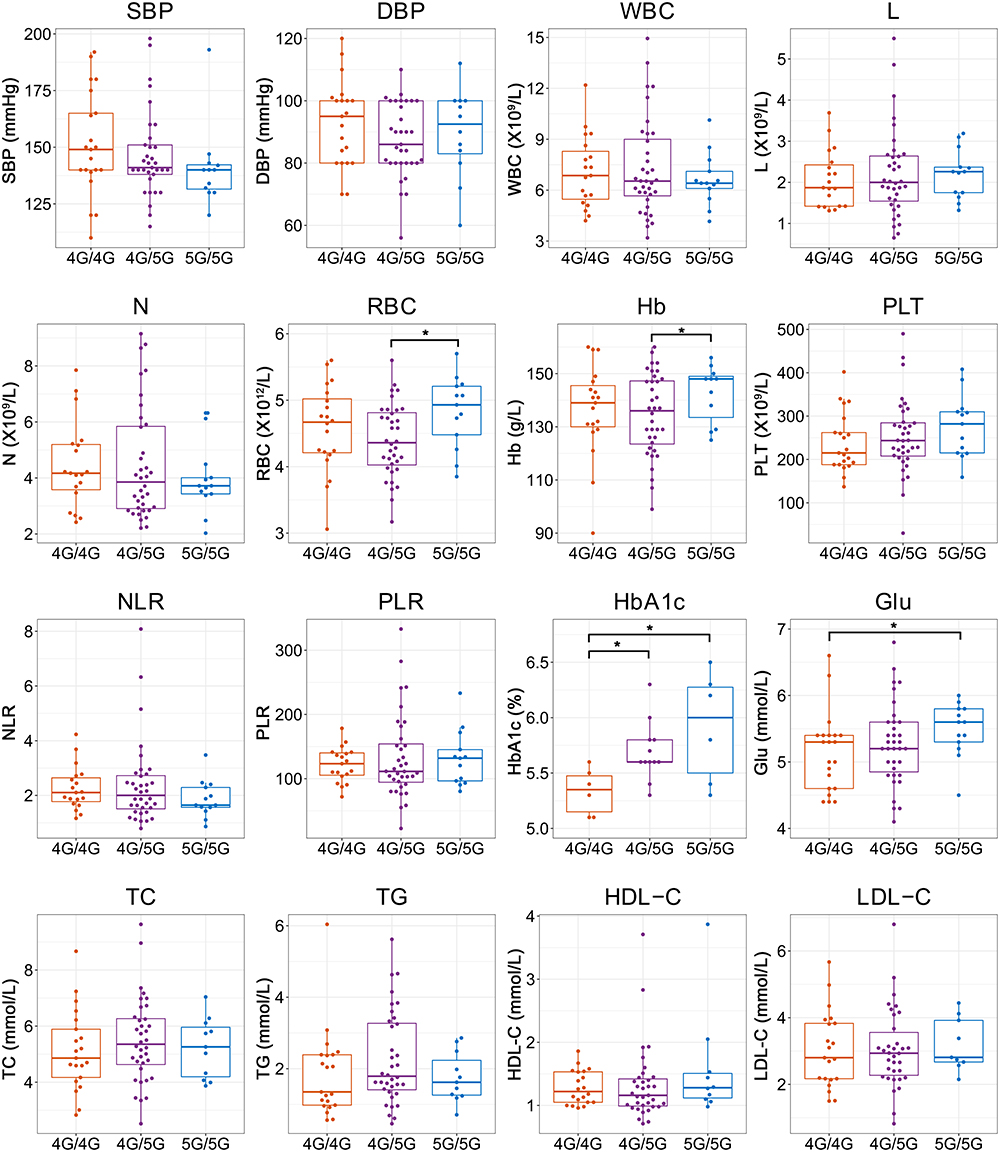 |
Figure 4 Differences in clinical characteristics of individuals carrying various PAI-1 genotypes in the HTN cohort. *P<0.05. Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure; HbA1c, hemoglobin A1c; WBC, white blood cell counts; L, lymphocyte counts; N, neutrophil counts; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; RBC, red blood cell counts; Hb, hemoglobin; PLT, platelet counts; Glu, glucose; TC, total cholesterol; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol. |
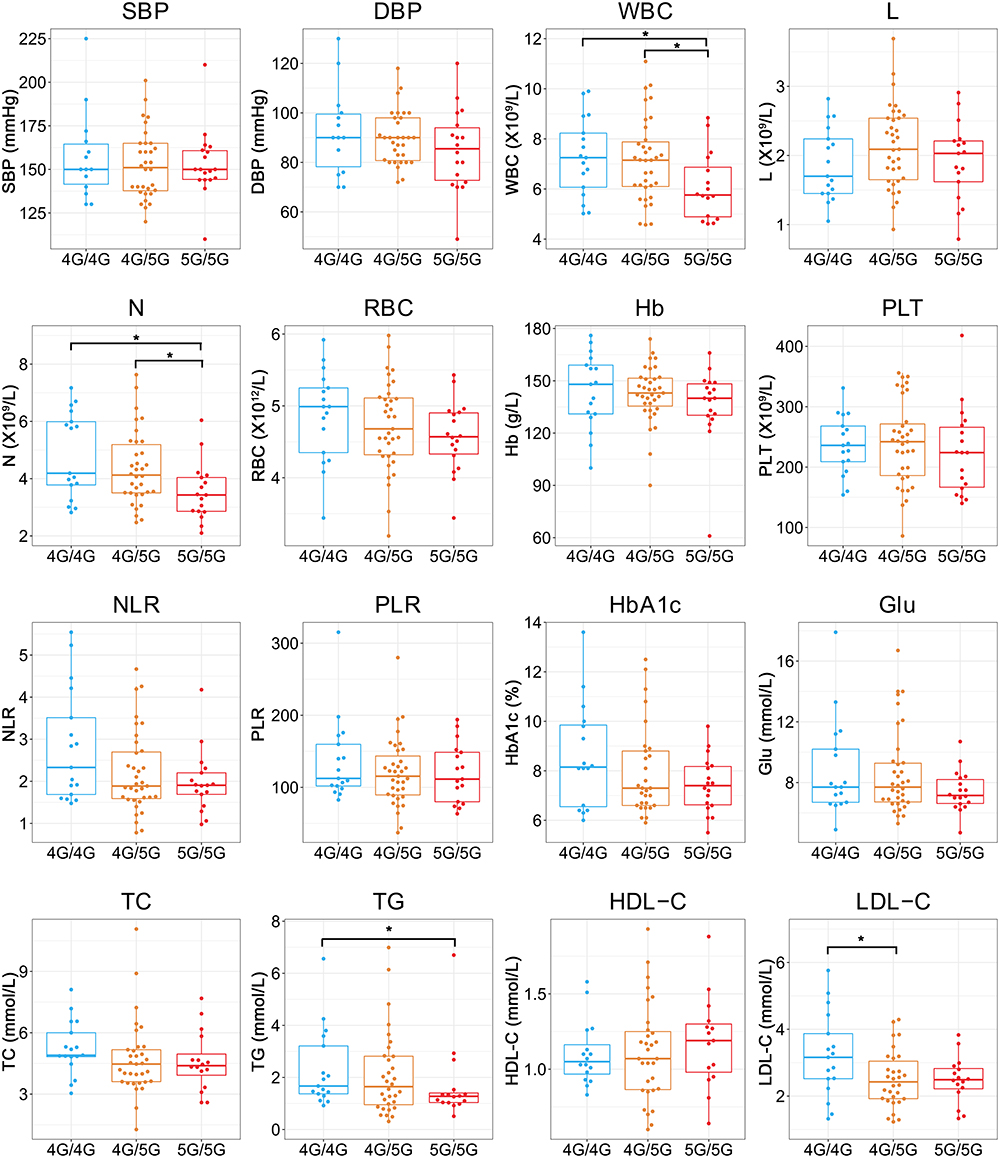 |
Figure 5 Differences in clinical characteristics of individuals carrying various PAI-1 genotypes in the DM+HTN cohort. *P<0.05. Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure; HbA1c, hemoglobin A1c; WBC, white blood cell counts; L, lymphocyte counts; N, neutrophil counts; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; RBC, red blood cell counts; Hb, hemoglobin; PLT, platelet counts; Glu, glucose; TC, total cholesterol; TG, triglyceride; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol. |
Discussion
Due to the large population and lack of health awareness in China, DM and HTN have become the major challenges that threaten the quality of life for the Chinese population. In addition to dietary and emotional factors, hereditary factor is also considered to be a crucial component in the development of DM and HTN. This study focused on exploring the association of the PAI-1 4G/5G polymorphism with susceptibility to DM and HTN and the differences in the clinical characteristics of individuals with various genotypes. Prior to the above analysis, we first evaluated the methodology and found that the RT-PCR method could accurately identify the PAI-1 4G/5G genotypes. After logistic regression analysis and logistic regression analysis adjusted for age and sex, we failed to detect the association of the PAI-1 4G/5G polymorphism with DM and HTN using all five genetic models. Finally, we observed some differences in the clinical characteristics of individuals carrying various genotypes in the DM, HTN and DM+HTN groups. We are convinced that these studies may provide some new perspectives on the role of PAI-1 4G/5G polymorphisms in the development of DM and HTN.
It is known that SNPs may provide abundant information on disease susceptibility and inheritance patterns, but precise localization involving a single base substitution poses high demands on detection methods. In recent years, there has been an explosion in the number of methods for SNP genotyping, of which numerous robust and reliable methods are available. Nevertheless, in clinical practice, it is necessary to consider accuracy, time-effectiveness, cost, and operational complexity to determine the appropriate genotyping method. The common genotyping methods include: sequencing, restricted fragment length polymorphisms (RFLP), gene chips, high-resolution melting (HRM) and RT-PCR methods. As for the gold standard for genotyping, DNA sequencing can accurately identify each base of the sequence, but it is expensive, complex, and not suitable for batch operations. The RT-PCR technique is accurate, rapid, sensitive, and specific, and it is suitable for clinical molecular biology assays. Notably, RT-PCR technique based on TaqMan probes combined with MGB ligands can effectively increase the Tm value of the probes and avoid the generation of non-specific products.23 In present study, the RT-PCR method yielded consistent results with the sequencing method for genotyping in a subset of the population, indicating the high accuracy of the RT-PCR method. Meanwhile, the RT-PCR method enables parallel testing of 96 samples for genotyping in less than 2 hours, making it applicable to large batches of samples. After methodological evaluation, we concluded that the RT-PCR method could precisely identify the PAI-1 4G/5G genotypes which can be used in subsequent studies.
The association of the PAI-1 4G/5G polymorphism with DM and HTN susceptibility was controversial. Miri et al found that the 5G/5G genotype may significantly increase the risk of T2DM in the Iranian population.24 A Meta-analysis conducted by Xu et al included 6 studies containing 1333 patients and 3011 controls demonstrated that the PAI-1 4G/5G polymorphism was not associated with the risk of DM and DM complications.25 This is in line with the results of our study. Our study indicated that the association between the PAI-1 4G/5G polymorphism and DM risk in five genetic models was not evident, even after adjusting for age and sex. The correlation between PAI-1 and HTN is mainly reflected in the contribution of PAI-1 to endothelial dysfunction and vascular remodeling. Jacobs et al pointed out that both PAI-1 activity [OR: 1.04 (1.01, 1.08)] and PAI-1 polymorphisms [4G/4G vs 5G/5G, OR: 1.82 (1.07, 3.12)] can raise the odds of HTN.26 Kim et al observed that carriers of the 4G allele were more likely to develop HTN relative to carriers of the 5G allele in the Korean population.27 These reports contradict our finding that the PAI-1 4G/5G polymorphism does not correlate with HTN susceptibility. The main reasons explaining this discrepancy may be the variations in baseline characteristics and concomitant diseases of patients in the separate studies and the fact that ethnic differences may contribute to biased conclusions. Additionally, we also uncovered that the PAI-1 4G/5G polymorphism was not linked to the risk of concurrent DM and HTN. These results have implicated that the effect of the PAI-1 4G/5G polymorphism in DM and HTN still needs to be further investigated and future multi-center collaborative studies with larger samples are required.
Understanding the diversity of clinical profiles among individuals with different genotypes would help to further investigate the clinical utility of PAI-1 4G/5G polymorphism. After implementing clinical profiles analysis, some interesting observations were presented. In the DM group, the 5G/5G genotype carriers had lower L relative to the 4G/5G genotype carriers. Since lymphocytes are associated with the body’s immune response, this result may imply that there are distinctions in the level of immune response in DM patients with different genotypes. For HTN patients, individuals with the 5G/5G genotype had higher RBC and Hb compared to individuals with the 4G/5G genotype. In a study comprising 9808 Iranian subjects, Emamian et al found that erythrocyte parameters including RBC, Hb, hematocrit (HCT), and mean corpuscular hemoglobin (MCH) were increased in HTN patients compared to controls.28 They hypothesized that excess erythrocyte counts may facilitate the development of HTN by placing additional cardiovascular stress, while Hb may contribute to increase blood pressure by limiting nitric oxide use through smooth muscle cells thereby exacerbating vasoconstriction. Accordingly, HTN patients carrying the 5G/5G genotype may have higher cardiovascular stress than the 4G/5G carriers. In terms of glucose metabolism parameters, HTN patients with the 4G/4G, 4G/5G, 5G/5G genotypes seem to have progressively higher HbA1c levels. Collectively, individuals harboring the 5G/5G genotype had higher HbA1c and Glu relative to individuals with the 4G/4G genotype. In a cross-sectional study involving 1462 non-diabetic Chinese population, Song et al noted that higher HbA1c may aggravate the risk of HTN in a synergistic manner.29 In this scenario, our findings may suggest that HTM patients with the 5G/5G genotype may have higher glucose metabolic stress. In the DM+HTN group, carriers of the 5G/5G genotype had reduced WBC and N as compared to other genotypes. Previous studies have proposed WBC and N as risk factors for HTN and HTN with first ischemic stroke, respectively.30,31 Similarly, a study has shown that N was associated with the occurrence and severity of DM as well as diabetic retinopathy.32 Based on this, we presumed that patients with DM and HTN of the 5G/5G genotype were at reduced risk of developing complications. Regrettably, information on complications was missing for most of the subjects in this study. Focusing on discrepancies in complications developing in patients with various genotypes might be a direction for future research. On the other hand, we also found that patients with the 4G/4G genotype had relatively elevated TG and LDL-C in the DM+HT group. Intriguingly, a research based on Italian patients with first stroke or vascular disorders identified the 4G/4G genotype was strongly associated with high TC (P=0.003) but not with TG (P=0.39).33 This was analogous to the results of our study. It is well known that abnormal changes in serum lipids, especially cholesterol, are risk factors for cardiometabolic syndromes such as DM and HTN. Elevated LDL-C has also been reported to worsen subclinical vascular damage and cognitive impairment in patients with HTN.34 A cross-sectional study revealed that glucose disposal rate (eGDR) was negatively associated with TC and LDL-C, which hinted that TC and LDL-C may be contributors to insulin resistance.35 Thus, for patients with both DM and HTN, the 4G/4G genotype might be a catalytic factor in the progression of the diseases.
Overall, the RT-PCR method can accurately identify the PAI-1 4G/5G genotype in different individuals. The PAI-1 4G/5G polymorphism may not be associated with genetic susceptibility to DM, HTN and DM+HTN, but differences in clinical characteristics among individuals with various genotypes may provide a reference for disease assessment and personalized treatment of patients.
Inevitably, there were some limitations to this study. Firstly, this study was a single-center retrospective analysis and the limited sample size might introduce skew to the findings. Future multi-center, prospective collaborative studies may contribute to further understanding of the effect of the PAI-1 4G/5G polymorphism in DM and HTN. Secondly, the missing information on the clinical characteristics of several patients might interfere with the statistical analysis and interpretation of the results. In addition, the relevance of the PAI-1 4G/5G polymorphism to the clinical classification, severity, treatment, and prognosis of DM and HTN should be investigated in the future.
Data Sharing Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Ethics Statement
This study was performed in compliance with Declaration of Helsinki and approved by the Ethics Committee of Peking Union Medical College Hospital (No. HS2019036). The Ethics Committee decided that patient consent to review their medical records was not required. The reason for the waiver is that this study would not interfere with the diagnosis or treatments of the patients. All data involving patients was strictly confidential in accordance with the national legislation and the institutional requirements.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Beijing Key Clinical Specialty for Laboratory Medicine Excellent Project (No. ZK201000).
Disclosure
The authors report no competing interests in this work.
References
1. Abuelgasim E, Shah S, Abuelgasim B, et al. Clinical overview of diabetes mellitus as a risk factor for cardiovascular death. Rev Cardiovasc Med. 2021;22(2):301–314. doi:10.31083/j.rcm2202038
2. Bailes BK. Diabetes mellitus and its chronic complications. Aorn J. 2002;76(2):266–276, 278–282; quiz 283–266. doi:10.1016/s0001-2092(06)61065-x
3. Ma RCW. Epidemiology of diabetes and diabetic complications in China. Diabetologia. 2018;61(6):1249–1260. doi:10.1007/s00125-018-4557-7
4. Wang L, Peng W, Zhao Z, et al. Prevalence and treatment of diabetes in China, 2013–2018. JAMA. 2021;326(24):2498–2506. doi:10.1001/jama.2021.22208
5. Mancia G, Scopelliti F, Grassi G. Hypertension and the heart. Semin Cardiothorac Vasc Anesth. 2006;10(3):198–202. doi:10.1177/1089253206291315
6. Lu Q, Zhang Y, Geng T, et al. Association of lifestyle factors and antihypertensive medication use with risk of all-cause and cause-specific mortality among adults with hypertension in China. JAMA Netw Open. 2022;5(2):e2146118. doi:10.1001/jamanetworkopen.2021.46118
7. Lu J, Lu Y, Wang X, et al. Prevalence, awareness, treatment, and control of hypertension in China: data from 1·7 million adults in a population-based screening study (China PEACE million persons project). Lancet. 2017;390(10112):2549–2558. doi:10.1016/s0140-6736(17)32478-9
8. Jin Z, Pan Z, Wang Z, et al. CYSLTR1 rs320995 (T927C) and GSDMB rs7216389 (G1199A) gene polymorphisms in asthma and allergic rhinitis: a proof-of-concept study. J Asthma Allergy. 2022;15:1105–1113. doi:10.2147/jaa.S371120
9. Wang Z, Kong L, Zhang H, et al. Tumor necrosis factor alpha −308G/A gene polymorphisms combined with neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio predicts the efficacy and safety of anti-TNF-α therapy in patients with ankylosing spondylitis, rheumatoid arthritis, and psoriasis arthritis. Front Pharmacol. 2021;12:811719. doi:10.3389/fphar.2021.811719
10. Gils A, Declerck PJ. Plasminogen activator inhibitor-1. Curr Med Chem. 2004;11(17):2323–2334. doi:10.2174/0929867043364595
11. Altalhi R, Pechlivani N, Ajjan RA. PAI-1 in diabetes: pathophysiology and role as a therapeutic target. Int J Mol Sci. 2021;22(6):6. doi:10.3390/ijms22063170
12. Wang TJ, Gona P, Larson MG, et al. Multiple biomarkers and the risk of incident hypertension. Hypertension. 2007;49(3):432–438. doi:10.1161/01.HYP.0000256956.61872.aa
13. Zhao L, Bracken MB, Dewan AT, Chen S. Association between the SERPINE1 (PAI-1) 4G/5G insertion/deletion promoter polymorphism (rs1799889) and pre-eclampsia: a systematic review and meta-analysis. Mol Hum Reprod. 2013;19(3):136–143. doi:10.1093/molehr/gas056
14. Du J, Lan J, Yang H, et al. Association of angiotensin-converting enzyme insertion/deletion (ACE I/D) gene polymorphism with susceptibility to prostate cancer: an updated meta-analysis. World J Surg Oncol. 2022;20(1):354. doi:10.1186/s12957-022-02812-x
15. Zhang J, Shi H, Xue M, et al. An insertion/deletion polymorphism in the interleukin-1A 3’untranslated region confers risk for gastric cancer. Cancer Biomark. 2016;16(3):359–365. doi:10.3233/cbm-160574
16. Zhang Q, Jin Y, Li X, et al. Plasminogen activator inhibitor-1 (PAI-1) 4G/5G promoter polymorphisms and risk of venous thromboembolism - a meta-analysis and systematic review. Vasa. 2020;49(2):141–146. doi:10.1024/0301-1526/a000839
17. Huang X, Li Y, Huang Z, Wang C, Xu Z. Pai-1 gene variants and COC use are associated with stroke risk: a case-control study in the Han Chinese women. J Mol Neurosci. 2014;54(4):803–810. doi:10.1007/s12031-014-0418-0
18. Gao WF, Guo YB, Bai Y, Ding XY, Yan YJ, Wu ZQ. Association between PAI-1 4G/5G polymorphism and diabetic nephropathy: a meta-analysis in the Chinese population. Int Urol Nephrol. 2016;48(9):1483–1489. doi:10.1007/s11255-016-1333-9
19. Wang S, Cao Q, Wang X, et al. PAI-1 4G/5G polymorphism contributes to cancer susceptibility: evidence from meta-analysis. PLoS One. 2013;8(2):e56797. doi:10.1371/journal.pone.0056797
20. Li W, Mao S, Wu L, Shi W, Zhang J, Wang Z. Association between the PAI-1 4G/5G gene polymorphism and the risk of systemic lupus erythematosus/lupus nephritis. Crit Rev Eukaryot Gene Expr. 2019;29(1):85–94. doi:10.1615/CritRevEukaryotGeneExpr.2019025311
21. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus provisional report of a WHO consultation. Diabet Med. 1998;15(7):539–553. doi:10.1002/(sici)1096-9136(199807)15:7<539::Aid-dia668>3.0.Co;2-s
22. Liu LS. 中国高血压防治指南2010 [2010 Chinese guidelines for the management of hypertension]. Zhonghua Xin Xue Guan Bing Za Zhi. 2011;39(7):579–615. Chinese.
23. Navarro E, Serrano-Heras G, Castaño MJ, Solera J. Real-time PCR detection chemistry. Clin Chim Acta. 2015;439:231–250. doi:10.1016/j.cca.2014.10.017
24. Miri S, Sheikhha MH, Dastgheib SA, Shaker SA, Neamatzadeh H. Association of ACE I/D and PAI-1 4G/5G polymorphisms with susceptibility to type 2 diabetes mellitus. J Diabetes Metab Disord. 2021;20(2):1191–1197. doi:10.1007/s40200-021-00839-7
25. Xu K, Liu X, Yang F, et al. PAI-1-675 4G/5G polymorphism in association with diabetes and diabetic complications susceptibility: a meta-analysis study. PLoS One. 2013;8(11):e79150. doi:10.1371/journal.pone.0079150
26. Jacobs A, Schutte AE, Ricci C, Pieters M. Plasminogen activator inhibitor-1 activity and the 4G/5G polymorphism are prospectively associated with blood pressure and hypertension status. J Hypertens. 2019;37(12):2361–2370. doi:10.1097/hjh.0000000000002204
27. Kim KN, Kim KM, Kim BT, Joo NS, Cho DY, Lee DJ. Relationship of plasminogen activator inhibitor 1 gene 4G/5G polymorphisms to hypertension in Korean women. Chin Med J). 2012;125(7):1249–1253.
28. Emamian M, Hasanian SM, Tayefi M, et al. Association of hematocrit with blood pressure and hypertension. J Clin Lab Anal. 2017;31(6):6. doi:10.1002/jcla.22124
29. Song J, Wei N, Zhao Y, Jiang Y, Wu X, Gao H. Elevated glycosylated hemoglobin levels and their interactive effects on hypertension risk in nondiabetic Chinese population: a cross-sectional survey. BMC Cardiovasc Disord. 2020;20(1):218. doi:10.1186/s12872-020-01501-5
30. Nakanishi N, Sato M, Shirai K, Suzuki K, Tatara K. White blood cell count as a risk factor for hypertension; a study of Japanese male office workers. J Hypertens. 2002;20(5):851–857. doi:10.1097/00004872-200205000-00018
31. Zhang Z, Zhou C, Liu M, et al. Neutrophil counts and the risk of first stroke in general hypertensive adults. Hypertens Res. 2021;44(7):830–839. doi:10.1038/s41440-021-00625-1
32. Woo SJ, Ahn SJ, Ahn J, Park KH, Lee K. Elevated systemic neutrophil count in diabetic retinopathy and diabetes: a hospital-based cross-sectional study of 30,793 Korean subjects. Invest Ophthalmol Vis Sci. 2011;52(10):7697–7703. doi:10.1167/iovs.11-7784
33. Boncoraglio GB, Bodini A, Brambilla C, Carriero MR, Ciusani E, Parati EA. An effect of the PAI-1 4G/5G polymorphism on cholesterol levels may explain conflicting associations with myocardial infarction and stroke. Cerebrovasc Dis. 2006;22(2–3):191–195. doi:10.1159/000093604
34. Kovács KR, Bajkó Z, Szekeres CC, et al. Elevated LDL-C combined with hypertension worsens subclinical vascular impairment and cognitive function. J Am Soc Hypertens. 2014;8(8):550–560. doi:10.1016/j.jash.2014.04.007
35. Luo SH, Yang DZ, Wei XY, et al. 成年1型糖尿病患者胰岛素抵抗与血脂紊乱的关系 [Association of insulin resistance with dyslipidemia in adults with type 1 diabetes]. Zhonghua Yi Xue Za Zhi. 2019;99(34):2665–2669. Chinese. doi:10.3760/cma.j.issn.0376-2491.2019.34.006
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Acute Helicobacter pylori Infection Prevalence Among Renal Failure Patients and Its Potential Roles with Other Chronic Diseases: A Retrospective Cohort Study
Alhoufie ST, Ibrahim NA, Alhhazmi AA, Makhdoom HM, Ali HM, Hemeg HA, Almutawif YA, Mahallawi WH, Alfarouk KO
Infection and Drug Resistance 2022, 15:6589-6599
Published Date: 10 November 2022
Trends and Comparisons of Blood Pressure and Fasting Plasma Glucose in Patients with Hypertension, Diabetes, and Comorbidity: 4-Year Follow-Up Data
Xu L, Wen X, Yang Y, Cui D
Risk Management and Healthcare Policy 2022, 15:2221-2232
Published Date: 25 November 2022
Association Between ALDH2 Polymorphisms and the Risk of Diabetes Mellitus in Hypertensive Patients
Zeng M, Liu Y, Xie Y
International Journal of General Medicine 2023, 16:5719-5727
Published Date: 6 December 2023
Metabolic Syndrome and Tendon Disease: A Comprehensive Review
Lai C, Li R, Tang W, Liu J, Duan XD, Bao D, Liu H, Fu S
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1597-1609
Published Date: 9 April 2024
Assessment of Health-Related Quality of Life Among Patients with Chronic Diseases and Its Relationship with Multimorbidity: A Cross-Sectional Study from Saudi Arabia
Alzarea AI, Khan YH, Alzarea SI, Alanazi AS, Alsaidan OA, Alrowily MJ, Al-Shammari M, Almalki ZS, Algarni MA, Mallhi TH
Patient Preference and Adherence 2024, 18:1077-1094
Published Date: 4 June 2024