Back to Journals » Infection and Drug Resistance » Volume 15
Acute Helicobacter pylori Infection Prevalence Among Renal Failure Patients and Its Potential Roles with Other Chronic Diseases: A Retrospective Cohort Study
Authors Alhoufie ST, Ibrahim NA ![]() , Alhhazmi AA
, Alhhazmi AA ![]() , Makhdoom HM, Ali HM
, Makhdoom HM, Ali HM ![]() , Hemeg HA
, Hemeg HA ![]() , Almutawif YA
, Almutawif YA ![]() , Mahallawi WH
, Mahallawi WH ![]() , Alfarouk KO
, Alfarouk KO
Received 9 September 2022
Accepted for publication 28 October 2022
Published 10 November 2022 Volume 2022:15 Pages 6589—6599
DOI https://doi.org/10.2147/IDR.S388361
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Sari T Alhoufie,1 Nadir A Ibrahim,1 Areej A Alhhazmi,1 Hatim M Makhdoom,1 Hamza M Ali,1 Hassan A Hemeg,1 Yahya A Almutawif,1 Waleed H Mahallawi,1 Khalid O Alfarouk2,3
1Medical Laboratories Technology Department, College of Applied Medical Sciences, Taibah University, Al- Madinah Al-Munwarah, Saudi Arabia; 2Zamzam Research Center, Zamzam Medical College, Khartoum, Sudan; 3Alfarouk Biomedical Research LLC, Temple Terrace, FL, 33617, USA
Correspondence: Sari T Alhoufie, Medical Laboratories Technology Department, College of Applied Medical Sciences, Taibah University, Al- Madinah Al-Munwarah, Saudi Arabia, Email [email protected]
Background: Helicobacter pylori (H. pylori) infection is relevant to several chronic human diseases, from digestive diseases to renal, metabolic, and cancer diseases. H. pylori infections and chronic kidney diseases are in increasing, global records; if not well controlled in a specific population, these diseases might lead to more clinical complications.
Methods: In this retrospective study, we investigated the prevalence of acute H. pylori infections among 127 dialysis patients via subjecting their serums to the enzyme-linked immunosorbent assay (ELISA) to detect the human Immunoglobulin M (IgM) against H. pylori infections. Samples were from dialysis patients in a single hemodialysis center in Medina, Saudi Arabia, from January to August 2021.
Results: Our results indicated the significant prevalence of H. pylori acute infections among 33.1% of renal failure patients recruited in this study, chi-squared: 14.559, p-value: 0.0001. In addition, no significant occurrence of acute H. pylori infection among males and females, chi-squared: 1.823, p-value: 0.177. Furthermore, the prevalence of acute H. pylori infection was not significant in different age groups of renal failure patients. Chi-squared: 6.803, p-value: 0.147, despite H. pylori-infected cases predominantly represented in patients above 51 years. Moreover, we noticed that hypertension, followed by diabetes, was the most prevalent underlying medical condition among acute infected H. pylori and renal failure patients.
Conclusion: We documented the significant prevalence of acute H. pylori infection among renal failure patients. We also highlighted and discussed the possible potential roles of H. pylori in renal failure and other chronic diseases. Routine screening and treatment for acute H. pylori infection for chronic kidney diseases, hypertension, and diabetes patients would positively reduce the bacterium’s progressive effects on them. They might even improve the control of these diseases.
Keywords: Helicobacter pylori, acute infection, chronic kidney disease, renal failure, hypertension, diabetes mellitus
Introduction
Helicobacter pylori is a gram-negative bacterium infecting both children and adults. It is the most common human chronic infection, causing gastrointestinal diseases such as gastric malignancies, gastritis, and ulcerative diseases. H. pylori can also be involved in other non-gastrointestinal infections such as diabetes and metabolic syndrome, heart disease, hematologic disorders, cancer, and chronic kidney disease (CKD) as well as chronic renal failure (CRF).1–6
Renal failure (RF), also termed end-stage kidney disease, is a kidney function decline of less than 15% compared to the normal kidney. When the kidney fails, the body loses its ability to remove waste, and water accumulates inside the body, leading to chemical imbalances that impact buffering capacity and electrolyte balances. Patients begin to receive hemodialysis.7 RF could be acute or chronic; acute kidney failure can be initiated by different causes such as low blood pressure, urinary tract blockage, and hemolytic uremic syndrome after digestive tract bacterial infections caused by E. coli O157:H7. Chronic renal failure can be caused by prolonged urinary tract blockage, chronic inflammation, eg, Systemic Lupus Erythematosus (SLE), chronic high blood pressure, diabetes mellitus, and other factors.8–11
However, some CRF patients who have received hemodialysis for long periods complained of gastrointestinal troubles. It has been postulated that high urea concentration makes the gastric mucosa of these patients more susceptible to H. pylori colonization.12,13 Previous observations in different countries reported the prevalence of H. pylori infection among patients with CRF ranging between 20 and 60%, and H. pylori infection can contribute to progressive renal dysfunction resulting in CKD development.14–16
In Saudi Arabia, the prevalence of CKD is 9892/100,000, which is higher compared to the North America 7919/100,000 and Western Europe 5446/100,000.17,18 On the other hand, the prevalence of H. pylori in some areas in Saudi Arabia might reach almost 50% of the population.19
Little is known about the prevalence of acute H. pylori infection among RF patients in Saudi Arabia. Therefore, we aimed to investigate this prevalence in this study and shed light on the crucial role that H. pylori can play in initiating or aggravating chronic diseases such as RF, hypertension, and diabetes.
Methodology
Study Design and Samples Collections
In this retrospective study, serum samples from 127 renal failure patients collected in previous projects20 were subjected to H. pylori IgM detection to investigate the prevalence of acute H. pylori infection among dialysis patients. Samples were collected from a single hemodialysis center in Madinah, Saudi Arabia, from January to August 2021 and preserved at −70 °C. Serum samples from patients whom undergoing hemodialysis were included in this study and those who not under dialysis procedure in the center were excluded. Demographic data, including patients’ age, gender, and frequency of dialysis per week, were extracted from their records.
Ethical Consideration
Ethical approval was acquired from the Research Ethics Committee of the College of Applied Medical Sciences, Taibah University (2022/142/125/MLT). Patients’ informed consents were waived by the Ethics Committee due to the retrospective nature of the study. Patients’ privacy and confidentiality of data were maintained in accordance with the Declaration of Helsinki.
Serological Detection for Helicobacter pylori Infection
Anti-Helicobacter pylori IgM antibodies were determined qualitatively with SERION classic Helicobacter pylori IgM ELISA kit (Institut Virion\Serion GmbH, Würzburg, Germany) according to the manufacturers’ guidelines. As part of the quality control of the assay, control and standard sera from the kits were included on each plate and were set up in duplicate. To avoid interference with rheumatoid factors, patient samples were pre-treated with rheumatoid factor absorbent by incubation the patient’s sample in diluted rheumatoid factors – absorbent for 15 minutes at room temperature. According to the manufacturer’s manual, all washing processes were carried out using a semi-automated ELISA washer and reader (Biotek, Winooski, US).
The ELISA is based on the specific interaction of antibodies in patient serum with their corresponding antigen with a sensitivity of 99% and 79.7% specificity. The SERION ELISA classic microtiter plate test strips were coated with specific antigens of Helicobacter pylori. In the first incubation, if antibodies in the patient’s serum sample were present, they bind to the fixed antigen. After washing unbound antibodies, a secondary antibody, conjugated with the enzyme alkaline phosphatase detects attaches to the immune complex. A second washing step was performed then the substrate p-nitrophenyl phosphate was added. The colorless substrate was converted into the colored product p-nitrophenol. Finally, sodium hydroxide was then added to stop the reaction. The signal intensity of this reaction product was proportional to the concentration of the antibodies in the sample and was measured spectrophotometrically at a single wavelength of 405 nm within 60 minutes. For qualitative evaluation, upper and lower cut-off ranges were calculated according to the user manual of the assay kits.
Statistical Analysis
H. pylori infection distributions to concerning sex, age and comorbidities were compared using the chi-squared (χ2) test. P-values of 0.05 were considered statistically significant. Descriptive statistics for categorical variables are presented as percentages and frequencies. Binary logistic regression analysis was performed to predict H. pylori infection with underlying diseases. Data were analyzed using the Statistical Package for the Social Sciences version 20 (IBM Corporation, Armonk, NY, USA).
Results
Demographic Characteristics of the Study Cohort
One hundred and twenty-seven patients with chronic renal failure were recruited for the study. The mean ± SD of patients’ ages was 48.28 ± 13.46 years (Minimum = 18, Maximum = 72). The majority (63%) of those patients were male (80 out of 127) patients, whereas (37%) were female (47 out of 127) (Table 1). Patients were grouped according to their ages, where most of them (47.2%) fall in the age of 51 years or older (60 out of 127), followed by patients aged between 41 and 50 years old with a percentage of 24.4% (31 out of 127). Patients between 21 and 30 years old were 19 patients with a percentage of 15%, and patients between the age of 31 and 40 were only 16, accounting for 12.6% of total patients (Table 2).
 |
Table 1 Distribution of H. pylori Infection Among Dialysis Patient’s Gender |
 |
Table 2 Distribution of H. pylori Among Different Age Groups of Dialysis Patients |
Patient’s medical records indicated several other underlying medical conditions, where most of the patients suffered from hypertension, 66.9% (85 out of 127), diabetic Mellitus 4.7% (6 out of 127), or both 24.4% (31 out of 127), and few patients with other underlying medical conditions 3.9% (5 out of 127) (Table 3). Most of those patients, 95.3% (121 out of 127), had been undergoing dialysis therapy three times a week, whereas only 6 (4.7%) patients had dialysis therapy twice weekly.
 |
Table 3 Distribution of H. pylori Infection with Other Underlying Medical Diseases |
H. pylori Prevalence Among Renal Failure Patients
Out of the 127 renal failure patients, 42 (33.1%) tested positive for H. pylori acute infection demonstrated by IgM seropositivity while 85 patients (66.9%) tested negative, chi-square: 14.559, p-value: 0.000136 (Figure 1). In addition, there was no significant difference in the occurrence of H. pylori acute infection among males 54.8% (23 out of 42) and females 45.2% (19 out of 42), chi-squared: 1.823 and P values: 0.177 (Table 1).
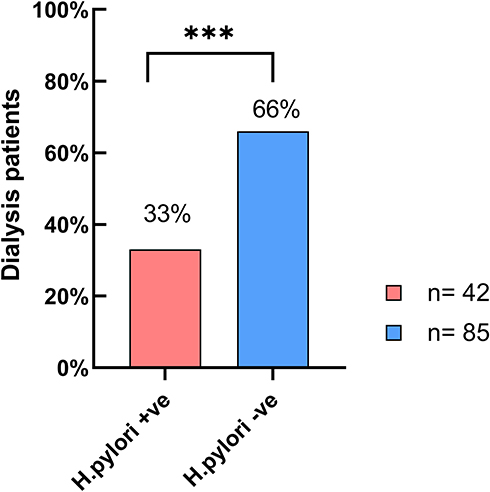 |
Figure 1 Prevalence of H. pylori acute infection among dialysis patients. (***) p-value: 0.0001. |
Distribution of H. pylori Among Different Age Groups of Dialysis Patients
No significant variation was observed in the probability distribution of H. pylori infection among patients from different age groups (10–20, 21–30, 31–40, 40–50, and >50 years) (chi-squared: 6.803 and p-value: 0.147) (Table 2). However, by excluding the H. pylori-negative cases, we found that H. pylori-infected cases were predominantly represented in patients aged 51 years or older, with a percentage of 42.9% (18 out of 42), followed by 26.2% (11 out of 42) among 21–30-year-olds, 19% (8 out of 42) 41–50-year-olds and 11.9% (5 out of 42) among 31–40-year-old patients (chi-squared: 8.857, p-value: 0.031) (Figure 2).
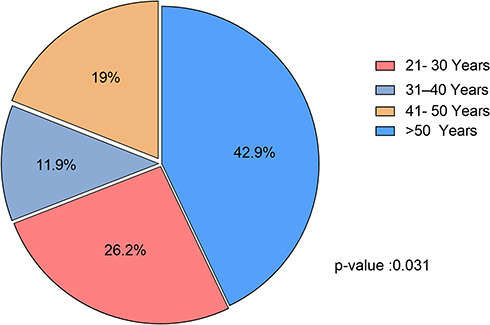 |
Figure 2 Distribution of H. pylori seropositivity among different age groups of 42 infected dialysis patients. |
Association of H. pylori Infection with Other Underlying Medical Diseases Among Dialysis Patients
Among dialysis patients recruited in this study, Hypertension noted in 66.9% (85 out of 127) of the patients and seropositivity for H. pylori IgM antibodies occurred in 32.9% of them (28 out of 85 patients) (Figure 3A). Furthermore, patients’ medical records revealed that 24.4% (31/127) of the participants suffered from hypertension and diabetes (Table 3) and 35.5% (11/31) of them were infected with H. pylori (Figure 3B). Participants with only diabetes as an underlying medical condition were 6 out of 127, and only two were infected with H. pylori (Figure 3C). Few patients have other distinctive underlying medical conditions (Table 3) such as systemic lupus erythematosus (SLE), anti-neutrophil cytoplasmic antibody (ANCA), and ischemic heart disease (IHD) those patients were negative for H. pylori infection, except for one patient who suffered from hypertension and ischemic heart disease (Figure 3D).
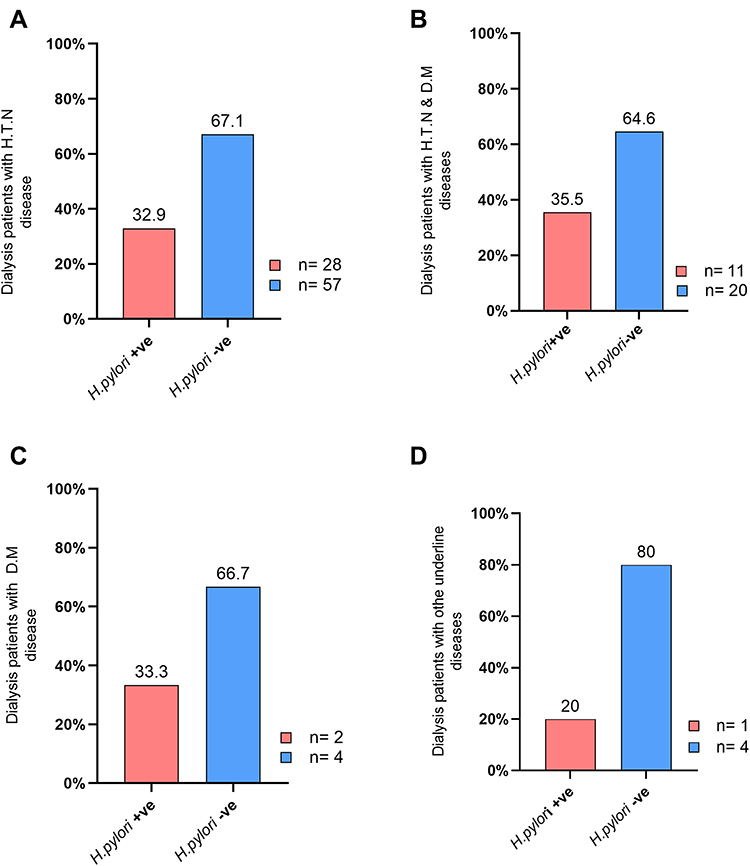 |
Figure 3 Association of H. pylori acute infection with other underlying medical diseases among dialysis patients. (A) Dialysis patients with hypertension (HTN), (B) dialysis patients with hypertension and diabetes mellitus, (C) dialysis patients with diabetes mellitus only (DM), (D) dialysis patients with other underlying medical conditions. |
No significant distribution of H. pylori seropositivity observed among different underlying medical conditions for the dialysis patients (chi-squared: 0.572; p-value 0.903) (Table 3).
However, by excluding H. pylori-negative cases, significant distribution of H. pylori seropositivity occurred among different underlying medical condition patients (Chi-squared: 44.667 p-value: <0.0001). In addition, we found that hypertension cases were predominantly represented among H. pylori-infected dialysis patients 66.7% (28 out of 42), followed by hypertension and diabetes patients 26.2% (11/42) of H. pylori-infected dialysis cases and diabetic patient with H. pylori seropositivity were 4.7% (2 out of 24) and other diseases were 2.3% (1 out of 42) (Figure 4).
 |
Figure 4 Distribution of different underlying medical diseases among positive H. pylori dialysis patients (p-value: <0.0001). |
Nevertheless, binary logistic regression analysis was performed to predict H. pylori infection with comorbid status, underlying medical condition variable which is classified into 4 classes (HTN, DM, HTN and DM, and others) was included in the model. The results of the logistic regression analysis showed that the model which considered the independent variable, underlying medical condition, was not statistically significant (p value = 0.918), log-likelihood=160.706 (Table 4).
 |
Table 4 Predictors of Change in H. pylori Infectivity |
Discussion
In this work, we conducted a retrospective study to investigate the prevalence of acute H. pylori infections among 127 randomly selected renal failure patients from a single hemodialysis center in Medina, Saudi Arabia, from January to August 2021. Our results revealed seropositivity (IgM) for H. pylori acute infections among 33% of dialysis patients indicating significant prevalence (p-value: 0.0001). In addition, we found no significant difference in the occurrence of H. pylori infection among males and females (p-values: 0.177), as well as among different age groups of renal failure patients (p-value: 0.147). Nevertheless, we noticed that H. pylori-infected cases were predominantly represented in patients aged 51 years old. Moreover, significant distribution (p-value:<0.0001) of H. pylori seropositivity occurred between different underlying medical conditions, whereas logistic regression analysis showed no predictors of change for H. pylori infectivity.
We conducted serological detection for H. pylori IgM, indicating acute and recent H. pylori infection. Alem and his colleagues found that the detection of H. pylori IgM is highly specific to indicate acute infection among 9043 symptomatic and asymptomatic individuals. Other researchers claimed that IgM detection reflects the bacterium’s recent infection and mucosal invasion phase. In addition, IgM antibodies can occur in the first 18 days of H. pylori infection.21–23
The significant prevalence of H. pylori in this study among renal failure patients (Figure 1) agrees with several previous studies.24–27 H. pylori infection is relevant to renal diseases such as membranous nephropathy (MN), immunoglobulin A nephropathy (IgAN), lupus nephritis, and diabetic nephropathy.28–34 Furthermore, Qian and colleagues detected H. pylori antigens in renal biopsy specimens of kidney patients.35,36 The bacterium can trigger renal diseases via inducing chronic inflammation, a significant cause of renal diseases. For instance, H. pylori induce inflammatory cytokines, chemokines, and growth factors that can damage a vascular endothelial structure in the kidney. In addition, C-reactive protein (CRP), tumor necrosis factor-alpha (TNF-a), interleukin 1 (IL-1), interleukin 6 (IL-6), interleukin 8 (IL-8), heat shock protein (HSP) is also induced by H. pylori infection which might aggravate microvascular damage in the kidney (Figure 5).37,38 However, other epidemiologic observations noticed an inconsistent association of H. pylori infection among such a group of patients.39–41 These contradictory findings can be attributed to several reasons. For instance, H. pylori prevalence varies clearly across different demographic and geographic areas due to the sanitary conditions, cultural habits, and economic situations. In addition, some medications commonly prescribed for renal failure patients, such as antibiotics, proton pump inhibitors, and bismuth, can affect the reliability of these diagnostic methods by increasing the possibility of false-negative results.42,43 Furthermore, there are several diagnostic methods for H. pylori infection, including a urea breath test, stool antigen, urease test, histology, and bacterium culturing, and the different used tests to detect H. pylori infection in each study might raise these paradoxical results.
 |
Figure 5 Potential roles of H. pylori infection and its interventions in the cyclic relation between chronic kidney disease (CKD), diabetes mellitus (DM) and hypertension (HTN). |
Early diagnosis and treatment for H. pylori infection might prevent its impact on renal function. A recent observation by Pan and colleagues reported a remarkable decrease in the albumin-to-creatinine ratio (ACR) in the urine after eradicating H. pylori infection for renal disease patients with peptic ulcers.44 Other studies noticed reduced proteinuria in patients with membranous nephropathy, patients suffering from dyspeptic complaints, and type 2 diabetic patients after eradicating H. pylori infection.35,45,46
Our result revealed no significant distribution (p-value: 0.147) of acute H. pylori infection among different age groups of renal failure patients. However, H. pylori-seropositivity was observed predominantly in the age group >51 years (Figure 2). Several studies reported a high prevalence of H. pylori incidences among elderly patients with gastroduodenal diseases up to 70% and might range from 40 to 60% in asymptomatic elderly individuals,47–49 which might stand behind the predominancy of H. pylori-seropositivity among renal failure patients age group >51 years in this work.
We also noted 32.9% of H. pylori-seropositivity for renal failure patients suffering from hypertension as underlying disease (Figure 3A) which concurs with recent observations.50,51 In addition, among H. pylori seropositive cases, hypertension was more common than others underlying diseases (Figure 4). The association between H. pylori and hypertension can be attributed to several factors. For instance, H. pylori can initiate the cascades of many disease pathways, including hypertension and atherosclerosis, as it decreases nitric oxide (NO) production and prevents the vasodilatation property resulting in diastolic blood pressure.52 In addition, H. pylori trigger many mediators that support hypertension pathogenicities such as fibrinogen, interleukin-1 (IL-1), tumor necrosis factor-α (TNF-α), and C-reactive protein (CRP), as they are related to insulin resistant which is one of the major causes that leads to hypertension and diabetes mellitus type 2 (Figure 5).53,54 Whether hypertension contributes to H. pylori infection or not is still unclear and needs to be investigated. Some studies claimed that H. pylori eradication improved blood pressure values among hypertension patients,55,56 indicating the importance of routine investigation for H. pylori infection.
Diabetes was reported among 37 renal failure patients, and H. pylori seropositivity occurred in 13 of them, 11 patients suffered from diabetes-hypertension, and 2 patients have diabetes only (Figure 3B and C). Early studies showed that hyperglycemia might play a role in H. pylori stomach infectivity via different aspects such as increasing endothelial permeability, altering basement membrane composition and structure, and enhancing H. pylori adhesion and other virulence factors expressions.57,58 H. pylori supports ROS production, leading to insulin resistance and developing DM type 2 (Figure 5). Moreover, ROS leads to kidney injury; at the same time, CKD increases ROS production and worsens insulin resistance.59,60 A recent study on type 2 diabetes patients with active H. pylori infection showed glycemic control improvement after eradicating such infection.61
From all above, H. pylori infections were reported among patients with underlying cycling-related diseases, such as CKD, DM, and HPT. Emerging results from different studies mentioned above revealed that H. pylori infections could trigger these chronic diseases either directly or indirectly; meanwhile, these diseases can make patients more susceptible to H. pylori infection, as illustrated in (Figure 5). In addition, in several observations, H. pylori infection eradication positively impacted these underlying diseases, including restoring renal functions and improving glycemic control and blood pressure values.
There were some limitations in this work; firstly, the patient’s medical report did not provide some essential details such as the patient’s medications, gastrointestinal discomfort complaints, and some chemical indicators for CKD such as ACR that would be useful in comparison between H. pylori-infected and non-infected renal failure patients. Secondly, we observed H. pylori prevalence in relatively small samples from a single dialysis center. Finally, a prospective study would consider conducting other confirmatory tests for H. pylori detection. However, our study highlights the prevalence of H. pylori acute infection among dialysis patients in Saudi Arabia, considering the impact of other underlying diseases that had not been discussed before.
Concluding Remarks and Recommendations
This study showed the significant prevalence of acute H. pylori infection among renal failure patients. We illustrated the potential role of the bacterium in aggravating other commonly associated diseases with CKD, such as diabetes and hypertension. Understanding the pathogenic impact of H. pylori on other chronic diseases would open a new milieu that presents proper management of gut ecology and might represent a potential and rational approach to managing these diseases. Therefore, implementing routine screening for H. pylori infection and treatments for renal failure and diabetes and hypertension patients, in general, would minimize the potential prognosis that H. pylori might result, as emerging studies have shown.
Data Sharing Statement
All data and materials generated during the current study are available from the corresponding author upon reasonable request.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Parkin DM. The global health burden of infection-associated cancers in the year 2002. Int J Cancer. 2006;118:3030–3044. doi:10.1002/ijc.21731
2. Gravina AG, Zagari RM, De Musis C, et al. Helicobacter pylori and extragastric diseases: a review. World J Gastroenterol. 2018;24:3204. doi:10.3748/WJG.V24.I29.3204
3. Jiang J, Chen Y, Shi J, et al. Population attributable burden of Helicobacter pylori-related gastric cancer, coronary heart disease, and ischemic stroke in China. Eur J Clin Microbiol Infect Dis. 2017;36:199–212. doi:10.1007/S10096-016-2810-X
4. Pan W, Zhang H, Wang L, et al. Association between Helicobacter pylori infection and kidney damage in patients with peptic ulcer. Ren Fail. 2019;41:1028–1034. doi:10.1080/0886022X.2019.1683029
5. Zizzi CF, Pellicano R, Biancone L. The relationship between Helicobacter pylori and chronic kidney disease: update 2020. Minerva Gastroenterol Dietol. 2020;66:343–349. doi:10.23736/S1121-421X.20.02729-4
6. Ranjbar R, Behzadi P, Farshad S. Advances in diagnosis and treatment of Helicobacter pylori infection. Acta Microbiol Immunol Hung. 2017;64:273–292. doi:10.1556/030.64.2017.008
7. Nagaraja P, Ghalli F. Renal Failure. Blandy’s Urology. 2019;117–126. doi:10.1002/9781118863343.ch7
8. Hilton R. Acute renal failure. BMJ. 2006;333:786–790. doi:10.1136/bmj.38975.657639.AE
9. Webster AC, Nagler EV, Morton RL, et al. Chronic Kidney Disease. Lancet. 2017;389:1238–1252. doi:10.1016/S0140-6736(16)32064-5
10. Perneger TV, Brancati FL, Whelton PK, et al. Studying the causes of kidney disease in humans: a review of methodologic obstacles and possible solutions. Am J Kidney Dis. 1995;25:722–731. doi:10.1016/0272-6386(95)90548-0
11. Kazancioğlu R. Risk factors for chronic kidney disease: an update. Kidney Int Suppl. 2013;3:368–371. doi:10.1038/kisup.2013.79
12. Araki H, Miyazaki R, Matsuda T, et al. Significance of serum pepsinogens and their relationship to Helicobacter pylori infection and histological gastritis in dialysis patients. Nephrol Dial Transplant. 1999;14:2669–2675. doi:10.1093/NDT/14.11.2669
13. Hazell SL, Lee A. Campylobacter pyloridis, urease, hydrogen ion back diffusion, and gastric ulcers. Lancet. 1986;2:15–17. doi:10.1016/s0140-6736(86)92561-4
14. Gladziwa U, Haase G, Handt S, et al. Prevalence of Helicobacter pylori in patients with chronic renal failure. Nephrol Dial Transplant. 1993;8:301–306. doi:10.1007/s40620-020-00808-y
15. Aydemir S, Boyacioglu S, Gur G, et al. Helicobacter pylori infection in hemodialysis patients: susceptibility to amoxicillin and clarithromycin. World J Gastroenterol. 2005;11:842–845. doi:10.3748/WJG.V11.I6.842
16. Schoonjans R, Van Vlem B, Vandamme W, et al. Dyspepsia and gastroparesis in chronic renal failure: the role of Helicobacter pylori. Clin Nephrol. 2002;57:201–207. doi:10.5414/CNP57201
17. Mousa D, Alharbi A, Helal I, et al. Prevalence and Associated Factors of Chronic Kidney Disease among Relatives of Hemodialysis Patients in Saudi Arabia. Kidney Int Reports. 2021;6:817–820. doi:10.1016/J.EKIR.2020.12.029/ATTACHMENT/BAA9DCFE-8AF4-4E0A-B684-76AA3E24BE42/MMC1.DOCX
18. Alsuwaida AO, Farag YMK, Al Sayyari AA, et al. Epidemiology of chronic kidney disease in the Kingdom of Saudi Arabia (SEEK-Saudi investigators) - a pilot study. Saudi J Kidney Dis Transpl. 2010;21:1066–1072.
19. Akeel M, Elmakki E, Shehata A, et al. Prevalence and factors associated with H. pylori infection in Saudi patients with dyspepsia. Electron Physician. 2018;10:7279. doi:10.19082/7279
20. Mahallawi WH, Ibrahim NA, Mumena WA. Effectiveness of COVID-19 Vaccines in Patients Under Maintenance Hemodialysis. Risk Manag Healthc Policy. 2021;14:5081. doi:10.2147/RMHP.S345686
21. Gatta L, Vakil N, Ricci C, et al. Effect of proton pump inhibitors and antacid therapy on 13C urea breath tests and stool test for Helicobacter pylori infection. Am J Gastroenterol. 2004;99:823–829. doi:10.1111/J.1572-0241.2004.30162.X
22. Alem M, Alem N, Cohen H, et al. Diagnostic value of detection of IgM antibodies to Helicobacter pylori. Exp Mol Pathol. 2002;72:77–83. doi:10.1006/EXMP.2001.2408
23. Eastham EJ, Elliott TSJ, Berkeley D, et al. Campylobacter pylori infection in children. J Infect. 1988;16:96205–96206. doi:10.1016/S0163-4453(88)
24. Özgür O, Boyacioǧlu S, Özdoǧan M, et al. Helicobacter pylori infection in haemodialysis patients and renal transplant recipients. Nephrol Dial Transplant. 1997;12:289–291. doi:10.1093/NDT/12.2.289
25. Shousha S, Arnaout AH, Abbas SH, et al. Antral Helicobacter pylori in patients with chronic renal failure. J Clin Pathol. 1990;43:397–399. doi:10.1136/JCP.43.5.397
26. Asl MKH, Nasri H. Prevalence of Helicobacter pylori infection in maintenance hemodialysis patients with non-ulcer dyspepsia. Saudi J Kidney Dis Transpl. 2009;20:223–226.
27. Lin SY, Lin CL, Liu JH, et al. Association between Helicobacter pylori infection and the subsequent risk of end-stage renal disease: a nationwide population-based cohort study. Int J Clin Pract. 2015;69:604–610. doi:10.1111/IJCP.12602
28. Nagashima R, Maeda K, Yuda F, et al. Helicobacter pylori antigen in the glomeruli of patients with membranous nephropathy. Virchows Arch. 1997;431(4):235–239. doi:10.1007/S004280050094
29. Liu XZ, Zhang YM, Jia NY, et al. Helicobacter pylori infection is associated with elevated galactose-deficient IgA1 in IgA nephropathy. Ren Fail. 2020;42:539. doi:10.1080/0886022X.2020.1772295
30. Zhu TT, Wang L, Wang HL, et al. Helicobacter pylori participates in the pathogenesis of IgA nephropathy. Ren Fail. 2016;38:1398–1404. doi:10.1080/0886022X.2016.1216713
31. Nesheiwat Z, Daboul J, Merugu GP, et al. Membranous nephropathy and autoimmune hepatitis in the setting of acute Helicobacter pylori infection: a case report. J Med Case Rep. 2021;15. doi:10.1186/S13256-021-02874-7
32. Wu MC, Leong PY, Chiou JY, et al. Increased Risk of Systemic Lupus Erythematosus in Patients With Helicobacter pylori Infection: a Nationwide Population-Based Cohort Study. Front Med. 2020;6:330. doi:10.3389/FMED.2019.00330/XML/NLM
33. Wang F, Liu J, Lv Z. Association of Helicobacter pylori infection with diabetes mellitus and diabetic nephropathy: a meta-analysis of 39 studies involving more than 20,000 participants. Scand J Infect Dis. 2013;45:930–938. doi:10.3109/00365548.2013.844351
34. Zhou F, Zhong X, Chen J, et al. Helicobacter pylori infection associated with type 2 diabetic nephropathy in patients with dyspeptic symptoms. Diabetes Res Clin Pract. 2015;110:328–334. doi:10.1016/J.DIABRES.2015.09.008
35. Moriyama T, Kaneko T, Fujii M, et al. High prevalence of Helicobacter pylori infection in Japanese patients with membranous nephropathy. Aliment Pharmacol Ther Symp Ser. 2006;2:189–193. doi:10.1111/J.1746-6342.2006.00044.X
36. Li Q, Lin X, Wu Z, et al. Immuno-histochemistry analysis of Helicobacter pylori antigen in renal biopsy specimens from patients with glomerulonephritis. Saudi J Kidney Dis Transpl. 2013;24:751–758. doi:10.4103/1319-2442.113871
37. Aydogan T, Ulas T, Selcoki Y, et al. Effects of Helicobacter pylori eradication on proteinuria: a prospective study. Wien Klin Wochenschr. 2012;124:241–244. doi:10.1007/S00508-012-0150-0
38. Kanbay M, Kasapoglu B, Akcay A. An occult risk factor for proteinuria: helicobacter pylori infection. Med Hypotheses. 2007;69:709–710. doi:10.1016/J.MEHY.2007.01.010
39. Afsar B, Ozdemir FN, Elsurer R, et al. Helicobacter pylori infection may increase renal resistive index. Med Hypotheses. 2007;69:956–957. doi:10.1016/J.MEHY.2007.01.061
40. Jaspersen D, Fassbinder W, Heinkele P, et al. Significantly lower prevalence of Helicobacter pylori in uremic patients than in patients with normal renal function. J Gastroenterol. 1995;30:585–588. doi:10.1007/BF02367783
41. Sugimoto M, Sakai K, Kita M, et al. Prevalence of Helicobacter pylori infection in long-term hemodialysis patients. Kidney Int. 2009;75:96–103. doi:10.1038/KI.2008.508
42. Seyrek N, Kocabas E, Hazar S, et al. Helicobacter pylori antibodies in patients on chronic hemodialysis. Nephron. 1996;72:725–726. doi:10.1159/000188978
43. Nakajima F, Sakaguchi M, Amemoto K, et al. Helicobacter pylori in patients receiving long-term dialysis. Am J Nephrol. 2002;22:468–472. doi:10.1159/000065278
44. Pan W, Zhang H, Wang L, et al. Association between Helicobacter pylori infection and kidney damage in patients with peptic ulcer. Ren Fail. 2019;41:1028. doi:10.1080/0886022X.2019.1683029
45. Sugimoto T, Furukawa T, Maeda T, et al. Marked reduction of proteinuria after eradication of gastric Helicobacter pylori infection in a patient with membranous nephropathy: coincidental or associated? Intern Med. 2007;46:1483–1484. doi:10.2169/INTERNALMEDICINE.46.0200
46. Aljahdli E, Almaghrabi SJ, Alhejaili TL, et al. Association Between Helicobacter pylori Eradication and Kidney Function in Patients With Chronic Gastritis: a Retrospective Single-Center Study. Cureus. 2022;14. doi:10.7759/CUREUS.21621
47. Pilotto A, Salles N. Helicobacter pylori infection in geriatrics. Helicobacter. 2002;7(Suppl 1):56–62. doi:10.1046/J.1523-5378.7.S1.9.X
48. Regev A, Fraser GM, Braun M, et al. Seroprevalence of Helicobacter pylori and length of stay in a nursing home. Helicobacter. 1999;4:89–93. doi:10.1046/J.1523-5378.1999.98640.X
49. Pilotto A, Fabrello R, Franceschi M, et al. Helicobacter pylori infection in asymptomatic elderly subjects living at home or in a nursing home: effects on gastric function and nutritional status. Age Ageing. 1996;25:245–249. doi:10.1093/AGEING/25.3.245
50. Xiong X, Chen J, He M, et al. Helicobacter pylori infection and the prevalence of hypertension in Chinese adults: the Dongfeng-Tongji cohort. Int J Med. 2020;22:1389–1395. doi:10.1111/jch.13928
51. Wan Z, Hu L, Hu M, et al. Helicobacter pylori infection and prevalence of high blood pressure among Chinese adults. J Hum Hypertens. 2018;32:158–164. doi:10.1038/S41371-017-0028-8
52. Gobert AP, Mersey BD, Cheng Y, et al. Cutting Edge: urease Release by Helicobacter pylori Stimulates Macrophage Inducible Nitric Oxide Synthase. J Immunol. 2002;168:6002–6006. doi:10.4049/JIMMUNOL.168.12.6002
53. Kountouras J, Papaefthymiou A, Polyzos SA, et al. Impact of Helicobacter pylori-Related Metabolic Syndrome Parameters on Arterial Hypertension. Microorg. 2021;9:2351. doi:10.3390/MICROORGANISMS9112351
54. Wellen KE, Hotamisligil GS. Inflammation, stress, and diabetes. J Clin Invest. 2005;115:1111–1119. doi:10.1172/JCI25102
55. Migneco A, Ojetti V, Specchia L, et al. Eradication of Helicobacter pylori infection improves blood pressure values in patients affected by hypertension. Helicobacter. 2003;8:585–589. doi:10.1111/j.1523-5378.2003.00180.x
56. Kopáčová M, Bureš J, Koupil I, et al. Body indices and basic vital signs in Helicobacter pylori positive and negative persons. Eur J Epidemiol. 2007;22:67–75. doi:10.1007/S10654-006-9090-1
57. Chronopoulos A, Trudeau K, Roy S, et al. High glucose-induced altered basement membrane composition and structure increases trans-endothelial permeability: implications for diabetic retinopathy. Curr Eye Res. 2011;36:747–753. doi:10.3109/02713683.2011.585735
58. Morss AS, Edelman ER. Glucose modulates basement membrane fibroblast growth factor-2 via alterations in endothelial cell permeability. J Biol Chem. 2007;282:14635–14644. doi:10.1074/JBC.M608565200
59. Aslan M, Horoz M, Nazligul Y, et al. Insulin resistance in H pylori infection and its association with oxidative stress. World J Gastroenterol. 2006;12:6865. doi:10.3748/WJG.V12.I42.6865
60. Alicic RZ, Rooney MT, Tuttle KR. Diabetic Kidney Disease. Clin J Am Soc Nephrol. 2017;12:2032–2045. doi:10.2215/CJN.11491116.
61. Cheng KP, Yang YJ, Hung HC, et al. Helicobacter pylori eradication improves glycemic control in type 2 diabetes patients with asymptomatic active Helicobacter pylori infection. J Diabetes Investig. 2019;10:1092–1101. doi:10.1111/JDI.12991
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Efficacy, Safety, Tolerability, and Real-World Data of Patiromer for the Treatment of Hyperkalemia
Colbert G, Sannapaneni S, Lerma EV
Drug, Healthcare and Patient Safety 2022, 14:87-96
Published Date: 14 July 2022
The Elevation of Pancreatic Enzymes in Serum and Their Distribution at Different Stages of Renal Insufficiency Among Diabetic Patients Attending Goba Referral Hospital
Regasa T, Dinku Y, Gezahegn B, Feleke Z, Regassa Z, Mamo A, Assefa T, Gezahegn H, Solomon D, Atlaw D, Dessie M
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2087-2093
Published Date: 18 July 2022
Empagliflozin in Adults with Chronic Kidney Disease (CKD): Current Evidence and Place in Therapy
Colbert GB, Madariaga HM, Gaddy A, Elrggal ME, Lerma EV
Therapeutics and Clinical Risk Management 2023, 19:133-142
Published Date: 2 February 2023
Metabolic Syndrome and Tendon Disease: A Comprehensive Review
Lai C, Li R, Tang W, Liu J, Duan XD, Bao D, Liu H, Fu S
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1597-1609
Published Date: 9 April 2024
Prevalence and Factors Associated with Albuminuria Screening Among High-Risk Adults in Saudi Arabia: A Retrospective Cross-Sectional Study
Albekery MA, Alnuhait M, Alhomoud IS, Alhussain K, Alkulaib MK, Alanazi GM, Alshaikh ZF, Alibrahim FS, Alburayman KY, Alhajji GH, Almalki BA, Aldossary IF, Al Turki L, Almulhim A
International Journal of Nephrology and Renovascular Disease 2026, 19:580140
Published Date: 6 March 2026