Back to Journals » International Journal of General Medicine » Volume 16
Association Between ALDH2 Polymorphisms and the Risk of Diabetes Mellitus in Hypertensive Patients
Received 13 September 2023
Accepted for publication 29 November 2023
Published 6 December 2023 Volume 2023:16 Pages 5719—5727
DOI https://doi.org/10.2147/IJGM.S435598
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Miao Zeng,1,2,* Yiping Liu,1,2,* Yunquan Xie1,2
1Department of Laboratory Medicine, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China; 2Center for Precision Medicine, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Miao Zeng, Department of Laboratory Medicine, Meizhou People’s Hospital, No. 63 Huangtang Road, Meijiang District, Meizhou, People’s Republic of China, Email [email protected]
Background: Aldehyde dehydrogenase 2 (ALDH2) polymorphisms have been extensively studied in patients with hypertension (HTN) and diabetes mellitus (DM) in recent years. However, it is unclear whether ALDH2 polymorphisms are correlated with the risk of developing DM in patients with HTN. This study was designed to examine the association between ALDH2 single nucleotide polymorphism (SNP) rs671 and the risks of DM in patients with HTN.
Methods: This study retrospectively analyzed the patients with HTN who were treated in Meizhou People’s Hospital from August 2016 to December 2020, 788 HTN patients with DM as case patients, and 1632 HTN patients without DM history as controls. ALDH2 polymorphisms were analyzed using a polymerase chain reaction (PCR)-gene chip. Differences in ALDH2 genotypes between subjects and controls were compared. To analyze the relationship between ALDH2 genotype and DM risk, multiple logistic regression analysis was performed after adjusting for gender, age, smoking history, and drinking history.
Results: The proportion of the G/A plus A/A genotype was significantly higher in patients with DM than in controls (52.8% vs 48.2%, P=0.033). DM patients with G/A genotype had lower LDL-C (P< 0.017) than those with G/G genotype. The results of logistic regression analysis indicated that the G/A genotype increased the risk of DM in HTN patients, with an adjusted odds ratio (OR) of 1.209 (95% confidence interval (CI) 1.010– 1.446) (P=0.038), whereas the G/A plus A/A genotype in the dominant model increased the risk of DM significantly, with an adjusted OR of 1.203 (95% CI 1.013– 1.428) (P=0.035).
Conclusion: ALDH2 A allele (G/A + A/A genotype) increased the risk of DM in patients with HTN.
Keywords: aldehyde dehydrogenase 2, gene polymorphism, hypertension, diabetes mellitus
Introduction
Hypertension (HTN) is a critical cardiovascular risk factor that may lead to stroke, coronary heart disease, and other diseases worldwide, and is the leading cause of death in China.1,2 A study has shown that approximately 23.2% of Chinese people aged 18 years or older had HTN, of which only 15.3% achieved blood pressure control.3 However, the annual incidence of HTN continues to increase, and it has become a significant global disease burden.4 Diabetes mellitus (DM) is a chronic medical condition that frequently co-exists with HTN.5 Tatsumi et al and Wei et al showed that DM is almost 1.5 to 2.5 times as likely to develop in patients with HTN than in normotensive patients.6,7 Meanwhile, a study in China indicated that the prevalence of DM was approximately 20% among HTN patients and suggested that HTN may be a provoking factor for the development of diabetes.8 When combined with DM, HTN has been shown to predict and promote an increased risk of cardiovascular disease events and all-cause mortality over and above each risk factor alone, thereby increasing morbidity and mortality.9 Therefore, predicting whether HTN patients would have a DM risk is very important for both prevention and treatment. With the development of molecular biology and genetics, there has been considerable overlap between DM and HTN in etiology and disease mechanisms, suggesting either shared genetic or environmental factors in the etiology.7,10 Thus, it is of great importance to investigate the risk factors of DM in patients with HTN.
Aldehyde dehydrogenase 2 (ALDH2) is a mitochondrial enzyme responsible for detoxification of alcohol-derived acetaldehyde and endogenous aldehydes.11 ALDH2 is widely distributed in human liver, kidney, heart, lung, brain, and other tissues.12,13 The ALDH2 gene is located on chromosome 12 (12q24) and contains 13 exons.14 ALDH2 activity in vivo is closely related to the ALDH2 gene polymorphisms.15 Currently, some single nucleotide polymorphisms (SNPs) have been identified in ALDH2 gene. Exon 12 of the human ALDH2 gene has a G to A mutation (SNP rs671), resulting in a mutation of the glutamate residue at position 504 to lysine, which reduces the activity or even complete loss of the ALDH2 enzyme. According to this genetic mutation, ALDH2 can be classified into 3 different genotypes: wild-type (Glu504Glu), mutant heterozygote (Glu504Lys), and mutant homozygote (Lys504Lys). The Glu504Lys polymorphism can lead to a 30–50% enzyme activity of ALDH2.16,17
Studies have reported that the ALDH2 polymorphism may be associated with susceptibility to HTN and DM.12,18–20 However, in patients with HTN, the association between ALDH2 polymorphisms and DM risk remains unclear. Meizhou is a city located in the northeast of Guangdong Province, where the majority of residents are Hakka people.21 To date, there have been no reports on the relationship between ALDH2 polymorphisms and the risk of DM in HTN patients in this population. In the present study, ALDH2 rs671 G˃A allele/genotype frequencies and the association between ALDH2 SNP rs671 and the risk of DM in HTN patients were analyzed among Hakka people in southern China.
Materials and Methods
Subjects
A total of 2420 individuals with HTN were recruited from the inpatients of Meizhou People’s Hospital, Guangdong, China, from August 2016 to December 2020, and consisted of 788 patients with DM and 1632 individuals without DM as controls. HTN and DM were diagnosed by a clinician based on the etiology, history, lifestyle characteristics, clinical manifestations, complications, and examinations.22–24 Individuals with pre-existing chronic illnesses such as cancer or diseases of the heart, liver, or kidney were excluded. Information about the factors that influence HTN was recorded, including age, sex, smoking history, and alcohol abuse history. All control subjects were randomly selected from the Meizhou People’s Hospital during the same period. Information on age, sex, history of smoking, and history of alcohol consumption was collected from the Hospital Information System (HIS) of Meizhou People’s Hospital. This case-control study was performed in accordance with the ethical standards of the Declaration of Helsinki and approved by the Human Ethics Committees of Meizhou People’s Hospital.
Biochemical Analysis
Approximately 3 mL of venous blood from each subject was placed in a tube without an anticoagulant, and the serum was isolated and tested promptly. Serum samples were evaluated using the Olympus AU5400 system (Olympus Corporation, Tokyo, Japan) for homocysteine (HCY), total cholesterol (TC), triglycerides (TG), low-density lipoprotein-cholesterol (LDL-C), high-density lipoprotein-cholesterol (HDL-C), apolipoprotein B (Apo-B) and apolipoprotein A1 (Apo-A1). TC, TG, LDL-C, HDL-C, Apo-A1/Apo-B analyses were performed using the cholesterol esterase/peroxidase (CHOD/PAP) enzymatic method,25 glycerophosphate oxidase/peroxidase (GPO-PAP) enzymatic method, direct surfactant removal method,26 direct immunoinhibition method,27 and immunoturbidimetry method,28 respectively.
DNA Isolation and ALDH2 Genotyping
Approximately 2 mL of venous blood from each subject was stored in a tube containing ethylenediaminetetraacetic acid (EDTA), and genomic DNA was extracted from the whole blood using a QIAamp DNA Blood Mini Kit (Qiagen GmbH, North Rhine-Westphalia, Germany). DNA concentration was measured using a Nanodrop 2000TM Spectrophotometer (ThermoFisher Scientific, Massachusetts, USA). Polymerase chain reaction (PCR)-gene chip method was used for ALDH2 genotyping. PCR was performed with 25 μL volume reaction containing 50 ng of genomic DNA, 0.5 pM of each primer, 0.25 mM dNTPs, and 2 U Taq polymerase with denaturation step: 94°C for 5 min; amplification of 35 cycles: 94°C for 25s, 56°C for 25s, and 72°C for 25s; final elongation:72°C for 5 min. A specific hybridization reaction was performed between the amplification product and the detection probe fixed on the chip, and the color of the specific hybridization signal was determined by an enzymatic chromogenic reaction. The ALDH2 genotypes were analyzed using the BaiO Array Doctor Version 2.0 gene chip image analysis software, and BaiO® BE-2.0 genotype analysis software (BaiO Technology Co, Ltd., Shanghai, China).
Statistical Analysis
Data analysis was performed using SPSS statistical software (version 21.0; IBM Inc., USA). Quantitative data are expressed as mean value ± standard deviation (SD). Normally distributed data were analyzed using the Student’s t-test. The significance of differences in the proportion of patients with a history of DM between the two groups was tested using the chi-square test (X2). Differences in the distribution frequencies of genotypes and alleles between the two groups were analyzed using the X2 test. Univariate logistic regression analysis was used to test the association between DM and ALDH2 polymorphisms, and the results are presented as unadjusted odds ratios (OR) with confidence intervals (95% CI). Multivariate logistic regression was used to determine the risk factors for developing DM in HTN patients with adjustment for potential covariates: age, sex, smoking, and alcoholism, and the results were presented as adjusted ORs. P< 0.05 was considered to be statistically significant.
Results
General Characteristics
This study included 2420 participants, including 788 patients with DM (522 males and 266 females) and 1632 individuals without DM (1088 males and 544 females) as controls. Table 1 presents the general characteristics and biochemical variables of the patients in the DM and control groups. No statistically significant differences were observed between the groups in age (67.72±10.73 vs 67.83±12.08, P=0.814), different gender (P=0.836), smoking history (8.5% vs 18.0%, P=0.789), history of alcoholism (1.6% vs 3.5%, P=0.836), HCY (17.26±8.14 vs 17.24±8.39, P=0.852), TC (5.00±1.42 vs 4.92±1.26, P=0.182), and LDL-C level (2.78±1.00 vs 2.77±0.91, P=0.736). However, the differences between the two groups of TG (2.20±2.05 vs 1.66±1.35, P<0.001), HDL-C (1.22±0.37 vs 1.29±0.38, P<0.001), Apo-A1 (1.09±0.30 vs 1.14±0.32, P=0.001) and Apo-B (0.89±0.30 vs 0.85±0.26, P=0.010) were statistically significant.
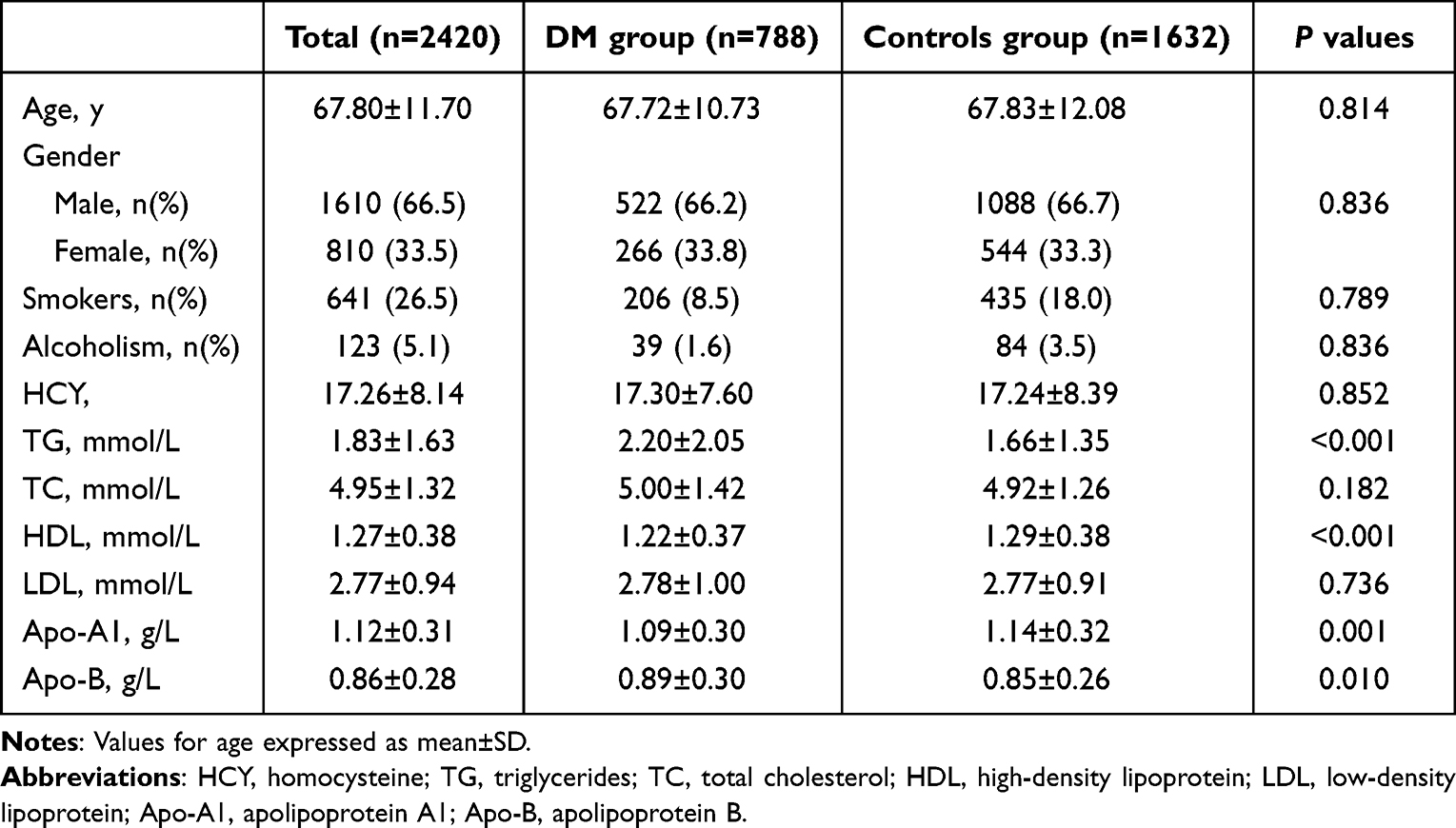 |
Table 1 Clinical Characteristics of the DM and the Control Groups |
ALDH2 Genotype and Allele Distribution
The observed ALDH2 genotype distributions in both the DM patients and controls were in Hardy-Weinberg equilibrium (χ2 = 1.992, P = 0.158 and χ2 = 0.030, P = 0.862, respectively). The proportion of the G/A + A/A genotypes was significantly higher in patients with DM (52.8%) than in controls (48.2%) (P=0.033, OR 1.204, 95% CI 1.015–1.427). There were no statistically significant differences in the G/A, and A/A genotypes between the DM patients and controls. Moreover, no statistically significant difference was observed in the proportion of G/G plus G/A genotypes between patients with DM and control participants (91.8% vs 92.3%, P=0.652). The frequencies of the G and A alleles in patients with DM were 69.5% and 30.5%, respectively, compared to 72.1% and 27.9% in controls, respectively, which was not statistically significant difference (P=0.063) (Table 2).
 |
Table 2 The Prevalence of ALDH2 Glu504Lys (rs671) Variants in DM Patients Group and Controls Group |
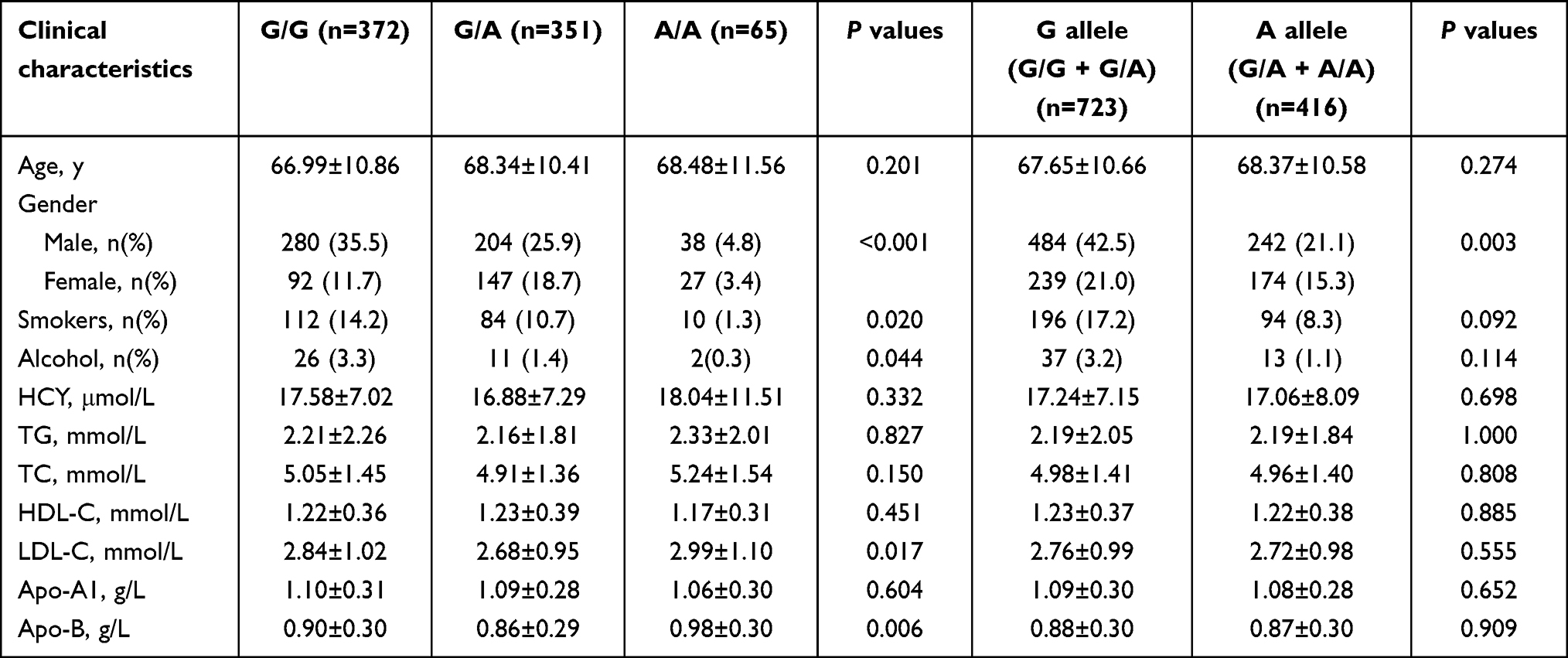 |
Table 3 Clinical Characteristics of DM Patients Stratified by ALDH2 Variants |
Clinical Characteristics of DM Patients Stratified by ALDH2 Genotypes and Alleles
The laboratory test results of patients with DM were analyzed according to ALDH2 variants, DM patients with ALDH2 G/G genotype had a higher percentage of male than those with the G/A and A/A genotypes (P<0.001). Furthermore, compared with G/G and G/A individuals, A/A individuals had lower frequencies of smoking (P=0.020) and alcohol consumption (P=0.044). DM patients with the G/A genotype had lower LDL-C (P<0.017) and Apo-B (P<0.006) levels than those in patients with the G/G and A/A genotypes. The clinical characteristics of DM patients with G and A allele were also compared. DM patients with the A allele had a lower percentage of female (P=0.003) than those with the G allele. There were no statistically significant differences in the percentage of smokers and alcohol consumption, age, HCY, TG, TC, HDL-C and Apo-A1 in patients with DM among G/G, G/A and A/A genotypes, as well as G and A alleles, respectively (Table 3).
Logistic Regression Analysis of Risk Factors Associated with DM in HTN Patients
Logistic regression analysis was used to evaluate independent predictors of DM. Univariate regression analysis was performed to obtain the unadjusted odds ratio (OR), and multiple logistic regression analysis was performed to obtain the adjusted OR. Relative analysis was used to evaluate the association between the genotypes frequencies of the ALDH2 gene polymorphisms and potential risk factors for DM. Three ALDH2 genetic modes of inheritance were identified: co-dominant mode (G/A vs G/G, A/A vs G/G, and A/A vs G/A), dominant mode (G/A + A/A vs G/G), and recessive mode (A/A vs G/G + G/A). Univariate logistic regression showed that ALDH2 rs671 G/A genotype (G/A vs G/G: OR 1.209, 95% confidence interval (CI): 1.012–1.445, P=0.036), and the G/A + A/A genotypes in the dominant model (G/A + A/A vs G/G: OR 1.204, 95% CI: 1.015–1.427, P=0.033) may increase the risk of DM in people with HTN.
The results of the multivariate logistic regression (adjusted for gender, age, smoking history, and drinking history) indicated that the G/A genotype increased the risk of DM in patients with HTN, with an adjusted OR of 1.209 (95% CI 1.010–1.446, P=0.038). Furthermore, the G/A + A/A genotype in the dominant model significantly increased the risk of DM, with an adjusted OR of 1.203 (95% CI 1.013–1.428, P=0.035). However, the A/A genotype was not an independent risk factor for DM in patients with HTN (Table 4).
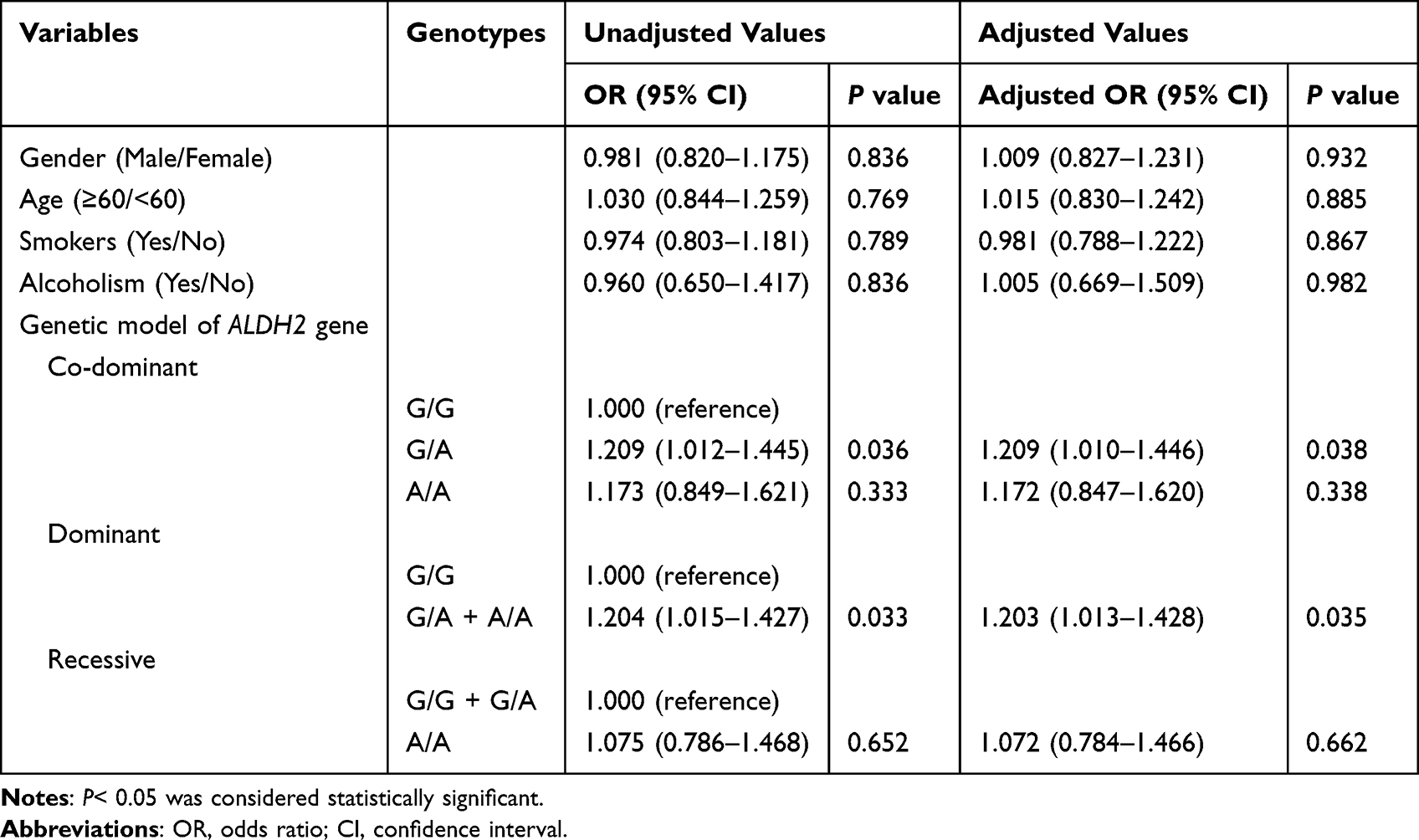 |
Table 4 Logistic Regression Analysis of Risk Factors Associated with DM |
Discussion
HTN is a common chronic disease and the most common preventable risk factor for all-cause death and disability worldwide.29 HTN commonly coexists with DM, leading to risk amplification.30 Some researchers have implied that focusing on the risk of developing DM may be beneficial for the treatment and control of HTN.31 ALDH2 polymorphisms are associated with HTN and DM, respectively.32,33
We found that TG and Apo-B levels were higher, and HDL-C and Apo-A1 levels were lower in the DM group than in the control group. Consistent with our results, a previous study showed that patients with abnormal lipid metabolism in HTN tend to have a higher risk of DM.34 In a rural Chinese population, high serum TG level and TG/HDL-C ratio increase the risk of T2DM.35 Low HDL-C level and high TG level increase the risk of T2DM in Chinese people.36 Ji et al found a gender difference between lipid ratio and T2DM prevalence.37 Therefore, regulating plasma lipid levels is a core issue for mitigating the risk of DM in patients with HTN. In addition, in present study, the proportion of alcohol in the DM patients with G/G genotype was significantly higher than that in the patients with G/A and A/A genotypes. People who carried the ALDH2 G/A and A/A genotypes have relatively low ALDH2 enzyme activity in the body, and various adverse reactions can occur quickly after a small amount of alcohol. This group of people is less able to clear acetaldehyde, so people with ALDH2 G/A and A/A genotypes will actively reduce their intake of ethanol.38,39
A study found that the prevalence of DM in HTN patients was about 20%, suggesting that HTN may be a predisposition factor for DM development.8 It is consistent with our findings. A meta-analysis based on genome-wide association studies (GWAS) data showed that the ALDH2 gene was associated with T2DM.40 Zhang et al reported that ALDH2 is one of the co-pathogenic genes of T2DM and mild cognitive impairment (MCI).41 Another study reported that the ALDH2 polymorphism might association with susceptibility to DM and showed a significantly lower risk of T2DM for ALDH2 G/G and G/A genotypes in China.42 Xu et al found that ALDH2 polymorphism is associated with an increased risk of T2DM in women with coronary artery disease (CAD).43 In terms of mechanism, Janus kinase-signal transducer and activator of transcription (JAK-STAT) is an important pathway of cytokine transduction, mainly involved in immune cell recognition and metabolic regulation.44,45 Studies have shown that Janus kinase 2 (JAK2) is related to insulin resistance, the destruction of JAK2 can promote insulin resistance and fat deposition, and the activation of JAK2 can cause STAT activation.46,47 STAT can activate insulin gene transcription and cell proliferation mediated by growth hormone or prolactin.48 Animal experiments have shown that STAT activation in islets can prevent lipid accumulation in islets and protect beta cells from the adverse effects of lipids, thus preventing the occurrence of diabetes.49 And the ALDH2 gene is associated with the JAK-STAT signaling pathway.50 According to the above studies, the results on the relationship between the risk of DM and HTN and the ALDH2 rs671 polymorphisms used as a predictor for the risk of T2DM still need more evidence with different sample sizes, regions, and ethnicities. Moreover, little is known about the link between ALDH2 gene polymorphisms and the risk of DM in HTN patients, and identification of susceptibility ALDH2 genes and other risk factors would be helpful for the prevention and treatment of DM in HTN patients.
In this study, no statistically significant differences were observed between the groups in terms of age, sex, smoking history, and alcohol consumption history. Studies have shown that the incidence of diabetes is related to age.51,52 Xue et al found that age is associated with an increased risk of DM.53 However, study has reported inconsistent results.54 This study showed that the incidence of DM in different age groups was not statistically significant. This may be related to the insufficient sample size of the study and age division. In addition, this study showed that gender is not a risk factor for DM in patients with HTN. DM is a major cardiovascular risk factor, and women with DM have a higher relative risk of cardiovascular events than men with DM.55 However, there are some differences in the results of some studies on the effect of gender on DM.56–58 Therefore, further research is needed to determine the effect of gender on DM risk. The relationship between smoking, alcohol consumption, and DM occurrence has been debated. Studies have shown that nicotine in tobacco affects the body composition, islet beta cells and insulin sensitivity.59 Holst et al showed that average weekly alcohol intake was associated with the risk of DM.60 Xue et al found that alcohol consumption is associated with an increased risk of DM.53 This study showed no clear correlation between the incidence of DM and smoking or alcohol consumption in HTN patients.60 In this study, there was no significant relationship between smoking and alcohol consumption and the risk of DM in HTN patients, which may be related to the differences in research methods, study sample size, and indicators included in the analysis of different studies, which need to be confirmed by further research.
The present study showed that patients who carried the G/A genotype had a 1.21-fold increased risk of developing DM. After adjusting for other established risk factors, the ALDH2 rs671 G/A genotype was an independent risk factor for DM in patients with HTN. However, this study had some limitations. First, this was a retrospective study, and there may have been selection bias because the patients were selected from one medical institution. Second, we analyzed the relationship between clinical indicators, smoking and drinking status, and ALDH2 gene polymorphisms in patients with HTN, without paying much attention to other complications. Third, all the participants in the present study had HTN, which made it more useful for specific patients. Finally, the region of the subjects in this study was relatively limited; therefore, there may be some deviations in the results. It is necessary to increase the sample size for this study, which will be the focus of our future work.
Conclusion
In the present study, among patients with HTN, the ALDH2 G/A + A/A genotype increased the risk of DM. Our results need to be confirmed in future studies with larger sample sizes. The results should enrich relevant data and provide valuable information for future research.
Abbreviations
ALDH2, Aldehyde dehydrogenase 2; HTN, hypertension; DM, diabetes mellitus; HCY, homocysteine; TG, triglycerides; TC, total cholesterol; HDL, high-density lipoprotein; LDL, low-density lipoprotein; Apo-A1, apolipoprotein A1; Apo-B, apolipoprotein B.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
As this study was a retrospective study, it was not possible for all participants to return to the hospital to sign informed consent. All participants were informed on the study procedures and goals and the informed consent from all the participants was obtained in verbal form through the telephone communication, which approved by the Ethics Committee of the Meizhou People’s Hospital. The study was performed under the guidance of the Declaration of Helsinki and approved by the Ethics Committee of Medicine, Meizhou People’s Hospital (Clearance No.: 2021-A-60).
Acknowledgments
The authors thank their colleagues, who were not listed in the authorship of the Department of Laboratory Medicine, Meizhou People’s Hospital, for their helpful comments on the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Program of Meizhou (Grant No.: 2019B0202001).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1736–1788. doi:10.1016/S0140-6736(18)32203-7
2. Zhang M, Shi Y, Zhou B, et al. Prevalence, awareness, treatment, and control of hypertension in China, 2004–18: findings from six rounds of a national survey. BMJ. 2023;380:e071952. doi:10.1136/bmj-2022-071952
3. Wang Z, Chen Z, Zhang L, et al. Status of hypertension in china: results from the china hypertension survey, 2012–2015. Circulation. 2018;137(22):2344–2356. doi:10.1161/CIRCULATIONAHA.117.032380
4. Turana Y, Tengkawan J. Hypertension and stroke in Asia: a comprehensive review from HOPE Asia. J Clin Hypertens. 2021;23(3):513–521. doi:10.1111/jch.14099
5. Sanchez R, Musso C. Hypertension and diabetes: an old association to be aware. Curr Hypertens Rev. 2021;17(2):84. doi:10.2174/157340211702211025101445
6. Tatsumi Y, Ohkubo T. Hypertension with diabetes mellitus: significance from an epidemiological perspective for Japanese. Hypertens Res. 2017;40(9):795–806. doi:10.1038/hr.2017.67
7. Cheung BM, Li C. Diabetes and hypertension: is there a common metabolic pathway? Curr Atheroscler Rep. 2012;14(2):160–166. doi:10.1007/s11883-012-0227-2
8. Deng H, Hu P, Li H, et al. Novel lipid indicators and the risk of type 2 diabetes mellitus among Chinese hypertensive patients: findings from the Guangzhou Heart Study. Cardiovasc Diabetol. 2022;21(1):212. doi:10.1186/s12933-022-01660-z
9. Alloubani A, Saleh A, Abdelhafiz I. Hypertension and diabetes mellitus as a predictive risk factors for stroke. Diabetes Metab Syndr. 2018;12(4):577–584. doi:10.1016/j.dsx.2018.03.009
10. Sunkara N, Ha C. Hypertension in diabetes and the risk of cardiovascular disease. Cardiovasc Endocrinol. 2017;6(1):33–38. doi:10.1097/XCE.0000000000000114
11. Zhang J, Guo Y. The role of aldehyde dehydrogenase 2 in cardiovascular disease. Nat Rev Cardiol. 2023;20(7):495–509. doi:10.1038/s41569-023-00839-5
12. Pang J, Wang J, Zhang Y, Xu F, Chen Y. Targeting acetaldehyde dehydrogenase 2 (ALDH2) in heart failure-Recent insights and perspectives. Biochim Biophys Acta Mol Basis Dis. 2017;1863(8):1933–1941. doi:10.1016/j.bbadis.2016.10.004
13. Chang YC, Chiu YF, Lee IT, et al. Common ALDH2 genetic variants predict development of hypertension in the SAPPHIRe prospective cohort: gene-environmental interaction with alcohol consumption. BMC Cardiovasc Disord. 2012;12:58. doi:10.1186/1471-2261-12-58
14. Yoshida A, Rzhetsky A, Hsu LC, Chang C. Human aldehyde dehydrogenase gene family. Eur J Biochem. 1998;251(3):549–557. doi:10.1046/j.1432-1327.1998.2510549.x
15. Mizoi Y, Yamamoto K, Ueno Y, Fukunaga T, Harada S. Involvement of genetic polymorphism of alcohol and aldehyde dehydrogenases in individual variation of alcohol metabolism. Alcohol Alcohol. 1994;29(6):707–710. PMID: 7695788.
16. Perez-Miller S, Younus H, Vanam R, Chen CH, Mochly-Rosen D, Hurley TD. Alda-1 is an agonist and chemical chaperone for the common human aldehyde dehydrogenase 2 variant. Nat Struct Mol Biol. 2010;17(2):159–164. doi:10.1038/nsmb.1737
17. Chen YC, Peng GS, Tsao TP, Wang MF, Lu RB, Yin SJ. Pharmacokinetic and pharmacodynamic basis for overcoming acetaldehyde-induced adverse reaction in Asian alcoholics, heterozygous for the variant ALDH2*2 gene allele. Pharmacogenet Genomics. 2009;19(8):588–599. doi:10.1097/FPC.0b013e32832ecf2e
18. Lee SW, Lee PH, Ahn JM, et al. Randomized trial evaluating percutaneous coronary intervention for the treatment of chronic total occlusion. Circulation. 2019;139(14):1674–1683. doi:10.1161/CIRCULATIONAHA.118.031313
19. Ma C, Yu B, Zhang W, Wang W, Zhang L, Zeng Q. Associations between aldehyde dehydrogenase 2 (ALDH2) rs671 genetic polymorphisms, lifestyles and hypertension risk in Chinese Han people. Sci Rep. 2017;7(1):11136. doi:10.1038/s41598-017-11071-w
20. He Q, Pan J, Wang L, Fang Y. Prospective study: aldehyde dehydrogenase 2 gene is associated with cardio-cerebrovascular complications in type 2 diabetes patients. J Diabetes Investig. 2021;12(10):1845–1854. doi:10.1111/jdi.13538
21. Wang WZ, Wang CY, Cheng YT, et al. Tracing the origins of Hakka and Chaoshanese by mitochondrial DNA analysis. Am J Phys Anthropol. 2010;141(1):124–130. doi:10.1002/ajpa.21124
22. O’Shea PM, Griffin TP, Fitzgibbon M. Hypertension: the role of biochemistry in the diagnosis and management. Clin Chim Acta. 2017;465:131–143. doi:10.1016/j.cca.2016.12.014
23. Parati G, Lombardi C, Pengo M, Bilo G, Ochoa JE. Current challenges for hypertension management: from better hypertension diagnosis to improved patients’ adherence and blood pressure control. Int J Cardiol. 2021;331:262–269. doi:10.1016/j.ijcard.2021.01.070
24. Harreiter J, Roden M. Diabetes mellitus: definition, classification, diagnosis, screening and prevention (Update 2023). Wien Klin Wochenschr. 2023;135(Suppl 1):7–17. doi:10.1007/s00508-022-02122-y
25. Trinder P, Webster D. Determination of HDL-cholesterol using 2,4,6-tribromo-3-hydroxybenzoic acid with a commercial CHOD-PAP reagent. Ann Clin Biochem. 1984;21(Pt 5):430–433. doi:10.1177/000456328402100516
26. Yu HH, Markowitz R, De Ferranti SD, et al. Direct measurement of LDL-C in children: performance of two surfactant-based methods in a general pediatric population. Clin Biochem. 2000;33(2):89–95. doi:10.1016/s0009-9120(00)00055-2
27. Langlois MR, Descamps OS, van der Laarse A, et al. Clinical impact of direct HDLc and LDLc method bias in hypertriglyceridemia. A simulation study of the EAS-EFLM Collaborative Project Group. Atherosclerosis. 2014;233(1):83–90. doi:10.1016/j.atherosclerosis.2013.12.016
28. Eugui J, Logroño MJ, Ruiz R, Zugaza C, Mirabel JL, Martínez C. Immunoturbidimetry of serum apolipoproteins A-I and B on the Cobas Bio centrifugal analyzer: method validation and reference values. Clin Biochem. 1994;27(4):310–315. doi:10.1016/0009-9120(94)90035-3
29. Oparil S, Acelajado MC, Bakris GL, et al. Hypertension. Nat Rev Dis Primers. 2018;4:18014. doi:10.1038/nrdp.2018.14
30. Li H, Hu YJ, Lin H, Xia H, Guo Y, Wu F. Hypertension and comorbidities in rural and urban Chinese older people: an epidemiological subanalysis from the SAGE study. Am J Hypertens. 2021;34(2):183–189. doi:10.1093/ajh/hpaa146
31. Wang J, Ma JJ, Liu J, Zeng DD, Song C, Cao Z. Prevalence and risk factors of comorbidities among hypertensive patients in China. Int J Med Sci. 2017;14(3):201–212. doi:10.7150/ijms.16974
32. Wu Y, Ni J, Cai X, et al. Positive association between ALDH2 rs671 polymorphism and essential hypertension: a case-control study and meta-analysis. PLoS One. 2017;12(5):e0177023. doi:10.1371/journal.pone.0177023
33. He Z, Guo Q, Ling Y, et al. Aldehyde dehydrogenase 2 rs671 polymorphism and multiple diseases: protocol for a quantitative umbrella review of meta-analyses. Syst Rev. 2022;11(1):185. doi:10.1186/s13643-022-02050-y
34. Hong M, Ling Y, Lu Z, et al. Contribution and interaction of the low-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and triglyceride to diabetes in hypertensive patients: a cross-sectional study. J Diabetes Investig. 2019;10(1):131–138. doi:10.1111/jdi.12856
35. Zhang M, Zhou J, Liu Y, et al. Risk of type 2 diabetes mellitus associated with plasma lipid levels: the rural Chinese cohort study. Diabetes Res Clin Pract. 2018;135:150–157. doi:10.1016/j.diabres.2017.11.011
36. Cui R, Qi Z, Zhou L, Li Z, Li Q, Zhang J. Evaluation of serum lipid profile, body mass index, and waistline in Chinese patients with type 2 diabetes mellitus. Clin Interv Aging. 2016;11:445–452. doi:10.2147/CIA.S104803
37. Ji XW, Feng GS, Li HL, et al. Gender differences of relationship between serum lipid indices and type 2 diabetes mellitus: a cross-sectional survey in Chinese elderly adults. Ann Transl Med. 2021;9(2):115. doi:10.21037/atm-20-2478
38. Zeng D, Huang Q, Yu Z, Wu H. Association between aldehyde dehydrogenase 2 gene rs671 G>A polymorphism and alcoholic liver cirrhosis in southern Chinese Hakka population. J Clin Lab Anal. 2021;35(7):e23855. doi:10.1002/jcla.23855
39. Chen Y, Liu H, Yu Z, et al. ALDH2 Polymorphism rs671 *1/*2 genotype is a risk factor for the development of alcoholic liver cirrhosis in Hakka alcoholics. Int J Gen Med. 2022;15:4067–4077. doi:10.2147/IJGM.S356761
40. Spracklen CN, Horikoshi M, Kim YJ. Identification of type 2 diabetes loci in 433,540 East Asian individuals. Nature. 2020;582(7811):240–245. doi:10.1038/s41586-020-2263-3
41. Zhang Y, Deng S, Zhong H, et al. Exploration and clinical verification of the blood co-expression genes of type 2 diabetes mellitus and mild cognitive dysfunction in the elderly. Biomedicines. 2023;11(4):993. doi:10.3390/biomedicines11040993
42. Li GY, Li ZB, Li F, et al. Meta-analysis on the association of ALDH2 polymorphisms and type 2 diabetic mellitus, diabetic retinopathy. Int J Environ Res Public Health. 2017;14(2):165. doi:10.3390/ijerph14020165
43. Xu F, Chen Y, Lv R, et al. ALDH2 genetic polymorphism and the risk of type II diabetes mellitus in CAD patients. Hypertens Res. 2010;33(1):49–55. doi:10.1038/hr.2009.178
44. Kaltenecker D, Themanns M, Mueller KM, et al. Hepatic growth hormone - JAK2 - STAT5 signalling: metabolic function, non-alcoholic fatty liver disease and hepatocellular carcinoma progression. Cytokine. 2019;124:154569. doi:10.1016/j.cyto.2018.10.010
45. Wu K, Tan XY, Xu YH, et al. JAK family members: molecular cloning, expression profiles and their roles in leptin influencing lipid metabolism in Synechogobius hasta. Comp Biochem Physiol B Biochem Mol Biol. 2017;203:122–131. doi:10.1016/j.cbpb.2016.10.004
46. Corbit KC, Camporez JPG, Edmunds LR, et al. Adipocyte JAK2 regulates hepatic insulin sensitivity independently of body composition, liver lipid content, and hepatic insulin signaling. Diabetes. 2018;67(2):208–221. doi:10.2337/db17-0524
47. Bousoik E, Montazeri Aliabadi H. “Do We Know Jack” about JAK? A closer look at JAK/STAT signaling pathway. Front Oncol. 2018;8:287. doi:10.3389/fonc.2018.00287
48. Friedrichsen BN, Galsgaard ED, Nielsen JH, Møldrup A. Growth hormone- and prolactin-induced proliferation of insulinoma cells, INS-1, depends on activation of STAT5 (signal transducer and activator of transcription 5). Mol Endocrinol. 2001;15(1):136–148. doi:10.1210/mend.15.1.0576
49. Jackerott M, Møldrup A, Thams P, et al. STAT5 activity in pancreatic beta-cells influences the severity of diabetes in animal models of type 1 and 2 diabetes. Diabetes. 2006;55(10):2705–2712. doi:10.2337/db06-0244
50. Yao S, Yin X, Chen T, et al. Exploring ALDH2 expression and immune infiltration in HNSC and its correlation of prognosis with gender or alcohol intake. Sci Rep. 2022;12(1):2504. doi:10.1038/s41598-022-06244-1
51. Bisson A, Bodin A, Fauchier G, et al. Sex, age, type of diabetes and incidence of atrial fibrillation in patients with diabetes mellitus: a nationwide analysis. Cardiovasc Diabetol. 2021;20(1):24. doi:10.1186/s12933-021-01216-7
52. Bastawrous A, Mathenge W, Wing K, et al. The incidence of diabetes mellitus and diabetic retinopathy in a population-based cohort study of people age 50 years and over in Nakuru, Kenya. BMC Endocr Disord. 2017;17(1):19. doi:10.1186/s12902-017-0170-x
53. Xue L, Wang H, He Y, et al. Incidence and risk factors of diabetes mellitus in the Chinese population: a dynamic cohort study. BMJ Open. 2022;12(11):e060730. doi:10.1136/bmjopen-2021-060730
54. Koye DN, Magliano DJ, Reid CM, et al. Trends in incidence of ESKD in people with type 1 and type 2 diabetes in Australia, 2002–2013. Am J Kidney Dis. 2019;73(3):300–308. doi:10.1053/j.ajkd.2018.10.005
55. Al-Salameh A, El Bouzegaoui N, Saraval-Gross M. Diabetes and cardiovascular risk according to sex: an overview of epidemiological data from the early Framingham reports to the cardiovascular outcomes trials Annales d’endocrinologie. Ann Endocrinol. 2023;84(1):57–68. doi:10.1016/j.ando.2022.09.023
56. Nakayama Y, Yamaguchi S, Shinzato Y, et al. Retrospective exploratory analyses on gender differences in determinants for incidence and progression of diabetic retinopathy in Japanese patients with type 2 diabetes mellitus. Endocr J. 2021;68(6):655–669. doi:10.1507/endocrj.EJ20-0630
57. Muilwijk M, Bolijn R, Galenkamp H, Stronks K, van Charante EM, van Valkengoed IGM. The association between gender-related characteristics and type 2 diabetes risk in a multi-ethnic population: the HELIUS study. Nutr Metab Cardiovasc Dis. 2022;32(1):142–150. doi:10.1016/j.numecd.2021.09.015
58. Yoshida Y, Chen Z, Rl B, et al. Sex differences in the progression of metabolic risk factors in diabetes development. JAMA Netw Open. 2022;5(7):e2222070. doi:10.1001/jamanetworkopen.2022.22070
59. Maddatu J, Anderson-Baucum E, Evans-Molina C. Smoking and the risk of type 2 diabetes. Transl Res. 2017;184:101–107. doi:10.1016/j.trsl.2017.02.004
60. Holst C, Becker U, Jørgensen ME, Grønbæk M, Tolstrup JS. Alcohol drinking patterns and risk of diabetes: a cohort study of 70,551 men and women from the general Danish population. Diabetologia. 2017;60(10):1941–1950. doi:10.1007/s00125-017-4359-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of CLTA-4 Gene Polymorphisms with Diabetes Mellitus: A Study Based on the Han Population of Northern China
Ren D, He L, Pang X
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2705-2712
Published Date: 3 September 2022
Acute Helicobacter pylori Infection Prevalence Among Renal Failure Patients and Its Potential Roles with Other Chronic Diseases: A Retrospective Cohort Study
Alhoufie ST, Ibrahim NA, Alhhazmi AA, Makhdoom HM, Ali HM, Hemeg HA, Almutawif YA, Mahallawi WH, Alfarouk KO
Infection and Drug Resistance 2022, 15:6589-6599
Published Date: 10 November 2022
Trends and Comparisons of Blood Pressure and Fasting Plasma Glucose in Patients with Hypertension, Diabetes, and Comorbidity: 4-Year Follow-Up Data
Xu L, Wen X, Yang Y, Cui D
Risk Management and Healthcare Policy 2022, 15:2221-2232
Published Date: 25 November 2022
Metabolic Syndrome and Tendon Disease: A Comprehensive Review
Lai C, Li R, Tang W, Liu J, Duan XD, Bao D, Liu H, Fu S
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1597-1609
Published Date: 9 April 2024
Assessment of Health-Related Quality of Life Among Patients with Chronic Diseases and Its Relationship with Multimorbidity: A Cross-Sectional Study from Saudi Arabia
Alzarea AI, Khan YH, Alzarea SI, Alanazi AS, Alsaidan OA, Alrowily MJ, Al-Shammari M, Almalki ZS, Algarni MA, Mallhi TH
Patient Preference and Adherence 2024, 18:1077-1094
Published Date: 4 June 2024