Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Perceived Diabetes Burden, Clinical Care Gap, and Intent to Prescribe a Diabetes Polypill to Indian Patients with Type 2 Diabetes
Authors Heine RJ, Bhattacharya I, Singh M
Received 20 August 2025
Accepted for publication 30 December 2025
Published 12 February 2026 Volume 2026:19 547492
DOI https://doi.org/10.2147/DMSO.S547492
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Robert J Heine,1 Indranil Bhattacharya,2 Maithri Singh3
1Cardiometabolic Health, Eli Lilly and Company, Indianapolis, IN, USA; 2Medical Affairs, Eli Lilly and Company Private Limited, Gurugram, Haryana, India; 3Primary Intelligence Division, IQVIA, Bengaluru, Karnataka, India
Correspondence: Indranil Bhattacharya, Eli Lilly & Company Pvt. Ltd., Plot No. 92, Sector 32, Institutional Area, Gurugram, 122001, India, Tel +91 9818536070, Email [email protected]
Purpose: Type 2 diabetes (T2D) is often associated with hypertension and dyslipidemia and is known to increase the risk for cardiovascular disease (CVD). A fixed-dose diabetes polypill, which can lower glycemia, blood pressure, and cholesterol, can improve treatment adherence in patients with T2D. This survey was conducted among healthcare professionals (HCPs) in India to assess the perceived T2D burden, clinical gaps, and intent to prescribe polypill to patients.
Methods: The study was conducted in two phases: Phase 1 quantitative online/in-person surveys to assess patient load, proportion of treatment-naïve patients, initiated/current treatment, patients achieving glycemic goals, and intent to prescribe polypill; and Phase 2 quantitative telephonic-aided online surveys to evaluate factors impacting treatment choice, validating polypill concept, and intention to prescribe.
Results: Phase 1 survey included 5,000 respondents (3,000 general practitioners [GPs], 1,500 diabetologists, 500 endocrinologists) and Phase 2 survey included 500 respondents (300 GPs, 150 diabetologists, 50 endocrinologists). Approximately 92% of HCPs indicated concern regarding treatment adherence for all risk factors. Treatment goals were reported to be achieved in 67%, 58%, and 52% patients for hyperglycemia, hypertension, and dyslipidemia, respectively. The most preferred pharmacological treatment approach was combination therapy (65%); around 84% of physicians preferred a fixed-dose therapy. Approximately, 79% HCPs believed that polypill demonstrated greater benefits compared to other products, and 86% of HCPs had high intention to prescribe polypill. The survey results indicated that most HCPs preferred fixed-dose therapy, and believed that a fixed-dose diabetes polypill could be beneficial in reducing T2D associated CVD risk factors in patients.
Conclusion: Most HCPs considered CVD risk management and adherence to medication as serious challenges and intended to prescribe an affordable and efficacious diabetes polypill to patients with T2D to lower CVD risk.
Keywords: cardiovascular disease, dyslipidemia, fixed-dose combinations, hypertension
Introduction
Diabetes is a chronic life-long metabolic disease characterized by hyperglycemia and the presence of multiple risk factors for cardiovascular disease (CVD). Diabetes is one of the major causes of morbidity and mortality, thereby posing a significant health burden from a human suffering and economic standpoint.1,2 Hypertension and dyslipidemia are common risk factors associated with the rising prevalence of Type 2 diabetes (T2D).3 As per the World Health Organization (WHO), approximately 17.9 million deaths were reported due to CVDs in 2019, and the number is expected to rise to 23.6 million by 2030.4,5 This number is particularly higher in low- and middle-income countries (LMICs).4 As per the Non-Communicable Diseases Risk Factor Collaboration (NCD-RisC), 828 million adults had diabetes in 2022 worldwide, with 212 million adults from India, of whom 30% were untreated.6
Adults with diabetes are more prone to CVD with 2–4 times higher risk than people without diabetes.7 There is strong evidence for the premise that effective risk factor management can lower cardiovascular complications in patients with T2D.8 However, CVD risk factor management is challenging in people with diabetes with only ~7.7% of patients in India achieving the recommended treatment goals of LDL, blood pressure, and glucose levels.9 As per the National Indian Council of Medical Research-India Diabetes-13 study, glycemic targets (hemoglobin A1c <7%) were achieved by around 1 in 3 patients with diabetes, blood pressure (<140/90) was achieved by 48.8% patients, and cholesterol (<100 mg/dl) was achieved by 41.5% patients.9 The current treatment guidelines recommend lifestyle modifications along with drug combinations to prevent diabetes-related and cardiovascular complications in patients with T2D.10,11 Adherence to medications has been shown to be a serious challenge in patients with T2D and is associated with poor outcomes in terms of disease progression, morbidity, and mortality.12 Only a minority of patients are prescribed and take the recommended CVD risk-lowering medications in LMICs, contributing to the high morbidity and mortality.13,14
Among the various factors contributing to non-adherence of treatment, including affordability, the number of daily prescribed pills is one of the most important factors.15 Implementation of a polypill strategy with an affordable fixed-dose combination (FDC) might provide an effective approach to manage non-adherence to prescribed treatment and CVD risk management.
Introduction of a diabetes polypill containing blood pressure- and blood glucose-lowering agents, along with a statin for patients with T2D, could boost adherence and close the gap between recommended and prescribed therapy. Clinical guidelines for the treatment of diabetes and CVD recommend fixed-dose combinations where it makes sense to enhance patient adherence, cost-effectiveness, and improve clinical outcomes.16,17 Several studies have demonstrated better patient adherence applying a polypill approach to prescribed medications in high-risk patients including patients with CV disease.18,19
To understand the acceptability and intention to prescribe a diabetes polypill to patients with T2D, this survey was conducted throughout India among the healthcare practitioners (HCPs), including public and private setups comprising metros, Tier 1, Tier 2, and Tier 3 cities. To our knowledge, this is the first large-scale survey conducted in India to assess HCPs’ perceptions of diabetes burden, clinical care gaps, and the intention to prescribe a diabetes polypill to patients with T2D.
Materials and Methods
Phase 1 and Phase 2 Surveys
This survey was conducted among the HCPs including general practitioners (GPs), diabetologists (including consulting physicians [CPs] with high diabetes practice), and endocrinologists using a structured questionnaire (Tables 1 and 2). Informed consent was obtained from all the participants in the survey; however, being a survey, the study was exempted from ethical approval.
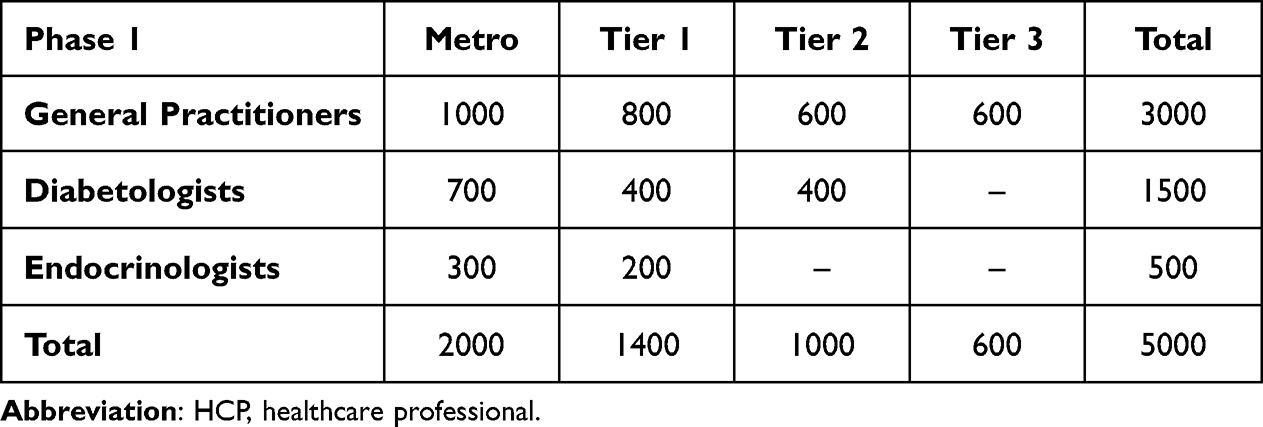 |
Table 1 Tier Wise Classification of the Types of HCPs Included in Phase 1 Survey |
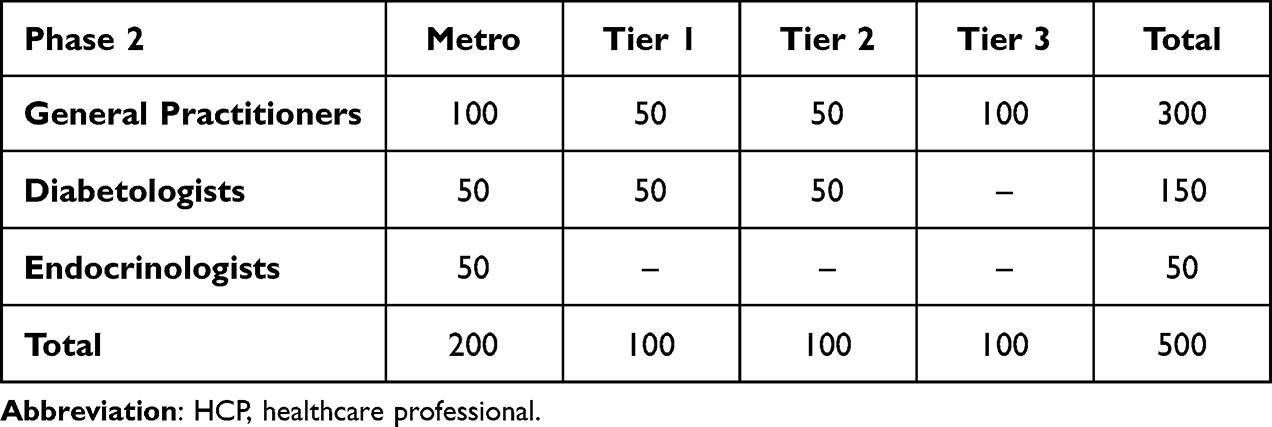 |
Table 2 Tier Wise Classification of the Types of HCPs Included in Phase 2 Survey |
HCPs with more than 3 years of experience in treating patients with diabetes and HCPs who were treatment initiators for at least 10% of the patients were included in the survey. Surveys were conducted in two phases, namely quantitative online and in-person surveys, and quantitative telephonic-aided online surveys. Phase 1 was conducted among 5,000 HCPs, and Phase 2 was conducted with a sample of 500. The sample size was representative and statistically significant for the HCP population surveyed with a confidence interval of 95% with a 5% margin of error.
The interview length for the quantitative interviews lasted 8–10 minutes for Phase 1 and 15–20 minutes for Phase 2. The survey questionnaire was designed and administered in a way to ensure that reliable, robust, and actionable results are achieved. Analysis was done at overall and tier class based (ie, metro cities [most developed cities with highest population], Tier 1 cities [population size >100,000], Tier 2 cities [50,000 to 100,000], and Tier 3 cities [population of 20,000 to 50,000]). City tiers were classified primarily based on population size, level of development, infrastructure, and economic activity.
Phase 1 survey evaluated the current T2D patient load, proportion of treatment-naïve patients, their current treatment (treatment initiated), proportion of patients achieving their treatment goals, and intention to prescribe polypill in patients. Phase 2 evaluated the factors impacting treatment choice for treatment-naïve patients among HCPs, validating the concept of polypill, and intention to prescribe a polypill.
Statistical Analysis
The study adopted a cross-sectional survey design. Data were collected using random sampling technique with an overall response rate of 1:4. To minimize bias, double-blind procedure was employed. Prior to data collection, five pilot interviews were conducted as a pre-test to validate the questionnaire flow. Statistical analyses were performed to summarize the data through frequency distributions, mean ratings, median, and other descriptive statistics. Significance testing was done at 95% confidence intervals at specialty level. Statistical procedures were adhered to the established standards to ensure the reliability and validity of the findings.
Results
Phase 1 results
Number of Patients per HCP/Clinic Among Cities (Tiers 1, 2, and 3) and HCPs (GP, CP/Diabetologists, Endocrinologists, Private and Public)
Overall, each HCP attended to 320 patients monthly on average. Patient load was lower in Tier 3 cities (284/HCP/month) and was higher among CP/diabetologists (388/HCP/month) and public set-ups (451/HCP/month) (Table 3). Approximately 23% patients were newly diagnosed with T2D, and 26% patients were not taking medication. A history of coronary artery disease was present in 24% patients. In total, 98% of HCPs considered lowering risk factors for CVD as important/very important.
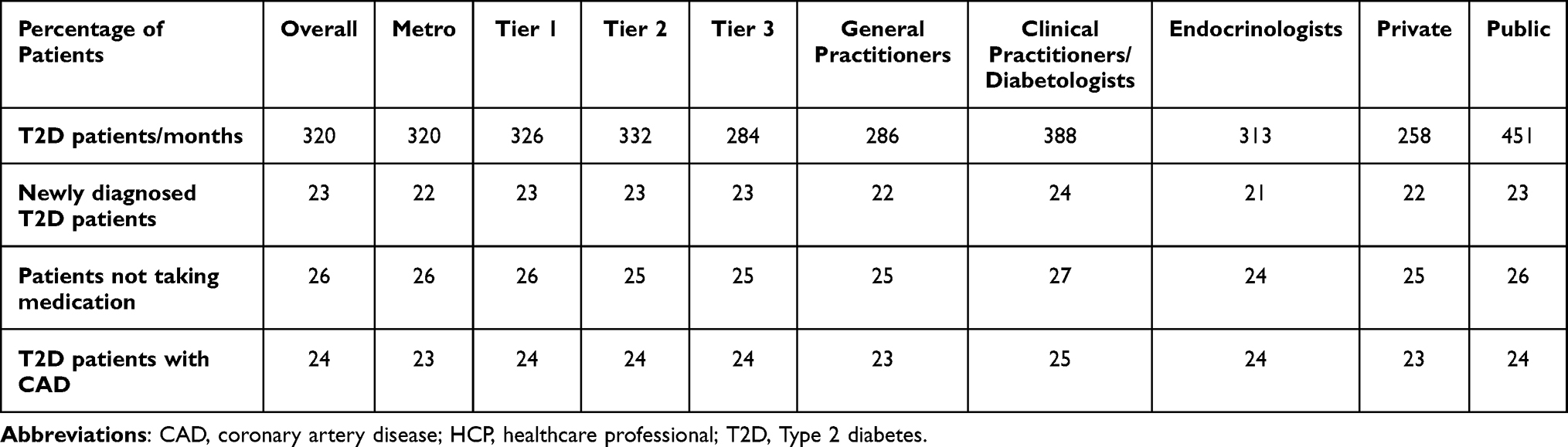 |
Table 3 Table Demonstrating T2D Patient Load Among Different HCPs and Cities Classified by Tiers and Metros |
Overall, HCP’s reported that 76% patients were receiving treatment for hyperglycemia and 67% patients were achieving treatment goals (Figure 1). Around 58% of patients were reported receiving treatment for hypertension, of whom only 58% of patients were achieving treatment goals. Of the 47% patients receiving treatment for dyslipidemia, only 52% were reported to have achieved treatment goals. Approximately 40% patients were receiving treatment for all three indications but only 48% of patients were reported to achieve treatment goals for all three indications.
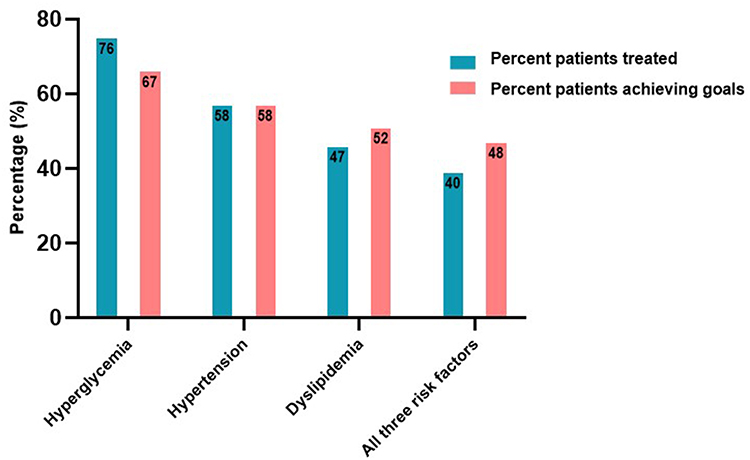 |
Figure 1 Figure demonstrating all data for proportion of patients receiving treatment and achieving goals for hyperglycemia, hypertension, dyslipidemia, and all three risk factors. Abbreviation: CV, cardiovascular. |
Approximately 80% of HCPs believed that the polypill demonstrated greater benefits compared to other products and 86% of HCPs had a good/high intention to prescribe a polypill. Majority of HCPs (82%) believed that the product would improve adherence to treatment, 81% believed that it would fulfil unmet treatment needs, and 77% believed that it would improve outcomes in treatment-naïve patients (Figure 2). Around 46% HCPs stated that they would prescribe the product 1–3 months post-launch.
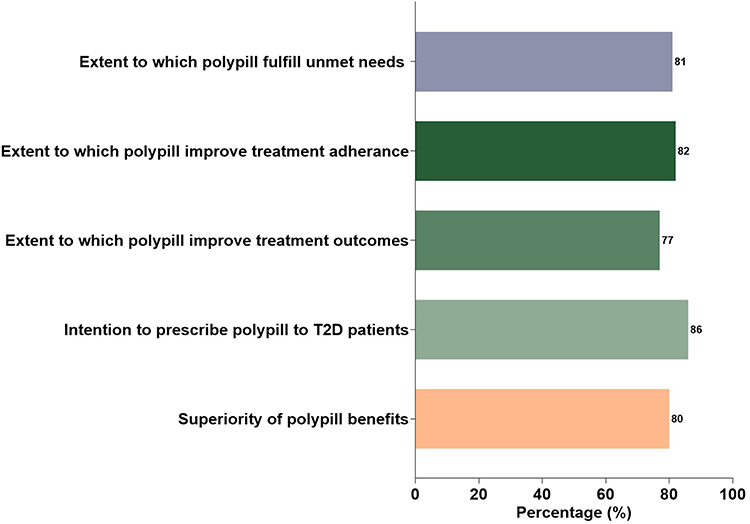 |
Figure 2 Figure demonstrating HCPs perceived benefits and intention to prescribe polypill as per Phase 1 survey. Abbreviations: HCP, healthcare professional; T2D, Type 2 diabetes. |
Phase 2 Results
Patient Load and Practice Dynamics
As reported, the average number of patients consulted per HCP/month was 320. About 24% of patients with T2D had not received treatment, and 26% of these were reported to be resistant to therapy. Among these, 14% of the patients resisted treatment due to high medication cost.
The profile of patients who resisted treatment was evenly distributed across age groups of <40 years (27%), 41–55 years (25%), 56–65 years (24%), and >65 years (24%), with 50% being non-smokers (Figure 3a and b).
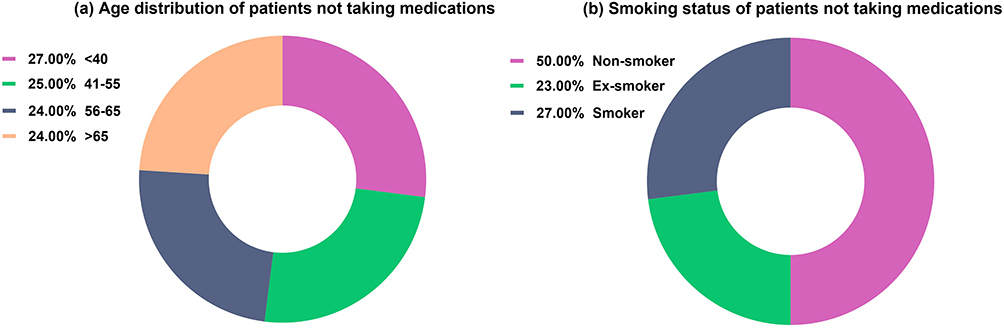 |
Figure 3 Pie chart demonstrating the (a) Age distribution (years), and (b) smoking status of patients who were not taking medication as per the Phase 2 survey results. |
Treatment Initiation Approach
The most preferred treatment initiation approach among the HCPs was pharmacological treatment (65%) compared to life-style modifications (35%) (Figure 4). This trend was higher in metros (79%) and especially among the endocrinologists (96%). Majority of the HCPs who initiated pharmacological treatment preferred to initiate glucose-lowering fixed-dose combination therapy (65%) compared to monotherapy (35%). FDC was the most preferred format among the HCPs who initiated a combination therapy (84%) compared to the free-form combination (16%). This trend was also observed, albeit at lower rate in Tier 3 cities (62%) and GPs (73%).
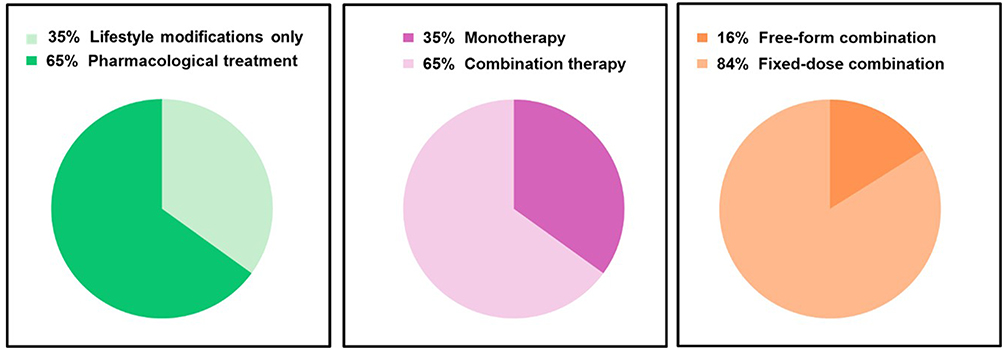 |
Figure 4 Pie chart demonstrating the most preferred treatment initiation approach undertaken by the HCPs as per Phase 2 survey. Abbreviation: HCP, healthcare professional. |
Hyperglycemia treatment was given the top priority (44%) for treatment initiation followed by hypertension (28%) and dyslipidemia (7%). Around 21% HCPs gave equal importance to all 3 indications. GPs assigned almost equal importance to treating hyperglycemia (39%) and hypertension (30%).
Biguanides/metformin was the most preferred molecule for hyperglycemia treatment initiation (62%) (Figure 5). This was followed by 18% preferring sulfonylureas and 11% preferring dipeptidylpeptidase-4 inhibitor; most preferred insulin was human premix. Angiotensin II receptor blocker (ARB) inhibitors were the most preferred drug class for hypertension treatment initiation (50%). This was followed by angiotensin-converting enzyme inhibitors (ACEi) (17% HCPs). Equal preference was given to ARBi (25%) and ACEi (26%) in Tier 3 cities.
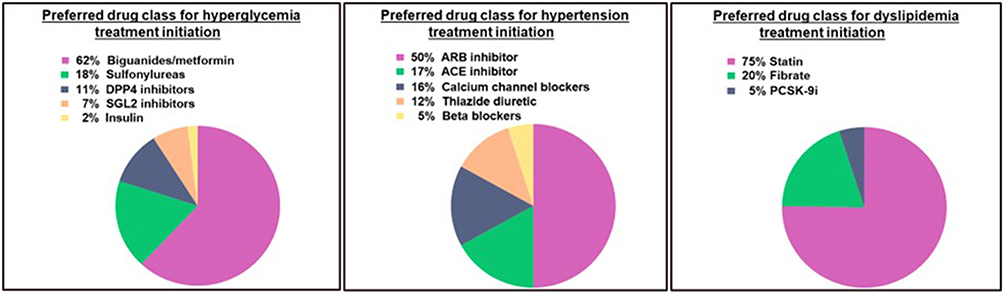 |
Figure 5 Pie chart demonstrating the preferred drug class choice for hyperglycemia, hypertension, and dyslipidemia treatment initiation by the HCPs. Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blocker; DPP4, dipeptidylpeptidase-4; HCP, healthcare professional; PCSK-9i, proprotein convertase subtilisin/kexin type 9 serine protease; SGL2, sodium-glucose cotransporter-2. |
Statins were the most preferred drug class for dyslipidemia treatment initiation (76%). This was followed by 20% preferring fibrates with fenofibrate being the most preferred drug.
Concerns Around Adherence and Generics
Overall, 80% to 90% of the HCPs stated concern over adherence to all the 3 risk factors (Table 4). Majority of HCPs (68%) preferred generic medications for treatment initiation in treatment-naïve patients with T2D. This preference was higher in Tier 3 cities (93%) and among GPs (81%). However, 92% of HCPs preferring generic medications expressed quality concerns.
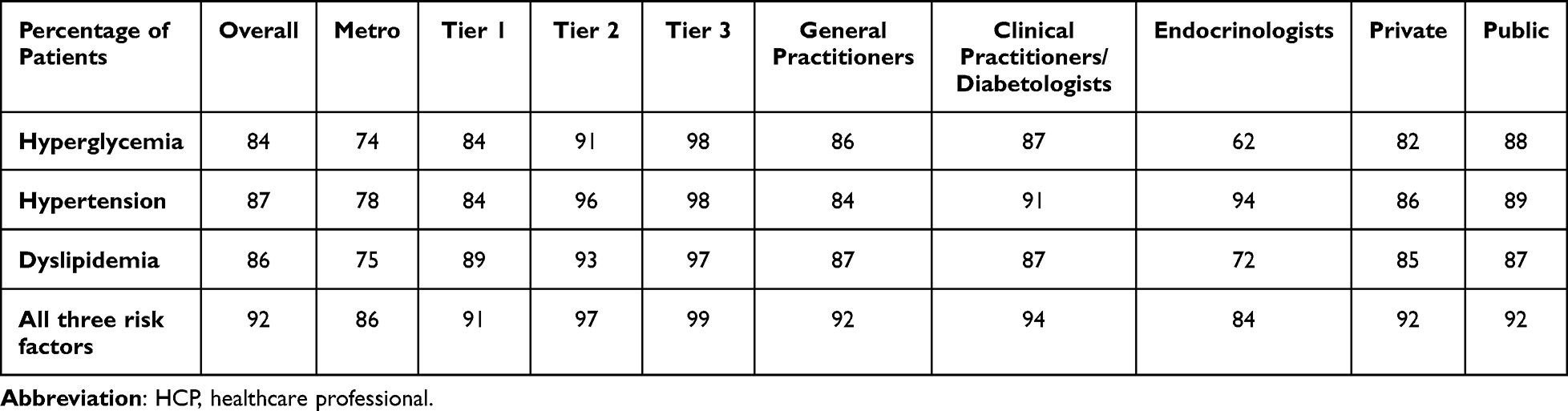 |
Table 4 Concern Towards Treatment Adherence Among Types of HCPs and Cities Classified by Tiers and Metros |
Intention to Prescribe a Polypill
Majority of HCPs (79%) believed that compared to other products, the polypill offered benefits (Figure 6) by improving adherence to treatment, fulfilling unmet needs, and improving patient outcomes. Approximately, 86% of HCPs had high intention to prescribe polypill.
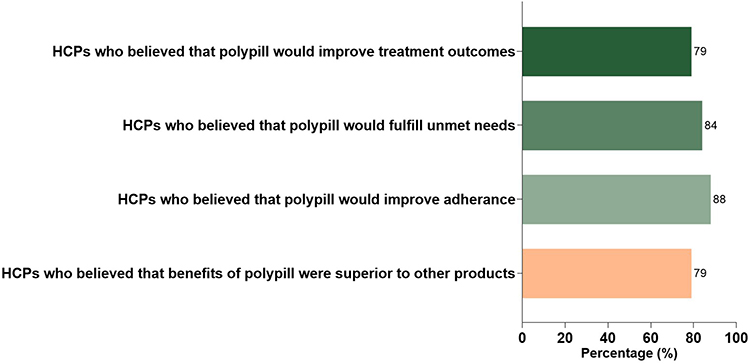 |
Figure 6 Bar graph demonstrating the perceived benefits and intention to prescribe polypill among HCPs as per Phase 2 survey. Abbreviation: HCP, healthcare professional. |
Around 1% HCPs had no/low intention to prescribe the polypill because of concerns related to different mechanism of action and onset of action of each molecule in the polypill.
Discussion
This survey was conducted to understand the readiness of HCPs to prescribe a polypill to patients with T2D and evaluate the existing clinical care gap. Almost all HCPs believed that it is important to lower all the three risk factors for CVD, that is, hyperglycemia, hypertension, and dyslipidemia. However, only 40% of patients attending the outpatient department were receiving treatment for all three indications and only 48% of patients were reported to achieve treatment goals, illustrating the existing clinical care gap. Proportion of patients being treated for all three conditions and achieving treatment goals were higher among endocrinologists than among GPs.
The HCPs indicated that a polypill could improve adherence and thereby outcomes; this perception was even higher in Tier 3 cities, and among GPs. The majority of the HCPs believed that the diabetes polypill provided benefits and expressed high intention to prescribe it to patients when available.
Adherence in patients with T2D to prescribed medications is around 50% and contributes to adverse healthcare outcomes.20 Major reported patient-related reasons for low adherence to medicines are lack of understanding about the disease, complications related to non-adherence, forgetfulness, and lack of family support. Health system-related barriers such as accessibility, affordability, and acceptability are also well documented. With almost half of the patients spending less than $11 (9 GBP) per month on their medication demonstrated affordability as a major barrier.21,22
Early and effective management of diabetes is important to prevent diabetes complications. In most LMICs, it is challenging to implement population-based prevention and management strategies for diabetes leading to a heightened disease burden.23 The WHO set targets for the management of people with T2D; by 2030, 80% of the patients will be diagnosed and 80% of patients will have a good control of glycaemia and hypertension, and 60% of those >40 years old will be receiving statins.24 To achieve the WHO targets and to bridge the gap between diagnosis, treatment, and achieving goals, it is essential to strengthen the healthcare system and to manufacture effective, safe, and affordable medicines. People with diabetes can benefit from a combination of drugs; however, adherence decreases with the number of prescribed pills and complex dosing regimens.25 A diabetes polypill seems an effective tool to improve adherence.15,16 The widespread acceptance and implementation of the cardiovascular polypill have thus far been slow, despite the available compelling evidence of its efficacy and safety.26–29 A polypill has shown to reduce the incidence of cardiovascular events in patients with intermediate cardiovascular risk,26 and significantly decrease the occurrence of a major cardiovascular event in patients when administered within 6 months of myocardial infarction without any major safety concerns.28 Similarly, the results from the QUARTET Phase 3 trial have shown that a polypill with 4 hypertensive drugs was able to manage blood pressure better than a single drug.29 Multiple polypills have been approved in India; however, their implementation into practice remains modest, and they are not yet part of the national guidelines due to various reasons including lack of awareness, availability, and affordability.14,30 It will require the availability of affordable medicines, medical education, awareness of physicians, and guidelines issued by healthcare systems recommending the use of these polypills.25 The acceptance and implementation of polypill are well-established in diseases such as malaria, tuberculosis, and HIV; however, there are still some barriers to its implementation for CVD prevention strategy in high-risk patients.25 This survey in India has demonstrated in the real-world setting the acceptability of a diabetes polypill by HCPs and highlights the conditions that need to be met for its successful implementation.
There are some limitations of the study. A survey could suffer from subjective bias which could be researchers’ bias or respondents’ bias and might compromise the objectivity of the study. Moreover, the findings from the survey may not be generalizable to the wider population. Other limitations include lack of real outcomes data, potential non-response bias, and short survey period. Despite these limitations, this is the first large-scale survey among different tiered cities and metros of its kind and adds value to the current literature by providing the real-world data regarding the HCPs acceptability of the concept of polypill, its perceived benefit for the treatment of T2D, and the conditions that need to be met in order to make an implementation successful. Further studies with real-world application are required to be conducted to assess the real benefits of the diabetes polypill and for its integration into the national guidelines.
Conclusions
A majority of HCPs indicated that an affordable, safe, and efficacious diabetes polypill that simultaneously lowers the main CVD risk factors could provide an opportunity to better manage the CVD risk factors by improving adherence to therapy. A majority of HCPs expressed the intent to prescribe a diabetes polypill to treatment-naïve patients with T2D. Real-world studies are required to validate the potential risks and benefits of a diabetes polypill-based treatment regimen.
Prior Presentations
The data from this paper was presented at the “52 Annual Conference of Research Society for The Study of Diabetes in India 2024” as poster presentation and at the “International Diabetes Federation World Diabetes Congress 2025” as an encore poster presentation with interim findings. The poster’s abstract was published in “Abstracts of The 52nd Annual Conference of Research Society for the Study of Diabetes in India. Int J Diabetes Dev Ctries 44 (Suppl 2), 83–172 (2024)”: DOI, https://doi.org/10.1007/s13410-024-01421-6.
Data Sharing Statement
Additional details relevant to materials, methods, and analyses used in this manuscript are available from the corresponding author upon reasonable request.
Ethics Statement
Data collection was undertaken in accordance with the Market Research Society of India (MRSI) code of conduct,31 and does not require approval from an ethical committee. Informed consent was obtained from all the participants in the survey.
Acknowledgments
Medical writing services were provided by Divya Kamboj from Syneos Health and were funded by Eli Lilly and Company.
Author Contributions
The authors have contributed to the manuscript as below:
Robert J Heine contributed to Conceptualization, Methodology, and Writing – Review & Editing. Indranil Bhattacharya was responsible for Conceptualization, Methodology, Writing – Original Draft, and Writing – Review & Editing. Maithri Singh handled Investigation, Data Curation, Formal Analysis, and Writing – Review & Editing.
All authors have given final approval of the version to be published, agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was sponsored by Eli Lilly and Company.
Disclosure
Robert J Heine and Indranil Bhattacharya are employees and shareholders of Eli Lilly and Company. Robert J Heine and Indranil Bhattacharya are involved in the development of novel medicines targeting the needs of low- and middle-income countries. Maithri Singh is an employee of IQVIA. The authors have no other conflicts of interest to declare.
References
1. Galindo RJ, Trujillo JM, Low Wang CC. et al. Advances in the management of type 2 diabetes in adults. BMJ Med. 2023;2(1):e000372. doi:10.1136/bmjmed-2022-000372
2. WHO diabetes fact sheet. Diabetes. Available from: https://www.who.int/health-topics/diabetes#tab=tab_1.
3. Hudspeth B. The burden of cardiovascular disease in patients with diabetes. Am J Manag Care. 2018;24(13):S268–10.
4. WHO fact sheet. Cardiovascular diseases (CVDs). Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
5. National Medical Research Council. Cardiovascular disease taskforce report. Available from: https://www.nmrc.gov.sg/docs/default-source/about-us-library/cvd-tf-summary-report.pdf.
6. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in diabetes prevalence and treatment from 1990 to 2022: a pooled analysis of 1108 population-representative studies with 141 million participants. Lancet. 2024;404(10467):2077–2093.
7. Dal Canto E, Ceriello A, Rydén L, et al. Diabetes as a cardiovascular risk factor: an overview of global trends of macro and micro vascular complications. Eur J Prev Cardiol. 2019;26(2_suppl):25–32. doi:10.1177/2047487319878371
8. Skyler JS. Effects of glycemic control on diabetes complications and on the prevention of diabetes. Clin Diabetes. 2004;22(4):162–166. doi:10.2337/diaclin.22.4.162
9. Anjana RM, Unnikrishnan R, Deepa M, et al. ICMR-INDIAB collaborators. Achievement of guideline recommended diabetes treatment targets and health habits in people with self-reported diabetes in India (ICMR-INDIAB-13): a national cross-sectional study. Lancet Diabetes Endocrinol. 2022;10(6):430–441. doi:10.1016/S2213-8587(22)00072-9
10. ElSayed NA, Aleppo G, Aroda VR, et al. On behalf of the American Diabetes Association. 3. Prevention or delay of type 2 diabetes and associated comorbidities: standards of care in diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S41–S48. doi:10.2337/dc23-S003
11. Denicolò S, Reinstadler V, Keller F, et al. Non-adherence to cardiometabolic medication as assessed by LC-MS/MS in urine and its association with kidney and cardiovascular outcomes in type 2 diabetes mellitus. Diabetologia. 2024;67(7):1283–1294. doi:10.1007/s00125-024-06149-w
12. Pourhabibi N, Sadeghi R, Mohebbi B, et al. Factors affecting nonadherence to treatment among type 2 diabetic patients with limited health literacy: perspectives of patients, their families, and healthcare providers. J Educ Health Promot. 2022;11:388. doi:10.4103/jehp.jehp_804_22
13. Short L, La VT, Patel M, et al. Primary and secondary prevention of CAD: a review. Int J Angiol. 2021;31(1):16–26. doi:10.1055/s-0041-1729925
14. Satheesh G, Gyawali B, Sun MFC, et al. A survey of availability and affordability of polypills for cardiovascular disease in selected countries. Glob Heart. 2024;19(1):56. doi:10.5334/gh.1335
15. Castellano J, Sanz G, Peñalvo J, et al. A polypill strategy to improve adherence: results from the FOCUS project. JACC. 2014;64(20):2071–2082. doi:10.1016/j.jacc.2014.08.021
16. Arya DS, Chowdhury S, Chawla R, et al. Clinical benefits of fixed dose combinations translated to improved patient compliance. J Assoc Physicians India. 2019;67(12):58–64.
17. Yazgi H, Mattikalli S, Fang B, et al. Efficacy of different polypill combinations for primary and secondary cardiovascular disease prevention: a systematic review and meta-analysis. Front Cardiovasc Med. 2025;12:1558579. doi:10.3389/fcvm.2025.1558579
18. Thom S, Poulter N, Field J, et al. Effects of a fixed-dose combination strategy on adherence and risk factors in patients with or at high risk of CVD: the UMPIRE randomized clinical trial. JAMA. 2013;310(9):918–929. doi:10.1001/jama.2013.277064
19. Patel A, Cass A, Peiris D, et al. A pragmatic randomized trial of a polypill-based strategy to improve use of indicated preventive treatments in people at high cardiovascular disease risk. Eur J Prev Cardiol. 2015;22(7):920–930. doi:10.1177/2047487314530382
20. Kronish IM, Ye S. Adherence to cardiovascular medications: lessons learned and future directions. Prog Cardiovasc Dis. 2013;55(6):590–600. doi:10.1016/j.pcad.2013.02.001
21. Krishnamoorthy Y, Rajaa S, Rehman T, Thulasingam M. Patient and provider’s perspective on barriers and facilitators for medication adherence among adult patients with cardiovascular diseases and diabetes mellitus in India: a qualitative evidence synthesis. BMJ Open. 2022;12(3):e055226. doi:10.1136/bmjopen-2021-055226
22. Kalra P, Mohan G, Tiewsoh I, et al. Clinico-epidemiological profile of type II diabetes mellitus in India – a multicentric institutional-based survey. medRxiv. 2024:2024–11. doi:10.1101/2024.11.06.24316048v1
23. Rasanathan K, Dako-Gyeke P, Isaranuwatchai W, et al. Non-communicable diseases: can implementation research change the game for policy and practice? Lancet. 2024;404(10466):1908–1910. doi:10.1016/S0140-6736(24)01309-6
24. Cheng AYY, Gomes MB, Kalra S, et al. Applying the WHO global targets for diabetes mellitus. Nat Rev Endocrinol. 2023;19(4):194–200. doi:10.1038/s41574-022-00793-1
25. Khan AA, Siddiqui SA, Yasmin F, et al. The era of polypills in the management of cardiovascular diseases: are we there yet? Curr Probl Cardiol. 2023;48(8):101233.
26. Yusuf S, Joseph P, Dans A, et al. Polypill with or without aspirin in persons without cardiovascular disease. N Engl J Med. 2021;384(3):216–228. doi:10.1056/NEJMoa2028220
27. Huffman MD, Patel A. Polypills - a central strategy for improving cardiovascular health. N Engl J Med. 2021;384(3):288–289. doi:10.1056/NEJMe2033310
28. Castellano JM, Pocock SJ, Bhatt DL, et al. Polypill strategy in secondary cardiovascular prevention. N Engl J Med. 2022;387(11):967–977.
29. Lim GB. Fixed-dose combination therapy and polypills to prevent and treat CVD. Nat Rev Cardiol. 2021;18(11):738–739.
30. Welcome Trust. Cardiovascular polypill. Current and evolving landscape for primary and secondary prevention. Available from: https://cms.wellcome.org/sites/default/files/cardiovascular-polypill-feb17.pdf.
31. Market Research Society of India. Code and Professional Standards. Available from: https://www.mrsi.co.in/code-of-conduct.html.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Critical Review of Medication Adherence in Hypertension: Barriers and Facilitators Clinicians Should Consider
Hamrahian SM, Maarouf OH, Fülöp T
Patient Preference and Adherence 2022, 16:2749-2757
Published Date: 7 October 2022
Patterns of Dyslipidemia in the Anemic and Nonanemic Hypertensive Saudi Population: A Cross-Sectional Study
Alfhili MA, Alsughayyir J, Basudan AM, Ghneim HK, Alfaifi M, Alamri HS, Awan ZA, Algethami MR
International Journal of General Medicine 2022, 15:7895-7906
Published Date: 21 October 2022
The Metabolic Score for Insulin Resistance (METS-IR) Predicts Cardiovascular Disease and Its Subtypes in Patients with Hypertension and Obstructive Sleep Apnea
Yang W, Cai X, Hu J, Wen W, Mulalibieke H, Yao X, Yao L, Zhu Q, Hong J, Luo Q, Liu S, Li N
Clinical Epidemiology 2023, 15:177-189
Published Date: 15 February 2023
Benefits of the Polypill on Medication Adherence in the Primary and Secondary Prevention of Cardiovascular Disease: A Systematic Review
Lopez-Lopez JP, Gonzalez AM, Lanza P, Lopez-Jaramillo P
Vascular Health and Risk Management 2023, 19:605-615
Published Date: 12 September 2023
Resistance Training in Cardiovascular Diseases: A Review on Its Effectiveness in Controlling Risk Factors
Nazir A, Heryaman H, Juli C, Ugusman A, Martha JW, Moeliono MA, Atik N
Integrated Blood Pressure Control 2024, 17:21-37
Published Date: 18 March 2024