Back to Journals » Infection and Drug Resistance » Volume 19
Penicillin Allergy Labels, Broad-Spectrum Antibiotic Use, and Chronic Obstructive Pulmonary Disease Exacerbations: A Population-Based Cohort Study from China
Authors Wu P, Xie T, Pan H, Tian Z, Wu B, Li Q, Chen Y, Hou X, Shao J, Gao S, Zhou X, Dong W, Xue J, Li T, Cai S, Chen Z ![]() , Liu Y, Zhou K
, Liu Y, Zhou K
Received 9 March 2026
Accepted for publication 6 June 2026
Published 20 June 2026 Volume 2026:19 597893
DOI https://doi.org/10.2147/IDR.S597893
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Peng Wu,1,2 Tian Xie,2 Haonan Pan,2,3 Zijian Tian,4 Benrui Wu,4 Qian Li,5 Ying Chen,6 Xiangqing Hou,2 Jian Shao,2 Shiteng Gao,2,3 Xiaozhou Zhou,5 Wanqing Dong,7 Jingnan Xue,1,2 Tao Li,8 Sijie Cai,8 Zhe Chen,8 Yijin Liu,1 Kaixin Zhou2,3
1State Key Laboratory of Medicinal Chemical Biology and College of Pharmacy, Nankai University, Tianjin, People’s Republic of China; 2Guangzhou National Laboratory, Guangzhou, People’s Republic of China; 3College of Public Health, Guangzhou Medical University, Guangzhou, People’s Republic of China; 4Institute of Biophysics, University of Chinese Academy of Sciences, Beijing, People’s Republic of China; 5College of Life Sciences, University of Chinese Academy of Sciences, Beijing, People’s Republic of China; 6Guangzhou Institutes of Biomedicine and Health, University of Chinese Academy of Sciences, Beijing, People’s Republic of China; 7College of Clinical Medicine, The First Affiliated Hospital of Henan University, Luoyang, People’s Republic of China; 8Department of Pulmonary and Critical Care Medicine, Affiliated Kunshan Hospital of Jiangsu University, Kunshan, People’s Republic of China
Correspondence: Yijin Liu; Kaixin Zhou, Email [email protected]; [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide, and acute exacerbations drive most of its burden. Around half of exacerbations are infection related, and penicillin-class antibiotics are widely used. However, penicillin allergy labels, often inaccurate, may divert prescribing towards broader-spectrum agents and worsen outcomes. We therefore examined whether such labels are associated with antibiotic prescribing patterns and subsequent risk of COPD exacerbations in a large cohort.
Methods: We conducted a retrospective cohort study in the Kunshan Aging Research with E-health (KARE) database (2016– 2024). We included 14,900 patients with COPD aged ≥ 40 years. Exposure was a documented penicillin allergy label in the electronic medical record. Outcomes were the risk and rate of subsequent COPD exacerbations. Cox proportional hazards models estimated the association with time to first exacerbation, and negative binomial regression assessed exacerbation rates.
Results: Of 14,900 patients, 722 (4.8%) had a penicillin allergy label. Overall, 2018 (13.5%) experienced at least one exacerbation during a median follow-up of 4.1 years. Compared with unlabeled patients, those with a penicillin allergy label received more broad-spectrum antibiotics and had a higher risk of exacerbations (adjusted hazard ratio 1.39, 95% confidence interval 1.17– 1.65) and higher exacerbation rates (adjusted incidence rate ratio 1.56, 95% confidence interval 1.25– 1.93).
Conclusion: In this Chinese COPD cohort, penicillin allergy labels were associated with broader-spectrum antibiotic use and an increased burden of exacerbations. Systematic verification and de-labelling of penicillin allergy may help optimise antibiotic use and improve COPD outcomes.
Keywords: chronic obstructive pulmonary disease, penicillin allergy, antibiotic stewardship, broad-spectrum antibiotics, exacerbation
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous, chronic respiratory condition characterized by persistent, progressive airflow limitation.1 It is currently the third leading cause of death worldwide, with acute exacerbations (AECOPD) being the primary cause of mortality.2 Bacterial infections account for up to 50% of AECOPD events, and penicillin-class antibiotics play a central role in managing exacerbations and recurrent respiratory infections.3,4 Despite this, approximately 5% to 16% of individuals in electronic medical records (EMRs) are labeled with a penicillin allergy, up to 90% of which has been disproven by formal testing.5,6 This widespread mis-labeling leads to unnecessary avoidance of penicillin, which increases the risk of treatment failure and adverse events in various medical conditions, ultimately contributing to poor patient outcomes.7,8
Although clinical studies have examined the consequences of penicillin allergy label in acute infections like pneumonia and COVID-19, little research has explored its impact on the long-term management of COPD.9,10 In contrast, managing COPD frequently necessitates recurrent antibiotic therapy throughout the disease course.11 A study from EXACOS-UK health care showed that respiratory infections and their antibiotics management prior to the first year of COPD diagnosis were associated with increasing rates of subsequent exacerbations in a median follow-up of 4 years. Consequently, the impact of allergy label on long-term exacerbation risk may also become apparent over an extended period.
A further complication in COPD management is unnecessary penicillin avoidance can promote consistent reliance on broad-spectrum alternatives. This, in turn, has been shown to increase the long-term risk of infections with methicillin-resistant Staphylococcus aureus and Clostridium difficile,12,13 potentially leading to faster disease progression in COPD patients.14–16 Hence, elucidating the long-term impact of penicillin allergy label on COPD management requires robust studies with large cohorts and extended follow-up periods.
Here, we leveraged a population-based longitudinal cohort linked with comprehensive EMRs spanning both primary and secondary care. Utilizing extensive prescribing data and medical diagnoses, we aimed to examine how penicillin allergy label impacts antibiotic prescription patterns and the risk of exacerbations among COPD patients.
Methods
Source Data
We conducted a retrospective cohort study using data from the Kunshan Aging Research with E-health database (KARE), an ongoing population-based study focused on aging-related diseases. The overall design of the KARE cohort has been described previously in a pharmacogenetic analysis and in a recent cohort profile.17,18 Briefly, KARE cohort currently includes approximately 130,000 older adults who were recruited through annual health examinations conducted in primary care settings. All participants provided written informed consent for the linkage of their electronic medical records, which integrate both primary and secondary care data, including prescription records, chronic disease management, and hospital-based diagnoses and treatments. The study protocol was approved by the Institutional Review Board of Kunshan First People’s Hospital, Affiliated to Jiangsu University (IEC-C-007-A07-V3.0).
Study Population
The study included patients aged ≥40 years old with a documented diagnosis of COPD (ICD-10 codes: J41-J44) between January 2016 and August 2024. COPD patients were identified with two outpatient codes on distinct dates or one inpatient codes to improve the reliability of case identification.19 Spirometry data were available only for 1139 participants and therefore were not required for inclusion in the primary analysis. To evaluate the long-term impacts of allergy label on antibiotic use and clinical outcomes, the study population was restricted to COPD patients with at least 2 years of antibiotics usage in the prescription database (Supplementary Figure 1). The index date was defined as the earliest recorded COPD diagnosis during the study period. Patients were tracked from the date diagnosed COPD to the first exacerbation event, death, or August 2024, whichever occurred first (Figure 1).
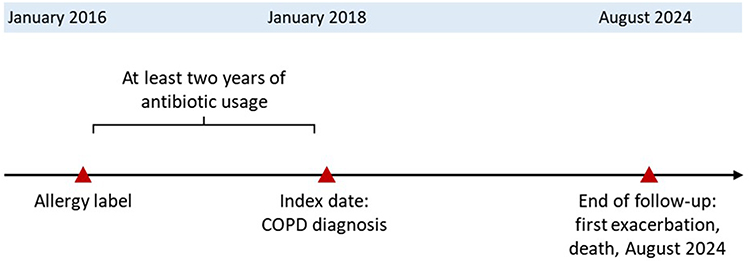 |
Figure 1 Study design and follow-up timeline. |
Allergy Documentation
The interest exposure was a documented penicillin allergy, defined as an allergy to penicillin-class antibiotics, including penicillin G derivatives, aminopenicillins, penicillinase-resistant penicillin, and extended-spectrum penicillin. Allergy documentation was extracted from the annual health examination system and medical history. Penicillin allergy status recorded prior to the index date was assumed to persist throughout the follow-up period. Patients with documented allergies to other drugs or foods were excluded.
Antibiotics Use
Antibiotic utilization during the 2 years before the start of follow-up was assessed to characterize baseline prescribing patterns associated with penicillin allergy labels. Prescription data were extracted from both primary care and hospital settings, ensuring comprehensive capture of outpatient and inpatient antibiotic use. Antibiotics were classified into therapeutic classes, including penicillins (eg, penicillin, benzathine penicillin, amoxicillin-clavulanate, and piperacillin-tazobactam), cephalosporins (first, second, and third generation), macrolides, quinolones, lincosamides, and aminoglycosides.
Clinical Outcome
The primary outcome was time to the first moderate or severe exacerbation during follow-up. Severe exacerbation was defined as a hospital admission with a primary diagnosis of COPD (ICD-10 codes J44.0 or J44.1). Moderate exacerbation was defined as a co-prescription of corticosteroid and antibiotic on the same day, accompanied by an outpatient respiratory diagnosis. Respiratory diagnoses included outpatient diagnoses of COPD, acute exacerbation, acute bronchitis, lower respiratory tract infection, or other respiratory conditions judged clinically compatible with treated COPD exacerbation. These definitions have been extensively used in observation studies.20,21 To avoid misclassifying prolonged events as multiple exacerbations, a 14-dayrolling window was applied to differentiate distinct exacerbation episodes. The secondary outcome was the total number of moderate and severe exacerbations during follow-up.
Statistical Analysis
Baseline characteristics were summarized as counts and percentages for categorical variables. Continuous variables were summarized as mean (SD) when approximately normally distributed and as median (interquartile range) when skewed. Differences between groups were assessed using the chi-squared test for categorical variables and the Wilcoxon rank-sum test for continuous variables.
Time-to-event analyses were performed using the Kaplan–Meier method with Log rank tests to compare cumulative incidence between exposure groups. Cox proportional hazards models were applied to estimate hazard ratios (HRs) with 95% confidence intervals (CIs) for time to first exacerbation. The proportional hazard assumption was tested by using the Schoenfeld global test. Negative binomial regression models were used to test incident rate ratios (IRR) differences between groups. Covariates used in the model included age, gender, body mass index (BMI), smoking status, hypertension, diabetes, Charlson Comorbidity Index (CCI, but excluding COPD itself), bronchiectasis, asthma, pneumonia, exacerbation history, prior antibiotic counts, long-acting beta-agonists use (LABA), long-acting muscarinic antagonists use (LAMA), short-acting beta-agonists use (SABA), short-acting muscarinic antagonists use (SAMA). Missing values in baseline variables were coded as “missing” and included in the final models.
Subgroup analysis was performed for patients with different CCI score (CCI = 0 or >0) at baseline, and frequency of broad-spectrum antibiotics usage. Moreover, as spirometry measurements were not included as covariates due to a high proportion of missing values, a tipping point analysis on the robustness of the results to an unobserved spirometry confounder (ie, FEV1).
All analyses were performed using R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria). A two-sided P-value <0.05 was considered statistically significant.
Result
Patient Characteristics
In total, 14,900 COPD patients (mean age 68.8 years) were included in the current study, 722 of whom (4.8%) had a documented penicillin allergy. Baseline characteristics of patients are detailed in Table 1. Overall, patients documented penicillin allergy were more likely to be female, less smokers, and have a higher burden of comorbidity, compared to those without penicillin allergy label. Patients with documented penicillin allergy also showed a higher prevalence of asthma and greater use of short-acting bronchodilators, whereas the use of long-acting bronchodilators was similar between groups. These patterns likely reflect underlying allergic or asthmatic predisposition among patients carrying an allergy label.
 |
Table 1 Baseline Characteristics of Entire Study Cohort Based on Allergy Label Grouping |
Antibiotic Use
We then compared 2 years antibiotic use prior to index date between COPD patients with and without documented penicillin allergies (Figure 2). Patients with documented penicillin allergies were more likely to be prescribed lincosamide (IRR: 2.58, 95% CI: 1.89–3.58), aminoglycosides (IRR: 1.88, 95% CI: 1.48–2.40), macrolides (IRR: 1.43, 95% CI: 1.29–1.59), and quinolones (IRR: 1.36, 95% CI: 1.19–1.56) compared to those without allergy documentation. Conversely, penicillin allergic patients had lower usage of penicillin (IRR: 0.75, 95% CI: 0.60–0.94). These findings suggest that penicillin allergy documentation was associated with prescribing broader-spectrum antibiotic shifts.
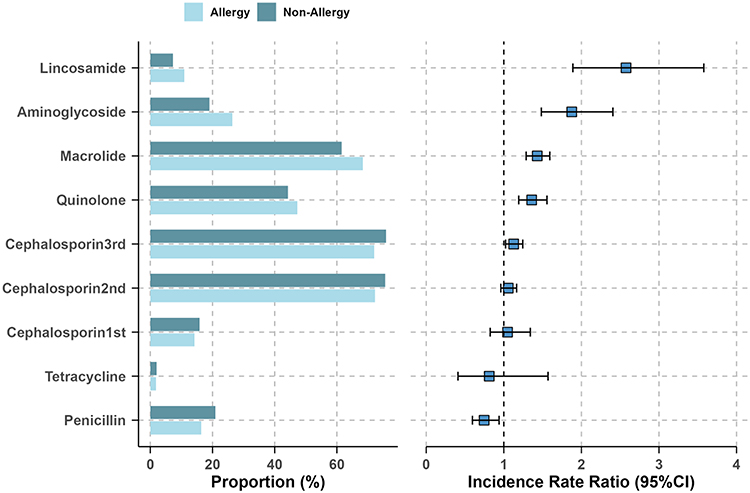 |
Figure 2 Antibiotic class usage and incidence rate ratios in COPD patients with and without penicillin allergy label. Incidence rate ratios compare antibiotic prescription counts between groups. |
Clinical Outcome
Among the 14,900 COPD patients, 2018 patients had an incidence of moderate or severe exacerbation (event rate 3.4 per 100 patient-years) during a median follow-up period of 4.1 years (IQR, 2.5–5.6 years). As shown in Figure 3, the univariable analysis suggested that the patients with penicillin allergy documentation had a significantly higher (HR=1.64, 95% CI: 1.39–1.94) risk than those non-allergies.
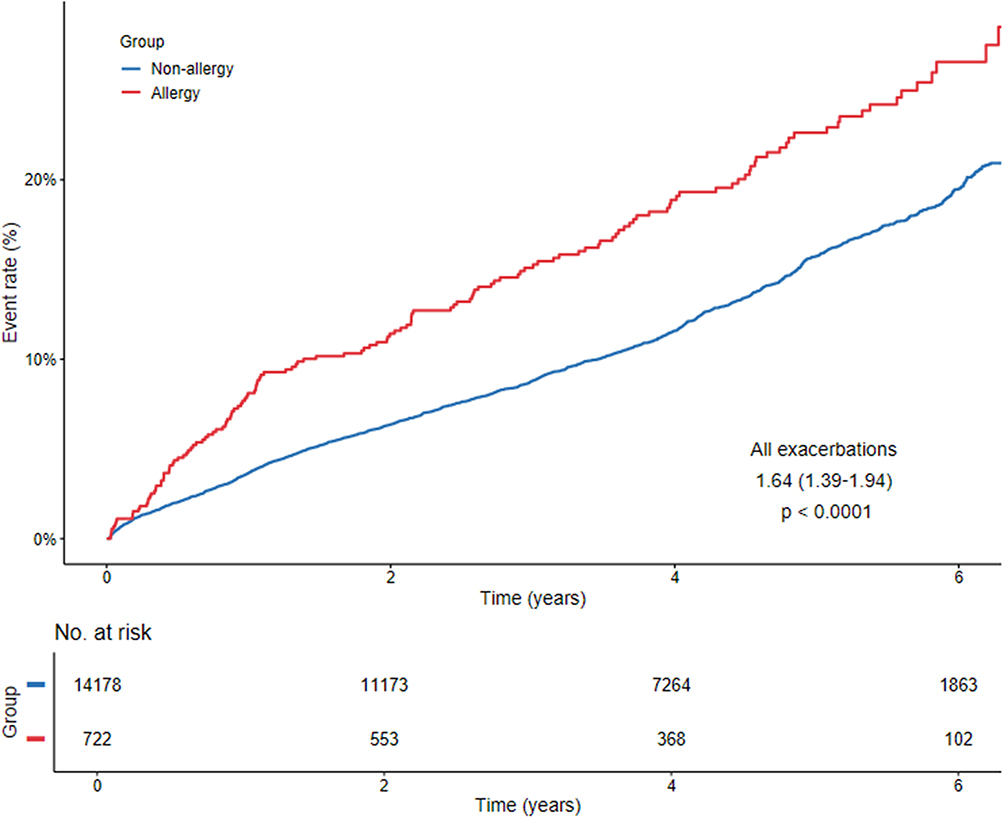 |
Figure 3 Cumulative risk of COPD exacerbation according to the presence of a penicillin allergy label, estimated by Kaplan-Meier analysis. P values were calculated using the Log rank test. |
For the primary outcome, penicillin allergy documentation was significantly associated with an increased risk of COPD exacerbations (Figure 4). Multivariable Cox regression analysis revealed that patients with documented allergies had a 39% higher risk of all exacerbations (adjusted HR: 1.39, 95% CI: 1.17–1.65) compared to non-allergic patients after adjusting for covariates. The heightened risk was even more pronounced for severe exacerbations (adjusted HR: 1.59, 95% CI: 1.20–2.11).
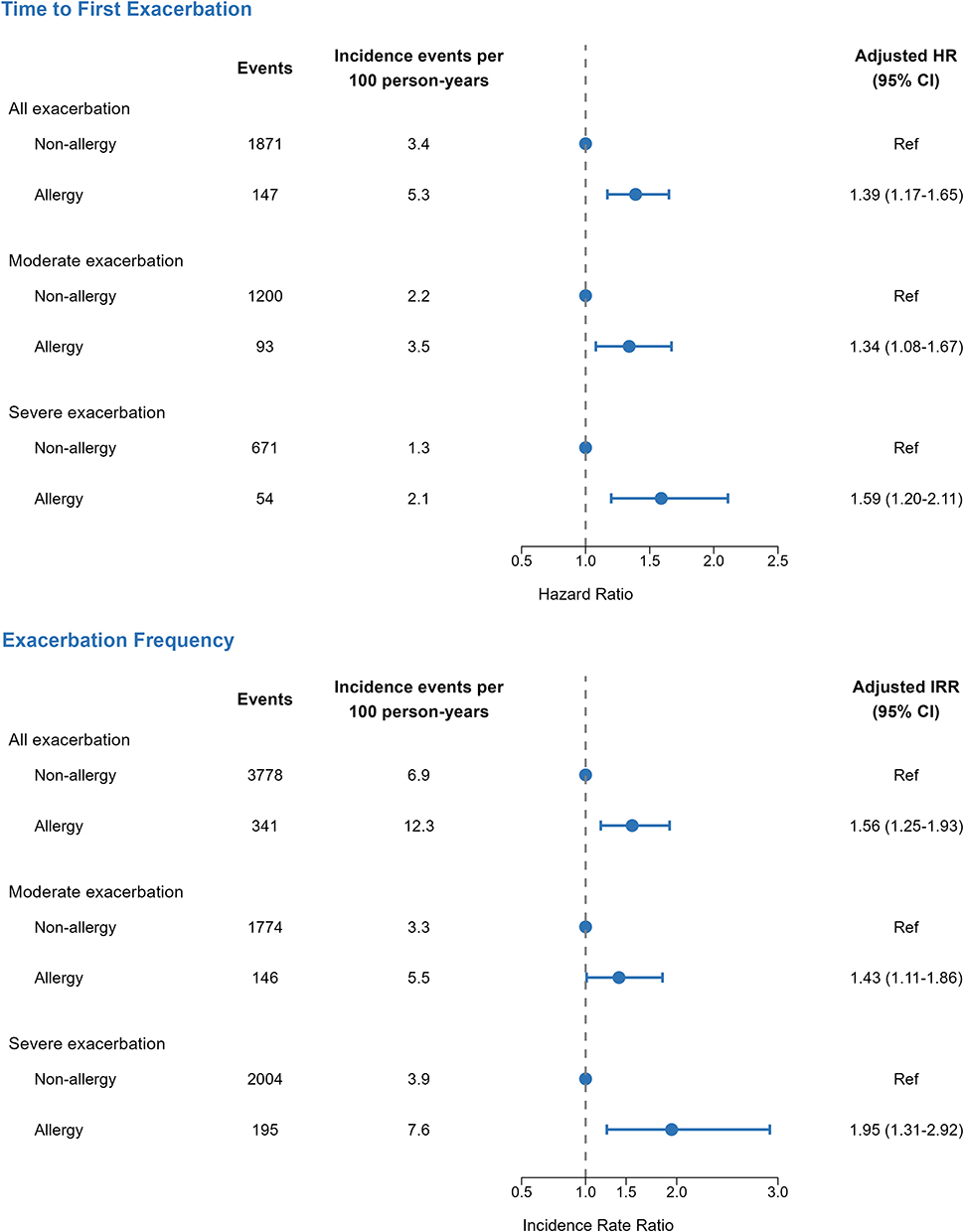 |
Figure 4 Associations between penicillin allergy label and COPD exacerbations. Hazard ratios were estimated using Cox proportional hazards models for time to first exacerbation, and incidence rate ratios were estimated using negative binomial regression models for exacerbation counts. |
Robustness of the regression results on exacerbation to unobserved spirometry metrics was evaluated. While only 1139 (7.6%) patients had spirometry data available, the airflow obstruction (FEV1/FVC <0.7) observed was 75.9% in the allergy group and 65.3% in the non-allergy group. After adjusting for FEV1/FVC, the hazard ratio for exacerbation remained significant (HR = 1.43; 95% CI, 1.01–2.04), and yielded a similar association with the main analysis (HR = 1.39; 95% CI, 1.18–1.65). In the tipping-point analysis, assuming a hazard ratio of 2.6 for exacerbation among patients with airflow obstruction versus those without based on prior literature,22 the proportion of obstruction in the non-allergy group would need to increase from 65.3% to approximately 83% to nullify the observed association. This exceeds the actual observed between-group difference, indicating that the findings are robust to potential bias from unobserved lung function.
Second outcome analysis using negative binomial regression demonstrated that penicillin allergy documentation was also associated with a marked elevation in exacerbation rates across all categories (Figure 4). A total of 4119 COPD exacerbation events were recorded over a median follow-up of 4.1 years (IQR, 2.5–5.6 years). Patients with recorded allergies exhibited increased rates of all exacerbations (adjusted IRR: 1.56, 95% CI: 1.25–1.93) compared to those without documented allergies. The effect was even more striking for severe exacerbations, with an approximately twofold increase in rates observed (adjusted IRR: 1.95, 95% CI: 1.31–2.92).
Subgroup Analysis
Two subgroup analyses were conducted to explore potential effect modifiers (Table 2). To address the concern that patients with a documented penicillin allergy carried a higher baseline burden of comorbidity, we stratified patients based on CCI score (excluding COPD itself) (Table 2). The increased risk associated with penicillin allergy label persisted across both risk groups and was particularly notable in patients with a CCI of 1 or greater (adjusted HR: 1.65, 95% CI: 1.29–2.12; adjusted IRR: 1.80, 95% CI: 1.30–2.48). We then used the total number of broad-spectrum antibiotic prescriptions as a proxy for the frequency of potential penicillin avoidance. COPD patients were stratified based on the median number of antibiotic prescriptions, which was 9 (IQR: 4–16). Compared with patients without allergy label, we observed that those with more frequent use of broad-spectrum antibiotics had the significant higher risk of exacerbation (adjusted HR: 1.58, 95% CI: 1.27–1.98; adjusted IRR: 1.96, 95% CI: 1.49–2.58). The association was not significant for patients with less frequent use of broad-spectrum antibiotics.
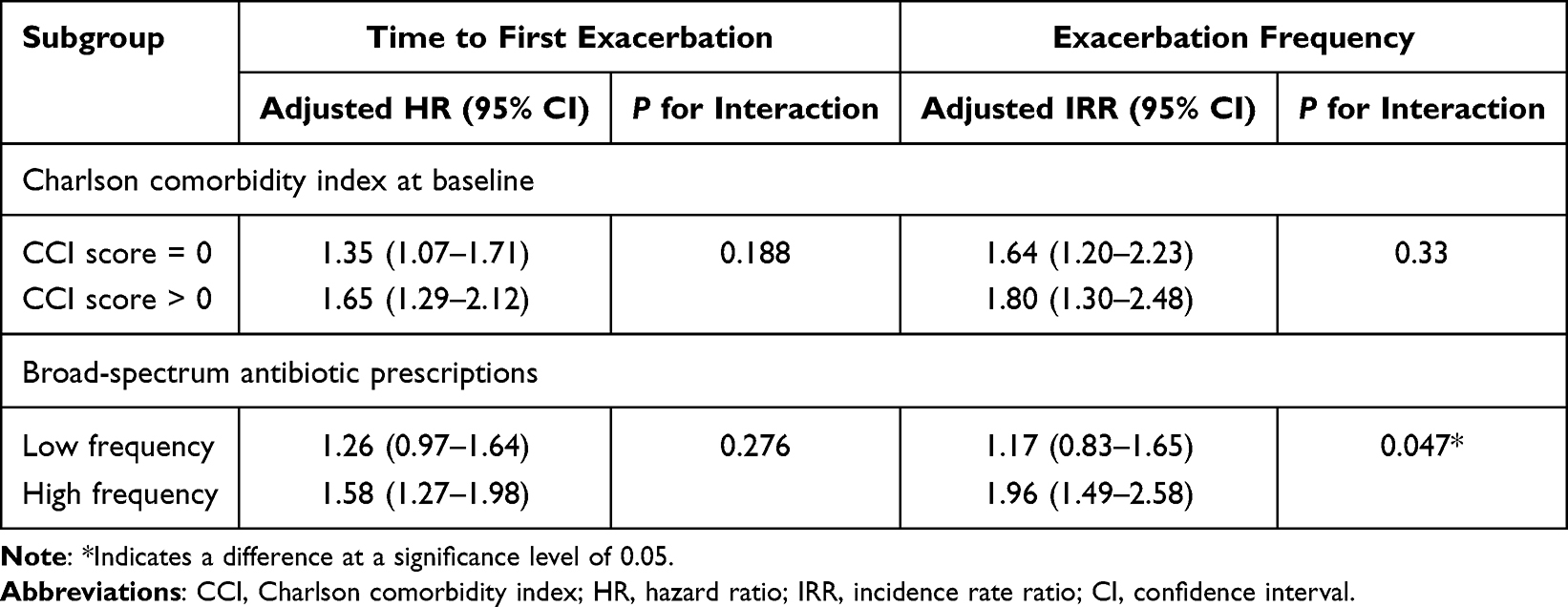 |
Table 2 Subgroup Analysis of Penicillin Allergy Label and COPD Exacerbations |
Discussion
In this population-based cohort study, documented penicillin allergy label identified a small but clinically important subgroup who received more broad-spectrum antibiotics and experienced a higher subsequent burden of exacerbations over more than four years of follow-up. These findings extend prior work on the adverse consequences of penicillin allergy labels in other populations to a chronic airway disease population characterized by frequent infection-related antibiotic exposure, and suggest that such labels function as an unrecognized, modifiable risk factor for infection-driven exacerbations.
Inappropriate use of antibiotics is a significant concern in the COPD management, contributing to the risk of antibiotic resistance and worse clinical outcomes.23,24 Here, we provide evidence demonstrated penicillin allergy label introduces an underrecognized burden on COPD antibiotic stewardship. In our cohort, 4.8% patients carried a documented penicillin allergy label, which is lower than rates reported in the Western countries,25,26 but consistent with previous studies in Chinese populations.27,28 This discrepancy likely reflects variations in penicillin skin testing (PST) policy between China and other countries, which can lead to inappropriate testing practices and reliance on restricted-use antibiotics.29 Nonetheless, even this modest prevalence, when applied to China’s estimated COPD population of over 100 million,30 translates into a substantial number of patients potentially affected by penicillin allergy label. This indicated that many patients could receive appropriate penicillin therapy if such labels were systematic assessed and removed when inaccurate.
Our study extends prior work by demonstrating the persistent and cumulative impact of penicillin allergy documentation on antibiotic prescribing patterns. Previous studies primarily focused on single episodes of acute infection, where avoidance of penicillin resulted in short-term (30 days) prescribing shifts.9,10 However, more than 80% of all documented drug allergies are never removed, allowing these labels to influence antibiotic decision across repeated clinical encounters.31 By examining antibiotic use over a two-year period before follow-up, we observed that COPD patients with documented penicillin allergy received more broad-spectrum antibiotics. Our findings, together with recent population-based study from UK, underscore the need to evaluate the long-term harms of these unnecessary alternative agents.
Importantly, we also observed that this altered prescribing pattern associated with allergy label was related to long-term exacerbation risk. After adjusting for covariates, patients with a documented penicillin allergy had a higher risk of experiencing any exacerbation and overall exacerbation rate, compared with those without such labels. Although causality cannot be established due to the observational nature of our study, mechanistic plausibility is supported by emerging evidence linking broad-spectrum antibiotic overuse to gut microbiome disruption, reduced colonization resistance, and the selection of resistant pathogens.32–34 These changes may in turn increase vulnerability to infection-triggered exacerbations and contribute to faster disease progression. This emphasizes the importance of evaluating historical penicillin allergy record and antibiotics exposure when estimating future risk of COPD exacerbations.
Previous studies have shown that frequent antibiotic use is associated with a higher risk of subsequent exacerbations.35 Patients carrying a penicillin allergy label may therefore be particularly vulnerable to repeated shifts toward broader-spectrum antibiotics during subsequent respiratory events. In our subgroup analysis, penicillin allergy documentation was associated with an increased risk of exacerbation risk among patients with baseline comorbidity and among patients with more frequent broad-spectrum antibiotic use. These findings support the hypothesis that repeated broad-spectrum antibiotic exposure partly mediates the association between allergy labels and exacerbation burden.36,37 Taken together, these results suggest that penicillin allergy label should be regarded not merely as a passive item in the medical record, but as a potentially modifiable risk factor that can shape antibiotic selection and long-term COPD outcomes.
Current COPD guidance does not support automatic escalation to broad-spectrum antibiotics solely because a penicillin allergy label is present. Antibiotic choice should instead be guided by exacerbation severity, likely pathogens, risk factors for resistant organisms, and local resistance patterns. For selected patients without features suggesting resistant or severe infection, narrower non-penicillin alternatives may be clinically reasonable, while allergy status remains unverified. Both Chinese and international COPD guidance recognize tetracycline as an option for suspected bacterial COPD exacerbations.38,39 However, such alternatives appear to be underused in routine practice. In our cohort, tetracyclines accounted for less than 5% of antibiotic use, suggesting that penicillin allergy labels may narrow clinicians perceived prescribing options and promote a shift toward broader-spectrum agents, even when a narrower alternative might be sufficient.
Another important strategy is to actively verify inaccurate allergy records and remove them when appropriate. Penicillin allergy delabeling has been shown to optimize antibiotic use and improve clinical outcomes, but large-scale implementation remains constrained by limited allergy specialist capacity.40–42 Current efforts have therefore often prioritized populations with the most immediate benefit, such as perioperative, obstetric, and immunocompromised patients.7 Our findings suggest that COPD patients represent another high-priority population for delabeling initiatives. Encouragingly, recent studies showed non-allergist clinicians can also safely and effectively perform risk-based delabeling,43 promoting scalable and cost-effective integration of delabeling programs into routine COPD care.
This study also has several limitations. First, penicillin allergy labels in EMRs may include both true allergic reactions and misclassified cases, and we lacked access to allergy testing data to distinguish between them. This limitation does not undermine the clinical relevance of the findings, because the label itself is what shapes prescribing behavior in routine care. Given that true penicillin allergy is confirmed in only a minority of labelled patients, changes in antibiotic selection are likely to be an important pathway linking allergy labels to subsequent outcomes. Second, COPD misclassification cannot be fully excluded, as diagnoses were based on ICD codes rather than systematic spirometry confirmation. However, the association remained directionally consistent among patients with available airflow-obstruction data, supporting the robustness of the main finding. Third, structured information on antibiotic indication and intended treatment duration was not consistently available, and microbiological culture or susceptibility testing data were unavailable in the linked records. Because these prescription-level factors could not be reliably timed or classified before each outcome event, we did not adjust for them directly. Instead, we focused on controlling for baseline antibiotic prescribing frequency, which partially captures prior infection burden, healthcare use and prescribing propensity. Nevertheless, residual confounding related to unmeasured antibiotic indication, treatment duration and resistance status may remain. Despite these limitations, our study suggests that penicillin allergy labels are associated with shifted prescribing patterns and increased exacerbation burden in patients with COPD.
Conclusion
In conclusion, in this large, population-based Chinese cohort of patients with COPD, penicillin allergy labels recorded in electronic medical records were associated with persistent use of broader-spectrum antibiotics and a markedly increased risk and rate of exacerbations. These results support incorporating systematic assessment and de-labelling of inaccurate penicillin allergy into antimicrobial stewardship programmes and long-term COPD management, with the goal of optimizing penicillin use and reducing infection-driven exacerbation burden.
Abbreviations
COPD, Chronic obstructive pulmonary disease; AECOPD, Acute exacerbation of chronic obstructive pulmonary disease; COVID-19, Coronavirus disease 2019; KARE, Kunshan Aging Research with E-health database; EMR, Electronic medical record; HR, Hazard ratio; IRR, Incidence rate ratio; CI, Confidence intervals; BMI, Body mass index; CCI, Charlson Comorbidity Index.
Data Sharing Statement
Interested collaborators are invited to contact the corresponding author to discuss potential partnerships and data access modalities at [[email protected]].
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the First People’s Hospital of Kunshan (Approval No. 2019-03-001-K01). All procedures involving human participants were conducted in accordance with the Declaration of Helsinki. Written informed consent for participation and linkage of electronic medical records was obtained from all participants.
Consent for Publication
All authors reviewed the final version of the manuscript and consented to submission and publication.
Acknowledgments
We would like to express our gratitude to all those who contributed to this research project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study is supported by the Major Project of Guangzhou National Laboratory (GZNL2025C01016) and the 2020 Suzhou Science and Technology Development Plan Project (SYS2020062). This study is supported by the National Natural Science Foundation of China (Grant No. 32500516), the Guangdong Provincial High-level Talent Program (Grant No. 2024QN11Y205), and the Young Scientists Program of Guangzhou Laboratory (Grant No. QNPG24-16).
Disclosure
The authors declare no competing interests in this work.
References
1. Soriano JB, Abajobir AA, Abate KH. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet Respir Med. 2017;5(9):691–12. doi:10.1016/s2213-2600(17)30293-x
2. Moghoofei M, Azimzadeh Jamalkandi S, Moein M, Salimian J, Ahmadi A. Bacterial infections in acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Infection. 2020;48(1):19–35. doi:10.1007/s15010-019-01350-1
3. Hunter MH, King DE. COPD: management of acute exacerbations and chronic stable disease. Am Fam Physician. 2001;64(4):603–612.
4. Kuijpers SME, Buis DTP, Ziesemer KA, et al. The evidence base for the optimal antibiotic treatment duration of upper and lower respiratory tract infections: an umbrella review. Lancet Infect Dis. 2025;25(1):94–113. doi:10.1016/s1473-3099(24)00456-0
5. Zhou L, Dhopeshwarkar N, Blumenthal KG, et al. Drug allergies documented in electronic health records of a large healthcare system. Allergy. 2016;71(9):1305–1313. doi:10.1111/all.12881
6. Providencia R, Aali G, Zhu F, et al. Penicillin allergy testing and delabeling for patients who are prescribed penicillin: a systematic review for a world health organization guideline. Clin Rev Allergy Immunol. 2024;66(2):223–240. doi:10.1007/s12016-024-08988-2
7. Anstey KM, Tsao L, Otani IM. Drug allergy delabeling programs: recent strategies and targeted populations. Clin Rev Allergy Immunol. 2022;62(3):484–504. doi:10.1007/s12016-021-08913-x
8. Su C, Belmont A, Liao J, Kuster JK, Trubiano JA, Kwah JH. Evaluating the PEN-FAST clinical decision-making tool to enhance penicillin allergy delabeling. JAMA Intern Med. 2023;183(8):883–885. doi:10.1001/jamainternmed.2023.1572
9. Kaminsky LW, Ghahramani A, Hussein R, Al-Shaikhly T. Penicillin allergy label is associated with worse clinical outcomes in bacterial pneumonia. J Allergy Clin Immunol Pract. 2022;10(12):3262–3269. doi:10.1016/j.jaip.2022.08.027
10. Kaminsky LW, Dalessio S, Al-Shaikhly T, Al-Sadi R. Penicillin allergy label increases risk of worse clinical outcomes in COVID-19. J Allergy Clin Immunol Pract. 2021;9(10):3629–3637.e2. doi:10.1016/j.jaip.2021.06.054
11. Vollenweider DJ, Frei A, Steurer-Stey CA, Garcia-Aymerich J, Puhan MA. Antibiotics for exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2018;10(10):Cd010257. doi:10.1002/14651858.CD010257.pub2
12. Gray MP, Kellum JA, Kirisci L, Boyce RD, Kane-Gill SL. Long-term outcomes associated with β-lactam allergies. JAMA Network Open. 2024;7(5):e2412313. doi:10.1001/jamanetworkopen.2024.12313
13. Blumenthal KG, Lu N, Zhang Y, Li Y, Walensky RP, Choi HK. Risk of meticillin resistant Staphylococcus aureus and Clostridium difficile in patients with a documented penicillin allergy: population based matched cohort study. BMJ. 2018;361:k2400. doi:10.1136/bmj.k2400
14. Narewski ER, Kim V, Marchetti N, Jacobs MR, Criner GJ. Is methicillin-resistant staphylococcus aureus colonization associated with worse outcomes in COPD hospitalizations? Chronic Obstr Pulm Dis. 2015;2(3):252–258. doi:10.15326/jcopdf.2.3.2014.0147
15. de Miguel-Díez J, López-de-Andrés A, Esteban-Vasallo MD, et al. Clostridium difficile infection in hospitalized patients with COPD in Spain (2001-2015). Eur J Intern Med. 2018;57:76–82. doi:10.1016/j.ejim.2018.06.022
16. Thabet S, Ali H, Tahir MW, et al. Incidence and impact of clostridioides difficile infection on patients admitted with COPD exacerbation. Chest. 2020;158(4):A2653. doi:10.1016/j.chest.2020.09.236
17. Xie T, Pan Y, Lu K, et al. Cohort profile: Kunshan Aging Research with E-health (KARE). Int J Epidemiol. 2025;54(3). doi:10.1093/ije/dyaf041
18. Wu P, Liu Z, Tian Z, et al. CYP2C19 loss-of-function variants associated with long-term ischemic stroke events during clopidogrel treatment in the chinese population. Clin Pharmacol Ther. 2023;114(5):1126–1133. doi:10.1002/cpt.3028
19. Chu SH, Wan ES, Cho MH, et al. An independently validated, portable algorithm for the rapid identification of COPD patients using electronic health records. Sci Rep. 2021;11(1):19959. doi:10.1038/s41598-021-98719-w
20. Pradhan R, Lu S, Yin H, et al. Novel antihyperglycaemic drugs and prevention of chronic obstructive pulmonary disease exacerbations among patients with type 2 diabetes: population based cohort study. BMJ. 2022;379(e071380):e071380. doi:10.1136/bmj-2022-071380
21. Rothnie KJ, Müllerová H, Hurst JR, et al. Validation of the RECORDING OF ACUTE EXACERBATions of COPD in UK primary care electronic healthcare records. PLoS One. 2016;11(3):e0151357. doi:10.1371/journal.pone.0151357
22. Fortis S, Comellas AP, Bhatt SP, et al. Ratio of FEV(1)/slow vital capacity of <0.7 is associated with clinical, functional, and radiologic features of obstructive lung disease in smokers with preserved lung function. Chest. 2021;160(1):94–103. doi:10.1016/j.chest.2021.01.067
23. Llor C, Bjerrum L. Antimicrobial resistance: risk associated with antibiotic overuse and initiatives to reduce the problem. Ther Adv Drug Saf. 2014;5(6):229–241. doi:10.1177/2042098614554919
24. Prins HJ, Duijkers R, van der Valk P, et al. CRP-guided antibiotic treatment in acute exacerbations of COPD in hospital admissions. Eur Respir J. 2019;53(5):1802014. doi:10.1183/13993003.02014-2018
25. Macy E, Contreras R. Health care use and serious infection prevalence associated with penicillin “allergy” in hospitalized patients: a cohort study. J Allergy Clin Immunol. 2014;133(3):790–796. doi:10.1016/j.jaci.2013.09.021
26. Van Gasse AL, Oulkadi R, Mousati Z, et al. Prevalence of self-reported and confirmed penicillin allergy in a Belgian outpatient population. Allergy. 2020;75(8):2111–2115. doi:10.1111/all.14292
27. Li PH, Siew LQC, Thomas I, et al. Beta-lactam allergy in Chinese patients and factors predicting genuine allergy. World Allergy Organ J. 2019;12(8):100048. doi:10.1016/j.waojou.2019.100048
28. Chiang V, Kan AKC, Saha C, Au EY, Li PH. Identifying the most at-risk age-group and longitudinal trends of drug allergy labeling amongst 7.3 million individuals in Hong Kong. BMC Med. 2024;22(1):30. doi:10.1186/s12916-024-03250-0
29. Shi W, Liu N, Huang JX, Xiao H, Meng J, Li PH. Penicillin allergy in china: consequences of inappropriate skin testing practices and policies. Clin Exp Allergy. 2025;55(8):625–633. doi:10.1111/cea.14546
30. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/s0140-6736(18)30841-9
31. Blumenthal KG, Acker WW, Li Y, Holtzman NS, Zhou L. Allergy entry and deletion in the electronic health record. Ann Allergy Asthma Immunol. 2017;118(3):380–381. doi:10.1016/j.anai.2016.12.020
32. Han MK, Huang YJ, Lipuma JJ, et al. Significance of the microbiome in obstructive lung disease. Thorax. 2012;67(5):456–463. doi:10.1136/thoraxjnl-2011-201183
33. Kitsios GD, Sayed K, Fitch A, et al. Longitudinal multicompartment characterization of host-microbiota interactions in patients with acute respiratory failure. Nat Commun. 2024;15(1):4708. doi:10.1038/s41467-024-48819-8
34. Patangia DV, Anthony Ryan C, Dempsey E, Paul Ross R, Stanton C. Impact of antibiotics on the human microbiome and consequences for host health. Microbiologyopen. 2022;11(1):e1260. doi:10.1002/mbo3.1260
35. Whittaker H, Nordon C, Rubino A, et al. Frequency and severity of respiratory infections prior to COPD diagnosis and risk of subsequent postdiagnosis COPD exacerbations and mortality: EXACOS-UK health care data study. Thorax. 2023;78(8):760–766. doi:10.1136/thorax-2022-219039
36. Stolbrink M, Bonnett LJ, Blakey JD. Antibiotics for COPD exacerbations: does drug or duration matter? A primary care database analysis. BMJ Open Respir Res. 2019;6(1):e000458. doi:10.1136/bmjresp-2019-000458
37. Aldeyab MA, McElnay JC, Scott MG, Darwish Elhajji FW, Kearney MP. Hospital antibiotic use and its relationship to age-adjusted comorbidity and alcohol-based hand rub consumption. Epidemiol Infect. 2014;142(2):404–408. doi:10.1017/s0950268813001052
38. Chinese Medical Association, Chinese Medical Association Publishing House, Chinese Society of General Practice, et al. Chinese guideline for management of chronic obstructive pulmonary disease in primary care (2024). Chin J Gen Pract. 2024;23(06):578–602. doi:10.3760/cma.j.cn114798-20240326-00174
39. Venkatesan P. GOLD COPD report: 2025 update. Lancet Respir Med. 2025;13(1):e7–e8. doi:10.1016/s2213-2600(24)00413-2
40. Copaescu AM, Vogrin S, James F, et al. Efficacy of a clinical decision rule to enable direct oral challenge in patients with low-risk penicillin allergy: the PALACE randomized clinical trial. JAMA Intern Med. 2023;183(9):944–952. doi:10.1001/jamainternmed.2023.2986
41. Blumenthal KG, Smith LR, Mann JTS, et al. Reaction risk to direct penicillin challenges: a systematic review and meta-analysis. JAMA Intern Med. 2024;184(11):1374–1383. doi:10.1001/jamainternmed.2024.4606
42. Krishna MT, Huissoon AP, Li M, et al. Enhancing antibiotic stewardship by tackling “spurious” penicillin allergy. Clin Exp Allergy. 2017;47(11):1362–1373. doi:10.1111/cea.13044
43. Wong JCY, Kan AKC, Chik TSH, et al. Prospective, multicenter, head-to-head comparison between allergists versus nonallergists in low-risk penicillin allergy delabeling: effectiveness, safety, and quality of life (HK-DADI2). J Allergy Clin Immunol Pract. 2024;12(7):1801–1808.e2. doi:10.1016/j.jaip.2024.04.010
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treatment Patterns, Socioeconomic Status and Clinical Burden in Mild COPD: A Swedish Real-World, Retrospective Cohort Study, the ARCTIC Study
Larsson K, Lisspers K, Ställberg B, Johansson G, Gutzwiller FS, Mezzi K, Bjerregaard BK, Jorgensen L, Koo H, Janson C
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1409-1421
Published Date: 21 June 2022
A Prediction Scoring Model for the Effect of Withdrawal or Addition of Inhaled Corticosteroids in Patients with Chronic Obstructive Pulmonary Disease
Lee JH, Kim S, Oh YM
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:113-127
Published Date: 15 February 2023
Effects of Early Pulmonary Rehabilitation on Hospitalized Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Lu HY, Chen CF, Lee DL, Tsai YJ, Lin PC
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:881-893
Published Date: 15 May 2023
Prognostic Nutritional Index (PNI) as a Potential Prognostic Tool for Exacerbation of COPD in Elderly Patients
Suzuki E, Kawata N, Shimada A, Sato H, Anazawa R, Suzuki M, Shiko Y, Yamamoto M, Ikari J, Tatsumi K, Suzuki T
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1077-1090
Published Date: 7 June 2023
Real-World Disease Burden and Healthcare Resource Utilization Among Patients with COPD and Asthma Using Triple Therapy (FF/UMEC/VI) in the United States
Igboekwe E, Verma S, Paczkowski R
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:281-296
Published Date: 25 January 2024