Back to Journals » International Journal of General Medicine » Volume 18
Patterns and Factors Associated with Dyslipidemia Among Patients with Diabetes Mellitus Attending Hoima Regional Referral Hospital, Uganda
Authors Hirsi AM, Abdi AA, Peris A, Jacinto A, Muhammad P, Nur IA, Mohamud MH, Hussein M, Qaws A, Jayte M ![]()
Received 6 September 2024
Accepted for publication 3 January 2025
Published 8 January 2025 Volume 2025:18 Pages 73—86
DOI https://doi.org/10.2147/IJGM.S494941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Abishir Mohamud Hirsi, Awil Abdukadir Abdi, Alina Peris, Amandua Jacinto, Propser Muhammad, Ibrahim Ahmed Nur, Muktar Hassan Mohamud, Mustafa Hussein, Abdi Qaws, Mohamed Jayte
Department of Internal Medicine, Faculty of Clinical Medicine and Dentistry, Kampala International University, Ishaka, Bushenyi, Uganda
Correspondence: Abishir Mohamud Hirsi, Email [email protected]
Background: Dyslipidemia in Sub-Saharan Africa has been on the disproportionate rise among diabetes patients across various contextual settings due to its patterns and associated factors. This study determined the patterns and factors associated with dyslipidemia among diabetes patients attending Hoima Regional Referral Hospital (HRRH).
Methods: This was a hospital-based cross-sectional study conducted at HRRH between October 2022 and January 2023, enrolled 375 adult diabetes patients consecutively from diabetic outpatient clinic. Data on socio-demographic, behavioral, medical history, physical examination, and laboratory diagnoses were collected and summarized using descriptive statistics. Patterns of dyslipidemia were presented as a proportion of each lipid profile either singly or in combination expressed as a percentage. In the bivariate analysis, variables with p-values < 0.2, crude odds ratios of ≥ 2 or ≤ 0.5, or those with biological plausibility were included in a multiple logistic regression model. Factors with p-values < 0.05 were considered statistically significant. All analyses were conducted using Stata version 17.
Findings: Of the 375 diabetes patients, 260 (69.3%) had abnormal total cholesterol (TC), and 185 (49.3%) had two lipid profile abnormalities. The majority of the patients were female, 235 (62.7%), and 38 (10.1%) had a diagnosis of coronary heart disease (CHD). Additionally, 134 (35.7%) were overweight, and 39 (10.4%) were obese. Female patients had higher odds of dyslipidemia (Adjusted Odds Ratio [AOR] = 2.2, 95% CI: 1.02– 4.86, p = 0.045). Those with coronary heart disease (CHD) had increased odds of dyslipidemia (AOR = 4.1, 95% CI: 1.51– 11.07, p = 0.006). All diabetes patients who were overweight or obese had dyslipidemia (p < 0.001).
Conclusion: The most common pattern of dyslipidemia in patients with diabetes was elevated total cholesterol, followed by high low-density lipoprotein, associated with overweight, obesity, female gender, and CHD. Routine screening of lipid profiles, BMI, and CHD in diabetic clinics is crucial for early intervention and improved outcomes.
Keywords: diabetes mellitus, dyslipidemia, total cholesterol, low-density lipoprotein, coronary heart disease, risk factors, Uganda
Introduction
Diabetes Mellitus is a global health problem that not only affects millions of people1 but also contributes to the cardiovascular complications.2 Diabetes mellitus (DM) is a cluster of metabolic disorders marked by chronic hyperglycemia, which arises due to deficiencies in insulin secretion, defects in insulin action, or a combination of both. This condition leads to alterations in the metabolism of carbohydrates, proteins, and fats.1 Among the metabolic complications associated with diabetes included dyslipidemia, which is a significant driver of cardiovascular complications, characterized by abnormal lipid metabolism that can result in elevated levels of low-density lipoprotein cholesterol (LDL-C), high triglycerides (TG), or reduced levels of high-density lipoprotein cholesterol (HDL-C).3 Dyslipidemia exacerbates the risk of vascular complications in diabetic patients by promoting flux of free fatty acids, a process driven by insulin resistance and further intensified by elevated inflammatory adipokine levels.2 Researchers have identified obesity and dyslipidemia as common issues among diabetes patients. A study conducted at Hi-tech Hospital and a 3-year cohort study in China found that a higher BMI and increased waist circumference were linked to dyslipidemia.4,5
Globally, diabetes accounts for 1.5 million deaths annually, making it the leading cause of mortality from non-communicable diseases (NCDs).6 The prevalence of diabetes has surged from 108 million in 1980 to 463 million,7 with low- and middle-income countries experiencing the fastest increase, placing immense pressure on healthcare systems in these regions.6
Dyslipidemia is a major concern among patients with diabetes in Sub-Saharan Africa. Research in Ethiopia reported a dyslipidemia prevalence of 59% among patients with Type 2 diabetes,8 while a study in Kenya found an even higher prevalence of 86.1% among diabetic patients.9
In Uganda, diabetes prevalence rate is notably high, with rural populations experiencing a rate of 16.1% compared to 7.6% in urban areas (Chiwanga et al, 2016). At Hoima Regional Referral Hospital (HRRH), diabetes management presents a significant challenge, with approximately 150 patients being treated in the diabetic outpatient clinic monthly (HRRH Records, 2022). Despite the high prevalence of diabetes, most patients are not routinely screened for dyslipidemia, even though evidence indicates that diabetes patients with dyslipidemia often have more atherogenic compared to non-diabetes individuals.2
Effective diabetes care is complex and extends beyond glycemic control, requiring the management of multiple risk factors, including lipid abnormalities, to prevent or delay complications.10 Evidence supports the importance of controlling both blood sugar and lipid levels to reduce the risk of cardiovascular complications.11 However, there remains a paucity of data on the patterns, and associated factors of dyslipidemia among diabetes patients in Uganda, particularly in Hoima region. This study addresses this gap by investigating the patterns, and factors associated with dyslipidemia among patients with diabetes at HRRH. Understanding these factors is crucial for necessitating the development of effective interventions that can improve the management of dyslipidemia and enhance patient outcomes.
Methodology
Study Design
This hospital-based cross-sectional study was conducted at the Diabetic Outpatient Clinic of HRRH from October 2022 to January 2023. Participants were enrolled using a consecutive sampling technique.
Study Site
The study was conducted at HRRH, the blood samples collected were analyzed in the hospital’s laboratory, which consists of four sections, hematology and blood bank, chemical and histopathology, parasitology and microbiology.
Study Population
All diabetes patients who presented at diabetic outpatient clinic at HRRH during the period of the study who are aged ≥18 years and accepted to consent for the study.
Inclusion Criteria
The study included all consented known diagnosed diabetes participants, age ≥18 years, who signed the informed consent form.
Exclusion Criteria
Diabetes patients on lipid-lowering drugs. Patients with psychiatric conditions or conditions that can deter them from participating in the study.
Sample Size Estimation
Daniel’s formula (2009) was used to determine the Sample size.

Where,
n = Minimum sample size
Zα = Z-statistic at α=1.96; 95% level of confidence
Zβ = Z-statistic at β = 0.84
P = Prevalence of characteristic being estimated
d = Margin error, set at 0.05
The sample size of prevalence of dyslipidemia in Diabetes patients was calculated using the estimated proportion based on the estimated prevalence of dyslipidemia, which 86.1% in a study done among Diabetes Patients in Turbo Sub-County.9

From the above the sample size was 375 participants.
The sample size for determining the patterns of dyslipidemia among diabetes patients was calculated using the results of a study done in a rural population in South-Western Uganda, which showed that high TC was 6.0%.12

From above, our sample size was 177 participants.
The sample size for factors associated with dyslipidemia among diabetes patients was calculated using the formula for double proportion by (Fleiss).


Where;
Z1 is Z value at 95% level of significance = 1.96,
Z2 is Z value at 80% power = 0.84,
P1 is proportion with blood transfusion among co-infected
P2 is proportion with blood transfusion among the non-co-infected
In a cross-sectional study done in Ethiopia on associated factors of dyslipidemia among diabetes by (Bekele et al, 2017):
P1 is proportion of dyslipidemia among <30 years = 21.9%
P2 is proportion of dyslipidemia among >30 years = 43.8%



Considering the calculated sample sizes for the above calculations, the biggest sample size to consider was 375.
Data Collection Procedure and Recruitment
Diabetes patients attending the diabetic outpatient clinic at HRRH were first educated and counselled about the study. They were then screened for eligibility based on pre-defined inclusion and exclusion criteria. Patients who met the criteria and agreed to participate were provided written informed consent, approved by the Kampala International University Research Ethics Committee (KIU-REC 2022–145).
The data collection process was carried out by the principal investigator, assisted by two trained nurses. A structured and pre-tested questionnaire was administered to gather comprehensive information, including socio-demographic details, medical history, lifestyle behaviours, and relevant clinical data.
Blood samples (5 mL) were drawn from participants by a certified medical laboratory technologist, using sterile techniques in compliance with standard operating procedures. The lipid profile, including total cholesterol (TC), triglycerides (TG), HDL-C, and LDL-C levels, was measured using the A25 Biosystems clinical chemistry analyzer. LDL-C levels were calculated using the Friedewald formula from the available lipid data.4
For glucose measurement, a One Touch glucose meter was used. The investigator ensured the glucometer was properly calibrated and tested a drop of blood collected from a finger prick using a sterile lancet. Measurements were taken immediately to ensure accuracy.
Measurement of Study Variables
Dependent Variable
Dyslipidemia was considered as lipid profile that consists of the following abnormalities either singly or in combination. These include TC ≥200 mg/dL (>5.3mmol/L), TG levels ≥150 mg/dL (>1.7mmol/L), HDL-C <40 mg/dL (<1mmol/L), and LDL-C ≥100 mg/dL (>3.4mmol/L).13
Independent Variables
Non Modifiable Factors
Age: Completed years from date of birth to data collection date.
Sex: Binary variable as male or female.
Behavioral Factors
Smoking: it was calculated using packs per year.
Physical exercise (WHO physical activity assessment),14
Alcohol: most of the patients were using local alcohol. Therefore, yes or no of current alcohol use were recorded.
Medical Factors
Duration of DM: Completed years from date of diagnosis with DM to data collection was considered.
Duration of diabetic therapy: Completed years from date of start of DM regimen to data collection was considered.
Type of diabetic therapy: current DM regimen at the time of data collection.
Fasting blood glucose (FBG) ≥7.0mmol/l. Fasting is defined as no caloric intake for at last eight hour.
BMI: The equation for calculating the body mass index (BMI) was as follows: Body mass index = Weight (kilogram) ÷ Height2 (meter2).
Hypertension: History of diagnosis with hypertension was recorded as binary variable; yes and no.
HIV: History of HIV as yes and no were recorded.
Drug adherence was recorded using Morisky Medication Adherence Scale (MMAS-8) which has 8 questions, each response in the scale measures a specific medication-taking behaviour. Responses were recorded as yes/no for each item with a dichotomous response and for the last item, it was a 5 -point likert scale. The Alpha reliability of the scale was 0.83.15,16
CHD: Rose Angina Questionnaire (RAQ) was administered.17
Quality Control Measures
Comprehensive quality control measures were implemented to maintain data validity and reliability, such as pre-testing equipment, daily data review, and regular calibration of devices. The inclusion and exclusion criteria were strictly followed. The same questionnaire was administered to all participants, and the research team double-checked all questionnaires daily to ensure completeness. The principal investigator approved and stored completed questionnaires securely in lockable safes, while data were entered into password-protected computers.
Data Management Measurements
Data were entered using EPI Data Version 7 and exported to STATA 17 for analysis. Exploratory analysis addressed missing values, error independence, multi-collinearity, and normality. The proportion of diabetes patients with dyslipidemia was calculated as a percentage of the total study population, with a 95% confidence interval (CI). Dyslipidemia patterns were categorized by lipid abnormalities and summarized in tables using frequencies and percentages. Logistic regression was used to identify factors associated with dyslipidemia. Variables from bivariate analysis (p < 0.2 or ORs ≥2 or ≤0.5) were included in a multivariable model, and factors were considered significant at p < 0.05 in the multivariate analysis.
Results of the Study
Socio-Demographic and Behavioral Characteristics of Participants (N = 375)
Of the 375 participants enrolled, the majority were females 68.5% (n = 257) and were aged 40–60 years, 63.2% (n = 237) with mean age of 52.9 (SD = 11.7) years. The majority had attained primary education, 52.8% (n = 198), resided in Hoima city, 54.1% (n = 203). The rest of socio-demographic and behavioral characteristics are shown in Table 1.
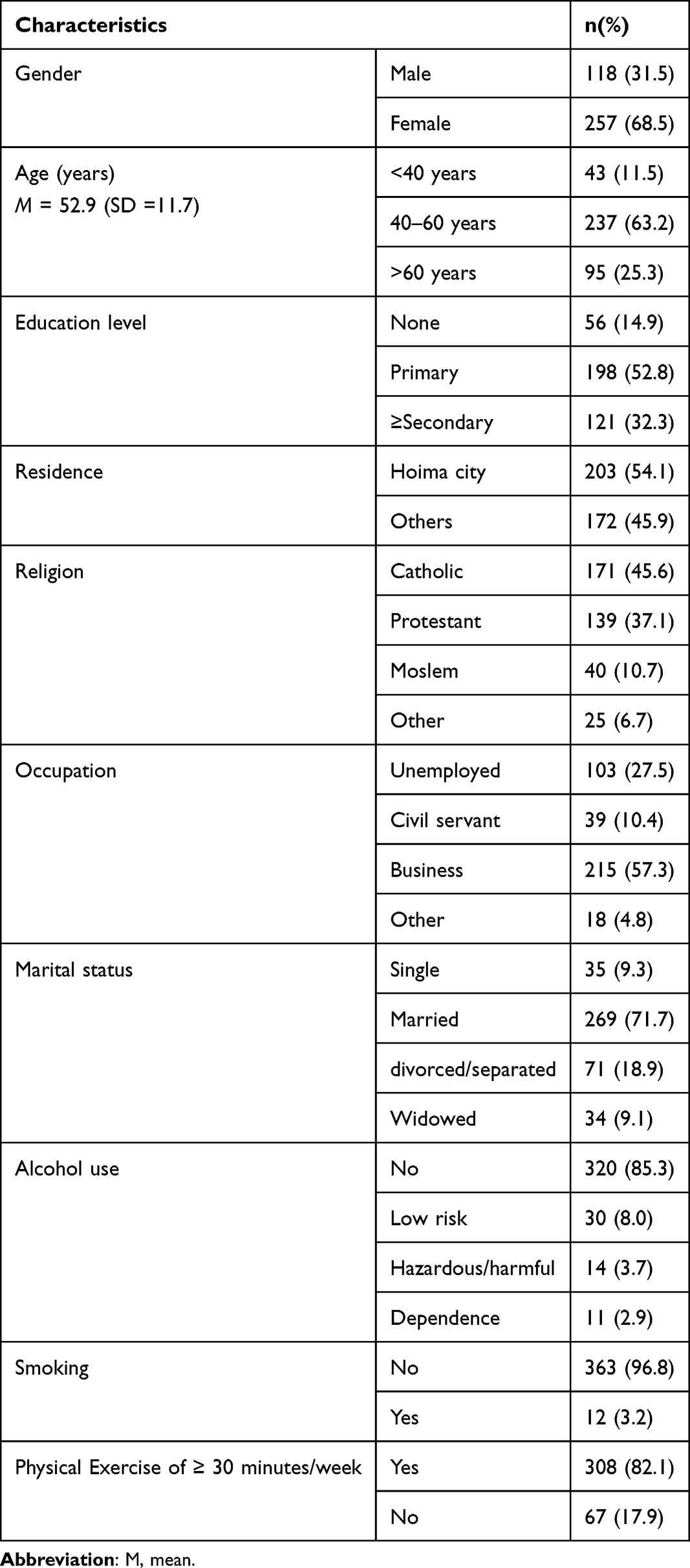 |
Table 1 Socio-Demographic and Behavioral Characteristics of Participants (N = 375) |
Medical and Clinical Characteristics of Participants (N = 375)
As shown in the table, of the 375 participants enrolled, the majority had normal BMI, 53.9% (n = 202), had history of HTN, 52.0% (n = 195), had elevated blood pressure [SBP, 87.5% (n = 328); DBP, 81.3% (n = 305)] and had low adherence to DM treatment, 77.3% (n = 290) and were on oral treatment, 75.2% (n = 282). Also, the majority were diagnosed with abnormal FBS, 92.8% (n = 348), as shown in Table 2. The remaining medical and clinical characteristics are in Table 2.
 |
Table 2 Medical and Clinical Characteristics of Participants (N = 375) |
Patterns of Dyslipidemia at Hoima Regional Referral Hospital (N = 375)
Of the 375 patients, the majority had abnormal TC, 69.3% (n = 260) and presented with two diagnoses of lipid profiles, 49.3% (n = 185). Also, more than half of the patients presented with abnormal LDL, 53.1% (n = 199) and abnormal HDL, 57.9% (n = 57.9%). The remaining patterns of dyslipidemia are shown in Table 3.
 |
Table 3 Patterns of Dyslipidemia at Hoima Regional Referral Hospital (N = 375) |
The overall prevalence of dyslipidemia among patients with DM was 86.4% (n = 324) [95% CI: 82.5–89.5%).
Bivariate Analysis Results of the Factors Associated with Dyslipidemia at HRRH (N=375)
The bivariate analysis identified several factors significantly associated with dyslipidemia, including marital status (with divorced/separated/widowed individuals having a lower risk), BMI (higher BMI being strongly associated), and the presence of coronary heart disease. Gender, age, education level, alcohol use, and hypertension showed no significant association, while marital status, BMI, and CHD had notable impacts on dyslipidemia prevalence as showing Table 4.
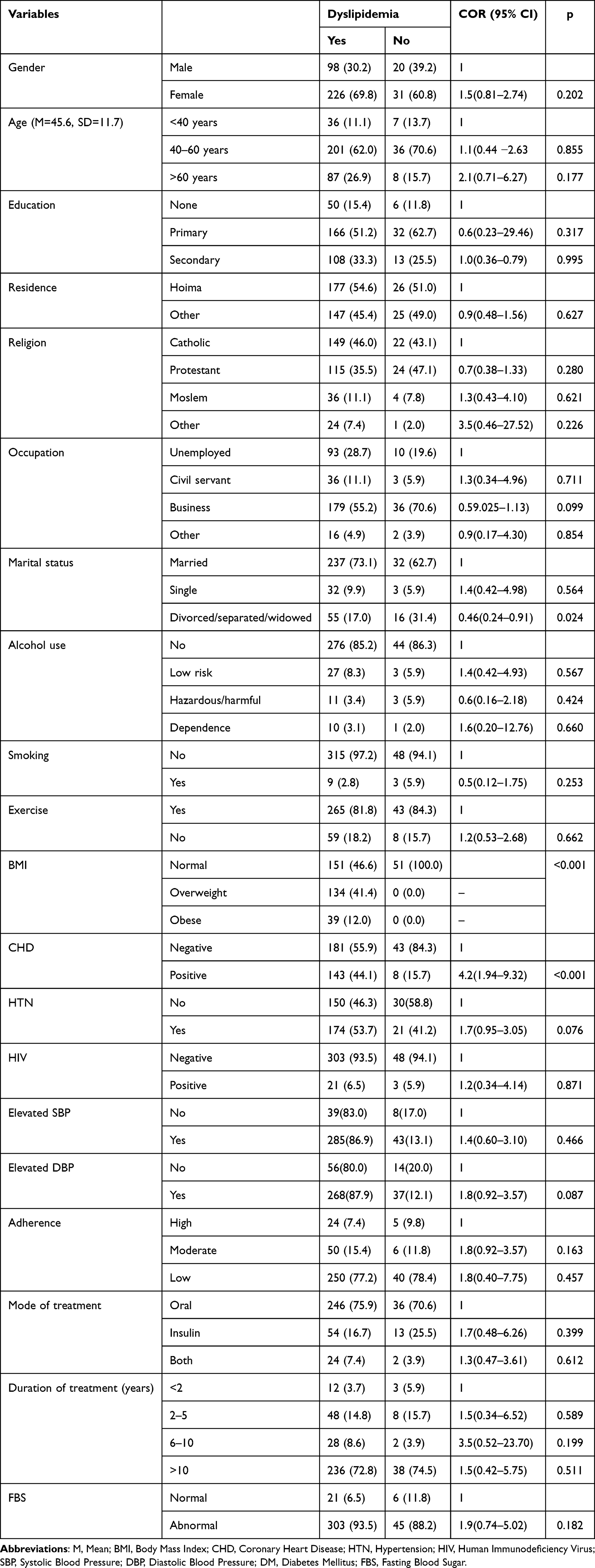 |
Table 4 Bivariate Analysis Results of the Factors Associated with Dyslipidemia at HRRH (N=375) |
Multivariate Analysis Results of the Factors Associated with Dyslipidemia (N=375)
Results in Table 5 indicate that in the multivariate model, female patients (AOR = 2.2, 95% CI: 1.02–4.86, p < 0.05) diagnosed with CHD (AOR = 4.1, 95% CI: 1.51–11.07, p < 0.01) were more likely to have dyslipidemia. The rest are in Table 5.
 |
Table 5 Multivariate Analysis Results of the Factors Associated with Dyslipidemia (N=375) |
Discussion
Patterns of Dyslipidemia Among Adult Patients with Diabetes
This hospital-based cross-sectional study at diabetic outpatient clinic of HRRH showed that the majority of the patients presented with abnormal TC and at least two diagnoses of abnormal lipid profiles. Similarly, in a study done from Yemen in Mukalla City, more than half of the patients (52.5%) had raised levels of TC.3 Also, in a study done among the Pakistani population revealed that most diabetes patients commonly suffered from combined dyslipidemia accounting for 35%.18
A study among diabetes patients who were receiving care from Durame General Hospital found out that abnormality of single lipids of raised TC, TG, LDL-C and reduced HDL-C were observed in 23.7%, 40.6%, 43.8% and 41.9%, respectively,19 which were comparably lower than in the present study except TG, which was higher than 40.3% in this study. Furthermore, in a study carried out at Hi-tech College of medicine and Hospital found 58.3% of diabetes patients had raised levels of TG.4 In addition, results from a study among 100 diabetes patients in Bangladesh showed that the study participants had raised levels of TC, raised levels LDL-C, raised TG levels but low levels of HDL-C; 28%, 50%, 44% and 60%, respectively.20 An implication is that there is a lot of disproportionalities in the patterns of dyslipidemia even in similar contextual settings.
Diabetes contributes to dyslipidemia through several mechanisms. Increased levels of glucose activate carbohydrate responsive element binding protein (ChREBP), which inhibits the expression of Apo A-I, a major component of HDL-C.21 Additionally, insulin normally stimulates Apo A-I expression, but in diabetes, insulin resistance or reduced insulin levels decrease Apo A-I production, leading to lower HDL-C levels.22 These changes lead to the typical dyslipidemia observed in patients with diabetes (increased triglycerides, decreased HDL-C, and increased LDL).22 Poor glycemic control further disrupts lipid metabolism by suppressing lipoprotein lipase activity, impairing the clearance of triglyceride-rich lipoproteins such as VLDL and chylomicrons, resulting in elevated triglyceride levels (Segundo et al, 2020).
Factors Associated with Dyslipidemia Among Adult Patients with Diabetes
The current study revealed that females were more likely to be diagnosed with dyslipidemia compared to their counterpart males. The finding of this study is in congruence with the results of a study conducted from North Eastern Ethiopia that found that being female was 2.6 times more likely to have dyslipidemia.8 Similarly, a study done in Saudi Arabia found that females who had diabetes had significantly higher level of cholesterol than their male counterparts.23 The result of this study is also in agreement with the result of a study that showed sex was an independent statistical association with dyslipidemia with females being more at risk of having the condition (Segundo et al, 2020). In contrast to the present study, study done in Pakistani population found that the prevalence of dyslipidemia was more in male patients than female patients which was 97.2% and 87.2%, respectively.18 A cross-sectional study among randomly selected patients from the diabetic registry at AL Noor Charity Center in Yemen found no association across sex of and occurrence of dyslipidemia.3 These findings imply gender variations in the prevalence of dyslipidemia among patients with diabetes mellitus. The association between dyslipidemia and female gender remains controversial, with studies yielding different results. However, it is hypothesized that estrogen influences body fat distribution, which may alter lipoprotein profiles and contribute to a higher atherogenic risk in females compared to males.24
This study found that overweight or obese patients with diabetes mellitus were significantly associated with dyslipidemia. Similarly, this finding corresponds to findings in cross-sectional study conducted from Bangladesh where obesity were statistically associated with dyslipidemia.1 Also, a cross-sectional study, which was institution-based in Ethiopia showed that being overweight was significantly associated with dyslipidemia and obesity had statistically significant association with dyslipidemia.8
In obesity, dyslipidemia results from increased free fatty acid flux to the liver, which leads to raised triglyceride synthesis and higher production of very low-density lipoproteins (VLDL).1 Also, lipolysis of triglyceride-rich lipoproteins is impaired due to reduced activity of lipoprotein lipase (LPL) which further exacerbates hypertriglyceridemia.25 This process also contributes to decreased levels of high-density lipoprotein cholesterol (HDL-C) and the formation of atherogenic low-density lipoprotein (LDL), increasing cardiovascular risk.26
This present study found that patients with CHD were 8 time more likely to have dyslipidemia compared to patients who were not having dyslipidemia. This finding is comparable to a study, which was done among patients suffering from diabetes in Cantabria at bivariate analysis but not at multivariate analysis.27 Findings imply that even with varying prevalence of overweight or obesity, they remain predictors of dyslipidemia among patients with diabetes mellitus irrespective of other factors. Hyperlipidemia is linked to CHD even before atherosclerosis occurs,28 studies show that dyslipidemia triggers oxidative stress and inflammatory cardiac fibrosis, reduces autophagy and microvascular density, and causes disruption of the mitochondrial function of cardiomyocytes, leading to myocardial damage and electrophysiological changes.28
Conclusions
Adult patients with diabetes at diabetic outpatient clinic of HRRH mostly present with abnormal TC and presented with two diagnoses of abnormal lipid profiles.
Being overweight or obese, female, and diagnosed with CHD were predictive of higher likelihood of dyslipidemia among adults with diabetes attending diabetic OPD clinic at HRRH.
Declaration of Helsinki
The study complies with the Helsinki declaration.
Availability of Supporting Data
Data can be obtained upon request from the corresponding author (Abishir Mohamud Hirsi, Email: [email protected]).
Ethical Approval and Consent to Participate
Ethics approval and consent to participate of the study was approved by Kampala International University – Research ethics committee (Ref no: KIU-2022-145).
Acknowledgment
Authors thank all the participants of the study.
Funding
This research was not funded by any specific grant from public or non-profit organizations.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Ahmmed S, Das SS, Paul DK, et al. Prevalence of dyslipidemia and associated risk factors among newly diagnosed Type-2 diabetes mellitus (T2DM) patients in Kushtia, Bangladesh.PLOS Glob Public Heal. 2021;1(12):1–13. doi:10.1371/journal.pgph.0000003
2. Narindrarangkura P, Bosl W, Rangsin R, Hatthachote P. Prevalence of dyslipidemia associated with complications in diabetic patients: a nationwide study in Thailand. Lipids Health Dis. 2019;18(1):1–8. doi:10.1186/s12944-019-1034-3
3. Salim A, Ghouth B, Ba-karman AA. Prevalence and patterns of dyslipidemia among type 2 diabetes mellitus patients in Mukalla City, Yemen, in 2017. J Community Med Public Heal Care. 2019;6(48):1–7. doi:10.24966/CMPH-1978/100048
4. Mukherjee B, Mohanty M. Diabetes mellitus and dyslipidemia- a detailed analysis. Asian J Med Sci. 2021;12(5):101–106. doi:10.3126/ajms.v12i5.33763
5. Liu L, Guan X, Yuan Z, et al. Different contributions of dyslipidemia and obesity to the natural history of type 2 diabetes: 3-year cohort study in China. J Diabetes Res. 2019;2019:1–11. doi:10.1155/2019/4328975
6. Robbiati C, Putoto G, Da Conceição N, et al. Diabetes and pre-diabetes among adults reaching health centers in Luanda, Angola: prevalence and associated factors. Sci Rep. 2020;10(1):1–8. doi:10.1038/s41598-020-61419-y
7. Ampofo AG, Boateng EB. Beyond 2020: modelling obesity and diabetes prevalence. Diabet Res Clin Pract. 2020;167:108362. doi:10.1016/j.diabres.2020.108362
8. Kebede WM, Gizachew KD, Mulu GB. Prevalence and risk factors of dyslipidemia among type 2 diabetes patients at a referral hospital, North Eastern Ethiopia. Ethiop J Heal Sci. 2020;31(6):1267–1277. doi:10.4314/ejhs.v31i6.23
9. Kiplagat SV, Lydia K, Jemimah K, Drusilla M. Prevalence of dyslipidemia and the associated factors among type 2 diabetes patients in Turbo Sub-County Kenya. J Endocrinol Diabetes. 2017;4(5):1–9. doi:10.15226/2374-6890/4/5/00190
10. WHO 2016. GLOBAL REPORT ON DIABETES. 2016:6.
11. Nisar MU, Asad A, Waqas A, et al. Association of diabetic neuropathy with duration of type 2 diabetes and glycemic control. Cureus. 2015;7(8). doi:10.7759/cureus.302
12. Asiki G, Murphy GAV, Baisley K, et al. Prevalence of dyslipidaemia and associated risk factors in a rural population in South-Western Uganda: a community based survey. PLoS One. 2015;10(5):e0126166. doi:10.1371/journal.pone.0126166
13. Rai S, Bhatnagar S. Novel lipidomic biomarkers in hyperlipidemia and cardiovascular diseases: an integrative biology analysis. Omi a J Integr Biol. 2017;21(3):132–142. doi:10.1089/omi.2016.0178
14. Ding M, Zhou Y, Li C, Li W, Jia N, Dong X. Can the WHO ‘s recommendations of physical activity volume decrease the risk of heart disease in middle and older aged Chinese People: the evidence from a seven year longitudinal survey. BMC Geriatr. 2022;22(1):1–10. doi:10.1186/s12877-022-03276-0
15. Arulmozhi S, Mahalakshmy T. Self care and medication adherence among type 2 diabetics in Puducherry, Southern India: a hospital based study. J Clin Diagn Res. 2014;8(4):9–11. doi:10.7860/JCDR/2014/7732.4256
16. Plakas S, Mastrogiannis D, Mantzorou M, et al. Validation of the 8-item morisky medication adherence scale in chronically III ambulatory patients in rural Greece. Open J Nurs. 2016;06(03):158–169. doi:10.4236/ojn.2016.63017
17. Rahman MA, Spurrier N, Mahmood MA, Rahman M, Choudhury SR, Leeder S. Rose angina questionnaire: validation with cardiologists’ diagnoses to detect coronary heart disease in Bangladesh. Indian Heart J. 2013;65(1):30–39. doi:10.1016/j.ihj.2012.09.008
18. Sarfraz M, Sajid S, Ashraf MA. Prevalence and pattern of dyslipidemia in hyperglycemic patients and its associated factors among Pakistani population. Saudi J Biol Sci. 2016;23(6):761–766. doi:10.1016/j.sjbs.2016.03.001
19. Bekele S, Yohannes T, Mohammed EA. Dyslipidemia and associated factors among diabetic patients attending durame general hospital in southern nations, nationalities, and people’s region. Diabetes Metab Syndr Obes. 2017;10:265–271. doi:10.2147/DMSO.S135064
20. Goel S, Garg PK, Malhotra V, Madan J, Mitra S, Grover S. Dyslipidemia in Type II diabetes mellitus-an assessment of the main lipoprotein abnormalities. Bangladesh J Med Sci. 2016;15(1):99–102. doi:10.3329/bjms.v15i1.21170
21. Gaudet D, Brisson D, Tremblay K, et al. Targeting APOC3 in the familial chylomicronemia syndrome. N Engl J Med. 2014;371(23):2200–2206. doi:10.1056/NEJMoa1400284
22. Kingwell BA, Chapman MJ, Kontush A, Miller NE. HDL-targeted therapies: progress, failures and future. Nat Rev Drug Discov. 2014;13(6):445–464. doi:10.1038/nrd4279
23. Alomaish MA, Alghanem ZA, Alsaqar AH, Alatiyyah AT. Prevalence of dyslipidemia in patients with type 2 diabetes mellitus: a cross-sectional study. Cureus. 2021;13(12):6–12. doi:10.7759/cureus.20222
24. Abdissa D, Hirpa D. Dyslipidemia and its associated factors among adult diabetes outpatients in West Shewa zone public hospitals, Ethiopia. BMC Cardiovasc Disord. 2022;22(1):1–8. doi:10.1186/s12872-022-02489-w
25. Klop B, Elte JWF, Cabezas MC. Dyslipidemia in Obesity: mechanisms and Potential Targets. Nutrients. 2013;5(4):1218–1240. doi:10.3390/nu5041218
26. Addisu B, Bekele S, Wube TB, Hirigo AT, Cheneke W. Dyslipidemia and its associated factors among adult cardiac patients at Ambo university referral hospital, Oromia region, west Ethiopia. BMC Cardiovasc Disord. 2023;23(1):1–12. doi:10.1186/s12872-023-03348-y
27. Segundo A, Vera D, Abellán J, et al. Endocrinología, Diabetes y Nutrición The prevalence and risk factors associated with dyslipidemia in type 2 diabetic patients in the autonomous Region of Cantabria ଝ. Endocrinol Diabetes y Nutr. 2020;67(2):102–112. doi:10.1016/j.endien.2019.04.006
28. Yao YS, Di LT, Zeng ZH. Mechanisms underlying direct actions of hyperlipidemia on myocardium: an updated review. Lipids Health Dis. 2020;19(1):1–6. doi:10.1186/s12944-019-1171-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Pattern of Dyslipidemia and Its Associated Factors Among Patients with Type 2 Diabetes Mellitus in Jordan: A Cross-Sectional Study
Al Quran TM, Bataineh ZA, Al-Mistarehi AH, Zein Alaabdin AM, Allan H, Al Qura'an A, Weshah SM, Alanazi AA, Khader YS
International Journal of General Medicine 2022, 15:7669-7683
Published Date: 4 October 2022
Prevalence of Hypercholesterolemia and Awareness of Risk Factors, Prevention and Management Among Adults Visiting Referral Hospital in Ethiopia
Belete AK, Kassaw AT, Yirsaw BG, Taye BA, Ambaw SN, Mekonnen BA, Sendekie AK
Vascular Health and Risk Management 2023, 19:181-191
Published Date: 30 March 2023
Evaluation of Vitamin B12 Deficiency Among Patients with Type 2 Diabetes Mellitus on Metformin at Hoima Regional Referral Hospital, Uganda
Ali HO, Agwu E, Ali MA, Jama YM, Ahmed AH, Yusuf MAM, Araye AA, Osobow IM, Sandeyl AA, Ahmed ZA, Onyanga N, Nor FI, Mohamed AH, Karshe AH, Hirsi AM, Mohamed AA, Jayte M
Diabetes, Metabolic Syndrome and Obesity 2026, 19:562440
Published Date: 21 January 2026
Clinical Manifestations and Risk Factors of Osteoporosis in Patients with Type 2 Diabetes Mellitus
Wang Y, Du Y, Zuo J, He L, Shi Y, Yuan Y, Liu Y, Zheng H, Wang H
Journal of Inflammation Research 2026, 19:575474
Published Date: 17 March 2026
Clinical Features and Risk Factors of Dermatitis Cruris Pustulosa et Atrophicans in Southwestern Uganda: A Cross-Sectional Study
Mulyowa GK, Engwau T, Galiwango M, Kamuganga F, Mirembe SK, Aloyo GO, Mwavu R, Wasswa W, Kaggwa F, Obua C
Clinical, Cosmetic and Investigational Dermatology 2026, 19:603936
Published Date: 9 June 2026