Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Clinical Features and Risk Factors of Dermatitis Cruris Pustulosa et Atrophicans in Southwestern Uganda: A Cross-Sectional Study
Authors Mulyowa GK ![]() , Engwau T
, Engwau T ![]() , Galiwango M
, Galiwango M ![]() , Kamuganga F, Mirembe SK, Aloyo GO
, Kamuganga F, Mirembe SK, Aloyo GO ![]() , Mwavu R, Wasswa W, Kaggwa F, Obua C
, Mwavu R, Wasswa W, Kaggwa F, Obua C ![]()
Received 17 February 2026
Accepted for publication 23 May 2026
Published 9 June 2026 Volume 2026:19 603936
DOI https://doi.org/10.2147/CCID.S603936
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monica K. Li
Grace Kitunzi Mulyowa,1 Tonny Engwau,2 Martin Galiwango,3 Francis Kamuganga,4 Stephen Kizito Mirembe,1 Gladys Onguti Aloyo,1 Rogers Mwavu,5 William Wasswa,6 Fred Kaggwa,4 Celestino Obua7
1Department of Dermatology, Mbarara University of Science and Technology, Mbarara, Uganda; 2Department of Software and Informatics Engineering, Mbarara University of Science and Technology, Mbarara, Uganda; 3Department of Electrical and Electronics Engineering, Mbarara University of Science and Technology, Mbarara, Uganda; 4Department of Computer Science, Mbarara University of Science and Technology, Mbarara, Uganda; 5Department of Information Technology, Mbarara University of Science and Technology, Mbarara, Uganda; 6Department of Biomedical Sciences and Engineering, Mbarara University of Science and Technology, Mbarara, Uganda; 7Department of Central Administration, Mbarara University of Science and Technology, Mbarara, Uganda
Correspondence: Grace Kitunzi Mulyowa, Department of dermatology, Mbarara University of Science and Technology, Mbarara, Uganda, Tel +256 785 345566, Email [email protected]
Background: Dermatitis cruris pustulosa et atrophicans (DCPA), a chronic skin inflammatory condition involving the shins, is a marginally recognized disorder in Uganda.
Purpose: To describe the clinical manifestation of DCPA and risk factors among populations in southwestern Uganda.
Patients and Methods: The study was conducted in Mbarara and Kabale Regional Referral Hospital Skin Clinics. Demographic data and digital images of affected shins were taken and stored on remote server. In a descriptive cross-sectional study, data was collected from 405 participants from 02/November/2022 to 04/January/2024 and was analyzed using R, a data visualization and statistical computing programming language.
Results: Most patients (74.9%) were aged 0– 25 years, with a mean age of 21.6 years (SD = 15.1). Females constituted 71.9% of cases. Patients were almost evenly distributed between Mbarara (46.2%) and Kabale (53.8%) Hospitals. The largest affected groups were students (38%) and pupils/infants (25.4%) followed by Farmers (16%) and semiskilled laborers (8.9%). Petroleum jelly was the most topical application (28.6%) while herbal remedies (11.9%), Systemic antibiotics (8.9%) and topical antifungal treatments (5.2%) were less frequently used.
Conclusion: DCPA presents with itching, pus discharge, and atrophic skin changes. In southwestern Uganda, it mainly affects young females. In its multifactorial etiopathogenesis oily cosmetic products is a contributory factor.
These findings, supported by Mbarara University Data Science Research Hub (MUDSReH), highlight the need for improved diagnostic tools and targeted interventions for DCPA. Further research is needed to assess the broader impact of DCPA in Uganda.
Keywords: dermatitis cruris pustulosa et trophicans, clinical manifestations, risk factors, petroleum jelly, Uganda
Introduction
DCPA is a chronic, inflammatory skin condition that affects the shins with recurrent itchy follicular pustular skin eruptions. These may resolve spontaneously or after treatment with various antibiotics. However, due to the chronic nature that the condition presents, it may last for over 20 years.1 The healing tends to leave the skin atrophied coupled with hair loss over the affected areas. The condition has been reported in tropical regions of Africa and also in Asia where it has been observed to affect people who use oily topical skin applications for various purposes.1,2
In sub-Saharan Africa, including Uganda, the burden of skin diseases is significant, yet conditions like DCPA are often underdiagnosed and misdiagnosed due to a lack of awareness, diagnostic resources, and research focus. The prevalence of DCPA in East Africa more so in Uganda has not yet been established. However, prevalence from West Africa and South India ranges from 0.4 to 4.8%.1 These are regions with some similarity with use of oily topical skin applications for various reasons. In West Africa DCPA affects the males more and it is more prevalent in the second to third decade of life.3 There are no published data on DCPA in southwestern Uganda let alone studies investigating the associated risk factors in East Africa.
One factor to consider about DCPA is its unclear etiopathogenesis. Previous studies have indicated it to be an entity of multifactorial etiological origin. It has been associated with chronic bacterial infection working together with environmental factors like heat, humidity and dusty conditions. The use of oily topical skin applications and occlusive dressing have also been observed to predispose individuals to DCPA while repeated chemical and physical trauma may also play a part.4
In the socioeconomic sector, DCPA has been noted to reduce productivity, while at the same time increasing the financial expenses used on the treatment of a chronic condition. The condition sometimes leads to failure to attend schools, and even when some of the students attend, the stigma attached to it is depressing. The need to put on school uniforms that reveal the legs exposes the scars or pus and this is demoralizing.
It is worth noting that most patients with skin disorders are treated by clinicians that are not trained in dermatology.5,6 The clinical presentation of DCPA, which may include pustules, atrophy, scarring, alopecia crusts xerosis and hyperpigmentation, often overlaps with other dermatological conditions, making diagnosis challenging without proper dermatologic expertise.7 With this lack of easy access to dermatologic services in Uganda, the management of DCPA may be improved by the use of Artificial Intelligence (AI), a technological application that allows machines to simulate human intelligence. Such tools can empower the non-dermatology-trained clinicians in the diagnosis of the disease. The use of AI is an evolving field in Uganda that still needs a lot of support.8 Understanding the risk factors of DCPA in southwestern Uganda is critical for developing targeted public health interventions and improving clinical management. Therefore, this study aimed at addressing the existing knowledge gap by investigating the risk factors of DCPA in this region. The same data can also be used to develop AI algorithms for machine learning aimed at better management of the condition.
Materials and Methods
This was a descriptive cross-sectional study conducted in the skin clinics of Mbarara Regional Referral Hospital (MRRH) and Kabale Regional Referral Hospital (KRRH) in southwestern Uganda. It was conducted from 02/November/2022 to 04/January/2024. MRRH is a tertiary referral hospital serving a population of approximately 2.5 million people in the Mbarara region, while KRRH serves a similar population of around 2.8 million in the Kabale region. Both hospitals provide a range of specialized medical services, including dermatology clinics that serve as primary points of care for skin conditions in their respective catchment areas. A consecutive non-probability sampling method was used in the recruitment of the participants as they presented in the clinics. This was due to the fact that DCPA is a chronic condition that patients tend to tolerate for long periods without presenting to specialized clinics. People tend to do self-medication for various reasons like the cost of the medications needed, the distances they have to travel to reach referral hospitals and even the lack of knowledge that such specialized clinics do exist. It is not unusual for patients to present with other complaints only for the clinician to also notice the pre-existing DCPA. Hence there was a need to visit some of the surrounding schools since from the clinical experience most of the patients were in the young age group. Both single and mixed gender primary and secondary schools were visited. All ethical requirements were met and participants were examined in adequate privacy. Both rural and urban schools were chosen depending on ease of accessibility in terms of physical road infrastructure and school administration. The school populations visited ranged from 600 to 1000 students/pupils. In the Kabale region 10 schools were visited while in Mbarara region 6 were visited.
The final diagnosis of DCPA was clinically made using a through history of the presenting complaint and together with the physical clinical findings. The documented history sought the following: Itching of the skin on the legs, how long the condition had existed, what type of cosmetic products one was using, types of medications used whether topical or systemic, if there was improvement or not, any other family members with a similar condition.
Physical examination was aimed at specifically identifying the following features: shiny skin, pustules, papules, skin atrophy, scarring, alopecia, crusts, hyperpigmentation, xerosis, varicose veins and scaling.
The use of petroleum jelly or other oily topical applications associated with at least 3 of the above physical features including especially pustules and skin atrophy led to DCPA diagnosis. The diagnosis was made solely on clinical manifestation, and there was one dermatologist attached to a team of registrars from the department of dermatology. Consensus was reached among 3 dermatologists after examining the images captured on the cases that were not recruited from within the referral hospitals.
Study Population and Selection Criteria
All patients who came to the skin clinics at MRRH and KRRH including those identified from a survey of nearby surrounding primary and secondary schools were used for participants’ recruitment because people with DCPA may not to go to the hospitals for treatment and yet school going children tend to be in the age group which is more affected by DCPA. These children who had suspicious lesions were referred to MRRH and KRRH, while those who could not afford had their images taken in privacy.
Patients with suspicious symptoms and signs of DCPA such as itchy shin skin eruption, pus collection on the legs, skin atrophy, scaling, and occasional crust formation were consecutively recruited.
Data Collection
Data was collected from all the 405 participants who presented with clinical symptoms and signs of DCPA. Open Data Kit (ODK) forms on Samsung A73 smartphone with 108 MP camera was used to collect the data. The form was validated against data constraints and values. Research assistants were trained on its application. The variables included documentation of the history referring to: Demographics (Name, age, gender, physical address, occupation), presenting complaint, duration of condition (Months), what topical applications were used and whether there was improvement or not.
Physical Examination
Identified which leg was affected (Left/Right, both), the affected orientation view (anterior, posterior, lateral, medial), skin texture: shiny atrophic skin, pustules, papules, scarring, xerosis, crusts, scaling and hyperpigmentation. Eight images were taken and stored on the university server directly.
Data Analysis
Data were entered and cleaned using Microsoft Excel, then exported to R (version 4.5.0) for analysis. Descriptive statistics were used to summarize demographic and clinical characteristics, including means, standard deviations, frequencies, and percentages. Associations between categorical variables (such as sex, age group, occupation, and use of topical applications) and DCPA diagnosis were assessed using chi-square tests.
Ethical Considerations
This study complies with the Helsinki declaration. Permission was obtained from the relevant research regulatory authorities in Uganda. The Institutional Review Board (IRB) of Mbarara University of Science and Technology Research Ethics Committee (IRB-MUST-2022-623) and the Uganda National Council of Science and Technology (UNCST-SIR186ES).
Informed consent and/or assent was obtained from all participants. A parent or legal guardian provided informed consent for participants under 18 years of age.
Results
Demographics
Four hundred and five participants were recruited in the study. They presented with symptoms and signs suggestive of DCPA in the two regional referral hospitals and surrounding schools in southwestern Uganda. Patients diagnosed with DCPA (n=220, 54.3%) were significantly younger (mean age 18.1 years, SD=12.8) compared to those with non-DCPA conditions (mean age 25.7 years, SD=16.3), with a predominance in the 0–25 age range. The condition disproportionately affected females (80.9% in DCPA vs 61.1% in non-DCPA), and students constituted nearly half of DCPA cases (49.1%). Geographic distribution showed similar representation from rural and urban locales, though occupational patterns revealed distinct epidemiological profiles between diagnostic groups. These baseline differences underscore the importance of age- and occupation-specific screening protocols in endemic regions as shown in Table 1.
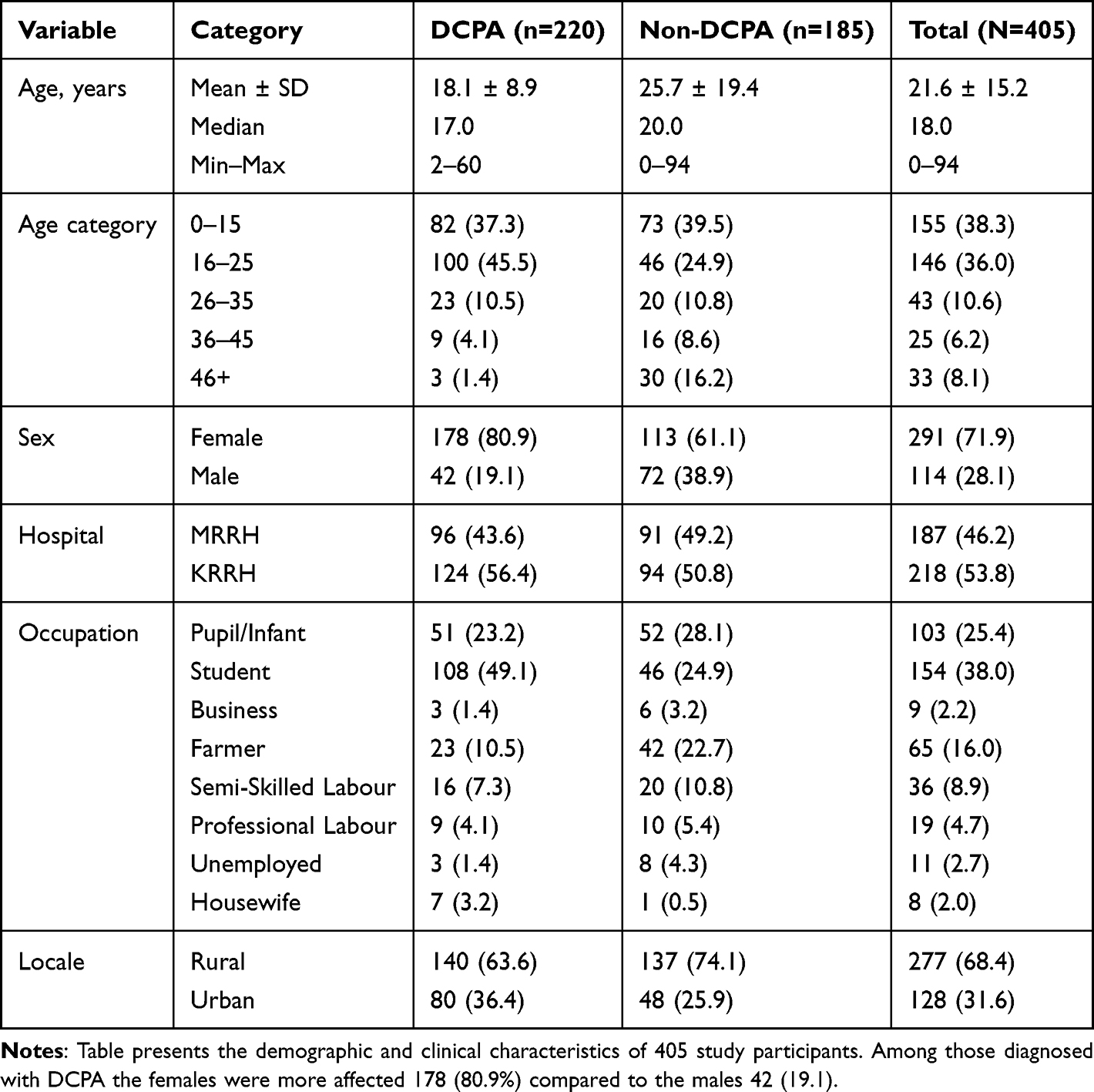 |
Table 1 Baseline Characteristics of Study Participants Stratified by Diagnosis |
Clinical Manifestation
The predominant presenting complaint in DCPA was “itchy legs with pus discharge” (62.3%), contrasting sharply with non-DCPA cases where simple “itchy legs” was more common (47.6%). DCPA patients experienced significantly longer symptom duration (mean 45.0 ± 48.0 months vs 31.2 ± 49.4 months), with 18.2% reporting symptoms persisting beyond 78 months. Despite prolonged illness, treatment-seeking patterns were similar across groups, with petroleum jelly/lotion being the most common topical application (73.2% DCPA vs 71.4% non-DCPA). However, DCPA patients were more likely to have used topical herbal remedies (15.5% vs 7.6%) and combined formulations (12.7% vs 5.4%). On the treatment outcome only 15.5% of DCPA patients reported improvement with prior treatments compared to 14.6% in non-DCPA, while 60.0% of DCPA cases explicitly reported no improvement as seen in Table 2.
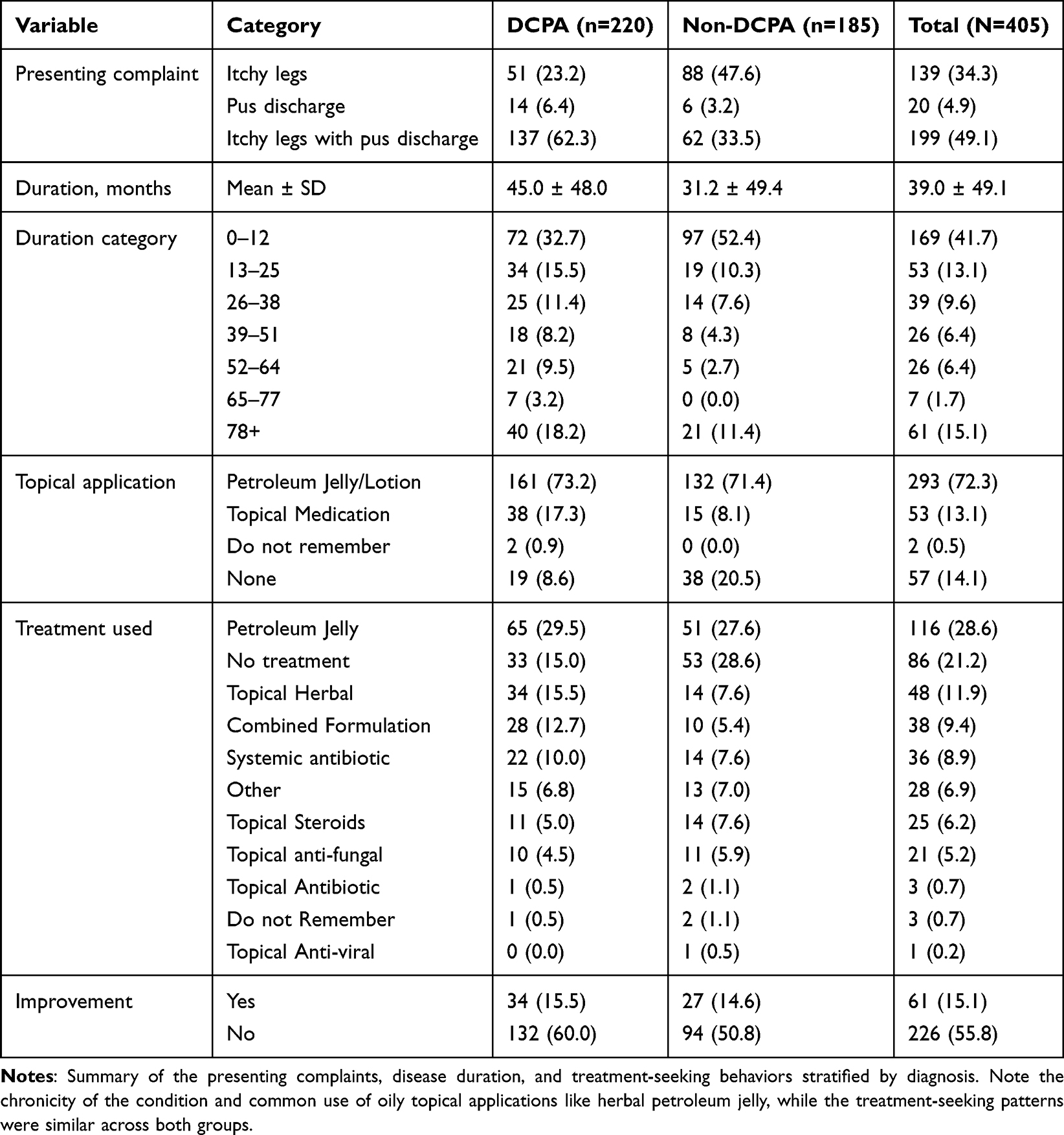 |
Table 2 Clinical History and Treatment Patterns by Diagnosis |
Physical Examination Findings
A significant number of patients with DCPA 102 (46.4) had seven lesions on physical examination. This was more than double the rate in non-DCPA (21.1%). Conversely, non-DCPA patients were three times more likely to exhibit fewer than three lesion types (34.6% vs 11.8%). The majority of both groups showed extensive anatomical distribution across four leg surface orientation views (71.4% DCPA vs 62.2% non-DCPA). The lesions were assessed on the anterior, posterior, lateral and medial aspects of the legs. DCPA lesions were characteristically well-demarcated (88.2% vs 74.1%). Atrophic skin changes a clinical hallmark of chronic tissue damage due to inflammation and healing were present in 82.7% of DCPA cases compared to 62.7% in non-DCPA as seen in Table 3.
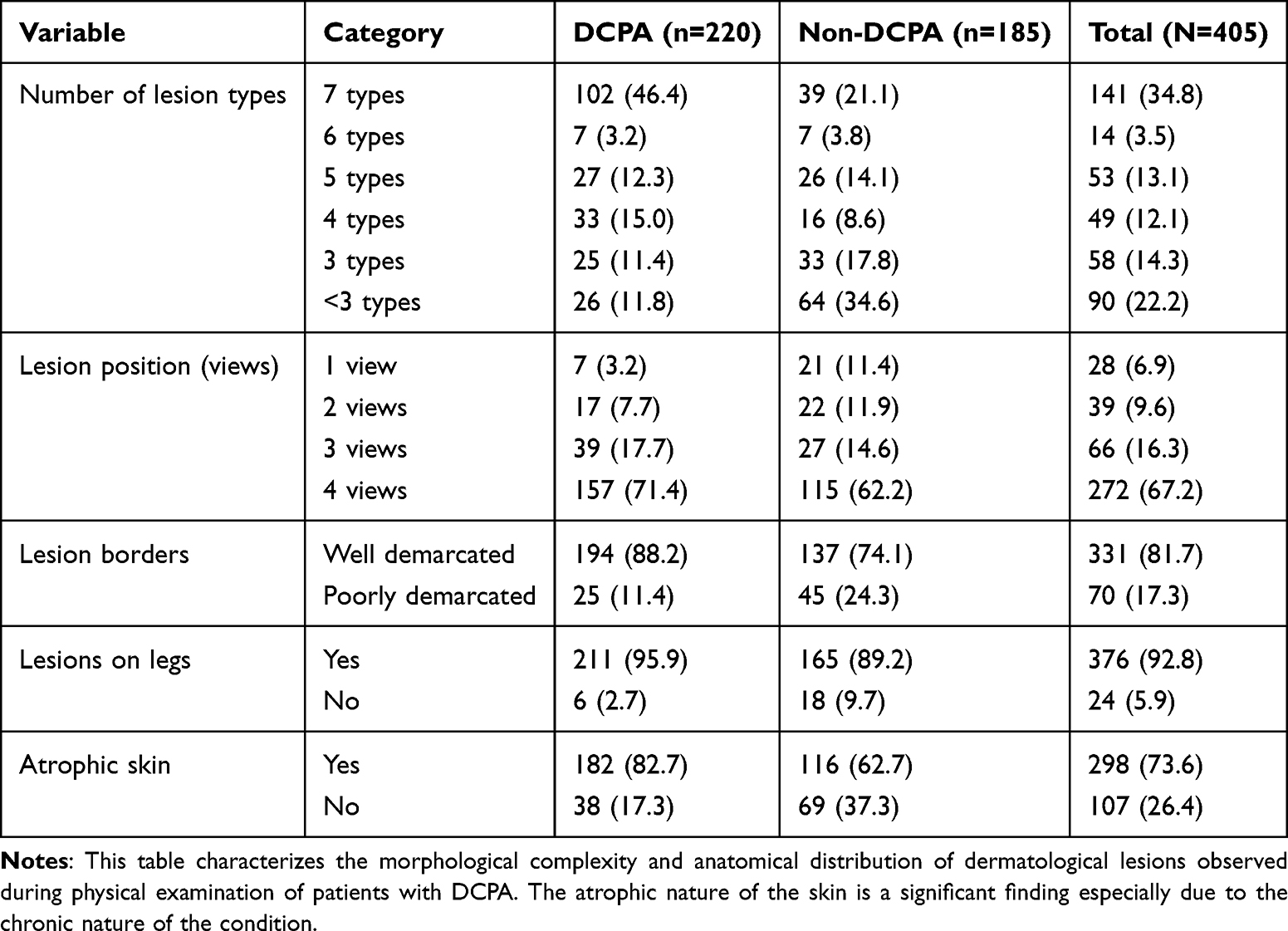 |
Table 3 Physical Examination Findings and Lesion Characteristics by Diagnosis |
As stated above, various patients had varying dermatologic primary and secondary lesions on the legs. DCPA patients exhibited a significantly higher prevalence of most lesion types compared to non-DCPA cases. The most distinctive features included papules (83.2% vs 47.6%, p<0.001), scars (83.6% vs 70.8%, p=0.003), pustules (80.0% vs 51.4%, p<0.001), and scales (77.3% vs 51.4%, p<0.001). Atrophic skin changes were present in 82.7% of DCPA cases compared to 62.7% in non-DCPA (p<0.001), representing the most significant clinical discriminator. Xerotic patterns also showed strong association with DCPA (75.9% vs 51.9%, p<0.001). Notably, crusts and lacerations showed no statistically significant difference between groups (p=0.186 and p=0.230, respectively) as seen in Table 4.
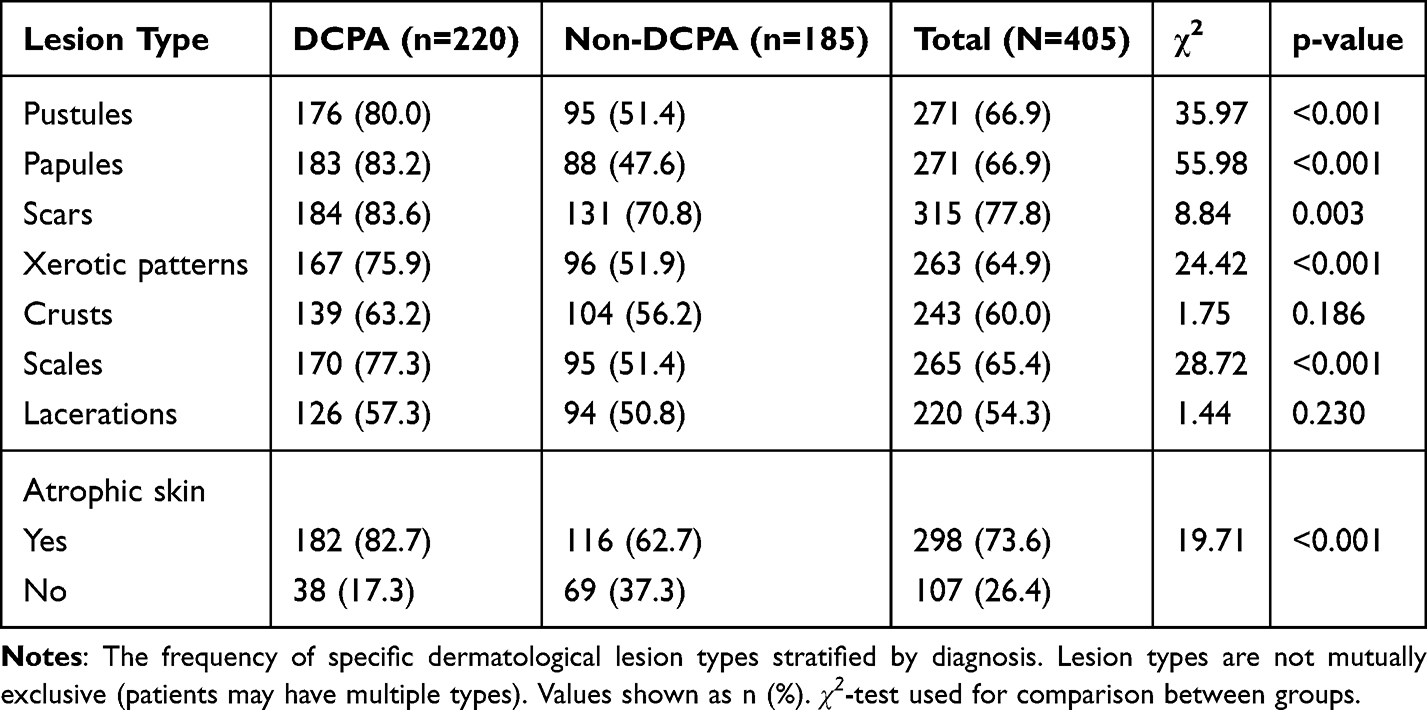 |
Table 4 Distribution of Individual Lesion Types by Diagnosis |
DCPA Predisposing Factors
Statistically analyzing the predisposing factors, the structural equation model successfully examined how Age, Sex, and Oily Topical Application (TA) predict Condition, explaining 11.2% of the variance (R2 = 0.112). The path diagram illustrates that Sex has the strongest effect (β = 0.26, p < 0.001), followed by Age (β = 0.09, p < 0.001) and TA (β = 0.05, p = 0.016), with all predictors showing statistically significant positive relationships with DCPA Condition. Weak correlations exist between predictors (Age-Sex: −0.04, Age-TA: 0.01, Sex-TA: −0.002), indicating minimal multicollinearity. The residual variance for Condition (0.221) confirms that whereas the model captures significant relationships, substantial unexplained variance remains as seen in Table 5.
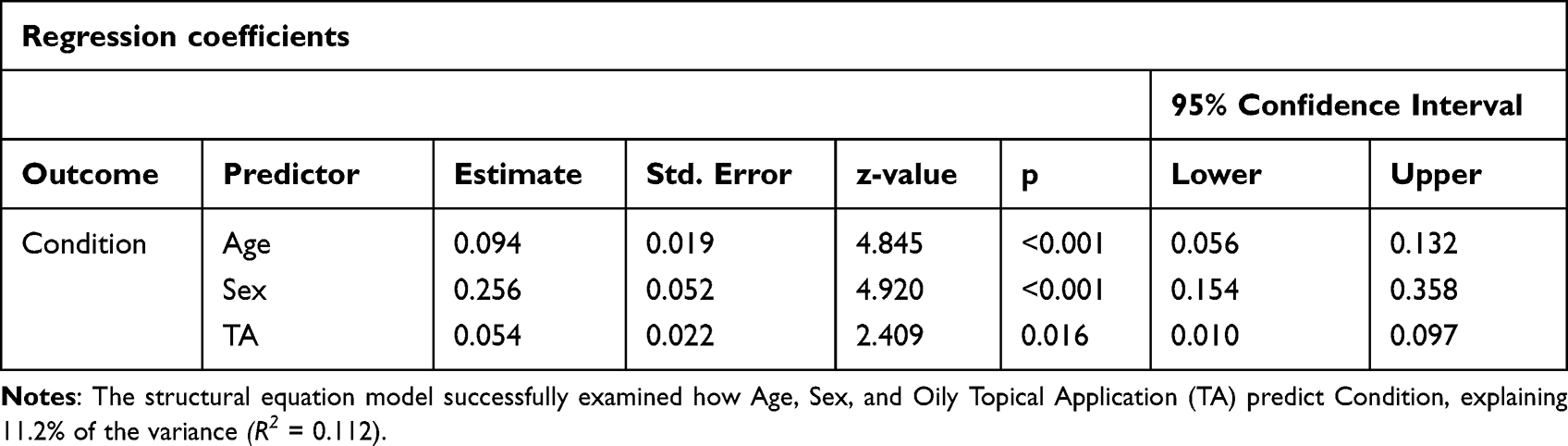 |
Table 5 Clinical Presentation and Physical Examination Findings by Diagnosis |
Discussion
DCPA in South west Uganda is a condition that has not yet been well documented and has therefore not attracted much attention from the clinicians. The specific estimated prevalence in Uganda and East Africa in general is not available. However, prevalence from West Africa and South India ranges from 0.4 to 4.8%.3 In this cross-sectional analysis from two clinic sites, the majority of the patients presented with complaints of itchy legs associated with pus discharges or dry scaling lesions on the shins. Most of the patients (44.4%) reported symptoms lasting 0–12 months, while 16% had symptoms persisting for 78 months or more. This suggests a wide range of disease chronicity, with a significant proportion experiencing long-term symptoms. Socioeconomically this leads to reduced productivity and increased amounts of money spent on the treatment. Furthermore, the young age group of the school going persons tend to get stigmatized to the extent that some refuse to attend schools. The need for wearing school uniforms that reveal the legs with lesions like scars, pus or crusts leaves some young people stigmatized, demoralized and sometimes depressed as well.
The study revealed significant gender disparity, with females comprising 71.9% of the affected population, contrasting with previous studies from West Africa and India where male predominance was reported.7
This variance may be attributed to regional differences in cosmetic practices, particularly the more frequent use of petroleum-based products among females in Southwestern Uganda.
Age distribution analysis showed a marked incidence (74.9%) in the 0–25 year age group, with a mean age of 21.6 years (SD=15.1). This demographic pattern correlates with increased use of petroleum jelly and heightened susceptibility to stigmatization, particularly affecting school attendance among female youth as earlier noted by João et al.1
Disease duration analysis revealed a bimodal distribution, with 44.4% of cases presenting within the first year of onset, while 16% demonstrated chronic persistence exceeding 78 months. This temporal pattern suggests both acute presentation and chronic progression, highlighting the condition’s potential for long-term morbidity and the need for effective early intervention strategies.
Occupational distribution revealed predominant involvement of students (38%) and pupils/infants (25.4%), suggesting age-related vulnerability. The significant representation of farmers (16%) and semiskilled laborers (8.9%) indicates potential environmental or occupational risk factors, while business professionals and housewives showed lower prevalence (6.9%).
The regression analysis revealed insights into the determinants of DCPA in southwestern Uganda. The model, which examined the predictive relationships of age, sex, and topical application (TA) on DCPA condition, demonstrated modest but statistically significant explanatory power (R2 = 0.112). Sex emerged as the strongest predictor (β = 0.26, p < 0.001), aligning with the observed female predominance (71.9%) in the study population. Age showed a moderate effect (β = 0.09, p < 0.001), consistent with the concentration of cases in younger demographics (74.9% within 0–25 years). Topical application, while significant (β = 0.05, p = 0.016), exhibited the weakest effect among the predictors, suggesting a more complex relationship between skincare practices and DCPA development than initially hypothesized.
The minimal intercorrelations among predictors (Age-Sex: −0.04, Age-TA: 0.01, Sex-TA: −0.002) indicate robust model specification without multicollinearity concerns. However, the substantial residual variance (0.221) and modest R2 value suggest that while these factors significantly influence DCPA occurrence, additional unmeasured variables likely contribute to the condition’s etiology. This finding highlights the need for more comprehensive research incorporating additional potential risk factors, particularly environmental and genetic variables, to better understand DCPA’s complex pathogenesis.
The visualization data further support these findings, particularly in the age and sex distribution patterns across DCPA and Non-DCPA cases.
Treatment modalities demonstrated a concerning reliance on non-medical interventions, with petroleum jelly (28.6%) being the predominant choice. The patients face a double jeopardy using petroleum jelly as a cosmetic application and as a form of treatment. A significant number no treatment (21.2%) and herbal remedies (11.9%). This suggests a reliance on nonmedical or homebased remedies, possibly due to limited access to healthcare. The limited utilization of conventional medical treatments like systemic antibiotics (8.9%) and topical antifungals (5.2%) suggests significant barriers to accessing appropriate healthcare services, reflecting similar patterns observed in neighboring regions like Kiambu, Kenya.6
This comprehensive analysis emphasizes the complex interplay of demographic, socioeconomic, and healthcare access factors in DCPA manifestation and management in Southwestern Uganda, highlighting the need for targeted interventions and improved healthcare accessibility.
Surprisingly, petroleum jelly was the most frequently used topical cosmetic application, probably due to its low cost on the market. However, as noted by Eunice S. Song et al there are various barriers that affect the health seeking behaviors of people in Uganda.9 The situation is not so different in Kiambu, Kenya where patients favored the use of non-conventional products such as bar soap and milking jelly as routine skincare products.6 In the case of MRRH, Edward, et al had previously documented the common skin infectious conditions and the causative microorganisms. For that matter extrapolation of the same antimicrobial agents would be of effective use for both MRRH and KRRH.10
Conclusion
This is one of the first studies on DCPA in southwestern Uganda aiming at identifying factors associated with its clinical manifestation. It fills a gap in the regional medical literature while demonstrating that the condition is prevalent in southwestern Uganda with a marked gender disparity, with females constituting 71.9% of cases. This indicates that the female sex was the strongest predictor of developing DCPA. This also points to potential gender-specific risk factors or healthcare-seeking behaviors in the society. The significant epidemiological patterns and clinical implications should warrant attention from healthcare providers and public health officials. The age-specific vulnerability shows that young age was also a significant factor in the development of DCPA. The common use of petroleum jelly had a modest statistical effect, suggesting a more complex relationship in the various factors that can predispose a person to develop DCPA. The occupational distribution, dominated by students and pupils/infants further emphasizes the impact on younger demographics and raises concerns about potential educational and social consequences. The treatment patterns observed, particularly the predominant use of non-medical interventions and limited utilization of evidence-based treatments, highlight critical gaps in healthcare access and management strategies.
Study Limitations
The findings in this study were limited by the use of a non-probability sampling method and the exclusive dependency on a clinical diagnosis made by the practicing clinicians together with the low R2, indicating unmeasured variables. There was also a possible selection bias in the clinics and schools where the clinical data was collected. Such factors for convenience could have had an impact on the study findings.
Recommendations
Considering the current status where DCPA is not even recognized as a stand-alone diagnosis, it would be helpful to consider training non-dermatology healthcare workers about the condition and its management. Targeted educational campaigns on use of over the counter topical medicated and non-medicated cosmetic products should be emphasized by the public health officers in the ministry of health in Uganda. Specific interventions targeting schools both in rural and urban communities should be emphasized going by the most affected group. There is a potential for future use of AI tools for early diagnosis of DCPA since the smartphones are now becoming common even in the rural areas. This should be pursued further to empower the non-dermatology trained clinicians which in turn will reduce the stigmatization and other unwanted effects of DCPA like missing of classes and work among the affected persons.
Abbreviations
AI, Artificial Intelligence; DCPA, Dermatitis cruris pustulosa et atrophicans; IRB, Institutional Review Board; KRRH, Kabale Regional Referral Hospital; MRRH, Mbarara Regional Referral Hospital; MUDSReH, Mbarara University Data Science Research Hub; MUST, Mbarara University of Science and Technology; NIH, National Institutes of Health; ODK, Open Data Kit; UNCST, Uganda National Council for Science and Technology.
Funding
This study was supported by Fogarty International Center, National Institutes of Health, under ward Number U54TW012043. We would like to thank Mbarara University of Science and Technology- Mbarara University Data Science Research Hub (MUDSReH).
Disclosure
The authors report no conflicts of interest in this work.
References
1. João AL, Cunha N, Pinheiro RR, Lencastre A. Dermatitis cruris pustulosa et atrophicans: scarring alopecia beyond scalp hair. Skin Appendage Disorders. 2022;8(4):280–9. doi:10.1159/000521267
2. Couppoussamy KI, Devanda R. Dermoscopic features of dermatitis cruris pustulosa et atrophicans: a retrospective study from a Tertiary Care Center in South India. Indian Dermatol Online J. 2024;15(5):801–804. doi:10.4103/idoj.idoj_855_23
3. Rita ALJNC, Lencastreb RPA. Dermatitis Cruris Pustulosa et Atrophicans: scarring Alopecia Beyond Scalp Hair; 2022.
4. Harman R. Dermatitis cruris pustulosa et atrophicans, the Nigerian shin disease. Br J Dermatol. 1968;80(2):97–107. doi:10.1111/j.1365-2133.1968.tb12268.x
5. Adamson AS, Suarez EA, McDaniel P, Leiphart PA, Zeitany A, Kirby JS. Geographic distribution of nonphysician clinicians who independently billed Medicare for common dermatologic services in 2014. JAMA Dermatol. 2018;154(1):30–36. doi:10.1001/jamadermatol.2017.5039
6. Njenga W, Mwancha-Kwasa M, Fossa K, et al. Skin care habits of patients with eczema at Kiambu Level 5 Hospital, Kiambu county, Kenya: a retrospective cross-sectional study. JAAD Int. 2024;16:214–220. doi:10.1016/j.jdin.2024.04.011
7. Kaimal S, D’Souza M, Kumari R. Dermatitis cruris pustulosa et atrophicans; 2009.
8. Kamulegeya L, Bwanika J, Okello M, et al. Using artificial intelligence on dermatology conditions in Uganda: a case for diversity in training data sets for machine learning. Afr Health Sci. 2023;23(2):753–763. doi:10.4314/ahs.v23i2.86
9. Song ES, Musinguzi P, Dieckhaus KD. Factors affecting patient presentation at a national dermatology referral clinic in Kampala, Uganda. Int J Dermatol. 2017;56(3):291–295. doi:10.1111/ijd.13435
10. Edward O, Bazira J, Grace M. Clinical description, bacterial causes and the association of HIV with pyodermas presenting at a skin clinic of a Tertiary Hospital in Rural South Western Uganda. Int J Trop Dis Health. 2014;5(3):230–238. doi:10.9734/IJTDH/2015/12294
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Herpes Zoster Ophthalmicus Clinical Presentation and Risk Factors for Lesion Recovery
Xiao Z, Wu H, Chen X, Chen X, Yu R, Chen A
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3767-3773
Published Date: 29 December 2023
Evaluation of Vitamin B12 Deficiency Among Patients with Type 2 Diabetes Mellitus on Metformin at Hoima Regional Referral Hospital, Uganda
Ali HO, Agwu E, Ali MA, Jama YM, Ahmed AH, Yusuf MAM, Araye AA, Osobow IM, Sandeyl AA, Ahmed ZA, Onyanga N, Nor FI, Mohamed AH, Karshe AH, Hirsi AM, Mohamed AA, Jayte M
Diabetes, Metabolic Syndrome and Obesity 2026, 19:562440
Published Date: 21 January 2026