")
Back to Journals » Vascular Health and Risk Management » Volume 19
Prevalence of Hypercholesterolemia and Awareness of Risk Factors, Prevention and Management Among Adults Visiting Referral Hospital in Ethiopia
Authors Belete AK , Kassaw AT , Yirsaw BG , Taye BA, Ambaw SN, Mekonnen BA , Sendekie AK
Received 15 February 2023
Accepted for publication 27 March 2023
Published 30 March 2023 Volume 2023:19 Pages 181—191
DOI https://doi.org/10.2147/VHRM.S408703
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Harry Struijker-Boudier
Aychew Kassa Belete,1 Abebe Tarekegn Kassaw,2 Bantie Getnet Yirsaw,3 Birhan Ambachew Taye,3 Samueal Nigatie Ambaw,1 Biset Asrade Mekonnen,4 Ashenafi Kibret Sendekie5
1Department of Sport Science, Faculty of Natural and Computational Science, Woldia University, Woldia, Ethiopia; 2Department of Pharmacy, College of Medicine and Health Sciences, Woldia University, Woldia, Ethiopia; 3Department of Statistics, Faculty of Natural and Computational Science, Woldia University, Woldia, Ethiopia; 4Department of Pharmaceutical Analysis, School of Pharmacy, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia; 5Department of Clinical Pharmacy, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Ashenafi Kibret Sendekie, Email [email protected]
Background: Unhealthy lifestyles and physical inactivity are among the contributing factors of hypercholesterolemia. This study assessed the prevalence, awareness of risk factors, and prevention and treatment of hypercholesterolemia among adults who visited Woldia referral hospital, Northeast Ethiopia.
Methods: A cross-sectional survey was conducted among adults who visited Woldia referral hospital from May to August 2022. Data was collected using a structured questionnaire through a face-to-face interview and patient medical record review. Logistic regression analysis was employed to determine the association between hypercholesterolemia and other variables. A p-value at a 95% confidence level was statistically significant.
Results: A total of 1180 eligible adults were included in the study. The magnitude of hypercholesterolemia was 26.4%. The majority of the respondents were aware of some risk factors, such as higher fat intake (82.3%), obesity (67.2%), and lack of adequate exercise (56.1%). However, the majority of the respondents were not aware that smoking, alcohol consumption, and age (86.8% for all) had cardiovascular risk. The majority of the respondents were aware that eating a limited amount of saturated fat (56.5%), maintaining a healthy weight (67.2%), and taking prescribed medications properly (86.8%) can prevent the risk of hypercholesterolemia. However, a larger proportion of respondents were unaware that smoking cessation (86.8%), exercise (55.3%), alcohol restriction (86.8%), and stress avoidance (75.3%) can prevent cardiovascular risks. Age (p = 0.036), smoking (p = 0.007), alcohol use (p = 0.013), fruit consumption (p = 0.019), saturated oil use (p = 0.031), level of physical activity (p < 0.001), and body mass index (p = 0.03) were significantly associated with hypercholesterolemia.
Conclusion: This study concluded that more than one-fourth of adults had hypercholesterolemia. The majority of the respondents did not have an awareness of common cardiovascular risk factors and prevention and treatment techniques regarding unhealthy lifestyles and physical inactivity.
Keywords: hypercholesterolemia, cholesterol, dyslipidemia, awareness, prevention, risk factors
A Letter to the Editor has been published for this article.
Introduction
Cholesterol is a fat-like substance that is produced inside the liver and absorbed from the diet.1 It is required by the body for the formation of cellular membranes, a building block of steroid hormones, and the formation of bile acids, which aid fat digestion.2 Hypercholesterolemia is an abnormality of lipids in the blood.3 Approximately 18% of strokes and 56% of heart attacks are caused by high blood cholesterol.4 Age, gender, family history, an unhealthy lifestyle, and physical inactivity, such as alcohol consumption, smoking, excessive dietary cholesterol, and sedentary lifestyle have been linked with increased cardiovascular risks and have either direct or indirect impact on hypercholesterolemia.5 Recent studies suggest that doing regular physical exercise, consuming more fruit, reducing saturated fat, stopping smoking, and managing stress all play significant roles in the prevention of hypercholesterolemia.6 According to one study, 65% of Saudi respondents have high levels of cholesterol.7 Recent evaluations have shown that around 28.5 million people in the adult population aged 20 years or older have high levels of total serum cholesterol.8
Cardiovascular disease, musculoskeletal disorder, cancer, pulmonary disorder, psychological problems, back pain, and metabolic disorder have all been linked to unhealthy lifestyles and physical inactivity.9 The world is currently being invaded by hypokinetic disease, which is spreading at an alarming rate.10,11 Many factors, including knowledge, attitude, sociodemographic characteristics, behavioral factors, and biomedical characteristics, could all play a role in hypercholesterolemia.12 As a result, research-based information on the prevalence, associated factors, and awareness of risk factors, prevention, and treatment of hypercholesterolemia is urgently required for its management.
Despite increasing these risk factors, limited data can be found about the prevalence and awareness of the population regarding risk factors and the prevention and treatment of hypercholesterolemia in Ethiopia, except that only two studies assessed the prevalence of dyslipidemia in two cities across the country.13,14 Although there is an increase in sedentary life and unhealthy diet, obesity, alcohol intake, and smoking, which can cause different cardiovascular diseases in Ethiopia,15,16 there is no single study that has assessed the community’s awareness of risk factors and the prevention and treatment of hypercholesterolemia. As a result, this study was aimed at assessing the prevalence and awareness of risk factors and the prevention and treatment of hypercholesterolemia among adults who visited the Woldia referral hospital.
Methods and Materials
Study Design and Setting
A cross-sectional survey was conducted among adults who visited Woldia referral hospital from May 1 to August 30, 2022. Woldia referral hospital is located in Woldia city, which is located in Ethiopia’s Northeast Amhara region, 521 kilometers from Addis Ababa, and the estimated total population of the city as of the time of the study was 180 thousand.17 The referral hospital serves both residents of the city and is used as a referral for rural health facilities. The majority of the people served in the hospital are rural in comparison with the rich city dwellers.
Study Population, Eligibility Criteria and Sampling Techniques
The sample size was estimated by approaching a total survey of adults who visited Woldia referral hospital with evidence of lipid profile measurement and/or diagnosed dyslipidemia during the data collection period. Participants were enrolled in the study using a survey method in which all adults who were eligible were included. The sample with complete lipid measurements or recorded evidence of diagnosis included 1305 patients. Consequently, a total of 1305 eligible adults were approached about the study, but only those who volunteered to participate in it were included in the final data collection.
Outcome Measures and Definition of Terms
We used commonly used measures to determine the prevalence, risk factor awareness, treatment, and prevention of dyslipidemia among the participants.18
Hypercholesterolemia
Hypercholesterolemia was defined as having a total cholesterol level higher than or equal to 5.0 mmol/L and/or evidence of diagnosed dyslipidemia in the patient’s medical record. Furthermore, we reviewed evidence of abnormally recorded diagnoses of other lipid profiles, such as low-density lipoprotein (LDL) and high-density lipoprotein (HDL) levels. Thus, the prevalence of hypercholesterolemia was determined from recorded evidence of diagnosis and/or having at least one abnormal level of total cholesterol, LDL and HDL in lipid profiles.
Awareness
It was defined as participants’ self-reported perceptions and/or knowledge of hypercholesterolemia risk factors, prevention, and treatment plans. The participants were interviewed to say “yes” or “no” for the statements that assessed their perceptions and/or knowledge on the risk factors and prevention and treatment of hypercholesterolemia.
Physical Activity
In this study, physical activity refers to all movement, including physical transport to and from places, transport during leisure time, or transport as part of an individual’s routine work. Sedentary physical activity indicates physical inactivity for a long period of time or a limited physical exercise that is below the optimum, while vigorous intensity indicates a regular physical activity, whether related to work or sports, active recreation, and play.
Data Collection Instruments, Procedures, and Quality Control Measures
The primary data was collected using a structured questionnaire through a face-to-face interview. The diagnosis of dyslipidemia and lipid profile were extracted from the participant’s medical records. The same questionnaire was prepared in English and translated to Amharic and then back to English to maintain its consistency. It is comprised of four sections. The first is regarding the sociodemographic characteristics of the participants, such as age, sex, marital status, educational level, religious affiliation, and monthly income. The second set of statements assessed the respondents’ behavioral, dietary, and biomedical characteristics, such as smoking, alcohol consumption, exercise, and vegetable consumption. The third section of the instrument consisted of seven statements that assessed the perceptions and/or knowledge of the participants regarding hypercholesterolemia and its risk factors, with has an optimal internal validity test of Cronbach’s alpha of 0.78. The fourth section contains eight statements that can be used to assess participants’ knowledge of hypercholesterolemia prevention and treatment. The internal validity was also examined and resulted well with a Cronbach’s alpha value of 0.80.
The data was collected by four trained nurses. They were trained regarding the purposes and goals of the study and the ethics of data collection of the study and the ethics of data collection. They took anthropometric measurements such as weight, height, and body mass index (BMI) during the interview. A pretest was administered to 10% of the participants prior to data collection. The cross-validity of the questionnaire was checked by three individuals who had expertise in the area. After a minor modification based on the feedback from the pretest that made the questionnaire clearer and easier, actual data collection was performed on a daily basis from Monday to Friday. The supervisors also followed the entire data collection period and closely monitored the quality, clarity, and cleanliness of the data collection procedure.
Data Entry and Statistical Analysis
After ensuring the quality and clarity of the data, it was entered, coded, and analyzed using the Statistical Package for Social Sciences version 26. The normal distribution of the data was examined using a Q-Q plot and histogram. Descriptive results were presented using frequency and percentage for categorical variables, while the mean with standard deviation was used to present continuous variables. Binary logistic regression analysis was used to determine the association between hypercholesterolemia and other independent risk factors. A p-value of < 0.05 at 95% CI was considered statistically significant.
Research Ethics Approval and Consent Form
The proposal was ethically approved by the ethical review board of Woldia University. An official permission letter was obtained from medical director office of Woldia referral hospital with a protocol number ERC/012/2022. Participants were informed and given both written and verbal consent forms after the objectives of the study were briefed. Participants involved in the study were in a position to provide informed consent and had a full understanding of the study’s purposes. All methods were carried out in accordance with relevant guidelines and regulations based on the Helsinki legislation.
Results
Sociodemographic Characteristics of the Participants
The final study included 1180 (90.4% response rate) of the 1305 adults who were approached. The mean age of the participants was 52.5±9.7. Similarly, more than half (54.5%) of the participants were male. In terms of educational status, the majority (62.1%) had a college degree or higher. Around three-fourths (72.7%) were self-employed regarding their occupation. A higher proportion of the participants (42%) had monthly income greater than 6000 Ethiopian Birr (ETB) (Table 1)
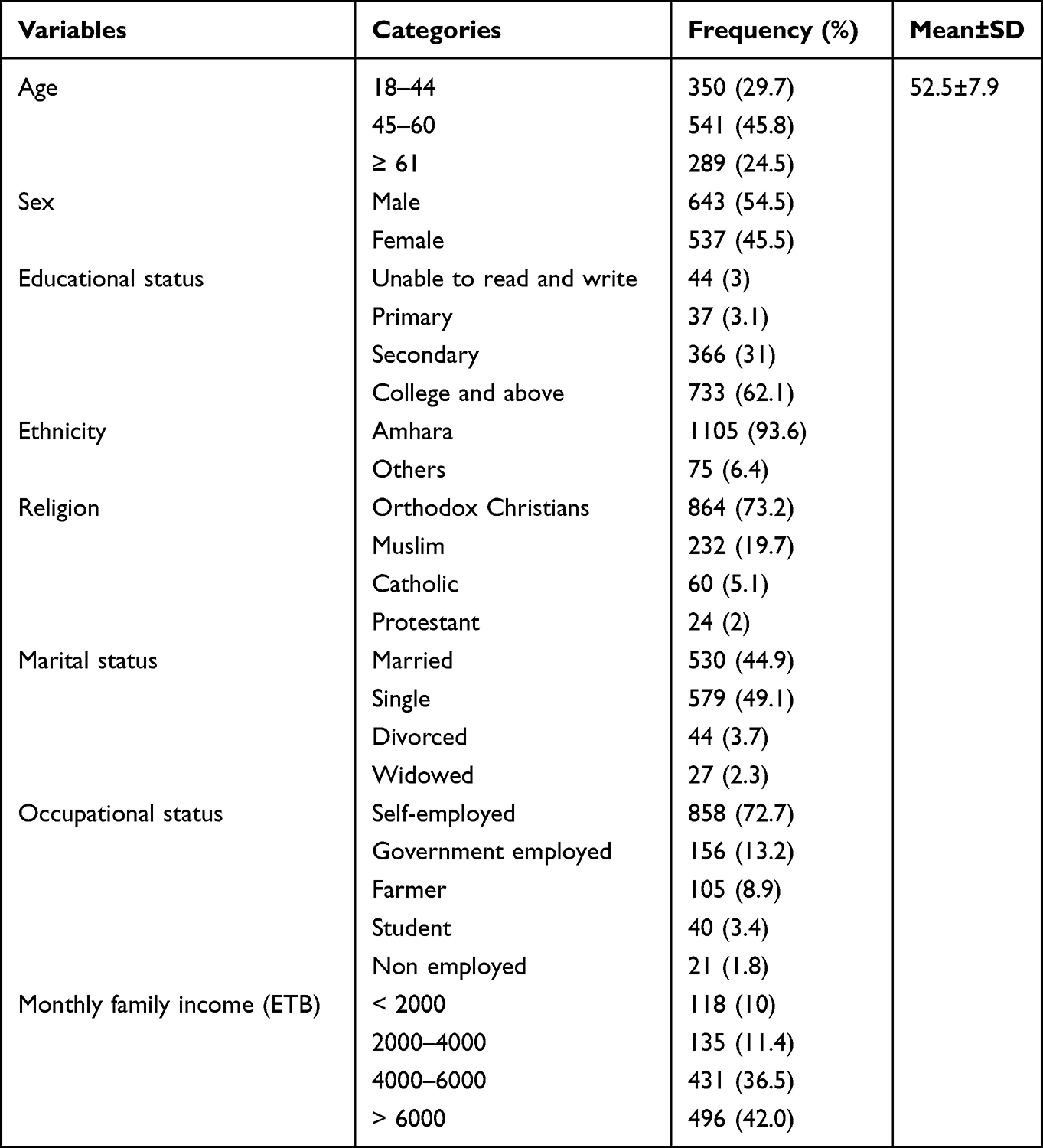 |
Table 1 Sociodemographic Characteristics Among Adults in Woldia City, Northeast Ethiopia from May 01 to August 30, 2022 |
Respondents’ Behavioral, Dietary, and Biomedical Characteristics
In terms of smoking habits, the majority of respondents (71.7%) were never smokers. Whereas, in terms of alcohol use, around two-thirds (64.7%) were current users of alcohol. When we look at the frequency of drinking alcohol per week among alcohol users, 52.6% drink less than or equal to three times per week. In terms of fruit consumption, 81.4% were fruit consumers, and 77.1% consumed fruit fewer than three times per week. Furthermore, half of the respondents (50%) had a normal weight corresponding to their body mass index (BMI) (BMI) (Table 2).
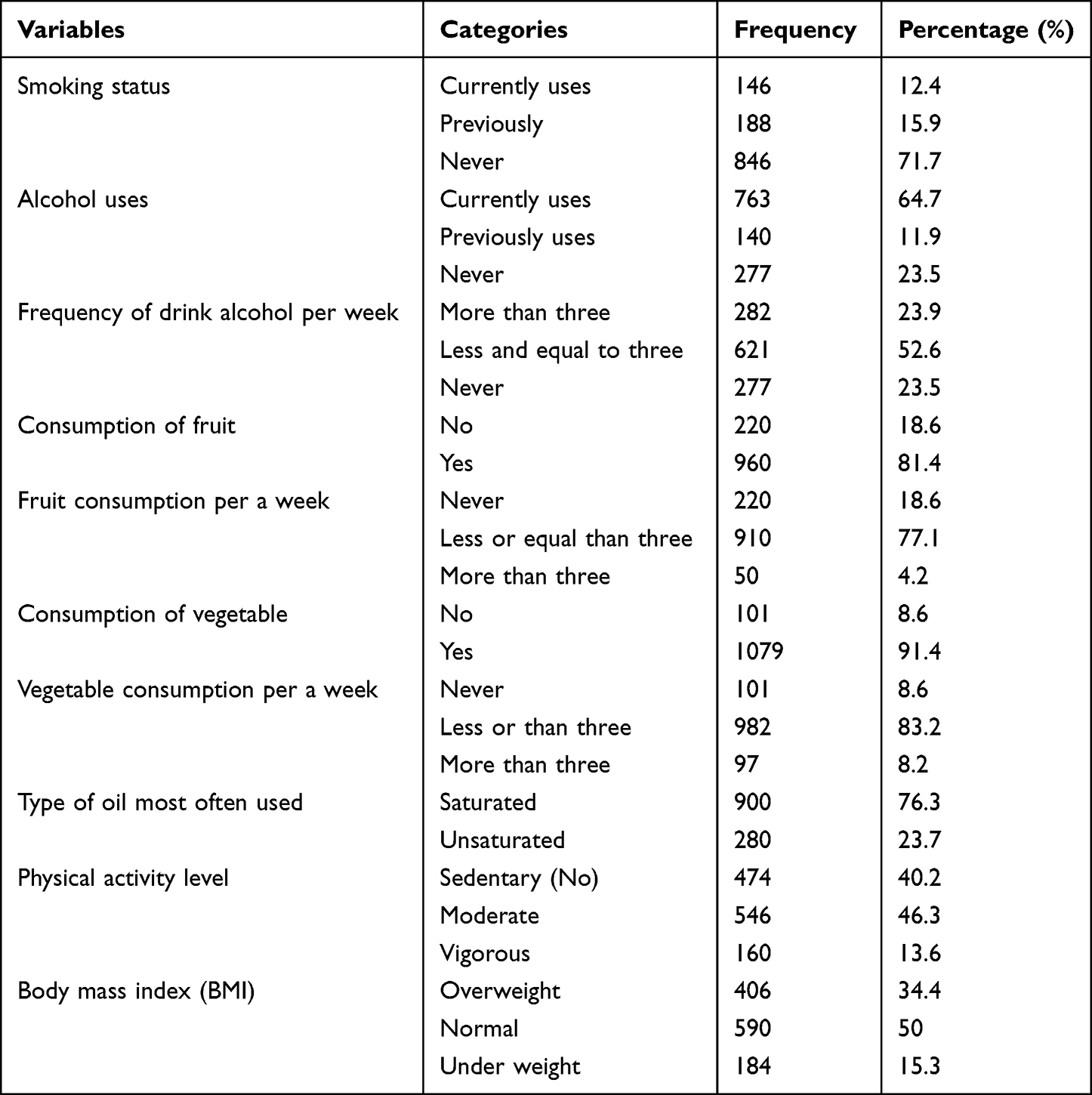 |
Table 2 Behavioral, Dietary, and Biomedical Related Characteristics Among the Participants |
Prevalence of Hypercholesterolemia
From a total of 1180 study participants, 311 were found to have at least one abnormal lipid profile level and/or been diagnosed with dyslipidemia, resulting in a magnitude of hypercholesterolemiato be 26.4% currently.
Participant’s Awareness on Hypercholesterolemia and Cardiovascular Risks
The majority of the respondents (89.1%) heard about hypercholesterolemia. Similarly, the majority of the respondents reported being aware of the risk factors, such as high fat consumption (82.3%), obesity (67.2%), and lack of exercise (56.1%). However, the majority of them were not aware about common cardiovascular risks that may have a direct or indirect contribution for hypercholesterolemia, such as smoking, drinking, and age (86.8% for all) (Table 3).
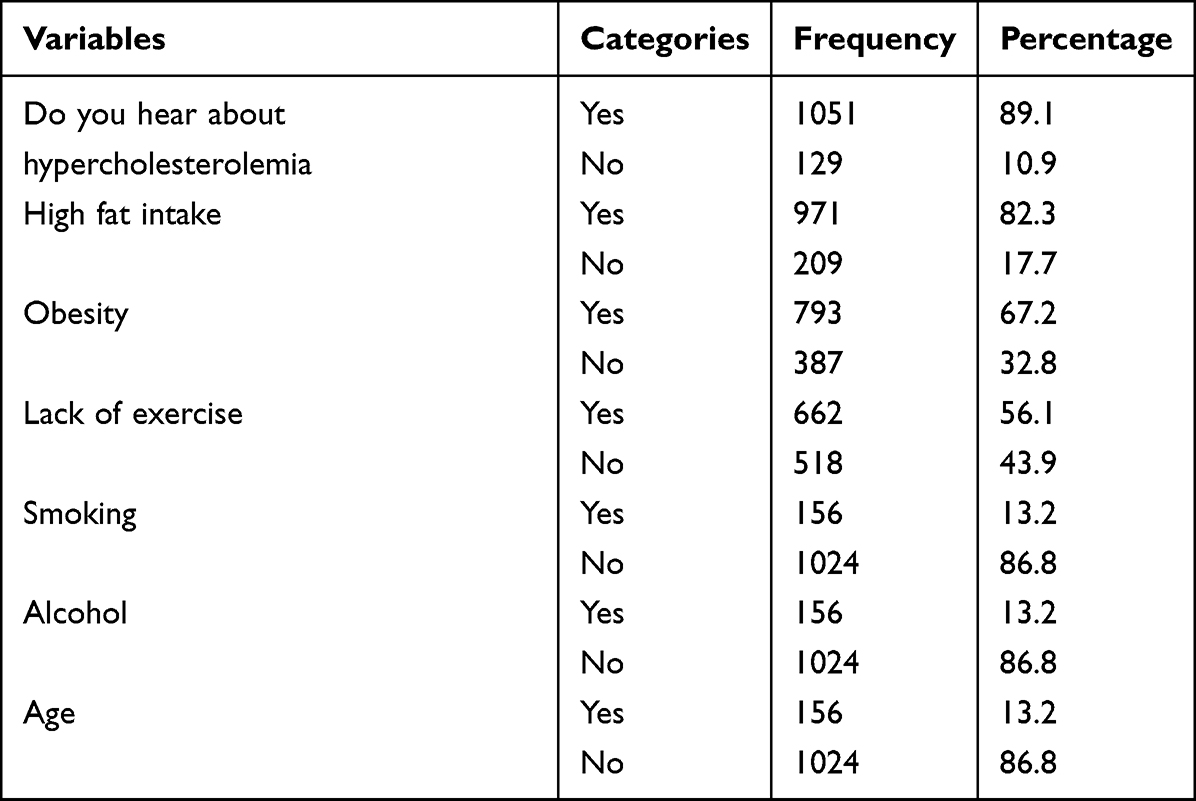 |
Table 3 The Awareness of Respondents on Unhealthy Lifestyle, Physical Inactivity, and Other Cardiovascular and Hypercholesterolemia Risks |
Participants’ Awareness on the Prevention and Treatment of Hypercholesterolemia and Cardiovascular Risks
The majority of respondents were aware of some direct or indirect risk factors for cardiovascular disease and hypercholesterolemia, such as eating more fruits (63.9%), limiting saturated fat (56.5%), maintaining a healthy weight (67.2%), and taking prescribed medications properly (86.8%). However, the majority of those respondents were not aware of other cardiovascular risk prevention techniques such as quitting smoking (86.8%), exercising (55.3%), decreasing alcohol consumption (86.8%), and managing stress (75.3%) (Table 4).
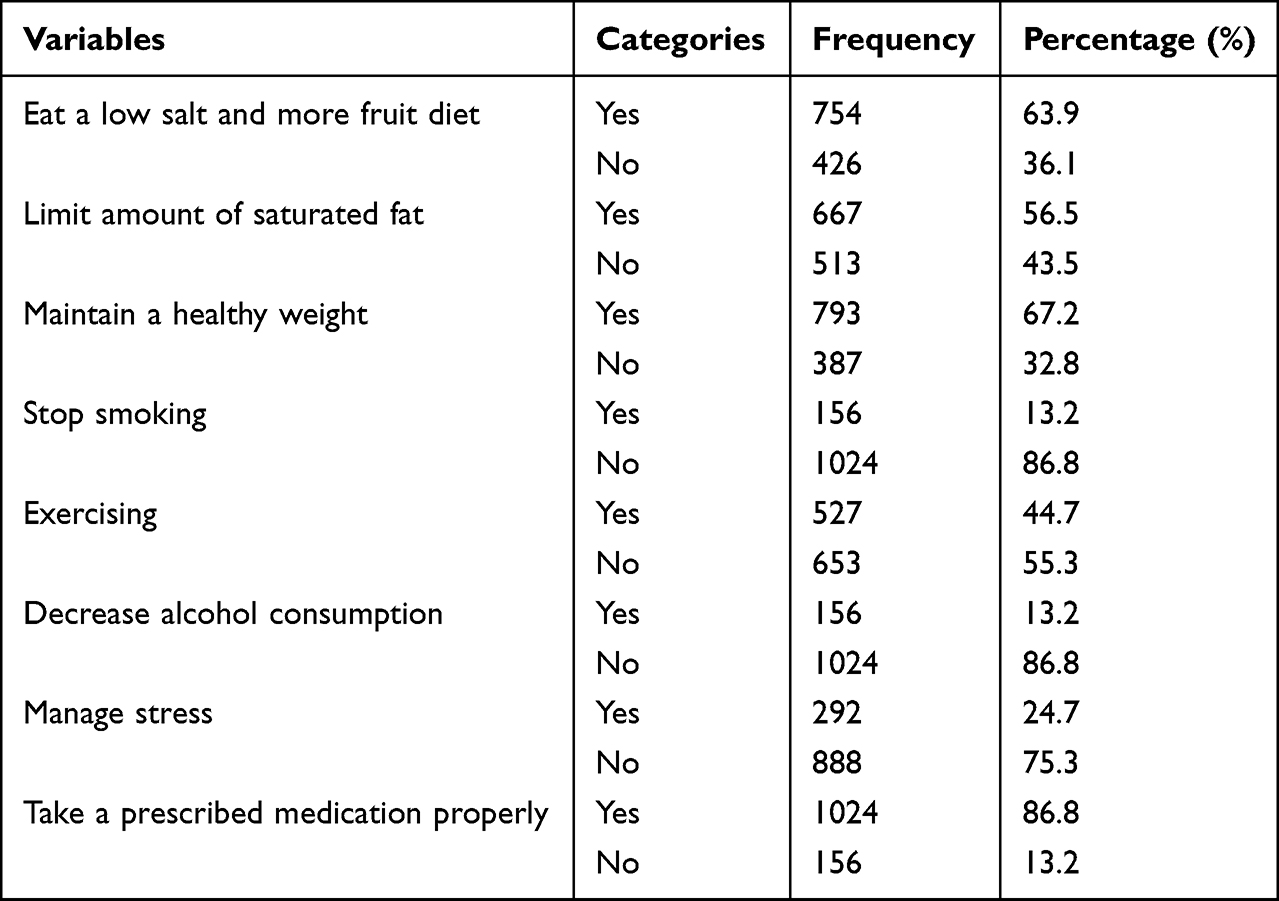 |
Table 4 The Awareness of Respondents on Prevention and Treatment of Hypercholesterolemia and Cardiovascular Risk Factors |
Association Between Prevalence of Hypercholesterolemia and Other Variables
The association between the presence of hypercholesterolemia and other independent variables was demonstrated using a binary logistic regression analysis. Based on the results, age, smoking, alcohol use, fruit consumption, saturated oil use, level of physical activity, and BMI were significantly associated with hypercholesterolemia. Participants aged 61 and higher were more likely to have hypercholesterolemia than those aged 18 to 44 [AOR = 1.134, 95% CI: 1.005–6.471; p = 0.036]. Similarly, those who currently smoked cigarettes [AOR = 1.997, 95% CI: 1.0167–6.231; p = 0.007], drank alcohol [AOR = 2.297, 95% CI: 1.078–6.134; p = 0.013], and did not consume fruits on a regular basis [A = 1.678, 95% CI: 1.045–8.120; p = 0.019] were more likely to have hypercholesterolemia. Participants who used saturated oil the most frequently [AOR = 2.195, 95% CI: 1.023–9.134; p = 0.031], those with a sedentary physical activity level [AOR = 4.321, 95% CI: 1.754–12.379; p 0.001], and those with an overweight BMI [AOR = 4.258, 95% CI: 1.745–10.702; p = 0.03] had higher levels of hypercholesterolemia compared with their counterparts (Table 5).
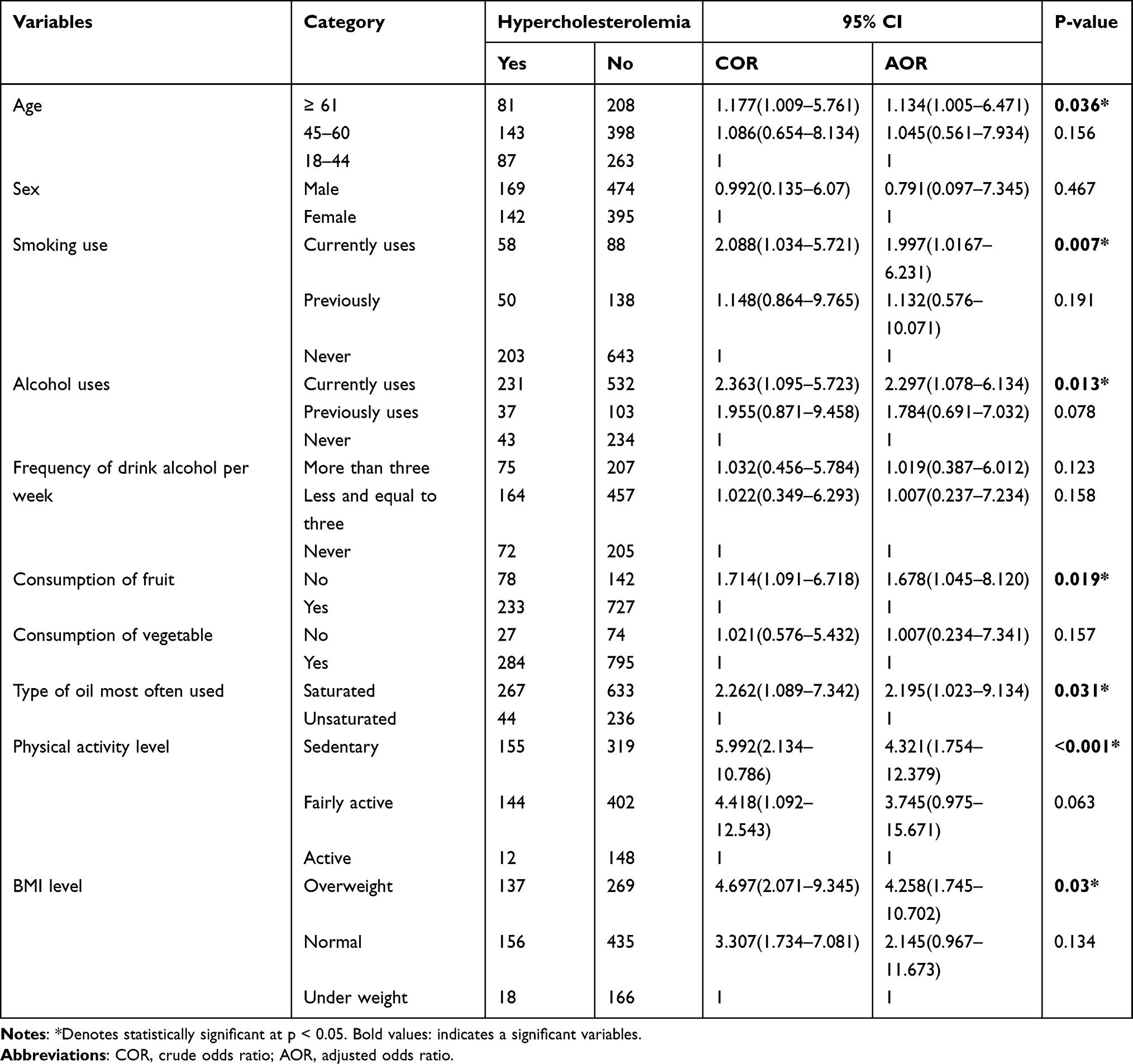 |
Table 5 Association Between Hypercholesterolemia and Other Independent Variables |
Discussion
Despite studies conducted in the European population19,20 and other African nations regarding perceptions about cardiovascular risk factors, based on the authors’ best searching strategy, there is no single published study that has assessed the level of community awareness regarding risk factors, preventions, and treatments of cardiovascular disease and hypercholesterolemia in the Ethiopian population. Therefore, this study assessed the magnitude and awareness of the risk factors, prevention, and treatment of hypercholesterolemia among adults who visited the Woldia referral hospital Northeast Ethiopia.
Indeed, the current study showed that more than one-fourth of adults had an abnormal lipid profile, resulting in a magnitude of hypercholesterolemia of 26.4%. The finding is in line with earlier studies.21–24 However, it is much lower than other studies conducted in Pakistan (96%),25 Jordan (81.6%), Turkey (79%),26 Northern Jordan (75.7%),27 Northern Ethiopia (66.7%),13 Nigeria (38%),14 and China (34%).28 On the other hand, the current finding is somewhat higher than the results of community-based study conducted in Saudi Arabia (12.5%),29 Egypt (22%),30 and the national survey results of 16%.14 The discrepancy might be due to differences in the risk factors because of socioeconomic and cultural variations across the study nations. Additionally, the reporting systems and methodological differences might result in variation.
Based on the current results, the majority (89.1%) of respondents were aware of hypercholesterolemia, which agreed with the study conducted in China.31 On the other hand, this study showed that the majority of the respondents were aware of risk factors such as high fat consumption (82.3%), obesity (67.2%), and lack of exercise (56.1%), which is in line with earlier studies.21,31 For instance, during an in-depth interview on risk factors, a number of respondents who had a better awareness of the risk factors for hypercholesterolemia were able to mention consumption of saturated fat, physical inactivity, and obesity as risk factors. For example, a 27-year-old man claimed that “high saturated fat intake and excessive drinking increase the risk of getting hypercholesterolemia”. The increased awareness of these risk factors is encouraging, but more work needs to be done to improve community awareness.
However, the majority of them were not aware that other cardiovascular risk factors related to unhealthy lifestyles, such as smoking and drinking, and age (86.8% for all).The lack of knowledge about risk factors was identified during the interview stage. During the in-depth interview, the majority of respondents mentioned feeding habits as risk factors for hypercholesterolemia. However, they failed to name a risky feeding habit. For instance, a 34-year-old woman claimed, “The most common risk factor for hypercholesterolemia is excessive food consumption of any kind”. Lack of knowledge on risk factors was also substantiated by another 60-year-old man who stated: “In general, I believe that people are exposed to hypercholesterolemia due to chance or God’s will, rather than any other factor”. This finding may imply that health care professionals, as well as the healthcare system as a whole, should address services in a way that increases individuals’ awareness of important medical conditions that are currently a public health issue.
In agreement with an earlier study,6 respondents were aware that eating a more fruitful diet (63.9%), limiting saturated fat (56.5%), maintaining a healthy weight (67.2%), and taking prescribed medications properly (86.8%) were direct or indirect prevention techniques for cardiovascular and hypercholesterolemia risks. Another study also suggests that doing regular physical exercise, consuming more fruit, reducing saturated fat, stopping smoking, and managing stress play a significant role in the prevention of hypercholesterolemia, either directly or through the prevention of cardiovascular risks.32 However, in this study, the majority of respondents were also not aware of common cardiovascular risk factor preventions that can contribute to decreasing hypercholesterolemia risks, such as quitting smoking (86.8%), exercising (55.3%), decreasing alcohol consumption (86.8%), and managing stress (75.3%). The possible difference might be a difference in lifestyle and sociocultural variation in understanding of different risk factors. In this study, during an in-depth interview, most of the respondents perceived that hypercholesterolemia was not preventable When they are asked to mention the preventive measures, most of them declare that it can be prevented by praying to God. Furthermore, the majority of the participants stated that they avoid eating a lot of fat. As a result, raising awareness and launching action at the community level may be critical.
Consistent with the earlier studies,5 the current study demonstrated that age, alcohol consumption, smoking, and eating excessive unsaturated fat have been linked with hypercholesterolemia. This could be because unhealthy lifestyles and physical inactivity have resulted in cardiovascular disease and metabolic disorders,9 both of which are linked to dyslipidemia. A patient’s advanced age may be a cause of dyslipidemia due to an increase in morbidity, which may be caused by limited exercise and physical inactivity, resulting in an increase in visceral fat. An earlier study also showed that an increase in total cholesterol was associated with an older age.25,33–37 In line with earlier studies, the current study showed that being overweight increases the odds of hypercholesterolemia.13,26,28,34,38,39 This might be because a higher level of BMI can be attributed to metabolic insulin resistance and an excess of visceral fat. In contradiction with the current study,28,38–42 an earlier study did not show a significant association between hypercholesterolemia and age, smoking, alcohol use, or dietary pattern. This variation could be explained by methodological differences in the samples and study designs used in the various studies. As a result, modifying the lifestyle through healthy eating (avoiding high cholesterol diets and consuming fruits), regular exercise, and smoking cessation plays an important role in avoiding risk factors. Recent studies suggest that doing regular physical exercise, consuming more fruit, reducing saturated fat, and stopping smoking play a significant role in the prevention of hypercholesterolemia.6
In general, the current study highlighted the magnitude and associated factors of hypercholesterolemia and the extent of adult awareness of risk factors, prevention, and management of the disease. However, because multifactorial risk factors exist and the associated burden has a negative impact on sociodemographic and the economy for the general public, multi-sectorial involvement may be required for community-level dyslipidemia prevention and management.
Study Strengths and Limitations
The use of a larger representative sample and the standardized survey methodology and measures can be mentioned as strengths of this study. However, selection bias may influence the composition of participants, so it is difficult to draw firm conclusions. The study design itself, a cross-sectional survey design, precludes drawing causal conclusions between the evaluated variables. Therefore, considering study limitations could be important to interpreting and using the finding. Further research considering these limitations in the area will be welcomed.
Conclusion
The current study can conclude that more than one-fourth of adults had dyslipidemia. The majority of the respondents did not have awareness about common cardiovascular risk factors and prevention and treatment techniques regarding unhealthy lifestyle, physical inactivity, and age. Furthermore, older age, smoking, alcohol use, inability to consume fruits, sedentary life, and being overweight were found to have a significant association with the occurrence of hypercholesterolemia.
Abbreviations
BMI, body mass index; LDL, low-density lipoproteins; HDL, high-density lipoprotein.
Data Sharing Statement
The data sets supporting the conclusions of this article are available upon reasonable request to the corresponding author.
Consent to Publication
Consent to publication from participants was not required because confidentiality was maintained according to the rules and regulations.
Acknowledgment
The authors would like to acknowledge the Woldia university for give an opportunity to conduct this research. We also extend our gratitude to the data collectors and study participants for their contribution.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We have not received any financial support for funding.
Disclosure
The authors report no conflicts of interest related to this work.
References
1. Clifford J, Kozil A. Dietary Fat and Cholesterol. Colorado State University; 2012.
2. Tabas I. Cholesterol in health and disease. J Clin Invest. 2002;110(5):583–590. doi:10.1172/JCI0216381
3. Goldstein JL, Hazzard WR, Schrott HG, Bierman EL, Motulsky AG. Hyperlipidemia in coronary heart disease. I. Lipid levels in 500 survivors of myocardial infarction. J Clin Invest. 1973;52(7):1533–1543. doi:10.1172/JCI107331
4. Murray CJ, Lauer JA, Hutubessy RC, et al. Effectiveness and costs of interventions to lower systolic blood pressure and cholesterol: a global and regional analysis on reduction of cardiovascular-disease risk. Lancet. 2003;361(9359):717–725. doi:10.1016/S0140-6736(03)12655-4
5. Kalmijn S, van Boxtel MP, Ocké M, Verschuren WM, Kromhout D, Launer LJ. Dietary intake of fatty acids and fish in relation to cognitive performance at middle age. Neurology. 2004;62(2):275–280. doi:10.1212/01.WNL.0000103860.75218.A5
6. Kromhout D, Menotti A, Kesteloot H, Sans S. Prevention of coronary heart disease by diet and lifestyle: evidence from prospective cross-cultural, cohort, and intervention studies. Circulation. 2002;105(7):893–898. doi:10.1161/hc0702.103728
7. Al-Zahrani J, Shubair MM, Al-Ghamdi S, et al. The prevalence of hypercholesterolemia and associated risk factors in Al-Kharj population, Saudi Arabia: a cross-sectional survey. BMC Cardiovasc Disord. 2021;21(1):22. doi:10.1186/s12872-020-01825-2
8. Arnett DK, Jacobs DR, Luepker RV, Blackburn H, Armstrong C, Claas SA. Twenty-year trends in serum cholesterol, hypercholesterolemia, and cholesterol medication use: the Minnesota Heart Survey, 1980–1982 to 2000–2002. Circulation. 2005;112(25):3884–3891. doi:10.1161/CIRCULATIONAHA.105.549857
9. Morewitz SJ. Chronic Diseases and Health Care: New Trends in Diabetes, Arthritis, Osteoporosis, Fibromyalgia, Low Back Pain, Cardiovascular Disease, and Cancer. Springer Science & Business Media; 2006.
10. Cardinal BJ. Toward a greater understanding of the syndemic nature of hypokinetic diseases. J Exerc Sci Fit. 2016;14(2):54–59. doi:10.1016/j.jesf.2016.07.001
11. Zou L, Zhang Y, Sasaki JE, et al. Wuqinxi Qigong as an alternative exercise for improving risk factors associated with metabolic syndrome: a meta-analysis of randomized controlled trials. Int J Environ Res Public Health. 2019;16(8):1396. doi:10.3390/ijerph16081396
12. Cremers AL, de Laat MM, Kapata N, Gerrets R, Klipstein-Grobusch K, Grobusch MP. Assessing the consequences of stigma for tuberculosis patients in urban Zambia. PLoS One. 2015;10(3):e0119861. doi:10.1371/journal.pone.0119861
13. Gebreegziabiher G, Belachew T, Mehari K, Tamiru D, Spradley FT. Prevalence of dyslipidemia and associated risk factors among adult residents of Mekelle City, Northern Ethiopia. PLoS One. 2021;16(2):e0243103. doi:10.1371/journal.pone.0243103
14. Asemu MM, Yalew AW, Deyessa N, Kassie DM. Prevalence and risk factors of dyslipidemia among adults: a community based study in Addis Ababa, Ethiopia. Am J Nurs Sci. 2022;11(1):20–29.
15. Ali S, Misganaw A, Worku A, et al. The burden of cardiovascular diseases in Ethiopia from 1990 to 2017: evidence from the Global Burden of Disease Study. Int Health. 2021;13(4):318–326. doi:10.1093/inthealth/ihaa069
16. Aragaw S, Tesfahun E, Derseh BT, Mamo B. Determinants of selected cardiovascular diseases among adult patients at cardiac clinic of Debre Berhan Referral Hospital, Ethiopia: unmatched Case-Control Study. Cardiovasc Ther. 2020;2020:1–8.
17. Fentaw B, Fissha W, Solomon M. Drivers of informal settlements at the peri-urban areas of Woldia: assessment on the demographic and socio-economic trigger factors. Land Use Policy. 2020;95:104573. doi:10.1016/j.landusepol.2020.104573
18. Supiyev A, Nurgozhin T, Zhumadilov Z, Peasey A, Hubacek JA, Bobak M. Prevalence, awareness, treatment and control of dyslipidemia in older persons in urban and rural population in the Astana region, Kazakhstan. BMC Public Health. 2017;17(1):651. doi:10.1186/s12889-017-4629-5
19. Reiner Z, Sonicki Z, Tedeschi-Reiner E. Public perceptions of cardiovascular risk factors in Croatia: the PERCRO survey. Prev Med. 2010;51(6):494. doi:10.1016/j.ypmed.2010.09.015
20. Mazalin Protulipac J, Sonicki Z, Reiner Ž. Cardiovascular disease (CVD) risk factors in older adults - Perception and reality. Arch Gerontol Geriatr. 2015;61(1):88–92. doi:10.1016/j.archger.2015.04.001
21. Ahmed AM, Ozbak HA, Hemeg HA. Effect of essential oil of traditional two Saudi mint types and its possible role in cardiovascular and throat health. Int J Clin Exp Med. 2015;8(5):8060–8068.
22. Tanaka T, Okamura T, Yamagata Z, et al.; HIPOP-OHP Research Group. Awareness and treatment of hypertension and hypercholesterolemia in Japanese workers: the High-risk and Population Strategy for Occupational Health Promotion (HIPOP-OHP) study. Hypertens Res. 2007;30(10):921–928. doi:10.1291/hypres.30.921
23. Ford ES, Mokdad AH, Giles WH, Mensah GA. Serum total cholesterol concentrations and awareness, treatment, and control of hypercholesterolemia among US adults: findings from the National Health and Nutrition Examination Survey, 1999 to 2000. Circulation. 2003;107(17):2185–2189. doi:10.1161/01.CIR.0000066320.27195.B4
24. Noubiap JJ, Bigna JJ, Nansseu JR, et al. Prevalence of dyslipidaemia among adults in Africa: a systematic review and meta-analysis. Lancet Glob Health. 2018;6(9):e998–e1007. doi:10.1016/S2214-109X(18)30275-4
25. Basit A, Sabir S, Riaz M, et al. NDSP 05: prevalence and pattern of dyslipidemia in urban and rural areas of Pakistan; a sub analysis from second National Diabetes Survey of Pakistan (NDSP) 2016–2017. J Diabetes Metab Disord. 2020;19(2):1215–1225. doi:10.1007/s40200-020-00631-z
26. Bayram F, Kocer D, Gundogan K, et al. Prevalence of dyslipidemia and associated risk factors in Turkish adults. J Clin Lipidol. 2014;8(2):206–216. doi:10.1016/j.jacl.2013.12.011
27. Khader YS, Batieha A, El-Khateeb M, Al Omari M, Ajlouni K. Prevalence of dyslipidemia and its associated factors among Jordanian adults. J Clin Lipidol. 2010;4(1):53–58. doi:10.1016/j.jacl.2009.12.004
28. Pan L, Yang Z, Wu Y, et al.; China National Survey of Chronic Kidney Disease Working Group. The prevalence, awareness, treatment and control of dyslipidemia among adults in China. Atherosclerosis. 248;2016:2–9. doi:10.1016/j.atherosclerosis.2016.02.006
29. Lam CS, Roger VL, Rodeheffer RJ, et al. Pulmonary hypertension in heart failure with preserved ejection fraction: a community-based study. J Am Coll Cardiol. 2009;53(13):1119–1126. doi:10.1016/j.jacc.2008.11.051
30. Bhatia JC. Levels and determinants of maternal morbidity: results from a community‐based study in southern India. Int J Gynecol Obstet. 1995;50:S153–S163. doi:10.1016/0020-7292(95)02504-6
31. Song PK, Man QQ, Hong LI, et al. Trends in lipids level and dyslipidemia among Chinese adults, 2002–2015. Biomed Environ Sci. 2019;32(8):559–570. doi:10.3967/bes2019.074
32. Boden-Albala B, Sacco RL. Lifestyle factors and stroke risk: exercise, alcohol, diet, obesity, smoking, drug use, and stress. Curr Atheroscler Rep. 2000;2(2):160–166. doi:10.1007/s11883-000-0111-3
33. Abujbara M, Batieha A, Khader Y, Jaddou H, El-Khateeb M, Ajlouni K. The prevalence of dyslipidemia among Jordanians. J Lipids. 2018;28(2018):6298739.
34. Tripathy JP, Thakur JS, Jeet G, et al. Burden and risk factors of dyslipidemia-results from a STEPS survey in Punjab India. Diabetes Metab Syndr. 2017;11(Suppl 1):S21–S27. doi:10.1016/j.dsx.2016.08.015
35. Huang C, Zhang WQ, Tang WW, et al. Prevalence and related factors of dyslipidemia among urban adults aged 35 to 79 years in Southwestern China. Sci Rep. 2021;11(1):17579. doi:10.1038/s41598-021-96864-w
36. Erem C, Hacihasanoglu A, Deger O, Kocak M, Topbas M. Prevalence of dyslipidemia and associated risk factors among Turkish adults: trabzon lipid study. Endocrine. 2008;34(1–3):36–51. doi:10.1007/s12020-008-9100-z
37. Malta DC, Szwarcwald CL, Machado IE, et al. Prevalence of altered total cholesterol and fractions in the Brazilian adult population: National Health Survey. Rev Bras Epidemiol. 2019;22(Suppl 02):E190005. Portuguese, English. doi:10.1590/1980-549720190005
38. Xi Y, Cao N, Bao H, et al. Prevalence of dyslipidemia and associated risk factors among adults aged ≥35 years in northern China: a cross-sectional study. BMC Public Health. 2020;20(1):1068. doi:10.1186/s12889-020-09172-9
39. Zhang FL, Xing YQ, Wu YH, et al. The prevalence, awareness, treatment, and control of dyslipidemia in northeast China: a population-based cross-sectional survey. Lipids Health Dis. 2017;16(1):61. doi:10.1186/s12944-017-0453-2
40. Liu C, Xue Y, Wang Y, et al. Association between dietary patterns and dyslipidemia in adults from the Henan Rural Cohort Study. Asia Pac J Clin Nutr. 2020;29(2):299–308. doi:10.6133/apjcn.202007_29(2).0013
41. Diarz J, Leyaro BJ, Kivuyo SL, et al. Red meat consumption and its association with hypertension and hyperlipidaemia among adult Maasai pastoralists of Ngorongoro Conservation Area, Tanzania. PLoS One. 2020;15(6):e0233777. doi:10.1371/journal.pone.0233777
42. Kjøllesdal M, Htet AS, Stigum H, et al. Consumption of fruits and vegetables and associations with risk factors for non-communicable diseases in the Yangon Region of Myanmar: a cross-sectional study. BMJ Open. 2016;6(8):e011649. doi:10.1136/bmjopen-2016-011649
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.