Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Outpatient Health Service Utilization Among Adults with Diabetes, Hypertension and Cardiovascular Disease During the COVID-19 Pandemic – Results of Population-Based Surveys in Germany from 2019 to 2021
Authors Du Y ![]() , Baumert J, Damerow S, Rommel A, Neuhauser H, Heidemann C
, Baumert J, Damerow S, Rommel A, Neuhauser H, Heidemann C
Received 21 October 2023
Accepted for publication 25 January 2024
Published 13 February 2024 Volume 2024:17 Pages 675—687
DOI https://doi.org/10.2147/JMDH.S445899
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Yong Du,1 Jens Baumert,1 Stefan Damerow,1 Alexander Rommel,1 Hannelore Neuhauser,1,2 Christin Heidemann1
1Department of Epidemiology and Health Monitoring, Robert Koch Institute, Berlin, Germany; 2German Centre for Cardiovascular Research (DZHK), Berlin, Germany
Correspondence: Yong Du, Department of Epidemiology and Health Monitoring, Robert Koch Institute, General-Pape-Str. 62-66, Berlin, D-12101, Germany, Tel +49-30-18754 3199, Fax +49 − 30-18754 3211, Email [email protected]
Purpose: Fear of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and lockdown measures may have an impact on health care utilization particularly for people with chronic diseases. We investigated changes in outpatient utilization behavior in pandemic phases among people with selected chronic diseases in Germany.
Methods: The nationwide population-based telephone surveys German Health Update (GEDA) 2019/2020 (April 2019 to September 2020) and GEDA 2021 (July to December 2021) covered 4 out of 7 pandemic phases from the pre-pandemic to the 4th pandemic wave. Data on hypertension, diabetes and major cardiovascular diseases (CVD) in the past 12 months and visiting a general practitioner (GP) or a specialist (excluding dentist) in the past 4 weeks was collected using a standardized questionnaire. Proportions and odds ratios were derived from logistic regression models adjusted for age, sex, education and federal states.
Results: Among 27,967 participants aged ≥ 16 years, 8,449, 2,497 and 1,136 individuals had hypertension, diabetes and major CVD. Participants with these chronic diseases visited a GP or specialist significantly more often than the overall study population, irrespective of pandemic phases. Compared to the pre-pandemic phase, a significant reduction in specialist-visiting was found in the first pandemic wave among people with hypertension (34.3% vs 24.1%), diabetes (39.5% vs 25.5%) and major CVD (41.9% vs 25.6%). GP-visiting was lower only among people with hypertension (53.0% vs 46.0%). No difference in GP or specialist visiting was found in the 4th pandemic wave compared to the pre-pandemic phase.
Conclusion: The observed decrease particularly in specialist utilization among people with the selected chronic diseases at the beginning of the pandemic was not observed for the second half of 2021 despite the ongoing pandemic. Further studies are required to examine whether the temporary changes in the utilization of ambulatory health care have affected the disease management of people with chronic diseases.
Keywords: health service utilization, outpatients, SARS-CoV-2, chronic disease, cardiometabolic diseases, diabetes, Germany
Introduction
The COVID-19 pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has impacted all sectors of society, especially healthcare systems. It not only posed a direct health threat to infected patients, but it also had a negative impact on people with chronic non-communicable diseases (NCDs).1–3 At the initial phase of the pandemic, strict contact restrictions, including social distancing, closure of public facilities, and stay-at-home orders among other measures, were implemented in many countries as part of the non-pharmaceutical measures to contain the spread of SARS-CoV-2. Further, clinical care and public health resources and capacities had to be reallocated with a shift from non-COVID-19 to COVID-19 patients given the unprecedented surge in COVID-19 cases. These measures impaired the accessibility of health services for people with NCDs. Furthermore, people with certain pre-existing NCDs,4 such as hypertension,5 heart disease,6 and diabetes,7–9 were found to be at increased risk for severe illness and death from COVID-19. Fear of being infected with SARS-CoV-2 may have discouraged at-risk individuals from using health care services, such as hospitals and out-patient facilities, where infected and non-infected people come together in close conditions.
Consequently, a considerable decrease in the utilization of health services including non-COVID-19 medical admissions, emergency department visits as well as outpatient visits has been observed in many countries at the earlier stage of the pandemic.1,10–14 For example, the number of visits to ambulatory care providers across all 50 states in the US had decreased by nearly 60% in April 2020.15 According to a rapid review of more than 500 studies concerning the early impact of COVID-19 on health service use, in-person outpatient care utilization fell by an average of 56% overall, with a range of 10% to 91%.14 The World Health Organization (WHO) global pulse survey on the continuity of essential health services indicated that health systems worldwide have still, ie more than two years after the outbreak, not recovered from the acute phase of the pandemic and that COVID-19 is still affecting essential health services in almost all countries.16
Chronic NCDs including cardiovascular diseases, cancer, diabetes and chronic respiratory diseases are the leading causes of death globally and together account for about 80% of mortality.17 Limited and disrupted accessibility to healthcare services may have compromised continuous medical care for disease management of these NCDs, raising concern about the long-term health impact and mortality of people with chronic diseases.18
Outpatient care provided by general practitioners (GPs) and specialists plays a critical role in the management of chronic diseases. Most previous studies examining the use of outpatient services focused on the period before and after the COVID-19 outbreak or before and after the implementation of containment measures in 2020.19,20 Our own previous studies found a significant decrease both in GP and specialist visits in the general population21 and a significant decrease in visits to specialists but not to GPs among people with known diabetes during the first wave of COVID-19 in 2020.22 However, the pandemic has gone through multiple phases worldwide. In Germany, during the first wave of COVID-19 (March 2 to May 17, 2020), the first lockdown was imposed on March 22, 202023 and was phased out in early May. During the second wave of COVID-19 (September 28, 2020 to February 28, 2021), a partial lockdown (lockdown light) was announced in early November 2020,24 followed by a stricter lockdown in early January 2021. In the third wave (February 29, 2021 to June 13, 2021), a strategy of mass rapid testing for COVID-19 and mandatory quarantine was pursued, while vaccination was initially offered to risk groups (such as older adults) and later to all adults. In the fourth wave (August 2, 2021 to December 26, 2021) and the fifth wave (December 27, 2021 to May 29, 2022), a nationwide campaign for mass vaccination and booster vaccination was promoted and a so-called 3G-rule was applied, according to which people who have been vaccinated (Geimpft), recovered (Genesen) or tested (Getestet) for infection had access to most public facilities.25,26 As the described phases of pandemic corresponded to different COVID-19 containment measures and prevention strategies, different effects on the use of healthcare services may have occurred. During the strict lockdown, when on-site outpatient visits were limited, a dramatic increase in telemedicine including telephone consultations and virtual visits has been observed.27–29 So far, few population-based studies have examined how healthcare utilization developed across different waves of the pandemic and if it returned to the pre-pandemic level in spite of the ongoing pandemic.30–32
Further, few previous studies differentiated between people with different chronic diseases when examining health service utilization.1 However, diabetes was one of the conditions reported to be most impacted by the reduction in healthcare resources.2 Hypertension is a key modifiable risk factor and the most common comorbidity of cardiovascular diseases. In addition, diabetes and hypertensive heart diseases belong to the ambulatory care sensitive conditions (ACSCs), for which effective and timely access to outpatient care can help to prevent complications and hospitalizations.33,34 Based on national survey data from Germany, 8.9% and 5.8% of adults reported the presence of a known diabetes mellitus and coronary heart disease in 2019/2020, respectively,35 and 31.8% had a physician-diagnosed hypertension in 2014/2015.36 Monitoring the use of outpatient services during the pandemic among people with these highly prevalent diseases helps to understand the lasting impact of the pandemic on health care and to inform health policymakers and stakeholders.
In the present study, we therefore aim to address the following questions: 1) How has the use of GP services (including telephone consultation) and specialist services developed among people with selected cardiometabolic diseases, namely hypertension, major cardiovascular diseases (CVD) and diabetes, across pandemic phases in Germany? 2) Did the use of outpatient services return to the pre-pandemic level and when did this occur? 3) Are there any differences in the development of outpatient service use between population subgroups?
Materials and Methods
Study Design
The included German Health Update (GEDA) studies are designed as nationwide cross-sectional telephone surveys aiming to provide information on the current health status of adults living in Germany. GEDA studies are conducted as part of health monitoring of the Robert Koch Institute (RKI) at multi-year intervals since 2008.37 GEDA 2019/2020, which incorporates the European Health Interview Survey (EHIS),38 was carried out between April 2019 and September 2020 among individuals aged ≥15 years with a permanent private household residency in Germany. The design and sampling methods of GEDA 2019/2020-EHIS have been described in detail elsewhere.39 Briefly, GEDA 2019/2020-EHIS used the established dual-frame method to generate random samples of telephone numbers at the national level, considering both landline and mobile phone numbers of all potentially reachable private households in Germany. The response rate (RR3) based on the standards of the American Association for Public Opinion Research (AAPOR) was 21.6%.39 With a similar study design and sampling procedure, GEDA 2021 was conducted as monthly cross-sectional samples between July 2021 and December 2021 among individuals aged ≥16 years (month-specific RR3 was between 17.6% and 22.5%, unpublished data40). Both GEDA 2019/2020-EIHS and GEDA 2021 were approved by the RKI’s Data Protection Officer and by the Ethics Committee of the Charité –Universitätsmedizin Berlin (application number EA2/070/19). Verbal informed consent was obtained from all the participants prior to the interview.
Study Population
A total of 23,001 individuals aged ≥15 years and 5,030 individuals aged ≥16 years participated in the GEDA 2019/2020-EHIS and GEDA 2021, respectively. For the present study, participants aged ≥16 years were included (22,937 in GEDA 2019/2020-EHIS and 5,030 in GEDA 2021, Table 1). On average, 1,165 (minimum: 394, maximum: 1,830) participants were interviewed each month.
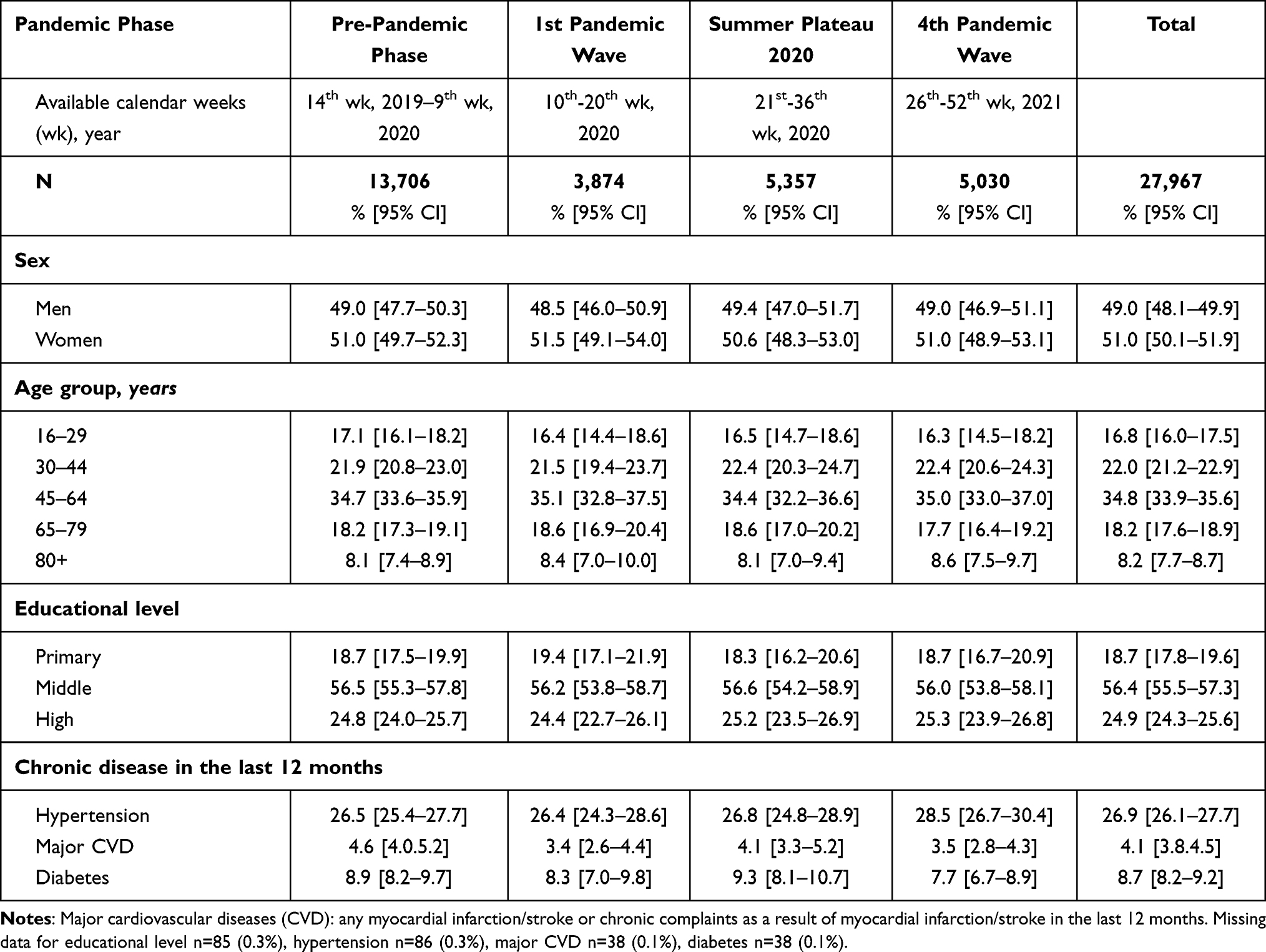 |
Table 1 Characteristics of the Study Population from the Nationwide Surveys GEDA 2019–2021 by Different Phases of the COVID-19 Pandemic in Germany |
Data Collection
Participants of GEDA 2019/2020-EHIS and GEDA 2021 were interviewed via structured computer-assisted telephone interviews (CATI). For both surveys GEDA 2019/2020-EHIS and GEDA 2021, a questionnaire was developed by RKI public health scientists.41 The telephone interviews were conducted by an external market and social research institute in Germany, USUMA GmbH, which specializes in collecting data via telephone interviews. The telephone interviews were carried out from Monday and Friday (from 8:30 a.m. to 9:00 p.m.) and on Saturday (from 10:00 a.m. to 3:00 p.m.) in a telephone studio, starting from mid-March 2020 in accordance with the applicable COVID-19 measures. Initial contact with potential interviewees usually took place between 2:30 p.m. and 9:00 p.m. On average, 4.3 calls were necessary to complete an interview, which took around 40 minutes. Throughout the survey process, employees from the RKI provided continuous supervision and comprehensive field monitoring.39
Definition of Indicators
Utilization of Outpatient Health Care Services
Participants were asked “How often have you consulted a general practitioner in the last 4 weeks for advice, an examination or treatment?”. This question was accompanied by the following note: “Please include visits to medical practices, home visits and consultations provided over the telephone”. Data on visits to a specialist was collected using an adapted version of the same question and was accompanied by the following note: “This does not include visits to a dentist or general practitioner”. The answers provided by the participants as number of physician contacts were used to create two dichotomous variables with regard to visiting a GP or a specialist in the last 4 weeks prior to the interview (yes/no).
Hypertension, Major CVD and Diabetes
Participants with selected chronic diseases, ie hypertension, major CVD, and diabetes in the last 12 months were identified using answers from the question “Have you had any of the following illnesses or complaints in the last 12 months?” both in GEDA 2019/2020-EHIS and GEDA 2021. For answering this question, a list of diseases and conditions was provided, which included hypertension, myocardial infarction (including chronic complaints as a result of myocardial infarction), stroke (including chronic complaints as a result of stroke), and diabetes (not including gestational diabetes). Those who answered with “yes” were classified as having hypertension, major CVD (ie myocardial infarction and/or stroke) and diabetes.
Pandemic Phase
The pandemic in Germany has been retrospectively divided into specific phases based on epidemiological parameters like COVID-19 positive rate, R-score, 7-day incidence and the proportion of severe respiratory illnesses with COVID-19 diagnosis in hospitals.26 Up to the end of 2021 these phases are defined as follows:
Phase 0: pre-pandemic (up to the 9th week of 2020, March 1, 2020);
Phase 1: the first wave of COVID-19 (10th–20th week of 2020, March 2–May 17, 2020);
Phase 2: summer plateau 2020 (21st–39th week of 2020, May 18–September 27, 2020);
Phase 3: the 2nd wave of COVID-19 (40th week of 2020–8th week of 2021, September 28, 2020–February 28, 2021);
Phase 4: the 3rd wave of COVID-19 (9th week of 2021–23rd week of 2021, February 29–June 13, 2021);
Phase 5: summer plateau 2021 (24th week of 2021–30th week of 2021, June 14–August 1, 2021);
Phase 6: the 4th wave of COVID-19 (31st week of 2021–51st week of 2021, August 2–December 26, 2021);
Phase 7: the 5th wave of COVID-19 (52nd week of 2021–21st week of 2022, December 27, 2021–May 29, 2022).
The interview dates of GEDA 2019/2020-EHIS participants (14th calendar week of 2019 to 36th calendar week of 2020) fall into the first 3 pandemic phases, ie phase 0–2, while the interview dates of GEDA 2021 participants (26th to 52nd calendar weeks 2021) fall largely into the phase 6, ie the 4th pandemic wave (including a small part of participants falling into phase 5 or phase 7).
Statistical Analysis
Statistical analyses were performed using Stata (version 17, StataCorp, U.S.). A weighting factor was used throughout the analysis, which considered design weights (selection probability for landlines and mobile phones) and corrected deviations of the distribution by sex, age, federal state and district type from the structure of the general population as of 31 December 2019 (for GEDA 2019/2020-EHIS) and of 31 December 2020 (for GEDA 2021) as well as the distribution by education level in the micro-census 2017 (for GEDA 2019/2020-EHIS) and 2018 (for GEDA 2021) according to the International Standard Classification of Education (ISCED).39 In the present study, we reported weighted percentages and unweighted absolute numbers.
Descriptive statistics were calculated to assess sample characteristics, overall, by pandemic phase, and by GP and specialist visits. Odds ratios (OR) and 95% confidence intervals (CI) were obtained from logistic regression models, which were fitted with use of health service, ie visiting a GP or a specialist in the last 4 weeks as dependent variable and pandemic phases as independent variable. Based on our previous analyses,21,22,32 we considered age, sex, educational level and federal states as covariables as they are closely associated with health service use and selected chronic diseases in Germany. For each logistic model, we additionally tested the interactions of the pandemic phase with age, sex and educational level and report significant interactions only. The models allow the estimation of adjusted proportions for the utilization of GP and specialists services.
The proportion of missing observations was overall very low (<1%). Among 27,967 individuals included in the present study, n = 89 (0.3%) and n = 133 (0.5%) had missing data for visiting a GP and a specialist, respectively. In addition, the numbers of participants with missing data on chronic disease or covariable were n = 86 (0.3%) for hypertension, n = 38 (0.1%) for major CVD and for diabetes, n = 85 (0.3%) for education (ISCED), and n = 47 (0.2%) for federal states. Due to the large sample size and the low proportions for missing observations, those with missing data were excluded from the descriptive analyses by pairwise deletion (ie any missing observations in the two variables) and from the multivariable analyses by listwise deletion (ie any missing observations in all variables).
To consider possible seasonal variation in the utilization of outpatient health services, eg low utilization due to summer vacations, we performed sensitivity analyses to compare identical seasonal periods in the pre-pandemic and pandemic phases: to examine the difference in health service utilization between phase 1 and the pre-pandemic, the pre-pandemic phase was redefined with the same calendar weeks as in phase 1 (week 14 to 20 of 2019 as the reference) and compared with available data from phase 1 (week 14 to 20 of 2020). Similarly, we redefined the pre-pandemic phase with the same calendar weeks as in phase 6 (week 26 to 52 of 2019 as the reference in comparison with week 26 to 52 of 2020).
Results
Table 1 shows the characteristics of the study sample. Of 27,967 individuals, 13,706, 3,874, 5,357 and 5,030 individuals were interviewed during the pre-pandemic phase, the first pandemic wave in 2020, the summer plateau in 2020, and the 4th pandemic wave in 2021, representing 49.0%, 13.9%, 19.2% and 18.0% of the study population, respectively. The mean age of the overall study population was 50.8 years; nearly half (49.0%) of them were male; and 26.9%, 4.1% and 8.7% reported hypertension, major CVD, and diabetes in the last 12 months, respectively. No differences in the distribution of sex, age group, educational level and the prevalence of selected chronic diseases were found across the sample subgroups for the different pandemic phases.
Table 2 shows GP and specialist visits in the past 4 weeks by sociodemographic variables and the selected chronic diseases. Overall, women visited a GP (37.8% vs 33.5%) and specialist (28.3% vs 21.1%) more often than men. Both GP and specialist visits increased along with age. The proportion of individuals who visited a GP rose from 27.1% among those under 30 years to 45.3% among those aged 80 years and over, while the proportion of individuals who visited a specialist rose accordingly from 17.4% to 26.9%. Individuals with a high educational level visited a GP less often, whereas they visited a specialist more often than individuals with a primary or middle educational level. Consistently, individuals with hypertension, diabetes and major CVD were more likely to visit a GP or a specialist than those without these conditions (Table 2).
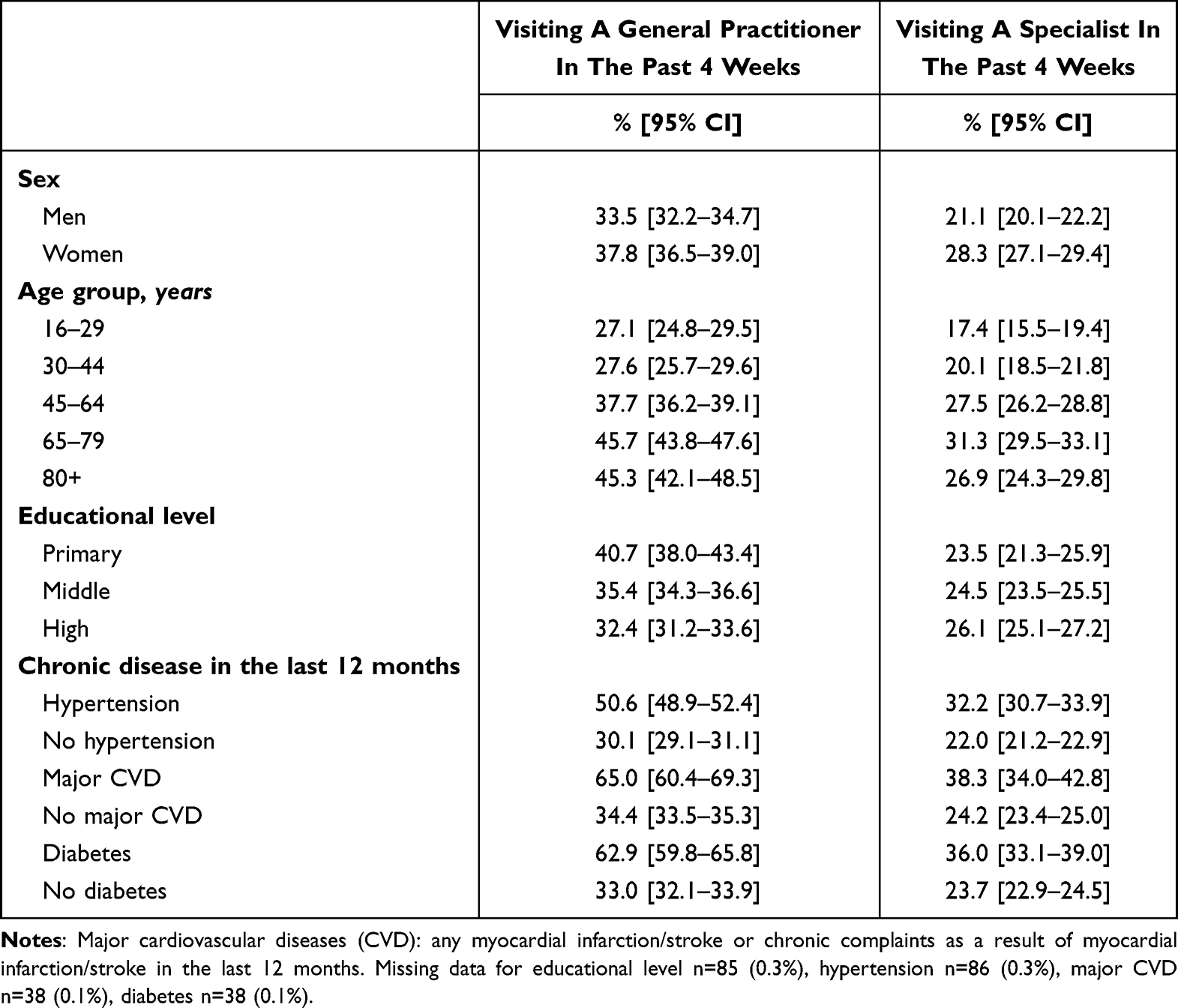 |
Table 2 Outpatient Health Service Utilization Among Adults by Sociodemographic Characteristics and Selected Chronic Diseases Based on the Nationwide Surveys GEDA 2019–2021 |
After adjustment for sex, age groups, educational level and federal states, individuals with hypertension, major CVD, and diabetes still visited a GP or specialist significantly more often than the general population irrespective of pandemic phases (Figure 1). Compared to the pre-pandemic phase, a significant reduction in specialist visits was found in the general population and among people with hypertension, major CVD and diabetes in the first pandemic wave, whereas GP visits were significantly lower in the general population and among people with hypertension, but not among people with major CVD (p = 0.053) or with diabetes (p = 0.634). While in the general population GP or specialist visits were still significantly lower during the summer plateau 2020, no such differences were found among people with the selected chronic diseases. In the 4th pandemic wave, no significant differences in GP or specialist visits were observed, overall or for people with the selected diseases (Table 3 and Figure 1).
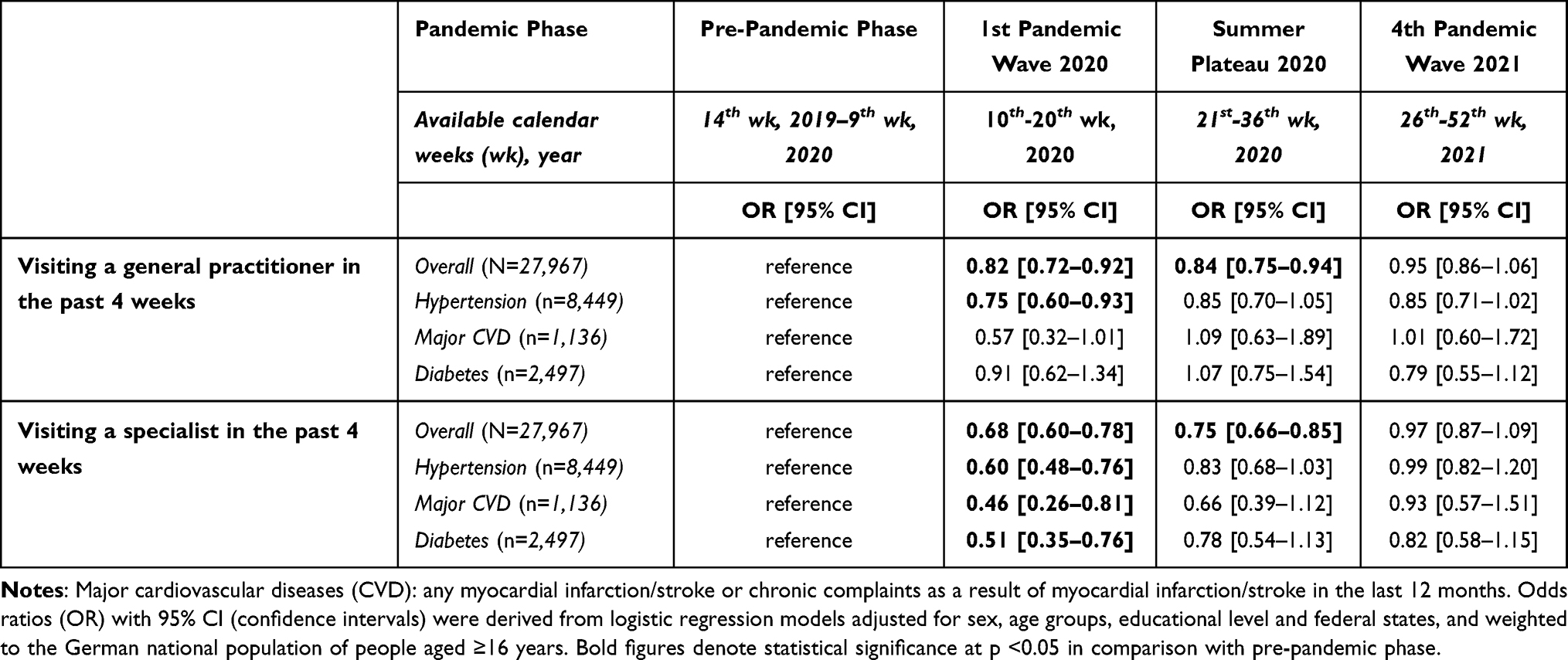 |
Table 3 Outpatient Health Service Utilization Among Adults Overall and Adults with Selected Chronic Diseases by Different Phases of the COVID-19 Pandemic in Germany Based on the Nationwide Surveys GEDA 2019–2021 |
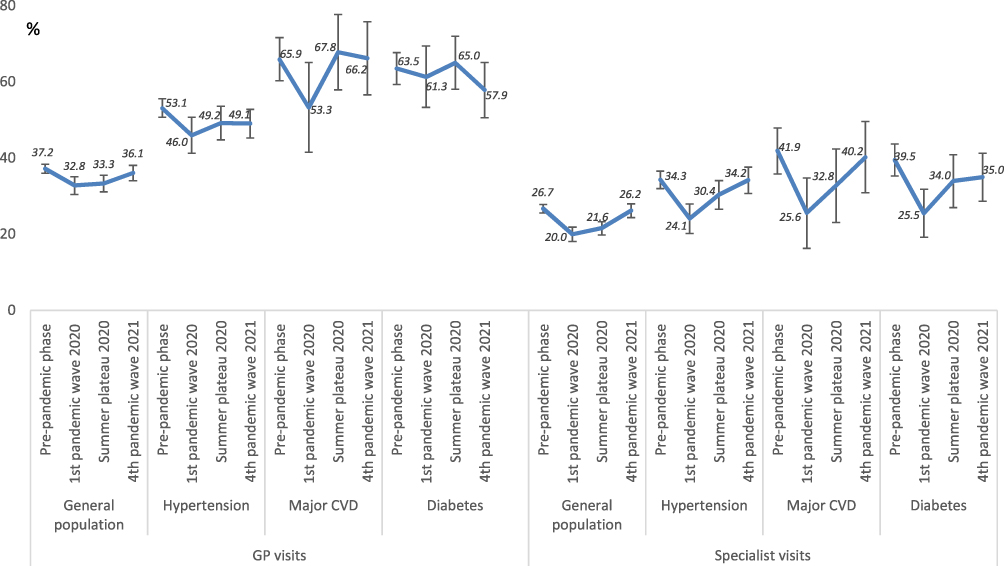 |
Figure 1 Outpatient health service utilization among adults overall and adults with selected chronic diseases by different phases of the COVID-19 pandemic in Germany based on the nationwide surveys GEDA 2019—2021. Notes: Percentages and 95% confidence intervals were adjusted for sex, age groups, educational level and federal states and weighted to the German national population of people aged ≥16 years. Major cardiovascular diseases (CVD): any myocardial infarction/stroke or chronic complaints as a result of myocardial infarction/stroke in the last 12 months. |
For GP visits, significant interactions were observed between pandemic phase and age for individuals with major CVD (p = 0.013) and diabetes (p = 0.022). Accordingly, further analysis revealed that in the first pandemic wave, elderly individuals with major CVD (30.4% vs 54.5% vs 61.1% for age group 80+ vs 65–79 vs <65 years) and diabetes (41.7% vs 59.8% vs 71.1% for age group 80+ vs 65–79 vs <65 years) visited a GP less often than younger ones. Significant interactions were also found between pandemic phase and sex for individuals with major CVD (p = 0.037) and between pandemic phase and educational level for those with diabetes (p = 0.030). Further analysis showed that in the 4th pandemic wave, women with major CVD visited a GP less often than men (56.2% vs.72.7%), and among individuals with diabetes, those with a low educational level were less likely to visit a GP than those with a high educational level (47.1% vs 59.1% vs 67.8% for low vs middle vs high educational level).
For specialist visits, a significant interaction between pandemic phase and education level was observed for individuals with major CVD (p = 0.038 for high vs low educational level in the first wave and p = 0.004 for middle vs low educational level in the 4th pandemic wave). While no difference was found by educational level with regard to specialist visits in the pre-pandemic phase (49.2% vs 37.1% vs 46.0% for low vs middle vs high educational level), educational differences were noted in the first wave (10.0% vs 25.8% vs 44.0%) and in the 4th pandemic wave (12.9% vs 49.6% vs 39.5%).
Sensitivity analyses using truncated identical seasonal periods in the pre-pandemic and pandemic phases revealed no changes in the statistical significance both in the general population and among people with the selected chronic diseases (data not shown).
Discussion
Main Findings
In this population-based study, we found that outpatient GP visits among people with hypertension and specialist visits among people with all of the selected chronic diseases declined considerably in the first wave of the pandemic compared with the pre-pandemic. While GP or specialist visits in the general population were still significantly lower in the summer plateau 2020 compared to the pre-pandemic phase, no difference in GP or specialist visits was found in the summer plateau 2020 among people with the selected chronic diseases. No difference was found for any group in the 4th pandemic wave compared to the pre-pandemic phase, suggesting that in spite of the ongoing pandemic at the end of 2021, outpatient GP and specialist visits had returned to the pre-pandemic level.
Comparison with Other Studies
It is not unexpected that the use of outpatient health care declined in the first pandemic wave in the general population and among people with selected chronic diseases. In March 2020, the German government in agreement with the federal states decided to implement comprehensive containment measures for infection control including strict contact restrictions and closure of most public facilities (the first lockdown).21,23 While visits to hospitals and doctor’s office were strictly limited, measures were taken to strengthen intensive care and ventilation capacities for COVID-19 patients, such as postponing planned procedures for non-COVID-19 patients.42 These measures were gradually phased out between the end of April 2020 and the end of October 2020, but were put in place again in November 2020 with essential public facilities remaining open (“slight” lockdown).21,24,43 The lockdown measures imposed during the first wave of the pandemic played a decisive role for the decline in utilization of outpatient health services and impaired also the accessibility of outpatient health care. In a population-based study conducted in four out of the most affected municipalities at the early pandemic stage in Germany showed that about one-third of the respondents gave up at least one of the health care services after the introduction of the containment measures.42 Cancellation of specialist check-ups (11.8%) was the second most frequently report after the cancellation of dental check-ups (15.2%), while cancellation of GP check-ups was less often (5.8%).42 Consistent with our findings, a substantial reduction in the number of consultations with GPs was found in a longitudinal observational study based on standardized interviews to GPs in the area around Hamburg.44 The mean number of GP consultations decreased by 49.0% from about 200 consultations per week in the time before the COVID-19 pandemic (defined as June 2015 to April 2017) to about 102 consultations per week during the first lockdown (defined as April to July 2020).44 In an analysis of more than 2 million patients aged 65 years and older who visited GPs and internal specialists or specialist practices in Germany, physician consultations were found to decrease slightly in February (−2%), increase in March (+9%), but decrease markedly during the first lockdown in April (−18%) and May (−14%) of 2020 compared with the same periods in 2019.20
The decline in the utilization of outpatient health care services was also observed universally with no clear patterns by income group or pandemic intensity.10,11 For example, the total number of outpatient visits decreased nationally by 9.4% in South Korea and by 40.5% in Mexico after the declaration of a pandemic by the WHO on 11 March 2020.10 In countries of the WHO South East Asia Region, health provision for cancers and cardiovascular diseases including outpatient services declined by more than 40% compared to the pre-pandemic period.11 In the US, outpatient office visits dropped dramatically after the outbreak of the pandemic, increased gradually after bottoming out in early of April 2020, but remained below pre-pandemic levels up to October 2020.45–47 In the last three months of 2020, outpatient visits remained fairly stable and did not differ from the baseline of March 1, 2020 despite the increase in COVID-19 cases according to data on visits to more than 50,000 providers across all 50 US states.15 Alike, in a cross-sectional study conducted in autumn 2020 in Lombardia (Italy), 22.4% of older adults decreased GP visits and 12.3% decreased outpatient visits, while 21.5% increased telephone contacts with the GPs compared to the year before.48 In a longitudinal study using data from a UK private health insurer, GP consultations and specialist consultations based on the frequency of claims per 1000 enrolled members decreased by 33.7% and 31.6%, respectively, in the COVID-19 year 2020 compared to the average of the years 2018 and 2019.19 A population-based retrospective cohort study of 3.8 million adults in Alberta, Canada, found that in-person outpatient visits for patients with cardiovascular ACSCs decreased by 38.9%, whereas their total outpatient visits increased by 4.1% in the first year of the pandemic after the introduction of virtual visits.27 In the present study, visiting a specialist decreased significantly in the first wave of the pandemic among the overall population as well as in people with hypertension, major CVD or diabetes, whereas visiting a GP declined in the overall population and among people with hypertension, but not among those with major CVD or diabetes. On the one hand, this difference may be partially due to the essential need for continuous care for chronic diseases, leading to less frequent cancellations of GP visits particularly among those with diabetes and major CVD. On the other hand, the difference may also be related to the wording in the questionnaire concerning GP and specialist visits. While the possibility of consultations provided over the telephone was mentioned in the explanation provided with the question for GP visits, it was not included in the explanation for specialist visits. Studies have shown that as in-person visits dropped, telemedicine including both telephone and video contacts increased sharply after the outbreak of the pandemic in the U.S.,28,29,45–47 Canada27 and in Italy.48 Similarly, it was observed in Germany based on data of Associations of Statutory Health Insurance Physicians (Kassenärztliche Vereinigungen) that telephone consultations increased by 69.0% in the period from March 1 to December 31, 2020 compared with the same period of the previous year.49 The decline in in-person visits was partially offset by the increase in telemedicine consultations; however, the rate of combined telemedicine and outpatient visits still declined during the early pandemic period.46,47 Although the decline returned to pre-pandemic levels for some subgroups,45 overall, there was still an about 10–30% decline in outpatient visits in the US up to June 2020 in spite of the increase of telemedicine.29,46,47
We found no difference in the utilization of outpatient health care service in the 4th pandemic wave in comparison with pre-pandemic phase, suggesting outpatient health care service returned to the level of the pre-pandemic period. This is supported by findings of a recent study conducted in March 2022 in Germany.30 The average number of GP and specialist visits was found to be 2.6 visits and 2.1 visits in the past 12 months, respectively. This was comparable to findings before the pandemic.30 Consistent with our findings, ACSC outpatient visit rates in a Canadian study decreased initially in “wave I” (March to May 2020) and then returned to the expected level in “Summer Lull 2020” (June to August 2020) and remained similar during “wave II” (September 2020 to March 2021).31
Interaction tests indicated that utilization of outpatient services partly differed within the groups with selected chronic conditions during the different pandemic phases, which may reflect differences in perceived risk of infection or of COVID-19 severity. For example, in the first pandemic wave, elderly individuals and particularly those with major CVD6 and diabetes8,9 were considered to be at higher risk of severe SARS-CoV2 infection; thus, they may have visited a GP less often than younger ones as observed based on the data of the present study. Further, the educational difference in specialist visits among individuals with major CVD, which was characterized by a decline in visits among the lower and middle educated in the first pandemic wave and by a persisting decline among the lower educated in the 4th pandemic wave compared to the pre-pandemic phase, suggests educational inequalities in outpatient care utilization during the pandemic waves. Furthermore, women with major CVD visited a GP less often than men in the 4th pandemic wave. Such potential gender and educational inequalities need to be further observed.
Strengths and Limitations
The major strength of our study is the use of nationwide population-based health survey data of adults in Germany and the large sample size. The telephone survey design was especially suitable during the pandemic. Weighted results can be generalized to the whole adult population in Germany.
However, this analysis has several limitations. First, the telephone interview survey – in spite of its strengths – has its limitations. For example, proficiency in the German language was a requirement for participation in the telephone interview, thus people with a limited knowledge of German may be underrepresented in the study population. Further, the low to moderate response rates may have resulted in a non-response bias. Although we used weights to account for differences in the distribution of demographic factors of the study sample compared to the general German adult population, a selection biased cannot be completely excluded. Thus, we cannot guarantee the full representativeness of the results. Second, data was based on self-reports, the collected information on healthcare utilization could therefore be subject to recall bias. However, as GP and specialist visits were examined for an observational window of the last 4 weeks prior to the interview, recall error should be small. Further, the number of GP and specialist visits was dichotomized (yes/no), which allows for certain degree of recall bias (either a single contact or eg 10 contacts with GPs and specialists will be treated as “yes”). Third, we investigated data of three selected self-reported chronic diseases, which could not be verified based on medical records. Data of other chronic NCDs such as cancers and respiratory diseases were not included. Fourth, GEDA 2019/2020-EHIS and GEDA 2021 covered only parts of the pandemic phases. Although GEDA 2019/2020-EHIS was continued with a shortened questionnaire from October 2020 to January 2021,32 data on chronic diseases was not collected in this extended period. Notably, our study did not cover the pandemic phases 4 and 5, so that it was not possible to examine health service utilization in the second and third pandemic wave in 2020 and 2021 or throughout all pandemic phases continuously. A previous study reflected that adults in Germany more frequently utilized health care services in December 2020 during the “light” second lockdown compared to March 2020 during the first lockdown, but less frequently compared to July 2020 during the summer plateau with only mild contact restrictions.50 Finally, regarding healthcare service use, we could only include visits to a GP and specialist while utilization of alternative sources of care such as telemedicine was not explicitly examined.
Conclusions
In spite of limitations, our analysis found that outpatient GP visits in people with hypertension and specialist visits in people with all selected chronic diseases declined considerably in the first pandemic wave, but returned to the pre-pandemic level at the second half of 2021. The less pronounced decrease of GP visits among people with major CVD or diabetes in the first pandemic wave may be explained at least partly by the need for continuous care for these diseases and the rise of telemedicine. Due to the observed temporary changes in the utilization of ambulatory health care, attention in healthcare practice should be paid to possible unfavorable developments in therapy goals and of long-term complications or secondary diseases of the selected diseases. Further studies with appropriate design are needed to confirm whether outpatients GP and specialist visits have remained at the pre-pandemic level through 2022 and afterwards and to understand whether changes in the ambulatory health care use have affected the disease management of chronic diseases and subsequent health outcomes including mortality.
Abbreviations
95% CI, 95% confidence interval; AAPOR, American Association for Public Opinion Research; ACSC, ambulatory care sensitive condition; CATI, computer-assisted telephone interviews; CVD, cardiovascular disease; EHIS, European Health Interview Survey; GEDA, German Health Update; GP, general practitioner; ISCED, International Standard Classification of Education; NCD, non-communicable disease; OR, odds ratio; RKI, Robert Koch-Institute; RR3, response rate 3; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; WHO, World Health Organization.
Data Sharing Statement
The dataset analysed for the current study is available from the corresponding author on reasonable request. The minimal data set underlying the findings presented in this manuscript is archived at the Health Monitoring Research Data Centre at the Robert Koch Institute (RKI) and can be accessed by all interested researchers. On-site access to the data set is possible at the Secure Data Center of the RKI’s Health Monitoring Research Data Centre. Requests should be submitted to [email protected].
Ethics Approval and Informed Consent
Both GEDA 2019/2020-EIHS and GEDA 2021 are subject to strict compliance with the data protection provisions set out in the EU General Data Protection Regulation (GDPR) and the Federal Data Protection Act (BDSG), and were approved by the Ethics Committee of the Charité –Universitätsmedizin Berlin (application number EA2/070/19) and performed in accordance with relevant guidelines and regulations including the Declaration of Helsinki. Participation in the study was voluntary. All participants were informed about the aims and contents of the study and about data protection. Verbal informed consent was obtained from all the participants prior to the interview, which was approved by the Ethics Committee of the Charité –Universitätsmedizin Berlin.
Acknowledgments
We thank all participants of the GEDA-study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by a research grant from the German Federal Ministry of Health to develop a diabetes surveillance system in Germany (Grant Numbers: 2522DIA700, 2523DIA002). The GEDA study was funded by the Robert Koch Institute and the Federal Ministry of Health, Germany. The Robert Koch Institute is a Federal Institute within the portfolio of the Federal Ministry of Health Germany.
Disclosure
The authors declare that they have no competing interests.
References
1. Seidu S, Kunutsor SK, Cos X, Khunti K. Indirect impact of the COVID-19 pandemic on hospitalisations for cardiometabolic conditions and their management: a systematic review. Prim Care Diabetes. 2021;15(4):653–681. doi:10.1016/j.pcd.2021.05.011
2. Chudasama YV, Gillies CL, Zaccardi F, et al. Impact of COVID-19 on routine care for chronic diseases: a global survey of views from healthcare professionals. Diabetes Metab Syndr. 2020;14(5):965–967. doi:10.1016/j.dsx.2020.06.042
3. Rosenbaum L. The untold toll - the pandemic’s effects on patients without Covid-19. N Engl J Med. 2020;382(24):2368–2371. doi:10.1056/NEJMms2009984
4. Rommel A, von der Lippe E, Treskova-Schwarzbach M, Scholz S. Population with an increased risk of severe COVID-19 in Germany. Analyses from GEDA 2019/2020-EHIS. J Health Monit. 2021;6(Suppl 2):2–15. doi:10.25646/7859
5. Zuin M, Rigatelli G, Zuliani G, Rigatelli A, Mazza A, Roncon L. Arterial hypertension and risk of death in patients with COVID-19 infection: systematic review and meta-analysis. J Infect. 2020;81(1):e84–e86. doi:10.1016/j.jinf.2020.03.059
6. Zuin M, Rigatelli G, Bilato C, Zanon F, Zuliani G, Roncon L. Pre-existing atrial fibrillation is associated with increased mortality in COVID-19 Patients. J Interv Card Electrophysiol. 2021;62(2):231–238. doi:10.1007/s10840-021-00992-2
7. Schlesinger S, Neuenschwander M, Lang A, et al. Risk phenotypes of diabetes and association with COVID-19 severity and death: a living systematic review and meta-analysis. Diabetologia. 2021;64(7):1480–1491. doi:10.1007/s00125-021-05458-8
8. Lim S, Bae JH, Kwon HS, Nauck MA. COVID-19 and diabetes mellitus: from pathophysiology to clinical management. review. Nat Rev Endocrinol. 2021;17(1):11–30. doi:10.1038/s41574-020-00435-4
9. Varikasuvu SR, Dutt N, Thangappazham B, Varshney S. Diabetes and COVID-19: a pooled analysis related to disease severity and mortality. Prim Care Diabetes. 2021;15(1):24–27. doi:10.1016/j.pcd.2020.08.015
10. Arsenault C, Gage A, Kim MK, et al. COVID-19 and resilience of healthcare systems in ten countries. Nat Med. 2022;28(6):1314–1324. doi:10.1038/s41591-022-01750-1
11. Gadsden T, Downey LE, Vilas VDR, Peiris D, Jan S. The impact of COVID-19 on essential health service provision for noncommunicable diseases in the South-East Asia region: a systematic review. Lancet Reg Health Southeast Asia. 2022;1:100010. doi:10.1016/j.lansea.2022.04.006
12. Moynihan R, Sanders S, Michaleff ZA, et al. Impact of COVID-19 pandemic on utilisation of healthcare services: a systematic review. BMJ Open. 2021;11(3):e045343. doi:10.1136/bmjopen-2020-045343
13. Roy CM, Brennan Bollman E, Carson LM, Northrop AJ, Jackson EF, Moresky RT. Assessing the indirect effects of COVID-19 on healthcare delivery, utilization and health outcomes: a scoping review. Eur J Public Health. 2021;31(3):634–640. doi:10.1093/eurpub/ckab047
14. Dupraz J, Le Pogam MA, Peytremann-Bridevaux I. Early impact of the COVID-19 pandemic on in-person outpatient care utilisation: a rapid review. BMJ Open. 2022;12(3):e056086. doi:10.1136/bmjopen-2021-056086
15. Mehrotra A, Chernew ME, Linetsky D, Hatch H, C M, Schneider EC. The impact of COVID-19 on outpatient visits in 2020: visits remained stable, despite a late surge in cases. Commonwealth Fund. 2024;25:1.doi:10.26099/bvhf-e411
16. WHO. Third round of the global pulse survey on continuity of essential health services during the COVID-19; 2022. Available from: https://iris.who.int/bitstream/handle/10665/351527/WHO-2019-nCoV-EHS-continuity-survey-2022.1-eng.pdf?sequence=1.
17. WHO. Noncommunicable Diseases: progress Monitor 2022;.2023. Available from: https://iris.who.int/bitstream/handle/10665/353048/9789240047761-eng.pdf;.
18. Kendzerska T, Zhu DT, Gershon AS, et al. The effects of the health system response to the COVID-19 Pandemic on chronic disease management: a narrative review. Risk Manag Healthc Policy. 2021;14:575–584. doi:10.2147/RMHP.S293471
19. Howarth A, Munro M, Theodorou A, Mills PR. Trends in healthcare utilisation during COVID-19: a longitudinal study from the UK. article. BMJ Open. 2021;11(7):e048151. doi:10.1136/bmjopen-2020-048151
20. Michalowsky B, Hoffmann W, Bohlken J, Kostev K. Effect of the COVID-19 lockdown on disease recognition and utilisation of healthcare services in the older population in Germany: a cross-sectional study. Age Ageing. 2021;50(2):317–325. doi:10.1093/ageing/afaa260
21. Damerow S, Rommel A, Prütz F, et al. Die gesundheitliche Lage in Deutschland in der Anfangsphase der COVID-19-Pandemie. Zeitliche Entwicklung ausgewählter Indikatoren der Studie GEDA 2019/2020-EHIS. J Health Monit. 2020;5(4):3–22. doi:10.25646/7171
22. Du Y, Baumert J, Damerow S, Rommel A, Scheidt-Nave C, Heidemann C. Utilisation of outpatient medical services by people with diagnosed diabetes during the COVID-19 pandemic in Germany. J Health Monit. 2021;6(2):51–58. doi:10.25646/8333
23. Erweiterung der beschlossenen Leitlinien zur Beschränkung sozialer Kontakte -Besprechung der Bundeskanzlerin mit den Regierungschefinnenund Regierungschefs der Länder vom 22.03.2020 [Extension of the adopted guidelines on the restriction of social contacts -Discussion between the Federal Chancellor and the heads of government of the federal states on 22.03.2020]; . Available from: https://www.bundesregierung.de/breg-de/themen/coronavirus/besprechung-der-bundeskanzlerin-mit-den-regierungschefinnen-und-regierungschefs-der-laender-vom-22-03-2020-1733248.
24. Bundesregierung. Der Beschluss von Bund und Ländern zur Bekämpfung der Corona-Pandemie [The decision by the federal and state governments to combat the coronavirus pandemic]; . Available from, https://www.bundesregierung.de/breg-de/aktuelles/bund-laender-beschluss-1805264.
25. Bundesgesundheitsministerium. Coronavirus-pandemie: was geschah wann? Chronik aller entwicklungen im kampf gegen COVID-19 (coronavirus sars-COV-2) UND der dazugehörigen maßnahmen des bundesgesundheitsministeriums [coronavirus pandemic: what happened and when? Chronicle of all developments in the fight against COVID-19 (coronavirus sars-cov-2) and the associated measures of the federal ministry of health]. 2021. Available from: https://www.bundesgesundheitsministerium.de/coronavirus/chronik-coronavirus.htm.
26. Tolksdorf K, Loenenbach A, Buda S. Dritte Aktualisierung der Retrospektiven Phaseneinteilung der COVID-19-Pandemie in Deutschland [The third update of the retrospective phasing of the COVID-19 pandemic in Germany]. Epid Bull. 2022;38:3–6. doi:10.25646/10598
27. McAlister FA, Hsu Z, Dong Y, Tsuyuki RT, van Walraven C, Bakal JA. Frequency and type of outpatient visits for patients with cardiovascular ambulatory-care sensitive conditions during the covid-19 pandemic and subsequent outcomes: a retrospective cohort study. J Am Heart Assoc. 2023;12(3):e027922. doi:10.1161/jaha.122.027922
28. Hays RD, Skootsky SA. Patient experience with in-person and telehealth visits before and during the COVID-19 pandemic at a large integrated health system in the United States. J Gen Intern Med. 2022;37(4):847–852. doi:10.1007/s11606-021-07196-4
29. Xu S, Glenn S, Sy L, et al. Impact of the COVID-19 pandemic on health care utilization in a large integrated health care system: retrospective cohort study. J Med Internet Res. 2021;23(4):e26558. doi:10.2196/26558
30. Hajek A, Konig HH. Determinants of Outpatient Physician Visits in the General Adult German Population during Later Stages of the COVID-19 pandemic. Healthcare. 2022;10(6). doi:10.3390/healthcare10061025
31. Kendzerska T, Zhu DT, Pugliese M, et al. Trends in all-cause mortality and inpatient and outpatient visits for ambulatory care sensitive conditions during the first year of the COVID-19 pandemic: a population-based study. J Hosp Med. 2022;17(9):726–737. doi:10.1002/jhm.12920
32. Damerow S, Rommel A, Beyer AK, et al. Health situation in Germany during the COVID-19 pandemic. developments over time for selected indicators of GEDA 2019/2020 - an update. J Health Monit. 2022;7(Suppl 3):2–19. doi:10.25646/9883
33. Sundmacher L, Fischbach D, Schuettig W, Naumann C, Augustin U, Faisst C. Which hospitalisations are ambulatory care-sensitive, to what degree, and how could the rates be reduced? Results of a group consensus study in Germany. Health Policy. 2015;119(11):1415–1423. doi:10.1016/j.healthpol.2015.08.007
34. World Health Organization. Regional Office for E. Assessing health services delivery performance with hospitalizations for ambulatory care sensitive conditions; 2016. Available from: https://apps.who.int/iris/handle/10665/348972.
35. Heidemann C, Scheidt-Nave C, Beyer AK, et al. Health situation of adults in Germany - results for selected indicators from GEDA 2019/2020-EHIS. J Health Monit. 2021;6(3):3–25. doi:10.25646/8459
36. Neuhauser H, Kuhnert R, Born S. 12-Month prevalence of hypertension in Germany. J Health Monit. 2017;2 1 :51–57 doi:10.17886/RKI-GBE-2017-016.
37. Lange C, Jentsch F, Allen J, et al. Data resource profile: German health update (GEDA)-the health interview survey for adults in Germany. Int J Epidemiol. 2015;44(2):442–450. doi:10.1093/ije/dyv067
38. Lange C, Finger JD, Allen J, et al. Implementation of the European health interview survey (EHIS) into the German health update (GEDA). Arch Public Health. 2017;75(1):40. doi:10.1186/s13690-017-0208-6
39. Allen J, Born S, Damerow S, et al. German health update (GEDA 2019/2020-EHIS) - background and methodology. J Health Monit. 2021;6(3):66–79. doi:10.25646/8559
40. Robert Koch-Institut. Gesundheit in Deutschland aktuell” (GEDA 2021); 2023. Available from: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Studien/Geda/Geda_2021_inhalt.html.
41. Robert Koch-Institut. Fragebogen zur Studie Gesundheit in Deutschland aktuell: GEDA 2019/2020-EHIS [Questionnaire for the German Health Update study: GEDA 2019/2020-EHIS]. J Health Monit. 2021;6(3):88–106. doi:10.25646/8560
42. Heidemann C, Reitzle L, Schmidt C, Fuchs J, Prutz F, Scheidt-Nave C. Non-utilisation of health care services during the COVID-19 pandemic: results of the CoMoLo study. J Health Monit. 2022;7(Suppl 1):2–17. doi:10.25646/9564
43. Mayr V, Nussbaumer-Streit B, Gartlehner G, Sroczynski G, Siebert U Quarantänemaßnahmen zur Eindämmung der COVID-19 Pandemie [Quarantine measures to contain the COVID-19 pandemic]. kompetenznetz public health COVID-19; 2021. https://www.public-health-covid19.de/images/2020/Ergebnisse/2020_05_29_Policy_Brief_Quarantine_SB_bn.pdf.
44. Schafer I, Hansen H, Menzel A, et al. The effect of COVID-19 pandemic and lockdown on consultation numbers, consultation reasons and performed services in primary care: results of a longitudinal observational study. BMC Fam Pract. 2021;22(1):125. doi:10.1186/s12875-021-01471-3
45. Qian L, Sy LS, Hong V, et al. Disparities in outpatient and telehealth visits during the COVID-19 pandemic in a large integrated health care organization: retrospective cohort study. J Med Internet Res. 2021;23(9):e29959. doi:10.2196/29959
46. Baum A, Kaboli PJ, Schwartz MD. Reduced in-person and increased telehealth outpatient visits during the COVID-19 pandemic. Ann Intern Med. 2021;174(1):129–131. doi:10.7326/M20-3026
47. Patel SY, Mehrotra A, Huskamp HA, Uscher-Pines L, Ganguli I, Barnett ML. Trends in outpatient care delivery and telemedicine during the COVID-19 pandemic in the US. JAMA Intern Med. 2021;181(3):388–391. doi:10.1001/jamainternmed.2020.5928
48. Vigezzi GP, Bertuccio P, Amerio A, et al. Older adults’ access to care during the COVID-19 pandemic: results from the lockdown and lifestyles (LOST) in lombardia project. article. Int J Environ Res Public Health. 2022;19(18):11271. doi:10.3390/ijerph191811271
49. Mangiapane S, Kretschmann J, Czihal T, von Stillfried D Veränderung der vertragsärztlichen Leistungsinanspruchnahme während der COVID-Krise- Tabellarischer Trendreport bis zum Ende des Jahres 2021 [Change in the use of services by SHI-accredited physicians during the COVID crisis -Tabular trend report up to the end of 2021]. Available from. https://www.zi.de/fileadmin/Downloads/Service/Publikationen/Zi-TrendReport_2021-Q4_2022-06-10.pdf.
50. Reitzle L, Schmidt C, Färber F, et al. perceived access to health care services and relevance of telemedicine during the COVID-19 pandemic in Germany. Int J Environ Res Public Health. 2021;18(14):7661. doi:10.3390/ijerph18147661
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Pharmaceutical Education on Medication Adherence and Its Clinical Efficacy in Patients with Type 2 Diabetes and Systemic Arterial Hypertension
Contreras-Vergara A, Sifuentes-Franco S, Haack S, Graciano-Machuca O, Rodriguez-Carrizalez AD, López-Contreras AK, Reyes-Pérez IV, Huerta-Olvera SG
Patient Preference and Adherence 2022, 16:1999-2007
Published Date: 5 August 2022
Pediatric Diabetes and Diabetic Ketoacidosis After COVID-19: Challenges Faced and Lessons Learnt
Agarwal A, Bansal D, Nallasamy K, Jayashree M, William V
Pediatric Health, Medicine and Therapeutics 2023, 14:281-288
Published Date: 4 September 2023
The Severity of the COVID-19 Among Chronic Disease Patients in the Selected Hospitals in Riyadh, Saudi Arabia – A Retrospective Study
Al-Rawi MBA, Khan AHI, Sheikh Ghadzi SM
Risk Management and Healthcare Policy 2024, 17:3327-3339
Published Date: 27 December 2024