Back to Journals » Patient Preference and Adherence » Volume 16
Impact of Pharmaceutical Education on Medication Adherence and Its Clinical Efficacy in Patients with Type 2 Diabetes and Systemic Arterial Hypertension
Authors Contreras-Vergara A, Sifuentes-Franco S, Haack S, Graciano-Machuca O, Rodriguez-Carrizalez AD, López-Contreras AK ![]() , Reyes-Pérez IV
, Reyes-Pérez IV ![]() , Huerta-Olvera SG
, Huerta-Olvera SG ![]()
Received 14 April 2022
Accepted for publication 22 July 2022
Published 5 August 2022 Volume 2022:16 Pages 1999—2007
DOI https://doi.org/10.2147/PPA.S370323
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Abelardo Contreras-Vergara,1,* Sonia Sifuentes-Franco,2,3,* Sally Haack,4 Omar Graciano-Machuca,2 Adolfo Daniel Rodriguez-Carrizalez,5 Ana Karen López-Contreras,1 Itzel Viridiana Reyes-Pérez,6 Selene G Huerta-Olvera1,7
1PhD in Pharmacology, Health Sciences University Center (CUCS), University of Guadalajara, Guadalajara, Jalisco, Mexico; 2Department of Health Sciences, Los Valles Campus (Cuvalles), University of Guadalajara, Ameca, Jalisco, Mexico; 3Department of Health Sciences - Disease as an Individual Process, Tonalá Campus, University of Guadalajara, Tonalá, Jalisco, Mexico; 4Drake University College of Pharmacy and Health Sciences, Des Moines, IA, USA; 5Department of Physiology, Health Sciences University Center, Institute of Clinical and Experimental Therapeutics, University of Guadalajara, Guadalajara, Jalisco, Mexico; 6Department of Molecular Biology and Genomics, Health Sciences University Center, University of Guadalajara, Guadalajara, Jalisco, Mexico; 7Medical and Life Sciences Department, La Ciénega University Center (CUCI), University of Guadalajara, Ocotlán, Jalisco, Mexico
*These authors contributed equally to this work
Correspondence: Selene G Huerta-Olvera, Medical and Life Sciences Department, La Ciénega University Center, University of Guadalajara, Ocotlán, Jalisco, 47810, Mexico, Tel +52 392 9259400, Email [email protected]
Purpose: To evaluate the impact of pharmaceutical education on medication adherence in patients with Type 2 Diabetes and Systemic Arterial Hypertension.
Patients and Methods: This randomized clinical trial enrolled patients with a diagnosis of Type 2 Diabetes Mellitus and Systemic Arterial Hypertension treated in an internal medicine outpatient clinic of a teaching hospital. One hundred and three patients were randomly assigned to the study groups; 51 to the control group and 52 to the intervention group with a 6 months follow-up. Medication adherence was assessed using the Morisky 8-item medication adherence scale. To improve patient adherence to treatment, a wallet card was provided with an up-to-date list of prescribed medications along with recommendations for follow-up care.
Results: One hundred and seventy-nine patients were screened for eligibility, of which 103 (57.5%) participated in the study. The intervention group showed a statistically significant decrease in capillary glucose levels, glycated hemoglobin, systolic and diastolic blood pressure, total cholesterol and triglycerides compared to the control group. The frequencies on medication adherence levels at 3 and 6 months in the control group remained similar to baseline, while in the intervention group the frequency of high adherence increased significantly at 6 months (8.7% to 43.5%).
Conclusion: A high percentage of patients are not achieving optimal control of their diabetes. Medication adherence rates were between 45– 50% in patients at the baseline of the study, but after receiving education and support from a pharmacist, the intervened group showed a significant increase in their adherence.
Keywords: adherence to treatment, chronic disease, health education, morisky medication adherence scale
Introduction
Chronic disease (CD) is defined by the World Health Organization as any disease of long duration, generally with slow progression and that is not transmitted from person to person.1 CD account for most deaths globally and are the leading contributors to disability, the development of serious complications, and high health care costs.2 The main types of CD are cardiovascular diseases, cancer, chronic respiratory diseases and diabetes.1 Type 2 diabetes is a complex chronic disease characterized by hyperglycemia, secondary to impairment in insulin secretory function and insulin resistance.3 Systemic arterial hypertension is a disease characterized by persistent high blood pressure. The American College of Cardiology (ACC) and American Heart Association (AHA) guidelines define hypertension as a systolic blood pressure of ≥130 mm Hg and/or a diastolic blood pressure of ≥80 mm Hg.4 Arterial hypertension and elevated fasting plasma glucose have been identified as the main risk factors for premature death and disability in the US and Latin America.5 Antihypertensive drugs, as well as oral hypoglycemic agents and insulin, are the mainstay in the treatment of patients with Type 2 Diabetes and Systemic arterial hypertension, coupled with a healthy diet and physical activity.6,7 The adequate treatment of patients with diabetes and/or hypertension is multifaceted. Despite the enormous benefit provided by pharmacotherapy, many patients have difficulty adhering to medication therapy which makes managing the conditions difficult.8 Adherence to treatment is the degree to which patients follow the agreed treatment recommendations prescribed by their physician.9 Approximately one in four people do not adhere to the prescribed medication10 and as such, poor adherence is considered a critical barrier to successful treatment and remains one of the main challenges for health professionals. Likewise, it has been shown that interventions through pharmaceutical education, patient counseling and other strategies, such as behavioral modification or mixed methodologies (education and behavioral changes), are favorable in improving adherence.11 Therefore, the involvement of a pharmacist, whose knowledge and skills enable them to provide pharmacotherapeutic support to patients and physicians, helps make drug therapy as efficient and safe as possible.12,14
There are different methodologies for measuring adherence to a medication regimen, among them some self-reported compliance questionnaires. The 8-item Morisky Medication Adherence Scale (MMAS-8), which classifies the degree of adherence and focuses on medication-taking behavior, has been reported to have acceptable validity and reliability in chronic conditions, especially in diabetes.15 The MMAS-8 is a test that evaluates adherence considering the reasons for omission of the medication by patients such as forgetfulness, carelessness in the schedule, suspending the medication when they feel better or starting to take the drug when they feel worse. It also includes additional elements that address the circumstances surrounding adherence behavior.15,16 There are other methods to evaluate adherence to treatment, such as the measurement of the concentrations of the drug or its metabolites in blood or urine. While they have good precision, they are also usually very expensive, which is why questionnaires such as MMAS-8 are widely used due to their ease, low cost and easy access in countries with low resources. Additionally, they have good sensitivity, specificity, high validity and reliability.17,18 This study aims to evaluate the impact of pharmaceutical education on therapeutic adherence in patients with Type 2 Diabetes Mellitus and Systemic Arterial Hypertension.
Materials and Methods
Patients and Study Design
This randomized, controlled clinical trial included a total of 103 patients with a diagnosis of type 2 diabetes mellitus and systemic arterial hypertension who attended the outpatient clinic of the O.P.D. Hospital Civil de Guadalajara “Dr. Juan I. Menchaca”. The patients were 18 to 60 years old and agreed to participate in the study by giving informed consent. Patients that were not prescribed pharmacological treatment for diabetes mellitus and systemic arterial hypertension (which was verified in the information presented in the clinical record of the Hospital), required hospitalization on the day of their appointment or with a limited literacy were excluded (Figure 1).
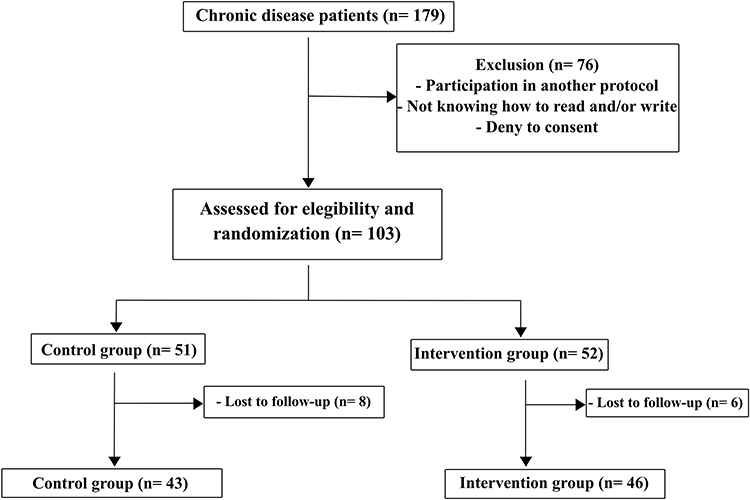 |
Figure 1 Diagram of patient screening. Participants were randomized 1:1. |
The patients were randomly assigned to the two study groups with evaluations occurring at 0, 3, and 6 months: the control group received regular (standard) education from their physician at each of their office visits, while the intervention group received regular education along with a pharmacist intervention on three occasions: baseline, at 3 and 6 months after the start of the study. The pharmacist spent between 20–25 minutes with each patient, who explained the main clinical characteristics and complications of these diseases, as well as, the importance of a healthy diet, exercise, adherence to medication and the usefulness of his treatment, all supported by a brochure. To improve medication adherence, patients were provided with a wallet card with an updated list of their prescription medications along with recommendations for follow-up care. Only one pharmacist, who had received previous training, participated from the beginning to the end of the study. For the evaluation of medication adherence, ©MMAS-8 was used. It is licensed: MMAR, LLC., Donald E. Morisky #6533-7069-1342-3041-5361.
Variables Analyzed
After randomization, patients were interviewed to obtain demographic data and medical history. Data collected were: time since disease diagnosis, number of prescribed medications, family support, and patient-reported cost of medications. In addition, glycated hemoglobin (Hb1Ac), fasting plasma glucose, cholesterol and triglyceride levels were collected.
Medication Adherence
Medication adherence was evaluated using the Morisky Medication Adherence Scale (MMAS-8),16 which is a validated instrument and generic scale used to assess medication adherence in patients with chronic diseases. The total score is calculated by adding the 8 items together (range 0–8). The final MMAS-8 value indicates the level of medication adherence, from high (8 points) to medium (6–7 points) to low (<6 points). In this research study, the medication adherence was evaluated in each patient with the medications that were individually prescribed.
Sample Size Calculation
A sample size calculation showed that 38 patients in each group would be sufficient to find a difference of 50% increase in treatment adherence. This calculation considers an alpha of 0.05 and a power of 0.80 of the Test, along with a 20% loss to follow-up. The calculation was performed with the expected proportion formula.
Statistical Analysis
We reported categorical variables as frequencies and percentages and analyzed them by χ2 or Fisher’s exact tests, as appropriate. Quantitative variables were presented as means and standard deviations. We used the Wilcoxon test for intragroup comparisons (baseline vs final data in each group). Mann–Whitney U-test was used for comparisons between the control group vs the intervention group. Considering two-tailed statistically significant p-value <0.05. Both R and SPSS version 24.0 Chicago II were used for all analyses.
Ethical Considerations
The study was conducted in agreement with guidelines as stipulated by the Declaration of Helsinki, 64th General Assembly in Fortaleza, Brazil in October 2013. It was approved by the Ethics Committee of the O.P.D. Nuevo Hospital Civil De Guadalajara “Dr. Juan I. Menchaca” (09/HCJIM-JAL/2019). This was recorded in ClinicalTrials.gov (NCT05202067). Patients were invited and informed consent forms were obtained and signed voluntarily. Patient confidentiality was maintained at all times.
Results
One hundred seventy-nine patients with type 2 diabetes and systemic arterial hypertension were screened for eligibility. Seventy-six patients were not eligible for the study for different reasons: they participated at the same time in another clinical study, had low literacy levels, or declined the invitation to participate. Of the 103 patients eligible for the study, they were randomly assigned to two study groups: 51 patients to the control group and 52 patients to the intervention group (Figure 1).
Demographic Measures
As shown in Table 1, there were no statistically significant differences in demographic characteristics between the two groups at baseline. The majority of study participants were women (60.5% in the control group versus 61.5% in the intervention group; p = 0.570). The mean age of the patients in the control group was 55.8 ± 3.6 years versus 56.6 ± 2.3 years in the intervention group (p = 0.481). The duration of diabetes was similar in both groups, presenting as a mean of 8.16 ± 2.7 years in the control group versus 7.65 ± 2.7 years in the intervention group. The same was observed for the duration of hypertension, group control with 8.53 ± 2.5 years and the intervention group with 8.92 ± 2.3 years.
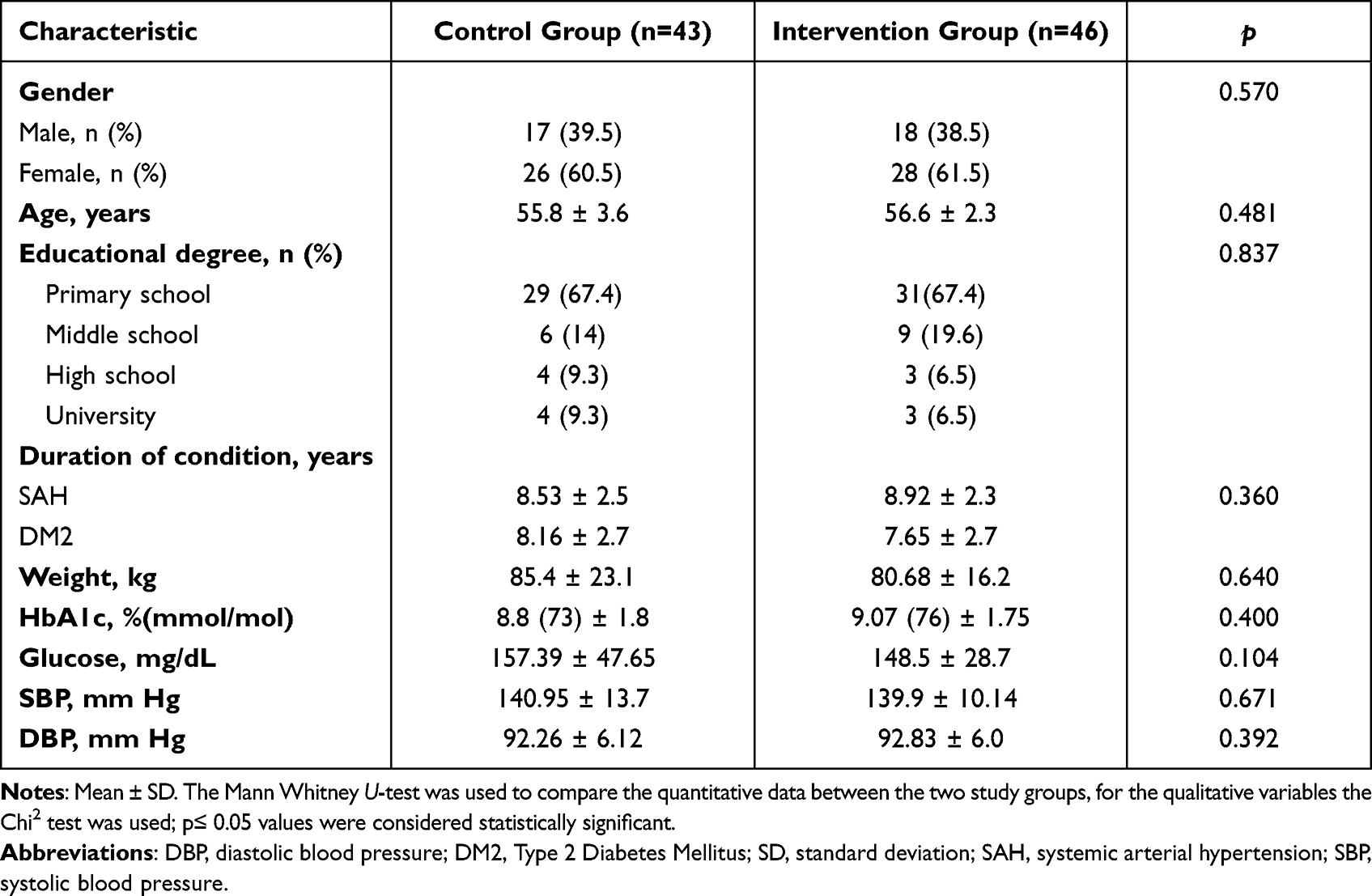 |
Table 1 Demographic Characteristics |
Regarding educational degree, most of the study participants only had primary school education (67.4% in the control group and 67.4% in the intervention group) with no significant differences in the distribution in both groups (p = 0.837).
Likewise, at baseline, no significant differences were observed between the study groups in the treatment effectiveness parameters. The glucose levels were 157.39 ± 47.65 mg/dL (control) and 148.5 ± 28.7 mg/dL (intervention) (p = 0.104) and Hb1Ac levels were 8.8% (73 mmol/mol) ± 1.8% (control) and 9.07% (76 mmol/mol) ± 1.75% (intervention) (p = 0.400). The control group patients presented a systolic blood pressure/diastolic blood pressure of 140.95 ± 13.7/92.26 ± 6.12 mm Hg versus the intervention group with 139.9 ± 10.14/92.83 ± 6.0 mm Hg (p =0.671/0.392).
Medication Adherence
As shown in Table 2, at baseline, both groups had a high percentage of patients with low adherence to treatment, 51.2% in the control group and 47.8% in the intervention group. The comparison between both groups did not show a significant difference, which indicates that the homogeneity of the groups (p= 0.931). After 6 months of follow-up this proportion changed significantly in the intervention group. There number of patients reaching the highest category of medication adherence increased from 8.7% (baseline) to 43.5% at the conclusion of the study.
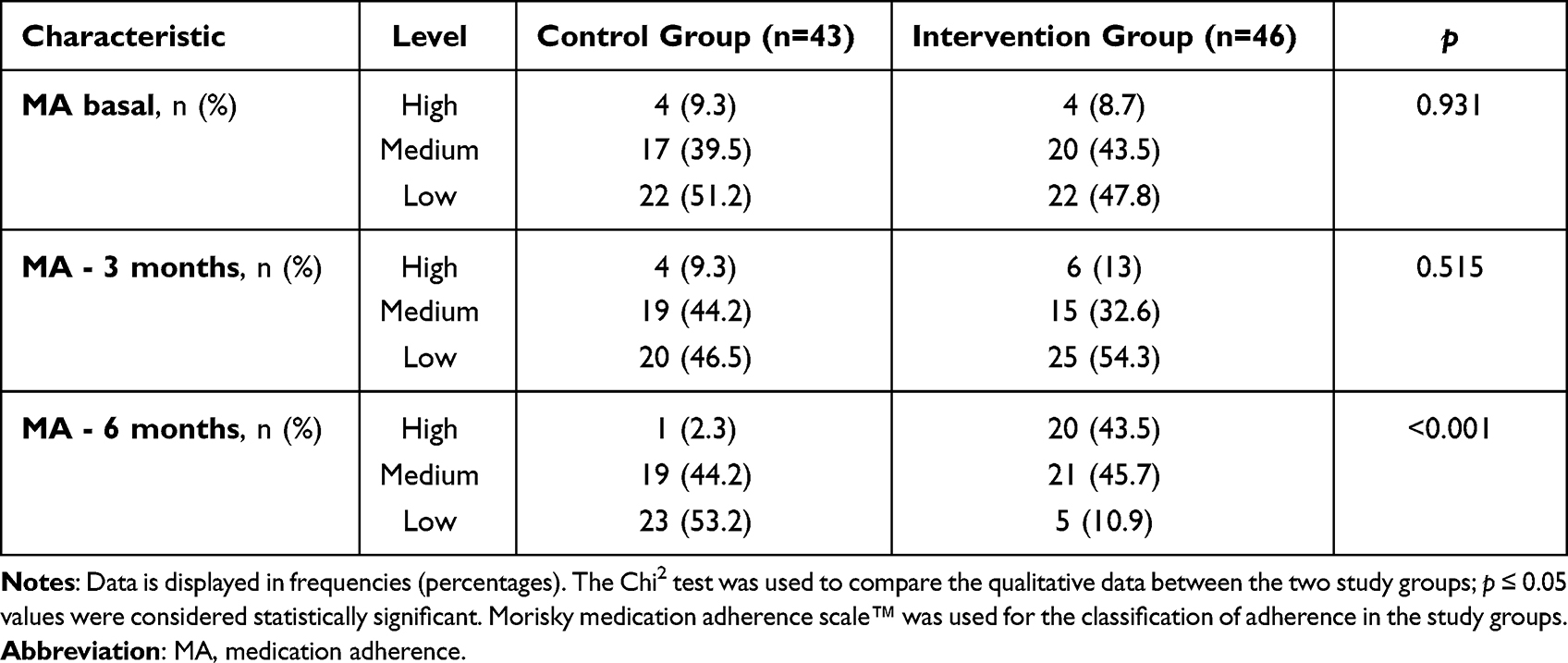 |
Table 2 Therapeutic Adherence of the Study Participants |
Therapeutic adherence resulted in positive changes in the clinical markers as well (see Table 3). The glycemic values showed a significant improvement (p˂0.001) in the intervention group after 6 months of follow-up. On the other hand, the control group showed no difference in the baseline comparison versus 6 months of follow-up (p = 0.194). The total cholesterol and triglyceride levels resulted in significant changes in both study groups, while the systolic and diastolic blood pressures only showed improvement in the intervention group.
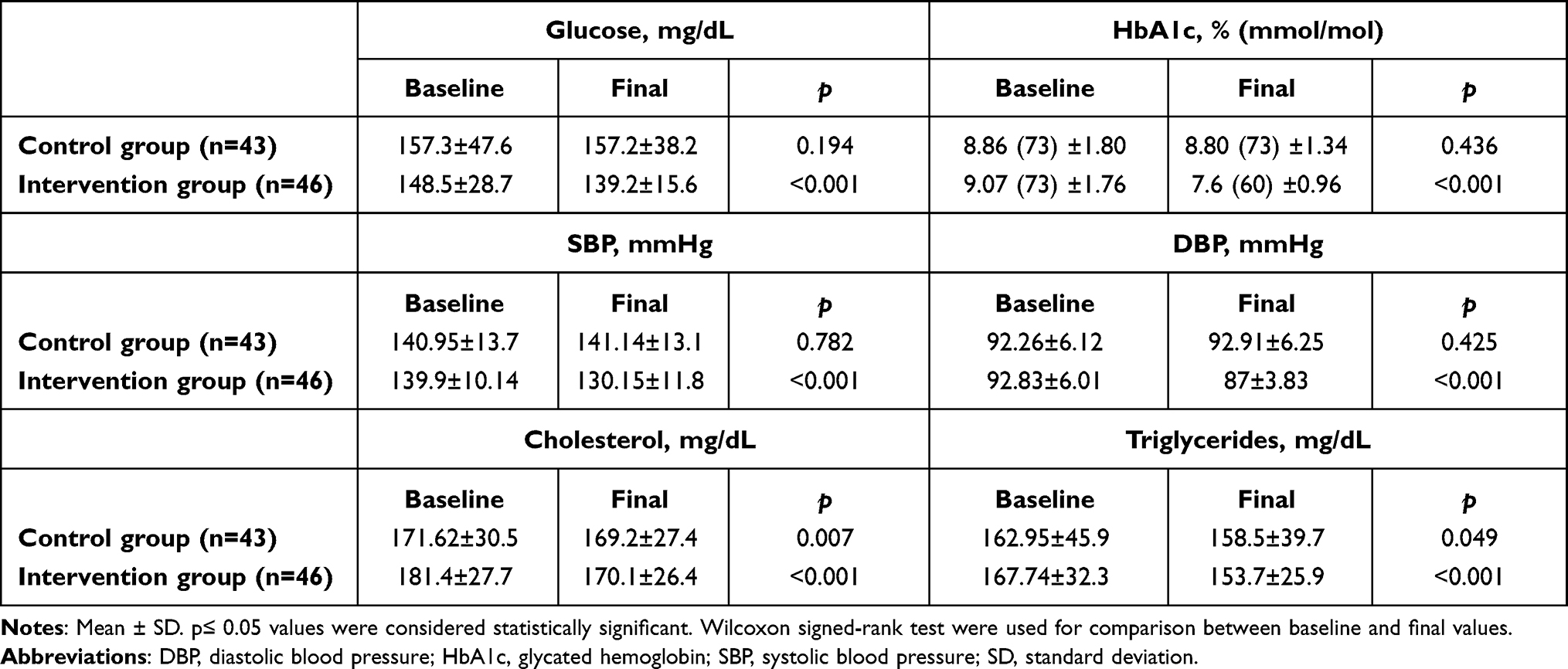 |
Table 3 Baseline and Final Values of Clinical Characteristics |
The average value MMAS-8 score at baseline for the control group was 4.9 ± 1.9 and for the intervention group was 4.5 ± 2.1 (p = 0.562). After the 6-month follow-up, a statistically significant improvement (p ˂ 0.001) in the score could be observed in the intervention group, achieving a value of 7.04 ± 1.4. The control group did not experience this same effect, with no statistically significant changes from baseline to 6-month follow-up. (Table 4). Sensitivity and specificity for diabetes control were calculated. MMAS-8 sensitivity of 79.1% and specificity of 35.4% were obtained, therefore the positive predictive value was 31.2% and the negative predictive value was 82.2%. Considering the distribution of patients with good control those with Hb1Ac ˂7% and inadequate control those with Hb1Ac ≥7%, adherence was also established for those who were at a high and medium level and poor adherence for those who presented low on the MMAS-8 scale. The sensitivity and specificity results for the scale based on hypertension control were 76.4% and 44.2%, respectively. The positive predictive value was 68.9% compared to the negative predictive value, which was 53.6% (Table 5).
 |
Table 4 Comparison of Adherence to Treatment Baseline Vs Final |
 |
Table 5 Relationship Between HbA1c %, Blood Pressure and Adherence Levels |
Discussion
CD has gained great importance due to the alarming increased prevalence in several countries, especially diabetes and hypertension. It is estimated that it will become a serious public health problem in the coming decades, including a significant economic impact on society.17,19 It is well known that non-adherence to medication is a relevant issue in medical care and that this has been associated with the inability to achieve optimal health outcomes.20,21 The treatment of CD commonly includes the long-term use of pharmacological treatment and despite the efficacy of pharmacologic options, the benefits are not consistently realized since it is estimated that approximately 50% of patients do not take their medications as prescribed.23 In this study, adherence to treatment and the efficacy of the intervention were evaluated through pharmaceutical education in patients with type 2 diabetes and systemic arterial hypertension who were receiving pharmacological treatment. We obtained similar results to those previously described, finding 49.5% of the patients at baseline had low adherence to the prescribed medication regimen.22
The main factors that contributed to the low adherence found in our study population were related to forgetfulness, modification of the medication schedule, lack of understanding of the chronic nature of therapy. These findings are similar to that described by other authors.19 Consequently, interventions that can help improve therapeutic adherence contribute not only to improving patient health education, but also to achieving better clinical results. In our population, it was found that after the pharmacist-delivered intervention, 43.5% presented high adherence to treatment. Under baseline conditions, both groups showed similar levels of medication adherence (p=0.931); this study demonstrated patient education delivered by a pharmacist can significantly increase medication adherence in patients with type 2 diabetes and hypertension compared to usual care.
Among the relevant findings, we found that patients belonging to the pharmacy intervention group showed a better understanding of the importance of taking their medications, which was reflected in the increase in their adherence. Having an increased percentage of patients with the highest level of medication adherence agrees with previous studies carried out in patients with type 2 diabetes. Despite the fact that the authors mentioned a suboptimal result, medication adherence improves the efficacy of the medication, obtaining beneficial results for patients.24
Poor adherence to medications has been reported in patients with chronic diseases. A study of patients with diabetes revealed that almost 60% were not adherent to hypoglycemic medications.25 A separate study showed that only 59% of patients with diabetes, hypertension and dyslipidemia had an MPR> 80% (medication possession ratio).26 Meanwhile, a systematic review and meta-analysis revealed that around 45% of patients with hypertension and a third (31.2%) of patients with hypertension and other comorbidities do not comply with their medication. Even a higher proportion of patients who have uncontrolled hypertension also have challenges with appropriate medication adherence (83.7%).27
The probability that patients adhere to their treatment is 1.76 times better if they have higher health literacy. This study showed there was a positive and significant correlation between health literacy and patient adherence. Therefore, it is understood that those patients with higher levels of health literacy are more adherent to their prescribed treatment. Those patients with higher levels of health literacy have been found to have adherence rates that are on average 14% higher than those with lower literacy.28 In this same sense, many elderly patients have a low literacy rate which increases the risk of non-adherence in a vulnerable patient population.
Our study concluded that patients who received pharmacist-delivered education significantly increased their medication adherence compared to the control group. We attribute this positive change in adherence to the knowledge and confidence that the patient obtained from the health education provided by a pharmacist. This type of education translates into an improvement in the self-management of their medication regimen and results in improved clinical outcomes.29 Additionally, an improvement in medication adherence has been shown through pharmacist-delivered interventions in other conditions as well.30
We observed a significant improvement in the following clinical variables in the intervention group at the end of the 6-month follow-up: glycated hemoglobin, fasting plasma glucose, SBP, DBP, triglycerides and cholesterol. Our results are consistent with other studies where an improvement in SBP control is observed 6 months after the intervention31 and significant reductions of glycated hemoglobin, SBP, and DBP after 12 months of evaluation.32
In this same sense, a study reported that greater adherence leads to a greater improvement in glycosylated hemoglobin regardless of hypoglycemic treatment in patients with type 2 diabetes.33 A systematic review also indicated that more than 90% of the included studies on pharmacist-led interventions for the management of type 2 diabetes demonstrated a greater reduction in glycosylated hemoglobin levels in the intervention group compared to the control group.34
The degree of medication adherence was measured using the MMAS-8, a survey instrument with high reliability and validity and frequently used to assess the level of medication adherence for chronic disease management.16 After six months of follow-up, more patients in the intervention group experience with high medication adherence compared to the control group. We also found a statistically significant decrease in the percentage of patients with low adherence in the intervention group at the conclusion of the study period.
The clinical variables also showed statistically significant improvements, specifically the plasma glucose levels decreased significantly in the intervention group, similar to the measurements of blood pressure, and glycosylated hemoglobin. Data were consistent with that of a study,35 where the effect of education on diabetes self-control was evaluated.
The obtained values of sensitivity for diabetes and hypertension were adequate (79.1% and 76.4%). Comparatively the specificity, which was low (35.4% and 44.2%), can lead to a high proportion of false positives for the applicability of this questionnaire. Our data are consistent with the results of other researchers.36–38 It is difficult to measure the exact causes medication non-adherence, since they can be based on the patient’s own individual circumstances. It is important to mention that this type of survey instrument carries a potential risk of response bias, since it is self-reported by the patient. It should be noted that more sensitive and specific methods such as direct measurements are currently available to evaluate medication adherence, but the most important advantage of this questionnaire is its low cost and easy applicability.16
This is one of the first studies in Mexico that demonstrated the positive impact that pharmacists can have on improving medication adherence in patients with type 2 diabetes and hypertension. By advancing the professional role of clinical pharmacists in Mexico and fully welcoming them into the interprofessional healthcare team, more patients will be able to self-manage their chronic diseases and, in turn, lead to beneficial health outcomes.
Limitations of this study include a 6-month follow-up duration. Although the trial was initially designed with a longer duration follow-up (9–12 months), however, the COVID-19 pandemic impacted the study. The high demand for COVID-related patient care at the hospital site where the clinical trial took place led to complications with patient enrollment, however new trials with longer follow-up could provide better adherence results.
Conclusion
It was found that pharmacist-delivered education improved the proportion of patients with high or medium adherence to the treatment of type 2 diabetes and hypertension. The evaluation of the efficacy of the intervention is determined with the improvement in variables such as glycemia, HbA1c, SBP and DBP, for which our results contribute to the support that medication adherence is a very important objective for the prognosis of the patient with chronic disease. This highlights the need for patient-centered medical care to include pharmacist-delivered educational and counseling strategies.
Acknowledgements
We are grateful for the facilities and support granted for this study by the physicians, students and nurses of the internal medicine outpatient area of this hospital.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. World Health organization. Noncommunicable diseases progress monitor 2020. Available from: https://www.who.int/publications/i/item/9789240000490.
2. Chronic Disease Center (NCCDPHP). CDC. Available from: https://www.cdc.gov/chronicdisease/index.htm.
3. Schmidt AM. Highlighting Diabetes Mellitus: the Epidemic Continues. Arterioscler Thromb Vasc Biol. 2018;38:e1–e8. doi:10.1161/ATVBAHA.117.310221
4. Whelton PK. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: executive Summary: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:1269–1324. doi:10.1161/HYP.0000000000000066
5. GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioral, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1345–1422. doi:10.1016/S0140-6736(17)32366-8
6. Ram CV. Antihypertensive drugs: an overview. Am j Cardiovascular Drugs. 2002;2(2):77–89. doi:10.2165/00129784-200202020-00002
7. Pearson ER. Type 2 diabetes: a multifaceted disease. Diabetologia. 2019;62(7):1107–1112. doi:10.1007/s00125-019-4909-y
8. Cramer JA. A systematic review of adherence with medications for diabetes. Diabetes Care. 2004;27(5):1218–1224. doi:10.2337/diacare.27.5.1218
9. Fernandez-Lazaro CI. Adherence to treatment and related factors among patients with chronic conditions in primary care: a cross-sectional study. BMC Fam Pract. 2019;20(1):132. doi:10.1186/s12875-019-1019-3
10. DiMatteo MR. Variations in patients’ adherence to medical recommendations: a quantitative review of 50 years of research. Med Care. 2004;42(3):200–209. doi:10.1097/01.mlr.0000114908.90348.f9
11. Lam WY, Fresco P. Medication Adherence Measures: an Overview. Biomed Res Int. 2015;2015:217047. doi:10.1155/2015/217047
12. Van Wijk BL, Klungel OH, Heerdink ER, de Boer A. Effectiveness of interventions by community pharmacists to improve patient adherence to chronic medication: a systematic review. Ann Pharmacother. 2005;39(2):319–328. doi:10.1345/aph.1E027
13. Readdean KC, Heuer AJ, Scott Parrott J. Effect of pharmacist intervention on improving antidepressant medication adherence and depression symptomology: a systematic review and meta-analysis. Res Social Adm Pharm. 2018;14(4):321–331. doi:10.1016/j.sapharm.2017.05.008
14. World Health organization. Adherence to long-term therapies: evidence for action/[edited by Eduardo Sabaté]. Available from: https://apps.who.int/iris/handle/10665/42682.
15. Tan X, Patel I, Chang J. Review of the four item Morisky Medication Adherence Scale (MMAS-4) and eight item Morisky Medication Adherence Scale (MMAS-8). Inov Pharm. 2014;5;87.
16. Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10(5):348–354.
17. Azharuddin M, Adil M, Sharma M, Gyawali B. A systematic review and meta-analysis of non-adherence to anti-diabetic medication: evidence from low- and middle-income countries. Int J Clin Pract. 2021;75(11):e14717. doi:10.1111/ijcp.14717
18. Culig J, Leppée M. From Morisky to Hill-bone; self-reports scales for measuring adherence to medication. Coll Antropol. 2014;38(1):55–62.
19. Chen L, Magliano DJ, Zimmet PZ. The worldwide epidemiology of type 2 diabetes mellitus–present and future perspectives. Nat Rev Endocrinol. 2008;8(4):228–236. doi:10.1038/nrendo.2011.183
20. Smith KB, Smith MS. Obesity Statistics. Prim Care. 2016;43(1):121–ix. doi:10.1016/j.pop.2015.10.001
21. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clinic Proce. 2011;86(4):304–314. doi:10.4065/mcp.2010.0575
22. Winkler A, Teuscher AU, Mueller B, Diem P. Monotoring adherence to prescribed medication in type 2 diabetic patients treated with sulfonylureas. Swiss Med Wkly. 2002;132(27):379–385.
23. Peeters B, Van Tongelen I, Boussery K, Mehuys E, Remon JP, Wilems S. Factors associated with medication adherence to oral hypoglycemic agents in different ethnic groups: a systematic literature review and suggestions for further research. Diabet Med. 2011;28:262–275. doi:10.1111/j.1464-5491.2010.03133.x
24. Miller TA. Health literacy and adherence to medical treatment in chronic and acute illness: a meta-analysis. Patient Educ Couns. 2016;99(7):1079–1086. doi:10.1016/j.pec.2016.01.020
25. Sefah IA, Okotah A, Afriyie DK, Amponsah SK. Adherence to Oral Hypoglycemic Drugs among Type 2 Diabetic Patients in a Resource-Poor Setting. Int j Applied Basic Med Res. 2020;10:102–109.
26. Bermeo-Cabrera J, Almeda-Valdes P, Riofrios-Palacios J, Aguilar-Salinas CA, Mehta R. Insulin Adherence in Type 2 Diabetes in Mexico: behaviors and Barriers. J Diabetes Res. 2018;2018:3190849. doi:10.1155/2018/3190849
27. Polonsky WH, Henry RR. Poor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributors. Patient Prefer Adherence. 2016;10:1299–1307. doi:10.2147/PPA.S106821
28. Abegaz TM, Shehab A, Gebreyohannes EA, et al. Nonadherence to antihypertensive drugs: a systematic review and meta-analysis. Medicine. 2017;96(4):e5641. doi:10.1097/MD.0000000000005641
29. Miller TA. Health literacy and adherence to medical treatment in chronic and acute illness: a meta-analysis. Patient Educ Couns. 2016;99(7):1079–1086.
30. Michiels Y, Bugnon O, Chicoye A, et al. Impact of a Community Pharmacist-Delivered Information Program on the Follow-up of Type-2 Diabetic Patients: a Cluster Randomized Controlled Study. Adv Ther. 2019;36:1291–1303. doi:10.1007/s12325-019-00957-y
31. Abdulsalim S, Unnikrishnan MK, Manu MK, et al. Structured pharmacist-led intervention programme to improve medication adherence in COPD patients: a randomized controlled study. Res Soc Admin Pharmacy. 2018;14:909–914. doi:10.1016/j.sapharm.2017.10.008
32. Anderegg MD, et al. Pharmacist Intervention for Blood Pressure Control in Patients with Diabetes and/or Chronic Kidney Disease HHS Public Access. Pharmacotherapy. 2018;38:309–318. doi:10.1002/phar.2083
33. Al Mazroui NR, Kamal MM, Ghabash NM, et al. Influence of pharmaceutical care on health outcomes in patients with Type 2 diabetes mellitus. Br J Clin Pharmacol. 2009;67(5):547–557. doi:10.1111/j.1365-2125.2009.03391.x
34. Patel S, Abreu M, Tumyan A, et al. Effect of medication adherence on clinical outcomes in type 2 diabetes: analysis of the SIMPLE study. BMJ Open Diabetes Res Care. 2019;7(1):e000761. doi:10.1136/bmjdrc-2019-000761
35. Pousinho S, Morgado M, Falcão A, Alves G. Pharmacist Interventions in the Management of Type 2 Diabetes Mellitus: a Systematic Review of Randomized Controlled Trials. J Managed Care Specialty Pharmacy. 2016;22:493–515. doi:10.18553/jmcp.2016.22.5.493
36. De Oliveira-Filho AD, Morisky DE, Neves SJ, Costa FA. The 8-item Morisky Medication Adherence Scale: validation of a Brazilian-Portuguese version in hypertensive adults. Res Social Adm Pharm. 2014;10(3):554–561. doi:10.1016/j.sapharm.2013.10.006
37. Martinez-Perez P, Orozco-Beltrán D, Pomares-Gomez F, et al. Validation and psychometric properties of the 8-item Morisky Medication Adherence Scale (MMAS-8) in type 2 diabetes patients in Spain. Aten Primaria. 2021;53(2):101942. doi:10.1016/j.aprim.2020.09.007
38. Ji H, Chen R, Huang Y, et al. Effect of simulation education and case management on glycemic control in type 2 diabetes. Diabetes Metab Res Rev. 2019;35:548. doi:10.1002/dmrr.3112
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Outpatient Health Service Utilization Among Adults with Diabetes, Hypertension and Cardiovascular Disease During the COVID-19 Pandemic – Results of Population-Based Surveys in Germany from 2019 to 2021
Du Y, Baumert J, Damerow S, Rommel A, Neuhauser H, Heidemann C
Journal of Multidisciplinary Healthcare 2024, 17:675-687
Published Date: 13 February 2024
The Severity of the COVID-19 Among Chronic Disease Patients in the Selected Hospitals in Riyadh, Saudi Arabia – A Retrospective Study
Al-Rawi MBA, Khan AHI, Sheikh Ghadzi SM
Risk Management and Healthcare Policy 2024, 17:3327-3339
Published Date: 27 December 2024