Back to Journals » International Journal of Women's Health » Volume 18
Nursing Interventions for Symptom Management in Breast Cancer: A Systematic Review
Authors Trisyani Y ![]() , Nuraeni A
, Nuraeni A ![]() , Anna A
, Anna A ![]() , Priambodo AP
, Priambodo AP ![]() , Sugiharto F
, Sugiharto F ![]()
Received 10 October 2025
Accepted for publication 23 January 2026
Published 4 February 2026 Volume 2026:18 573338
DOI https://doi.org/10.2147/IJWH.S573338
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Yanny Trisyani,1 Aan Nuraeni,1 Anastasia Anna,1 Ayu Prawesti Priambodo,1 Firman Sugiharto2
1Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Doctoral Program, Faculty of Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Yanny Trisyani, Department of Critical Care and Emergency Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia, Fax +620227795596, Email [email protected]
Background: Breast cancer (BC) is among the most common types of cancer among women globally, with a significant impact on both physical and psychological health. The treatment for BC, including chemotherapy, radiotherapy, and hormonal therapy, frequently results in symptoms including pain, fatigue, anxiety, depression, and sleep disturbances. These symptoms can markedly diminish patients’ quality of life and overall well-being.
Purpose: This review aimed to identify the effectiveness of nursing interventions for symptom management in patients with breast cancer.
Methods: A systematic review was conducted by searching four electronic databases (PubMed, EBSCOhost, ScienceDirect, and SAGE Journals) for studies published between 2002 and 2025. Randomised controlled trials (RCTs) evaluating nursing interventions for symptom management in patients with breast cancer were included. The search strategy used keywords related to breast cancer, symptom management, and nursing interventions.
Results: 18 studies involving 3,937 patients met the inclusion criteria. The interventions were categorised into three domains: psychological and behavioural interventions, nursing care coordination, and physical and educational interventions. Nursing interventions contributed to the alleviation of both physical and psychological symptoms, thereby improving overall patient well-being and QoL.
Conclusion: Nursing interventions are essential for managing symptoms in breast cancer patients and improving both physical and psychological well-being. This review demonstrates the effectiveness of various interventions in alleviating common symptoms, including pain, fatigue, and emotional distress. Psychologically focused interventions and coordinated nurse-led care consistently showed the most substantial benefits in improving symptom management and overall quality of life. Future research should refine and validate these interventions to ensure their applicability in diverse clinical settings. Comprehensive, patient-centred nursing interventions are vital for optimising care and QoL in this population.
Keywords: breast cancer, nursing intervention, symptom management, quality of life
Introduction
Breast cancer (BC) is one of the most common malignancies among women worldwide. In 2020, an estimated 2.26 million women were living with breast cancer globally.1 In 2020, breast cancer deaths numbered 685,000, making it the second most common cause of cancer-related death among women.2 The global burden of breast cancer continues to increase, especially in low and middle-income countries, where late diagnosis and limited access to treatment contribute significantly to high mortality rates.
The majority of BC patients require comprehensive therapy such as chemotherapy, radiotherapy, or hormonal therapy, which is given according to each individual’s pathology.3 Chemotherapy plays an essential role in the treatment of breast cancer. However, its long-term effects are often associated with a reduced quality of life (QoL) and increased psychological distress.1,4 BC patients who experience psychological distress more frequently report fatigue, pain, and sleep disturbances.5 Previous research involving 733 patients with breast cancer found that the five most frequently reported physical symptoms were pain, nausea, fatigue, limb swelling, and sleep disturbances.6
The various symptoms, both physical and psychological, affect changes in the patient’s QoL.7 The more severe the symptoms experienced, the more severe the decline in body function and the patient’s QoL. Therefore, efforts to reduce and manage symptoms are the primary goals of rehabilitation in BC patients.8 Comprehensive symptom management in breast cancer patients is essential, as it not only enhances QoL but may also play a crucial role in enhancing long-term survival outcomes.8 To achieve this, it is necessary to involve a process of managing physical, emotional, and social needs, both with medication therapy, lifestyle modifications, and supportive care.
In this case, nurses must act as a reliable source of information to facilitate continuity of care (CoC) and provide psychosocial support for BC patients and their families throughout every phase of the care continuum, including the diagnostic process, treatment, rehabilitation, follow-up, and palliative care.9 Nurses must act as advocates, educators, coordinators, and counsellors for patients and families, where each nurse’s role can differ depending on their clinical competence and service/care model.9 Therefore, strengthening nurses’ competencies in communication, emotional support, and patient education is essential to ensure comprehensive and holistic breast cancer care.
Although numerous studies have explored nursing interventions for symptom management in breast cancer patients, there remains considerable variability in the approaches, types of interventions, outcome measures, and findings reported across studies. Several reviews have been conducted such as symptom clusters in breast cancer patients receiving adjuvant chemotherapy,10 focus only on telehealth interventions,11 and their focus is on managing lymphedema after breast cancer.12 In contrast, this review comprehensively synthesizes the latest evidence on nursing interventions, approaches, and outcomes in managing symptoms in breast cancer patients. This review is expected to strengthen evidence-based nursing practice and facilitate the implementation of effective and cutting-edge interventions that improve the quality of care and patient survival.
Materials and Methods
Study Design
This study used a systematic review design to evaluate interventions for managing symptoms in patients with BC. This systematic review was compiled in accordance with the Cochrane Handbook for Systematic Reviews of Interventions, and the article selection process was reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Eligibility Criteria
The PICOS framework, comprising Population, Intervention, Comparator, Outcome, and Study Design, is used to structure the research question systematically. This study population (P) focuses on breast cancer patients, without any restrictions regarding the disease stage (whether early-stage or metastatic), patient age, type of ongoing anticancer treatment, or prior treatment history. This approach aims to provide a comprehensive understanding of the various patient characteristics that may influence the effectiveness of the nursing interventions. The interventions (I) examined encompass a range of nursing approaches designed to manage symptoms, addressing both physical and psychological symptoms. The comparator (C) is the usual or standard care typically provided to breast cancer patients, allowing an assessment of whether nursing interventions have a greater impact than conventional care. The outcomes (O) include notable changes in patients’ health status, such as improvements in quality of life, reductions in anxiety and depression, increased self-efficacy, pain management, and alleviation of other symptoms commonly experienced by breast cancer patients. Only Randomised Controlled Trials (RCTs) will be included as study design (S), as they provide the most substantial evidence for assessing intervention effectiveness.
The inclusion criteria for this review consist of articles discussing nursing interventions for symptom management in breast cancer patients, in full-text format, with an RCT design, and published in English. Articles involving secondary research, those not accessible, or those published in languages other than English will be excluded to ensure consistency and high-quality data for analysis.
Search Strategy
The literature search was conducted by three independent reviewers (AN, APP, and FS). The database search was conducted from January 2002 to March 2025, and only articles published in English were included to ensure linguistic consistency and accessibility. The identification of articles was conducted systematically through four central databases: PubMed, EBSCOhost, ScienceDirect, and SAGE Journals. The keywords used in the search process included:
(Breast Neoplasms”[Mesh] OR breast cancer OR breast neoplasms OR breast tumor*) AND (symptom management OR symptom control OR symptom relief) AND (nursing OR nurs* OR “nursing intervention*” OR “nurse-led”) AND (intervention* OR strateg* OR “best practice*” OR therap* OR program* OR management) AND (randomized controlled trial[Publication Type] OR random* OR trial)
Boolean operators “AND” and “OR” were applied to narrow or expand the search strategy, ensuring comprehensive retrieval of relevant studies across multiple databases.
Study Selection and Quality Appraisal
The studies were independently reviewed by three individuals (AN, APP, and FS) following established criteria to determine their suitability. Mendeley Reference Manager was used to find and remove any duplicate records. Using predetermined inclusion and exclusion criteria, the titles, summaries, and the entire content of the texts were checked to determine their relevance. The Joanna Briggs Institute (JBI) critical appraisal checklist was used to assess the quality of the chosen papers. The PRISMA flow diagram (Figure 1) summarizes the selection process.
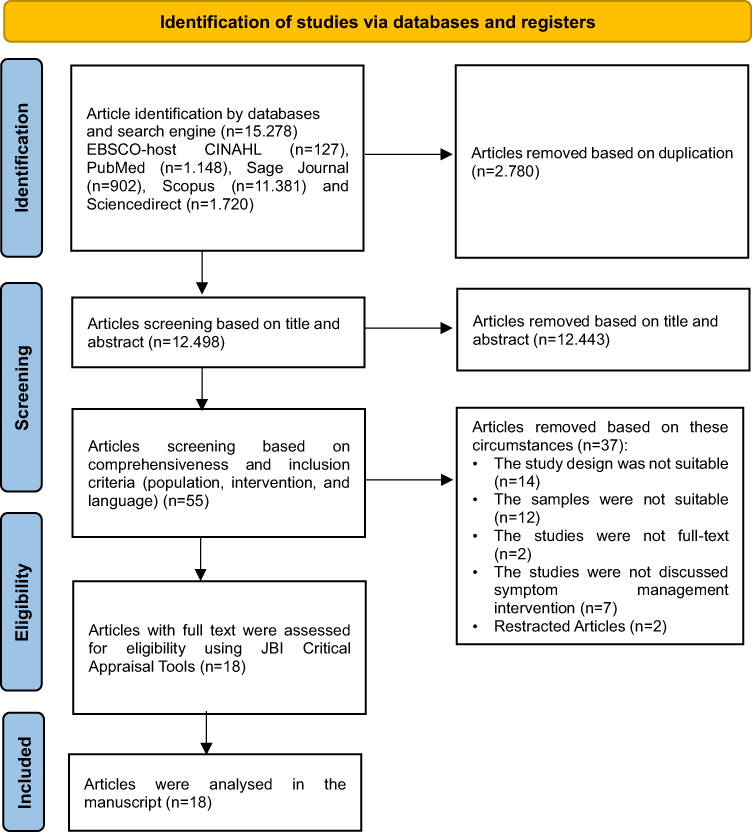 |
Figure 1 PRISMA Flowchart. |
To assess quality, studies using randomized controlled trials (RCTs) were examined using a checklist of 13 criteria. Each item had four potential answers: Yes, No, Not Applicable, and Unclear. For each “Yes” answer, a score of 1 was given, but all other answers received a score of 0. Studies that scored below 75% on the Joanna Briggs Institute (JBI) overall score were not considered for this analysis. The authors discussed any differences in the appraisal results as a group until they reached agreement. However, there were no disagreements about whether to include the chosen articles. If there were differences, two reviewers (YT and AA) worked together to make a final decision on whether to include a study following discussion.
Data Extraction and Analysis
In this systematic review, information from the selected studies was comprehensively gathered and arranged in summary tables that emphasized the main findings aligned with the research aims. Data extraction was carried out independently by two reviewers (FS and AN). The extraction matrices contained critical details, including the study design, participant characteristics, and the components of the intervention. Subsequently, a thematic analysis using an exploratory descriptive framework was applied. This procedure involved classifying and presenting the extracted information in tables for each study, followed by in-depth interpretation and synthesis of the results. To maintain precision and reduce possible extraction discrepancies, all included studies underwent a meticulous final verification by the research team.
Given that this review is a systematic review without meta-analysis, a thematic and narrative synthesis approach was adopted to ensure an appropriate and rigorous integration of findings across heterogeneous studies. A thematic analysis was applied to all included studies to systematically identify recurring patterns, similarities, and distinctions among nursing interventions and reported outcomes. Studies were first examined in detail to extract key characteristics, including intervention components, delivery methods, and targeted symptom outcomes. Interventions that shared conceptual foundations, mechanisms of action, or aligned nursing philosophies were then grouped into a single thematic domain. Through an iterative comparison process, three overarching domains emerged: psychological and behavioural interventions, nursing care coordination, and physical and educational interventions. Within each domain, outcomes were compared narratively by examining the direction, consistency, and significance of effects across studies, rather than relying on pooled statistical estimates. This structured thematic framework enabled a transparent and reproducible synthesis of evidence, allowing meaningful comparison across diverse interventions while appropriately accounting for clinical and methodological heterogeneity.
Results
Study Selection
The database search identified a total of 15,278 records from five electronic sources, including PubMed, Scopus, ScienceDirect, SAGE Journals, and CINAHL via EBSCOhost. After the removal of 2,780 duplicate records, 12,498 articles remained and were screened based on titles and abstracts (Figure 1). Of these, 12,443 records were excluded for not meeting the predefined inclusion criteria, resulting in 55 articles assessed for full-text eligibility. Following comprehensive evaluation using the Joanna Briggs Institute (JBI) critical appraisal tools, 37 articles were excluded due to unsuitable study design, inappropriate samples, lack of full-text availability, irrelevance to symptom management interventions, or retraction. Ultimately, 18 randomized controlled trials met the inclusion criteria and were included in the final synthesis.
Quality Appraisal Results
Most of the reviewed studies demonstrated high methodological rigor, with the majority of quality scores meeting or closely approaching the standards established by the Joanna Briggs Institute (JBI) (Table 1). Several studies exhibited strong adherence to essential methodological domains, including randomization, concealed allocation, appropriate statistical analyses, and homogeneity across treatment groups. Nevertheless, a few studies had methodological limitations, particularly the lack of participant or provider blinding and insufficient clarity regarding the implementation of certain criteria. Overall, the methodological quality was robust, with most studies meeting approximately 10 of 13 JBI criteria. In contrast, six of the top-tier studies met all JBI quality indicators, underscoring the overall strength and credibility of the included evidence.
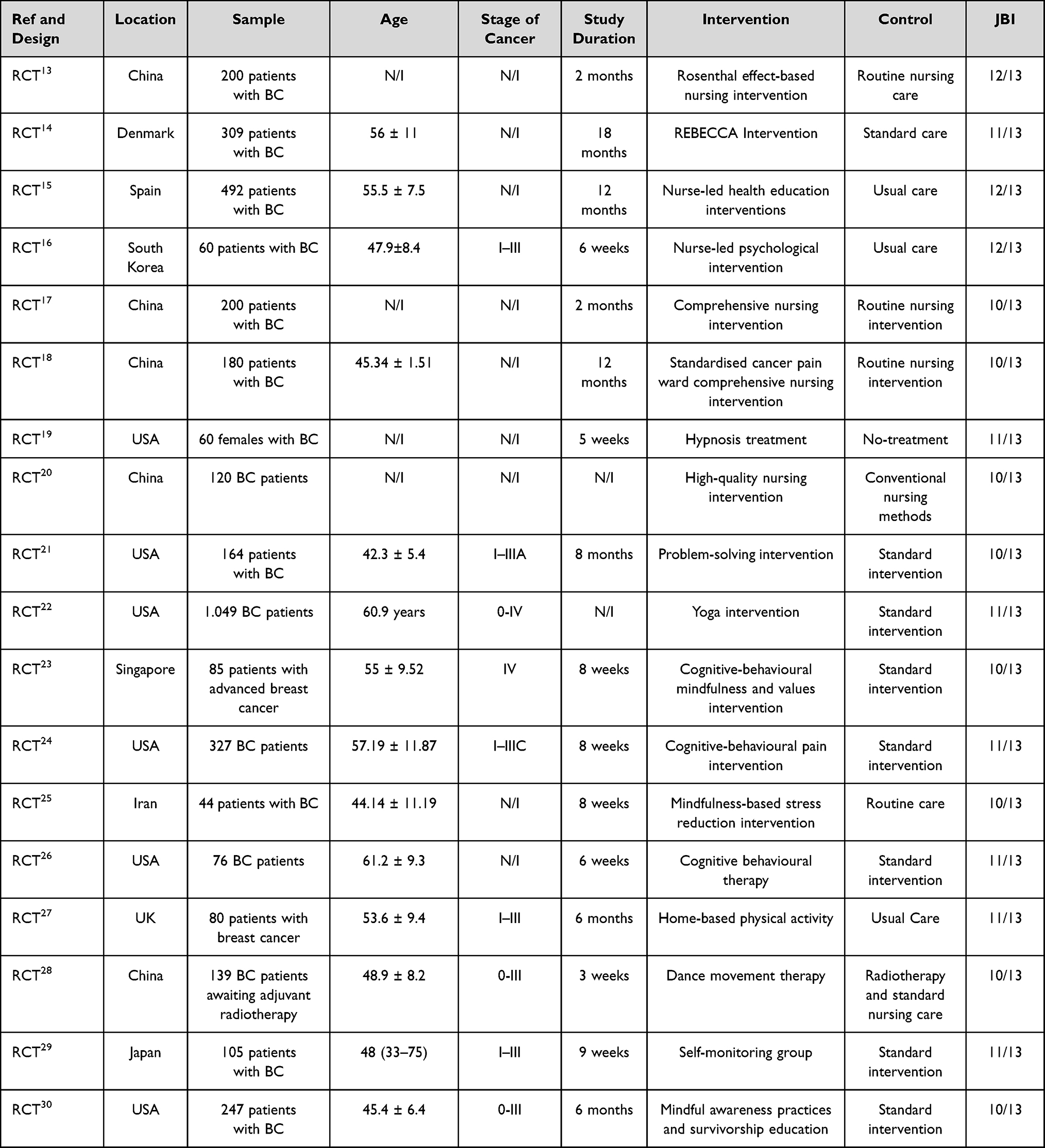 |
Table 1 Characteristics of Included Studies |
Characteristic of Studies
18 RCT studies were analysed in this systematic review (see Table 1). A total of 3.937 patients with BC, the majority of whom were at stage 0-IIIB, with the smallest sample size being 44 patients25 and the largest being 1.049 BC patients.22 The comprehensive articles were released at different times, ranging from 2002 to 2025. Then, geographically, Most studies were conducted in Asian countries (n = 9), including China (n = 5), South Korea, Singapore, Iran, and Japan (1 study each). In addition, another study was conducted in the USA (n=6), Denmark, Spain, and the UK (1 study each).
Characteristic Participants
A total of 3.937 breast cancer patients, ranging from stage 0-IIIB to advanced stage (IV), were involved in the study (Table 1). The participants’ ages ranged from 45 to 51 years, with the youngest at 30 and the oldest at 76. The majority of participants received curative therapies such as radiotherapy and chemotherapy, and experienced various unpleasant symptoms, including anxiety, stress, depression, vasomotor disturbances such as hot flashes, taste alteration, sleep disturbances, activity limitations, weight gain due to adjuvant hormonal therapy, and a decreased QoL.
Characteristics of Intervention
Based on the characteristics of the interventions used in symptom management for breast cancer patients, these interventions are divided into three main categories: Psychological and Behavioural Interventions, Nursing Care Coordination, and Physical and Educational Interventions. Each of these categories is designed to meet the needs of patients with different symptom characteristics and responses to therapy (see Figure 2 and Table 2).
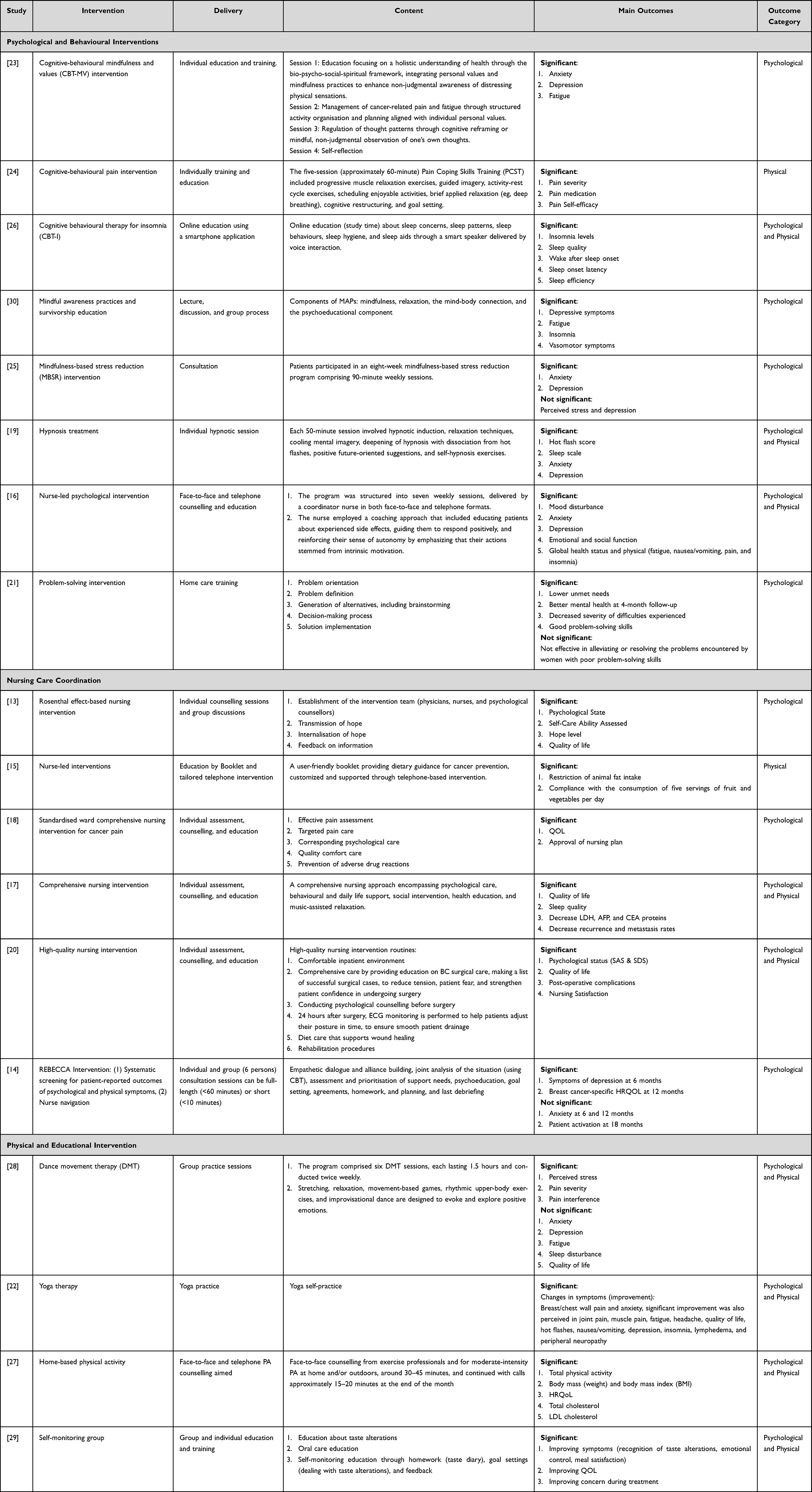 |
Table 2 Characteristics of Intervention, Delivery Method, Content, and Main Outcome |
 |
Figure 2 Overview of Symptoms Management Content Based on Intervention. |
Domain I: Psychological and Behavioural Interventions
In this systematic review, the phenomenon was obtained that research that focused on psychological and behavioural interventions for patients with BC was the intervention most frequently applied in reducing both psychological and physical symptoms in BC patients.16,19,21,23–26,30 Psychological interventions such as cognitive behavioural therapy (CBT) have been widely used to address various cancer-related symptoms, including pain, insomnia, and stress. The application of CBT to symptom management in BC patients focuses on changes in cognition, maladaptive emotions, and behaviour, and has demonstrated effectiveness in reducing individual symptoms in early-stage cancer patients.23,24,26 Besides CBT, other behavioral therapies such as mindfulness are also considered capable of reducing psychological symptoms such as depression, fatigue, insomnia, and vasomotor disorders in BC patients.25,30 Problem-based interventions and counseling are also considered capable of reducing the inability of BC patients to meet their needs independently, improving mental health, and training BC patients to solve problems related to the uncomfortable symptoms they experience.21
Domain II: Nursing Care Coordination
Coordination in nursing care is an important complement to standard nursing services, given the absence of a systematic, continuous assessment mechanism for patient needs and for the implementation of care, both during treatment and after discharge.31 Interventions are structured according to Orem’s self-care model.32 The goal of nursing interventions is to bathe the patient and restore self-care to an adequate level as quickly as possible. In this review, RCTs discussing nursing care coordination reported that after nursing interventions, levels of anxiety, distress, depression, fatigue, and anger significantly decreased.13,14,20,31,33,34 In addition, patient satisfaction with nursing care and QoL increased significantly.18
Rosenthal’s model, which focuses on the transmission and internalisation of hope, can significantly improve self-care skills, the level of hope for recovery for patients, and, of course, the quality of life of BC patients.13 In addition, the REBECCA model, which includes nurse-led navigation interventions to assess support needs, psychoeducation, and develop treatment goals for BC patients using the SMART method, is also considered to have a positive impact on depressive symptoms and quality of life for patients.14 In addition, nurse-led interventions that focus on educational programs regarding cancer treatment, both using booklets and telephone, are considered capable of increasing patient compliance in managing their daily nutrition.15 In addition to impacting the patient’s psychological condition, nursing care coordination is also considered to improve the physical condition of BC patients, as evidenced by decreases in LDH, AFP, and CEA protein levels, and can even reduce metastasis recurrence rates.17
Domain III: Physical and Educational Intervention
Previous studies have shown that physical movement can reduce fatigue and improve psychotherapy outcomes.35 Integrated interventions combining elements of movement and psychotherapy may be more effective in reducing bothersome symptoms in cancer patients.22,27–29 Dance movement therapy (DMT) is a psychosocial intervention involving movement that incorporates elements of dance and group psychotherapy. This review found that, while patients receiving DMT reported significant reductions in fatigue levels, there were no significant changes in QoL, anxiety, depression, pain severity, or sleep disturbances.28 In addition to DMT, home-based yoga therapy and physical activity have a positive impact on changes in laboratory indices, such as reducing RC and LDL-C, improving physical symptoms (including muscle, joint, and headache pain), reducing symptoms of nausea and vomiting, and preventing neuropathy.22,27 From a previous study that focused on direct physical activity, implementing self-monitoring interventions that focus on changes in taste alteration symptoms through educational procedures and routine monitoring with daily diaries, and obtained quite significant results in increasing self-efficacy towards taste alteration, how to overcome it, and improving the quality of life that had previously decreased due to taste alteration.29
Discussion
This systematic review aimed to synthesize recent evidence on nursing interventions, delivery approaches, and outcome measures for symptom management in patients with breast cancer. A total of 18 RCTs were identified, reflecting a growing body of high-quality evidence supporting the role of nursing interventions in addressing the multifaceted symptom burden experienced by this population. Overall, nursing interventions contribute not only to statistically significant improvements in selected physical and psychological symptoms but also to broader clinical outcomes such as enhanced self-efficacy, coping capacity, treatment adherence, and patient-reported well-being. Notably, several studies reported variable or domain-specific effects, indicating that the impact of nursing interventions may differ depending on symptom type, intervention design, duration, and patient characteristics.
The interventions identified in this review were categorised into three key domains: psychological and behavioural interventions, nursing care coordination, and physical and education-based interventions. Most studies demonstrated significant improvements in patient-reported outcomes following the interventions, with quality of life (QoL/HRQoL) being the most consistently improved outcome.13,14,17,18,20,22,27,29 Significant reductions in anxiety and depression were also reported in several studies.16,19,22,23,25 Improvements in fatigue were observed in multiple studies,16,22,23,30 while significant reductions in pain were reported in pain-focused, movement-based, and yoga interventions.22,24,28 In addition, improvements in physical symptoms, encompassing multiple symptom clusters, were reported in interventions specifically targeting symptom management.16,22,29
The findings of this review indicate mixed effects of the interventions across outcomes. While many studies reported significant improvements in QoL,13,14,17,18,20,22,27,29 Ho et al (2016) found that dance movement therapy did not result in significant improvements in QoL, nor did it produce significant changes in anxiety, depression, fatigue, or sleep disturbance.28 Similarly, Mirmahmoodi et al (2020) reported non-significant effects of mindfulness-based stress reduction on perceived stress and depressive symptoms, despite improvements observed in other psychological outcomes (anxiety).25 In addition, Bidstrup et al (2023) demonstrated that anxiety outcomes were not significant at 6 and 12-month follow-up, and patient activation did not reach statistical significance at 18 months.14 Furthermore, Allen et al (2002) showed that a problem-solving intervention was not significantly effective among participants with poor baseline problem-solving skills, highlighting the limited impact of the intervention within specific subgroups.21 Overall, these findings suggest that intervention effects are outcome-specific and context-dependent, influenced by intervention characteristics, follow-up duration, and participant profiles.
In contrast to previous reviews that primarily focused on the effectiveness of psychological nursing interventions in improving the QoL of patients with BC, particularly in the post-mastectomy context,36 this review offers a more comprehensive perspective. This review not only evaluates QoL outcomes but also critically examines various nursing intervention delivery models and a broader range of outcomes across psychological, physical, and behavioural domains. Beyond psychological and behavioural interventions, this study highlights the important role of nursing care coordination, as well as physical and educational interventions, in managing complex symptoms such as pain, fatigue, sleep disturbances, nutritional changes, and emotional distress throughout the breast cancer care trajectory. Consequently, the findings of this review extend current understanding from a single-domain focus to a holistic, multidimensional approach that better reflects the real-world clinical needs of patients with breast cancer across different disease stages and treatment.
Based on the review results, psychological and behavioral interventions are the most researched domains and show consistent clinical impact in symptom management in breast cancer patients. This category has an excellent clinical impact in overcoming both physical and psychological clinical symptoms in BC patients, such as reducing cancer pain and symptoms of anxiety and depression.16,19,21,23–26,30 Psychological and behavioural interventions typically involve intensive communication between nurses and patients, alongside cognitive approaches such as CBT for insomnia and pain. The CBT approach enables patients to gain an understanding of their breast cancer condition, recognise and manage symptoms more effectively, regulate emotional responses, and engage collaboratively with nurses in the overall process of symptom management and care.37 In addition to the direct impact on psychological symptoms, several studies also show that improvements in psychological aspects contribute indirectly to the reduction of physical symptoms, such as pain and fatigue,23,24,30 through increased adherence to therapy and self-care behaviors. These findings confirm that psychological interventions are not only supportive but are an important therapeutic component of holistically oriented breast cancer.
Coordination of nursing care is emerging as a key component in bridging the complexity of breast cancer care involving multiple phases and disciplines. Nursing care coordination, such as the Rosenthal model26 and REBECCA,14 can increase patient self-confidence through psychological suggestions such as hope, praise, and trust, and provide positive motivation for healing,38 and has been shown to significantly reduce post-operative anxiety and depression. The nurse’s role as coordinator enables ongoing symptom monitoring, effective interprofessional communication, and the tailoring of interventions to the patient’s individual needs. Rosenthal effect–based interventions can strengthen patients’ self-identity and cognitive focus, thereby reducing negative emotions through active listening, positive affirmation, and comfort and encouragement.39 In addition, the REBECCA model shows promising results in alleviating psychological symptoms and improving QoL through nurse navigation. Although it is cost-effective for supportive care in BC patients, the REBECCA system remains limited in managing symptoms.40
Physical and education-based interventions such as dance movement therapy, yoga therapy, home-based physical activity, and self-monitoring interventions.22,27–29 DMT is a psychosocial intervention that combines movement, dance, and group psychotherapy, with evidence suggesting its effectiveness in reducing pain intensity and disturbance in breast cancer patients undergoing radiotherapy, making it a suitable component of integrative cancer care, particularly for early or prophylactic pain management.28 In addition, Yoga is commonly practiced among breast cancer patients, with approximately one-third of participants in the Mayo Clinic Breast Cancer Registry reporting prior use. Studies indicate that patients perceive yoga as a beneficial complementary approach for managing cancer-related symptoms.22
Home-based physical activity interventions led to marked improvements in physical activity performance among breast cancer survivors, accompanied by favorable changes in light and vigorous physical activity, anthropometric indices (weight and BMI), HRQoL scores, and lipid profiles, relative to usual care.27 Research evaluating the effectiveness of self-monitoring group (SMG)–based educational interventions in breast cancer patients experiencing chemotherapy-induced taste alterations demonstrated that self-monitoring reduced negative cognitions related to taste changes and alleviated associated discomfort. These findings support self-monitoring as an effective nursing intervention for managing taste-related side effects of chemotherapy.29
While psychological and behavioural interventions, nursing care coordination, and physical and educational approaches each demonstrated independent effectiveness, this review indicates that optimal symptom management in breast cancer care is best achieved through their integration. Psychological interventions can enhance self-efficacy and emotional regulation, thereby supporting adherence to self-management behaviours, while coordinated nursing care ensures continuity and reinforcement across the care trajectory. These findings underscore the importance of holistic, patient-centred nursing models that address both physical and psychosocial symptoms. Future research should focus on refining and validating integrated nursing intervention models, particularly regarding intervention components, duration, and applicability across clinical settings.
Strengths and Limitations of the Study
This study has several strengths that make it relevant to symptom management practices in breast cancer patient care. Firstly, it employs a systematic review methodology that adheres to the rigorous PRISMA guidelines, ensuring transparency and clarity in the selection and analysis of studies. Second, only RCTs are of lower quality and more prone to bias than other designs. The broad geographic coverage of the included studies provides a global perspective and increases the generalizability of findings to diverse patient populations. Next, the review identifies three main domains of nursing interventions: 1) psychological and behavioural interventions, 2) nursing care coordination, and 3) physical and education-based interventions. This categorisation provides a comprehensive overview of the various intervention methods used in clinical practice and offers valuable insights into approaches for managing breast cancer symptoms. However, this study has several limitations that need to be considered. The considerable variation in intervention approaches, program duration, materials, and outcome measures across the included studies led to substantial heterogeneity. These differences make it difficult to conduct direct comparisons and identify universally effective nursing interventions. Further research with more controlled designs is required to provide consistent and applicable recommendations across diverse clinical settings.
Conclusion
This systematic review synthesized evidence from 18 studies and identified three core domains of nursing interventions: psychological and behavioural interventions, nursing care coordination, and physical and educational interventions, which collectively address the review objectives of improving symptom management and QoL in patients with breast cancer. Among these domains, psychologically focused interventions and coordinated nurse-led care demonstrated the most consistent and robust effects in reducing psychological distress (anxiety and depression) while managing persistent symptoms and improving overall QoL.
These findings underscore the critical role of nursing interventions as an integral component of holistic breast cancer care. In clinical practice, integrating structured psychological support, continuous care coordination, and targeted physical and educational strategies can enhance symptom management, promote patient self-management, and improve both physical and psychological well-being throughout the cancer care trajectory. From an educational perspective, the results highlight the need to strengthen nursing training in psychosocial care, symptom assessment, and coordinated, patient-centred intervention delivery. Future research should move beyond broad effectiveness evaluations and focus on identifying the optimal characteristics of nursing interventions, including intervention intensity, duration, delivery models, and combinations of approaches. Well-designed, multicentre randomized trials with standardized outcome measures are particularly needed to reduce heterogeneity and to determine which nursing interventions are most effective and scalable across diverse clinical settings.
Acknowledgments
The authors gratefully acknowledge Universitas Padjadjaran for the financial support provided through a research grant (Contract Number: 1974/UN6.L/PT.00/2025), which made this study possible.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rezanejad Gatabi Z, Mirhoseini M, Khajeali N, Rezanezhad Gatabi I, Dabbaghianamiri M, Dorri S. The accuracy of electrical impedance tomography for breast cancer detection: a systematic review and meta-analysis. Breast J. 2022;2022:8565490. doi:10.1155/2022/8565490
2. Jacobs JM, Post K, Massad K, et al. A telehealth intervention for symptom management, distress, and adherence to adjuvant endocrine therapy: a randomized controlled trial. Cancer. 2022;128(19):3541–14. doi:10.1002/cncr.34409
3. NICE. Early and locally advanced breast cancer: diagnosis and management. 2025.
4. Wang X, Wang N, Zhong L, et al. Prognostic value of depression and anxiety on breast cancer recurrence and mortality: a systematic review and meta-analysis of 282,203 patients. Mol Psychiatry. 2020;25(12):3186–3197. doi:10.1038/s41380-020-00865-6
5. McFarland DC, Shaffer KM, Tiersten A, Holland J. Physical symptom burden and its association with distress, anxiety, and depression in breast cancer. Psychosomatics. 2018;59(5):464–471. doi:10.1016/j.psym.2018.01.005
6. Tang J, Guo B, Zhong C, et al. Detection of differences in physical symptoms between depressed and undepressed patients with breast cancer: a study using K-medoids clustering. BMC Cancer. 2025;25(1). doi:10.1186/s12885-024-13387-z
7. Al Qadire M, Alsaraireh M, Alomari K, et al. Symptom clusters predictive of quality of life among jordanian women with breast cancer. Semin Oncol Nurs. 2021;37(2):151144. doi:10.1016/j.soncn.2021.151144
8. Wang YF, He RJ, Yuan XJ, et al. Dynamic changes and correlation between symptoms and quality of life in patients with breast cancer during chemotherapy. Technol Heal Care. 2023;31(4):1365–1373. doi:10.3233/THC-220657
9. Luck L, Chok H, Scott N, Wilkes L. The role of the breast care nurse in patient and family care. J Clin Nurs. 2016;26. doi:10.1111/jocn.13704.
10. Qi Y, Li H, Guo Y, Cao Y, Wong C. symptom clusters in breast cancer patients receiving adjuvant chemotherapy: a systematic review. J Clin Nurs. doi:10.1111/jocn.17479.
11. Trisyani Y, Nuraeni A, Anna A, et al. Telehealth approach in breast cancer care: a systematic review of models and outcomes telehealth approach in breast cancer care: a systematic review of models and outcomes. Int J Womens Health. 2025;1411:2759–2775. doi:10.2147/IJWH.S549643
12. Alkılınç G, Akıncı M, Kılıç B. A systematic review of nursing intervention studies for lymphedema after breast cancer. Black Sea J Heal Sci. doi:10.19127/bshealthscience.1684336
13. Ye YY, Cao YC, Lu XJ, Xiang X. Impact of Rosenthal effect-based nursing intervention on self-care ability and hope level in patients undergoing breast surgery. BMC Surg. 2025;25(1). doi:10.1186/s12893-025-02797-w
14. Bidstrup PE, Johansen C, Kroman N, et al. Effect of a nurse navigation intervention on mental symptoms in patients with psychological vulnerability and breast cancer: the REBECCA randomized clinical trial. JAMA Netw open. 2023;6(6):e2319591. doi:10.1001/jamanetworkopen.2023.19591
15. Valle MO, Payo RARM, Briand LABC, Manager P, Rn AL. Impact of two nurse-led interventions targeting diet among breast cancer survivors: results from a randomized controlled trial. Eur J Cancer. doi:10.1111/ecc.12854
16. Hee KY, Sook CK, Kihye H, Won KH. A psychological intervention program for patients with breast cancer under chemotherapy and at a high risk of depression: a randomized clinical trial. J Clin Nurs. 2018;27(3–4):572–581. doi:10.1111/jocn.13910
17. Kang X, Fang Y, Kong Y. Effect of comprehensive nursing intervention on therapy and life quality of patients with breast cancer. Biomed Res Int. 2017;28(20):8801–8805.
18. Chen F, He Y, Lao L. effect of comprehensive nursing intervention in standardized cancer pain ward on pain relief and quality of life in patients with breast cancer Breast. Minerva Surg. 2024;79(4):501–503. doi:10.23736/S2724-5691.21.09278-9
19. Elkins G, Marcus J, Stearns V, et al. Randomized trial of a hypnosis intervention for treatment of hot flashes among breast cancer survivors. J Clin Oncol. 2008;26(31):5022–5026. doi:10.1200/JCO.2008.16.6389
20. Zhai Y, Wang X. Study on the effect of high-quality nursing intervention mode on the improvement of emotional status of breast cancer patients Breast. Panminerva Med. 2022;64(2):294–295. doi:10.23736/S0031-0808.21.04430-X
21. Allen SM, Shah AC, Nezu AM, et al. A problem-solving approach to stress reduction among younger women with breast carcinoma: a randomized controlled trial. Cancer. 2002;94(12):3089–3100. doi:10.1002/cncr.10586
22. Patel SR, Zayas J, Medina-Inojosa JR, et al. Real-world experiences with yoga on cancer-related symptoms in women with breast cancer. Glob Adv Heal Med. 2021:10. doi:10.1177/2164956120984140.
23. Teo I, Vilardaga JP, Tan YP, et al. A feasible and acceptable multicultural psychosocial intervention targeting symptom management in the context of advanced breast cancer. Psychooncology. 2020;29(2):389–397. doi:10.1002/pon.5275
24. Fisher HM, Hyland KA, Winger JG, et al. Effect of pain coping skills training on pain and pain medication use for women with breast cancer. J Pain Symptom Manag. 2024;66(1):70–79. doi:10.1016/j.jpainsymman.2023.03.012.Effect
25. Mirmahmoodi M, Mangalian P, Ahmadi A, Dehghan M. The effect of mindfulness-based stress reduction group counseling on psychological and inflammatory responses of the women with breast cancer. Integr Cancer Ther. 2020;19. doi:10.1177/1534735420946819
26. Starling CM, Greendenberg D, Lewin D, et al. Voice-activated cognitive behavioral therapy for insomnia a randomized clinical trial. JAMA Intern Med. 2024;7(9):1–12. doi:10.1001/jamainternmed.2024.4419
27. Lahart I, Metsios GS, Nevill AM, Kitas GD, Carmichael AR. Randomised controlled trial of a home-based physical activity intervention in breast cancer survivors. BMC Cancer. 2016;16(1):234. doi:10.1186/s12885-016-2258-5
28. RTH H, Fong TCT, Cheung IKM, Yip PSF, Luk MY. Effects of a short-term dance movement therapy program on symptoms and stress in patients with breast cancer undergoing radiotherapy: a randomized, controlled, single-blind trial. J Pain Symptom Manage. 2016;51(5):824–831. doi:10.1016/j.jpainsymman.2015.12.332
29. Kinjo T, Kanda K, Fujimoto K. Effects of a self-monitoring intervention in breast cancer patients suffering from taste alterations induced by chemotherapy: a randomized, parallel-group controlled trial. Eur J Oncol Nurs. 2021;52:101956. doi:10.1016/j.ejon.2021.101956
30. Bower JE, Partridge AH, Wolff AC, et al. Targeting depressive symptoms in younger breast cancer survivors: the pathways to wellness randomized controlled trial of mindfulness meditation and survivorship education. J Clin Oncol. 2021;39(31):3473–3484. doi:10.1200/JCO.21.00279
31. Wengström Y, Häggmark C, Strander H, Forsberg C. Effects of a nursing intervention on subjective distress, side effects and quality of life of breast cancer patients receiving curative radiation therapy - A randomized study. Acta Oncol. 1999;38(6):763–770. doi:10.1080/028418699432923
32. Orem D. Nursing: Concepts of Practice. Mosby Company; 1995.
33. Zhang H, Weiqian Y. Influence of motivational nursing intervention combined with spouse support on negative emotion and quality of life of patients undergoing breast cancer surgery. Minerva Surg. 2023;78(4):450–452. doi:10.23736/S2724-5691.21.09383-7
34. Wengström Y, Häggmark C, Forsberg C. Coping with radiation therapy: effects of a nursing intervention on coping ability for women with breast cancer. Int J Nurs Pract. 2001;7(1):8–15. doi:10.1046/j.1440-172x.2001.00239.x
35. Cramp F, Byron-Daniel J. Exercise for the management of cancer-related fatigue in adults. Cochrane Database Syst Rev. 2012;11(11):CD006145. doi:10.1002/14651858.CD006145.pub3
36. Li H, Li J, Wang X, et al. Systematic review and meta-analysis of the efficacy and safety of psychological intervention nursing on the quality of life of breast cancer patients. Gland Surg. 2022;11(5):882–891. doi:10.21037/gs-22-206
37. Li M, Xie X, Xu H, Li H. A psychological nursing intervention for patients with breast cancer on inflammatory factors, negative emotions and quality of life. Iran J Public Health. 2022;51(9):2041–2047. doi:10.18502/ijph.v51i9.10559
38. Tsaras K, V PI, Mitsi D, et al. Assessment of depression and anxiety in breast cancer patients: prevalence and associated factors. Asian Pac J Cancer Prev. 2018;19(6):1661–1669. doi:10.22034/APJCP.2018.19.6.1661
39. Jun W, Tian Y. Application of meditation relaxation training and rosenthal effect in patients with adenoidectomy. Evid Based Complement Alternat Med. 2022;2022:1420639. doi:10.1155/2022/1420639
40. Ruiz-Pérez I, Rodríguez-Gómez M, Pastor-Moreno G, Escribá-Agüir V, Petrova D. Effectiveness of interventions to improve cancer treatment and follow-up care in socially disadvantaged groups. Psychooncology. 2019;28(4):665–674. doi:10.1002/pon.5011
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nursing Interventions to Improve Quality of Life Among Children and Adolescents with Thalassemia: A Scoping Review
Mardhiyah A, Panduragan SL, Mediani HS, Yosep I
Journal of Multidisciplinary Healthcare 2023, 16:1749-1762
Published Date: 23 June 2023
Psychometric Properties and Factorial Analysis of the Arabic McGill-QoL Questionnaire in Breast Cancer
Omar MTA, Alnahdi AH
Breast Cancer: Targets and Therapy 2023, 15:813-824
Published Date: 14 November 2023
Predictive Models of Psychological Distress, Quality of Life, and Adherence to Medication in Breast Cancer Patients: A Scoping Review
Pezzolato M, Spada GE, Fragale E, Cutica I, Masiero M, Marzorati C, Pravettoni G
Patient Preference and Adherence 2023, 17:3461-3473
Published Date: 19 December 2023
Impact of Empowerment Theory-Based Nursing Intervention on the Quality of Life and Negative Emotions of Patients Diagnosed with Brain Metastasis Post Breast Cancer Surgery
Jiang R, Liu H, Jiang X, Wang D, Li X, Shang Y
Journal of Multidisciplinary Healthcare 2024, 17:2303-2312
Published Date: 14 May 2024
Nursing Interventions in Palliative Care for Advanced Dementia: A Systematic Review of Symptom, Relief, Comfort, and Caregiver Support
Pujante VGB, Sami W, Al-Kuwari NF, Rizvi MR
Journal of Multidisciplinary Healthcare 2025, 18:6545-6564
Published Date: 9 October 2025