Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Nursing Interventions in Palliative Care for Advanced Dementia: A Systematic Review of Symptom, Relief, Comfort, and Caregiver Support
Authors Pujante VGB, Sami W ![]() , Al-Kuwari NF, Rizvi MR
, Al-Kuwari NF, Rizvi MR ![]()
Received 11 June 2025
Accepted for publication 21 September 2025
Published 9 October 2025 Volume 2025:18 Pages 6545—6564
DOI https://doi.org/10.2147/JMDH.S546183
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jacqueline Dunbar-Jacob
Vianca Gloriene Barcoma Pujante,1 Waqas Sami,2 Noof Fahad Al-Kuwari,2 Moattar Raza Rizvi3,4
1College of Nursing, QU-Health Sector, Qatar University, Doha, Qatar; 2Department of Pre-Clinical Affairs, College of Nursing, Health Sector, Qatar University, Doha, Qatar; 3College of Healthcare Professions, Dehradun Institute of Technology (D.I.T) University, Mussoorie, Uttarakhand, 248009, India; 4Allied Health Sciences, Santosh Deemed to Be University, Ghaziabad, Delhi NCR 201009, India
Correspondence: Waqas Sami, Department of Pre-Clinical Affairs, College of Nursing, QU Health Sector, Qatar University, P.O. Box 2713, Doha, Qatar, Email [email protected]
Purpose: Individuals with advanced dementia often endure high symptom burden and receive limited specialized palliative care. Nurses play a central role in delivering end-of-life care, yet the impact of nurse-led interventions remains underexplored. This review synthesizes available evidence on nursing-led approaches, with a focus on symptom relief, patient comfort, and caregiver support.
Methods: A systematic review was conducted in accordance with PRISMA 2020 guidelines. Four databases (PubMed, Embase, CINAHL, and Cochrane Library) were searched for studies published between January 2015 and March 2025. Eligible studies included randomized controlled trials (RCTs), cluster RCTs, and non-randomized studies evaluating nurse-led palliative interventions in institutional or community dementia settings. Risk of bias was assessed using Cochrane RoB 2.0 and ROBINS-I tools. Data extraction focused on intervention types, delivery modes, nurse training, and clinical outcomes.
Results: Twenty-three studies from 12 countries were included (8 cluster RCTs, 9 individual RCTs, 6 non-randomized trials). Nurse-led programs improved care planning (≥ 75% documentation rates), reduced caregiver decisional conflict (20– 30%), and enhanced communication quality (by up to 20 percentage points). Pain detection increased by 41%, with validated tools reducing pain scores by up to 30%. Psychosocial therapies reduced agitation by up to 25% and improved care cooperation. Multicomponent models decreased emergency visits and improved transitions, with over 40% increases in advance directive completion. Risk of bias varied by design and domain.
Conclusion: Nurse-led palliative care interventions show consistent benefits in communication, symptom control, and caregiver support. However, evidence on long-term caregiver outcomes is limited, and heterogeneity in design and measurement limits comparability. Standardized, scalable models are needed to fully integrate nursing-led approaches into palliative dementia care.
Keywords: dementia, palliative care, nursing care, advance care planning, symptom management, quality of life
Introduction
Dementia remains a major global health concern, characterized by progressive cognitive decline, memory loss, behavioral disturbances, and increasing functional dependence.1 These impairments significantly diminish quality of life and place substantial emotional, physical, and financial strain on caregivers.2 Current estimates indicate that over 55 million people worldwide are living with dementia, a figure projected to rise to 78 million by 2030 and 139 million by 2050 due to global population aging.3,4 In its advanced stages, dementia is marked by severe neurological deterioration, complete dependence in activities of daily living, and a heightened risk of hospitalization, institutionalization, and mortality.5,6 Critically, individuals with advanced dementia frequently experience unrecognized pain, agitation, and distress, particularly when verbal communication becomes impaired and care shifts from person-centered goals to a focus on medical stabilization.7,8 Emerging neurobiological evidence demonstrates that such symptoms often manifest atypically in dementia due to underlying neural disruption. For example, degeneration of the prefrontal cortex and limbic pathways contributes to dysregulated affect and agitation; disconnection in cortical–subcortical pain circuits leads to under-recognition or atypical expression of pain; and progressive damage to frontotemporal and parietal networks impairs communication and emotional signaling.9–11 These mechanisms underscore the complexity of symptom recognition in dementia and highlight the advanced clinical skills required of nurses at the bedside.
Palliative care is increasingly recognized as a critical, though often underutilized, component in the management of advanced dementia. The WHO defines it as a holistic approach that addresses physical, psychological, and spiritual distress, which is essential for individuals with complex needs such as those in advanced stages of dementia. These individuals often endure multifaceted suffering that spans physical symptoms, emotional challenges, and social isolation.12 Despite its importance, the integration of palliative care into dementia services remains inconsistent and insufficiently developed. Unlike patients with terminal cancer, those with advanced dementia are less often identified as being in the terminal phase of illness, leading to missed opportunities for implementing comfort-centered and person-focused end-of-life care.7,13 This under-recognition is largely due to the unpredictable disease trajectory, absence of specific terminal-stage biomarkers, and lack of clear guidelines regarding the initiation of palliative interventions.14,15 As a result, many individuals experience inadequately managed symptoms, fragmented communication with families, and unnecessary hospitalizations that compromise comfort and dignity.
In the absence of consistent specialist involvement, nurses play a central role in delivering palliative care to individuals with advanced dementia. Positioned at the frontline in both nursing homes and home-based settings, they are often the first to detect subtle clinical or behavioral changes, enabling timely and personalized interventions.16 Nursing responsibilities extend beyond routine clinical care to encompass pain assessment, communication with families, psychosocial support, advanced care planning, and interdisciplinary coordination. Validated nursing tools and interventions, such as the PAINAD scale, person-centered therapeutic activities, nurse-facilitated case conferences, and non-pharmacological strategies, have demonstrated effectiveness in improving symptom control, reducing agitation, and alleviating caregiver burden.8,17–19
Despite growing recognition of the pivotal role nurses play in palliative dementia care, the empirical evidence supporting their contributions remains limited and fragmented. Much of the existing literature continues to focus on physician-led or pharmacological interventions, thereby underrepresenting the breadth and sustained impact of nursing practices.14,20 In studies that do examine nurse-led interventions, methodological limitations, such as small sample sizes, heterogeneous intervention protocols, inconsistent outcome measures, and limited generalizability, compromise the strength and applicability of findings.21,22 Moreover, few studies offer standardized frameworks for ethically complex aspects of care, such as communication with non-verbal patients or culturally sensitive end-of-life planning, leaving many nurses without clear, evidence-based guidance.23,24
In response to these knowledge gaps, this systematic review synthesizes evidence from peer-reviewed studies published between 2015 and 2025 on nurse-led interventions in palliative care for individuals with advanced dementia. It evaluates the impact of these interventions on symptom relief, emotional well-being, patient comfort, family engagement, and healthcare utilization. For the purposes of this review, we defined nurse-led interventions as those in which nurses were the principal coordinators, facilitators, or decision-makers in delivering the intervention, even when part of a multidisciplinary team. By contrast, nurse-supported interventions were those in which nurses contributed to implementation but were not central to design or leadership. This distinction is important for understanding the scope of nursing leadership and interpreting the findings within the context of professional practice boundaries. This review therefore provides a comprehensive synthesis of available evidence to guide future practice, education, and policy in nursing-led palliative care for advanced dementia.
Materials and Methods
Registration and Reporting Framework
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA, 2020) guidelines to ensure methodological transparency and completeness.25 The review protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD42025633207), providing a publicly accessible record of the review’s objectives, eligibility criteria, and planned methods.
Study Design
A systematic review approach was used to identify, appraise, and synthesize evidence from randomized controlled trials (RCTs), cluster-RCTs, and relevant non-randomized studies evaluating nursing-led palliative care interventions in advanced dementia.
Study Objectives
The primary objective was to assess the effectiveness of these interventions in improving symptom control, patient comfort, quality of life, caregiver experience, and family satisfaction during end-of-life care.
Secondary objectives were to:
- Examine implementation challenges, methodological heterogeneity, and risk of bias in included studies.
- Identify evidence gaps in long-term caregiver outcomes, system-level integration, and feasibility of scaling interventions across different healthcare contexts.
- Provide recommendations to inform clinical practice, nursing education, and policy development in palliative dementia care.
Eligibility Criteria
Eligibility criteria were developed using the PICO framework to guide the selection of studies relevant to nursing-led interventions in palliative care for advanced dementia. Studies were included if they: (1) involved participants diagnosed with advanced dementia based on validated staging tools (eg, Functional Assessment Staging (FAST) ≥6a or Global Deterioration Scale (GDS) stages 4–7); (2) evaluated the effects of nursing-led or nurse-facilitated interventions, defined as those where registered nurses, clinical nurse specialists, or advanced practice nurses had a central role in delivering care, coordinating treatment, or initiating palliative protocols, including in multidisciplinary contexts; (3) compared the intervention to usual care, non-nurse-led care, or inactive control; and (4) assessed outcomes such as symptom burden (eg, pain, agitation), comfort at end of life, quality of life, caregiver experience, or care planning. Eligible studies were peer-reviewed randomized controlled trials (RCTs), cluster-RCTs, or non-randomized controlled studies published in English between January 2015 and March 2025 in institutional or community settings. The 10-year limit was chosen to capture evidence most relevant to contemporary dementia and palliative care practices, as standards, tools, and guidelines have evolved significantly over the past decade. Studies were excluded if they (a) targeted only early or moderate dementia stages, (b) did not clearly define the nurse-led component of the intervention, (c) used non-validated outcome measures, or (d) were non-empirical (eg, commentaries, reviews, or protocol-only publications without outcome data).
For this review, nurse-led interventions were defined as those in which nurses were the principal care providers, intervention facilitators, or coordinators, and where their actions were central to the design and implementation of the intervention. In line with this, we distinguished between nurse-led interventions, where nurses exercised leadership and decision-making authority (including in multidisciplinary contexts), and nurse-supported interventions, where nurses contributed to implementation but did not occupy a central leadership role. Studies were included if nurses functioned independently or as leaders in multidisciplinary teams, but were excluded if nursing roles were ancillary or non-specific.
Search Strategy
A comprehensive and systematic search was conducted across four electronic databases: PubMed, Scopus, CINAHL (via EBSCO), and the Cochrane Central Register of Controlled Trials. The search strategy combined controlled vocabulary (eg, MeSH terms) and free-text keywords related to advanced dementia, palliative or end-of-life care, nurse-led interventions, and trial design. Boolean operators and database-specific syntax were used to enhance sensitivity and specificity. Search terms included: (“dementia” OR “Alzheimer’s disease”) AND (“palliative care” OR “end-of-life care”) AND (“nurse-led” OR “nursing intervention”) AND (“randomized controlled trial” OR “cluster randomized trial”). Filters were applied to limit results to English-language articles published between January 2015 and March 2025. In addition to database searching, the reference lists of included studies and relevant reviews were manually screened to identify additional eligible publications. Protocols without outcome data and grey literature were excluded to maintain methodological consistency. The final search was conducted on March 31, 2025, to ensure inclusion of the most recent eligible studies published up to that date. In accordance with PRISMA 2020 guidance, we provide the full search strategy for PubMed below to ensure transparency. The search terms combined controlled vocabulary and keywords as follows: (“dementia” OR “Alzheimer’s disease”) AND (“palliative care” OR “end-of-life care”) AND (“nurse-led” OR “nursing intervention”) AND (“randomized controlled trial” OR “cluster randomized trial”). Filters were applied to limit results to English-language publications between January 2015 and March 2025. The strategy was developed collaboratively by two authors but was not externally peer-reviewed using the Peer Review of Electronic Search Strategies (PRESS) checklist.
Study Selection Process
Following the comprehensive database search, a total of 570 records were identified. Duplicate records (n = 298) were removed using EndNote X9 and manual verification. The remaining 272 records were screened by two independent reviewers based on predefined inclusion criteria. Disagreements at any stage were resolved through discussion and, if needed, adjudicated by a third reviewer. Agreement was calculated using Cohen’s kappa to assess inter-rater reliability.
During the screening process, 178 studies were excluded based on predefined criteria, including a lack of focus on nursing roles in palliative care, irrelevance to nursing interventions, targeting other healthcare professionals, absence of original data, and non-English language. A full breakdown of exclusion reasons is provided in Figure 1. Full-text retrieval was attempted for 94 records, but 24 could not be retrieved. The remaining 70 full-text articles were assessed independently for eligibility. Forty-seven studies were excluded due to insufficient focus on the nursing role (n = 19), absence of validated outcome measures (n = 12), inappropriate study designs (n = 7), or other issues such as incomplete data or unclear interventions (n = 9). Ultimately, 23 studies met the eligibility criteria and were included in the final synthesis.
 |
Figure 1 PRISMA flow diagram illustrating the study selection process, including identification, screening, eligibility assessment, and inclusion. |
Quality Assessment and Risk of Bias
Risk of bias (RoB) was assessed using validated tools appropriate to the study design. RoB 2 assessments addressed five domains as per Cochrane guidance, including randomization, intervention deviations, missing data, outcome measurement, and reporting. For cluster trials, additional considerations specific to the timing of recruitment, cluster loss, and baseline imbalances were included. Two reviewers conducted independent evaluations, with disagreements resolved by consensus or consultation with a third reviewer. Inter-rater agreement was strong (Cohen’s κ = 0.82). Risk of bias was categorized as low, some concerns, or high at both domain and overall levels.
For non-randomized intervention studies, risk of bias was assessed using the ROBINS-I tool, covering seven standard domains including confounding, participant selection, intervention classification, deviations, missing data, outcome measurement, and selective reporting. Two reviewers independently conducted all assessments using predefined criteria, resolving any disagreements through discussion or, when needed, third-party adjudication. Although inter-rater reliability was not formally calculated, full consensus was achieved. Risk of bias judgments were used to inform interpretation, but did not determine study inclusion. Visual summaries were presented using traffic light plots and bar charts to enhance transparency.
Data Synthesis and Analysis
Due to substantial methodological and clinical heterogeneity across the included studies, encompassing variations in study design (RCTs, cluster RCTs, non-randomized trials), intervention types (eg, communication training, symptom protocols, multicomponent models), outcome measures, and follow-up durations, a meta-analysis was deemed inappropriate. Therefore, a structured narrative synthesis approach was employed in accordance with PRISMA guidelines. Findings were thematically categorized under key domains, including patient symptom management, quality of life, emotional and psychosocial well-being, caregiver burden, and family satisfaction. Where available, quantitative results from individual studies were presented descriptively to highlight effect sizes and outcome directionality. Qualitative findings were integrated using thematic analysis to capture deeper insights into nursing roles, interdisciplinary collaboration, culturally tailored interventions, and the emotional toll on caregivers and nursing staff. This approach allowed for a comprehensive synthesis of both measurable outcomes and contextual factors that influence the implementation and effectiveness of nursing-led palliative care in advanced dementia.
Ethical Considerations
Ethics approval was not required for this systematic review, as it involves the synthesis of previously published studies. All original studies included had obtained appropriate ethical approval and informed consent as described in their original publications.
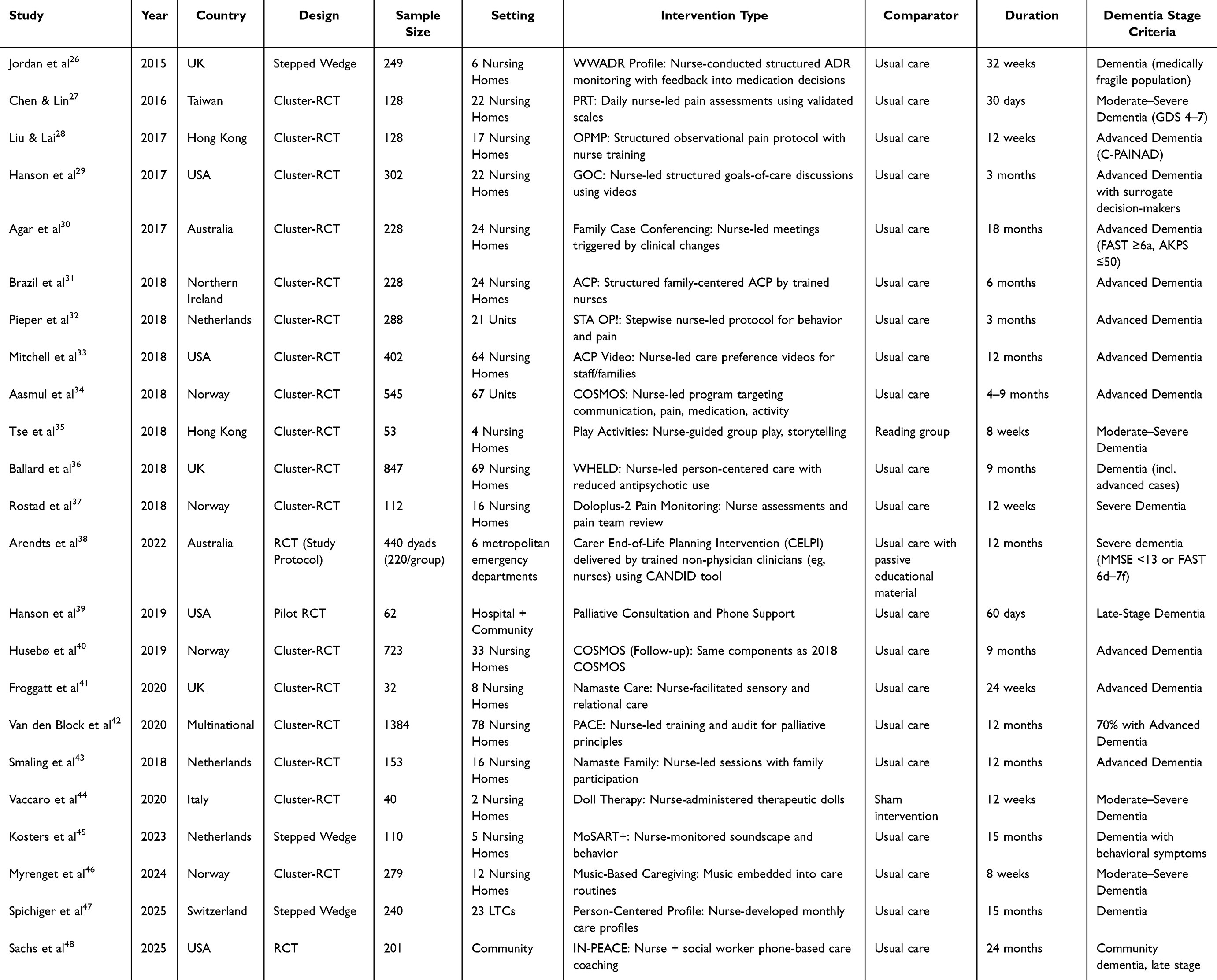 |
Table 1 Demographic and Geographical Characteristics of Included Studies |
Results
Study Characteristics and Scope
This review included 23 studies comprising 8 cluster RCTs, 9 individual RCTs, and 6 non-randomized studies, conducted across 12 countries from 2015 to 2025 (Table 1). The majority were set in nursing homes or long-term care units, with two community-based interventions38,48 and one hospital–community hybrid model.39 Sample sizes ranged from 3241 to 1384,42 with follow-up durations between 4 weeks and 24 months. The stage of dementia varied, but over 75% of studies targeted residents with advanced dementia, operationalized using tools like FAST (≥6a), GDS (4–7), and PAINAD-based assessments.
While 18 studies reported formal inclusion criteria based on dementia staging, only 14 provided a clear definition of advanced disease stages. Seven studies used stepped-wedge or quasi-experimental designs,26,47 which raises concerns regarding temporal confounders and consistency in implementation timing. Only half of the trials described randomization or allocation concealment procedures adequately. Similarly, only a minority (n = 10) reported any fidelity monitoring, contamination checks, or protocol adherence metrics, highlighting a recurrent limitation in complex intervention studies within long-term care.
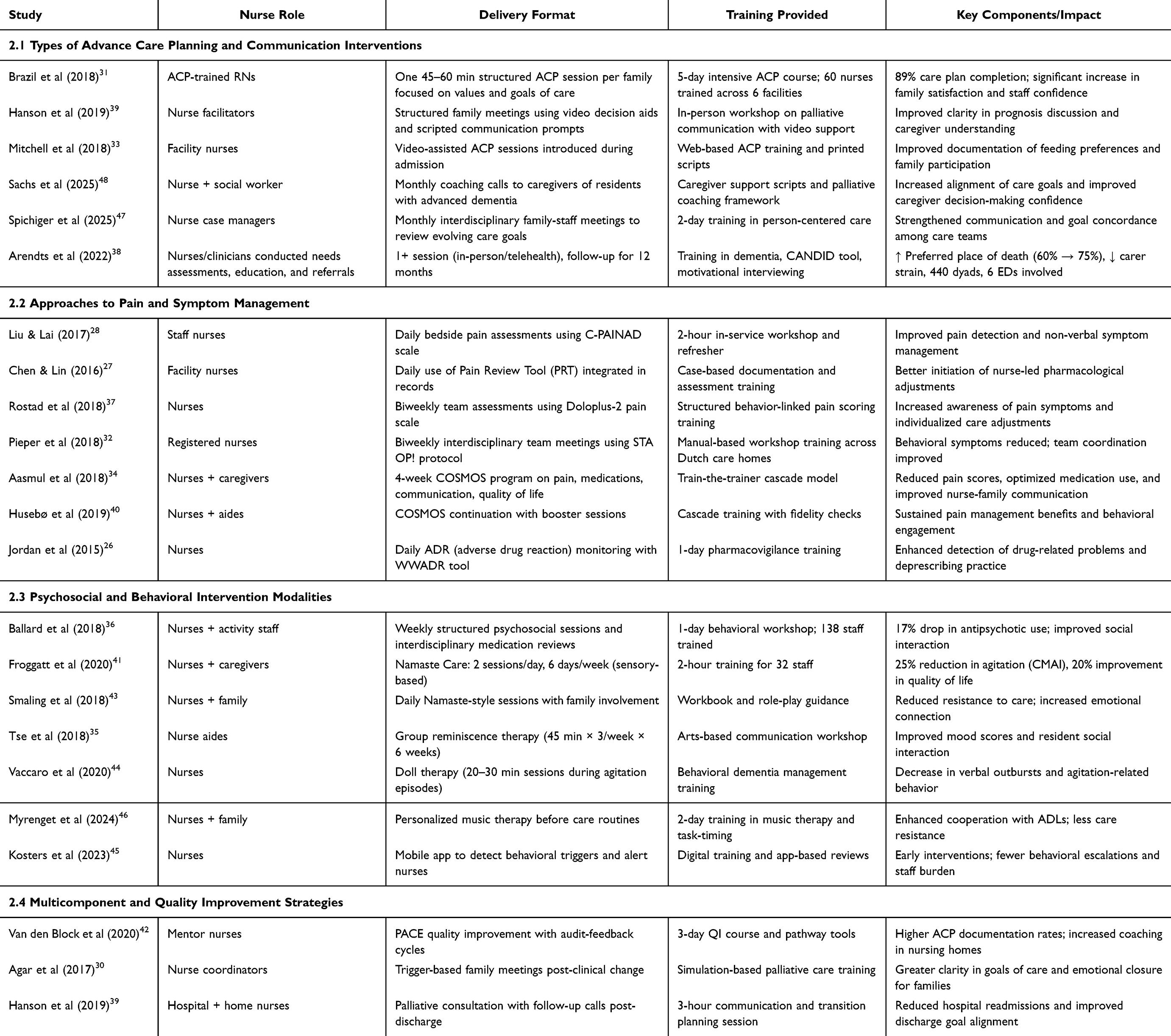 |
Table 2 Nurse-Led Intervention Characteristics Grouped by Intervention Type |
Nurse-Led Interventions by Type
Advance Care Planning and Communication Interventions
Six studies implemented nurse-led ACP and communication-focused models (Table 2). These ranged from structured face-to-face sessions31,47 to telephone-based caregiver coaching.38,48 A common feature was nurse facilitation of goal-of-care conversations, often using scripts or video aids. Notably, Brazil et al (2018) trained 60 RNs to conduct 45–60 minute sessions, achieving high care plan completion and improved caregiver satisfaction.31 Sachs et al (2025) extended this by combining nurse and social worker input over 24 months, indicating the feasibility of long-term community-based delivery.48 However, variation in nurse training (ranging from brief online modules to 5-day immersive workshops) and inconsistent documentation of the communication process raise concerns about intervention standardization. Most ACP interventions reported increased alignment between patient values and documented preferences, but cultural sensitivity and use of interpreters were discussed in only two trials.39,47
Pain and Symptom Management
Seven studies (Table 2) addressed pain and symptom relief through validated tools such as C-PAINAD,28 Doloplus-2,37 and the WWADR profile.26 These tools empowered nurses to initiate timely pharmacological or non-drug interventions. COSMOS34 combined training with interdisciplinary protocols and showed consistent reductions in polypharmacy and pain scores. Similarly, the STA OP! protocol32 provided a stepwise nurse-led approach with clear documentation pathways. However, only three studies reported integration with existing electronic medical records, and none conducted formal economic evaluations. Training formats were also heterogeneous, ranging from single workshops to cascade training with booster sessions.40 Although several programs reported behavioral symptom reduction, they did not always distinguish between effects attributable to pain relief versus general engagement. Training intensity ranged from single 2-hour sessions to multi-day workshops, which may explain variability in outcomes. Few studies reported fidelity monitoring or integration into existing care pathways, limiting generalizability across diverse settings. Cultural adaptation of symptom management tools was also rarely described, raising questions about applicability in non-Western contexts.
Psychosocial and Behavioral Intervention Modalities
This group included eight studies (Table 2), emphasizing sensory engagement eg, Namaste Care,41,43 reminiscence-based interaction,35 music integration,46 and technology-enhanced behavioral monitoring.45 Nurse roles varied from session facilitators to app-based monitors, and training ranged from arts workshops to task-specific protocols.
Outcomes frequently included reductions in agitation, resistance to care, and emotional withdrawal, although only three studies employed validated tools such as Cohen-Mansfield Agitation Inventory (CMAI) or Quality of Life in Dementia scale (QUALIDEM). Importantly, several interventions45,46 embedded psychosocial engagement directly into routine care rather than isolating it as a therapy, a design strength for sustainability. Nevertheless, duration and intensity of exposure were inconsistently reported. Only one study43 included structured family engagement over the long term. Overall, the evidence suggests promise but lacks standardization in outcome measurement and fails to address intervention fatigue or staff burden. In addition, details about training duration ranged from short single-session workshops to more extended modules, which may have influenced consistency of delivery. Cultural adaptation of activities such as reminiscence or music therapy was rarely described, suggesting variation in applicability across different settings.
Multicomponent and Quality Improvement Strategies
Five studies (Table 2) implemented comprehensive models combining multiple domains: communication, symptom control, staff education, and documentation audits.30,42 These interventions often emphasized a train-the-trainer or mentor-nurse model, facilitating diffusion of practices across facilities. Van den Block et al (2020), reported increased documentation and staff coaching rates,42 while Hanson et al (2019) showed improved discharge planning and hospital transition outcomes.39
Intervention Outcomes and Effectiveness
Outcomes of Advance Care Planning and Communication
Advance care planning (ACP)-focused studies showed consistently positive outcomes: care plan documentation increased (often to >75%), decisional conflict scores dropped by 20–30%, and caregiver confidence improved.31,48 Spichiger et al (2025) uniquely highlighted the importance of culturally aligned communication,47 reporting a 20-point rise in perceived communication quality (Table 3). However, a common limitation was the lack of control for prior ACP exposure or existing facility-level ACP practices, which may have influenced results. Notably, only two studies evaluated the concordance between documented care preferences and the care actually delivered at the end of life. This gap is significant, as aligning care with patient and family wishes is a core goal of ACP and a key indicator of intervention success. Without measuring this alignment, it is difficult to assess whether ACP discussions lead to meaningful changes in care delivery. While documentation rates and caregiver confidence improved consistently, only a minority of studies examined whether documented preferences were honored in practice. This represents a critical gap in ACP research. In addition, intervention delivery formats varied widely, from single structured meetings to ongoing multi-month coaching, suggesting a need for greater standardization to allow comparability across settings.
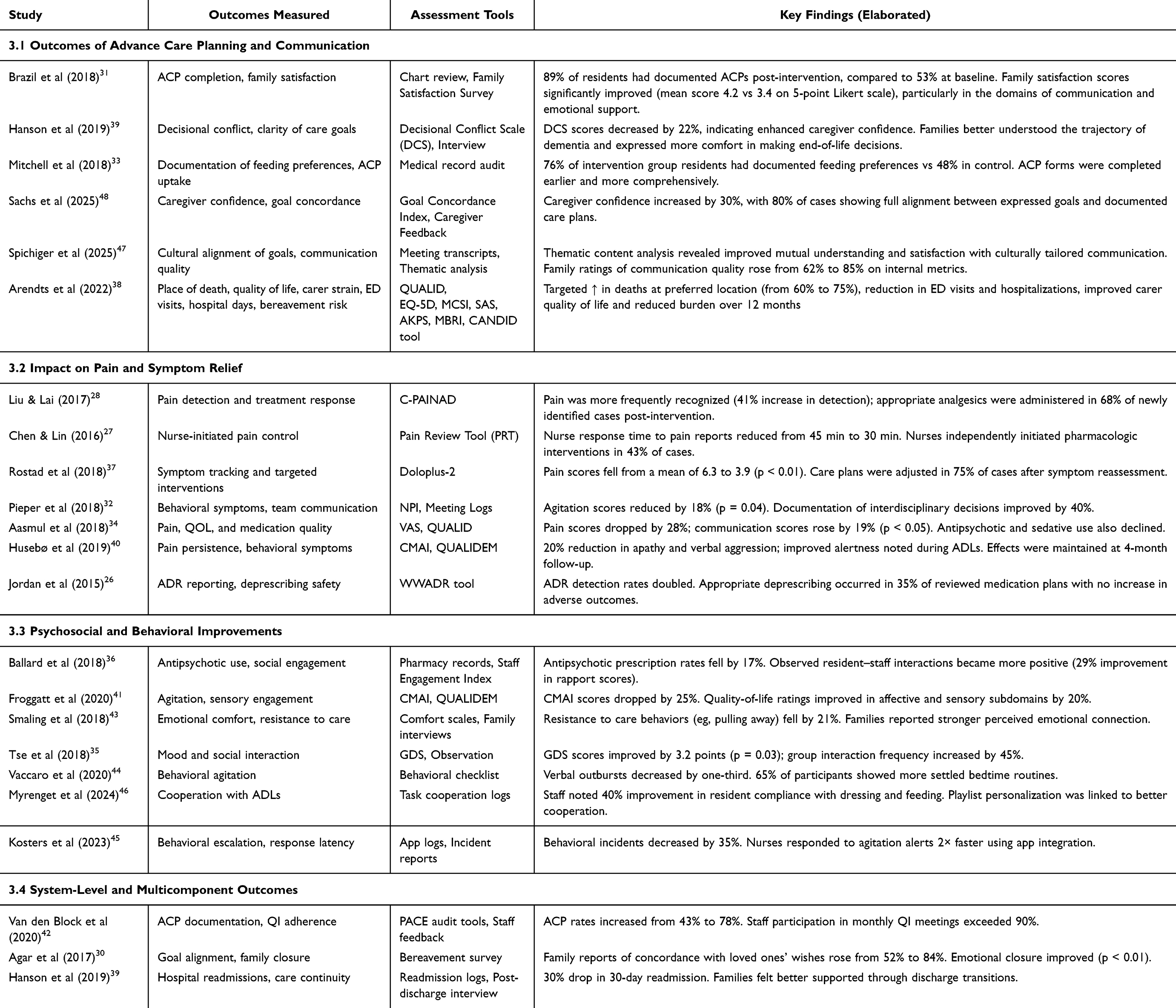 |
Table 3 Outcome Measures and Assessment Tools with Key Findings |
Impact on Pain and Symptom Relief
Pain detection improved significantly in tool-based interventions, eg, 41% increase in new cases identified post-intervention,28 with faster nurse-initiated analgesia.27 COSMOS and STA OP! programs resulted in pain score reductions ranging from 25–30% and enhanced communication scores (Table 3).32,40 However, none of the studies reported on analgesic burden, sedation-related adverse events, or detailed deprescribing frameworks. Follow-up beyond 3 months was rare, making it difficult to assess whether improvements were sustained or simply temporary effects of intensive implementation. Training approaches varied considerably, from brief orientation sessions to multi-day formats with refresher components, which may account for differences in outcomes. Only a minority of studies incorporated fidelity checks or monitoring systems, limiting clarity on whether improvements were due to intervention content or training quality. Adaptation of pain assessment tools to different linguistic or cultural contexts was largely absent, even in multicountry studies.
Psychosocial and Behavioral Improvements
Five studies (Table 3) reported significant reductions in agitation, eg, Froggatt et al, 2020 noted a 25% CMAI reduction41 and resistance to care.43 Music-based and doll therapy interventions improved task compliance and social interaction metrics.44,46 However, most relied on subjective observations, and only two blinded assessors to group allocation. Moreover, while emotional and behavioral gains were reported, resident-reported outcomes were entirely absent. No study included post-intervention staff workload or burnout measures, despite increased expectations placed on nurses to deliver structured psychosocial sessions. Training intensity also varied widely, with some studies relying on single-session protocols and others embedding repeated booster sessions. This heterogeneity complicates comparisons and raises questions about the durability of outcomes. Moreover, cultural adaptation of pain assessment tools was seldom reported, despite evidence that symptom expression may differ across populations.
System-Level and Multicomponent Outcomes
Among quality improvement models, moderate effects were noted (Table 3): reduced ER visits,38 improved transition alignment,39 and higher ACP documentation.42 These effects were most robust in stepped-wedge or audit-feedback designs. Yet, implementation science variables such as acceptability, feasibility, and cost-effectiveness were rarely addressed. No trial reported direct comparisons across sites or explored health system integration beyond the facility level.
Risk of Bias and Certainty of Evidence
Risk of Bias Assessment in Randomized Controlled Trials
Figure 2A and B illustrate the risk of bias assessments for the included randomized controlled trials using the ROB2 tool. Figure 2A (traffic light plot) displays domain-specific judgments across individual studies, with color codes representing risk levels: green for “low risk” and yellow for “some concerns.” Most studies demonstrated low risk across all domains, with some concerns noted specifically in domain D2 (bias due to deviations from intended interventions) in a subset of studies.37,44,48 Figure 2B (summary bar chart) quantifies these findings, showing that 33.3% of studies had some concerns in D2, while the remaining domains, including randomization (D1), missing outcome data (D3), measurement of outcomes (D4), and selective reporting (D5), were consistently rated as low risk in all studies. These findings reflect a generally strong methodological quality among the RCTs included in the review.
 |
Figure 2 Risk of Bias Assessment Using the Cochrane ROB2 Tool. (A) Presents a traffic light plot illustrating domain-specific risk of bias judgments across the included randomized controlled trials. Each domain, D1 (randomization), D2 (deviations from intended interventions), D3 (missing outcome data), D4 (outcome measurement), and D5 (selection of reported result), is color-coded: green indicates “low risk”, yellow denotes “some concerns”, and red (if applicable) reflects “high risk.” (B) Summarizes the proportion of studies categorized under each risk level per domain using a stacked bar chart, including the overall risk of bias. This visual overview highlights methodological strengths and areas requiring caution in interpreting study findings. |
Risk of Bias Assessment in Cluster Randomized Controlled Trials
Based on the cluster randomized controlled trials assessed (Figure 3), all studies demonstrated low risk of bias in five key domains: bias arising from the randomization process (D1), deviations from intended interventions (D2), missing outcome data (D3), measurement of outcomes (D4), and selection of the reported result (D5). However, domain D1b, concerning the timing of identification and recruitment of individual participants, revealed some concerns in three studies,36,39,42 due to issues such as delayed or staggered recruitment relative to cluster allocation. As a result, while most studies30,32,39,40,46 were judged to have an overall low risk of bias, those with concerns in D1b were rated as having some concerns overall. These findings highlight the methodological challenge of synchronizing participant recruitment with cluster assignment in such designs.
 |
Figure 3 Risk of Bias Traffic Light Plot for Cluster Randomized Controlled Trials (ROB2 Tool – Cluster Extension). Each row represents a study, and columns represent domains of bias: randomization (D1), timing of identification and recruitment (D1b), deviations from intended intervention (D2), missing outcome data (D3), measurement of outcome (D4), and selection of reported result (D5). Judgments are shown using color codes: Low risk (green) and Some concerns (yellow). |
Risk of Bias in Non-Randomized Studies
Figure 4A and B present the risk of bias assessment for non-randomized controlled trials using the ROBINS-I tool. As illustrated in Figure 4A (traffic light plot), all included studies exhibited low risk in domains related to participant selection (D2), classification of interventions (D3), and missing data (D5). However, moderate risk was frequently observed in domains such as confounding (D1), deviations from intended interventions (D4), measurement of outcomes (D6), and selection of reported results (D7). Notably, Tse et al (2018) demonstrated a serious risk in both D1 and the overall assessment,35 while the rest of the studies26–28,33,47 were judged as having moderate overall risk. Figure 4B (summary bar chart) confirms these findings, showing 100% low risk in three domains, approximately 71.4% moderate risk in D1, and 14.3% serious risk overall. These findings underscore the need for careful adjustment for confounding variables and enhanced blinding of outcome assessors in future non-randomized trials to strengthen methodological rigor.
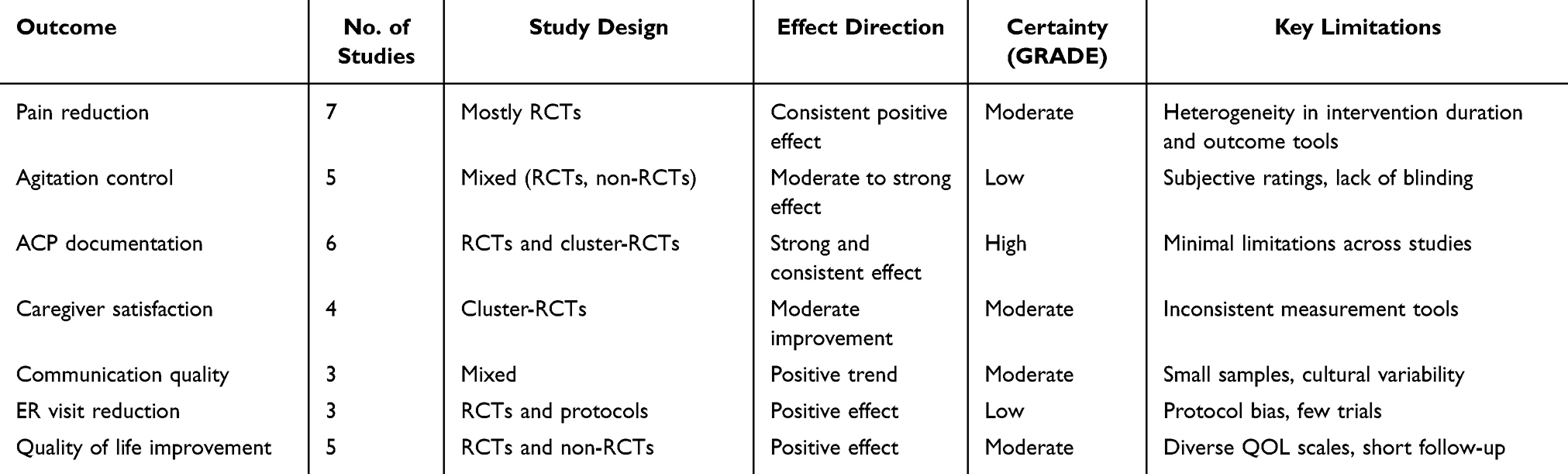 |
Table 4 GRADE Summary of Evidence for Key Outcomes |
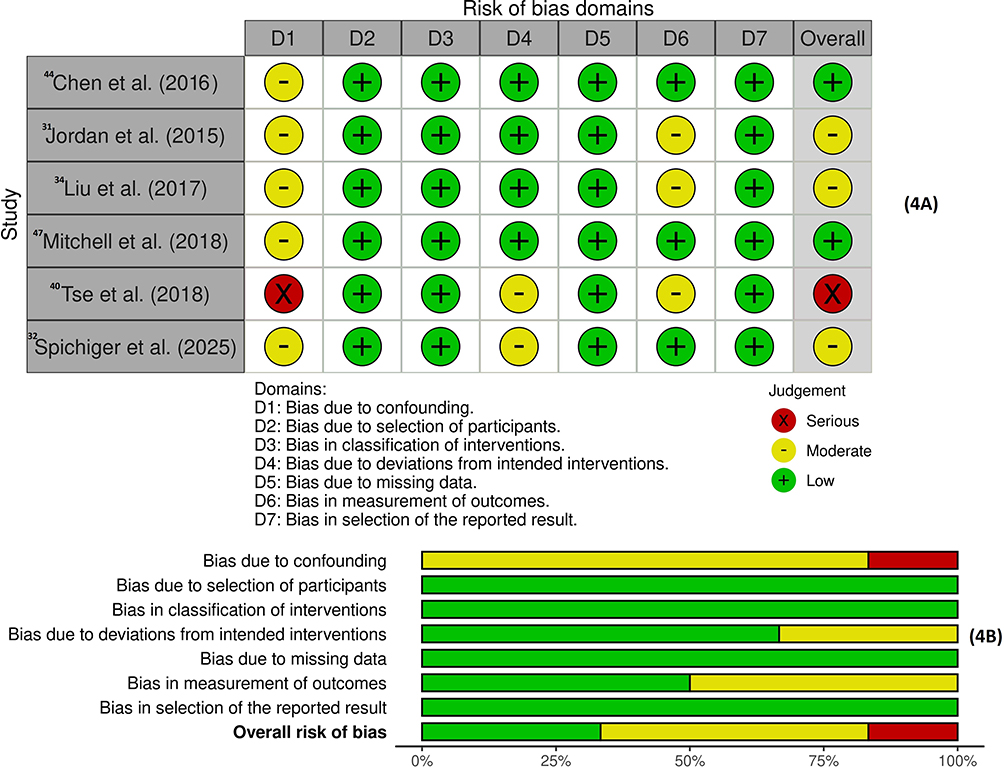 |
Figure 4 Risk of Bias Summary for Non-Randomized Studies (ROBINS-I). (A) Shows a traffic light plot of domain-level judgments across seven non-randomized studies, covering seven ROBINS-I domains: confounding, selection, classification, deviations, missing data, outcome measurement, and reporting. Green = low risk, yellow = moderate risk, red = serious risk. (B) Presents a bar chart summarizing the proportion of studies rated at each risk level across all domains and overall bias. |
Certainty of Evidence (GRADE Assessment)
While nurse-led interventions demonstrated meaningful benefits across key domains, the certainty of evidence, assessed using the GRADE framework, varied by outcome (Table 4). High certainty was observed for advance care planning completion, supported by consistent findings from well-designed RCTs. Moderate certainty was assigned to outcomes such as caregiver satisfaction and communication quality, due to some heterogeneity and reliance on subjective assessments. Pain and agitation control were supported by moderate-to-low certainty, primarily due to inconsistencies in measurement tools and limited follow-up durations. Future trials should aim for standardized outcome reporting and longer-term assessments to enhance certainty and generalizability.
Discussion
Individuals with advanced dementia face profound physical, emotional, and existential distress driven by progressive cognitive and functional decline.49,50 Addressing these needs requires proactive, nursing-led palliative care approaches tailored to communication barriers and complex symptom profiles. This systematic review highlights the critical role of nurses in delivering such care, leveraging their sustained bedside presence, clinical judgment, and familiarity with patient needs. Through person-centered interventions, nurses can facilitate meaningful goals-of-care conversations, reduce distress, and preserve dignity in the final stages of life.31,47
Evidence across reviewed studies suggests that nursing-led interventions play a pivotal role in alleviating pain, breathlessness, agitation, and psychological discomfort in advanced dementia. By embedding palliative care principles into daily routines, nurses can respond more promptly and individually to unmet needs.40,50 Importantly, these interventions align with emerging neurobiological insights into the disease: atypical pain behaviors may arise from disrupted pain-processing pathways, while agitation and affective dysregulation reflect frontotemporal and limbic dysfunction.9,51,52 Integrating such pathophysiological perspectives underscores why nursing strategies must be tailored, vigilant, and symptom-specific. Although symptom burden in dementia often mirrors that of advanced cancer, patients with dementia are less likely to receive timely symptom relief.53 The use of validated tools such as PAINAD,28 Doloplus-2,37 and STA OP!32 has enhanced the recognition of pain in non-verbal individuals and facilitated appropriate intervention. These outcomes reinforce the importance of proactive symptom surveillance by frontline nurses to reduce distress and prevent unnecessary hospitalizations.54
Although psychotropic medications and acetylcholinesterase inhibitors are frequently used to address neuropsychiatric symptoms,55 non-pharmacological strategies have gained traction. Person-centered modalities, such as reminiscence therapy, sensory stimulation, and Namaste Care, reduce agitation, improve mood, and foster engagement.56–58 In our review, music therapy, doll therapy, and multisensory programs, delivered by trained nursing staff, produced measurable behavioral gains.44,46,50 Embedding these approaches into daily routines enhances both feasibility and sustainability. Nevertheless, standardization of outcome metrics, evaluation of staff workload, and assessment of long-term benefits remain important gaps.59
Engaging families in care planning is essential to high-quality palliative dementia care. Nursing-led case conferences promote structured dialogue around prognosis, treatment57 preferences, and care goals, improving alignment between families and care teams.47,60 Such involvement enhances satisfaction, emotional preparedness, and decisional confidence.61,62 These forums also support personalized goal setting, consistent with person-centered care principles.63 However, challenges such as infrequent scheduling, poor documentation, and caregiver literacy gaps persist, particularly in resource-limited environments.31,64 Proactive use of structured communication protocols may help overcome these barriers and support consistent family involvement.
Structured caregiver support is a critical component of palliative dementia care due to the emotional and psychological burden of caregiving. Nurse-led psychoeducational programs, such as those described by Gonella et al (2022), equip caregivers with coping tools, practical skills, and emotional support.65 These interventions reduce caregiver stress and enhance engagement in care planning. Peer support groups, often facilitated by nurses, further mitigate isolation and promote resilience.19,66 Active caregiver involvement in advance care planning has also been linked to greater confidence in end-of-life decisions and reduced uncertainty.67,68 However, long-term outcomes, such as grief adjustment, financial strain, and post-bereavement support, remain underexplored and warrant further research.
While the overall findings were encouraging, the lack of standardization in intervention design and nurse training emerged as a key limitation. Programs varied widely in duration, delivery mode, and content, making it difficult to compare outcomes or replicate effective models. In many cases, the absence of fidelity monitoring and inconsistent documentation of implementation processes further weakened the strength of evidence. To enhance generalizability and scalability, future studies should adopt unified frameworks that define core intervention components, training protocols, and reporting standards.69 Moreover, digital innovations such as MoSART+, which support real-time symptom tracking and clinical decision-making, were rarely utilized, representing a missed opportunity to improve intervention efficiency and responsiveness.45
The evidence base is geographically skewed, with most trials conducted in high-income, well-resourced settings. This limits generalizability to low- and middle-income countries (LMICs), where care delivery is shaped by staff shortages, limited infrastructure, and distinct cultural contexts. Methodological issues, such as small sample sizes, short follow-up periods, and lack of blinding, further weaken the strength of evidence in some studies.35,63 Future research should focus on rigorously designed, multicenter trials in diverse contexts and apply implementation science frameworks to assess scalability, cost-effectiveness, and long-term sustainability. Long-term caregiver outcomes, including bereavement adjustment and post-care trajectories, were rarely assessed, indicating an important gap for future research.
This review highlights the need to formally embed nursing-led palliative care into standard dementia care pathways. Nurses should be equipped to initiate advanced care planning, use validated tools like PAINAD and QUALIDEM, and deliver person-centered, non-pharmacological interventions. Routine integration of case conferencing and family education can strengthen shared decision-making and caregiver preparedness. Achieving these goals requires institutional investment in nurse training, adequate staffing, and policy frameworks that support sustainable implementation (National Consensus Project, 2021). Incorporating palliative competencies into training curricula and fostering interdisciplinary collaboration are also critical for delivering comprehensive, high-quality care.
Limitations
Despite the methodological rigor and comprehensive scope of this review, several limitations must be acknowledged. A major challenge was the substantial heterogeneity in intervention components, delivery formats, training protocols, and outcome measures, which limited cross-study comparability and precluded meta-analytic synthesis. Additionally, many randomized controlled trials lacked detailed reporting on allocation concealment, blinding of outcome assessors, and fidelity monitoring, especially in cluster designs, where contamination and inconsistent timing of recruitment added further complexity. While the inclusion of non-randomized studies enhanced real-world applicability, it also introduced a higher risk of confounding and potential bias. Another key limitation lies in the geographical concentration of evidence: the majority of studies were conducted in high-income countries, limiting generalizability to low- and middle-income settings where healthcare systems, cultural practices, and nursing capacities differ significantly. The feasibility, scalability, and sustainability of nursing-led interventions in LMICs remain insufficiently explored. Moreover, important implementation science dimensions, such as cost-effectiveness, intervention acceptability, and system-level integration, were rarely assessed, limiting insights into real-world translation. Lastly, caregiver-centered outcomes such as long-term psychological health, bereavement adjustment, and economic burden were underreported, highlighting the need for more comprehensive outcome evaluation in future studies.
Future Scope
Building on these conclusions, future research should focus on developing standardized, scalable models of nursing-led palliative care that are adaptable across diverse clinical and cultural contexts. Multicenter trials with rigorous designs, longer follow-up periods, and mixed-method evaluations are needed to assess the long-term effectiveness and generalizability of these interventions. Culturally sensitive frameworks should be embedded to ensure relevance in low- and middle-income countries, where healthcare resources and caregiving structures may differ substantially. There is also a pressing need for economic evaluations to determine cost-effectiveness, resource use, and return on investment, key considerations for health system adoption. Digital technologies, including real-time symptom tracking, decision-support systems, and mobile applications, represent underutilized tools that could enhance nursing efficiency and care personalization. In addition, future studies should prioritize caregiver-reported outcomes and include follow-up into the post-bereavement period to fully capture the psychosocial impact of interventions. Finally, integrating implementation science frameworks, such as hybrid effectiveness-implementation models, can support the translation of evidence into practice. By evaluating real-world feasibility, acceptability, and fidelity, these approaches will be essential for informing policy, workforce planning, and sustainable care delivery models.
Conclusion
This systematic review demonstrates that nurse-led palliative care interventions play a central role in alleviating pain, agitation, communication difficulties, and psychological distress, while also supporting advance care planning and caregiver engagement in advanced dementia. Evidence across studies shows consistent improvements in these domains, though evidence on long-term caregiver outcomes, such as bereavement adjustment, remains limited. Structured tools such as PAINAD, Doloplus-2, and STA OP! were instrumental in enabling timely, accurate assessment and management of distressing symptoms, particularly in non-verbal patients. Notably, interventions integrated into routine nursing workflows proved more feasible and sustainable than isolated or externally driven programs. However, wide variability in intervention design, training models, and outcome reporting limits the comparability of findings and challenges replication. These results reinforce the central role of nurses as frontline providers of person-centered, evidence-based palliative care and underscore the importance of institutional investment in standardized, scalable models. Embedding nursing-led palliative approaches into dementia care pathways and national policies will be essential for ensuring dignity, comfort, and improved outcomes for this vulnerable population. Beyond immediate clinical benefits, these findings advance the theoretical understanding of nursing leadership in dementia care and highlight practical directions for policy, education, and research integration.
Funding
Article Processing Charge (APC) was funded by QU-Health Qatar University.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. WHO. Global Status Report on the Public Health Response to Dementia. Geneva: Switzerland: WHO; 2021.
2. Culberson JW, Kopel J, Sehar U, Reddy PH. Urgent needs of caregiving in ageing populations with Alzheimer’s disease and other chronic conditions: support our loved ones. Ageing Res Rev. 2023;90:102001. doi:10.1016/j.arr.2023.102001
3. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396(10248):413–446. doi:10.1016/S0140-6736(20)30367-6
4. Catala-Lopez F, Collaborators GDF, Vollset SE. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. 2022;7(2):e105–e125. doi:10.1016/S2468-2667(21)00249-8
5. Gaugler J, James B, Johnson T, et al. Alzheimer’s disease facts and figures. Alzheimers Dement. 2022;18(4):700–789.
6. Kenigsberg P-A, Aquino J-P, Berard A, et al. Dementia beyond 2025: knowledge and uncertainties. Dementia. 2016;15(1):6–21. doi:10.1177/1471301215574785
7. Eisenmann Y, Golla H, Voltz R, Perrar KM. Palliative care in advanced dementia. Front Psychiatry. 2020;11:699. doi:10.3389/fpsyt.2020.00699
8. Browne B, Kupeli N, Moore KJ, Sampson EL, Davies N. Defining end of life in dementia: a systematic review. Palliat Med. 2021;35(10):1733–1746. doi:10.1177/02692163211025457
9. Yao K, Wang S, Xu Z, et al. Mechanisms of comorbidity between Alzheimer’s disease and pain. Alzheimers Dement. 2025;21(2):e14605. doi:10.1002/alz.14605
10. Palermo S, Benedetti F, Costa T, Amanzio M. Pain anticipation: an activation likelihood estimation meta‐analysis of brain imaging studies. Human Brain Mapp. 2015;36(5):1648–1661. doi:10.1002/hbm.22727
11. Di Gregorio F, Battaglia S. The intricate brain–body interaction in psychiatric and neurological diseases. Adv Clin Exp Med. 2024;33(4):321–326. doi:10.17219/acem/185689
12. World Health Organization. Palliative Care. Geneva: WHO; 2020.
13. Lopez RP, Kris AE, Rossmassler SC. Nursing leadership and palliative care in long-term care for residents with advanced dementia. Nurs Clin North Am. 2022;57(2):259–271. doi:10.1016/j.cnur.2022.02.006
14. Walsh SC, Murphy E, Devane D, et al. Palliative care interventions in advanced dementia. Cochrane Database Syst Rev. 2021;9(9). doi:10.1002/14651858.CD011513.pub3.
15. Pocknell CE, Hartigan I, Brady N, et al. Education and training for the delivery of person-centred palliative care in advanced dementia in nursing homes: a scoping review protocol. OSF Registries. 2024. doi:10.17605/OSF.IO/X9W5T
16. David L, Popa SL, Barsan M, et al. Nursing procedures for advanced dementia: traditional techniques versus autonomous robotic applications. Exp Ther Med. 2022;23(2):124. doi:10.3892/etm.2021.11047
17. Cabrera E, Sutcliffe C, Verbeek H, et al. Non-pharmacological interventions as a best practice strategy in people with dementia living in nursing homes. A systematic review. Eur Geriatric Med. 2015;6(2):134–150. doi:10.1016/j.eurger.2014.06.003
18. Endsley S, Main R. Palliative care in advanced dementia. Am Family Phys. 2019;99(7):456–458.
19. Navia RO, Constantine LA. Palliative care for patients with advanced dementia. Nurs2024. 2022;52(3):19–26.
20. Wang T, Tan J-YB, Liu X-L, Zhao I. Barriers and enablers to implementing clinical practice guidelines in primary care: an overview of systematic reviews. BMJ Open. 2023;13(1):e062158. doi:10.1136/bmjopen-2022-062158
21. Evans CJ, Harding R, Higginson IJ. MORECare ‘Best practice’in developing and evaluating palliative and end-of-life care services: a meta-synthesis of research methods for the MORECare project. Palliative Med. 2013;27(10):885–898. doi:10.1177/0269216312467489
22. Huang KH, Saragih ID, Suarilah I, Son NT, Lee B-O. Systematic review and meta-analysis of effects of nurse-led intervention for people with dementia. Nurs Res. 2023;72(6):430–438. doi:10.1097/NNR.0000000000000685
23. Hendriks SA, Smalbrugge M, Galindo-Garre F, Hertogh CM, van der Steen JT. From admission to death: prevalence and course of pain, agitation, and shortness of breath, and treatment of these symptoms in nursing home residents with dementia. J Am Med Directors Assoc. 2015;16(6):475–481. doi:10.1016/j.jamda.2014.12.016
24. Knapp M, Iemmi V, Romeo R. Dementia care costs and outcomes: a systematic review. Int J Geriatric Psychiatry. 2013;28(6):551–561. doi:10.1002/gps.3864
25. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;29(372):n71. doi:10.1136/bmj.n71
26. Jordan S, Gabe-Walters ME, Watkins A, et al. Nurse-led medicines’ monitoring for patients with dementia in care homes: a pragmatic cohort stepped wedge cluster randomised trial. PLoS One. 2015;10(10):e0140203. doi:10.1371/journal.pone.0140203
27. Chen Y-H, Lin L-C. Ability of the pain recognition and treatment (PRT) protocol to reduce expressions of pain among institutionalized residents with dementia: a cluster randomized controlled trial. Pain Manage Nurs. 2016;17(1):14–24. doi:10.1016/j.pmn.2015.08.003
28. Liu JY, Lai CK. Implementation of observational pain management protocol for residents with dementia: a cluster‐RCT. J Am Geriatr Soc. 2017;65(3):e56–e63. doi:10.1111/jgs.14763
29. Hanson LC, Zimmerman S, Song M-K, et al. Effect of the goals of care intervention for advanced dementia: a randomized clinical trial. JAMA Intern Med. 2017;177(1):24–31. doi:10.1001/jamainternmed.2016.7031
30. Agar M, Luckett T, Luscombe G, et al. Effects of facilitated family case conferencing for advanced dementia: a cluster randomised clinical trial. PLoS One. 2017;12(8):e0181020. doi:10.1371/journal.pone.0181020
31. Brazil K, Carter G, Cardwell C, et al. Effectiveness of advance care planning with family carers in dementia nursing homes: a paired cluster randomized controlled trial. Palliative Med. 2018;32(3):603–612. doi:10.1177/0269216317722413
32. Pieper MJ, van der Steen JT, Francke AL, Scherder EJ, Twisk JW, Achterberg WP. Effects on pain of a stepwise multidisciplinary intervention (STA OP!) that targets pain and behavior in advanced dementia: a cluster randomized controlled trial. Palliative Med. 2018;32(3):682–692. doi:10.1177/0269216316689237
33. Mitchell SL, Shaffer ML, Cohen S, Hanson LC, Habtemariam D, Volandes AE. An advance care planning video decision support tool for nursing home residents with advanced dementia: a cluster randomized clinical trial. JAMA Intern Med. 2018;178(7):961–969. doi:10.1001/jamainternmed.2018.1506
34. Aasmul I, Husebo BS, Sampson EL, Flo E. Advance care planning in nursing homes–improving the communication among patient, family, and staff: results from a cluster randomized controlled trial (COSMOS). Front Psychol. 2018;9:2284. doi:10.3389/fpsyg.2018.02284
35. Tse MM, Lau JL, Kwan R, et al. Effects of play activities program for nursing home residents with dementia on pain and psychological well‐being: cluster randomized controlled trial. Geriatrics Gerontol Int. 2018;18(10):1485–1490. doi:10.1111/ggi.13509
36. Ballard C, Corbett A, Orrell M, et al. Impact of person-centred care training and person-centred activities on quality of life, agitation, and antipsychotic use in people with dementia living in nursing homes: a cluster-randomised controlled trial. PLoS Med. 2018;15(2):e1002500. doi:10.1371/journal.pmed.1002500
37. Rostad HM, Utne I, Grov EK, Småstuen MC, Puts M, Halvorsrud L. The impact of a pain assessment intervention on pain score and analgesic use in older nursing home residents with severe dementia: a cluster randomised controlled trial. Int J Nursing Stud. 2018;84:52–60. doi:10.1016/j.ijnurstu.2018.04.017
38. Arendts G, Chenoweth L, Hayes B, et al. CELPI: trial protocol for a randomised controlled trial of a Carer End of Life Planning Intervention in people dying with dementia. BMC Geriatr. 2022;22(1):869. doi:10.1186/s12877-022-03534-1
39. Hanson LC, Kistler CE, Lavin K, et al. Triggered palliative care for late-stage dementia: a pilot randomized trial. J Pain Sympt Manage. 2019;57(1):10–19. doi:10.1016/j.jpainsymman.2018.10.494
40. Husebø BS, Ballard C, Aarsland D, et al. The effect of a multicomponent intervention on quality of life in residents of nursing homes: a randomized controlled trial (COSMOS). J Am Med Directors Assoc. 2019;20(3):330–339. doi:10.1016/j.jamda.2018.11.006
41. Froggatt K, Best A, Bunn F, et al. A group intervention to improve quality of life for people with advanced dementia living in care homes: the Namaste feasibility cluster RCT. Health Technol Assess. 2020;24(6):1. doi:10.3310/hta24060
42. Van den Block L, Honinx E, Pivodic L, et al. Evaluation of a palliative care program for nursing homes in 7 countries: the PACE cluster-randomized clinical trial. JAMA Intern Med. 2020;180(2):233–242. doi:10.1001/jamainternmed.2019.5349
43. Smaling HJ, Joling KJ, van de Ven PM, et al. Effects of the Namaste care family programme on quality of life of nursing home residents with advanced dementia and on family caregiving experiences: study protocol of a cluster-randomised controlled trial. BMJ open. 2018;8(10):e025411. doi:10.1136/bmjopen-2018-025411
44. Vaccaro R, Molteni V, Molteni V, et al. Doll therapy intervention for women with dementia living in nursing homes: a randomized single-blind controlled trial protocol. Trials. 2020;21:1–12. doi:10.1186/s13063-020-4050-8
45. Kosters J, Janus SI, van den Bosch KA, et al. Soundscape awareness intervention reduced neuropsychiatric symptoms in nursing home residents with dementia: a cluster-randomized Trial with MoSART+. J Am Med Directors Assoc. 2023;24(2):192–198.e5. doi:10.1016/j.jamda.2022.11.010
46. Myrenget ME, Rustøen T, Myskja A, et al. The effect of a music-based caregiving intervention on pain intensity in nursing home patients with dementia: a cluster-randomized controlled study. Pain. 2024;165(7):1550–1558. doi:10.1097/j.pain.0000000000003156
47. Spichiger F, Koppitz AL, Riese F, et al. Person profile dementia intervention in long-term care: a stepped-wedge cluster-randomized trial. J Am Med Directors Assoc. 2025;26(1):105351. doi:10.1016/j.jamda.2024.105351
48. Sachs GA, Johnson NM, Gao S, et al. Palliative care program for community-dwelling individuals with dementia and caregivers: the IN-PEACE randomized clinical trial. JAMA. 2025;333:962–971.
49. Dening KH, Scates C, Lloyd-Williams M. Palliative care in dementia: a fragmented pathway? Int J Palliative Nurs. 2018;24(12):585–596. doi:10.12968/ijpn.2018.24.12.585
50. Van der Steen JT, Radbruch L, Hertogh CM, et al. White paper defining optimal palliative care in older people with dementia: a Delphi study and recommendations from the European Association for Palliative Care. Palliative Med. 2014;28(3):197–209. doi:10.1177/0269216313493685
51. Di Fazio C, Scaliti E, Stanziano M, et al. rTMS for enhancing cognitive reserve: a case report. Brain Disorders. 2025;18:100221. doi:10.1016/j.dscb.2025.100221
52. Palermo S, Di Fazio C, Scaliti E, Stanziano M, Nigri A, Tamietto M. Cortical excitability and the aging brain: toward a biomarker of cognitive resilience. Front Psychol. 2025;16:1542880. doi:10.3389/fpsyg.2025.1542880
53. Volicer L. Review of programs for persons facing death with dementia. Healthcare. 2019;7(2):62. doi:10.3390/healthcare7020062
54. Mitchell SL, Palmer JA, Volandes AE, Hanson LC, Habtemariam D, Shaffer ML. Level of care preferences among nursing home residents with advanced dementia. J Pain Sympt Manage. 2017;54(3):340–345. doi:10.1016/j.jpainsymman.2017.04.020
55. Knight R, Khondoker M, Magill N, Stewart R, Landau S. A systematic review and meta-analysis of the effectiveness of acetylcholinesterase inhibitors and memantine in treating the cognitive symptoms of dementia. Dementia Geriatric Cognit Disord. 2018;45(3–4):131–151. doi:10.1159/000486546
56. Yanagida N, Yamaguchi T, Matsunari Y. Evaluating the Impact of Reminiscence Therapy on Cognitive and Emotional Outcomes in Dementia Patients. J Personal Med. 2024;14(6):629. doi:10.3390/jpm14060629
57. Yous ML, Ploeg J, Kaasalainen S, McAiney C. Namaste care delivered by caregivers of community‐dwelling older adults with moderate to advanced dementia: a mixed methods study protocol. J Adv Nurs. 2021;77(2):1027–1036. doi:10.1111/jan.14623
58. Lee KH, Lee JY, Kim B. Person-centered care in persons living with dementia: a systematic review and meta-analysis. Gerontologist. 2022;62(4):e253–e264. doi:10.1093/geront/gnaa207
59. Sieradzki B Addressing the strengths and gaps in education and training for long-term care staff who provide direct care to individuals living with dementia [Master’s thesis]. Winnipeg (MB): University of Manitoba; 2017. Available from: https://mspace.lib.umanitoba.ca/server/api/core/bitstreams/673e9041-5013-482b-9101-909d6abe28ca/content
60. Balconi M, Angioletti CA-KR-L, Allegretta K-R-RA, Angioletti L, Crivelli D, Balconi CA-LA-M. Why a dynamic multicomponent model of decision making: some milestones and a preliminary tool. Neuropsychol Trends. 2023;33(33):9–16. doi:10.7358/neur-2023-033-balm
61. Mbakile-Mahlanza L, Van Der Ploeg ES, Busija L, Camp C, Walker H, O’Connor DW. A cluster-randomized crossover trial of Montessori activities delivered by family carers to nursing home residents with behavioral and psychological symptoms of dementia. Int Psychogeriatrics. 2020;32(3):347–358. doi:10.1017/S1041610219001819
62. Tasseron-Dries PE, Smaling HJ, Nakanishi M, Achterberg WP, van der Steen JT. What are best practices for involving family caregivers in interventions aimed at responsive behaviour stemming from unmet needs of people with dementia in nursing homes: a scoping review. BMJ open. 2023;13(12):e071804. doi:10.1136/bmjopen-2023-071804
63. Luckett T, Chenoweth L, Phillips J, et al. A facilitated approach to family case conferencing for people with advanced dementia living in nursing homes: perceptions of palliative care planning coordinators and other health professionals in the IDEAL study. Int Psychogeriatrics. 2017;29(10):1713–1722. doi:10.1017/S1041610217000977
64. Tieman J, Gravier S, Erny-Albrecht K Palliative care guidance in aged care: role of palliAGED. In:
65. Gonella S, Mitchell G, Bavelaar L, et al. Interventions to support family caregivers of people with advanced dementia at the end of life in nursing homes: a mixed-methods systematic review. Palliative Med. 2022;36(2):268–291. doi:10.1177/02692163211066733
66. Hines S, McCrow J, Abbey J, et al. The effectiveness and appropriateness of a palliative approach to care for people with advanced dementia: a systematic review. JBI Evidence Synth. 2011;9(26):960–1131.
67. Dixon J, Karagiannidou M, Knapp M. The effectiveness of advance care planning in improving end-of-life outcomes for people with dementia and their carers: a systematic review and critical discussion. J Pain Sympt Manage. 2018;55(1):132–150.e1. doi:10.1016/j.jpainsymman.2017.04.009
68. Huang H-L, Lu W-R, Liu C-L, Chang H-J. Advance care planning information intervention for persons with mild dementia and their family caregivers: impact on end-of-life care decision conflicts. PLoS One. 2020;15(10):e0240684. doi:10.1371/journal.pone.0240684
69. Webster L, Groskreutz D, Grinbergs-Saull A, et al. Core outcome measures for interventions to prevent or slow the progress of dementia for people living with mild to moderate dementia: systematic review and consensus recommendations. PLoS One. 2017;12(6):e0179521. doi:10.1371/journal.pone.0179521
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Feasibility Study of Individuals Living at Home with Alzheimer’s Disease and Related Dementias: Utilization of Visual Mapping Assistive Technology to Enhance Quality of Life and Reduce Caregiver Burden
Han SS, White K, Cisek E
Clinical Interventions in Aging 2022, 17:1885-1892
Published Date: 23 December 2022
Implementing the Hospice Shared Care Model to Support a Patient with Advanced Colon Cancer: A Case Report
Qiao S, Zhang X, Xiang W, Yao L, Xian X
Patient Preference and Adherence 2023, 17:1019-1024
Published Date: 14 April 2023
Caregiver Burden in Bladder Cancer Patients with Urinary Diversion Post-Radical Cystectomy and the Need for Comprehensive Nursing Education: A Narrative Literature
Zhang T, Qi X
Journal of Multidisciplinary Healthcare 2024, 17:3825-3834
Published Date: 7 August 2024
Effectiveness of a Short-Term Advance Care Planning Intervention (VOICE) for Dialysis Patients with ESRD: A Randomized Controlled Trial
Xu F, Cheng S, Shu P, Liang Y, Chen J, Bai H
Patient Preference and Adherence 2025, 19:4191-4206
Published Date: 22 December 2025
Nursing Interventions for Symptom Management in Breast Cancer: A Systematic Review
Trisyani Y, Nuraeni A, Anna A, Priambodo AP, Sugiharto F
International Journal of Women's Health 2026, 18:573338
Published Date: 4 February 2026