Back to Journals » International Journal of General Medicine » Volume 19
Novel Clinically Validated Machine Learning Model for Early Pregnancy Loss in Recurrent Spontaneous Abortion: Integrating Serum Autoantibodies and Ultrasonic Parameters
Authors Li J, Yang Y, Li T, Sun B, Zhang Y
Received 21 October 2025
Accepted for publication 18 December 2025
Published 8 January 2026 Volume 2026:19 572373
DOI https://doi.org/10.2147/IJGM.S572373
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Jing Li,1 Yang Yang,2 Teng Li,1 Bowei Sun,3 Yongai Zhang1
1Department of Nursing and Rehabilitation College, Xi’an Medical University, Xi’an, Shaanxi, 710021, People’s Republic of China; 2Department of Reproductive Medicine, Xi’an People’s Hospital (Xi’an Fourth Hospital), Xi’an, Shaanxi, 710004, People’s Republic of China; 3Department of the School of Foreign Languages, Xian Medical University, Xi’an, Shaanxi, 710021, People’s Republic of China
Correspondence: Yongai Zhang, Email [email protected]
Objective: To explore the correlation between autoantibodies, ultrasonic endometrial receptivity parameters and early miscarriage in recurrent spontaneous abortion (RSA) patients during subsequent pregnancies, and to establish and validate a predictive model for early miscarriage.
Methods: A retrospective analysis was conducted on RSA patients who visited Xi’an People’s Hospital from January 2019 to December 2024. Patients were randomly divided into a training set (70%, n=412) and a validation set (30%, n=177). Baseline data, serum autoantibodies (anti-β 2-glycoprotein 1 antibody [aβ 2-GP1], thyroglobulin antibody [TgAb], anti-sperm antibody [AsAb], anti-cardiolipin antibody [ACA]) and ultrasonic parameters (resistance index [RI], endometrial thickness, endometrial volume, vascularization index [VI], vascularization flow index [VFI]) were collected. Multiple machine learning models (logistic regression [LR], XGBoost, random forest, etc.) were developed. Model performance was evaluated using area under the receiver operating characteristic curve (AUC), accuracy, and other metrics. A nomogram was constructed based on the optimal model.
Results: The abortion subgroup had significantly higher positive rates of aβ 2-GP1, TgAb, ACA and RI, but lower endometrial thickness, endometrial volume, VI and VFI than the normal subgroup (all P< 0.05). Eight variables (aβ 2-GP1, TgAb, AsAb, RI, endometrial thickness, endometrial volume, VI, VFI) were identified as candidate predictors. The LR model was optimal, with AUC=0.94 and accuracy=0.93 in the training set, and AUC=0.92 and accuracy=0.90 in the validation set. The nomogram based on this model showed good alignment between predicted probabilities and actual outcomes.
Conclusion: A practical and accurate LR model for predicting early miscarriage in RSA patients was established using autoantibodies and ultrasonic parameters. It can assist in clinical risk stratification and individualized intervention. Future multicenter prospective studies with larger samples and more variables are needed to optimize the model.
Keywords: recurrent spontaneous abortion (RSA), early miscarriage, autoantibody, ultrasonic parameter, machine learning, prediction model
Introduction
Recurrent spontaneous abortion (RSA) refers to women who experience multiple (≥2) miscarriages during pregnancy.1 Previous studies have reported that the incidence of RSA ranges from 1% to 5%.2,3 Many women develop psychological issues such as anxiety and depression after experiencing RSA, which not only affects their physical health but also imposes a significant burden on their mental state, exerting negative impacts on both families and society.
The etiologies of RSA mainly include chromosomal or genetic abnormalities, anatomical structural abnormalities (including congenital and acquired types), autoimmune diseases, prethrombotic states (including hereditary and acquired types), endocrine factors, infectious factors, male factors, environmental factors, and psychological factors.4–9 A considerable proportion of RSA patients have unclear specific causes and pathogenesis of the disease, thus being classified as “unexplained recurrent spontaneous abortion (URA)”10 Despite the availability of extensive screening and diagnostic tests with current technologies, more than 40% of patients still have unknown causes of miscarriage.10,11 These patients face a risk of miscarriage in subsequent pregnancies, especially those with a history of 3 consecutive miscarriages, for whom the recurrence risk is as high as 33%.12
In recent years, studies have established models for predicting pregnancy outcomes based on RSA-related factors, but different international guidelines recommend different prediction models. For instance, the 2012 guidelines of the American Society for Reproductive Medicine (ASRM) recommend the Lund model.13 The latest ESHRE guidelines propose the Kolte & Westergaard model.14 However, these models have limitations such as incomplete risk factors, single modeling methods, and lack of internal or external validation, leading to room for improvement in their predictive performance.
Furthermore, with the evolution of RSA definitions, changes in demographic characteristics, advances in etiological research, and improvements in treatment methods, there is an urgent clinical need to develop more accurate and practical risk prediction models. These models aim to achieve risk stratification for patients, identify high-risk populations, and provide early intervention and individualized treatment for these groups, thereby effectively preventing recurrent miscarriages. An ideal model should include a small number of easily accessible variables, with clinical practicality and excellent predictive performance.
Establishing a live birth prediction model for RSA patients requires comprehensive consideration of multiple factors, including women’s age, history of previous miscarriages, genetic factors, lifestyle, environmental factors, and male factors.15,16 In recent years, with the further development of big data and artificial intelligence, technologies such as machine learning and neural networks have demonstrated significant advantages in establishing precision medicine modeling methods.17,18 It is expected that through continuous iterative training of machine learning algorithms and neural networks, the risk of early miscarriage in RSA patients during subsequent pregnancies can be accurately predicted to guide clinical practice.
Recent studies in reproductive immunology have shown that more than half of RSA cases are associated with immune dysfunction.4 The immunopathological changes leading to miscarriage vary among different factors, and immune miscarriage can be divided into autoimmune RSA (AI-RSA) and alloimmune RSA (Allo-RSA).19,20 Among these, AI-RSA includes the production of tissue-nonspecific autoantibodies (such as anti-phospholipid antibodies [aPL], anti-nuclear antibodies [ANA], and anti-DNA antibodies) and tissue-specific autoantibodies (such as anti-sperm antibodies [AsAb] and anti-thyroid antibodies [ATA]).
Existing studies have indicated that 5% to 20% of RSA patients exhibit abnormal expression of tissue-nonspecific autoantibodies (eg, aPL) in clinical practice, and the live birth rate of untreated patients in subsequent pregnancies decreases to 10%.21–23 In view of this, the present study intends to explore the correlation between autoantibodies and early miscarriage in RSA patients during subsequent pregnancies. It also attempts to establish and validate a prediction model for early miscarriage in pregnant RSA patients based on autoantibodies and ultrasonic endometrial receptivity parameters, aiming to better assist in guiding clinical decision-making and fertility guidance for RSA patients.
Materials and Methods
Study Subjects
A retrospective analysis was performed on RSA patients who visited the Department of Reproductive Medicine of Xi’an People’s Hospital (Xi’an Fourth Hospital) from January 2019 to December 2024. Inclusion criteria for RSA patients was as follows: (1) History of ≥2 previous spontaneous miscarriages; (2) Current menopause duration of 6~12 weeks, with positive results for urinary human chorionic gonadotropin (hCG) and serum hCG; (3) Ultrasound examination indicating intrauterine pregnancy and singleton gestation. Exclusion criteria: (1) Complications with other diseases that may cause uterine abnormalities, such as adenomyosis, intrauterine adhesions, inflammation, and tumors; (2) Diseases affecting hemodynamics, including abnormal thyroid function, hypertension, diabetes mellitus, and arrhythmia. This study was approved by the Medical Ethics Committee of Xi’an People’s Hospital, and all patients signed the informed consent form. The process of patient enrollment and predictive model construction is detailed in Figure 1.
 |
Figure 1 Flowchart of Patient Enrollment and Predictive Model Construction & Validation. |
Patients were divided into the live birth group and the miscarriage group based on pregnancy outcomes. Patients with no obvious fetal malformations and normal full-term delivery were assigned to the live birth group, while those with a clear diagnosis of embryonic arrest were included in the miscarriage group. According to the standards of the Society of Radiologists in Ultrasound (SRU), embryonic arrest can only be diagnosed by ultrasound if any of the following criteria are met: (1) Crown-rump length (CRL) ≥7 mm without cardiac activity; (2) Mean gestational sac diameter (MGSD) ≥25 mm without detectable fetal bud; (3) Gestational sac with no yolk sac detected by ultrasound, and no embryo with cardiac activity observed in the re-examination after ≥2 weeks; (4) Gestational sac with a detectable yolk sac by ultrasound, and no embryo with cardiac activity observed in the re-examination after ≥11 days.
In accordance with the routine clinical diagnosis and treatment protocols of the department, RSA patients underwent three transvaginal ultrasound examinations for monitoring uterine artery hemodynamics at 6–8 weeks, 8–10 weeks, and 10–12 weeks of gestation. Patients who did not undergo transvaginal ultrasound for uterine artery blood flow measurement during pregnancy were excluded.
Collection and Detection of Clinical Baseline Data and Serum-Related Indicators
Baseline data of all included patients, such as age, Body Mass Index (BMI), and comorbidities (hypertension, diabetes mellitus, dyslipidemia), were collected through the electronic medical record system. A 4 mL sample of fasting venous blood was collected from each subject in the morning (on the day after diagnosis confirmation). The serum was separated by centrifugation for 10 minutes and stored in a −80°C refrigerator. The concentrations of various indicators were determined using the enzyme-linked immunosorbent assay (ELISA) method, with strict adherence to the kit instructions. The instruments and kits used were as follows: Centrifuge (Model: 5757, Shanghai Yuanyao Biotechnology Co., Ltd).; Microplate reader (Model: 20220204588, Shanghai Yuanyao Biotechnology Co., Ltd).; Anti-β2-glycoprotein 1 antibody (aβ2-GP1) kit (Catalogue No.: FY-B021407, Shanghai Fuyu Biotechnology Co., Ltd).; Thyroglobulin antibody (TgAb) kit (Catalogue No.: ZK-E1024, Shanghai Zhenke Biotechnology Co., Ltd).; Anti-sperm antibody (AsAb) kit (Catalogue No.: RE52001, Shenzhen Kerunda Biotechnology Co., Ltd., acting as an agent for products of IBL GmbH, Germany); Anti-cardiolipin antibody (ACA) kit (Catalogue No.: FS-E1106, Shanghai Fusheng Industrial Co., Ltd).
Monitoring and Acquisition of Ultrasonic Parameters
An HD-15 color Doppler ultrasound diagnostic instrument manufactured by Philips (USA) was used, with a transvaginal ultrasound probe frequency of 4–8 MHz. The specific examination procedures were as follows: Examination of the uterus, uterine cavity morphology, and the size, location, and morphology of the gestational sac; observation of the presence of yolk sac, fetal bud, and primitive heart tube pulsation; and assessment of fetal bud development and the morphology and size of bilateral ovaries.
Monitoring of hemodynamic parameters of the left and right uterine arteries separately. After the uterine artery branches off from the internal iliac artery, a transverse section was obtained at the level of the internal cervical os. Multiple tortuous arterial branches were generally detectable, and the ascending branch was the arterial blood flow supplying the uterus. The branch vessel with blood flow away from the probe and abundant blood flow signals was selected as far as possible. The color Doppler was adjusted appropriately to ensure good display of blood flow signals without overflow or loss, and the sampling gate width was set to 2 mm. The sampling line was aligned with the direction of blood flow, with an angle of <30° between the sampling line and the blood flow direction, and the blood flow velocity was greater than 50 m/s. Six consecutive stable cardiac cycle spectra were recorded. The automatic spectrum envelope and calculation function of the system were activated to measure and record the resistance index (RI), pulsatility index (PI), and peak uterine artery systolic/end-diastolic velocity (S/D) of the left and right uterine arteries separately, and the average values were calculated. The relationship between the uterine artery blood flow resistance parameters in early pregnancy and different pregnancy outcomes of RSA patients was analyzed. All parameters were measured three times by a professional technician for each patient.
Establishment of the Prediction Model and Evaluation of Predictive Efficacy
All included patients were randomly divided into a training set and a validation set at a ratio of 7:3. The occurrence of recurrent miscarriage in RSA patients was used as the outcome variable to establish the prediction model.
In this study, R software (Version 4.2.3) was used, with R packages including “autoReg”, “XGBoost”, “e1071”, “randomForest”, and “caret” to develop and test multiple models. These models included decision tree (DT), elastic net (Enet), logistic regression(LR), multi-layer perceptron (MLP), random forest (RF), regularized support vector machine (Rsvm), and extreme gradient boosting (Xgboost). When constructing the classic machine learning prediction models, univariate analysis was first performed in the training cohort to screen factors related to the “outcome variable”. Subsequently, factors with P<0.10 in the univariate analysis were included in the stepwise binary logistic regression analysis. Due to the small number of original independent variables in this study and the potential positive effect of variables with low importance on model training, all feature variables were included in the training process of the prediction model.
All machine learning prediction models were optimized through 5-fold cross-validation or hyperparameter tuning. The “pROC” package was used to plot the receiver operating characteristic (ROC) curve and calculate the area under the curve (AUC). The AUC was used as the comprehensive evaluation index of the model, and the Delong method was adopted to compare the AUC values of different models. In addition, the predictive performance of each model was further evaluated from multiple dimensions, including accuracy, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and F1-score. A two-tailed P-value <0.05 was considered statistically significant.
Statistical Analysis
GraphPad Prism software was used for statistical analysis. Baseline characteristics were expressed as median and interquartile range. The Mann–Whitney U-test was used for nonparametric testing to analyze the differences in baseline characteristics, age, and BMI between RSA patients and the control group. The Kruskal–Wallis test was used in this study. Dunn’s correction for multiple comparisons was adopted to compare two variables among multiple variables. MedCalc software (Version 15.2.2) was used to plot the ROC curve and calculate the AUC. Logistic regression was used to calculate the AUC for the combined use of all parameters of interest under the default settings of MedCalc software. A P-value <0.05 was considered statistically significant.
Result
Comparison of Baseline Characteristics Between RSA Patients with and without Early Pregnancy Loss
To compare the baseline characteristics between RSA patients who experienced early pregnancy loss and those who did not, relevant data were summarized in Table 1. In both the training cohort (N=412) and testing cohort (n=177), no significant differences were observed between the abortion and normal subgroups in terms of age, BMI, infertility duration, gravidity, parity, hormone levels (FSH, LH, estradiol, progesterone, TSH, FT4, prolactin), metabolic indicators (fasting glucose, total cholesterol, triglycerides, LDL, HDL), blood pressure (systolic and diastolic), platelet count, or coagulation parameters (PT, APTT) (all P>0.05). However, the positive rates of aβ2-GP1, TgAb, and ACA were significantly higher in the abortion subgroup than in the normal subgroup across both cohorts (all P<0.05), while AsAb showed a significant difference only in the training cohort (P=0.001). Additionally, the abortion subgroup had higher uterine artery RI and lower endometrial thickness, endometrial volume, VI, and VFI in both cohorts (all P<0.05). These findings indicate that autoantibody positivity (aβ2-GP1, TgAb, ACA), increased uterine artery resistance, and poor endometrial morphology and vascularity are associated with early pregnancy loss in RSA patients.
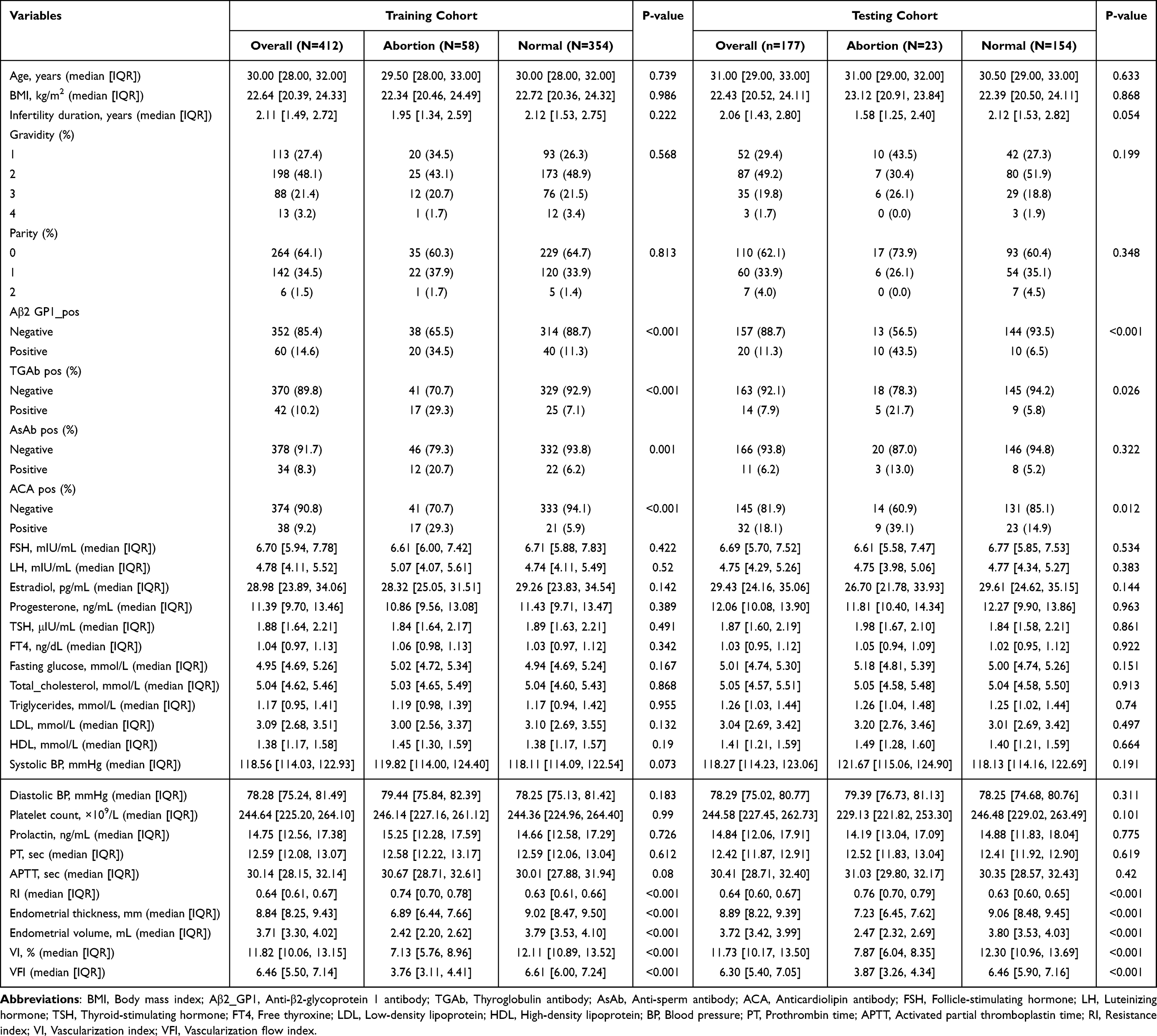 |
Table 1 Baseline Characteristics for Predicting Early Pregnancy Loss in Patients with Recurrent Spontaneous Abortion |
Screening of Candidate Variables for Machine Learning-Based Prediction of Early Pregnancy Loss in RSA Patients
To screen candidate variables for machine learning-based prediction of early pregnancy loss in RSA patients, univariate and multivariate logistic regression analyses were conducted, with findings summarized in Table 2. Univariate analysis identified nine variables significantly associated with early pregnancy loss (all P<0.001), including positivity for aβ2-GP1, TgAb, AsAb and ACA, increased RI, as well as decreased endometrial thickness, endometrial volume, VI and VFI. In multivariate analysis, ACA positivity no longer showed significance (P=0.072), while the other eight variables remained significantly correlated with the outcome (all P<0.001). Figure 2 provided multi-method validation for these variables, covering Pearson correlation analysis heatmap, Lasso regression plots (binomial deviance vs number of trees, variable coefficients vs log lambda) and SHAP value-based candidate variable weight ranking. These results confirm that the eight variables with persistent significance are reliable candidates for constructing the machine learning prediction model for early pregnancy loss in RSA patients.
 |
Table 2 Univariate and Multivariate Logistic Regression Analyses for Predicting Early Pregnancy Loss in Patients with Recurrent Spontaneous Abortion |
 |
Figure 2 Multi-Method Validation for Candidate Variable Selection in Machine Learning. (A) Pearson Correlation Analysis Heatmap; (B) Lasso Regression Plot (Binomial Deviance vs Number of Trees); (C) Lasso Regression Plot (Variable Coefficients vs Log Lambda); (D) Candidate Variable Weight Ranking Based on SHapley Additive exPlanations Value Analysis. |
Evaluation and Comparison of Predictive Efficacy of Machine Learning Models
To assess the predictive efficacy of different machine learning models for early pregnancy loss in RSA patients, performance metrics were analyzed using Table 3 and Figure 3 (heatmaps for train and test datasets), with multidimensional validation via Figure 4. In the training dataset, the logistic regression model showed the highest ROC-AUC (0.94) and high accuracy (0.93), outperforming other models such as decision tree (DT, ROC-AUC 0.78) and Xgboost (ROC-AUC 0.88). In the test dataset, logistic regression remained superior with ROC-AUC 0.92 and accuracy 0.90, exceeding random forest (RF, ROC-AUC 0.86) and multi-layer perceptron (Mlp, ROC-AUC 0.81). Figures 4A–B decision curve analysis (DCA, Panels A, C) and ROC curve analysis (Panels B, D) further confirmed its favorable clinical utility and discriminative ability in both cohorts. These findings demonstrate that the logistic regression model has the most robust and stable predictive efficacy for early pregnancy loss in RSA patients among the seven tested models.
 |
Table 3 Performance Metrics of Various Models on Training and Testing Datasets |
 |
Figure 3 Heatmaps of Model Evaluation Metrics for Train (A) and Test (B) Datasets. |
 |
Figure 4 Multidimensional Evaluation of the Predictive Performance of Various Predictive Models. Notes: (A) (Training cohort) and (C) (Testing cohort) refer to the analysis results for evaluating model performance from one dimension, corresponding to Decision Curve Analysis (DCA); (B) (Training cohort) and (D) (Testing cohort) refer to the analysis results for evaluating model performance from another dimension, corresponding to Receiver Operating Characteristic (ROC) Curve Analysis. |
Clinical Application of the Optimal Predictive Model in Machine Learning
Since the logistic regression model was confirmed as the optimal one for predicting early pregnancy loss in RSA patients, a clinical prediction tool was developed and displayed in Figure 5. Figure 5A shows the online prediction nomogram, which integrates the eight validated candidate variables (aβ2-GP1, TgAb, AsAb, RI, endometrial thickness, endometrial volume, VI, VFI). Each variable is assigned corresponding points; clinicians can sum the points of individual variables to get a patient’s total points, thereby estimating the probability of early pregnancy loss. Additionally, calibration curves were used to evaluate the model’s prediction consistency. Figure 5B corresponds to the training set and Figure 5C to the test set, and both curves demonstrate good alignment between predicted probabilities and actual outcomes. This indicates that the nomogram’s predictive results are highly consistent with real clinical situations. Overall, the nomogram derived from the optimal logistic regression model provides a practical and accurate tool for clinicians to assess the risk of early pregnancy loss in RSA patients, which is conducive to formulating individualized clinical intervention strategies.
 |
Figure 5 Online Nomogram for Predicting Early Pregnancy Loss. Notes: Subfigure (A) shows the online prediction nomogram; Subfigures (B and C) denote the calibration curves of the training set and test set, respectively. |
Discussion
Globally, RSA remains a major clinical challenge in the field of reproductive medicine. Even after completing comprehensive examinations covering chromosomes, anatomy, immunity, and other aspects, more than half of RSA patients still have unclear etiologies and are thus diagnosed with URA.24 These patients often experience intense anxiety during subsequent pregnancies, creating an urgent need for reliable pregnancy monitoring methods. Currently, serum β-hCG, estradiol, and progesterone have been used in early pregnancy assessment, but the predictive value of their dynamic changes for pregnancy outcomes remains unclear.25–27 The machine learning prediction model established in this study based on positive aβ2-GP1, positive TgAb, endometrial thickness, endometrial volume, and VFI can effectively evaluate the risk of early miscarriage in RSA patients during subsequent pregnancies.
To date, the specific mechanism by which prethrombotic states (PTS) cause spontaneous miscarriage has not been fully clarified. It is generally recognized that the hypercoagulable state during pregnancy alters the blood flow status at the uteroplacental interface, easily leading to the formation of local microthrombi or even placental infarction.28,29 This reduces blood supply to placental tissue, causing ischemia and hypoxia in the embryo or fetus, and ultimately resulting in poor embryonic or fetal development and miscarriage. Known acquired PTS mainly include antiphospholipid syndrome (APS), acquired hyperhomocysteinemia, and other diseases that cause hypercoagulable states.30 Currently, indicators commonly used to detect PTS include coagulation-related tests and relevant autoantibodies, such as aPL, aβ2-GP1, lupus anticoagulant (LA), and homocysteine (Hcy). Among them, the aβ2-GP1 is widely present in human plasma, and the placenta participates in the production of aβ2-GP1 during pregnancy.31 aβ2-GP1 plays an important role in the occurrence of autoimmune diseases, adverse pregnancy histories, and other conditions. Previous studies have shown that positive expression of aβ2-GP1 antibodies in pregnant women may lead to habitual abortion, stillbirth, and pregnancy-induced hypertension, and has predictive value for adverse pregnancy outcomes.32
In this study, serum aβ2-GP1 antibodies were detected in all subjects, and the results showed that the positive rate of serum aβ2-GP1 antibodies in RSA patients was significantly higher than that in the control group, which was consistent with the above findings. Moreover, the positive rate of serum aβ2-GP1 antibodies in RSA patients was significantly positively correlated with the risk of recurrent miscarriage in subsequent pregnancies, indicating that an increased positive rate of serum aβ2-GP1 antibodies is associated with an elevated risk of miscarriage in RSA patients during subsequent pregnancies. It is speculated that serum aβ2-GP1 antibodies may play a role in the assessment of RSA severity.
Previous studies have indicated that pregnancy is regulated by multiple factors, including the uterine environment, hormones, and immunity.33–35 Dysfunction of any of these factors may lead to adverse pregnancy outcomes. aβ2-GP1 can inhibit the activity of prothrombin on the platelet surface, promote thrombosis, and damage trophoblast cells, ultimately resulting in adverse pregnancy outcomes. Consistent with the results of this study, the positive rate of serum aβ2-GP1 antibodies in patients with adverse pregnancy outcomes was significantly higher than that in patients with favorable pregnancy outcomes, and aβ2-GP1 antibodies had high accuracy in predicting adverse pregnancy outcomes in RSA patients. These findings suggest that aβ2-GP1 antibodies have certain value in predicting adverse pregnancy outcomes in patients with RSA.
Previous studies have shown that thyroid autoimmunity (TAI) is a common autoimmune disease in women of childbearing age, with a prevalence of approximately 18%.36 TAI is associated with a variety of anti-thyroid antibodies (ATA), mainly including anti-thyroid peroxidase antibody (TPOAb), anti-thyroglobulin antibody (TgAb), and thyroid-stimulating hormone receptor antibody (TSHRAb). Epidemiological data show that ATA can be detected in approximately 5% to 15% of women of childbearing age.37–39 A large-scale epidemiological survey in China showed that 23.3% of pregnant women tested positive for TPOAb and 9.9% tested positive for TgAb.40 Consistent with the results of previous studies, this study found that TgAb was significantly associated with adverse outcomes of recurrent miscarriage in RSA patients during subsequent pregnancies.
It is speculated that the regularity of the female menstrual cycle and normal ovulation depend on the precise regulation of the hypothalamic-pituitary-ovarian axis (HPO axis), and the presence of ATA may disrupt this balance mechanism, thereby causing ovulation disorders and menstrual irregularities. In addition, previous studies have found that the presence of ATA is associated with increased levels of proinflammatory cytokines (interferon-gamma [IFN-γ] and interleukin-17A [IL-17A]) and decreased levels of transforming growth factor-beta (TGF-β). These changes can affect embryo implantation and pregnancy maintenance.
This study also found that AsAb is an independent risk factor for early miscarriage in RSA patients during subsequent pregnancies. In fact, there is no consistent clinical consensus in the academic community regarding studies on recurrent spontaneous abortion caused by AsAb. However, it has long been recognized that sperm act as antigens in the female body. When sperm enter the female bloodstream under the influence of factors such as infection or trauma, the body produces immune antibodies, and AsAb is the immune complex generated by the body. Previous studies have shown that AsAb can inhibit the tight binding between sperm and the zona pellucida (ZP) through two mechanisms: one is direct binding to the ZP ligand in the sperm membrane, and the other is binding to the corresponding antigen near the ZP ligand in the sperm membrane.41–43 Both mechanisms interfere with the binding between the ZP ligand in the sperm membrane and the sperm receptor in the ZP, ultimately leading to miscarriage and infertility. However, sperm antigens are quite complex, and the known types include sperm-specific antigens, sperm membrane antigens, ABO blood group antigens, and histocompatibility antigens.
Studies have indicated that the presence of antisperm antibodies (AsAb) in the human body may lead to infertility, and this factor is associated with a considerable proportion of infertile cases.44,45 Additionally, among women who experience spontaneous abortion, the rate of AsAb positivity also constitutes a notable percentage.46 Therefore, immune infertility caused by AsAb has received widespread clinical attention. Since the production of AsAb is not correlated with age and can cause infertility in all main reproductive age groups, the detection of AsAb is a prerequisite for the effective treatment of infertile patients.
In this study, endometrial thickness, endometrial volume, and Vascular Flow Index (VFI) were found to be independent protective factors against early miscarriage in RSA patients during subsequent pregnancies. The endometrium is a key site for embryo implantation and development, and its morphology, thickness, and microenvironment have important impacts on pregnancy outcomes. From the perspective of the microenvironment, the endometrial microenvironment consists of complex components such as cells, molecules, and flora, which work together to affect the process of embryo implantation and development.47 Among these, endometrial stromal cells and metabolism influence the decidualization process. Notably, during early pregnancy, significant changes occur in maternal blood circulation to meet the growing needs of the uterus and fetus. Embryo implantation, trophoblast invasion, and placental development are critical for successful pregnancy, and uterine artery blood flow plays an important role in these processes. Domestic and international studies have confirmed that abnormal uterine artery blood flow is associated with adverse pregnancy outcomes.48 In the monitoring of uterine artery blood flow parameters in this study, the mean systolic/diastolic ratio (mS/D), mean pulsatility index (mPI), and mean resistance index (mRI) in the miscarriage group were higher than those in the live birth group at 8–10 weeks of gestation (ie, the second ultrasound examination), with statistically significant differences. This suggests that patients with recurrent pregnancy loss have increased uterine artery Doppler parameters during the 8~10 weeks period, which is associated with a corresponding increase in the risk of miscarriage.
In addition, some scholars have shown that trophoblast invasion has little effect on uterine artery blood flow at 4~5 weeks of gestation, and the blood flow resistance of the uterine artery decreases very slowly before 8 weeks of gestation.49–51 Other scholars have also compared the uterine artery PI values between women with no history of miscarriage and those with unexplained recurrent pregnancy loss, and found that the PI values of patients with unexplained recurrent pregnancy loss were significantly higher than those of women without a history of miscarriage.52,53 Based on these findings, we speculate that the uterine artery may regulate endometrial receptivity, and poor uterine blood perfusion may be one of the causes of unexplained miscarriage and may also contribute to implantation failure. In conclusion, the results of our study indicate that VFI in early pregnancy can be used as a risk factor for miscarriage, and in particular, the rate of decrease in uterine artery blood flow parameters in early pregnancy can predict adverse pregnancy outcomes.
This study also inevitably has the following three key limitations. First, it employed a retrospective single-center design, with all data derived from the electronic medical records of Xi’an People’s Hospital. This design may introduce selection bias (eg, the exclusion of patients with incomplete records) and information bias (eg, unrecorded factors like psychological stress), which could compromise the reliability of the established model. Second, the sample size was little and homogeneous, as participants were recruited from a single institution and had similar demographic backgrounds. This restricts the model’s external validity when applied to RSA patients in other regions or of different ethnic groups. Third, the set of variables included was incomplete. The model did not account for lifestyle factors (eg, environmental toxin exposure), male-related indicators (eg, sperm quality), and dynamic biochemical markers (eg, serial β-hCG changes), thereby reducing its comprehensiveness.
Conclusion
This study established a logistic regression model for early pregnancy loss in RSA patients using 8 predictors (aβ2-GP1, TgAb, AsAb, RI, endometrial thickness, endometrial volume, VI, VFI), with an AUC of 0.94 in the training set and 0.92 in the validation set. The model’s nomogram enables practical risk stratification, thereby supporting individualized clinical intervention. Limitations include a single-center, retrospective study design; however, future multicenter prospective studies incorporating more variables (eg, male factors, lifestyle) are expected to optimize the model.
Funding
1. Support Plan for Sanqin Scholars Innovation Team ([2020]45), Shaanxi province. 2. The Project Supported by Natural Science Basic Research Plan in Shaanxi Province of China (Program No. 2025JC-YBMS-808).
Disclosure
The authors report no conflicts of interest in this work.
References
1. La X, Wang W, Zhang M, Liang L. Definition and multiple factors of recurrent spontaneous abortion. Adv Exp Med Biol. 2021;1300:231–16.
2. Deng T, Liao X, Zhu S. Recent advances in treatment of recurrent spontaneous abortion. Obstetrical Gynecol Surv. 2022;77(6):355–366. doi:10.1097/OGX.0000000000001033
3. Devall AJ, Coomarasamy A. Sporadic pregnancy loss and recurrent miscarriage. Best Pract Res Clin Obstet Gynaecol. 2020;69:30–39. doi:10.1016/j.bpobgyn.2020.09.002
4. Yao Y, Ye Y, Chen J, Zhang M, Cai X, Zheng C. Maternal-fetal immunity and recurrent spontaneous abortion. Am J Reprod Immunol. 2024;91(5):e13859. doi:10.1111/aji.13859
5. Odendaal J, Black N, Bennett PR, Brosens J, Quenby S, MacIntyre DA. The endometrial microbiota and early pregnancy loss. Human Reprod. 2024;39(4):638–646. doi:10.1093/humrep/dead274
6. Yang X, Tian Y, Zheng L, Luu T, Kwak-Kim J. The update immune-regulatory role of pro- and anti-inflammatory cytokines in recurrent pregnancy losses. Int J Mol Sci. 2022;24(1):132. doi:10.3390/ijms24010132
7. Wang RQ, Deng ZM, Chen GT, Dai FF, Xia LB. Obesity and recurrent spontaneous abortion: the crucial role of weight management in pregnancy. Reproductive Biol Endocrinol. 2025;23(1):10. doi:10.1186/s12958-024-01326-3
8. Guan D, Sun W, Gao M, Chen Z, Ma X. Immunologic insights in recurrent spontaneous abortion: molecular mechanisms and therapeutic interventions. Biomed Pharmacother. 2024;177:117082. doi:10.1016/j.biopha.2024.117082
9. Ma W, Gu Z, Lin Q, et al. Integrative genetic and multi-omics analysis reveals the interleukin-6 receptor’s role in recurrent spontaneous abortion. Front Immunol. 2025;16:1659251. doi:10.3389/fimmu.2025.1659251
10. Yu N, Kwak-Kim J, Bao S. Unexplained recurrent pregnancy loss: novel causes and advanced treatment. J Reprod Immunol. 2023;155:103785. doi:10.1016/j.jri.2022.103785
11. Giouleka S, Tsakiridis I, Arsenaki E, et al. Investigation and management of recurrent pregnancy loss: a comprehensive review of guidelines. Obstetrical Gynecol Surv. 2023;78(5):287–301. doi:10.1097/OGX.0000000000001133
12. Dimitriadis E, Menkhorst E, Saito S, Kutteh WH, Brosens JJ. Recurrent pregnancy loss. Nat Rev Dis Prim. 2020;6(1):98. doi:10.1038/s41572-020-00228-z
13. Lund M, Kamper-Jørgensen M, Nielsen HS, Lidegaard Ø, Andersen AM, Christiansen OB. Prognosis for live birth in women with recurrent miscarriage: what is the best measure of success? Obstetrics Gynecol. 2012;119(1):37–43. doi:10.1097/AOG.0b013e31823c0413
14. Bender Atik R, Christiansen OB, Elson J, et al. ESHRE guideline: recurrent pregnancy loss. Human Reprod Open. 2018;2018(2):hoy004. doi:10.1093/hropen/hoy004
15. Rotondo JC, Oton-Gonzalez L, Selvatici R, et al. SERPINA1 gene promoter is differentially methylated in peripheral blood mononuclear cells of pregnant women. Front Cell Develop Biol. 2020;8:550543. doi:10.3389/fcell.2020.550543
16. Annunziata A, Fiorentino G, Coppola A, et al. Alpha-1 antitripsyn deficiency and augmentation therapy in pregnancy: two case reports. Front Med. 2024;11:1479877. doi:10.3389/fmed.2024.1479877
17. Sung J. Artificial intelligence in medicine: ethical, social and legal perspectives. Ann Acad Med Singapore. 2023;52(12):695–699. doi:10.47102/annals-acadmedsg.2023103
18. Haug CJ, Drazen JM. Artificial intelligence and machine learning in clinical medicine, 2023. New Engl J Med. 2023;388(13):1201–1208. doi:10.1056/NEJMra2302038
19. Wang F, Jia W, Fan M, et al. Single-cell immune landscape of human recurrent miscarriage. Genomics Proteomics Bioinformatics. 2021;19(2):208–222. doi:10.1016/j.gpb.2020.11.002
20. Chen P, Zhou L, Chen J, et al. The immune atlas of human deciduas with unexplained recurrent pregnancy loss. Front Immunol. 2021;12:689019. doi:10.3389/fimmu.2021.689019
21. Murvai VR, Galiș R, Panaitescu A, et al. Antiphospholipid syndrome in pregnancy: a comprehensive literature review. BMC Pregnancy Childbirth. 2025;25(1):337. doi:10.1186/s12884-025-07471-w
22. Wang A, Wu F, Liu M, Zhang Z, Li S, Tan Q. Analysis of treatment and subsequent pregnancy outcomes in patients with antinuclear antibody-positive recurrent spontaneous abortion. Immunity Inflammation Dis. 2025;13(6):e70216. doi:10.1002/iid3.70216
23. Chen J, Yue J, Lu Y, Li T, Li X, Zhang JY. Recurrent miscarriage and low-titer antiphospholipid antibodies. Clin Rheumatol. 2024;43(4):1327–1334. doi:10.1007/s10067-023-06843-x
24. Tong F, Wang Y, Gao Q, et al. The epidemiology of pregnancy loss: global burden, variable risk factors, and predictions. Human Reprod. 2024;39(4):834–848. doi:10.1093/humrep/deae008
25. Deng W, Sun R, Du J, et al. Prediction of miscarriage in first trimester by serum estradiol, progesterone and β-human chorionic gonadotropin within 9 weeks of gestation. BMC Pregnancy Childbirth. 2022;22(1):112. doi:10.1186/s12884-021-04158-w
26. Özdemir AZ, Karli P, Gülümser Ç. Does high estrogen level negatively affect pregnancy success in frozen embryo transfer? Archiv Med Sci. 2022;18(3):647–651. doi:10.5114/aoms.2020.92466
27. Li Y, Zhang J, Zhang K, Wang E, Shu J. Significance of dynamically monitoring serum estrogen and β-human chorionic gonadotropin in early pregnancy assessment. J Clin Lab Analysis. 2021;35(1):e23559. doi:10.1002/jcla.23559
28. Wu Y, Xin M, Han Q, et al. Extensive serum biomarker analysis in the prethrombotic state of recurrent spontaneous abortion. J Cell Mol Med. 2021;25(14):6679–6694. doi:10.1111/jcmm.16671
29. Tang C, Hu W. The role of Th17 and Treg cells in normal pregnancy and unexplained recurrent spontaneous abortion (URSA): new insights into immune mechanisms. Placenta. 2023;142:18–26. doi:10.1016/j.placenta.2023.08.065
30. Knight JS, Branch DW, Ortel TL. Antiphospholipid syndrome: advances in diagnosis, pathogenesis, and management. BMJ. 2023;380:e069717. doi:10.1136/bmj-2021-069717
31. Shang X, Li J, Wang X, Zhang P. Diagnostic efficacy of ACA, aβ2-GP1, hs-CRP, and Hcy for cerebral infarction and their relationship with the disease severity. Am J Transl Res. 2024;16(6):2369–2378. doi:10.62347/DDWQ9504
32. Pan Y, Bao R, Xiang J, Cai Z. Correlation of anti-phosphatidylethanolamine antibodies with premature birth in women with a history of miscarriage: a retrospective study. BMJ open. 2025;15(4):e090323. doi:10.1136/bmjopen-2024-090323
33. Zhu XZ, Deng ZM, Dai FF, Liu H, Cheng YX. The impact of early pregnancy metabolic disorders on pregnancy outcome and the specific mechanism. Eur J Med Res. 2023;28(1):197. doi:10.1186/s40001-023-01161-z
34. Inversetti A, Zambella E, Guarano A, Dell’Avanzo M, Di Simone N. Endometrial microbiota and immune tolerance in pregnancy. Int J Mol Sci. 2023;24(3):2995. doi:10.3390/ijms24032995
35. Blazheva S, Pachkova S, Bodurska T, et al. Unlocking the uterine code: microbiota, immune cells, and therapy for recurrent reproductive failure. Microorganisms. 2024;12(3):547. doi:10.3390/microorganisms12030547
36. Tańska K, Gietka-Czernel M, Glinicki P, Kozakowski J. Thyroid autoimmunity and its negative impact on female fertility and maternal pregnancy outcomes. Front Endocrinol. 2022;13:1049665. doi:10.3389/fendo.2022.1049665
37. Rasoulizadeh Z, Eftekhar M, Ghadiri-Anari A, et al. Prevalence of anti-thyroid peroxidase antibodies among women with polycystic ovary syndrome. Sci Rep. 2025;15(1):33563. doi:10.1038/s41598-025-18582-x
38. van der Ham K, Stekelenburg KJ, Louwers YV, et al. The prevalence of thyroid dysfunction and hyperprolactinemia in women with PCOS. Front Endocrinol. 2023;14:1245106. doi:10.3389/fendo.2023.1245106
39. Song H, Cui T, Shi S, Xiao H, Wei A. Effect of anti-thyroid antibodies on recurrent miscarriage: a meta-analysis. J Obstetrics Gynaecol Res. 2024;50(7):1095–1105. doi:10.1111/jog.15944
40. Wu M, Wan Y, Zhao L, et al. Association between thyroid autoimmunity and antinuclear antibody prevalence among pregnant women: a cross-sectional study in Qingdao, China. Front Endocrinol. 2024;15:1403917. doi:10.3389/fendo.2024.1403917
41. Lu JC, Ge YM, Xu YH, Tang SS, Liang YJ. Screening of sperm antigen epitopes by phage display technique and its preliminary clinical application. Basic Clin Androl. 2022;32(1):22. doi:10.1186/s12610-022-00172-w
42. Samoylova TI, Cochran AM, Samoylov AM, et al. Phage display allows identification of zona pellucida-binding peptides with species-specific properties: novel approach for development of contraceptive vaccines for wildlife. J Biotechnol. 2012;162(2–3):311–318. doi:10.1016/j.jbiotec.2012.10.006
43. Mortazavi B, Allahyari Fard N, Karkhane AA, Shokrpoor S, Heidari F. Evaluation of multi-epitope recombinant protein as a candidate for a contraceptive vaccine. J Reprod Immunol. 2021;145:103325. doi:10.1016/j.jri.2021.103325
44. Šemeklienė B, Gradauskienė B. Infertility and auto-antibodies: a review. Antibodies. 2025;14(3). doi:10.3390/antib14030076
45. Fang Y, Su Y, Xu J, et al. Varicocele-mediated male infertility: from the perspective of testicular immunity and inflammation. Front Immunol. 2021;12:729539. doi:10.3389/fimmu.2021.729539
46. Lu JC, Huang YF, Lu NQ. Antisperm immunity and infertility. Expert Rev Clin Immunol. 2008;4(1):113–126. doi:10.1586/1744666X.4.1.113
47. Wang Y, Tang Z, Teng X. New advances in the treatment of thin endometrium. Front Endocrinol. 2024;15:1269382. doi:10.3389/fendo.2024.1269382
48. Babazadeh R, Sharifi F, Amel Barez M. Domestic violence in pregnancy: a systematic review of clinical guidelines. BMC Pregnancy Childbirth. 2025;25(1):336. doi:10.1186/s12884-025-07459-6
49. Vaupel P, Multhoff G. Blood flow and respiratory gas exchange in the human placenta at term: a data update. Adv Exp Med Biol. 2022;1395:379–384.
50. Schiffer V, Evers L, de Haas S, Ghossein-Doha C, Al-Nasiry S, Spaanderman M. Spiral artery blood flow during pregnancy: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2020;20(1):680. doi:10.1186/s12884-020-03150-0
51. Yang X, Tian X, Liu H, Wang J, Wang F. Homocysteine increases uterine artery blood flow resistance in women with pregnancy loss. J Gynecol Obstetrics Human Reprod. 2023;52(2):102533. doi:10.1016/j.jogoh.2023.102533
52. Lee J, Cho H. Fetal pulmonary vein pulsatility index in the third trimester of pregnancy as a predictor of small for gestational age. J Ultrasound Med. 2022;41(1):53–60. doi:10.1002/jum.15678
53. Abonyi EO, Idigo FU, Anakwue AC, Agbo JA. Sensitivity of uterine artery Doppler pulsatility index in screening for adverse pregnancy outcome in first and second trimesters. J Ultrasound. 2023;26(2):517–523. doi:10.1007/s40477-022-00766-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Using Machine Learning Algorithms to Predict High-Risk Factors for Postoperative Delirium in Elderly Patients
Liu Y, Shen W, Tian Z
Clinical Interventions in Aging 2023, 18:157-168
Published Date: 8 February 2023
Ten-Year Multicenter Retrospective Study Utilizing Machine Learning Algorithms to Identify Patients at High Risk of Venous Thromboembolism After Radical Gastrectomy
Liu Y, Song C, Tian Z, Shen W
International Journal of General Medicine 2023, 16:1909-1925
Published Date: 18 May 2023
Development of Machine Learning Models for Predicting Osteoporosis in Patients with Type 2 Diabetes Mellitus—A Preliminary Study
Wu X, Zhai F, Chang A, Wei J, Guo Y, Zhang J
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1987-2003
Published Date: 30 June 2023
Prediction of the Risk of Bone Mineral Density Decrease in Type 2 Diabetes Mellitus Patients Based on Traditional Multivariate Logistic Regression and Machine Learning: A Preliminary Study
Zhang J, Xu Z, Fu Y, Chen L
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2885-2898
Published Date: 19 September 2023
Risk Prediction of Diabetes Progression Using Big Data Mining with Multifarious Physical Examination Indicators
Chen X, Zhou S, Yang L, Zhong Q, Liu H, Zhang Y, Yu H, Cai Y
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1249-1265
Published Date: 11 March 2024