Back to Journals » Journal of Pain Research » Volume 19
Non-Pharmacological Complementary and Alternative Therapies for Knee Osteoarthritis: A Scoping Review of Randomized Controlled Trials
Authors Kang Y ![]() , Shi B, Huang Q, Liu Y, Hu WG, Cai GQ, Zhu FH
, Shi B, Huang Q, Liu Y, Hu WG, Cai GQ, Zhu FH
Received 11 March 2026
Accepted for publication 8 June 2026
Published 20 June 2026 Volume 2026:19 608480
DOI https://doi.org/10.2147/JPR.S608480
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rodrigo Diez-Tafur
Yanhong Kang,1 Bing Shi,1 Qiong Huang,2 Yan Liu,2 Wei Guo Hu,1 Guang Qing Cai,1 Fang Hui Zhu1
1Orthopedics Department, Changsha Hospital of Traditional Chinese Medicine (Changsha Eighth Hospital), Changsha, Hunan, 410100, People’s Republic of China; 2Nursing Department, Changsha Hospital of Traditional Chinese Medicine (Changsha Eighth Hospital), Changsha, Hunan, People’s Republic of China
Correspondence: Fang Hui Zhu, Orthopedics Department, Changsha Hospital of Traditional Chinese Medicine (Changsha Eighth Hospital), No. 22 Xingsha Avenue, Changsha, Hunan, 410100, People’s Republic of China, Email [email protected]
Background: Knee osteoarthritis (KOA) is a prevalent chronic degenerative joint disorder and a major contributor to pain, disability, and impaired quality of life. Non-pharmacological complementary and alternative medicine (CAM) approaches are widely used in KOA care, but randomized controlled trial (RCT) evidence is distributed across diverse intervention types, settings, comparators, and outcome measures.
Methods: Following the Arksey and O’Malley scoping review framework and the PRISMA-ScR reporting guideline, we searched PubMed, Web of Science, Embase, and the Cochrane Library for RCTs published from 1 January 2016 to 10 January 2026. Eligible studies enrolled adults with clinically or imaging-confirmed KOA and evaluated non-pharmacological, non-surgical CAM or related integrative interventions. The review question was structured according to the population-concept-context framework. Two reviewers independently screened records and charted study characteristics, intervention features, comparator types, outcomes, follow-up time points, and key design features. Evidence was summarized descriptively and narratively; no pooled treatment-effect estimates were calculated.
Results: Fifty-three RCTs were included. The evidence base covered acupuncture-related therapies, manual and body-based therapies, exercise and mind-body programs, physical agent modalities, psychological and behavioral interventions, and other complementary or integrative approaches. Studies were geographically concentrated in China, the United States, Turkey, and several other countries. Protocols, intervention dose, provider background, comparator selection, and follow-up duration varied substantially. Pain and physical-function outcomes were the most frequently mapped domains, whereas quality of life, psychological outcomes, mechanistic biomarkers, neuroimaging indices, adherence, and implementation variables were reported less consistently.
Conclusion: This scoping review maps the breadth, distribution, and methodological features of RCT evidence on non-pharmacological CAM approaches for KOA. The findings identify a heterogeneous and expanding evidence base, but also reveal gaps in standardized intervention reporting, long-term follow-up, head-to-head comparisons, generalizability beyond TCM-centered Chinese settings, and design-characteristic reporting. These evidence-mapping findings can inform future systematic reviews, pragmatic trials, and implementation-focused research.
Keywords: knee osteoarthritis, complementary and alternative medicine, non-pharmacological intervention, scoping review, randomized controlled trial, evidence mapping
Background
Knee osteoarthritis (KOA) is a chronic degenerative joint disease characterized by progressive cartilage loss, osteophyte formation, synovial inflammation, pain, stiffness, and functional limitation. It is one of the leading causes of disability worldwide, and its burden is increasing with population ageing and rising obesity prevalence.1,2 Current clinical guidelines recommend education, exercise, weight management, and other non-pharmacological strategies as core components of KOA management, while pharmacological and surgical options are selected according to symptoms, risk profile, and disease severity.3,4 Although analgesics and non-steroidal anti-inflammatory drugs may relieve symptoms, long-term or inappropriate use can be limited by gastrointestinal, cardiovascular, and renal adverse events.5
In this review, complementary and alternative medicine (CAM) is used as an umbrella term for health practices, products, and therapeutic systems that are not usually regarded as part of conventional biomedicine when used alone, or that are used alongside conventional care when applied as complementary or integrative approaches. For KOA, CAM-related non-pharmacological interventions include traditional medicine techniques such as acupuncture, moxibustion, Tuina, Gua Sha, and mind-body exercise, as well as manual therapy, yoga, massage, behavioral self-management, physical agent modalities, and other non-drug supportive approaches when evaluated as alternatives or adjuncts to usual care.3,4,6
Several systematic reviews, meta-analyses, umbrella reviews, and network meta-analyses have already examined specific non-pharmacological modalities or compared selected intervention classes for KOA.6–12 These studies are useful for estimating comparative effects when interventions, comparators, and outcomes are sufficiently similar. However, the present literature also contains substantial diversity in intervention concepts, treatment dose, provider background, control design, follow-up schedule, and outcome domains. A scoping review is therefore appropriate when the objective is not to pool effects, but to map the range of available RCT evidence, clarify how interventions have been conceptualized and studied, and identify evidence gaps that can guide future systematic reviews and pragmatic trials.13
The objective of this scoping review was to map RCT evidence on non-pharmacological CAM and related integrative interventions for adults with KOA. Specifically, we aimed to describe the distribution of studies, classify intervention categories, summarize comparator and outcome patterns, identify key methodological and reporting features, and clarify evidence gaps relevant to future research and clinical implementation.
Methods
This scoping review followed the methodological framework proposed by Arksey and O’Malley and was reported in accordance with the PRISMA-ScR guideline.13 A formal effect-size synthesis or risk-of-bias-based certainty assessment was not planned because the purpose was evidence mapping rather than comparative efficacy estimation.
Research Questions Based on PCC
The review question was structured using the population-concept-context framework. The population was adults with clinically or imaging-confirmed KOA. The concept was non-pharmacological CAM, complementary, alternative, or integrative interventions evaluated in RCTs. The context included hospital, outpatient, community, home-based, online, and other clinical or research settings. The review addressed four questions: (1) Which categories of non-pharmacological CAM or related integrative interventions have been evaluated in RCTs for KOA? (2) What intervention components, dose parameters, provider backgrounds, and delivery settings have been reported? (3) What comparator types and outcome domains have been used? (4) What evidence gaps and methodological patterns can be identified from the included RCTs?
Eligibility Criteria
Inclusion criteria were as follows: (1) study design: RCTs; (2) participants: adults aged 18 years or older with clinically or imaging-confirmed KOA; (3) interventions: non-pharmacological, non-surgical CAM, complementary, alternative, or integrative interventions, including traditional medicine techniques, mind-body exercise, manual or body-based therapies, physical agent modalities, behavioral/self-management programs, and other non-drug supportive approaches; and (4) outcomes: at least one pain, physical function, quality-of-life, psychological, biomechanical, physiological, safety, adherence, or implementation-related outcome.
Trials were eligible when the CAM or non-pharmacological component could be separated from the pharmacological effect by study design. Therefore, trials comparing a non-pharmacological intervention plus the same background pharmacological treatment versus that pharmacological treatment alone were included, because the incremental contribution of the non-pharmacological component could be mapped. Trials using pharmacological comparators were also included when the experimental arm was a non-pharmacological intervention and the comparator was used as an active control. Trials were excluded when the effect of the non-pharmacological component could not be separated from a co-intervention, when participants had inflammatory arthritis or non-KOA pain conditions without separable KOA data, when critical data were missing, or when the publication was a conference abstract, protocol, review, commentary, or retracted article.
Information Sources and Search Strategy
PubMed, Embase, the Cochrane Library, and Web of Science were searched from 1 January 2016 to 10 January 2026. Search strategies combined terms for KOA, complementary or alternative therapies, and randomized trials. Full database-specific strategies were added to Supplementary File 1. The PubMed strategy is shown below as an example.
#1 “Osteoarthritis, Knee”[Mesh] OR (“Knee Osteoarthritides”[tiab] OR “Knee Osteoarthritis”[tiab] OR “Osteoarthritis of Knee”[tiab] OR “Osteoarthritis of the Knee”[tiab])
#2 “Complementary Therapies”[Mesh] OR (“Complementary Therapy”[tiab] OR “Alternative Medicine”[tiab] OR “Complementary Medicine”[tiab] OR “Alternative Therapies”[tiab] OR acupuncture[tiab] OR moxibustion[tiab] OR Tuina[tiab] OR massage[tiab] OR yoga[tiab] OR Tai Chi[tiab] OR Baduanjin[tiab] OR “manual therapy”[tiab] OR “mind-body”[tiab] OR “transcutaneous electrical nerve stimulation”[tiab] OR TENS[tiab])
#3 “randomized controlled trial”[Publication Type] OR randomized[Title/Abstract] OR randomised[Title/Abstract] OR placebo[Title/Abstract] OR sham[Title/Abstract]
#4 #1 AND #2 AND #3
The Embase strategy used Emtree terms and title/abstract keywords for knee osteoarthritis, complementary therapy, acupuncture, moxibustion, Tuina, massage, yoga, Tai Chi, Baduanjin, manual therapy, mind-body therapy, TENS, and randomized trial design. The Cochrane Library and Web of Science strategies used equivalent controlled vocabulary where available and free-text terms in title, abstract, and keyword fields. Complete strategies are provided in Supplementary File 1 to enable replication.
Study Selection and Data Charting
Two reviewers independently screened titles/abstracts and full texts according to the eligibility criteria. Disagreements were resolved by discussion or consultation with a third reviewer. A predesigned charting form was used and is provided as Supplementary File 2. Extracted items included bibliographic details, country, study setting, participant characteristics, sample size, intervention category, intervention components, dose and duration, provider background, comparator type, follow-up schedule, outcome domains, safety reporting, and key design features.
Synthesis of Results
Evidence was summarized descriptively and narratively. We mapped the included trials by intervention category, comparator type, follow-up duration, geographic distribution, outcome domain, and design characteristics. Because intervention protocols, comparators, and outcome measures were heterogeneous, and because the aim was to characterize the evidence base rather than estimate comparative effectiveness, no meta-analysis or network meta-analysis was conducted.
Critical Appraisal and Design-Characteristic Summary
A formal risk-of-bias assessment was not undertaken because it is not mandatory for scoping reviews and was not aligned with the evidence-mapping objective. However, to improve interpretability, we added a design-characteristic summary documenting sample size, blinding or sham-control status, comparator type, and follow-up duration for each included RCT (Supplementary Table S1). These data provide a minimal quality signal and help readers judge the maturity and limitations of the evidence base.
Results
Study Selection
The database searches identified 1141 records: Cochrane Library (n=361), PubMed (n=444), Web of Science (n=67), and Embase (n=269). After removal of 609 duplicates, 532 records were screened by title and abstract. Of these, 446 were excluded because they were clearly irrelevant (n=299), had an ineligible study type (n=133), or were not written in English (n=14). Eighty-six full-text articles were assessed for eligibility. Thirty-three were excluded because the outcome was not eligible or insufficiently reported (n=14), the intervention did not meet the review concept (n=8), the population was not KOA or KOA data were not separable (n=6), or critical information/full text was unavailable (n=5). Finally, 53 RCTs were included in the scoping review. The selection process is shown in Figure 1.
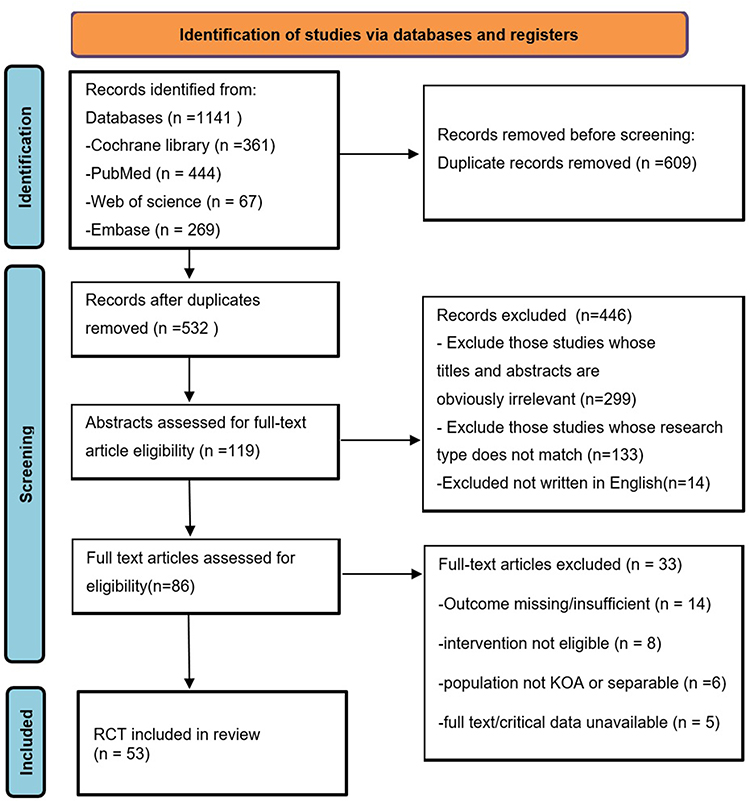 |
Figure 1 PRISMA flow diagram of study selection. The flow diagram reports 1141 records identified, 609 duplicates removed, 532 records screened, 446 title/abstract exclusions, 86 full-text articles assessed, 33 full-text exclusions, and 53 RCTs included in the scoping review. |
Characteristics of Included Studies
The 53 included RCTs were published between 2016 and 2026 and were conducted across multiple countries, with a high concentration in China, the United States, Turkey, and several other regions. Table 1 summarizes the characteristics of included trials. The evidence base included hospital-based, outpatient, community, home-based, and online delivery settings. Sample sizes ranged from small pilot trials to larger multicenter or multi-arm studies. Intervention duration ranged from a single session to 32 weeks, while most studies assessed outcomes at baseline and immediately after treatment; longer follow-up beyond 6 months was less common.
 |
Table 1 Characteristics of Included Randomized Controlled Trials (n=53) |
Intervention Categories
The included studies were reorganized into six evidence-mapping categories according to intervention concept, delivery mechanism, and clinical tradition. Acupuncture and related traditional needling therapies included manual acupuncture, electroacupuncture, superficial needling, Fu’s subcutaneous needling, acupotomy, thread-embedding acupuncture, warm needling/moxibustion, and intradermal needling. Manual and body-based therapies included Tuina, Swedish massage, Persian massage, joint mobilization, dry needling, reflexology, and Gua Sha. Exercise and mind-body programs included Tai Chi, yoga, chair yoga, Baduanjin, structured strengthening, treadmill-based rehabilitation, and isokinetic training. Physical agent modalities included TENS, NMES, interferential current, periosteal stimulation therapy, and related device-based stimulation. Psychological and behavioral interventions included positive psychological activities, guided imagery, mindfulness meditation, self-management support, transtheoretical model-based exercise adherence support, gamification, and graded motor imagery. The remaining interventions were classified as other integrative or complementary approaches, including aromatherapy, black cumin seed oil massage, non-contact spiritual therapy/Reiki, rTMS, and multimodal integrative programs. Because this last group was clinically heterogeneous, it was interpreted as a residual evidence-mapping category rather than a single coherent therapeutic class.
Outcome Domains Mapped Across Studies
Patient-reported pain and function were the dominant outcome domains. Pain was commonly assessed using VAS, NRS, WOMAC pain, KOOS pain, SF-MPQ, and related measures. Function and symptoms were commonly assessed using WOMAC, KOOS, Lequesne index, Oxford Knee Score, KOOS JR, patient acceptable symptom state, global assessment, or responder definitions. Performance-based tests included Timed Up and Go, 6-minute walk test, walking speed, 30-second chair stand, repeated chair rise, stair climb, single-leg stance, balance tests, and simulated activities of daily living.
Quality-of-life and psychological outcomes were reported less consistently. These included SF-36/SF-12, EQ-5D, WHOQOL-BREF, HADS, BDI, PHQ-4/PHQ-9, DASS-21, pain catastrophizing, kinesiophobia, self-efficacy, sleep quality, fatigue, and treatment satisfaction. Mechanistic and objective outcomes were present in a smaller subset of trials and included range of motion, quadriceps strength, pressure pain threshold, conditioned pain modulation, inflammatory markers, gut microbiota profiles, ultrasound-measured cartilage thickness, step counts, adherence, and neuroimaging indices such as resting-state functional connectivity and ALFF.
Comparator Types and Design Features
Comparator designs varied substantially. Sham or placebo controls were common in acupuncture, electrical stimulation, massage, physical therapy, and energy-therapy trials. Other trials used usual care, wait-list or no-intervention controls, education, home exercise, active non-pharmacological comparators, pharmacological comparators, or combination designs in which the non-pharmacological component was added to background pharmacological or rehabilitation care. This diversity is important for evidence mapping, but it limits any direct interpretation of comparative treatment effects across categories.
Evidence Mapping Patterns and Gaps
Table 2 summarizes the main evidence-mapping patterns by intervention category. Acupuncture-related and exercise/mind-body trials formed the largest clusters, whereas psychological/behavioral interventions, rTMS, energy therapies, aromatherapy, and some multimodal integrative programs were represented by fewer trials. Most trials emphasized short-term changes in pain and function; fewer studies examined long-term durability, adverse events in detail, implementation fidelity, adherence maintenance, costs, or healthcare utilization. Direct head-to-head comparisons between major CAM categories were uncommon. There were also gaps in population reporting, including KOA severity grades, comorbidity burden, older adults with frailty, and participants outside TCM-centered healthcare systems.
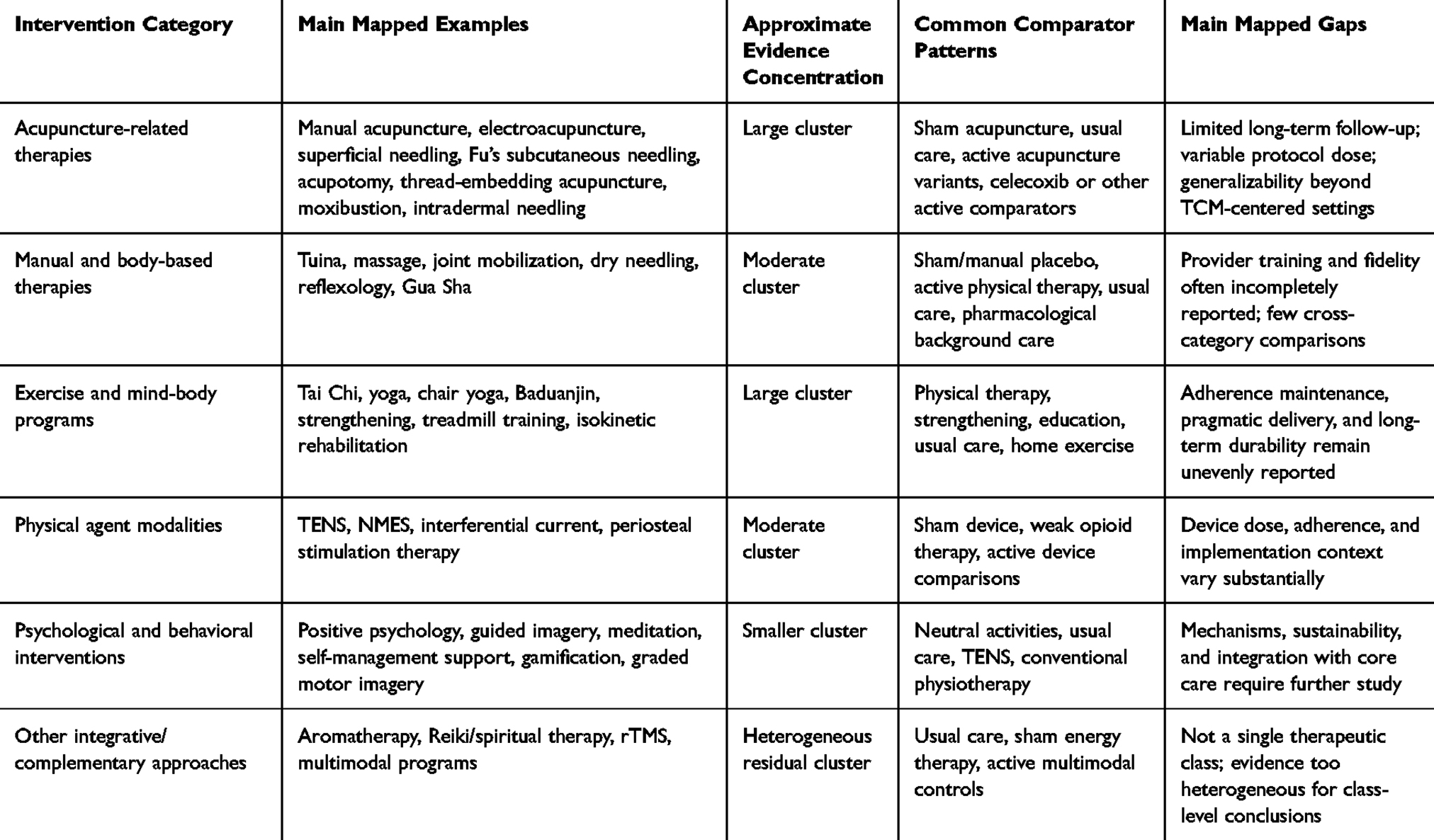 |
Table 2 Evidence-Mapping Summary by Intervention Category |
Discussion
Principal Evidence-Mapping Findings
This scoping review mapped the distribution and design characteristics of RCT evidence on non-pharmacological CAM and related integrative interventions for KOA. The main finding is not that one intervention category is superior to another, but that the RCT evidence base is broad, heterogeneous, and unevenly developed. Acupuncture-related therapies, exercise and mind-body programs, and manual/body-based approaches account for much of the available trial literature, whereas several emerging or less conventional approaches are represented by small numbers of studies. Across categories, the most frequently measured domains were pain and physical function, while long-term durability, implementation outcomes, cost-related outcomes, safety detail, and mechanistic measures were less consistently reported.
The choice of a scoping review is supported by this heterogeneity. Existing systematic reviews and meta-analyses have synthesized selected modalities or intervention classes.6–12 In contrast, the present review maps how the broader RCT landscape is organized, including intervention taxonomies, comparator selection, design features, outcome domains, and evidence gaps. These mapping results can help determine where future systematic reviews are feasible and where primary research remains too sparse or heterogeneous for formal comparative synthesis.
Methodological Patterns and Implications for Interpretation
Several methodological patterns limit direct interpretation. First, many trials used short intervention periods and short follow-up, making it difficult to map durability beyond treatment completion. Second, comparator designs differed substantially, ranging from sham controls to active pharmacological comparators, usual care, education, home exercise, and complex combination controls. Third, provider training, fidelity monitoring, intervention dose, and maintenance strategies were often incompletely reported. Fourth, a subset of studies used small sample sizes, single-session designs, or limited blinding. These features do not invalidate the scoping map, but they indicate that readers should avoid interpreting the included trials as a uniform evidence base for comparative efficacy.
The evidence map also highlights reporting priorities. Future RCTs should report intervention components, provider qualifications, dose, frequency, duration, adherence, co-interventions, comparator rationale, blinding feasibility, allocation concealment, attrition, adverse events, and follow-up time points in sufficient detail. Such information is necessary for later systematic reviews, implementation studies, and guideline translation.
Intervention Categorization and Heterogeneous Residual Groups
Intervention classification required careful handling because many CAM and integrative approaches overlap conceptually. For example, graded motor imagery was classified under psychological and behavioral interventions rather than exercise/mind-body therapies because its primary mechanism is neurocognitive imagery and pain-related sensorimotor representation rather than physical training. Similarly, the category of other integrative or complementary approaches was retained only as a residual mapping category. It includes aromatherapy, spiritual or energy-based interventions, rTMS, and multimodal integrative programs, which should not be interpreted as clinically equivalent. This distinction was added to avoid overgeneralization from heterogeneous interventions.
Generalizability and Geographic Concentration
A large proportion of included RCTs originated from China, particularly trials evaluating TCM-centered interventions such as acupuncture, Tuina, Baduanjin, moxibustion, Gua Sha, and acupotomy. This concentration is important for interpretation. Trials conducted in Chinese TCM hospitals or TCM-integrated health systems may involve provider training, patient expectations, treatment credibility, cultural familiarity, and care pathways that differ from those in non-TCM health systems. Therefore, generalizability to regions where these therapies are less integrated into routine care should be considered cautiously. Future trials should include more diverse healthcare contexts and report setting-specific implementation factors.
Specific Evidence Gaps Identified from Included Trials
The included studies suggest several specific gaps. First, direct comparisons between major CAM categories, such as acupuncture versus manual therapy, acupuncture versus structured exercise, and mind-body exercise versus conventional strengthening, remain limited. Second, long-term follow-up beyond 6 to 12 months is uncommon, limiting evidence on durability and maintenance. Third, implementation outcomes such as adherence, fidelity, provider training, patient preference, treatment credibility, cost, and scalability are under-reported. Fourth, mechanistic outcomes are concentrated in a small subset of studies and are rarely linked to pragmatic clinical outcomes. Fifth, many trials lack detailed reporting of KOA severity, comorbidities, medication use, and population characteristics needed to evaluate applicability to older adults, frail patients, or patients with advanced structural disease.
Strengths and Limitations
This review has several strengths. It focused on RCTs, covered multiple databases, used duplicate screening and data charting, and mapped intervention categories, outcome domains, comparator types, follow-up schedules, and key design characteristics. The revision also included complete database-specific search strategies, clarified eligibility for pharmacological comparators and combination designs, followedthe PRISMA flow, and included a design-characteristic summary.
This review also has limitations. First, no formal risk-of-bias assessment or certainty grading was performed, consistent with the scoping objective, so the results should not be interpreted as comparative efficacy conclusions. Second, because only English-language publications were included, relevant trials in other languages may have been missed. Third, the broad review concept produced substantial heterogeneity, especially in the residual category of other integrative or complementary approaches. Fourth, some methodological details were incompletely reported in the included trials, limiting the granularity of the evidence map. Fifth, the geographic concentration of TCM-centered trials may limit generalizability.
Conclusions
This scoping review maps a broad and heterogeneous body of RCT evidence on non-pharmacological CAM and related integrative interventions for KOA. The available trials are concentrated in several intervention clusters, especially acupuncture-related therapies, exercise and mind-body programs, manual and body-based therapies, and physical agent modalities. The evidence base is characterized by diverse comparators, short-term follow-up, variable reporting of intervention dose and provider features, and uneven reporting of design quality signals. Rather than supporting direct comparative effectiveness claims, the review identifies where evidence is concentrated and where research remains insufficient. Future work should prioritize transparent reporting, longer follow-up, better characterization of intervention fidelity and implementation context, more diverse populations and settings, and targeted systematic reviews or pragmatic trials where the evidence base is sufficiently mature.
Abbreviations
AE, adverse event; CAM, complementary and alternative medicine; KOA, knee osteoarthritis; PCC, population-concept-context; PRISMA-ScR, Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews; RCT, randomized controlled trial; TCM, traditional Chinese medicine.
Data Sharing Statement
All data generated or analyzed during this study are included in this article and its supplementary materials; additional materials are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Hunan Provincial Natural Science Foundation (2026JJ82657).
Disclosure
The authors declare that they have no competing interests.
References
1. Glyn-Jones S, Palmer AJ, Agricola R, et al. Osteoarthritis. Lancet. 2015;386(9991):376–19. doi:10.1016/S0140-6736(14)60802-3
2. GBD 2021 Osteoarthritis Collaborators. Global, regional, and national burden of osteoarthritis, 1990-2020 and projections to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(9):e508–e522. doi:10.1016/S2665-9913(23)00163-7
3. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, Hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578–1589. doi:10.1016/j.joca.2019.06.011
4. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2020;72(2):149–162. Erratum in: Arthritis Care Res. 2021;73(5):764. doi:10.1002/acr.24131. doi:10.1002/acr.24131
5. Bally M, Dendukuri N, Rich B, et al. Risk of acute myocardial infarction with NSAIDs in real world use: bayesian meta-analysis of individual patient data. BMJ. 2017;357:j1909. doi:10.1136/bmj.j1909
6. Macfarlane GJ, Paudyal P, Doherty M, et al. A systematic review of evidence for the effectiveness of practitioner-based complementary and alternative therapies in the management of rheumatic diseases: osteoarthritis. Rheumatology. 2012;51(12):2224–2233. doi:10.1093/rheumatology/kes200
7. Liu CY, Duan YS, Zhou H, et al. Clinical effect and contributing factors of acupuncture for knee osteoarthritis: a systematic review and pairwise and exploratory network meta-analysis. BMJ Evid Based Med. 2024;29(6):374–384. doi:10.1136/bmjebm-2023-112626
8. Yan L, Li D, Xing D, et al. Comparative efficacy and safety of exercise modalities in knee osteoarthritis: systematic review and network meta-analysis. BMJ. 2025;391:e085242. doi:10.1136/bmj-2025-085242
9. Mapinduzi J, Ndacayisaba G, Mitchaϊ PM, et al. Supervised or home-based? Exploring the best exercise approach for knee osteoarthritis management: a systematic review and meta-analysis. J Clin Med. 2025;14(2):525. doi:10.3390/jcm14020525
10. Tang L, Wang MM, Wang HX, et al. mHealth-based exercise vs. traditional exercise on pain, functional disability, and quality of life in patients with knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Front Physiol. 2025;15:1511199. doi:10.3389/fphys.2024.1511199
11. Moseng T, Vliet Vlieland TPM, Battista S, et al. EULAR recommendations for the non-pharmacological core management of Hip and knee osteoarthritis: 2023 update. Ann Rheum Dis. 2024;83(6):730–740. doi:10.1136/ard-2023-225041
12. Ferreira RM, Martins PN, Gonçalves RS. Non-pharmacological and non-surgical interventions to manage patients with knee osteoarthritis: an umbrella review 5-year update. Osteoarthr Cartil Open. 2024;6(3):100497. doi:10.1016/j.ocarto.2024.100497
13. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
14. Cherian JJ, Harrison PE, Benjamin SA, et al. Do the effects of transcutaneous electrical nerve stimulation on knee osteoarthritis pain and function last? J Knee Surg. 2016;29(6):497–501. doi:10.1055/s-0035-1566735
15. Wang C, Schmid CH, Iversen MD, et al. Comparative effectiveness of tai chi versus physical therapy for knee osteoarthritis: a randomized trial. Ann Intern Med. 2016;165(2):77–86. doi:10.7326/M15-2143
16. Elbadawy MA. Effectiveness of periosteal stimulation therapy and home exercise program in the rehabilitation of patients with advanced knee osteoarthritis. Clin J Pain. 2017;33(3):254–263. doi:10.1097/AJP.0000000000000404
17. Hausmann LRM, Youk A, Kwoh CK, et al. Testing a positive psychological intervention for osteoarthritis. Pain Med. 2017;18(10):1908–1920. doi:10.1093/pm/pnx141
18. Park J, McCaffrey R, Newman D, et al. A pilot randomized controlled trial of the effects of chair yoga on pain and physical function among community-dwelling older adults with lower extremity osteoarthritis. J Am Geriatr Soc. 2017;65(3):592–597. doi:10.1111/jgs.14717
19. Altmış H, Oskay D, Elbasan B, et al. Mobilization with movement and kinesio taping in knee arthritis-evaluation and outcomes. Int Orthop. 2018;42(12):2807–2815. doi:10.1007/s00264-018-3938-3
20. Innes KE, Selfe TK, Kandati S, et al. Effects of mantra meditation versus music listening on knee pain, function, and related outcomes in older adults with knee osteoarthritis: an exploratory Randomized Clinical Trial (RCT). Evid Based Complement Alternat Med. 2018;2018:7683897. doi:10.1155/2018/7683897
21. Kong J, Wang Z, Leiser J, et al. Enhancing treatment of osteoarthritis knee pain by boosting expectancy: a functional neuroimaging study. Neuroimage Clin. 2018;18:325–334. doi:10.1016/j.nicl.2018.01.021
22. Lin LL, Li YT, Tu JF, et al. Effectiveness and feasibility of acupuncture for knee osteoarthritis: a pilot randomized controlled trial. Clin Rehabil. 2018;32(12):1666–1675. doi:10.1177/0269215518790632
23. Wang P, Zhang C-R, Chen D-C, et al. A randomized controlled trial on the treatment of knee osteoarthritis with acupotomy therapy based on the Meridian sinew theory. World J Acupunct Moxibustion. 2018;28(4):246–250. doi:10.1016/j.wjam.2018.12.009
24. Lv ZT, Shen LL, Zhu B, et al. Effects of intensity of electroacupuncture on chronic pain in patients with knee osteoarthritis: a randomized controlled trial. Arthritis Res Ther. 2019;21(1):120. doi:10.1186/s13075-019-1899-6
25. Perlman A, Fogerite SG, Glass O, et al. Efficacy and safety of massage for osteoarthritis of the knee: a randomized clinical trial. J Gen Intern Med. 2019;34(3):379–386. doi:10.1007/s11606-018-4763-5
26. Chen H, Wang Y, Liu C, et al. Benefits of a transtheoretical model-based program on exercise adherence in older adults with knee osteoarthritis: a cluster randomized controlled trial. J Adv Nurs. 2020;76(7):1765–1779. doi:10.1111/jan.14363
27. Wang Q, Lu T, Cai G, et al. Therapeutic effect observation on thumb-tack needling for knee osteoarthritis in elderly patients: a random control trial. World J Acupunct Moxibustion. 2020;30(4):268–271. doi:10.1016/j.wjam.2020.11.006
28. Wang TQ, Li YT, Wang LQ, et al. Electroacupuncture versus manual acupuncture for knee osteoarthritis: a randomized controlled pilot trial. Acupunct Med. 2020;38(5):291–300. doi:10.1177/0964528419900781
29. Ye J, Zheng Q, Zou L, et al. Mindful Exercise (Baduanjin) as an adjuvant treatment for older adults (60 Years Old and Over) of knee osteoarthritis: a randomized controlled trial. Evid Based Complement Alternat Med. 2020;2020:9869161. doi:10.1155/2020/9869161
30. Zhu J, Zheng Z, Liu Y, et al. The effects of small-needle-knife therapy on pain and mobility from knee osteoarthritis: a pilot randomized-controlled study. Clin Rehabil. 2020;34(12):1497–1505. doi:10.1177/0269215520938852
31. Alinaghizadeh M, Hawkins J, Abbassian A, et al. Effect of Persian acupressure (Ghamz) on patients with knee osteoarthritis: a single-blinded parallel clinical trial. Pain Manag Nurs. 2021;22(6):820–827. doi:10.1016/j.pmn.2021.06.002
32. Bunsanong T, Chaimongkol N. A self-management support intervention on knee functional status and health-related quality of life among middle-age women: a randomized controlled trial. J Adv Nurs. 2021;77(1):376–386. doi:10.1111/jan.14600
33. Guo JM, Xiao Y, Cai TY, et al. Chinese medicine involving triple rehabilitation therapy for knee osteoarthritis in 696 outpatients: a multi-center, randomized controlled trial. Chin J Integr Med. 2021;27(10):729–736. doi:10.1007/s11655-021-3488-6
34. Lam WC, Au KY, Qin Z, et al. Superficial needling acupuncture vs sham acupuncture for knee osteoarthritis: a randomized controlled trial. Am J Med. 2021;134(10):1286–1294.e2. doi:10.1016/j.amjmed.2021.05.002
35. Maheu E, Soriot-Thomas S, Noel E, et al. Wearable transcutaneous electrical nerve stimulation (actiTENS®) is effective and safe for the treatment of knee osteoarthritis pain: a randomized controlled trial versus weak opioids. Ther Adv Musculoskelet Dis. 2022;14:1759720X211066233. doi:10.1177/1759720X211066233
36. Tu JF, Yang JW, Shi GX, et al. Efficacy of intensive acupuncture versus sham acupuncture in knee osteoarthritis: a randomized controlled trial. Arthritis Rheumatol. 2021;73(3):448–458. doi:10.1002/art.41584
37. Zacaron KAM, Dos Santos CS, Corrêa CPS, et al. Effect of laying on of hands as a complementary therapy for pain and functioning in older women with knee osteoarthritis: a randomized controlled clinical trial. Int J Rheum Dis. 2021;24(1):36–48. doi:10.1111/1756-185X.13952
38. Bennell KL, Schwartz S, Teo PL, et al. Effectiveness of an unsupervised online yoga program on pain and function in people with knee osteoarthritis: a randomized clinical trial. Ann Intern Med. 2022;175(10):1345–1355. doi:10.7326/M22-1761
39. Dasa V, Skrepnik NV, Petersen D, et al. A novel mobile app-based neuromuscular electrical stimulation therapy for the management of knee osteoarthritis: results from an extension study of a randomized, double-blind, sham-controlled, multicenter trial. J Am Acad Orthop Surg Glob Res Rev. 2022;6(9):e2200115. doi:10.5435/JAAOSGlobal-D-22-00115
40. Sax OC, Gesheff MG, Mahajan A, et al. A novel mobile app-based neuromuscular electrical stimulation therapy for improvement of knee pain, stiffness, and function in knee osteoarthritis: a randomized trial. Arthroplast Today. 2022;15:125–131. doi:10.1016/j.artd.2022.03.007
41. Woo SH, Lee HJ, Park YK, et al. Efficacy and safety of thread embedding acupuncture for knee osteoarthritis: a randomized controlled pilot trial. Medicine. 2022;101(31):e29306. doi:10.1097/MD.0000000000029306
42. Artuç ŞE, Uçkun AÇ, Sivas FA, et al. Comparison of the effects of transcutaneous electrical nerve stimulation and interferential current therapies in central sensitization in patients with knee osteoarthritis. Korean J Pain. 2023;36(3):392–403. doi:10.3344/kjp.23118
43. Deng Y, Zhang M, Li W, et al. Investigation of the therapeutic effect and mechanism of holographic meridian scraping therapy on knee osteoarthritis. Altern Ther Health Med. 2023;29(7):440–443. PMID: 37573584. doi:10.1089/ath.2023.0036
44. Zheng A, Zheng F, Jin K, et al. Manual Acupuncture at LI11, local points and both for knee osteoarthritis: a pilot randomized controlled trial. J Pain Res. 2023;16:4393–4404. doi:10.2147/JPR.S445770
45. Zhou J, Zeng F, Cheng S, et al. Modulation effects of different treatments on periaqueductal gray resting state functional connectivity in knee osteoarthritis knee pain patients. CNS Neurosci Ther. 2023;29(7):1965–1980. doi:10.1111/cns.14153
46. Gillcrist RL, Doherty CR, Olave M, et al. A remote behaviorally designed intervention to promote physical activity in patients with knee osteoarthritis: results of a pilot randomized clinical trial. J Clin Rheumatol. 2024;30(8):336–339. doi:10.1097/RHU.0000000000002148
47. Döner Şİ, Gerçek H, Sert ÖA, et al. The effects of aromatherapy massage in menopausal women with knee osteoarthritis: a randomized controlled study. Explore. 2024;20(6):103014. doi:10.1016/j.explore.2024.05.012
48. Mou J, Wang Q, Wu J, et al. The effect of Fu’s subcutaneous needling in treating knee osteoarthritis patients: a randomized controlled trial. Explore. 2024;20(4):562–571. doi:10.1016/j.explore.2023.12.015
49. Abafita BJ, Singh A, Aitken D, et al. Yoga or strengthening exercise for knee osteoarthritis: a randomized clinical trial. JAMA Network Open. 2025;8(4):e253698. doi:10.1001/jamanetworkopen.2025.3698
50. Agost-González A, Escobio-Prieto I, de Los Ángeles Cardero-Durán M, et al. Effects of dry needling combined with exercise on knee osteoarthritis at 6 month follow up a randomized clinical trial. Sci Rep. 2025;15(1):44117. doi:10.1038/s41598-025-27821-0
51. Akdeniz G, Tığlı K, Akıncı NE, et al. Mental imagery enhances pain reduction and visual processing in knee osteoarthritis patients: a comparative study. Pain Res Manag. 2025;2025:5576698. doi:10.1155/prm/5576698
52. Atan T, Bildik YE, Demir Y, et al. Comparison of anti-gravity treadmill training and traditional treadmill training in patients with moderate to severe knee osteoarthritis: a randomized controlled trial. Ir J Med Sci. 2025;194(1):125–136. doi:10.1007/s11845-024-03836-w
53. Awan S, Rehman AU, Khan MI, et al. Sports medicine-based isokinetic rehabilitation of the quadriceps in knee osteoarthritis. Int J Pharm Res Technol. 2025;15(2):2028–2036. doi:10.48047/ijprt/15.02.270
54. Dantas AT, Braga M, Barreto G, et al. Effect of manual therapy and transcranial magnetic stimulation on pain in knee osteoarthritis: a randomized clinical trial. J Manipulative Physiol Ther. 2025;48(1–5):311–318. doi:10.1016/j.jmpt.2025.10.009
55. Godziuk K, Forhan M, Vieira FT, et al. Improving muscle function through a multimodal behavioural intervention for knee osteoarthritis and obesity: the POMELO Trial. J Cachexia Sarcopenia Muscle. 2025;16(4):e70025. doi:10.1002/jcsm.70025
56. Guo X, Guo L, Lu QZ, et al. Effect of electroacupuncture combined with Tuina therapy on gut microbiota in patients with knee osteoarthritis. World J Gastroenterol. 2025;31(18):105495. doi:10.3748/wjg.v31.i18.105495
57. Hanley AW, Nakamura Y, Edwards RR, et al. Complementary therapies for chronic knee pain: a placebo-controlled RCT of Reiki and mindfulness. Complement Ther Med. 2025;95:103278. doi:10.1016/j.ctim.2025.103278
58. Katz JN, Collins JE, Bisson L, et al. A randomized trial of physical therapy for meniscal tear and knee pain. N Engl J Med. 2025;393(17):1694–1703. doi:10.1056/NEJMoa2503385
59. Kızkın ZY, Oğuz S, Ak S. The effect of graded motor imagery on pain and function in individuals with knee osteoarthritis: a comparative randomized controlled trial. Am J Phys Med Rehabil. 2025;104(6):534–543. doi:10.1097/PHM.0000000000002663
60. Ma P, Liu L, Li S, et al. Comparative effectiveness of Tuina therapy versus manual physical therapy for knee osteoarthritis: a randomized controlled trial. BMC Complement Med Ther. 2025;25(1):128. doi:10.1186/s12906-025-04850-w
61. Momen Arani Z, Zamani B, Barati AM, et al. The effect of aromatherapy massage with peppermint oil on functional impairments in patients with knee osteoarthritis. Int J Orthop Trauma Nurs. 2025;59:101221. doi:10.1016/j.ijotn.2025.101221
62. Ng HP, Tan CY, Lim CJ, et al. Heat and acupuncture restore mobility in knee osteoarthritis (HARMOKnee): a pragmatic integrated care, randomized controlled study. Complement Ther Med. 2025;93:103223. doi:10.1016/j.ctim.2025.103223
63. Sun J, Liang Y, Luo KT, et al. Efficacy of different acupuncture techniques for pain and dysfunction in patients with knee osteoarthritis: a randomized controlled trial. Pain Ther. 2025;14(2):737–751. doi:10.1007/s40122-025-00713-x
64. Tsai AWW, Hsing WT, Ueda MYH, et al. Acupuncture plus cupping relieve pain and reduce the consumption of analgesics in patients with advanced knee osteoarthritis. Med Acupunct. 2025;37(6):442–449. doi:10.1177/19336586251374534
65. Wei XY, Wang ZY, Shi GX, et al. Effect of acupuncture treatment for patients with knee osteoarthritis on brain fluctuation amplitude and functional connectivity: a randomized three-armed fMRI study. BMC Complement Med Ther. 2025;25(1):244. doi:10.1186/s12906-025-04985-w
66. Bakir E, Baglama SS. The effect of foot reflexology and knee massage with black cumin seed oil on knee osteoarthritis symptoms. Holist Nurs Pract. 2026;40(1):56–65. doi:10.1097/HNP.0000000000000714
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Acupuncture on the Cognitive Control Network of Patients with Knee Osteoarthritis: Study Protocol for a Randomized Controlled Trial

Yin S, Zhang ZH, Chang YN, Huang J, Wu ML, Li Q, Qiu JQ, Feng XD, Wu N
Journal of Pain Research 2022, 15:1443-1455
Published Date: 18 May 2022
Predictive Value of Pain Sensitization Associated with Response to Exercise Therapy in Patients with Knee Osteoarthritis: A Prospective Cohort Study
Hattori T, Ohga S, Shimo K, Niwa Y, Tokiwa Y, Matsubara T
Journal of Pain Research 2022, 15:3537-3546
Published Date: 8 November 2022
Acupuncture and Related Therapies for Endometriosis: A Network Meta-Analysis of Randomized Controlled Trials
Li H, Wang X, Wang Y, Gao Y, Zheng X, Zhang X, Li X, Zheng X, Fan X, Zuo G, She Y
Journal of Pain Research 2024, 17:3197-3216
Published Date: 2 October 2024
Efficacy and Safety of Non-Pharmacological Therapies for Primary Dysmenorrhea: A Network Meta-Analysis
Liu J, Wang Y, Zhang J, Fan X, Chen H, Zuo G, Wang X, She Y
Journal of Pain Research 2025, 18:975-991
Published Date: 27 February 2025
Therapeutic Potential of Acupuncture in Knee Osteoarthritis: Clinical Efficacy and Mechanistic Insights
Yao K, Shamim MF, Xia J, Liu TT, Guo Y, Lin X
Journal of Inflammation Research 2025, 18:12169-12190
Published Date: 5 September 2025