Back to Journals » Journal of Pain Research » Volume 18
No Evidence for a Causal Association Between Depression and Herpes Zoster or Post-Herpetic Neuralgia: A Mendelian Randomization Study
Authors Zhang X ![]() , Chen Y
, Chen Y ![]() , Lin J, Guo W, Zhou H, Yang X, Zhao Q
, Lin J, Guo W, Zhou H, Yang X, Zhao Q ![]()
Received 12 July 2025
Accepted for publication 26 November 2025
Published 6 December 2025 Volume 2025:18 Pages 6579—6589
DOI https://doi.org/10.2147/JPR.S553378
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor King Hei Stanley Lam
Xuerong Zhang,* Yuqing Chen,* Jingrun Lin,* Weibing Guo, Hongchun Zhou, Xueying Yang, Qiong Zhao
Department of Anesthesiology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, 510120, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiong Zhao, Department of Anesthesiology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, Guangdong, 510120, People’s Republic of China, Tel +86-177-2425-0727, Email [email protected] Xueying Yang, Department of Anesthesiology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, Guangdong, 510120, People’s Republic of China, Tel +86-188-0204-0810, Email [email protected]
Background: Observational studies have suggested a correlation between depression and herpes zoster (HZ), as well as post-herpetic neuralgia (PHN); however, the causal relationship remains unclear. This study aimed to assess the causal relationships between depression and HZ and PHN via a two-sample bidirectional Mendelian randomization (MR) approach.
Methods: We collected data for major depressive disorder (MDD, 246,363 cases/561,190 controls), depressive status (442,840 individuals), HZ (7,132 cases/480,316 controls) and PHN (490 cases/435,371 controls) from genome-wide association studies (GWASs) in European populations, along with depression-related consultations (430 cases/2,152 controls) and zoster infections (2,209 cases/166,603 controls), for validation analysis in East Asian populations. We employed inverse variance weighted (IVW), MR-Egger, weighted median, weighted mode, and MR-PRESSO for our analysis.
Results: Although suggestive, no statistically significant associations were found between genetic MDD and the risk of HZ (IVW, OR: 1.190, 95% CI: 0.984– 1.439, P=0.073) or PHN (IVW, OR: 0.820, 95% CI: 0.428– 1.570, P=0.549) in Europeans. The same was true for depressive status and HZ (IVW, OR: 1.688, 95% CI: 0.820– 3.477, P=0.155) or PHN risk (IVW, OR: 9.535, 95% CI: 0.227– 400.820, P=0.237). In East Asians, genetic depression-related consultation did not significantly affect the risk of herpes infection (IVW, OR: 0.976, 95% CI: 0.922– 1.033, P=0.401). No reverse causality was observed.
Conclusion: A comprehensive MR study suggested that depression is not causally related to susceptibility to HZ or PHN, and vice versa. Future studies should focus on how environmental/clinical, not genetic factors that cause depression affect the risk of HZ and PHN.
Keywords: depression, herpes zoster, post-herpetic neuralgia, mendelian randomization
Introduction
Depression, often accompanied by anxiety, sleep disorders, and immune dysfunction, is a prevalent mental condition characterized by pronounced and enduring glooming.1 A WHO statistical analysis in March 2023 revealed that approximately 280 million people worldwide suffer from depression, with a prevalence of 3.8%, and that approximately 5% of adults suffer from depression; depression is projected to be the number one disease burden globally by 2030.2 Most of the current antidepressant treatment regimens are for temporary control of symptoms and maintenance of a person’s basic ability to live; they cannot be cured, and etiologic treatment seems to be more important. The etiology of depression is complex and involves genetic, biochemical, and psychosocial factors. Certain viral infections, such as herpesvirus and influenza virus, are linked to the onset and worsening of depression.3 Depressed individuals have a 1.3 times greater incidence of zoster than healthy controls do (4.58 per 1,000 person-years vs 3.54 per 1,000 person-years).1 Herpes viruses may be more easily activated in depressed patients, leading to neuroinflammation and nerve damage, which can exacerbate the symptoms of depression.4 Moreover, studies have shown that individuals with depression exhibit significantly lower frequencies of varicella-zoster virus (VZV)-specific reactive cells than healthy controls do, and this reduction is negatively correlated with the severity of depressive symptoms.5,6
VZV is a highly contagious double-stranded DNA virus. Initial infection with VZV through droplets or direct contact in childhood typically presents as chickenpox, characterized by symptoms including fever, a pruritic rash, and the formation of blisters. After chickenpox resolves, a minor fraction of VZV evades immune clearance by downregulating the expression of major histocompatibility complex class I on the infected cell surface, persisting in a latent and prolonged state within the dorsal root sensory ganglia of the host spinal cord.7 When the body’s immunity decreases (eg, in elderly individuals, immunosuppressed patients, chronic stress patients, etc)., the virus may reactivate replication and spread along nerve fibers, leading to herpes zoster (HZ), which manifests as a painful rash and blisters distributed along the nerves, commonly unilaterally on the chest, lower back, or face. The pain may be very severe, such as cuts, pins and needles, or electric shocks, and may persist for more than 3 months even after the rash has subsided; it may even develop into post-herpetic neuralgia (PHN).8 Research has indicated that within 90 days of zoster onset, 55% of patients experience depression and anxiety. By 180 days post-rash onset, 45% of patients remain depressed due to PHN.9 A separate study indicated that PHN significantly impacts quality of life and persistent pain, and the limited effectiveness of current treatments may result in depression, substance dependence, feelings of hopelessness, and potentially suicide.10
Recent observational studies indicate that individuals with depression are at increased risk of developing HZ and PHN, and patients with HZ or PHN are more likely to be depressed.9–12 Nonetheless, other investigations have indicated a null correlation between them.13,14 Determining whether there is a genuine causal relationship between depression and HZ and its associated neuralgia will deepen our understanding of disease mechanisms, optimize health education and treatment strategies, and further reduce the waste of healthcare resources. However, existing observational studies9–14 have relatively small sample sizes, making it impossible to determine the temporal sequence between exposure and outcome and unable to avoid confounding factors (clinical or environmental factors) and selection bias, which hinders the establishment of causal relationships. Randomized controlled trials, recognized as the gold standard for causal inference methods, require significant labor investment and large sample sizes for rare diseases. They also have difficulty passing ethical reviews for high-risk diseases and often necessitate long follow-up times, resulting in poor compliance. Here, we employed Mendelian randomization (MR) to investigate the potential causal relationship between depression and HZ or PHN. MR is a causal inference method that uses genetic variation as instrumental variables (IVs) to evaluate causal relationships between exposures and outcomes.15 The random assignment of genes during gamete formation establishes genetic variation at conception, which minimizes the impact of confounding factors on causal inference. MR studies can address the effects of lifetime exposures, circumvent ethical issues, and leverage existing large-sample-size Genome-Wide Association Study (GWAS) data to infer causal relationships between multiple exposures and diseases broadly and efficiently.
Method
Study Design
Our bidirectional two-sample Mendelian randomization trial strictly followed the STROBE-MR guidelines16 (Supplementary Table 1). For forward MR, we applied depression as exposures and HZ and PHN as outcomes. For reverse MR, we applied HZ and PHN as exposures and depression as outcomes. In addition, we aimed to strengthen our conclusions via the GWAS dataset from two distinct populations.
Data Resources
GWAS for the European Population
For Europeans, the dataset for depression was obtained from the current and largest GWAS meta-analysis conducted by Howard DM,17 which included 33 cohorts from the Psychiatric Genomics Consortium (PGC),18 the broad depression phenotype from the UK Biobank (UKB),19 and the discovery cohort from 23andMe.20 This dataset17 included 807,553 participants (246,363 patients and 561,190 controls), and 102 single-nucleotide polymorphisms (SNPs) were identified as significantly related to major depressive disorder (MDD). In the PGC, depression was identified on the basis of international consensus diagnostic criteria (DSM-IV, ICD-9, or ICD-10).18 In the UKB, an expansive definition of depression was utilized, asking individuals whether they had disclosed symptoms of mental problems, worry, stress, or depression to their medical practitioner or psychiatrist.19
To control for confounding effects from variations in depression intensity, we adopted an additional dataset reflecting depressive status from a study conducted by the Medical Research Council-Integrative Epidemiology Unit (MRC-IEU) consortium (https://gwas.mrcieu.ac.uk/), which contains 442,840 individuals experiencing a specific rate of depression over 14 days. The raw genetic data were normalized via Z scores prior to subsequent analysis, given the large beta values in the original dataset.
Summary-level information for HZ21 was collected from the FinnGen Consortium, which analyzed 21,311,644 variants, including 7,132 patients and 480,316 controls, classified under certain infectious and parasitic diseases (AB1). For PHN,21 which was also sourced from the FinnGen Consortium, 435,861 individuals of European descent, comprising 490 patients and 435,371 controls, were classified as having VI diseases of the nervous system.
GWAS for East Asian Population
For East Asians, as an independent replication, the dataset for depression-related consultation was derived from the UKB (http://www.nealelab.is/uk-biobank), which consists of 2,582 individuals from East Asia (430 cases and 2,152 controls). The validation dataset for HZs, constructed by Sakaue S,22 included 2,209 cases and 166,603 controls. Regrettably, we were unable to discover any available databases on PHN for East Asian populations to date.
Importantly, the samples from the depression, HZ, and PHN datasets used in this research did not overlap. The overall research plan is depicted in Figures 1–2, and the comprehensive data sources are presented in Table 1.
 |
Table 1 A Comprehensive Summary of the GWAS Datasets Utilized in the MR Study |
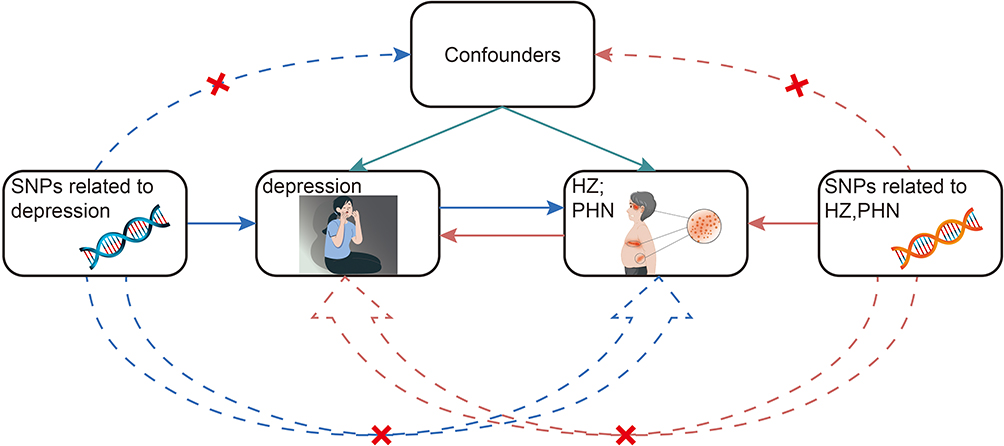 |
Figure 1 Basic assumptions of Mendelian randomization. The red cross symbol indicates that the path of the SNP is not allowed to be strongly associated with the trait. It reflects the second rule of instrumental variable selection (the instrumental variables are independent of confounding factors) and the third rule (the instrumental variables are not directly related to the outcome) in Mendelian randomization. Abbreviations: HZ, herpes zoster; PHN, post-herpetic neuralgia; SNP, single-nucleotide polymorphism. |
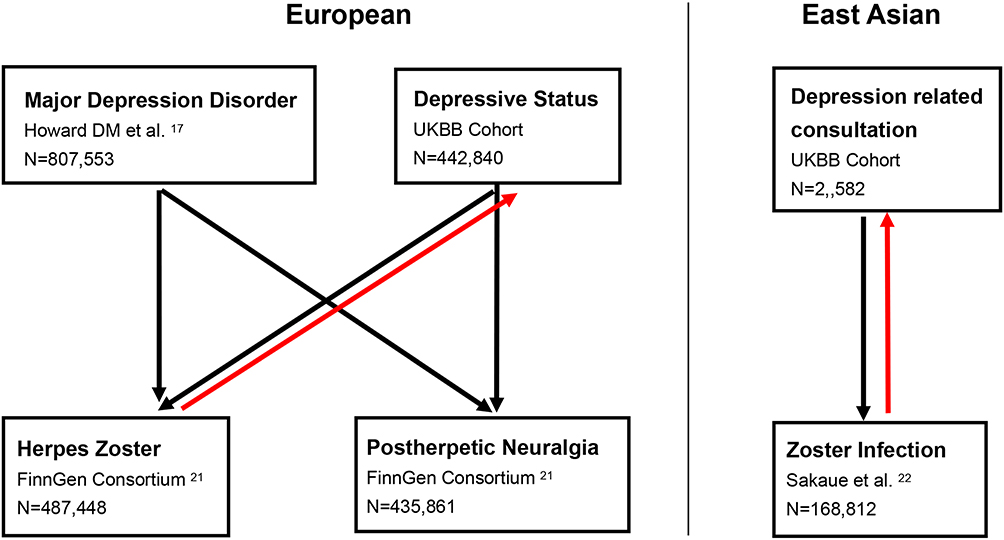 |
Figure 2 Overview of the MR analysis and datasets used in this study. Sample sizes (N) for all datasets and cohorts, as well as different directions (arrows) of MR exposure-outcome analyses. |
Screening of Instrumental Variables
The screening of instrumental variables (IVs) must fulfill the following 3 conditions simultaneously (Figure 1): 1. Association: IVs (genetic variants) are linked to exposure. 2. Independence: IVs are not confounded by any relevant factors (malignant tumors, autoimmune diseases, diabetes mellitus, immunosuppressed status due to medication, HIV infection, or organ transplantation),23,24 as studies support that these common conditions can lead to reduced immunity, significantly increasing the risk of herpes infection, and chronic disease status also elevates the risk of depression. 3. Exclusivity: IVs shape the outcomes exclusively through the exposures, not through other routes. For MDD and depressive status as exposures, we set P < 5×10−8 with linkage disequilibrium (LD, r2 < 0.001, kb=10,000). For depression-related consultations, HZ, and PHN as exposures, as no SNPs can be extracted in the corresponding outcome when P < 5×10−8 or P < 5×10−7, we eventually obtain enough SNPs when P < 5×10−6 with linkage disequilibrium (LD, kb=10,000, r2 < 0.001).25 All IVs were checked through the Phenoscanner database (http://www.phenoscanner.medschl.cam.ac.uk/)26 to verify independence and exclusivity. The power of the IVs was assessed via an equation (F = (β2/se2)).27,28 F>10 indicates strong IVs, and the results are robust and reliable.
Statistical Analysis
We employed four MR methods—the inverse variance weighted (IVW), MR-Egger, weighted median, and weighted mode—to assess the causality between exposures and outcomes. These methods were utilized since they possess distinct foundational premises regarding horizontal pleiotropy. IVW29 is a meta-analysis of the Wald ratio of a single SNP, assuming that all IVs are valid and free of horizontal pleiotropy, and serves as the primary analytical method for our MR analyses. The MR-Egger30 method evaluates the pleiotropy of IVs by detecting whether the intercept is significantly different from zero. The regression line is permitted to deviate from the origin owing to the existence of directional horizontal pleiotropy among the included instrumental variables. A significant intercept term suggests the potential presence of pleiotropy or a breach of the exclusivity assumption for the IVs.30 The weighted median method,31 which takes the median of the effect values of all the genetic variants ranked in order of their weights as an assessment of the causal impact, is insensitive to outliers and provides a robust estimate even if a portion of the instrumental variables are invalidated.31 The weighted mode32 is robust to horizontal pleiotropy, and even in the presence of invalid IVs (eg, proportions as high as 40%), the weighted mode approach maintains low bias and type I error rates.32
Sensitivity analysis, which primarily involves heterogeneity and pleiotropy tests, can be used to assess the robustness of our MR results. Heterogeneity is checked by the Cochran Q test (stemming from the IVW approach29 and MR-Egger30); when the P value of both exceeds 0.05, it suggests no substantive heterogeneity in all IVs. The MR-Egger intercept methods30 along with MR PRESSO33 were used to assess pleiotropy, and when the P value was above 0.05, there was no notable pleiotropy for all IVs. MR-Egger30 detects and corrects for horizontal pleiotropy by introducing an intercept term, which is suitable for situations where horizontal pleiotropy exists, but it is not sensitive to outliers and has lower efficiency. MR-PRESSO,33 on the other hand, corrects for horizontal pleiotropy by detecting and removing outliers, which is suitable for pleiotropy caused by a few outliers, but it may produce a higher false positive rate when there are many invalid IVs. Reliable MR results must be guaranteed to be free of pleiotropy, and when there is no heterogeneity, the estimation leverages a fixed effects model. If there was some heterogeneity, the evaluation involved a random effects model. When there was horizontal pleiotropy, MR-Radial34 was combined with MR-PRESSO to reject some outlier SNPs before performing a secondary MR analysis. The leave-one-out methodology is used to check whether MR calculations are biased or driven by a single SNP. Statistical analyses of the MR studies were conducted via R software (version 4.3.3) along with the R packages “TwoSampleMR”, “MR PRESSO”, and “MR Radial”.
Results
MR Analysis in the European Population
Causal Effects of MDD on HZ and PHN
We obtained 71 MDD-related SNPs, and the causal effect of MDD on HZ risk was null (IVW: OR=1.079, 95% CI=0.906–1.286; P=0.393). Similar results were obtained with the weighted median (OR=1.115, 95% CI= 0.868–1.434, P=0.393) and weighted mode (OR=1.315, 95% CI=0.763–2.267, P=0.328), but significantly reduced HZ susceptibility was also obtained via MR-Egger (OR=0.320, 95% CI=0.119–0.849, P=0.027). In addition, the MR-Egger intercept method revealed pleiotropy (integer-intercept=0.032, P=0.017) (Figure 3, Supplementary Tables 2 and 3). With respect to the inconsistency in the OR effect sizes obtained by the four methods and pleiotropy, we conducted a secondary analysis.
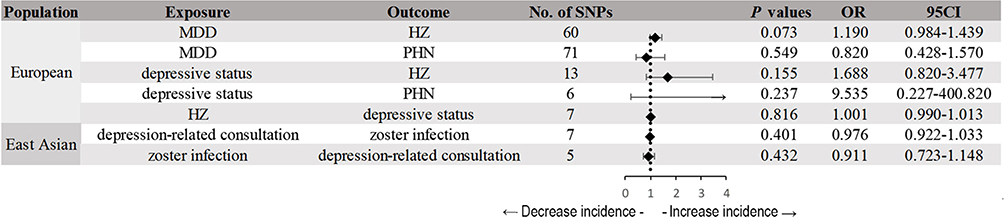 |
Figure 3 IVW-MR was used to assess the causal associations between depression and herpes zoster (HZ) and post-herpetic neuralgia (PHN). The results are presented as odds ratios (ORs) and 95% confidence intervals (CIs). Abbreviations: IVW, inverse variance weighted; MR, Mendelian randomization. |
Five outliers (rs34488670, rs3823624, rs4346585, rs5734448, and rs5995992) were identified via MR-Radial (Supplementary Figure 1 and Supplementary Table 4). Phenoscape was then employed to screen for six SNPs that may serve as confounders. rs2568958 was highly correlated with BMI, as previous studies have shown that BMI is significantly associated with HZ.35 Education level was associated with 4 SNPs (rs10149470, rs12967855, rs17641524, and rs34937911), as we considered that a higher education level could be associated with better perceptions of and compliance with medical treatment for both depression and HZ. Diabetes is associated with 1 SNP (rs2043539), as our previous study revealed that diabetes can significantly increase the risk of HZ.23
With five outliers and six confounder-related SNPs removed, we obtained 60 IVs for the second MR analysis, and the MR estimates remained insignificant (IVW: OR: 1.190, 95% CI: 0.984–1.439, P=0.073), which is consistent with the evaluation of the other three MR analyses, indicating that the increase in genetically predicted MDD was not significantly correlated with HZ risk and that no pleiotropy was found for the MR-PRESSO (P=0.968) or MR-Egger (intercept=0.021, se=0.014, P=0.146) methods. The Cochran Q test (Q value=41.343, P=0.961) revealed no heterogeneity. The leave-one-out method yielded a final result that was not strongly violated by a single SNP (Supplementary Figure 2, Supplementary Tables 2–5).
With 71 MDD-related SNPs, we found a negative association between MDD and PHN risk (IVW: OR=0.820, 95% CI=0.428–1.570, P=0.549), and the results were further confirmed via MR-Egger (OR=34.026, 95% CI=0.815–1420.619, P = 0.068), the weighted median (OR=1.162, 95% CI=0.453–2.982, P= 0.755) and the weighted mode (OR=1.348, 95% CI =0.176–10.344, P = 0.775). Heterogeneity (Cochran Q P-IVW=0.493) and pleiotropy (MR Egger intercept P=0.051, MR PRESSO P=0.498) were not detected, and the leave-one-out method revealed that no single SNP drove the primary outcome (Supplementary Figure 2, Supplementary Tables 2–5).
Causal Effects of HZ and PHN on MDD
Using screening thresholds at P< 5 × 10−6, we subsequently obtained 7 HZ-related SNPs and 7 PHN-related SNPs.23 However, we failed to extract these exposure-related IVs from the MDD GWAS and therefore could not perform subsequent MR analyses.
Causal Effects of Depressive Status on HZ and PHN
We obtained 13 SNPs to explore the associations between depressive status and HZ. The findings of IVW (OR: 1.688, 95% CI: 0.820–3.477, P=0.155) provided a negative result, which was consistent with the null results of MR Egger (OR: 72.756, 95% CI: 0.120–44,232.633, P=0.217), the weighted median (OR: 1.751, 95% CI: 0.603–5.083, P=0.303), and the weighted mode (OR: 0.595, 95% CI: 0.072–4.919, P=0.639). The sensitivity findings supported the absence of heterogeneity (Cochran Q P-IVW=0.458) and pleiotropy (MR Egger intercept P=0.271, MR PRESSO P=0.461) (Supplementary Figure 3, Supplementary Tables 2–5).
We identified 13 SNPs for depressive status when PHN was the outcome. The four MR methods detected no significant associations between depressive status and PHN; however, the Cochran Q test revealed heterogeneity (Q P−IVW=0.0494). Two outliers were screened with MR-Radial (rs12330258, rs618869) (Supplementary Figure 4 and Supplementary Table 6), and the remaining 11 SNPs were used for a second MR analysis. Because the IVW (OR=19.967, 95% CI=1.031–38,686.535, P=0.048) and MR-Egger (OR=0.006, 95% CI=2.134–1,745,563,791,590.98, P=0.771) estimates were inconsistent, we tightened the IV P value screening limitation to 1 × 10−8 36 and finally, 6 SNPs were utilized as effective IVs. In the third MR approach, IVW (OR: 9.535, 95% CI: 0.227–400.820, P=0.237) became insignificant, as did the other three MR methods did, suggesting that genetics-related MDD was not statistically linked to PHN susceptibility, and sensitivity analyses revealed null pleiotropy (MR Egger intercept P=0.858, MR PRESSO P=0.738) or heterogeneity (Cochran Q P-IVW = 0.754) (Supplementary Figure 3, Supplementary Tables 2–5).
Causal Effects of HZ and PHN on Depressive Status
We identified 8 IVs associated with exposure (HZ) at a relatively lenient threshold (P < 5×10−6), as no SNPs can be extracted in the corresponding outcome when P < 5×10−8 or P < 5×10−7. The F-statistics of the IVs were all above 10, indicating that they were strong instruments (Supplementary Table 5). The results of four MR approaches (IVW: OR 1.001, 95% CI 0.990–1.013, P=0.816) revealed no significant correlation between herpes zoster infection and depressive status. Sensitivity analyses indicated no pleiotropy (MR Egger intercept P=0.902, MR PRESSO P=0.350) or heterogeneity (Cochran Q P-IVW=0.309), and the results were robust (Supplementary Figure 5, Supplementary Tables 2–5).
We subsequently obtained 7 IVs from the PHN GWAS. However, we failed to extract these exposure-related IVs from the depressive status GWAS and therefore could not perform subsequent MR analyses.
MR Analysis in the East Asian Population
Causal Effects of Depression-Related Consultation on Zoster Infection Incidence
As the dataset of depression-related consultations had no IVs in the strict screening criteria (P < 5×10−8 and P < 5×10−7), we applied a loose screening threshold (P < 5×10−6) to obtain 7 IVs. The F-statistic values for individual SNPs, as presented in Supplementary Table 5, ranged from 21–25, with a mean value of 23, indicating that they are strong and valid IVs for subsequent analysis. The IVW results revealed no evidence (OR: 0.976, 95% CI: 0.922–1.033, P=0.401) that depressive status can influence HZ risk, which was consistent with the findings of the other 3 MR methods. The Cochran Q test (P−IVW=0.948), the MR-Egger intercept method (P=0.836), and MR-PRESSO (P=0.948) did not reveal heterogeneity or pleiotropy, suggesting that our results are reliable (Supplementary Figure 6, Supplementary Tables 2–5).
Causal Effects of Zoster Infection on Depression-Related Consultation
Because no IVs in the strict screening criteria (P < 5×10−8 and P < 5×10−7) could be extracted from the outcome dataset, we identified 5 zoster infection-related IVs at relatively loose thresholds (P < 5×10−6). The F-statistic values for all the SNPs were above 10 (ranging from 21–23), suggesting that no weak IVs were included. The results of IVW (OR: 0.911, 95% CI: 0.723–1.148, P=0.432), MR Egger (OR: 0.964, 95% CI: 0.715–1.298, P=0.823), the weighted median (OR: 0.944, 95% CI: 0.722–1.233, P=0.671), and the weighted mode (OR: 0.945, 95% CI: 0.726–1.229, P=0.693) all suggested no significant correlation between herpes infection and depression-related consultation, and the sensitivity analysis suggested no pleiotropy (MR Egger intercept P=0.604, MR PRESSO P=0.733) or heterogeneity (Cochran Q P-IVW=0.694) (Supplementary Figure 6, Supplementary Tables 2–5).
Discussion
People with depression may contract VZV by chance, which can lead to more serious complications. Several studies have reported a suspected association between depression and HZ, but no studies have revealed a clear causal relationship. This study employed MR methods to evaluate the causal or reverse causal relationship between depression and HZ, along with its associated neuralgia. There is no evidence indicating that genetically predicted depression increases susceptibility to HZ and PHN, or vice versa.
Currently, some studies supporting the mechanisms by which depression affects the risk of VZV infection have focused mainly on immune aspects. The VZV-specific responder cell frequency is significantly lower in depressed patients than in age- and sex-matched healthy controls, and this reduced immune response is negatively associated with the intensity of depression symptoms.6 Antidepressant medication improved the reduction in VZV-RCF in the depression group.5 Patients with depression exhibit diminished VZV-CMI responses to VZV vaccination, whereas antidepressant therapy has been linked to the restoration of these responses to normal levels. Increased levels of VZV-CMI are associated with a reduced risk and severity of HZ; therefore, untreated depression may increase both the risk and severity of HZ and diminish the efficacy of VZV vaccination.37 However, in contrast to the results of the studies mentioned above, depressed male patients presented elevated IL-6 levels (immune activation) and reduced natural killer (NK) cell activity (immunosuppression),38 suggesting that these immune changes may be complex. A review noted that the levels of proinflammatory factors (IL-1β, IL-6, TNF-α, and CRP) in depressed patients had opposite results.39 Moreover, the counts of a variety of immune cells (total lymphocytes, CD3+ T cells, CD8+ cytotoxic T cells, T regulatory cells, the CD4+/CD8+ ratio, naïve T cells, and memory T cells) in depressed patients are similar to those in healthy controls.40 This discrepancy in findings may be related to the different sample sizes, study designs, heterogeneity of depression severity or subtype, and environmental/clinical variables. Our study revealed that depression does not increase the risk of HZ/PHN, providing negative genetic evidence in terms of mechanisms. These findings suggest that future research should focus on modifiable environmental and clinical factors associated with depression rather than genetic predispositions.
Most clinical studies still suggest an association between the two. A multicenter prospective study revealed that sleep, enjoyment of life, and general daily activities were affected in individuals with HZ and that depression was common during PHN.9 A European systematic review revealed a significantly greater prevalence of depression in HZs (7.2–7.6/1000 people/year) than in controls (3–5/1000 people/year).12 German depressed patients presented a markedly elevated risk of developing HZ (incidence rate ratio: IRR=1.16; P < 0.0001), PHN (IRR=1.16; P < 0.0001), and HZ recurrence (IRR=1.22; P < 0.0001).11 A meta-analysis that included nine depression-related HZ studies revealed that the risk of HZ was approximately 27% greater in depressed patients than in nondepressed patients (95% CI: 1.08–1.49).4 However, some findings also suggest that there is no significant correlation. Two population-based case-control studies conducted in Denmark and the United Kingdom reported a marginally elevated incidence of HZ among individuals with depression.14 Nevertheless, the incidence of HZ in the depressed group using antidepressant medication was comparable to that in patients who did not use antidepressant medication,14 suggesting that the effect of depression on the onset of HZ may be unclear. A longitudinal follow-up of a national sample cohort in South Korea revealed that the incidence of HZ among depressed individuals varied according to the severity of their depression, with higher rates in patients with mild or unspecified depression and lower rates in patients with severe depression,13 suggesting that there is not a simple linear correlation between depression severity and the incidence of HZ.13 These opposing findings may explain why our MR findings were negative. Consistent with our findings, there has been an MR study that revealed no positive causal association between VZV infection and depression41, but the exposure data applied in that study were the Finnish 2021 version of finn-b-AB1_VARICELLA (case: 710, control: 211856), and the type of disease it studied was Varicella (chickenpox), unlike the Zoster (herpes zoster) we studied, which, as we mentioned in the background, are two disease states of the same viral infection, with initial infection with VZV as chickenpox, which occurs most often in childhood, and disease in which latent VZV is reactivated in adulthood as HZ, and the study did not reverse extrapolate the presence or absence of depression affecting the risk of developing HZ; therefore, our study more fully and adequately explains the noncausal and reverse causal relationship between HZ and depression in adults. In summary, it is difficult for existing observational clinical studies to fully control for all confounding factors (socioeconomic status, psychological stress, comorbid states and therapeutic medications, lifestyle). These environmental or clinical factors can even lead to the simultaneous occurrence of symptoms of depression and herpes zoster.12
To our knowledge, this is the first MR investigation examining the causal validity of the relationship between depression and HZ, together with accompanying neuralgia. Our study has the following strengths: 1. A larger sample size than traditional observational studies, 2. Genetic variables strictly related to exposure, excluding confounders and reverse causality, 3. Multiple MR methods to increase the robustness of the validation findings, and 4. Dual validation in European and East Asian populations.
Our study has several drawbacks: 1. Although we have attempted to avoid interference from known confounders, unknown confounders are unavoidable and may compromise the accuracy of our findings. 2. Although the sample sizes of depression, HZ and its neuralgia GWAS for European and East Asian populations used in our MR analyses are the largest of the known GWAS databases, they exhibited substantial differences. Furthermore, the prevalence of depression could not be compared homogeneously due to differences in recruitment criteria across the original GWASs. However, zoster infection rates were comparable between European and East Asian populations (0.0148 vs 0.0132). Moreover, the relatively small sample size of PHN (490 cases) raises concerns about statistical power. These differences in sample size and population prevalence limit the generalizability of our findings, which may require further validation in future larger GWAS-related studies in various populations. 3. This study utilized datasets involving only MDD, depressive status within the past two weeks, and depression-related medical visits, and further investigations into the effects of other specific depressive disorders, such as post-partum depression, menopausal depression, and depression in elderly individuals or children, could contribute to a more comprehensive understanding of the associations between depression and both HZ and PHN. 4. Owing to the inability to extract sufficient SNPs from the corresponding GWAS databases for the outcomes, the reverse MR analysis could not be sufficiently paired with forward MR for a comprehensive analysis. Therefore, our reverse MR results are relatively incomplete. We look forward to the use of more GWAS databases in the future to address this limitation. 5. As the VZV vaccination programs in Finland and Japan were initiated in 2017 and 2018, respectively, it is unclear whether these GWAS databases have been adjusted for the vaccinated population.
Conclusions
This Mendelian randomization study revealed no causal relationships between depression, herpes zoster, or post-herpetic neuralgia in European or East Asian populations. These findings suggest that the associations observed in clinical studies likely reflect environmental, clinical, or psychosocial factors rather than genetic predispositions. Future work should prioritize prospective cohort studies and mechanistic research on modifiable risk factors.
Data Sharing Statement
All datasets utilized in the present investigation are publicly accessible GWAS summary data (https://gwas.mrcieu.ac.uk/, http://www.nealelab.is/uk-biobank, https://www.finngen.fi/fi/hyodynna_tuloksia), and all data generated or analyzed during this study are included in this published article and its supplementary information files.
Ethics Approval
The study protocol was approved by the Institutional Review Board (IRB) of Sun Yat-sen Memorial Hospital (approval number: SYSEC2-2025-BA-593).
Acknowledgment
We express our sincere appreciation to the FinnGen Consortium, the MRC-IEU database, the PGC collaboration, UKB 23andMe, and the EBI for their generous provision of GWAS data.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
All the authors declare that they have no conflicts of interest.
References
1. Liao CH, Chang CS, Muo CH, Kao CH. High prevalence of herpes zoster in patients with depression. J Clin Psychiatry. 2015;76(9):e1099–e1104. doi:10.4088/JCP.14m09311
2. World health statistics. 2023. – monitoring health for the SDGs.
3. Wang X, Zhang L, Lei Y, et al. Meta-analysis of infectious agents and depression. Sci Rep. 2014;4(1):4530. doi:10.1038/srep04530
4. Steinmann M, Lampe D, Grosser J, et al. Risk factors for herpes zoster infections: a systematic review and meta-analysis unveiling common trends and heterogeneity patterns. Infection. 2024;52(3):1009–1026. doi:10.1007/s15010-023-02156-y
5. Irwin MR, Levin MJ, Carrillo C, et al. Major depressive disorder and immunity to varicella-zoster virus in the elderly. Brain Behav Immun. 2011;25(4):759–766. doi:10.1016/j.bbi.2011.02.001
6. Irwin M, Costlow C, Williams H, et al. Cellular immunity to varicella‐zoster virus in patients with major depression. J Infect Dis. 1998;178(s1):S104–S108. doi:10.1086/514272
7. Ye Y, Li S, Yan X, et al. VZV IE4 downregulates cellular surface MHC-I via sequestering it to the Golgi complex. Cell Mol Life Sci CMLS. 2024;82(1):23. doi:10.1007/s00018-024-05477-9
8. Gnann JW, Whitley RJ. Herpes zoster. N Engl J Med. 2002;347(5):340–346. doi:10.1056/NEJMcp013211
9. Drolet M, Brisson M, Schmader KE, et al. The impact of herpes zoster and postherpetic neuralgia on health-related quality of life: a prospective study. Can Med Assoc J. 2010;182(16):1731–1736. doi:10.1503/cmaj.091711
10. Makharita MY. Prevention of post-herpetic neuralgia from dream to reality: a ten-step model. Pain Physician. 2017;20(2):E209–E220. doi:10.36076/ppj.2017.E220
11. Marijic P, Witte J, Surmann B, et al. The risk of herpes zoster in patients with depressive disorders: a German claims database analysis. Infect Dis Ther. 2025;14(3):627–642. doi:10.1007/s40121-025-01116-3
12. Marijam A, Vroom N, Bhavsar A, Posiuniene I, Lecrenier N, Vroling H. Systematic literature review on the incidence of herpes zoster in populations at increased risk of disease in the EU/EEA, Switzerland, and the UK. Infect Dis Ther. 2024;13(5):1083–1104. doi:10.1007/s40121-024-00963-w
13. Choi HG, Kim EJ, Lee YK, Kim M. The risk of herpes zoster virus infection in patients with depression: a longitudinal follow-up study using a national sample cohort. Medicine. 2019;98(40):e17430. doi:10.1097/MD.0000000000017430
14. Schmidt SAJ, Langan SM, Pedersen HS, et al. Mood disorders and risk of herpes zoster in 2 population-based case-control studies in Denmark and the United Kingdom. Am J Epidemiol. 2018;187(5):1019–1028. doi:10.1093/aje/kwx338
15. Bowden J, Holmes MV. Meta‐analysis and
16. Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the reporting of observational studies in epidemiology using mendelian randomization: the STROBE-MR statement. JAMA. 2021;326(16):1614–1621. doi:10.1001/jama.2021.18236
17. Howard DM, Adams MJ, Clarke TK, et al. Genome-wide meta-analysis of depression identifies 102 independent variants and highlights the importance of the prefrontal brain regions. Nat Neurosci. 2019;22(3):343–352. doi:10.1038/s41593-018-0326-7
18. Wray NR, Ripke S, Mattheisen M, et al. Genome-wide association analyses identify 44 risk variants and refine the genetic architecture of major depression. Nat Genet. 2018;50(5):668–681. doi:10.1038/s41588-018-0090-3
19. Howard DM, Adams MJ, Shirali M, et al. Genome-wide association study of depression phenotypes in UK biobank identifies variants in excitatory synaptic pathways. Nat Commun. 2018;9(1):1470. doi:10.1038/s41467-018-03819-3
20. Hyde CL, Nagle MW, Tian C, et al. Identification of 15 genetic loci associated with risk of major depression in individuals of european descent. Nat Genet. 2016;48(9):1031–1036. doi:10.1038/ng.3623
21. Kurki MI, Karjalainen J, Palta P, et al. FinnGen provides genetic insights from a well-phenotyped isolated population. Nature. 2023;613:7944):508–518. doi:10.1038/s41586-022-05473-8
22. Sakaue S, Kanai M, Tanigawa Y, et al. A cross-population atlas of genetic associations for 220 human phenotypes. Nat Genet. 2021;53(10):1415–1424. doi:10.1038/s41588-021-00931-x
23. Yang X, Li D, Chen Y, Zhang X, Zhao Q. Exploring the link between diabetes, herpes zoster, and post-herpetic neuralgia: insights from mendelian randomization. J Pain Res. 2025;18:1479–1489. doi:10.2147/JPR.S501674
24. Maier A, Riedel-Heller SG, Pabst A, Luppa M. Risk factors and protective factors of depression in older people 65+. A systematic review. PLoS One. 2021;16(5):e0251326. doi:10.1371/journal.pone.0251326
25. Zheng Q, Wang D, Lin R, et al. Mendelian randomization analysis suggests no associations of human herpes viruses with amyotrophic lateral sclerosis. Front Neurosci. 2023;17:1299122. doi:10.3389/fnins.2023.1299122
26. Kamat MA, Blackshaw JA, Young R, et al. PhenoScanner V2: an expanded tool for searching human genotype-phenotype associations. Bioinforma Oxf Engl. 2019;35(22):4851–4853. doi:10.1093/bioinformatics/btz469
27. Zheng Q, Wang D, Lin R, et al. Effects of circulating inflammatory proteins on osteoporosis and fractures: evidence from genetic correlation and Mendelian randomization study. Front Endocrinol. 2024;15:1386556. doi:10.3389/fendo.2024.1386556
28. Zheng Q, Lin R, Wang D, Zheng C, Xu W. Effects of circulating inflammatory proteins on spinal degenerative diseases: evidence from genetic correlations and Mendelian randomization study. JOR Spine. 2024;7(2):e1346. doi:10.1002/jsp2.1346
29. Burgess S, Scott RA, Timpson NJ, Davey Smith G, Thompson SG. InterAct Consortium. Using published data in mendelian randomization: a blueprint for efficient identification of causal risk factors. Eur J Epidemiol. 2015;30(7):543–552. doi:10.1007/s10654-015-0011-z
30. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
31. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
32. Hartwig FP, Davey Smith G, Bowden J. Robust inference in summary data mendelian randomization via the zero modal pleiotropy assumption. Int J Epidemiol. 2017;46(6):1985–1998. doi:10.1093/ije/dyx102
33. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
34. Bowden J, Spiller W, Del Greco MF, et al. Improving the visualization, interpretation and analysis of two-sample summary data mendelian randomization via the radial plot and radial regression. Int J Epidemiol. 2018;47(6):2100. doi:10.1093/ije/dyy265
35. Huang M, Liu Y, Chen C, Dai W. Causal effect of lifestyle and metabolic indicator with herpes zoster: a two-sample mendelian randomization study. Front Nutr. 2024;11:1433570. doi:10.3389/fnut.2024.1433570
36. Ong JS, MacGregor S. Implementing MR-PRESSO and GCTA-GSMR for pleiotropy assessment in mendelian randomization studies from a practitioner’s perspective. Genet Epidemiol. 2019;43(6):609–616. doi:10.1002/gepi.22207
37. Irwin MR, Levin MJ, Laudenslager ML, et al. Varicella zoster virus-specific immune responses to a herpes zoster vaccine in elderly recipients with major depression and the impact of antidepressant medications. Clin Infect Dis. 2013;56(8):1085–1093. doi:10.1093/cid/cis1208
38. Pike JL, Irwin MR. Dissociation of inflammatory markers and natural killer cell activity in major depressive disorder. Brain Behav Immun. 2006;20(2):169–174. doi:10.1016/j.bbi.2005.05.004
39. Hughes MM, Connor TJ, Harkin A. Stress-related immune markers in depression: implications for treatment. Int J Neuropsychopharmacol. 2016;19(6):pyw001. doi:10.1093/ijnp/pyw001
40. Foley ÉM, Parkinson JT, Mitchell RE, Turner L, Khandaker GM. Peripheral blood cellular immunophenotype in depression: a systematic review and meta-analysis. Mol Psychiatry. 2023;28(3):1004–1019. doi:10.1038/s41380-022-01919-7
41. Yan B, Liao P, Wang C, Han Z, Cheng F, Lei P. Genetic causal association between varicella-zoster virus infection and psychiatric disorders: a 2-sample Mendelian randomization study. Behav Brain Res. 2024;464:114927. doi:10.1016/j.bbr.2024.114927
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fire Needling Acupuncture for Adult Patients with Acute Herpes Zoster: Protocol of a Systematic Review and Meta-Analysis
Liu L, Chen Q, Yang J, Gang W, Zhao L, Lyu T, Jing X, Zhang CS, Li B
Journal of Pain Research 2022, 15:2161-2170
Published Date: 2 August 2022
Effects of Intradermal Botulinum Toxin Injections on Herpes Zoster Related Neuralgia
Peng F, Xia TB
Infection and Drug Resistance 2023, 16:2159-2165
Published Date: 12 April 2023
Relationship Between the Ovarian Cyst and Depression: A Two-Sample Mendelian Randomization Study
Wen J, Zhou W, Lin Y
International Journal of Women's Health 2023, 15:1727-1732
Published Date: 10 November 2023
Causal Impact of Immune Phenotypes on Herpes Zoster and Postherpetic Neuralgia: Insights from Mendelian Randomization Analysis
Yan Z, Shen D, Qiu X, Ai B, Xiong C
Clinical, Cosmetic and Investigational Dermatology 2025, 18:919-928
Published Date: 15 April 2025
Dissecting the Causal Pathway from Herpes Zoster to Postherpetic Neuralgia: A Multi-Stage Mendelian Randomization Study Implicating VZV-Specific IgE and Cerebrospinal Fluid Metabolites
Zhang J, Chen Y, Li X, Feng C, Li J, Hu Z, Fan G, Liao X
Journal of Pain Research 2026, 19:581884
Published Date: 1 May 2026