Back to Journals » International Journal of Women's Health » Volume 15
Relationship Between the Ovarian Cyst and Depression: A Two-Sample Mendelian Randomization Study
Received 27 April 2023
Accepted for publication 26 September 2023
Published 10 November 2023 Volume 2023:15 Pages 1727—1732
DOI https://doi.org/10.2147/IJWH.S415640
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Jiajia Wen,1 Wamei Zhou,2 Yin Lin3
1Department of Psychiatry III, Hainan an Ning Hospital, Haikou, People’s Republic of China; 2Department of Neurology, Hainan an Ning Hospital, Haikou, People’s Republic of China; 3Department of Psychiatry, Hainan an Ning Hospital, Haikou, People’s Republic of China
Correspondence: Yin Lin, Department of Psychiatry, Hainan an Ning Hospital, No. 10, Nanhai Avenue East, Haikou, Hainan, 570100, People’s Republic of China, Tel +8613876245292, Email [email protected]
Objective: Explore the causal relationship between the ovarian cyst and depression using a two-sample Mendelian randomization approach (MR).
Methods: Based on data pooled from genome-wide association studies, genetic variants of the ovarian cyst and depression were selected as instrumental variables, as well as the Mendelian randomization analysis was conducted using inverse variance weighted (IVW) as the main analysis method and MR-Egger regression analysis, MR-PRESSO and other sensitivity analysis methods as supplements.
Results: The IVW analysis showed a direct causal association between ovarian cysts and depression (OR=1.040; 95% CI: 1.003, 1.078; p=0.031). Meantime, there was a causal effect of genetically predicted depression on ovarian cysts (OR=1.327.; 95% CI: 1.197, 1.470; p< 0.001). Sensitivity analyses such as MR-Egger regression analysis and MR-PRESSO indicated that the IVW results were robust and reliable.
Conclusion: This study suggested since ovarian cysts and female depression are mutually causal, the comorbidity of ovarian cysts and depression in women should be actively attended to and given appropriate prevention and treatment besides the diagnosis and treatment of depression or ovarian cysts.
Keywords: Mendelian randomization, depression, ovarian cyst, genetic variation
Introduction
Ovarian cyst is a common gynecological disease that can occur at any age, with typical symptoms including abdominal masses and pain.1 The prevalence of ovarian cysts in women has been reported to range from 5% to 17%.2,3 Furthermore, it has been discovered that ovarian cysts can cause endocrine system dysfunction in women, which has a negative impact on their physical and mental health.4
Studies have found that endocrine dysfunction, inflammation, stressful environments and genetics are the main causes of ovarian cysts in women.5,6 Moreover, ovarian cysts have been linked to a variety of psychological disorders. For instance, the research revealed that ovarian cysts affect the synthesis and secretion of hormones, thereby triggering depression.7 Additionally, significant pro-inflammatory and endocrine system dysfunction has been discovered in depressed people.8–10 Meanwhile, chronic inflammation could induce ovarian cysts.11 This implies that depression may also be a risk factor for the development of ovarian cysts in women. However, depression has long been considered a comorbidity of ovarian cysts rather than a risk factor.12 This could be due to poorly documented studies on the effect of depression on ovarian cysts, as well as the fact that causal inferences from available observational studies can be challenged by potential confounding bias and reverse causality. Therefore, the bidirectional causal relationship between depression and ovarian cysts remains to be further elucidated.
Mendelian randomization (MR) analysis is a promising tool for causal inference in the context of the rapid development of large-scale Genome-wide association studies (GWAS).13 It explores the causal relationship between exposure and outcome using genetic variants that are closely related to exposure as instrumental variables. Meanwhile, given that genetic variants for exposure and outcome are randomly assigned, they are relatively independent of environmental factors and the relationship exists before disease occurrence, thus reducing problems such as confounding and reverse causality to a minimum.14 Two-sample MR analysis refers to the exposure and outcome from GWAS databases of different or non-overlapping populations, while bidirectional MR analysis attempts to explore reverse causality.15
Therefore, this study proposed a two-sample bivariate MR with publicly available GWAS summary statistics explore the causal relationship between depression and ovarian cysts, intending to provide some implications for the prevention and treatment of depression, ovarian cysts and their co-morbid diseases.
Methods and Materials
Data Sources
The summary single nucleotide polymorphism (SNP)–phenotype association data for depression, ovarian cyst and female infertility were obtained on the MR-Base platform. Specifically, genetic association estimates for ovarian cyst were obtained from FinnGen biobank analysis round 5, including 79,817 European ancestry. Patients with ovarian cysts were diagnosed with International Classification of Diseases-10 (ICD-10), including follicular cysts of ovary, corpus luteum cysts, as well as other and unspecified ovarian cysts. The genetic associations for depression were obtained from Psychiatric Genomics Consortium (PGC) and UK Biobank (excluding 23andme) which includes 170,756 cases and 329,443 control of European participants.16
Genetic Instruments
Genetic instruments for depression or ovarian cyst were selected as single-nucleotide polymorphisms (SNPs) that were associated with the exposure at genome-wide significance (P < 5*10−6) and were independent, ie, pairwise linkage disequilibrium (r2 < 0.001 and distance >10,000 kb). Moreover, the F-statistics of each exposure was calculated to assess instrument strength, of which more than 10 were considered valid instruments.17
Mendelian Randomization Analysis
The TwoSampleMR and Mendelian Randomization R packages were used to perform Mendelian randomization analysis (MR). Firstly, the MR analyses were performed for depression and ovarian cyst separately to estimate the bi-directional causality. Briefly, the inverse-variance weighted method (IVW) was used as the main MR analysis. Additionally, a bilateral p<0.05 was considered indicative of significance.
Sensitivity Analyses
Sensitivity analysis has been pivotal in MR studies to assess the robustness of the findings. Specifically, the IVW and MR Egger approaches were used to evaluate the heterogeneity. While the directional pleiotropy was estimated by MR-PRESSO18 and the intercept obtained from the MR-Egger regression.14 Moreover, the leave-one-out analysis was conducted to assess whether MR estimates were driven or biased by a single SNP. The p<0.05 of indicators for sensitivity analysis was considered acceptable.
Results
Genetic Instruments
In total, 175 and 14 independent SNPs were used as genetic instrumental variables for depression and ovarian cyst, respectively (Table S1). The F-statistic values of individual SNPs ranged from 21 to 75, which the means of 27.86 and 25.67 for depression and ovarian cyst, respectively. All greatly surpass the limited value (F > 10), further suggesting that causal associations are less likely to be affected by weak instrumental variable bias.
Mendelian Randomization
The IVW analysis indicated a direct causal association between ovarian cyst and depression (OR=1.040; 95% CI: 1.003, 1.078; p=0.031). Meantime, there was a causal effect of genetically predicted depression on ovarian cyst (OR=1.327.; 95% CI: 1.197, 1.470; p<0.001). These were similar to the estimates from the weighted median, simple mode and weighted mode analyses (Table 1). Concerning the effect values of individual SNPs, the rs17641524 and rs12967143 loci had the most significant effect on the causal relationship between depression and ovarian cysts, while the most important loci affecting the causal relationship between ovarian cysts and depression were rs1853279 and rs10204333 (Figure 1).
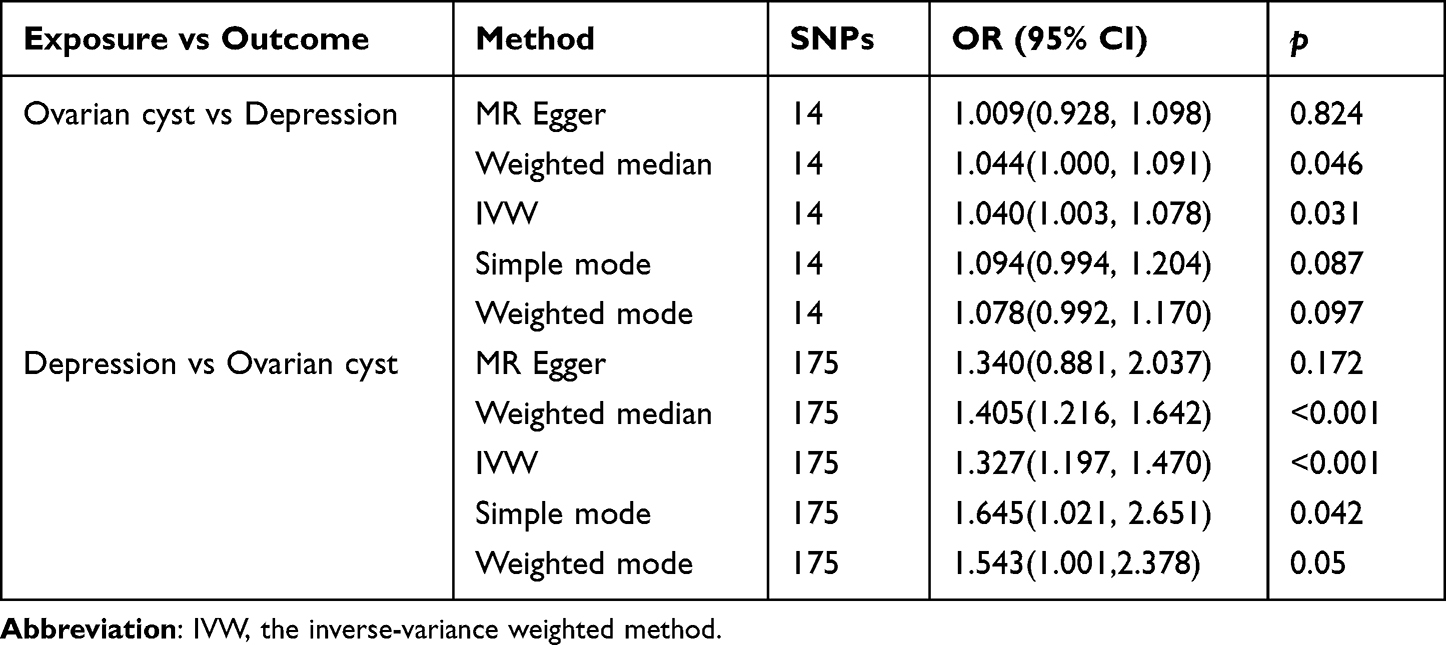 |
Table 1 The MR Results for the Relationship Among Depression and Ovarian Cyst |
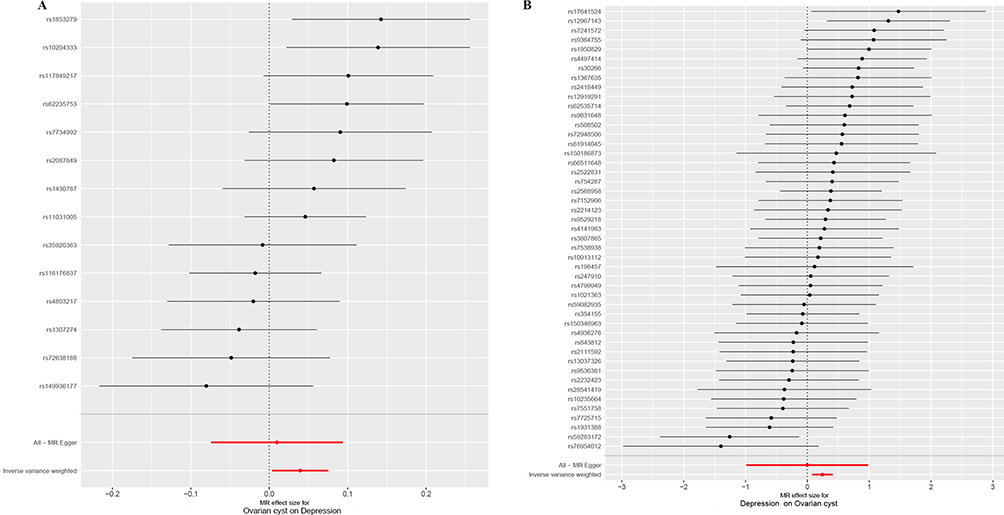 |
Figure 1 Mendelian Randomization (MR) Plots for Relationship between ovarian cyst and depression. (A), Mendelian Randomization summary effects for the risk of ovarian cyst associated with depression. (B), Mendelian Randomization summary effects for the risk of depression associated with ovarian cyst. Summary effects were computed using an inverse-variance weighted (IVW) method from each individual SNP. Dots represent the coefficient and the extremities represent the 95% confidence interval of the odds ratio. |
Sensitivity Analysis
Although the IVW approach is effective for inferring exposure causality for complicated outcomes, a well-known vulnerability to weak instrumental biases. Sensitivity analyses (the IVW, MR Egger, leave-one-out analysis and MR-PRESSO approaches) were performed to overcome these biases. Concerning the relationship among depression and ovarian cyst, the direction of effect of the inverse variance weighted and other methods was mainly consistent (Figure 2). Although the CI of MR-Egger included 0 (Figure S1), indicating a possible violation of the assumption of no measurement error,19 the funnel plot is overall symmetrical indicating less heterogeneity of the included SNP loci (Figure S2), the MR-Egger intercept analysis did not indicate horizontal pleiotropy (Table S2) and the results of leave-one-out analysis (Table S3) and MR-PRESSO (Table S4) could be accepted.
 |
Figure 2 Scatter plots for MR analyses of the bi-directional causality between ovarian cyst and depression. (A), scatter plot of single-nucleotide polymorphism (SNP) potential effects on ovarian cyst vs depression. (B), scatter plot of single-nucleotide polymorphism (SNP) potential effects on depression vs ovarian cyst. |
Discussion
Large-scale GWAS data were used to investigate the genetically predicted relationship between depression and ovarian cyst within an MR framework, providing genetic evidence to support a bidirectional causal relationship between depression and ovarian cyst.
The key finding of this study was that ovarian cysts could cause depression in women, which is consistent with previous research that patients with ovarian cysts frequently have symptoms of depression and anxiety.20,21 As a common gynecological disease, ovarian cyst could impair the ovarian reserve function of an individual, manifested by the disturbance of E2(estradiol)and anti-müllerian hormone (AMH) levels, as well as a reduction in ovarian volume and follicle density.1,22,23 Furthermore, E2 was discovered to have a potential role in regulating 5-hydroxytryptamine (5-HT) receptor mRNA, implying that E2 deficiency could cause depression.24 Furthermore, Gordon et al discovered that ovarian cysts affect the ovarian cortex, causing a continuous decrease in follicular release, which affects hormone synthesis and secretion. Additionally, pregnanolone could effectively promote the role of gamma-amino-butyric acid (GABA) and changes in pregnanolone derived GABAergic neurosteroids may induce dysfunction of the GABAergic system, which in turn causes disorders of the hypothalamic-pituitary-adrenal (HPA) axis and mood disorders.7,25 In general, these may indicate that ovarian cysts also induce depression by affecting the changes of E2 and progesterone in women.
Additionally, this study expanded on prior research that indicated depression was a risk factor for ovarian cysts.26 Depressed patients have been found to have a dysregulation of natural and acquired immunity.27 Meanwhile, numerous studies have shown that early depression can induce late inflammation in individuals.8–10 Inflammation also contributes to the development of ovarian cysts, having a significant negative impact on women’s endocrine systems11 and a direct impact on ovarian function,28 oocyte quality29 and endometrial receptivity.30 Furthermore, individuals with ovarian cysts have a persistent state of pro-inflammation,31 which may also affect normal ovarian function, impairing sex hormone synthesis and release, as well as follicular maturation and subsequent ovulation.11 This imply that depression causes ovarian cysts in women by inducing an inflammatory response.
In conclusion, this study suggested since ovarian cysts and female depression are mutually causal, the comorbidity of ovarian cysts and depression in women should be actively attended to and given appropriate prevention and treatment besides the diagnosis and treatment of depression or ovarian cysts. Furthermore, as the GWAS data included in this study were all of European ancestry, future studies to investigate the relationship between ovarian cysts and depression across different ancestries or ethnicities are warranted.
Ethics Statement
This study is part of a research project on neurobiological mechanisms in patients with psychiatric disorders, which has been reviewed by the Ethics Committee of Hainan An Ning Hospital in 2022 (No. 202205).
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported by Hainan Provincial Natural Science Foundation China (21A200382).
Disclosure
The authors declare that they have no competing interests.
References
1. Legendre G, Catala L, Morinière C, et al. Relationship between ovarian cysts and infertility: what surgery and when? Fertil Steril. 2014;101(3):608–614. doi:10.1016/j.fertnstert.2014.01.021
2. Choi SH, Hong S, Kim M, et al. Robotic-assisted laparoscopic myomectomy: the feasibility in single-site system. Obst Gynecol Sci. 2019;62(1):56–64. doi:10.5468/ogs.2019.62.1.56
3. Zhang Y, Shi L, Li C, Zhang B. Therapeutic effect of transumbilical single-port laparoscopic surgery versus triple-port laparoscopic surgery for ovarian cyst. Am J Trans Res. 2021;13(12):14023–14030.
4. Shu J, Xing L, Zhang L, Fang S, Huang H. Ignored adult primary hypothyroidism presenting chiefly with persistent ovarian cysts: a need for increased awareness. Reprod Biol Endocrinol. 2011;9(1):119. doi:10.1186/1477-7827-9-119
5. Xu J, Shao H, Yang Y, Shi X, Tao M. Improvement and effect of stress responses and ovarian reserve function in patients with ovarian cysts after laparoscopic surgery. J Int Med Res. 2019;47(7):3212–3222. doi:10.1177/0300060519851333
6. Abrahamsson G, Ekerhovd E, Janson PO, et al. Ovarian cyst formation in women of reproductive age receiving mitotane as part of the treatment of adrenocortical carcinoma: clinical and experimental observations. Acta Obst Gynecol Scandi. 2020;99(10):1297–1302. doi:10.1111/aogs.13869
7. Gordon JL, Girdler SS, Meltzer-Brody SE, et al. Ovarian hormone fluctuation, neurosteroids, and HPA axis dysregulation in perimenopausal depression: a novel heuristic model. Am J Psych. 2015;172(3):227–236. doi:10.1176/appi.ajp.2014.14070918
8. Copeland WE, Shanahan L, Worthman C, Angold A, Costello EJ. Cumulative depression episodes predict later C-reactive protein levels: a prospective analysis. Biol Psych. 2012;71(1):15–21. doi:10.1016/j.biopsych.2011.09.023
9. Mac Giollabhui N, Swistun D, Murray S, et al. Executive dysfunction in depression in adolescence: the role of inflammation and higher body mass. psychol Med. 2020;50(4):683–691. doi:10.1017/S0033291719000564
10. Miller GE, Cole SW. Clustering of depression and inflammation in adolescents previously exposed to childhood adversity. Biol Psych. 2012;72(1):34–40. doi:10.1016/j.biopsych.2012.02.034
11. Velez LM, Seldin M, Motta AB. Inflammation and reproductive function in women with polycystic ovary syndrome†. Biol Reprod. 2021;104(6):1205–1217. doi:10.1093/biolre/ioab050
12. van Hoesel MH, Chen YL, Zheng A, Wan Q, Mourad SM. Selective oestrogen receptor modulators (SERMs) for endometriosis. Coch Data System Rev. 2021;5(5):CD011169. doi:10.1002/14651858.CD011169.pub2
13. Emdin CA, Khera AV, Kathiresan S. Mendelian randomization. JAMA. 2017;318(19):1925–1926. doi:10.1001/jama.2017.17219
14. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
15. Bowden J, Del Greco MF, Minelli C, et al. Improving the accuracy of two-sample summary-data Mendelian randomization: moving beyond the NOME assumption. Int J Epidemiol. 2019;48(3):728–742. doi:10.1093/ije/dyy258
16. Howard DM, Adams MJ, Clarke T-K, et al. Genome-wide meta-analysis of depression identifies 102 Independent variants and highlights the importance of the prefrontal brain regions. Nat Neurosci. 2019;22(3):343–352. doi:10.1038/s41593-018-0326-7
17. Sanderson E. Multivariable Mendelian randomization and mediation. Cold Spr Harbor Pers Med. 2021;11(2):a038984. doi:10.1101/cshperspect.a038984
18. Verbanck M, Chen C-Y, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Gene. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
19. Zhou W, Liu G, Hung RJ, et al. Causal relationships between body mass index, smoking and lung cancer: univariable and multivariable Mendelian randomization. Int J Cancer. 2021;148(5):1077–1086. doi:10.1002/ijc.33292
20. Nowak-Psiorz I, Ciećwież SM, Brodowska A, Starczewski A. Treatment of ovarian endometrial cysts in the context of recurrence and fertility. Adv Clin Exper Med. 2019;28(3):407–413. doi:10.17219/acem/90767
21. Sheela S, Sumathi M. An evaluation of effectiveness of a texture feature based computerized diagnostic model in classifying the ovarian cyst as benign and Malignant from static 2D B-mode ultrasound images. Curr Med Imag. 2022. doi:10.2174/1573405618666220516120556
22. Pfister A, Crawford NM, Steiner AZ. Association between diminished ovarian reserve and luteal phase deficiency. Fertil Steril. 2019;112(2):378–386. doi:10.1016/j.fertnstert.2019.03.032
23. Tal R, Seifer DB. Ovarian reserve testing: a user’s guide. Am J Obstet Gynecol. 2017;217(2):129–140. doi:10.1016/j.ajog.2017.02.027
24. Osterlund MK, Hurd YL. Acute 17β-estradiol treatment down-regulates serotonin 5HT1A receptor mRNA expression in the limbic system of female rats. Molecul Brain Res. 1998;55(1):169–172. doi:10.1016/s0169-328x(98)00018-7
25. Odore R, Re G, Badino P, et al. Modifications Of Receptor Concentrations For Adrenaline, Steroid Hormones, Prostaglandin F2αand Gonadotropins In Hypophysis And Ovary Of Dairy Cows With Ovarian Cysts. Pharmacol Res. 1999;39(4):297–304. doi:10.1006/phrs.1998.0442
26. Daly RC, Danaceau MA, Rubinow DR, Schmidt PJ. Concordant Restoration of Ovarian Function and Mood in Perimenopausal Depression. Am J Psych. 2003;160(10):1842–1846. doi:10.1176/appi.ajp.160.10.1842
27. Beurel E, Toups M, Nemeroff CB. The bidirectional relationship of depression and inflammation: double trouble. Neuron. 2020;107(2):234–256. doi:10.1016/j.neuron.2020.06.002
28. Camaioni A, Klinger FG, Campagnolo L, Salustri A. The Influence of Pentraxin 3 on the Ovarian Function and Its Impact on Fertility. Front Immunol. 2018;9:2808. doi:10.3389/fimmu.2018.02808
29. Ermisch AF, Bidne KL, Kurz SG, Bochantin KA, Wood JR. Ovarian inflammation mediated by toll-like receptor 4 increased transcripts of maternal effect genes and decreased embryo development†. Biol Reprod. 2023;108(3):423–436. doi:10.1093/biolre/ioac212
30. Jabbour HN, Sales KJ, Catalano RD, Norman JE. Inflammatory pathways in female reproductive health and disease. Reproduction. 2009;138(6):903–919. doi:10.1530/REP-09-0247
31. Ikeda M, Negishi Y, Akira S, Morita R, Takeshita T. Inflammation related to high-mobility group box-1 in endometrial ovarian cyst. J Reprod Immunol. 2021;145:103292. doi:10.1016/j.jri.2021.103292
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessing Causality Between Androgenetic Alopecia with Depression: A Bidirectional Mendelian Randomization Study
Li H, Cai H, Li P, Zeng Y, Zhang Y
Clinical, Cosmetic and Investigational Dermatology 2025, 18:445-451
Published Date: 22 February 2025
The Causal Association Analysis between Depression and Cerebrospinal Fluid: From the Perspective of Mendelian Randomization
Zhang Y, Wu P, Liu Z
Psychology Research and Behavior Management 2025, 18:1085-1097
Published Date: 5 May 2025
Advances in Mendelian Randomization Studies of Obesity Over the Past Decade: Uncovering Key Genetic Mechanisms
Lu X, Ji L, Chen D, Lian X, Yuan M
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2399-2415
Published Date: 17 July 2025
No Evidence for a Causal Association Between Depression and Herpes Zoster or Post-Herpetic Neuralgia: A Mendelian Randomization Study
Zhang X, Chen Y, Lin J, Guo W, Zhou H, Yang X, Zhao Q
Journal of Pain Research 2025, 18:6579-6589
Published Date: 6 December 2025
Circadian Biology and Gynecological Diseases: Genetic Mechanisms and Potential Therapeutic Targets Underlying the Causal Link Between Insomnia and Ovarian Cysts
Geng H, Wu H, Liu M, Zhu J, Song L
International Journal of Women's Health 2026, 18:562401
Published Date: 11 March 2026