Back to Journals » Journal of Asthma and Allergy » Volume 19
Multidisciplinary Recommendations for the Use of Chest CT and Bronchial Biopsy in Severe Asthma: An Expert Consensus Based on Real-World Experience
Authors Garcia-Rivero JL ![]() , Peña E
, Peña E ![]() , González-Piñeiro A, Mosteiro Añón M, Cosio BG
, González-Piñeiro A, Mosteiro Añón M, Cosio BG ![]()
Received 5 March 2026
Accepted for publication 4 May 2026
Published 23 May 2026 Volume 2026:19 604260
DOI https://doi.org/10.2147/JAA.S604260
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Juan Luis Garcia-Rivero,1 Elena Peña,2 Ana González-Piñeiro,3 Mar Mosteiro Añón,4 Borja G Cosio,5 On behalf of the AGHORA Group
1Respiratory Department, Marqués de Valdecilla University Hospital, IDIVAL, Santander, Spain; 2Radiology Department, Marqués de Valdecilla University Hospital, Santander, Spain; 3Pathology Department, Hospital Álvaro Cunqueiro, Vigo, Spain; 4Respiratory Medicine Department, Hospital Álvaro Cunqueiro, Vigo, Spain; 5Respiratory Medicine Department, Hospital Son Espases-IdISBa-CIBERES, Palma de Mallorca, Spain
Correspondence: Juan Luis Garcia-Rivero, Email [email protected]
Background: Chest computed tomography (CT) and bronchial biopsy can refine severe asthma phenotyping beyond systemic biomarkers, yet real-world implementation re mains heterogeneous and reporting is often non-standardized. Multidisciplinary integration is therefore needed to maximize clinical utility and comparability across centres.
Methods: This manuscript reports a multidisciplinary expert consensus developed during the AGHORA workshop held in Santander, Spain (21– 22 November 2025). Experts in severe asthma care, bronchoscopy, thoracic imaging, and pulmonary pathology from 13 predominantly tertiary hospitals participated. Recommendations were generated through structured plenary and discipline-focused sessions followed by cross-disciplinary discussion. Draft statements were refined in real time and submitted to show-of-hands voting; agreement was categorized qualitatively as high, moderate, or low.
Results: The panel identified key decision points where CT is most likely to change management, particularly prior to biologic initiation and in cases of inadequate response to biologic therapy. When tracheobronchomalacia/central airway collapse was clinically suspected, expiratory imaging was considered essential. A minimum dataset for CT acquisition and structured reporting was proposed, emphasizing systematic assessment (and, where feasible, quantification) of mucus plugging, bronchial wall thickening/bronchiectasis distribution and extent, and air trapping/small-airway disease patterns, complemented by an actionable impression for multidisciplinary decision-making. For bronchial biopsy, experts agreed on scenarios where tissue assessment adds value (eg, suspected T2 low asthma, discordant biomarkers, and biologic non-response) and proposed minimum technical and reporting standards. Standardized histopathology reporting was anchored to the validated 11-item pathological score (PS score), enabling structured item-level reporting and benchmarking across inflammatory and remodelling domains.
Conclusion: This expert statement provides pragmatic, multidisciplinary recommendations and minimum reporting standards for CT and bronchial biopsy in severe asthma. Implementation may reduce inter-centre variability, improve personalized clinical decision-making, and facilitate multicentre research and prospective validation.
Keywords: severe asthma, computed tomography, bronchial biopsy, histopathology, airway remodelling, mucus plugging, multidisciplinary team, precision medicine
Introduction
Severe asthma remains a heterogeneous condition with a disproportionate burden in terms of symptoms, exacerbations, healthcare utilization, and impaired quality of life.1–3 Over the last decade, the advent of targeted biologic therapies has reshaped the management of severe asthma, shifting the clinical paradigm toward precision medicine.4 In this context, selecting the most appropriate therapy increasingly depends on an accurate characterization of the individual patient, integrating clinical features with inflammatory and structural traits.
Although systemic biomarkers such as peripheral blood eosinophil counts, fractional exhaled nitric oxide (FeNO), and IgE levels are widely used and clinically useful, they only provide an indirect approximation of airway pathology. Importantly, severe asthma is not solely an “inflammatory label” but a clinically, biologically, and structurally heterogeneous airway disease in which inflammatory activity and airway remodelling may coexist, vary spatially, evolve over time, and jointly influence airway behaviour during bronchoconstriction.5 As a result, reliance on systemic biomarkers alone can be insufficient to fully capture clinically relevant mechanisms that may influence treatment response or explain persistent disease activity despite optimal therapy.6 However, complete and sustained response to currently available biologic therapies is not achieved in a substantial proportion of patients, most likely reflecting the limitations of current phenotyping approaches.7
Against this background, chest computed tomography (CT), particularly high-resolution CT, has evolved from a tool primarily used to exclude alternative diagnoses to an increasingly relevant instrument for phenotyping severe asthma.8,9 CT can provide actionable information on airway and parenchymal abnormalities—such as bronchial wall thickening, bronchiectasis, mucus plugging, air trapping and small-airway disease patterns—that may define treatable traits, refine diagnostic confidence, and support complex therapeutic decisions.10–14 Importantly, emerging evidence suggests that effective biologic therapies may modify some of these airway abnormalities over time, including mucus plugging and airway wall thickening, highlighting the potential role of CT not only for baseline phenotyping but also for longitudinal assessment of structural response to targeted treatment.15,16 However, real-world practice still shows marked variability across hospitals regarding when CT is requested, how it is acquired (eg, inspiratory versus combined inspiratory–expiratory protocols), and how findings are reported.17 This heterogeneity limits comparability across centres, reduces the clinical utility of radiology reports in multidisciplinary decision-making, and hampers the development of shared research frameworks.
Current evidence supports the role of CT in identifying structural and functional airway traits relevant to severe asthma phenotyping, including mucus plugging, airway wall thickening, bronchiectasis, air trapping, and distal airway abnormalities.11,18–20 Likewise, bronchial biopsy may provide tissue-level information on eosinophilic and non-eosinophilic inflammation, epithelial injury, airway remodelling, and, in selected cases, contributory processes such as infection.21 At the same time, both approaches have relevant limitations: CT involves radiation exposure and variability in acquisition and interpretation, whereas bronchoscopy with biopsy is invasive, resource-dependent, and subject to sampling constraints.21,22
Bronchial biopsy is gaining renewed interest as an approach to directly assess airway inflammation and remodelling in severe asthma. Histopathological evaluation can add complementary information that is not readily captured by systemic biomarkers, potentially clarifying inflammatory patterns (eosinophilic, neutrophilic, mixed, or paucigranulocytic) and documenting remodelling features relevant to disease chronicity and prognosis.21,23,24 Bronchoscopy with endobronchial biopsy has shown an acceptable safety profile in severe asthma when performed in experienced settings, although it remains an invasive procedure and should therefore be reserved for appropriately selected patients.22 Moreover, it may help predict response to biologic therapy, particularly to anti-IL-5/IL-5R agents and especially in oral corticosteroid-dependent patients.25 Nevertheless, bronchial biopsy remains unevenly implemented in severe asthma care, and substantial variability persists regarding indications, sampling strategy, specimen handling, and the degree of standardization in pathology reporting.21 Without a shared minimum dataset and structured reporting, the clinical value of biopsy findings may be inconsistent and difficult to integrate into treatment pathways. Recent work has demonstrated that a standardized histopathological assessment of endobronchial biopsies in severe uncontrolled asthma is feasible and reproducible across expert pathologists, with good interobserver agreement for key inflammatory and remodelling features. Moreover, tissue eosinophilia may be present despite low blood eosinophils, particularly in patients receiving oral corticosteroids, supporting the need for tissue-based phenotyping and harmonized reporting.26
A consistent theme emerging from clinical experience is that the highest added value of CT and bronchial biopsy is achieved when they are used within a coordinated, multidisciplinary workflow.27 Effective integration requires (i) clear clinical questions from the referring clinician, (ii) radiology protocols and reports tailored to severe asthma decision points, (iii) pathology reports structured around clinically meaningful inflammatory and remodelling domains, and (iv) a forum for multidisciplinary discussion analogous to other established respiratory multidisciplinary boards. Such an approach may also enable image-informed sampling strategies and a more coherent interpretation of potentially heterogeneous and patchy airway disease.
To address these unmet needs, the AGHORA multidisciplinary meeting, a workshop specifically focused on severe asthma and airway assessment through imaging and histopathology, convened experts in severe asthma management, bronchoscopy, thoracic imaging, and pulmonary pathology from tertiary-care settings, with the aim of generating pragmatic, practice-oriented recommendations grounded in real-world experience. The name AGHORA combines the Spanish expression “es la hora del asma grave” (“it is time for severe asthma”) with the Greek concept of the agora as a place for expert gathering and debate. The purpose of the present expert statement is to propose recommendations on: (1) indications and acquisition protocols for chest CT in severe asthma; (2) minimum elements for standardized radiology reporting; (3) indications and technical considerations for bronchial biopsy; (4) minimum elements for standardized pathology reporting; and (5) principles for multidisciplinary integration to support treatment decisions. We also highlight current evidence gaps and priority areas for future research and prospective validation, acknowledging that these recommendations are intended to complement—rather than replace—existing guideline-based care.
This consensus was developed for the assessment of adult patients with severe asthma; paediatric severe asthma was outside the scope of the meeting.
Methods
Design and Scope
This manuscript reports a multidisciplinary expert consensus developed during the AGHORA meeting, held in Santander (Spain) on 21–22 November 2025. The objective of the meeting was to generate practice-oriented recommendations on the use of chest computed tomography (CT) and bronchial biopsy in the work-up of adult patients with severe asthma, with a particular focus on standardizing radiology and pathology reporting and improving multidisciplinary decision-making. Paediatric severe asthma was outside the scope of the meeting, and no paediatric specialists participated in the panel.
The scope of the consensus was intentionally pragmatic and centred on real-world implementation in tertiary-care settings. The recommendations were designed to complement (rather than replace) existing guideline-based care, addressing areas where evidence is evolving and where inter-centre variability remains high.
Expert Panel and Representation
Participants were purposively selected and invited by the convening group based on recognized expertise in at least one of the following domains: severe asthma management, interventional bronchoscopy, thoracic imaging, and pulmonary pathology. The final panel represented 13 hospitals across Spain, most of them tertiary referral centres, and included pulmonologists with expertise in severe asthma (including bronchoscopists), thoracic radiologists, and pulmonary pathologists. This approach ensured balanced input across all disciplines directly involved in airway assessment and interpretation of imaging and tissue findings.
Participation required representation from all involved disciplines at each centre. Accordingly, each participating hospital attended with a multidisciplinary team comprising pulmonology/bronchoscopy, thoracic radiology, and pulmonary pathology. This requirement ensured that the multidisciplinary perspective reflected real-world hospital-based teams accustomed to shared clinical workflows and joint decision-making in severe asthma care.
No paediatricians or non-thoracic imaging/pathology specialists were included, as the meeting was intentionally designed around adult severe asthma and the current real-world implementation of chest CT and bronchial biopsy.
Consensus Process
The consensus was developed through an in-person, structured, discussion-based process. The meeting format combined plenary sessions to establish shared conceptual foundations, followed by discipline-focused sessions and cross-disciplinary discussion aimed at producing actionable recommendations. Key topics included: (1) clinical indications for chest CT in severe asthma; (2) CT acquisition protocols (including inspiratory and expiratory imaging); (3) clinically meaningful radiologic findings and structured reporting; (4) indications and sampling strategy for bronchial biopsy; (5) minimum histopathologic items and structured pathology reporting; and (6) principles for integrating imaging and pathology into multidisciplinary treatment decisions.
For each recommendation, a draft statement was introduced and discussed openly. Statements were refined in real time when needed to improve clarity, feasibility, and relevance across centres. After discussion, recommendations were submitted to a show-of-hands vote to assess the degree of agreement. This process was designed to achieve convergence through face-to-face discussion rather than through iterative anonymous rounds.
To inform the histopathology recommendations, the panel reviewed available evidence and existing standardized frameworks for reporting endobronchial biopsies in severe asthma. Emphasis was placed on the validated “pathological score” (PS score) proposed for severe uncontrolled asthma, which operationalizes a systematic assessment of key inflammatory and remodelling features across 11 histopathologic items and demonstrated good-to-excellent interobserver reliability for several core components.26 The PS score framework was used as a reference to define a minimum dataset for standardized reporting and to facilitate harmonization across participating centres.
The questions prioritized during the meeting were selected because they represented recurrent areas of variability across participating centres and were considered the most likely to influence clinical decision-making in routine severe asthma practice.
Voting and Level of Agreement Definitions
Because voting was conducted in person and was not intended to provide exact quantitative agreement thresholds, we categorized agreement qualitatively into three levels based on the observed degree of convergence during voting:
- High agreement: clear convergence of most experts; interpreted as a strong consensus supporting a solid recommendation.
- Moderate agreement: partial convergence with identifiable dissenting views; interpreted as a recommendation requiring contextualization or centre-level adaptation.
- Low agreement: divergent opinions without clear convergence; interpreted as an area of controversy where decisions should rely on individualized clinical judgment and local expertise/resources.
This approach explicitly acknowledges that the process did not follow a formal Delphi methodology and did not include multiple iterative voting rounds or predefined percentage cut-offs.
Manuscript Development
A writing group drafted the manuscript based on the meeting content, including structured notes and the recorded discussions. The text was organized into thematic sections (CT, bronchial biopsy/pathology, and multidisciplinary integration), with recommendations presented alongside the corresponding level of agreement and practical considerations. The document was subsequently revised to improve consistency, reduce redundancy, and ensure an internationally readable scientific style.
The scope of the consensus, the key clinical questions addressed, the corresponding consensus outputs, and the qualitative level of agreement are summarized in Table 1, which provides an overview of the conceptual framework and deliverables of the AGHORA meeting. The main outputs of the consensus are presented as practice-oriented recommendations. Chest CT-related indications, acquisition protocols, and standardized reporting are summarized i Tables 2–4, while bronchial biopsy-related indications, acquisition standards, and standardized pathology reporting are detailed in Tables 5–7. Evidence gaps and future research priorities are summarized in Table 8.
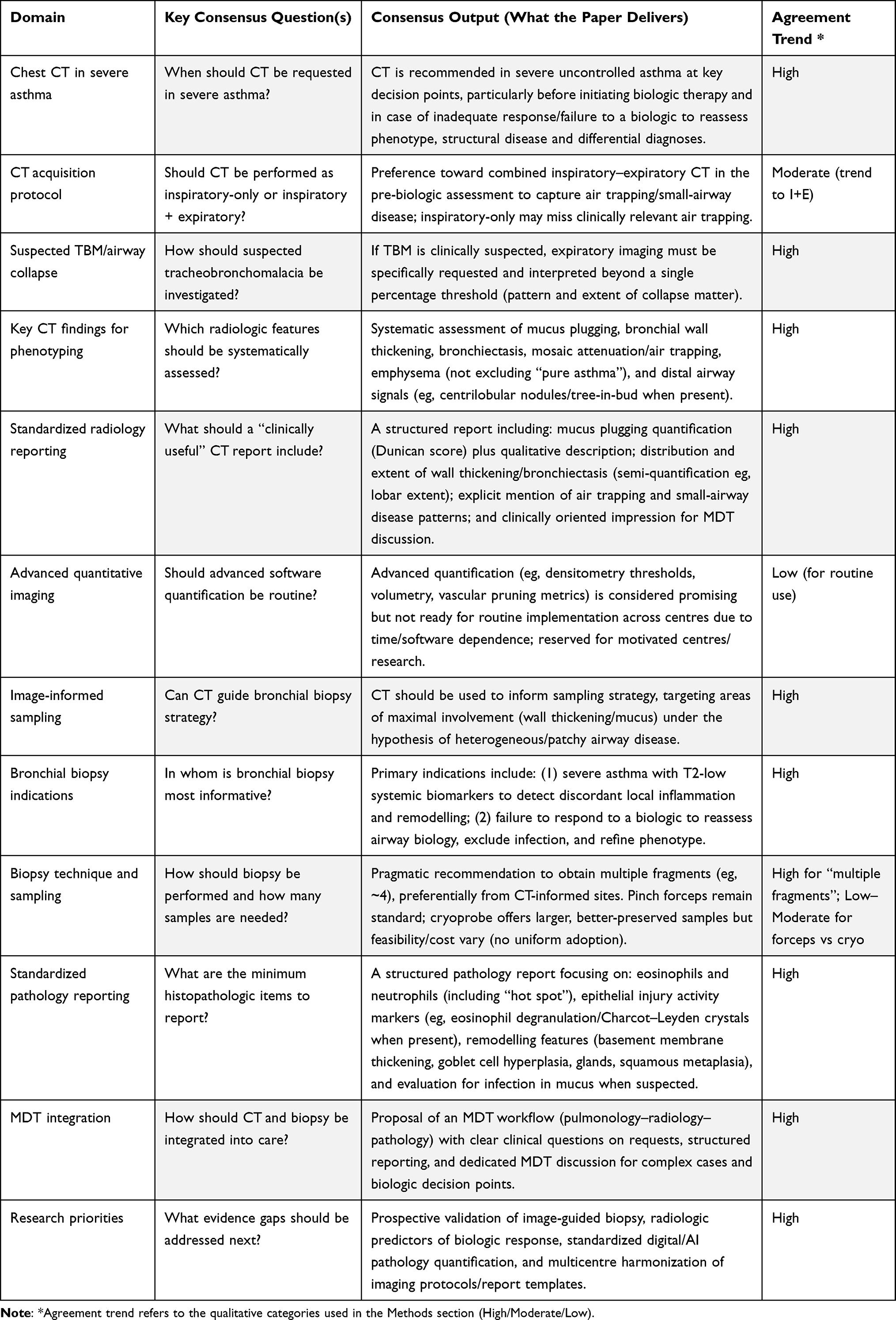 |
Table 1 Consensus Scope, Key Questions, and Outputs |
 |
Table 2 Indications for Chest CT in Severe Asthma (AGHORA Expert Consensus) |
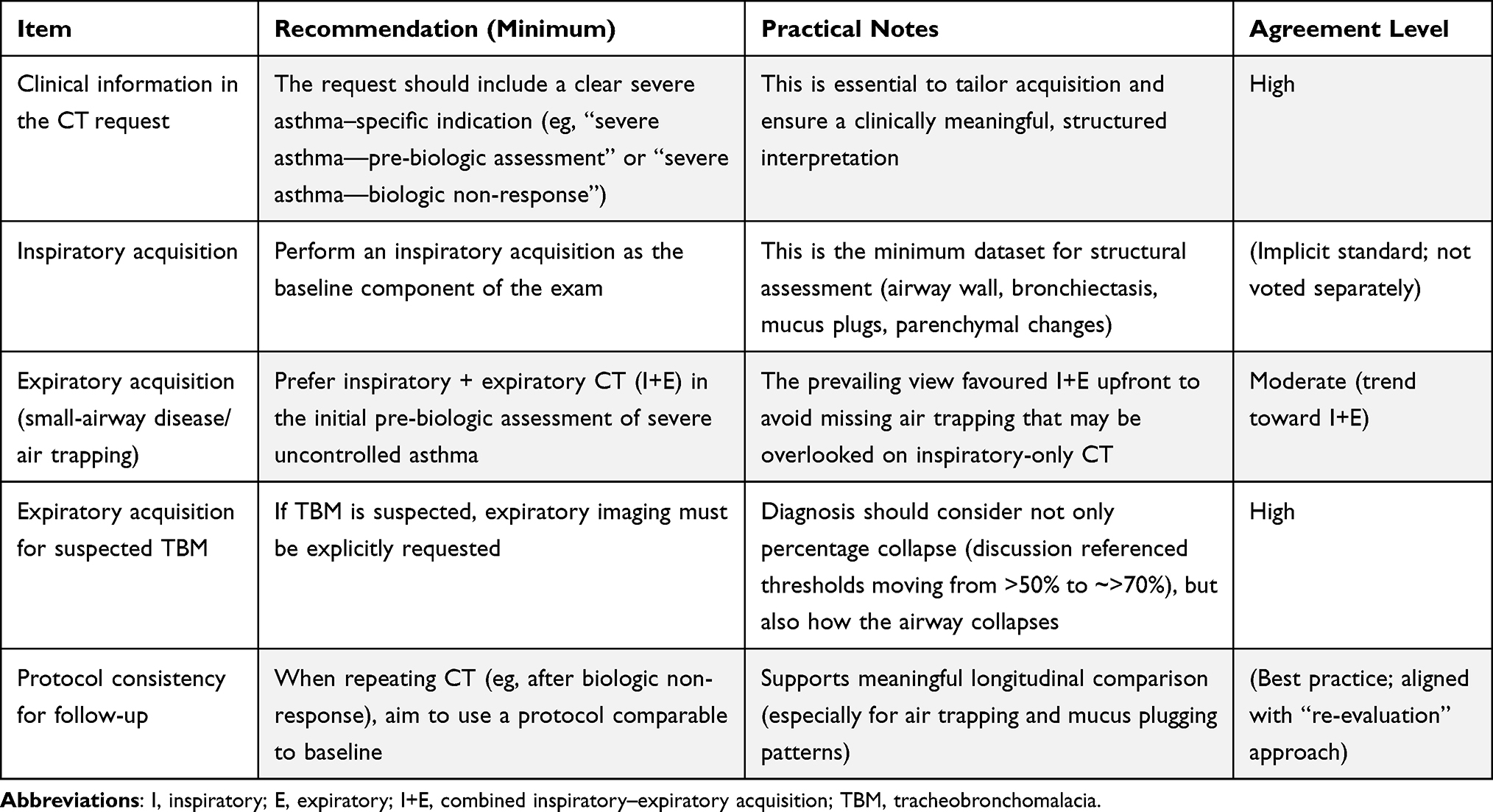 |
Table 3 Recommended CT Acquisition Protocol (Minimum) and Request Specifications |
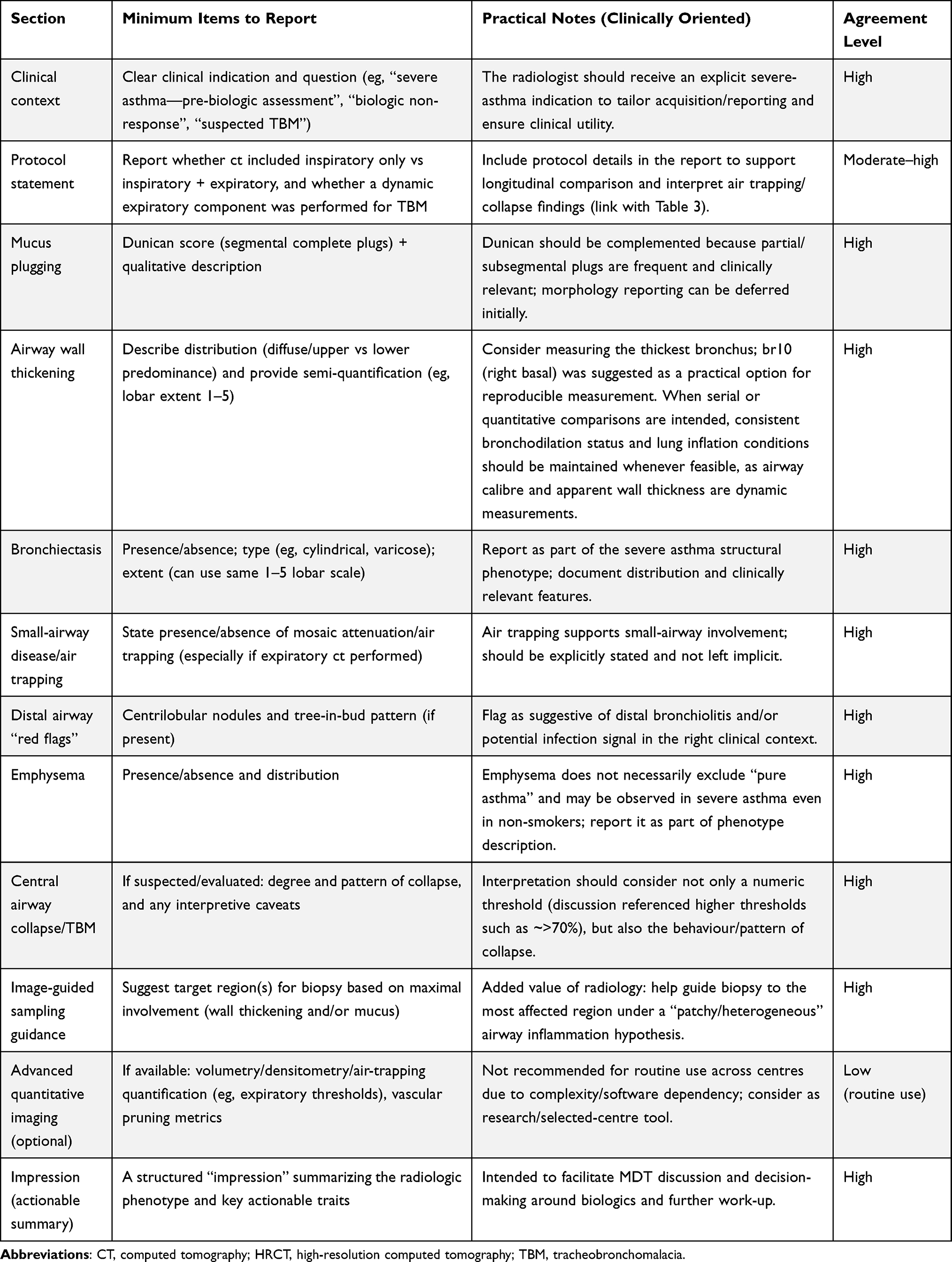 |
Table 4 Minimum Dataset for Standardized Chest CT Reporting in Severe Asthma (AGHORA Expert Consensus) |
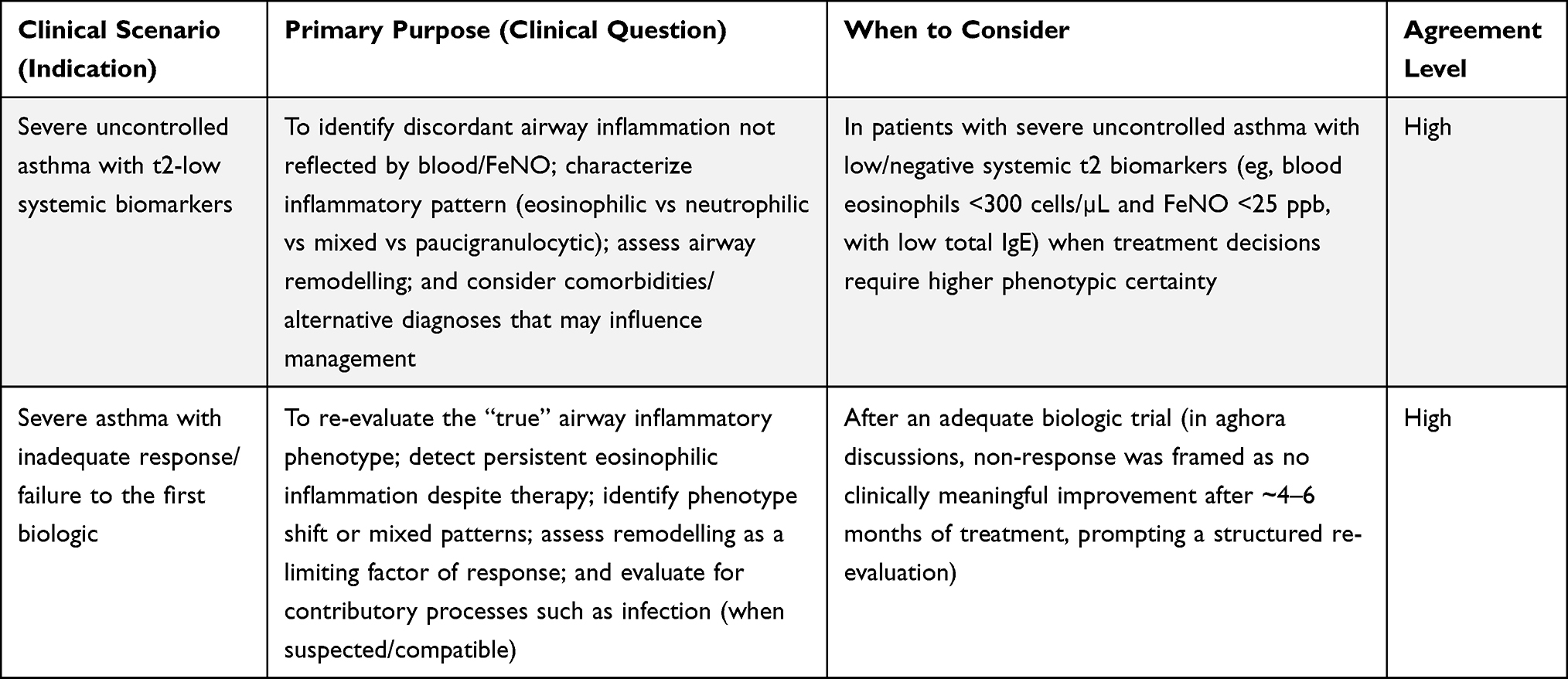 |
Table 5 Indications for Bronchial Biopsy in Severe Asthma (AGHORA Expert Consensus) |
 |
Table 6 Recommended Bronchial Biopsy Acquisition and Specimen Handling (Minimum) (AGHORA Expert Consensus) |
 |
Table 7 Minimum Dataset for Standardized Pathology Reporting of Bronchial Biopsy in Severe Asthma (AGHORA Expert Consensus) |
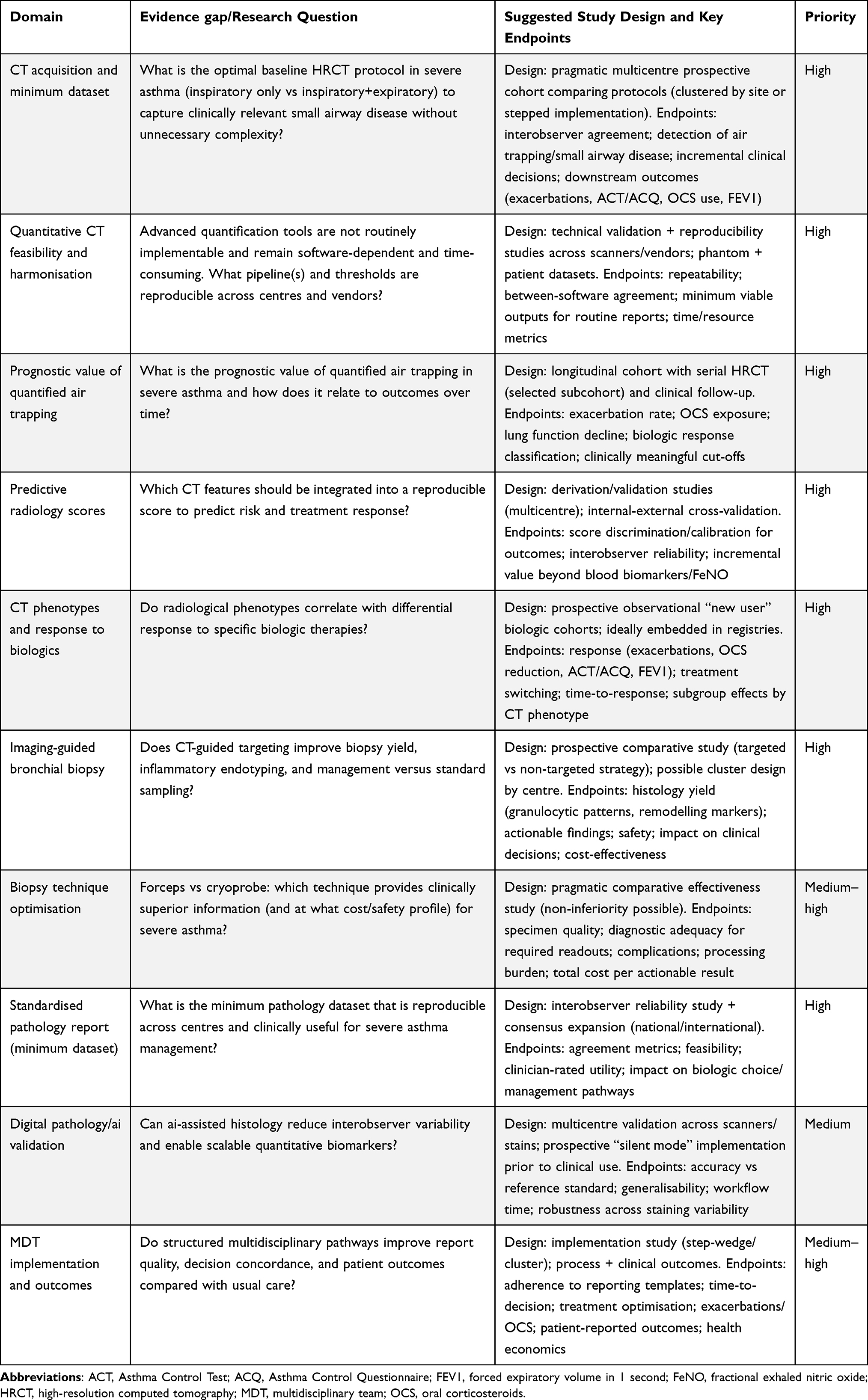 |
Table 8 Evidence Gaps and Future Research Priorities Proposed by the AGHORA Panel |
The manuscript was drafted and revised by the listed authors; no professional or external medical writer was involved.
Ethics and Governance
No individual-level patient data were collected or analysed for this expert consensus. Therefore, institutional review board approval and informed consent were not required. Any funding, logistical support, and potential conflicts of interest should be reported transparently in the Funding and Disclosure sections, in accordance with journal requirements.
Meeting governance and participant consent: All AGHORA meeting participants were informed in advance that the outcomes of the meeting would be synthesized into a consensus manuscript for publication, and they agreed to this. No individual-level patient data were collected or discussed.
Consensus Outputs and Practice-Oriented Recommendations
Chest CT in Severe Asthma: Indications, Acquisition Protocol, and Standardized Reporting
Chest CT has become increasingly relevant in severe asthma as a phenotyping and decision-support tool, particularly in the era of biologic therapies. During the AGHORA consensus, experts agreed that CT provides actionable structural and functional information that may complement clinical assessment and systemic biomarkers, and that its clinical value is maximized when requested at predefined decision points and interpreted using a structured reporting approach.
Indications for CT were centred on scenarios where imaging is most likely to change management. As summarized in Table 2, the panel recommended CT assessment in severe uncontrolled asthma prior to biologic initiation, and in patients with inadequate response to a biologic, as part of a structured re-evaluation aimed at refining the working phenotype and identifying comorbidities or alternative explanations for persistent symptoms. Here, baseline airway/parenchymal traits refer to structural and parenchymal features relevant to phenotyping and future comparison, including mucus plugging burden, airway wall thickening, bronchiectasis, air trapping/mosaic attenuation, emphysema, and other distal airway abnormalities. In addition, when tracheobronchomalacia (TBM) or central airway collapse is clinically suspected, the panel considered CT (with an expiratory component) essential to support diagnostic clarification (Table 2).
For clarity, the key CT-dependent decisions considered by the panel included whether to proceed with biologic initiation with a defined structural baseline, whether persistent symptoms or biologic non-response might be explained by structural airway abnormalities or competing diagnoses, whether expiratory imaging was required for suspected central airway collapse, and whether CT findings could help guide bronchial biopsy targeting.
Regarding CT acquisition, the consensus emphasized that protocol selection should be aligned with the clinical question. The minimum recommended acquisition elements are outlined in Table 3. While some variability in practice persists, the prevailing view supported combined inspiratory–expiratory acquisition in the pre-biologic setting to improve detection of air trapping and small-airway disease, acknowledging a moderate level of agreement on this specific point. By contrast, in suspected TBM, the panel agreed that expiratory imaging should be explicitly requested to enable appropriate assessment of airway collapsibility (Table 3).
To reduce inter-centre variability and improve multidisciplinary interpretability, the group proposed a minimum dataset for standardized radiology reporting (Table 4). This dataset emphasizes clinically meaningful traits, including systematic assessment of mucus plugging (quantification plus qualitative description), airway wall thickening and bronchiectasis distribution/extent, explicit evaluation of air trapping/small-airway disease patterns, and an actionable “Impression” summarizing the radiologic phenotype. Where appropriate, the report should also provide image-informed guidance for sampling, suggesting target regions for biopsy based on areas of maximal involvement (Table 4).
Bronchial Biopsy in Severe Asthma: Indications, Sampling Strategy, and Standardized Pathology Reporting
Bronchial biopsy may provide complementary information to systemic biomarkers by directly characterizing airway inflammation and remodelling, potentially clarifying severe asthma endotypes in complex clinical scenarios. Likewise, biopsy-dependent decisions included whether airway eosinophilia was present despite low systemic T2 biomarkers, whether mixed inflammation or infection could contribute to biologic non-response, and whether tissue findings should support treatment reassessment within multidisciplinary discussion.25
The AGHORA consensus highlighted the practical value of bronchial biopsy when systemic markers may be discordant with airway biology, or when treatment response does not match the expected inflammatory profile.
Indications for bronchial biopsy are summarized in Table 5. The panel supported biopsy in patients with severe uncontrolled asthma and T2-low systemic biomarker profiles, where tissue assessment may reveal discordant eosinophilic inflammation, alternative inflammatory patterns, or clinically relevant remodelling features. In addition, bronchial biopsy was recommended in biologic non-responders after an adequate therapeutic trial, as part of a structured re-evaluation to better understand the drivers of persistent disease activity and to inform subsequent treatment strategy (Table 5).
The consensus also addressed sampling strategy and minimum acquisition standards to optimize feasibility and reproducibility across centres. These recommendations were intended to address not only the indication for biopsy, but also the pragmatic elements that determine clinical usefulness in routine practice, including sampling strategy, number of fragments, specimen handling, and the minimum clinical information that should accompany the sample. As shown in Table 6, the panel recommended obtaining multiple fragments (pragmatic minimum) and, when CT information is available, considering image-informed targeting toward regions of maximal involvement. Conventional forceps biopsy was considered a reasonable and widely available standard, while cryoprobe techniques were recognized as potentially advantageous in terms of tissue quality but not uniformly required due to feasibility and resource considerations (Table 6). For routine clinical workflows, a pragmatic approach to specimen handling was favoured to maximize adoption.
Finally, the panel emphasized that the clinical usefulness of bronchial biopsy depends heavily on the quality and standardization of the pathology report. A minimum dataset for structured pathology reporting is detailed in Table 7, including inflammatory domains (eosinophils and neutrophils with hotspot reporting), key remodelling features, assessment for infection when clinically indicated, and an integrated interpretive summary (inflammatory phenotype and remodelling burden) designed to support multidisciplinary decision-making.
A major barrier to translating bronchial biopsy findings into routine severe asthma care is the lack of standardized, reproducible reporting. The panel recommends adopting a structured histopathology template mapped to the validated pathological score (PS score) for endobronchial biopsies in severe uncontrolled asthma.26 The PS score provides a pragmatic framework covering both inflammatory and airway remodelling domains through 11 items, including submucosal eosinophils (semi-quantitative grade), eosinophil count/field, epithelial denudation, goblet cell hyperplasia, squamous metaplasia, epithelial dysplasia, basement membrane thickening, prominent airway smooth muscle, prominent mucosal glands, submucosal neutrophils, and submucosal plasma cells.
In the original validation, interobserver agreement was good-to-excellent for several key items (notably tissue eosinophilia-related components and selected remodelling features), supporting feasibility for multicentre implementation. The panel therefore proposes that participating centres report, at minimum, the PS-score-aligned items (Table 7), either using the original ordinal definitions or an equivalent standardized mapping, to enable comparability across hospitals and future pooled analyses.
Where local constraints preclude complete scoring (eg, limited tissue size, variable orientation, or resource limitations), the panel recommends prioritizing the PS score items with the highest reproducibility and clinical interpretability (tissue eosinophilia metrics and core epithelial/remodelling descriptors) while documenting reasons for missing elements.
Multidisciplinary Integration and Decision-Making
A central theme of the AGHORA consensus was that the highest clinical value of chest CT and bronchial biopsy is achieved when both tools are implemented within a coordinated multidisciplinary workflow. To enable consistent interpretation and reduce practice variability, the panel proposed aligning (i) the clinical question in imaging and pathology requests, (ii) standardized reporting elements for radiology and pathology (Tables 4–7), and (iii) structured multidisciplinary discussion for complex cases and key decision points (eg, biologic initiation and biologic non-response).
Within this framework, chest CT can inform tissue sampling strategies by identifying the most affected regions, while pathology provides direct confirmation of airway inflammatory and remodelling patterns that can refine phenotyping. The proposed minimum datasets (Tables 4–7) aim to establish a shared language across specialties and facilitate reproducible, clinically actionable conclusions in real-world settings. The proposed multidisciplinary workflow for integrating chest CT, bronchial biopsy, and structured radiology/pathology reporting into adult severe asthma care is summarized in Figure 1.
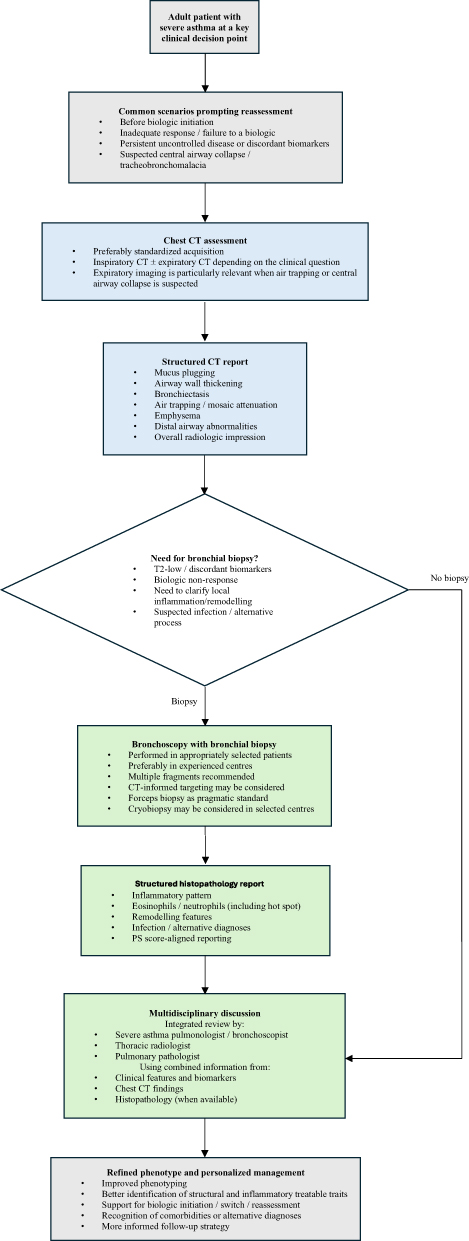 |
Figure 1 Proposed multidisciplinary workflow for the use of chest CT and bronchial biopsy in adult severe asthma. This figure summarizes the AGHORA practice-oriented approach to integrating chest CT and bronchial biopsy into the work-up of adult severe asthma at key clinical decision points. Chest CT is positioned as an initial structural and phenotyping tool, whereas bronchial biopsy is reserved for selected complex cases in which tissue assessment may refine inflammatory characterization, remodelling assessment, or diagnostic clarification. The workflow emphasizes structured radiology and pathology reporting and final integration through multidisciplinary discussion to support personalized management. Abbreviations: CT, computed tomography; MDT, multidisciplinary team; PS score, pathological score. |
The main practice-oriented recommendations derived from the AGHORA multidisciplinary consensus are summarized in Table 9.
 |
Table 9 Key Recommendations From the AGHORA Multidisciplinary Consensus |
Evidence Gaps and Future Research Priorities
Despite the increasing clinical interest in airway tissue phenotyping and CT-based airway assessment in severe asthma, the evidence supporting when, how, and for whom these techniques should be implemented remains fragmented. A major driver for this consensus was the marked inter-centre heterogeneity in indications, acquisition protocols, reporting standards, and the way imaging and pathology findings are integrated into therapeutic decisions. Ultimately, the goal of this standardization effort is to enable prospective studies and clinical trials capable of determining whether harmonized CT- and biopsy-based assessments improve phenotyping, treatment selection, and patient outcomes.
The AGHORA panel proposes pragmatic standards for HRCT acquisition and reporting, as well as recommendations for bronchial biopsy sampling and pathology reporting. However, moving from expert-based best practice to evidence-informed guidance requires a structured research agenda—an approach commonly used in multidisciplinary workshop reports to accelerate translation into practice. In line with the research priorities explicitly identified by the panel (Table 8), the most relevant evidence gaps can be grouped into the following domains.
Standardisation, Feasibility, and Reproducibility of CT Acquisition and Reporting
Even within expert centres, there is variability in acquisition choices that directly affects the ability to characterise small airway disease. For instance, the role of inspiratory-only CT versus combined inspiratory–expiratory acquisition as part of the baseline pre-biologic assessment remains debated; the prevailing view favours inspiratory+expiratory imaging to avoid missing air trapping and distal airway involvement, but comparative outcome data are lacking. In parallel, advanced quantitative post-processing (eg, densitometry-based air trapping quantification, volumetry, vascular pruning metrics) is not ready for routine clinical deployment in many settings because it is time-consuming and dependent on specialised software, and therefore risks widening inter-centre variability rather than reducing it. Research should prioritise harmonised acquisition parameters, minimum reporting datasets, interobserver reliability studies, and pragmatic feasibility assessments in real-world severe asthma clinics.
Validation of Radiological Biomarkers and Development of Predictive Imaging Scores
The panel agreed that CT can add clinically meaningful information to severe asthma phenotyping and decision-making, but robust validation is still required for several imaging features as predictive or prognostic biomarkers. There is a need to (i) develop and validate reproducible radiological scores, (ii) determine which CT features “matter” for outcomes, and (iii) define how these features should be incorporated into clinical pathways. A specific, high-impact gap is the ability of CT-derived phenotypes (eg, mucus plugging burden, airway wall thickening patterns, bronchiectasis, mosaic attenuation/air trapping, distal airway abnormalities) to predict differential response to specific biologic classes—one of the explicit priorities raised by the group.
Clinical Utility and Prognostic Value of Quantified Small Airway Disease
Air trapping is widely recognised as a marker of small airway disease, but the prognostic meaning of visually assessed versus quantitatively measured air trapping, and how changes over time relate to exacerbations, symptom control, lung function, and biologic response, remains uncertain. The panel identified “prognostic value of quantified air trapping” and “standardisation of quantification software” as priority research targets. Additionally, given the current feasibility constraints of advanced quantification, a staged research strategy is needed: first harmonise software pipelines and thresholds in motivated expert centres, and then test simplified, scalable outputs suitable for broader adoption.
Imaging-Guided Bronchial Biopsy: Does “Targeting” Improve Yield and Decision-Making?
A central hypothesis discussed during AGHORA is that airway inflammation and remodelling may be heterogeneous and patchy. For this reason, radiologists should attempt to guide bronchial biopsy (or alternative distal sampling approaches) towards the most affected areas (eg, maximal thickening or mucus), but the added value of this strategy requires prospective validation and demonstration of clinical “return on investment” Accordingly, the group explicitly prioritised prospective validation of image-guided biopsy. Key unanswered questions include: (i) how many segments need to be targeted to overcome heterogeneity; (ii) whether imaging-guided sampling improves inflammatory endotyping beyond blood biomarkers; (iii) whether it increases actionable findings (eg, occult infection, mixed granulocytic inflammation) that change management; and (iv) whether it ultimately improves patient outcomes (eg, biologic selection success, exacerbation reduction).
Optimising Tissue Acquisition methods (Forceps vs Cryoprobe) and Safety/Implementation Trade-Offs
Another clinically important gap is the absence of robust comparative data on sampling techniques. While cryobiopsy can provide larger specimens and better epithelial preservation, it has higher cost and limited availability; conversely, many centres consider forceps sampling sufficient for the information typically required in severe asthma decision-making, and the panel recognised this as an area of ongoing debate. Pragmatic comparative effectiveness studies (including safety, yield, processing requirements, and downstream clinical impact) are needed to inform scalable recommendations.
Standardisation and Clinical Validation of Pathology Reporting (Including Digital/AI Support)
The group underscored the need for consensus around a structured pathology report for severe asthma management and highlighted this as a research priority. In addition to defining minimum datasets (eg, granulocytic inflammation, remodelling features), future work must address interobserver variability, reporting reproducibility, and how pathology outputs should be integrated into multidisciplinary decisions.
Digital pathology and AI tools may help reduce interobserver variability and automate quantitative readouts (eg, eosinophil/neutrophil counting, basement membrane thickness, fibrosis area), but require careful validation across scanners, staining protocols, and centres before any clinical adoption.
Multidisciplinary Pathways and Implementation Science
Finally, the clinical value of HRCT and bronchial biopsy in severe asthma is likely to depend not only on the tests themselves but also on how results are communicated and acted upon. The panel emphasised that multidisciplinary collaboration (radiology–pulmonology–pathology) is fundamental to ensure clinically meaningful requests, interpretable reports, and consistent decision-making—analogous to established interstitial lung disease boards. Future studies should therefore evaluate structured MDT pathways as complex interventions, including process metrics (timeliness, adherence to reporting templates, decision concordance) and patient-centred outcomes, together with health economic evaluations.
Discussion
This multidisciplinary expert consensus provides pragmatic recommendations on when and how to use chest CT and bronchial biopsy in severe asthma, and—crucially—how to make both modalities clinically actionable through standardized radiology and pathology reporting embedded within a coordinated multidisciplinary team (MDT) workflow. The AGHORA meeting was intentionally grounded in real-world implementation across tertiary-care settings, where substantial inter-centre heterogeneity persists regarding CT indications/protocols, biopsy indications/sampling, and the integration of findings into biologic decision-making. Our statement is therefore designed to complement (not replace) guideline-based care, focusing on decision points where CT and/or biopsy are most likely to refine phenotype, clarify competing drivers of poor control, and support structured reassessment.
Chest CT as Decision Support at Key Inflection Points
While chest CT has traditionally been positioned as a tool to exclude alternative diagnoses and identify comorbidities, the panel endorsed a broader, precision-oriented role in severe uncontrolled asthma: CT can function as a phenotyping and decision-support tool when requested at predefined therapeutic inflection points—particularly (i) before first biologic initiation and (ii) during reassessment after inadequate response to a biologic. In these settings, CT can document baseline structural traits for future within-patient comparison and subsequent treatment-reassessment decisions and reveal treatable traits and competing processes (eg, mucus plugging burden, bronchiectasis evolution, small-airway disease patterns, distal airway “red flags”), which may explain persistent symptoms despite optimized therapy and influence subsequent management.
A recurring practical message is that CT value depends not only on performing a scan, but on aligning acquisition and reporting with the clinical question. The panel trended toward combined inspiratory–expiratory acquisition in the pre-biologic setting to avoid missing clinically relevant air trapping/small-airway disease that may be under-recognized on inspiratory-only studies, while acknowledging feasibility and radiation considerations across centres. In suspected tracheobronchomalacia (TBM) or central airway collapse, expiratory imaging should be explicitly requested, and interpretation should incorporate collapse pattern and clinical context rather than relying on a single numerical threshold.
Standardizing CT reporting was one of the central outputs. A minimum dataset and structured “Impression” are intended to reduce interpretive variability, improve MDT usability, and enable longitudinal comparison where repeat imaging is needed. In contrast, advanced quantitative CT post-processing (eg, densitometry/volumetry/vascular metrics) was regarded as promising but not ready for routine adoption across centres because of software dependence, time burden, and limited harmonization; at present, its most appropriate role is in research or in selected centres with validated pipelines. An additional methodological consideration is that airway calibre and apparent wall thickness are dynamic rather than fixed anatomical measurements, and may be influenced by bronchomotor tone, parenchymal tethering, and airflow-related airway behaviour. This is particularly relevant when serial CT examinations are used for longitudinal assessment or when structural changes are interpreted in response to targeted therapies. For this reason, whenever quantitative or within-patient comparisons are intended, CT acquisition should be performed under as consistent conditions as possible, including bronchodilation status and lung inflation, to improve interpretability and comparability.18
Beyond baseline phenotyping, an additional rationale for standardized CT acquisition and reporting is the possibility of longitudinal structural assessment in selected patients receiving targeted biologic therapy. Emerging data suggest that effective biologics may be associated with measurable changes in CT-visible airway abnormalities over time, particularly mucus plugging and airway wall thickening, reinforcing the concept that imaging may capture treatment-responsive “structural treatable traits”.15 This raises the question of whether follow-up CT could have a role in specific scenarios—such as persistent symptoms despite clinical improvement, biologic non-response, or research-oriented monitoring—if acquisition protocols are harmonized and reporting is sufficiently standardized to support meaningful within-patient comparison (eg, using consistent inspiratory–expiratory protocols and reproducible scoring approaches).
Bronchial Biopsy for Airway Biology in Complex Scenarios
Bronchial biopsy is gaining renewed interest to directly characterize airway inflammation and remodelling—domains that may be incompletely captured by systemic biomarkers, particularly in steroid-exposed patients and in biologic non-responders. The panel prioritized biopsy in two scenarios where it is most likely to add actionable information: (i) severe uncontrolled asthma with a T2-low systemic biomarker profile when higher phenotypic certainty is required and (ii) inadequate response/failure to an initial biologic after an adequate treatment trial, as part of a structured reassessment of airway biology, remodelling burden, and potential contributory processes (including infection when clinically suspected).
However, the clinical utility of biopsy hinges on reproducibility: (a) pragmatic sampling that acknowledges potential spatial heterogeneity, (b) feasible handling approaches that support broad adoption, and (c) pathology reporting that is structured, interpretable, and explicitly linked to clinical decision-making. The panel therefore supported obtaining multiple fragments (pragmatic minimum) and considering CT-informed targeting toward regions of maximal involvement when imaging is available. Conventional forceps biopsy was considered a pragmatic standard given accessibility, whereas cryoprobe techniques were recognized as potentially advantageous for specimen quality but not uniformly required due to feasibility, cost, and local expertise variability.
Standardized Histopathology Reporting and the PS Score
A major translational barrier is the lack of standardized, reproducible histopathology reporting for endobronchial biopsies in severe asthma. Without harmonized minimum datasets, biopsy interpretation becomes centre- and reader-dependent, limiting clinician confidence, undermining cross-centre comparability, and constraining multicentre research. The panel therefore endorsed PS score–aligned reporting as a pragmatic framework for standardization. The PS score operationalizes key inflammatory and remodelling domains through 11 items and has demonstrated good-to-excellent interobserver reliability for several core components (eg, submucosal eosinophils ICC 0.849; eosinophilic count/field ICC 0.807; goblet cell hyperplasia ICC 0.848; squamous metaplasia ICC 0.968; mucosal gland prominence ICC 0.869), supporting feasibility for multicentre implementation.
Beyond item-level reporting, the panel emphasized two operational principles to make pathology “MDT-ready.” First, hotspot reporting (in addition to mean values) was prioritized for granulocytic inflammation to capture focal activity in a heterogeneous disease. Second, bidirectional communication was considered essential: pathology interpretation is strengthened when specimens are accompanied by minimum clinical context (indication, biomarkers, current/prior therapies—especially systemic steroids and biologics—treatment response, and key CT findings), while pathology outputs should include a structured, clinically oriented interpretive summary (dominant inflammatory phenotype and remodelling grade) to support treatment planning.
Why MDT Integration is the “Multiplier”
Across discussions, a consistent conclusion emerged: the highest added value of CT and biopsy is achieved when both are implemented within a coordinated MDT workflow. In severe asthma, interpretability and actionability depend on (i) a well-posed clinical question, (ii) tailored acquisition and structured reporting, and (iii) shared interpretation across pulmonology, radiology, and pathology. The proposed workflow is conceptually analogous to established interstitial lung disease boards but adapted to severe asthma decision points (notably biologic initiation and biologic non-response). Within this framework, CT can inform sampling strategies under the hypothesis of patchy/heterogeneous airway involvement, and pathology can provide complementary confirmation of inflammatory and remodelling patterns that refine phenotyping beyond systemic biomarkers alone. The standardized datasets proposed for radiology and pathology create a shared language across specialties and provide the infrastructure required for meaningful multicentre benchmarking and research.
Limitations
This work has limitations inherent to its design. First, the recommendations were generated through an in-person, discussion-based process with show-of-hands voting rather than a formal Delphi methodology; accordingly, agreement levels are qualitative and reflect observed convergence rather than predefined quantitative thresholds. Second, the panel was purposively selected from predominantly tertiary-care settings, which may limit generalizability to non-tertiary environments or health systems with different resource constraints. Third, no patient-level outcome data were collected; therefore, these recommendations should be interpreted as practice-oriented expert guidance rather than evidence-based directives. Fourth, the scope of the AGHORA meeting was intentionally restricted to chest CT and bronchial biopsy. Other imaging modalities, including MRI, were not addressed and may represent relevant areas for future research. Finally, broader implementation considerations—including health economics, resource availability, radiation exposure associated with serial CT strategies, and the procedural risks and logistical requirements of bronchoscopy/biopsy pathways—require dedicated evaluation. Chest CT should therefore be requested selectively at clinically meaningful decision points, and bronchoscopy with bronchial biopsy should be reserved for appropriately selected patients and performed in centres with relevant expertise.
Implications and Future Directions
The consensus provides a pragmatic starting point for harmonizing CT and biopsy pathways in severe asthma and for reducing inter-centre variability that currently limits both clinical utility and research scalability. Priority evidence gaps include prospective validation of standardized CT protocols and reporting templates; development and validation of predictive imaging scores; clarification of the prognostic meaning of visually assessed versus quantified air trapping; evaluation of CT-guided biopsy strategies; pragmatic comparisons of biopsy techniques and their clinical impact; and multicentre validation of PS score–aligned reporting supported by digital pathology/AI-assisted quantification. MDT implementation itself should be studied as a complex intervention, incorporating process measures (template adherence, timeliness, decision concordance) and patient-centred outcomes with health economic analyses.
In summary, the AGHORA consensus defines practical indications and minimum datasets for chest CT and bronchial biopsy in severe asthma and proposes PS score–aligned histopathology and structured CT reporting as key enablers of reproducible, clinically actionable airway phenotyping within MDT decision-making.
Conclusions
In conclusion, the AGHORA multidisciplinary consensus proposes pragmatic, MDT-centred recommendations for when and how to use chest CT and bronchial biopsy in severe asthma, emphasizing standardized radiology and pathology reporting and PS score–aligned histopathology as key enablers of reproducible, clinically actionable airway phenotyping. By defining minimum datasets and decision-point indications, this statement aims to support more consistent practice across centres, facilitate meaningful multidisciplinary interpretation, and establish a platform for prospective validation and future precision-medicine research in severe asthma.
Data Sharing Statement
No datasets were generated or analysed during the current study. Therefore, data sharing is not applicable to this article.
Ethics Statement
This manuscript reports an expert consensus based on the AGHORA meeting discussions and does not include individual-level patient data. Therefore, institutional review board/ethics committee approval and informed consent were not required.
Acknowledgments
The authors would like to acknowledge the Asociación Cántabra de Investigación en Aparato Respiratorio (ACINAR) for its institutional support in the organization of the AGHORA meeting. We also thank Joan Rojas Crespo (Brand Manager, Respiratory, Sanofi) and Alejandra Ellacuria (Medical Scientific Liaison, Immunology Medical Department) for their logistical coordination and support in facilitating the meeting. Their contribution was limited to organizational aspects and did not influence the scientific content, discussions, or conclusions of this manuscript.
Collaborators
The AGHORA Group includes the following participants (in alphabetical order):
Abascal Bolado, Beatriz – Hospital Universitario Marqués de Valdecilla, Santander, Spain; Armendariz Tellitu, Karmele – Hospital Galdakao-Usansolo, Galdakao, Spain; Arrieta Artieda, Irma – Hospital de Urduliz, Urduliz, Spain; Carrascosa Anguiano, María Inés – Hospital de Urduliz, Urduliz, Spain; Castellanos Romero, Lucía – Hospital Universitario de Burgos, Burgos, Spain; Castillo De Juan, Javier – Hospital Universitario Basurto, Bilbao, Spain; Chavarri Ibáñez, Elena – Hospital Álvaro Cunqueiro, Vigo, Spain; Curi Chercoles, Sergio – Complejo Hospitalario de Navarra, Pamplona, Spain; Dorronsoro Quintana, Silvia – Hospital Universitario Donostia, San Sebastián, Spain; Echegoyen Silanes, Ana – Complejo Hospitalario de Navarra, Pamplona, Spain; Egurrrola Izquierdo, Mikel – Hospital Galdakao-Usansolo, Galdakao, Spain; Etxebarria Kaiuela, Laida – Complejo Hospitalario de Navarra, Pamplona, Spain; Etxegaray Ganboa, Leire – Hospital Galdakao-Usansolo, Galdakao, Spain; Fernández Abad, Luisa María – Hospital Universitario de Burgos, Burgos, Spain; Fernández Nebreda, Asier – Hospital Universitario Basurto, Bilbao, Spain; Fernández Solé, Soledad – Hospital Universitario Cruces, Barakaldo, Spain; Galardi Mendiluze, Ainhoa – Hospital Universitario Donostia, San Sebastián, Spain; García Alberdi, Eva – Hospital de Urduliz, Urduliz, Spain; García Hernaez, Raquel – Hospital San Pedro, Logroño, Spain; García Martín, Sergio – Hospital de Laredo, Laredo, Spain; Gómez Román, José Javier – Hospital Universitario Marqués de Valdecilla, Santander, Spain; González Gutiérrez, Mari Paz – Hospital Universitario Central de Asturias, Oviedo, Spain; Gutiérrez Urra, Tamara – Complejo Hospitalario de Navarra, Pamplona, Spain; Hermoso de Mendoza Aristegui, Sara – Complejo Hospitalario de Navarra, Pamplona, Spain; Juez García, Laura – Hospital Río Ortega, Valladolid, Spain; Juristi Abaunz, María Aranzazu – Hospital Universitario Donostia, San Sebastián, Spain; López González, Francisco Julián – Hospital Universitario Central de Asturias, Oviedo, Spain; Madrid González, Juan Cruz – Hospital Universitario Marqués de Valdecilla, Santander, Spain; Mardones Charroalde, Aizea – Hospital Universitario Basurto, Bilbao, Spain; Martínez-Cachero García, Álvaro – Hospital Universitario Central de Asturias, Oviedo, Spain; Michel de la Rosa, Francisco Javier – Hospital Universitario Donostia, San Sebastián, Spain; Ortiz Portal, Félix – Hospital Universitario Marqués de Valdecilla, Santander, Spain; Pueyo Bastida, Ana María – Hospital Universitario de Burgos, Burgos, Spain; Saiz Camín, Mónica – Hospital Universitario Cruces, Barakaldo, Spain; Urrutia Landa, Isabel – Hospital Galdakao-Usansolo, Galdakao, Spain.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This expert meeting (AGHORA) was supported by an unrestricted educational grant from Sanofi and Regeneron Pharmaceuticals, Spain. The sponsor had no role in the scientific content of the meeting, including study conception, methodology, data interpretation, expert discussions, or in the writing, review, and approval of the manuscript. The views and opinions expressed in this article are solely those of the authors.
Disclosure
García-Rivero JL, reports speaker fees from Zambon, Gebro Pharma, Grifols, GSK, AstraZeneca, Chiesi, Menarini and Sanofi; consulting fees from GSK, AstraZeneca, ALK, and Sanofi; and research grants from AstraZeneca. Cosio BG reports speaker fees from GSK, AstraZeneca, Chiesi, Menarini and Sanofi; consulting fees from GSK, AstraZeneca, and Sanofi; and research grants from AstraZeneca and Menarini. The other authors report no conflicts of interest in this work.
References
1. Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43(2):343–21. doi:10.1183/09031936.00202013
2. Busse WW, Castro M, Casale TB. Asthma management in adults. J Allergy Clin Immunol Pract. 2023;11(1):21–33. doi:10.1016/j.jaip.2022.10.015
3. Brusselle GG, Koppelman GH. Biologic therapies for severe asthma. New Engl J Med. 2022;386(2):157–171. doi:10.1056/NEJMra2032506
4. Tiotiu A. Applying personalized medicine to adult severe asthma. Allergy Asthma Proc. 2021;42(1):e8–e16. doi:10.2500/aap.2021.42.200100
5. Winkler T, Frey U. Airway remodeling: shifting the trigger point for exacerbations in asthma. J Allergy Clin Immunol. 2021;148(3):710–712. doi:10.1016/j.jaci.2021.07.010
6. Oberle AJ, Abbas F, Adrish M, et al. Biologic management in severe asthma for adults: an American college of chest physician clinical practice guideline. Chest. 2025;169(2):336–348. doi:10.1016/j.chest.2025.08.042
7. Perez-de-llano L, Scelo G, Tran TN, et al. Exploring definitions and predictors of severe asthma clinical remission post-biologic in adults. Am J Respir Crit Care Med. 2024;210(7):869–880. doi:10.1164/rccm.202311-2192OC
8. Verbanck S. Quantitative computed tomography in asthma: for good measure. Am J Respir Crit Care Med. 2020;201(8):885–886. doi:10.1164/rccm.201912-2481ED
9. Cozzi D, Gozzi L, Giovannelli S, et al. Back to the future in asthma imaging: quantitative assessment and new perspectives. Radiol Med. 2025;131(1):88–101. doi:10.1007/s11547-025-02125-5
10. Eddy RL, Svenningsen S, Kirby M, et al. Is computed tomography airway count related to asthma severity and airway structure and function? Am J Respir Crit Care Med. 2020;201(8):923–933. doi:10.1164/rccm.201908-1552OC
11. Luzzi S, Pianigiani T, Dilroba A, et al. Computed tomography in severe asthma assessment: a systematic review. J Asthma. 2025:1–10. doi:10.1080/02770903.2025.2460549
12. Zounemat Kermani N, Chung KF, Macis G, et al. Radiomultiomics: quantitative CT clusters of severe asthma associated with multiomics. Eur Respir J. 2024;64(5):2400207. doi:10.1183/13993003.00207-2024
13. Ueda T, Niimi A, Matsumoto H, et al. Role of small airways in asthma: investigation using high-resolution computed tomography. J Allergy Clin Immunol. 2006;118(5):1019–1025. doi:10.1016/j.jaci.2006.07.032
14. Gupta S, Siddiqui S, Haldar P, et al. Qualitative analysis of high-resolution CT scans in severe asthma. Chest. 2009;136(6):1521–1528. doi:10.1378/chest.09-0174
15. Castro M, Papi A, Porsbjerg C, et al. Effect of dupilumab on exhaled nitric oxide, mucus plugs, and functional respiratory imaging in patients with type 2 asthma (VESTIGE): a randomised, double-blind, placebo-controlled, Phase 4 trial. Lancet Respir Med. 2025;13(3):208–220. doi:10.1016/S2213-2600(24)00362-X
16. Porsbjerg C, Dunican EM, Lugogo NL, et al. Effect of dupilumab on mucus burden in patients with moderate-to-severe asthma: the VESTIGE trial. Am J Respir Crit Care Med. 2025. doi:10.1164/rccm.202410-1894OC
17. Kim S, Lee CH, Jin KN, Cho SH, Kang HR. Severe asthma phenotypes classified by site of airway involvement and remodeling via chest CT scan. J Invest Allergol Clin Immunol. 2018;28(5):312–320. doi:10.18176/jiaci.0265
18. Winkler T, Fain SB. Mucus plugs and remodeling in the small airways: considerations for complex airway behavior and instability in asthma. Am J Respir Crit Care Med. 2026;212(2):199–201. doi:10.1164/rccm.202508-1859ED
19. Mummy DG, Dunican EM, Carey KJ, et al. Mucus plugs in asthma at CT associated with regional ventilation defects at (3)He MRI. Radiology. 2022;303(1):184–190. doi:10.1148/radiol.2021204616
20. Tang M, Elicker BM, Henry T, et al. Mucus plugs persist in asthma, and changes in mucus plugs associate with changes in airflow over time. Am J Respir Crit Care Med. 2022;205(9):1036–1045. doi:10.1164/rccm.202110-2265OC
21. Cosío BG, Shafiek H, Mosteiro M, et al. Redefining the role of bronchoscopy in the workup of severe uncontrolled asthma in the era of biologics: a prospective study. Chest. 2023;164(4):837–845. doi:10.1016/j.chest.2023.03.012
22. Moore WC, Evans MD, Bleecker ER, et al. Safety of investigative bronchoscopy in the severe asthma research program. J Allergy Clin Immunol. 2011;128(2):328–336.e3. doi:10.1016/j.jaci.2011.02.042
23. Hsieh A, Assadinia N, Hackett T-L. Airway remodeling heterogeneity in asthma and its relationship to disease outcomes. Review. Front Physiol. 2023;14. doi:10.3389/fphys.2023.1113100
24. Tiotiu Cepuc A, Steiropoulos P, Novakova S, et al. Airway remodeling in asthma: mechanisms, diagnosis, treatment, and future directions. Archivos de bronconeumologia. 2024. doi:10.1016/j.arbres.2024.09.007
25. Cosío BG, Iglesias A, Shafiek H, et al. The role of bronchial biopsy in the prediction of response to biologic therapy in severe uncontrolled asthma: a prospective study. Chest. 2025;167(4):945–955. doi:10.1016/j.chest.2024.11.045
26. Cosio BG, Shafiek H, Iglesias A, et al. Validation of a pathological score for the assessment of bronchial biopsies in severe uncontrolled asthma: beyond blood eosinophils. Archivos de bronconeumologia. 2023;59(8):502–509. doi:10.1016/j.arbres.2023.05.014
27. Berair R, Hartley R, Mistry V, et al. Associations in asthma between quantitative computed tomography and bronchial biopsy-derived airway remodelling. Eur Respir J. 2017;49(5). doi:10.1183/13993003.01507-2016
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Awareness and Predictors of the Use of Bioinformatics in Genome Research in Saudi Arabia
Alomair L, Abolfotouh MA
International Journal of General Medicine 2023, 16:3413-3425
Published Date: 11 August 2023
Precision Medicine in Asthma: The Role of Biomarkers
Quek E, Horn N, Siddiqui S
ImmunoTargets and Therapy 2025, 14:1479-1513
Published Date: 28 December 2025
Uterine Leiomyomas with Intravenous Leiomyomatosis: A Report of Two Cases
Jiang S, Feng Z, Han L
International Journal of Women's Health 2026, 18:608143
Published Date: 4 June 2026
Assessing Invasiveness of Ground-Glass Nodules Using Ternary-Class CT Radiomics Models: A Multi-Center Study with SHAP Explanations
Zhao P, Chen H, Gu H, Lin Y, Ma Y
Cancer Management and Research 2026, 18:602730
Published Date: 5 June 2026