Back to Journals » International Journal of Women's Health » Volume 18
Uterine Leiomyomas with Intravenous Leiomyomatosis: A Report of Two Cases
Authors Jiang S ![]() , Feng Z, Han L
, Feng Z, Han L
Received 10 March 2026
Accepted for publication 24 May 2026
Published 4 June 2026 Volume 2026:18 608143
DOI https://doi.org/10.2147/IJWH.S608143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Shengping Jiang,1,* Zhen Feng,2,* Lin Han3
1Department of Radiology, The First People’s Hospital of Yulin, Yulin, Guangxi, People’s Republic of China; 2Department of Vascular Surgery, The First People’s Hospital of Yulin, Yulin, Guangxi, People’s Republic of China; 3Department of Rehabilitation Medicine, The First People’s Hospital of Yulin, Yulin, Guangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lin Han, Department of Rehabilitation Medicine, The First People’s Hospital of Yulin, Yulin, Guangxi, People’s Republic of China, Email [email protected]
Purpose: Intravenous leiomyomatosis (IVL) is a rare histological variant of uterine leiomyoma characterized by benign smooth muscle cells proliferating within the venous system. Despite its benign histology, IVL exhibits “quasi-malignant” behavior through intravascular extension, often leading to misdiagnosis as venous thrombosis or malignancy.
Case Presentation: We report two cases of uterine leiomyoma complicated by IVL. In Case 1, a 42-year-old woman with initially suspected iliac vein and inferior vena cava (IVC) thrombosis underwent contrast-enhanced computed tomography (CT), which demonstrated a continuous tumor extending from the uterus through the left ovarian vein and IVC into the right atrium. Based on the characteristic imaging findings and multidisciplinary evaluation, the preliminary clinical diagnosis of IVL was established and a one-stage combined surgery involving total hysterectomy, excision of the venous tumor, and cardiac resection under extracorporeal circulation was successfully performed. In Case 2, a 43-year-old woman with a history of myomectomy presented with broad ligament leiomyoma and intravascular extension into the iliac vein and IVC. The imaging appearance similarly raised strong suspicion for IVL rather than thromboembolic disease. The patient underwent total hysterectomy with bilateral adnexectomy and vascular reconstruction to remove the intraluminal tumor. Histopathology in both cases confirmed IVL. No recurrence was observed during the 22-month and 12-month follow-up periods, respectively.
Conclusion: These cases highlight the importance of considering IVL in women presenting with uterine masses and unexplained venous filling defects. Recognition of characteristic CT findings, particularly continuous intravascular extension along venous anatomy, is essential for differentiating IVL from deep vein thrombosis (DVT) and leiomyosarcoma. Early multidisciplinary assessment and complete surgical resection are critical for successful management and favorable long-term outcomes.
Keywords: intravenous leiomyomatosis, uterine leiomyoma, multidisciplinary team, computed tomography, case report
Introduction
Uterine leiomyomas are the most common tumors in women, with an age-standardized prevalence of approximately 2841.07 per 100,000 population (95% CI, 2164.43–3682.27) and an age-standardized incidence of 250.93 per 100,000 population (95% CI, 183.44–330.94) worldwide in 2021.1 Clinical manifestations range from asymptomatic disease to abdominal pain, menorrhagia, and infertility. Although most uterine leiomyomas are confined to the uterus and follow a benign clinical course, a rare subgroup of smooth muscle tumors exhibits distinct quasi-malignant behaviors.2 Among these, intravenous leiomyomatosis (IVL) is a rare entity characterized by intravascular extension of uterine leiomyomas into the pelvic veins, inferior vena cava (IVC), right atrium, and occasionally the pulmonary arteries.3 Due to its rarity and insidious clinical presentation, IVL is frequently misdiagnosed as intravenous thrombosis or leiomyosarcoma,4 which may lead to misguided therapeutic strategies. Herein, we report two cases of uterine leiomyoma complicated by IVL, emphasizing the critical role of preoperative imaging and multidisciplinary evaluation.
Case Presentation
Case 1
A 42-year-old woman (G3P3) presented with menstrual irregularities and menorrhagia. She was initially diagnosed with uterine leiomyomas, with an incidental finding of suspected IVC and iliac vein thrombosis identified via ultrasound at a local hospital. She was subsequently referred to our gynecology department for further evaluation. The patient reported no symptoms such as chest tightness, palpitations, or dyspnea. Physical examination revealed no lower extremity swelling, with normal muscle strength and tone, and no localized tenderness. Pelvic examination revealed a significantly enlarged, firm, and irregularly shaped uterus, with a palpable mass in the left adnexal region. There was no family history of thromboembolism, and common causes for venous thrombosis were ruled out through clinical history and laboratory screening, including normal coagulation profiles. Contrast-enhanced computed tomography (CT) revealed hypodense space-occupying lesions within the myometrium and left adnexal region, extending along the left ovarian vein, left renal vein, and IVC, ultimately progressing into the right atrium (Figure 1A and B).
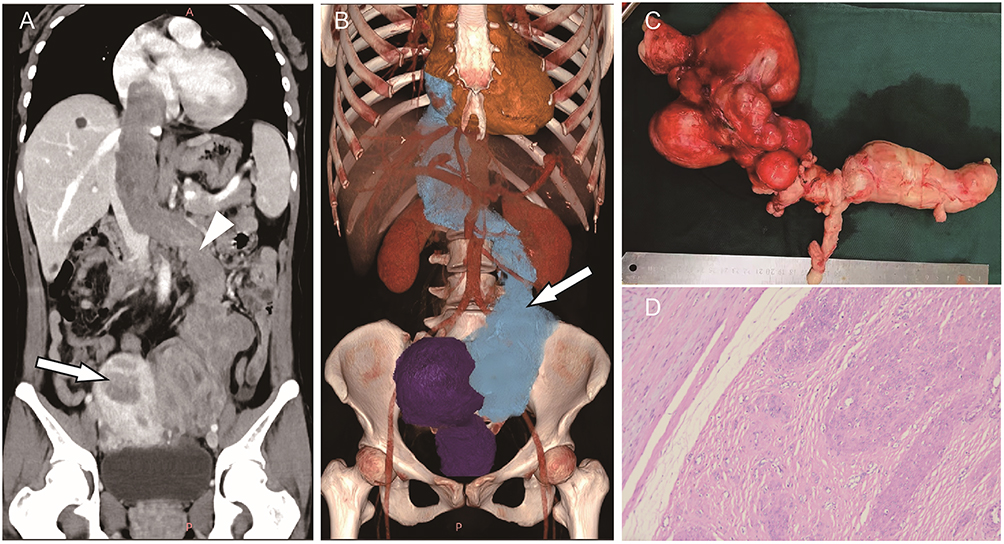 |
Figure 1 Imaging and pathological findings of case 1. (A) Coronal CT showing the uterine leiomyoma (white arrow) and intravenous leiomyomatosis (white arrowhead). (B) Volume rendering technique (VRT) image clearly demonstrating the intravascular course of the tumor. (C) Gross appearance of the resected tumor specimen. (D) Histopathological examination of the tumor (Hematoxylin and eosin stain; magnification, ×100). |
Given the complexity of the case, a multidisciplinary team (MDT) involving gynecologists, vascular surgeons, cardiac surgeons, and radiologists was convened. After a thorough review of the clinical symptoms and the characteristic filling defects on contrast-enhanced CT, a preliminary diagnosis of uterine leiomyoma complicated by IVL with cardiac involvement was established. Consequently, anti-coagulant therapy was intentionally withheld to avoid unnecessary bleeding hazards, and the patient was scheduled directly for a one-stage synchronized surgical resection. A coordinated surgical plan was devised to ensure complete tumor resection. Intraoperatively, a large, firm uterine tumor was observed in the pelvic cavity, characterized by distinct margins and an absence of adhesion or infiltration into the surrounding tissues. The tumor mass extended along the left ovarian vein, the left renal vein, and the IVC, ultimately reaching the right atrium. During the procedure, the gynecological team performed a total hysterectomy and left salpingectomy. The vascular surgeons resected the intravascular tumor extension from the left ovarian vein to the left renal vein, isolated the IVC, and achieved vascular control using proximal and distal occlusion tapes. Simultaneously, cardiac surgeons performed a median sternotomy, established cardiopulmonary bypass, and conducted a right atriotomy. The tumor components within the right atrium and IVC were bluntly dissected and mobilized, then completely extracted through the IVC incision (Figure 1C).
Postoperative histopathological examination of the resected uterus, pelvic masses, and the intravascular tumor components—retrieved from the ovarian vein, inferior vena cava, and right atrium—consistently revealed spindle-shaped tumor cells arranged in intersecting fascicles with a woven pattern. These cells were characterized by abundant eosinophilic cytoplasm and an absence of necrosis, with numerous surrounding venous channels of varying luminal sizes and wall thicknesses observed (Figure 1D). Immunohistochemical (IHC) staining showed that the tumor cells were positive for estrogen receptor (ER) and desmin (Des), while CD34 was negative in the tumor cells. These findings confirmed the final diagnosis of IVL. The patient underwent regular clinical and imaging surveillance and remained free of recurrence during the 22-month postoperative follow-up period.
Case 2
A 43-year-old woman (G4P4) presented with a 3-month history of abdominal discomfort and lumbar distension. Her surgical history included a laparotomy for ovarian teratoma and uterine myomectomy 10 years prior, followed by the excision of a broad ligament leiomyoma at another institution 14 months prior to admission. Physical examination revealed a firm, relatively immobile, non-tender mass measuring approximately 10 cm in the left adnexal region, with well-defined margins. No abnormalities were noted in the right adnexa. Pelvic ultrasonography demonstrated a large left broad ligament leiomyoma (12.6 × 9.4×9.9 cm) and a concomitant uterine leiomyoma. However, subsequent contrast-enhanced CT revealed intravascular filling defects extending into the internal iliac vein, the left common iliac vein, and the IVC (Figure 2A–D), in addition to the uterine masses. Recalling our experience with the first case, these clinical and imaging features immediately triggered a high index of clinical suspicion for IVL. Following the exclusion of common thromboembolic risk factors through systematic laboratory screening, which showed no evidence of a hypercoagulable state, the diagnosis of IVL was further solidified based on these characteristic radiological hallmarks.
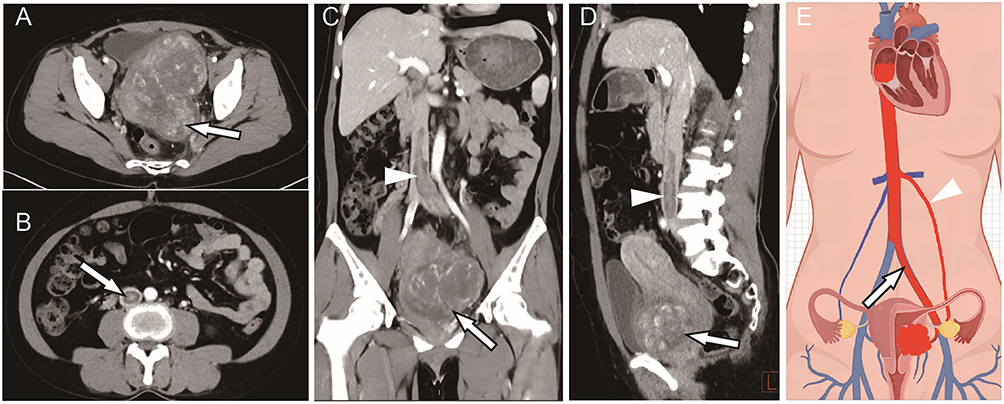 |
Figure 2 Contrast-enhanced CT findings of case 2. (A) A giant leiomyoma involving the uterus and the left broad ligament (white arrow). (B) Intravascular extension of the tumor into the left internal iliac vein, common iliac vein, and inferior vena cava (white arrowhead). (C and D) Coronal (C) and sagittal (D) views showing the uterine and broad ligament leiomyomas (white arrow) and the intravenous leiomyomatosis (white arrowhead). (E) Schematic illustration of the two primary pathways of leiomyoma extension into the venous system: the iliac vein (arrow) and the ovarian vein (arrowhead). |
Following MDT consultation, a one-stage combined surgical approach was undertaken. Intraoperatively, a 12-cm irregular, firm mass was identified in the uterus and the left broad ligament, with partial adhesions to the rectum and mesentery. Additionally, an elongated, mobile tumor with distinct margins was palpated within the left iliac vein and the IVC. First, urologists prophylactically placed a left ureteral stent, followed by the gynecological team performing a transabdominal total hysterectomy and bilateral salpingo-oophorectomy. Vascular surgeons subsequently resected the extrauterine pelvic tumor mass, bluntly dissected the left common iliac vein, performed a venotomy to extract the intraluminal tumor extension, and completed a primary venous repair. Postoperative histopathological analysis confirmed the diagnosis of uterine and broad ligament leiomyomas concomitant with IVL. The patient experienced an uneventful recovery and remained free of recurrence during the 12-month postoperative follow-up period.
Discussion
In this report, we present two cases of uterine leiomyoma presenting with intravascular filling defects, which were ultimately confirmed as IVL via histopathological examination. In clinical practice, the rarity of IVL poses a significant diagnostic challenge, as it often mimics more common conditions.
The primary differential diagnosis includes extensive deep vein thrombosis (DVT) and primary intravenous leiomyosarcoma. DVT is frequently the initial suspicion; however, it is typically associated with Virchow’s triad (venous stasis, endothelial injury, and hypercoagulability).5 Radiologically, IVL can be distinguished by its mild-to-moderate enhancement on contrast-enhanced CT, whereas thrombi typically show no enhancement. Furthermore, IVL often exhibits a characteristic “floating sign” within the vessel lumen without adhering to the vein wall, a feature seldom observed in thrombi.
Distinguishing IVL from intravenous leiomyosarcoma is also crucial. While both entities may show enhancement, leiomyosarcoma is typically more aggressive, characterized by vessel wall destruction and invasion of adjacent tissues. In contrast, IVL follows the venous anatomy smoothly, even when extending into the right heart. For patients presenting with right atrial masses, the longitudinal continuity of the lesion—extending from the iliac or renal veins through the IVC—is a pathognomonic sign that helps clinicians rule out primary cardiac tumors, such as myxomas. Recognizing these radiological patterns at an early stage is paramount for optimizing surgical intervention and patient outcomes.
Intravenous leiomyomatosis (IVL) is a rare variant of uterine leiomyoma, accounting for approximately 0.097% of all cases.6 Affected patients typically have a history of uterine leiomyomas or prior uterine surgeries, such as hysterectomy or myomectomy,7 with a median age at diagnosis of approximately 46 years (range: 21–81 years).8 Although histologically benign, IVL demonstrates biologically aggressive, quasi-malignant behavior due to its propensity for profound intravascular extension.9 Yin et al10 elucidated the pathological and molecular features of IVL through an integrative multi-omics analysis. Their study revealed that, compared to normal myometrium and typical uterine fibroids, IVL exhibits a higher degree of fibrosis and hyalinization, poorer vascular supply, and altered vascular morphology. At the molecular level, IVL is further characterized by the dysregulation of focal adhesion, actin cytoskeleton alterations, and chromosome 10q deletions.10
The clinical manifestations of IVL are highly variable and depend on the extent of venous involvement, ranging from asymptomatic discovery to severe complications such as syncope, heart failure, or sudden death.11 Consequently, precise preoperative mapping of the lesion’s extent is paramount for tailoring surgical strategies and evaluating prognosis. To standardize treatment planning, Wen et al proposed a staging system based on the cephalad extent of tumor involvement: Stage I involves tumors confined to the pelvic veins (including uterine, parametrial, iliac, or renal veins) without IVC involvement; Stage II involves extension into the IVC but not the heart; Stage III involves extension into the right atrium or ventricle without reaching the pulmonary arteries; and Stage IV involves extension into the pulmonary vasculature.12 This staging framework provides clinicians with a standardized approach to assess disease severity, select optimal surgical interventions, and anticipate potential intraoperative risks.
Computed tomography (CT) offers distinct advantages in the evaluation of IVL due to its rapid acquisition, high spatial resolution, and versatile post-processing techniques. Advanced tools such as multiplanar reconstruction (MPR), curved planar reconstruction (CPR), and volume rendering (VR) provide comprehensive anatomical visualization, which is essential for precise preoperative assessment. Contrast-enhanced CT plays a pivotal role in delineating lesion morphology and its complex spatial relationship with the vasculature, thereby facilitating meticulous surgical planning. Characteristically, IVL presents on CT as a large uterine or adnexal mass associated with continuous, low-attenuation intraluminal filling defects. These lesions typically extend from the pelvic veins (ovarian, iliac, or renal) into the IVC (Figure 2E), and may further progress into the right heart chambers or, in rare instances, the pulmonary arteries.
Complete surgical resection remains the primary therapeutic objective of IVL management.13 The clinical significance of resection completeness was underscored by Wen et al,12 who reported a recurrence rate of 9.7% (18/185) following complete resection during a mean follow-up of 26.3 months (range, 1–210 months), compared to a significantly higher disease progression rate of 39.0% (12/31) among those with incomplete resection. Therefore, a preoperative multidisciplinary evaluation—comprising cardiothoracic, vascular, gynecologic, urologic, and radiologic specialists—is imperative. Such an integrative approach, coupled with seamless intraoperative collaboration, is essential for achieving radical tumor extirpation while minimizing perioperative complications, particularly in complex cases with extensive vascular and cardiac involvement.14 For young, nulliparous patients without extrauterine vascular involvement, conservative surgery may be considered as a temporary measure; however, rigorous postoperative monitoring is mandatory to ensure early detection and surgical resection of any potential recurrence. For patients with recurrent disease or extensive involvement of major extrauterine vessels and the heart, total hysterectomy and bilateral salpingo-oophorectomy are strongly recommended—even for those who have not yet given birth—to minimize recurrence and prolong survival. Furthermore, anti-estrogen therapy serves as a critical alternative for IVL patients who are ineligible for surgery, or those presenting with postoperative tumor residuals or recurrence.15 Given the potential for late recurrence, life-long and regular postoperative imaging surveillance is strongly recommended to ensure early detection.16 Clinical evidence suggests regular imaging surveillance every 3–6 months for the first two years postoperatively, followed by annual check-ups. Contrast-enhanced CT of the chest, abdomen, and pelvis is the preferred modality. In cases where CT is unavailable, a combination of transvaginal, transanal, and abdominal ultrasound should be utilized to monitor the retroperitoneal and pelvic spaces.8
Conclusion
In conclusion, IVL is a rare entity that frequently mimics deep vein thrombosis or intravenous leiomyosarcoma. Our cases underscore that an accurate preoperative diagnosis relies on a high index of clinical suspicion and the recognition of characteristic radiological patterns. Early differentiation is crucial as it directly dictates the surgical strategy. A multidisciplinary approach is essential for optimized staging and perioperative management. To minimize recurrence, standard treatment should involve a total hysterectomy and bilateral salpingo-oophorectomy, combined with the radical resection of all intravascular and intracardiac tumor extensions.17
Registration of Research Studies
Registration of research is not applicable in our study.
Abbreviations
IVL, intravenous leiomyomatosis; CT, computed tomography; IVC, inferior vena cava; MDT, multidisciplinary team; IHC, immunohistochemical; ER, estrogen receptor; Des, desmin; MPR, multiplanar reconstruction; CPR, curved planar reconstruction; VR, volume rendering.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
The study was approved by the Ethical Committee of The First People’s Hospital of Yulin (No. YLSY-IRB-SR-2026047).
Informed Consent Patient Statement
Written informed consent was obtained from the patients for the publication of this article and any accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that there is no conflict of interests in this study.
References
1. Zhang Z, Huang H, Jiang K, Liu W, Xuan Y, Lu W. Global, regional and national uterine fibroid burdens from 1990 to 2021 and projections until 2050: results from the GBD study. BMC Women’s Health. 2025;25(1):423. doi:10.1186/s12905-025-03974-y
2. Li J, Huang H, Chen X, Zeng Q. Pathological characteristics and clinical prognostic analysis of intravenous leiomyomatosis: a retrospective study of 43 cases. Front Med. 2025;12.
3. Wu X, Yang S, Liang Y. Intravenous leiomyomatosis presenting as pulmonary embolism: a cardiovascular perspective in two cases. J Geriatric Cardiol. 2025;22(12):992–6. doi:10.26599/1671-5411.2025.12.008
4. Jiang R, Gong M. Misdiagnosed intravenous leiomyomatosis. Eur J Vasc Endovasc Surg. 2024;68(6):783. doi:10.1016/j.ejvs.2024.09.027
5. Stone J, Hangge P, Albadawi H, et al. Deep vein thrombosis: pathogenesis, diagnosis, and medical management. Cardiovasc Diagn Ther. 2017;7(S3):S276–S284. doi:10.21037/cdt.2017.09.01
6. Wang J, Hu Q, Bi Z, et al. MR imaging findings of stage I intravenous leiomyomatosis: a retrospective single-center study in 19 cases. Abdom Radiol. 2024;49(2):512–522. doi:10.1007/s00261-023-04132-4
7. Zhao J, Liao J, Fan W, Yu Q, Lei Z. Multimodality imaging applications in the diagnosis of and surgical treatment strategy for intravenous leiomyomatosis: a case description and literature analysis. Quant Imaging Med Surg. 2024;14(6):4281–4287. doi:10.21037/qims-23-1772
8. Zhou X, Qi X, Zhao X, Yang F. Update on clinical characteristics and molecular insights for uterine intravenous leiomyomatosis (Review). Oncol Lett. 2024;27(1).
9. Momeni-Boroujeni A, Nucci MR, Chapel DB. Risk stratification of uterine smooth muscle tumors: the role of morphology, immunohistochemistry, and molecular testing. Adv Anat Pathol. 2025;32(1):44–56. doi:10.1097/PAP.0000000000000478
10. Yin S, Shi P, Han J, et al. Pathological and molecular insights into intravenous leiomyomatosis: an integrative multi-omics study. J Transl Med. 2025;23(1). doi:10.1186/s12967-024-05919-9
11. Gan J, Ma X, Shao J, Wang J, Cao D. Intravenous leiomyomatosis presenting as Budd–Chiari syndrome: a case report and literature review. Orphanet J Rare Dis. 2025;20(1). doi:10.1186/s13023-025-03556-z
12. Wen Y, Ma G, Miao Q, et al. The largest single-center report on intravenous leiomyomatosis and development of a classification to guide surgical management. J Vasc Surg Venous Lymph Disord. 2025;13(1):101989. doi:10.1016/j.jvsv.2024.101989
13. Lim WH, Lamaro VP, Sivagnanam V. Manifestation and management of intravenous leiomyomatosis: a systematic review of the literature. Surg Oncol. 2022;45:101879. doi:10.1016/j.suronc.2022.101879
14. Gu Z, Shen J, Lu S, Chen J, Guan R. Multidisciplinary management of intravenous leiomyomatosis extending to the inferior vena cava and heart: a case series. BMC Cardiovasc Disord. 2025;25(1):847. doi:10.1186/s12872-025-05320-4
15. Group of Gynecologic Oncology, Chinese Medical Doctor Association. Chinese expert consensus on clinical diagnosis and treatment of pelvic intravenous leiomyomatosis. Chin J Obstet Gynecol. 2023;58(4):252–258. (in Chinese). doi:10.3760/cma.j.cn112141-20230104-00005
16. Zhang T, Zhou J, Li H, Zhang X, Chang L. Ultrasound diagnostic value and clinical analysis of 61 uterine intravenous leiomyomatosis cases. Quant Imaging Med Surg. 2025;15(4):3347–3359. doi:10.21037/qims-24-1724
17. He G, Yao T, Zhao L, et al. Surgical strategy for intravenous leiomyomatosis spreading from uterine to the right atrium presenting with recurrent syncope. J Cardiothorac Surg. 2024;19(1). doi:10.1186/s13019-024-02681-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Uterine Intravenous Leiomyomatosis with Internal Iliac Artery Involvement
Dang M, Cai S, Yao J, Zhang B, Zhang L, Xu W, Huang P
International Journal of Women's Health 2025, 17:3699-3706
Published Date: 15 October 2025
Amniotic Fluid Embolism Complicated with Hepatic Rupture: A Case Report
Xu Y, Zhang Y, Zheng J, Chen C, Xu X, Yan J
International Journal of Women's Health 2025, 17:3929-3935
Published Date: 29 October 2025
Multidisciplinary Recommendations for the Use of Chest CT and Bronchial Biopsy in Severe Asthma: An Expert Consensus Based on Real-World Experience
Garcia-Rivero JL, Peña E, González-Piñeiro A, Mosteiro Añón M, Cosio BG
Journal of Asthma and Allergy 2026, 19:604260
Published Date: 23 May 2026