Back to Journals » Clinical Interventions in Aging » Volume 20
Multidimensional Analysis of Frailty and Its Influencing Factors in Hospitalized Elderly Stroke Patients
Authors Zhou H, Han Y, Xie D, Zheng K, Zhu H ![]() , Zhou Z, Ji Y
, Zhou Z, Ji Y
Received 13 June 2025
Accepted for publication 3 October 2025
Published 11 October 2025 Volume 2025:20 Pages 1741—1755
DOI https://doi.org/10.2147/CIA.S546975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Huimin Zhou,* Yan Han,* Dan Xie,* Kai Zheng, Haohao Zhu, Zhenhe Zhou, Yingying Ji
Rehabilitation Department, The Affiliated Mental Health Center of Jiangnan University, Wuxi Central Rehabilitation Hospital, Wuxi, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhenhe Zhou, Rehabilitation Department, The Affiliated Mental Health Center of Jiangnan University, Wuxi Central Rehabilitation Hospital, Wuxi, Jiangsu, People’s Republic of China, Email [email protected] Yingying Ji, Rehabilitation Department, The Affiliated Mental Health Center of Jiangnan University, Wuxi Central Rehabilitation Hospital, Wuxi, Jiangsu, People’s Republic of China, Email [email protected]
Background: Frailty is a common geriatric syndrome, and its occurrence in elderly stroke patients may further worsen clinical outcomes, yet the influencing factors and potential causal relationship remain unclear.
Objective: This study aimed to identify the influencing factors of frailty in elderly hospitalized stroke patients and to analyze the potential causal relationship between stroke and frailty.
Methods: A multicenter cross-sectional survey including 210 elderly stroke patients was conducted, and bidirectional Mendelian randomization analysis was applied to examine the causal relationship between stroke and frailty. Univariate and multivariate logistic regression analyses were used to explore the impact of physiological, psychological, and clinical symptom factors on frailty.
Results: The frailty index was positively correlated with stroke, and Mendelian randomization confirmed a bidirectional causal relationship. Univariate analysis showed significant associations between frailty and diabetes, lesion site, lesion location, and brain atrophy. Multivariate logistic regression further identified Fugl-Meyer score, Berg score, and MoCA score as independent risk factors for frailty in elderly hospitalized stroke patients.
Conclusion: Frailty is strongly associated with stroke, and elderly stroke patients face an increased risk of frailty during hospitalization. These findings provide a basis for early identification of high-risk patients and the development of targeted intervention strategies in clinical practice, with important implications for stroke rehabilitation and elderly care.
Keywords: frailty, stroke, elderly, Mendelian randomization, influencing factors
Introduction
As the global population continues to age, stroke has emerged as a prevalent and significant health concern among elderly people. According to data from the Global Burden of Disease Study (GBD),1 the incidence of stroke in China is increasing, positioning it as the leading cause of premature mortality within the country. Stroke accounts for a substantial number of disability-adjusted life years (DALYs) and is the primary contributor to death and disability among adults in China, characterized by high rates of morbidity, disability, mortality, and recurrence and a considerable economic burden. The consequences of stroke extend beyond immediate physical dysfunction and cognitive decline; it is also intricately linked to the multifaceted geriatric syndrome of frailty. Fried initially defined frailty as a non-specific clinical condition resulting from a decline in physiological reserves in older adults, which leads to increased vulnerability and diminished resilience to stressors.2 Frailty has a significant effect on the rehabilitation process, quality of life and long-term prognosis of elderly stroke patients. An intermediary analysis by Madoka Noguchi et al revealed that frailty is independently related to poor functional outcomes after stroke.3 A systematic review by Bao et al confirmed that frailty is an important predictor of poor functional prognosis and mortality in patients with acute ischemic stroke undergoing endovascular treatment.4 Furthermore, frailty is associated with a high risk of readmission within 90 days in stroke patients aged 18 and over,5 poorer cognitive function in adults aged 55 and above,6 and severe disability within one year in elderly patients with acute cerebral infarction.7 A multicentre prospective cohort study involving 677 patients found that baseline frailty in adult stroke patients at discharge was significantly associated with unplanned readmission, major adverse cardiac and cerebrovascular events, and post-stroke disability at three months.8 Consequently, a thorough investigation into the factors influencing frailty in elderly stroke patients has significant clinical and public health implications, particularly for the development of personalized care strategies and the improvement of patient outcomes.
In recent years, frailty has emerged as a significant area of research within geriatric medicine, particularly concerning its relationship with stroke care in the elderly population. One study noted that frailty is an important risk factor for stroke,9 highlighting a bidirectional association between the two conditions.10 Predominantly, international researchers have employed cohort studies to investigate the impact of frailty on the prognosis of stroke patients. Findings indicate a substantial correlation between frailty and adverse functional outcomes, as well as increased mortality rates among stroke patients.11 At present, research on the influencing factors of frailty in elderly individuals, including age, sex, chronic diseases, nutritional status, physical activity level and other aspects, is relatively extensive.12 However, research specifically targeting elderly hospitalized stroke patients remains limited, despite a growing interest in this demographic. Most existing studies tend to focus on singular dimensions—either physiological or psychological factors—while neglecting a comprehensive analysis that incorporates multiple dimensions and extensive multicenter research. Furthermore, the prevalence and influencing factors of frailty in elderly stroke patients vary across studies, often due to differences in selected populations or methodologies, thereby underscoring the heterogeneity present in study designs. A meta-analysis encompassing 12 cohort studies and 2 cross-sectional studies revealed that the prevalence of frailty among patients experiencing acute stroke ranges from 2.2% to 54%.13 Additionally, a systematic review and meta-analysis conducted by Huang et al indicated that the prevalence of frailty in stroke patients varies between 11.6% and 68.4%, with identified risk factors including female sex, advanced age, diabetes, hyperlipidemia, atrial fibrillation, and the National Institutes of Health Stroke Scale (NIHSS) admission score.14 Research by Zhang Kaili and others shows that the prevalence of frailty among middle-aged and elderly stroke patients is 54.7%. Factors influencing frailty in this population include advanced age, low educational level, severe stroke, concurrent anxiety and depression, and low scores in activities of daily living.15 Recently, Mendelian randomization (MR) has gained traction as a methodological approach in genetic epidemiology, utilizing genetic variation as an instrumental variable to elucidate direct causal relationships between exposure and outcome factors, thereby mitigating confounding influences. Moreover, the results of Mendelian randomization (MR) can help inform personalized early intervention and lifestyle recommendations. For instance, Song J et al, through MR analysis, identified a causal relationship between sarcopenia-related traits (appendicular lean mass [ALM] and hand grip strength [HGS]) and ischemic stroke. They found that higher ALM has a protective effect against ischemic stroke. Consequently, ALM could be incorporated into risk assessment metrics for ischemic stroke, guiding individuals to maintain sufficient muscle mass.16 In light of the aforementioned research landscape, this study aims to perform a bidirectional Mendelian randomization analysis, utilizing stroke and frailty indices as exposure and outcome variables, respectively. The study will also gather cross-sectional data to conduct a thorough and systematic analysis of the factors influencing frailty in elderly hospitalized stroke patients, evaluating these factors across multiple dimensions, including physiological and psychological states, as well as clinical symptom scores. This research aims to assist clinical practitioners in the early identification of high-risk frail patients, facilitating the development of personalized intervention strategies to enhance rehabilitation outcomes and quality of life. Additionally, it aims to alleviate the medical burden on society and families while contributing valuable insights and data to the discourse on frailty in the context of elderly care and stroke rehabilitation.
Materials and Methods
Study Design
This research employed a combination of cross-sectional studies and Mendelian randomization analysis to examine elderly patients hospitalized due to stroke. The Mendelian randomization approach uses genetic variation as an instrumental variable, thereby enabling a precise inference of the causal relationships between exposure factors and outcome variables, which significantly enhances the robustness of scientific inquiry. In the context of the Mendelian randomization analysis, genetic variation served as an instrumental variable to facilitate a bidirectional exploration of the relationship between stroke and the frailty index, with the objective of elucidating the causal dynamics between these two variables. Concurrently, clinical sample data were collected to gain a more comprehensive understanding of the frailty status of elderly stroke patients and the independent factors influencing frailty status.
Participants
Genetic data pertaining to exposure and outcome phenotypes utilized in the Mendelian randomization analysis were sourced from the Medical Research Council-Integrative Epidemiology Unit (MRC-IEU) and pertain to European populations. The genetic data for the Mendelian randomization study, as detailed in Table 1, were derived from a comprehensive genome-wide association study (GWAS) meta-analysis employing the GWAS pipeline, which incorporates Phesant-derived variables from the UK Biobank. All summary statistics can be obtained directly from the database (https://opengwas.io/datasets/). Information regarding the frailty index was collected from a study involving 175,226 European participants, whereas self-reported stroke data were obtained from a separate analysis encompassing 446,696 European participants, which included 40,585 cases and 406,111 controls. This multicenter cross-sectional study ultimately included 210 patients diagnosed with stroke between January 2023 and August 2024. Data were collected from all 210 stroke patients, and after excluding 7 cases with incomplete data, a total of 203 cases were analyzed. These data were obtained from the Traditional Chinese Medicine Rehabilitation Department and Geriatric Rehabilitation Department of Wuxi Central Rehabilitation Hospital, the Second Neurology Department of the North Campus of the Affiliated Hospital of Jiangnan University, and the Stroke Center 7B Ward of Wuxi First People’s Hospital. Among the cross-sectional study sample, 59.1% (n=120) of the participants were male, and 40.9% (n=83) were female. The mean age of the participants was 73.55 years (±7.02), with an age range of 60--90 years. The inclusion criteria for the study were as follows: 1) fulfillment of the 4th National Diagnostic Criteria for Cerebrovascular Disease and a stroke diagnosis confirmed by cranial CT or MRI; 2) age of 60 years or older; and 3) maintained consciousness. The exclusion criteria included the following: 1) a history of mental illness; 2) the presence of significant medical conditions such as organ failure or cancer; and 3) severe cognitive impairment that would hinder cooperation with the investigation.
 |
Table 1 The Genetic Data for the Mendelian Randomization Study |
The sample size was determined via the logistic independent variable event number (EPV) method, with a threshold of EPV ≥ 5. Taking into account a 10% rate of invalid samples, the minimum sample size was ultimately calculated to be 164 cases, on the basis of a frailty incidence of 74.4% among elderly stroke patients.17
This study was approved by the Ethics Committee of Wuxi Mental Health Centre, with grant number WXMHCIRB2021LLKY145, and informed consent was secured from all participants involved in the study. This study complies with the ethical guidelines of the Declaration of Helsinki.
Survey Tools
Instrumental Variable Selection
The selection criteria for single nucleotide polymorphisms (SNPs) associated with exposure in the GWAS summary data were as follows: 1) a threshold for genome-wide significance was set at P < 5 × 10−8; 2) SNPs exhibiting linkage disequilibrium were excluded to ensure the independence of the selected SNPs (r² < 0.01, with a window size of 5000 KB); and 3) relevant correlation data were included in the GWAS summary results. To evaluate the potential for weak instrumental variable (IV) bias among the selected IVs, the F statistic was calculated. An F value exceeding 10 suggests the absence of weak IV bias, thereby reinforcing the validity of the association hypothesis. The F statistic was computed via the following formula: [(N-K-1)/K] × [R²/(1-R²)], where N denotes the number of samples for the exposure factor, K represents the number of IVs, and R² indicates the proportion of variance in the exposure factor that is accounted for by the IV.
Questionnaire
The Fugl-Meyer Motor Function Scale18 has a total score of 100 (upper limbs: 66 points; lower limbs: 34 points). The higher the score is, the better the motor function. Severe motor impairment is scored as less than 50 points, obvious motor impairment is scored as 50–84 points, moderate motor impairment is scored as 85–95 points, and mild motor impairment is scored as 96–99 points.
The Berg balance scale (BBS), established in 1989, serves as a measure of balance capabilities in the elderly population. This scale includes 14 items, each scored from 0 to 4, resulting in a cumulative score that ranges from 0 to 56. A higher total score correlates with improved balance.19
The modified Barthel Index (MBI) scale20 has a maximum score of 100, with higher scores indicating better self-care ability. A score of 60 or higher indicates basic self-care, 41–59 indicates moderate functional impairment and the need for assistance, 21–40 indicates moderate functional impairment and obvious dependence, and 20 or lower indicates complete dependence.
The Mini-Mental State Examination (MMSE) was developed by Folstein in the United States in 1975. It includes 10 items, including time and place orientation, immediate memory, attention and calculation, recall, naming, repetition, level 3 instruction, reading comprehension, writing and tracing.21 The full score of the MMSE is 30 points, and the critical value is 24. The lower the score is, the worse the patient’s cognitive function.22
The Montreal Cognitive Assessment (MoCA) scale is designed to yield a maximum score of 30 points and comprises 12 individual tests that assess seven cognitive domains: visual-spatial and executive function, attention, calculation, language, abstract thinking, memory, and orientation. A higher total score reflects superior cognitive functioning, whereas a score of less than 26 is indicative of cognitive impairment.23
The Hamilton Anxiety Scale (HAMA), developed by Hamilton in 1959, is recognized as one of the earliest and most widely utilized assessment tools in psychiatric settings. This scale comprises 14 items, each rated on a scale from 0 to 4 points. A cumulative score of 29 or higher suggests the presence of severe anxiety, while scores of 21 or higher indicate significant anxiety, scores of 14 or higher reflect certain anxiety, scores exceeding 7 suggest possible anxiety, and scores below 7 denote the absence of anxiety symptoms.24
The Hamilton Depression Scale (HAMD),25 also created by Hamilton in 1960, is the predominant instrument for the clinical evaluation of depression. This scale encompasses various items that assess emotional, cognitive, and somatic dimensions, primarily relying on self-reported data from patients.
Fried frailty phenotype (FFP) scale was proposed by Fried et al26 in 2001 and consists of five criteria: unintentional weight loss, fatigue, reduced physical activity, slower walking speed, and diminished grip strength. Each criterion contributes one point to the total score, which can range from 0 to 5. A score of 0 indicates no frailty, scores of 1–2 suggest a pre-frailty condition, and scores of 3 or higher are indicative of frailty.
Data Collection
This study collected patients’ basic demographic information, disease-related data, and clinical function assessment data after admission. Basic demographic data included sex, age, smoking history, drinking history, hypertension history, diabetes history, number of chronic diseases, baseline heart rate, clinical diagnosis, lesion site, specific location of lesions, brain atrophy, and white matter degeneration.
The personal smoking history was as follows: smoking history, an average of not less than 10 cigarettes per day for more than 5 years; drinking, men drinking no less than 25 grams per day and women drinking more than 12.5 grams per day for 5 years or more;27 history of hypertension, systolic blood pressure not less than 140 mmHg and/or diastolic blood pressure not less than 90 mmHg; history of hypertension or use of antihypertensive drugs, one of which is met;28 history of diabetes, fasting blood glucose not less than 7.0 mmol/L; 2-hour postprandial blood glucose not less than 11.1 mmol/L; glycosylated hemoglobin level not less than 6.5%; history of diabetes or use of hypoglycemic drugs, one of these conditions is met;29 and the number (type) of chronic diseases. Imaging data for the patients were extracted from electronic medical records to ascertain the etiology of the stroke, the location of the lesions, and the specific sites of involvement. The classification of the specific stroke sites was based on the vascular supply territories of the carotid and vertebral artery systems, which included the basal ganglia, frontal lobe, parietal lobe, temporal lobe, cerebellum, or brainstem. Furthermore, the diagnosis and documentation of cerebral cortical atrophy and white matter degeneration were conducted. Stroke patients who fulfilled the established criteria were assessed via a questionnaire within one week of admission.
The questionnaires were evaluated by postgraduate students of nursing or rehabilitation therapists who had received unified training to ensure consistency among evaluators. Demographic data and disease-related information were cross-verified through electronic medical records and conversations with patients. Lesion sites, brain atrophy, and white matter degeneration were evaluated by two doctors based on the CT/MRI reports of the subjects. In case of disagreement, a senior and more experienced physician would make the final decision. All data were double-checked by two people before being entered into an Excel spreadsheet to ensure accuracy.
Statistical Analysis
MR studies primarily utilize inverse variance weighted (IVW) analysis as the principal method for MR analysis. To increase the robustness of the primary analysis, supplementary analyses were conducted employing the weighted median, weighted mode, and MR Egger methods. The MR Egger method specifically serves to evaluate horizontal pleiotropy, with a significance threshold established at P < 0.05.30 In instances where evidence of horizontal pleiotropy is identified (ie, an MR Egger intercept of less than 0.05), the MR Egger method is favored as the primary analytical approach. Conversely, if no pleiotropic effects are detected (ie, if the P value of the MR Egger intercept exceeds 0.05), the IVW method is adopted as the primary analysis technique. If the IVW method yields a significant result (P < 0.05), this finding is deemed positive, provided that the direction of the β values across the various methods is consistent, even if the other methods do not indicate significance and no pleiotropy is observed.31 The heterogeneity of the IVW and MR Egger regression methods was assessed via the Q test; a P value of less than 0.05 indicates significant heterogeneity, indicating the use of a random effects model (REM) for result evaluation, whereas a P value greater than 0.05 suggests no heterogeneity, suggesting the application of a fixed effects model (FEM). The sensitivity of the Mendelian randomization analysis was evaluated through leave-one-out analysis, which involves sequentially excluding a specific single-nucleotide polymorphism (SNP), recalculating the MR analysis effect of the remaining SNPs as instrumental variables, and observing any resultant changes in the findings. Quantitative data from cross-sectional studies that conformed to a normal distribution are expressed as the mean ± standard deviation (x ± s). If the data did not conform to a normal distribution, non-parametric tests were used, and categorical data were expressed as composition ratios. Quantitative data and categorical data were compared via t tests or Mann‒Whitney U-tests and chi‒square tests, respectively. Independent variables with statistical significance in the single-factor analysis were further used to analyze the factors affecting post-stroke frailty using multi-factor logistic regression model. All the statistical analyses were executed via SPSS version 27.0, with the significance level set at P < 0.05.
Results
Mendelian Randomization
Causal Relationship Between the Frailty Index and Stroke
To investigate the causal relationship between stroke and the frailty index, we employed MR analysis, designating the frailty index as the exposure variable and stroke as the outcome variable. After excluding abnormal IVs (Table 2), we identified 14 relevant SNPs within the stroke database. The F statistic for each IV exceeded 10, suggesting the absence of weak instrument bias.
 |
Table 2 Causal Relationship Between the Frailty Index and Stroke |
Causal effects were analyzed via MR‒Egger, weighted median, IVW and weighted methods. The frailty index was positively correlated with stroke [IVW method: OR=1.360, 95% CI: 1.006--1.838, P=0.046; weighted median method: OR=1.758, 95% CI: 0.811--3.808, P=0.176]. Although the P values of MR‒Egger and weighted methods were greater than 0.05, the results of the IVW method and weighted median method were consistent with those of the other analysis methods (Figure 1), which further verified the reliability of the results. Additionally, a leave-one-out analysis was conducted, wherein each SNP was systematically excluded from the analysis. This examination revealed that no individual SNP significantly influenced the stability of the results. Consequently, the findings from the two-sample Mendelian randomization analysis concerning the relationship between the frailty index and stroke are deemed stable and reliable (Figure 2A and B).
 |
Figure 1 Results of the correlation analysis between the frailty index and stroke. |
 |
Figure 2 (A and B) Causal relationship between the frailty index and stroke. (A) Forest plot of the causal relationship between IVs related to the frailty index and stroke. The red line represents the MR‒Egger test and IVW MR results. (B) Scatter plot of the causal relationship between the frailty index and stroke. |
Causal Relationship Between Stroke and Frailty Index
To examine the causal relationship between stroke and the frailty index, an MR analysis was conducted, with stroke serving as the exposure variable and the frailty index as the outcome variable. Instances of abnormal IVs were excluded from the analysis, resulting in the identification of 8 stroke-related SNPs from the study population (Table 3). The F statistic for each IV exceeded 10, suggesting the absence of weak instrument bias.
 |
Table 3 Causal Relationship Between Stroke and the Frailty Index |
Causal effects were analyzed via MR‒Egger, weighted median, inverse variance weighting (IVW) and weighted modes. Stroke was positively correlated with the frailty index [IVW method: OR=1.124, 95% CI: 1.075--1.175, P=3.02E-07; weighted median method: OR=1.075, 95% CI: 0.994--1.162, P= 1.14E-01]. Although the P values for MR‒Egger and weighted mode exceeded 0.05, the directional outcomes of IVW and the weighted median were consistent with those obtained from the other analytical methods (Figure 3), suggesting the reliability of the findings. Furthermore, a leave-one-out analysis was conducted, systematically excluding each SNP from the analysis. The results indicated that no individual SNP significantly influenced the stability of the overall findings. Consequently, the outcomes of the two-sample Mendelian randomization analysis examining the relationship between stroke and the frailty index are deemed stable and reliable (Figure 4A and B).
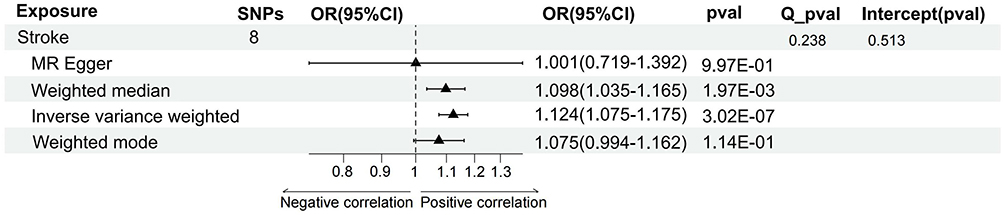 |
Figure 3 Results of the correlation analysis between the stroke and frailty index. |
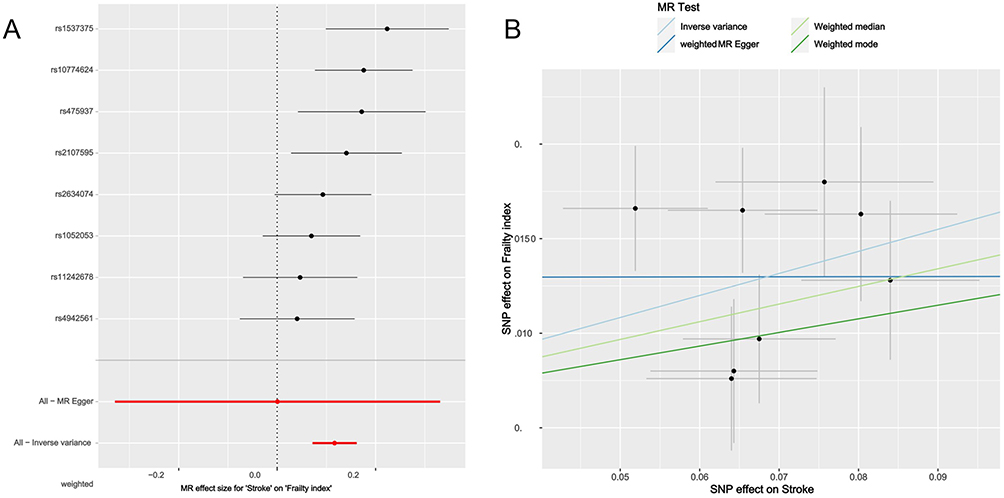 |
Figure 4 (A and B) Causal relationship between stroke and the frailty index. (A) Forest plot of the causal relationship between IVs related to stroke and the frailty index. The red line represents the MR‒Egger test and IVW MR results. (B) Scatter plot of the causal relationship between stroke and the frailty index. |
Factors Influencing Frailty in Stroke Patients
A total of 210 patients participated in this study. Following the exclusion of 7 patients due to incomplete data, the analysis was conducted on the remaining 134 patients, of whom 66% were diagnosed with frailty, whereas 34% (69 patients) were classified as non-frail. Consequently, the incidence of frailty observed in this study was 66%. There are notable disparities in both basic and disease-related information, specifically concerning diabetes (χ2 = 3.865, P < 0.05), lesion location (χ2 = 24.576, P < 0.05), the precise location of the lesion (χ2 = 17.107, P < 0.05), and brain atrophy (χ2 = 7.081, P < 0.05). Furthermore, the Fugl-Meyer score (z = −9.866, P < 0.05), BBS score (z = −6.168, P < 0.05), and MBI score (z = −10.166, P < 0.05) also exhibited significant differences. Additionally, the HAMA score (z = −4.082, P < 0.05), HAMD score (z = −4.176, P < 0.05), MMSE score (z = −6.168, P < 0.05), and MoCA score (t = −9.237, P < 0.05) were significantly different. For detailed results, refer to Tables 4 and 5.
 |
Table 4 Incidence and Influencing Factors of Frailty |
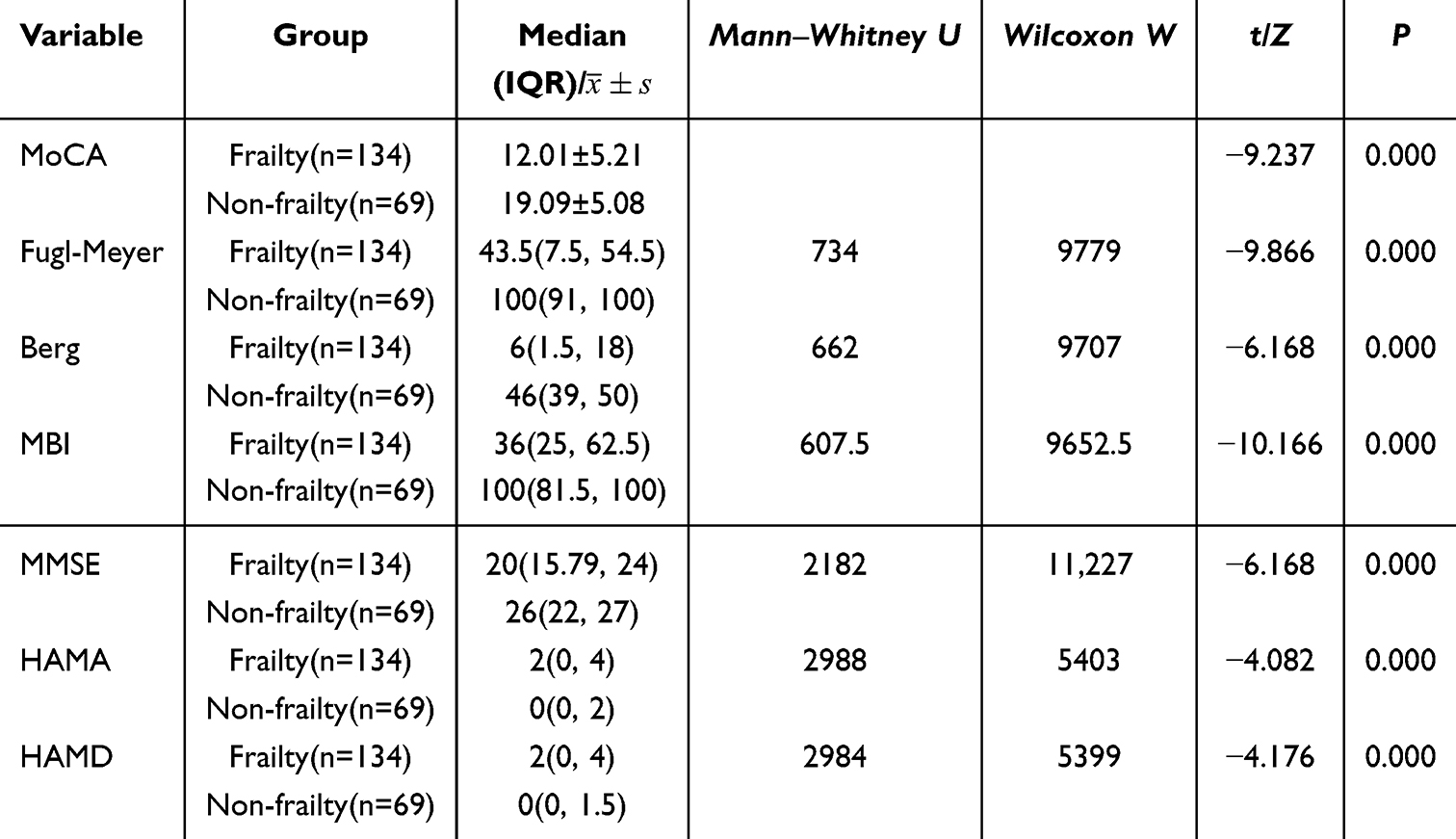 |
Table 5 Influencing Factors of the Clinical Symptoms of Frailty |
Multivariate Logistic Regression Analysis of Factors Influencing Frailty in Stroke Patients
In this study, the development of frailty among elderly stroke patients was designated as the dependent variable. A multivariate logistic regression analysis was conducted, utilizing the statistically significant variables identified in the univariate analysis as independent variables (Table 6). The findings from the multivariate logistic regression analysis indicated that the Fugl-Meyer assessment (OR=1.032, 95% CI: 1.005--1.059), the BBS (OR=1.073, 95% CI: 1.016--1.134), and the MoCA (OR=1.324, 95% CI: 1.071--1.638) were identified as independent risk factors contributing to the frailty of elderly stroke patients (Table 7).
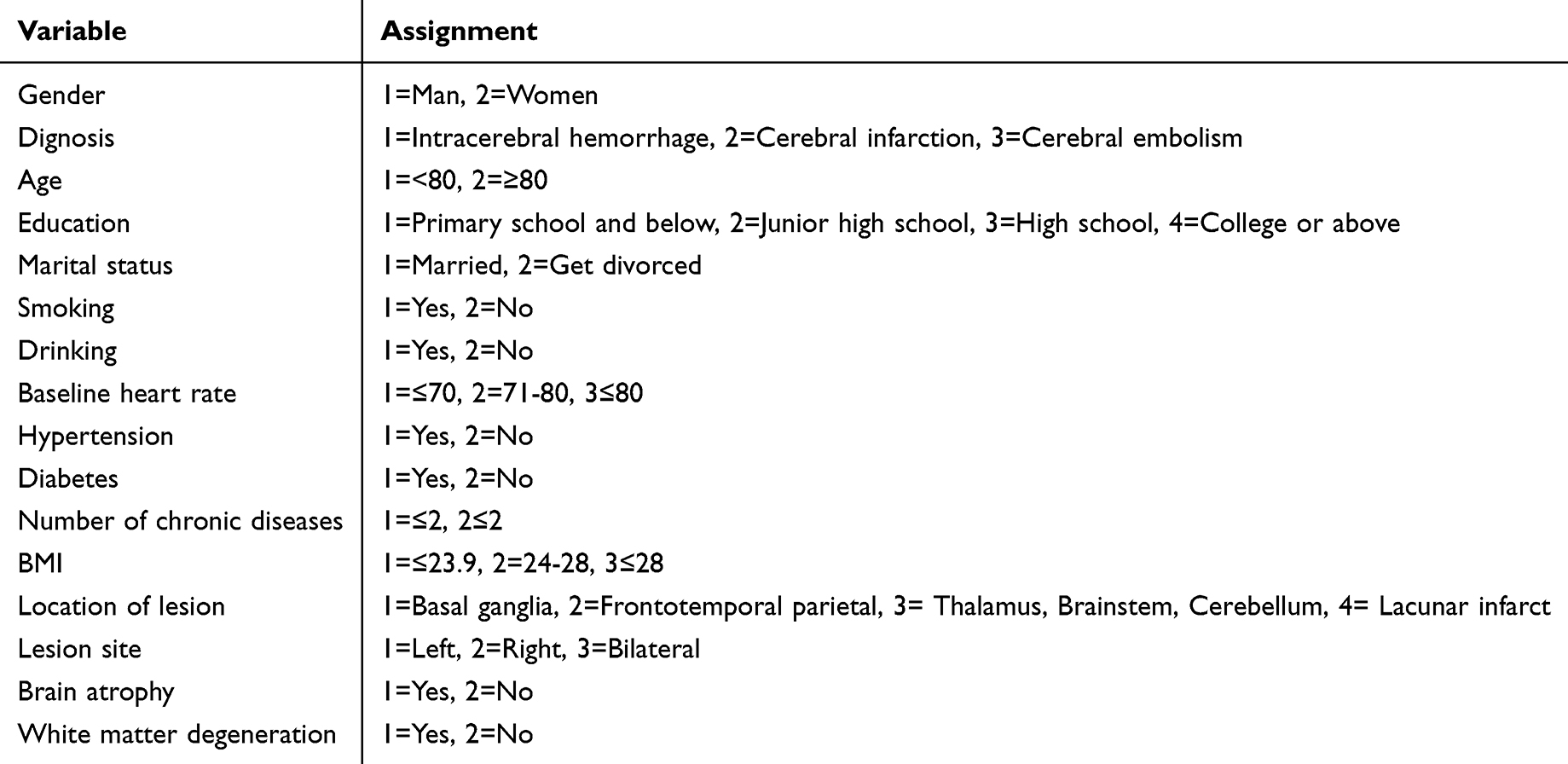 |
Table 6 Variable Assignment |
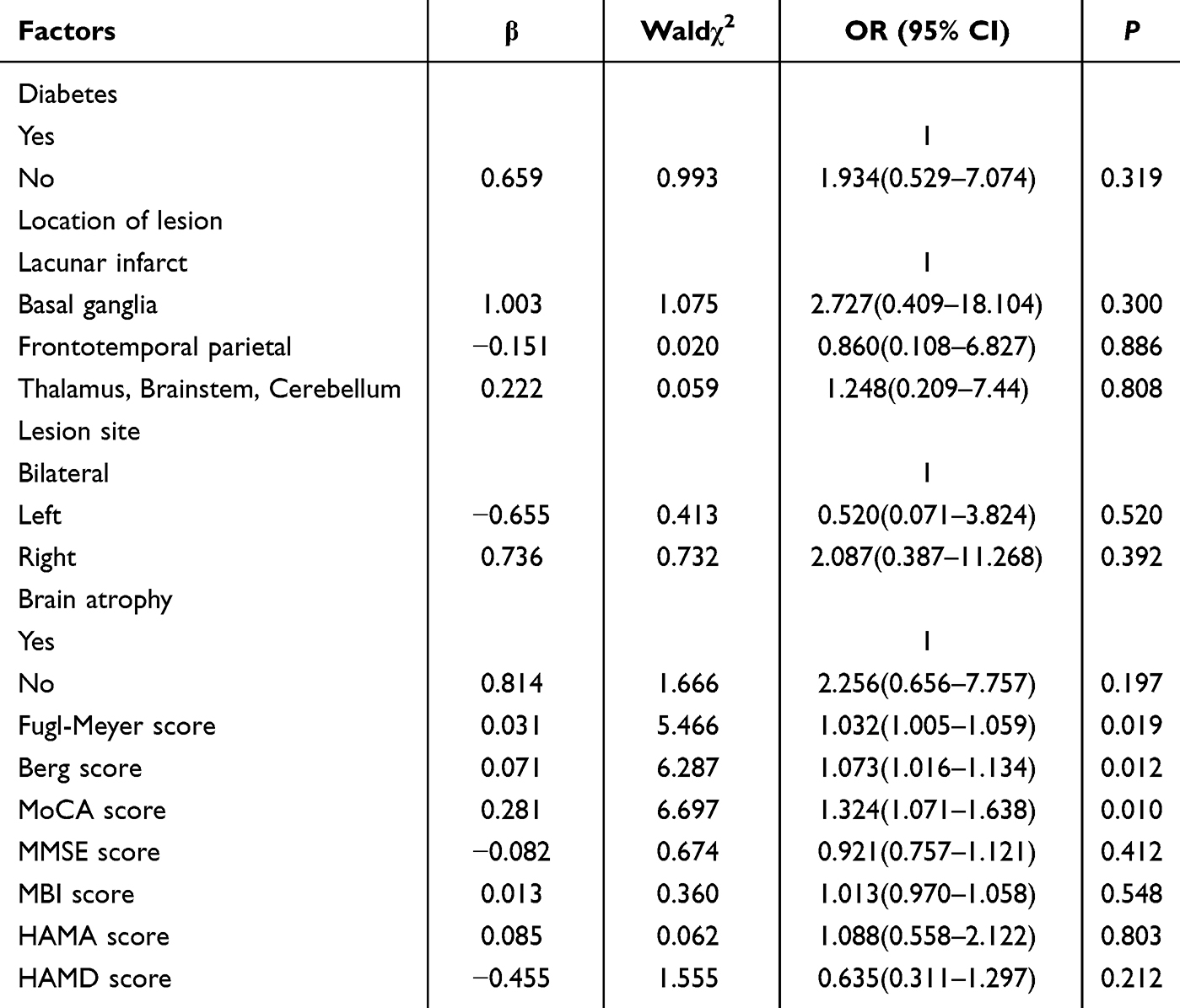 |
Table 7 Multivariate Logistic Regression Analysis of Influencing Factors of Frailty |
Discussion
This research investigated the determinants of frailty among elderly patients hospitalized for stroke via both cross-sectional studies and Mendelian randomization analysis. These findings indicate a positive correlation between the frailty index and stroke incidence, suggesting a bidirectional relationship wherein stroke may contribute to the development of frailty. Additionally, the results from the cross-sectional analysis revealed that the Fugl–Meyer score, BBS score, and MoCA score were independent risk factors for frailty in this population.
Different studies have used various frailty assessment tools (frailty index, frailty phenotype, hospital frailty risk score), resulting in differing identification rates of frailty and varying strengths of association with outcomes within the same population. One study employing the hospital frailty risk score also demonstrated that frailty is associated with an increased risk of any type of stroke, but the effect size and subtype differences were not entirely consistent with those observed in studies using the frailty index.32 Recently, a study using data from the US National Health and Nutrition Examination Survey (NHANES) and the China Health and Retirement Longitudinal Study (CHARLS) to investigate the association between frailty and stroke found that in both populations, higher frailty index scores were associated with a greater likelihood of stroke. Specifically, in NHANES and CHARLS, for every 0.1 unit increase in the frailty index, the odds of stroke increased by 2.90 times and 1.78 times, respectively.33 This is consistent with the findings of this study that the frailty index is positively associated with stroke. This relationship may be attributed to the fact that frailty is associated with diminished physiological reserves and reduced resilience to stress, which in turn compromises the body’s capacity to respond to external stimuli. Additionally, frailty may impair self-regulatory mechanisms, such as the regulation of blood pressure and blood glucose levels, thereby hindering the maintenance of physiological equilibrium in the face of physical or psychological stressors. Consequently, this increased vulnerability may increase the risk of stroke. A study by Masashi Kanai et al reported that the degree of prestroke frailty in elderly patients with acute stroke is significantly related to the severity of stroke.34 A systematic review and meta-analysis by Jing Li et al revealed that frailty is significantly associated with increased mortality and poor functional prognosis in stroke patients.35 At the same time, stroke severity was positively correlated with the frailty index. This may be because the physical damage caused by stroke directly affects an individual’s physiological function, weakens their resistance to external pressure and self-regulation ability, and thus aggravates the frail state. Hassan EB et al36 noted that stroke affects the musculoskeletal system, leading to a rapid decrease in muscle volume, and that there may be continuous muscle atrophy and decreased bone density. Freid proposed that reduced grip strength is one of the signs of frailty, which coincides with muscle loss. In addition, in the study of cognitive dysfunction in stroke patients, interleukin-6, C-reactive protein and tumor necrosis factor inflammatory markers, which are related to decreases in muscle and bone volume, were detected.37 Other studies have shown that the incidence of frailty in stroke patients is twice that in nonstroke patients.38 A cross-sectional survey by Rowan et al39 revealed that approximately 25% of acute stroke patients were frail. Stroke not only increases the risk of frailty but also places a heavy burden on stroke patients. Therefore, clinicians should identify and intervene early to slow disease progression, reduce the burden on families and society, and promote patients’ return to society.
Long-term motor dysfunction after stroke can cause changes in brain structure and functional networks, especially in the motor control areas of the brain, including the prefrontal cortex, basal ganglia, and cerebellum. These changes affect motor function.40 For example, lesions in specific areas of the brain may affect motor, sensory, cognitive and other functions. The Fugl-Meyer score is an important tool for evaluating motor function after stroke. The lower the score is, the more severe the motor dysfunction, which is closely related to the development of frailty.41 Most stroke patients have movement disorders because impaired motor function can lead to muscle atrophy due to disuse and a decrease in muscle mass. Studies have shown that muscle loss is associated with frailty and have listed sarcopenia, neuroendocrine disorders, and cognitive impairment as risk factors for frailty.42 Motor dysfunction can lead to reduced glucose uptake by muscles, a reduction in the number of mitochondria and impaired function, which in turn leads to insufficient energy production. This not only affects the contractile ability of muscles but also induces a series of metabolic disorders, such as increased insulin resistance,43 and insufficient levels of insulin-like growth factor 1 (IGF-1), free testosterone or dihydroepiandrosterone sulfate (DHEAS) can greatly increase the likelihood of frailty.44 Long-term motor impairment can also affect a patient’s mental state, causing them to experience negative emotions such as anxiety, depression, fatigue, and apathy,45 reducing their confidence and enthusiasm for rehabilitation and further aggravating their physical weakness. This study revealed that the BBS score is an independent risk factor for frailty in elderly hospitalized stroke patients. The Berg balance function score reflects a patient’s balance ability. Decreased balance ability may lead to an increased risk of falls. Decreased balance function makes patients prone to balance loss during daily activities such as walking and standing, increasing the risk of falling. Falls may not only cause physical injuries but also cause patients to develop fear, reduce their activity, and aggravate their frailty. A cross-sectional study using the Brief Balance Assessment System Test (BESTest) was performed to examine the relationship between poor balance function and frailty in community-dwelling older women. The results revealed that frail and non-frail older women had significant differences in stability limitations, and APAs (Anti-perturbation movements), sensory orientation and gait stability were significantly different, suggesting that balance function is related to frailty.46 A study by Juan Corral-Pérez et al47 noted that physical activity, a sense of balance, health and daily activities are multidimensionally associated with frailty. Among these factors, single-leg balance is a protective factor for patients with type 2 diabetes and frailty; that is, the better their balance function is, the less likely they are to suffer from frailty. The above indicates that the interplay of post-stroke inflammatory activation, reduced physical activity, sarcopenia, decreased balance, and fear of falling can drive the progression of frailty; therefore, early identification and intervention are necessary. Research evidence shows that resistance training combined with nutritional intervention can improve muscle strength, neurological function, and nutritional status, potentially delaying or reversing the progression of frailty.48
The literature indicates that post-stroke cognitive impairment (PSCI) is closely associated with frailty, and together they exacerbate adverse outcomes. A cross-sectional study pointed out that frailty is common among stroke patients, and the prevalence of cognitive frailty is as high as 37.59%.49 A multicentre prospective cohort study demonstrated that, even after adjusting for cardiovascular risk factors, a significant relationship remains between frailty and poorer cognitive ability following stroke.8 This study also found that cognitive dysfunction in the elderly is a risk factor for frailty. Stroke can lead to brain atrophy and connectivity disorders in the prefrontal cortex, leading to cognitive decline and memory loss.50 Impaired cognitive function not only weakens a patient’s self-management ability and ability to cope with disease and external stimuli but also leads to a lack of cognition of their own condition, thereby increasing their risk of frailty. Studies have shown that compared with non-frail and pre-frail elderly people, frail elderly people tend to be older, have decreased cognitive function, and have depression and anxiety.51 Logistic regression analysis revealed that the severity of frailty was positively correlated with cognitive function and the incidence of depression. Cognitive dysfunction is an independent risk factor for frailty syndrome in elderly individuals.52 Moreover, a cross-sectional study investigating the status of physical frailty and cognitive function in community-dwelling elderly people aged 75 years and above revealed that frailty is also an influencing factor for cognitive impairment.53 These findings suggest that frailty and cognitive impairment are closely related and influence each other.
Strength and Limitations of the Work
This study is subject to several limitations. First, regarding the sample size, while a considerable number of elderly hospitalized stroke patients were included, the overall sample may still be relatively small, predominantly representing the Chinese population. This limitation raises concerns about the generalizability and reliability of the findings to other global contexts. Second, in terms of research design, although a combination of cross-sectional study methods and Mendelian randomization analysis was employed, cross-sectional studies are inherently limited in their ability to capture data at a single time point, thereby failing to establish the temporal nature of causal relationships. Additionally, the reliance on self-reported data from patients may introduce bias.
Recommendations for Further Research
Consequently, future research should aim to expand the sample size to encompass a broader range of ethnic and regional populations, thereby enhancing the generalizability and applicability of the findings. A prospective cohort study design is recommended to monitor and analyze changes in patients’ frailty status over time, which would facilitate a more accurate determination of the causal relationship between stroke and frailty. Furthermore, investigating the interactions between potential factors such as social support and economic status in relation to post-stroke frailty is essential. Finally, intervention studies should be conducted to assess the effectiveness of various strategies aimed at improving post-stroke frailty, thereby providing valuable insights for clinical practice.
Conclusion
This research employed a combination of cross-sectional studies and Mendelian randomization analysis to elucidate the multifaceted factors influencing frailty among elderly patients hospitalized for stroke. These findings suggest a potential bidirectional causal relationship between stroke and frailty. In contrast to conventional research methodologies, Mendelian randomization mitigates the influence of confounding variables, thereby enhancing the reliability of the findings and providing more robust evidence. The identification of independent risk factors establishes a scientific foundation for the early detection and intervention of frailty in clinically high-risk populations. This approach is instrumental in developing personalized intervention strategies, which can enhance rehabilitation outcomes and improve the quality of life for elderly stroke patients while also alleviating the medical burden on families and society. The results of this study indicate that elderly stroke patients are at an elevated risk of frailty during hospitalization and that the application of specific assessment tools can be used to identify these individuals effectively, thereby informing clinical interventions. Consequently, healthcare professionals must conduct comprehensive assessments of elderly stroke patients, paying particular attention to these independent risk factors, to implement appropriate preventive and interventional measures aimed at improving patient prognosis and quality of life.
Data Sharing Statement
The dataset generated and analysed during the current study is available from the corresponding author (Yingying Ji, [email protected]) on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Wuxi Mental Health Centre, with grant number WXMHCIRB2021LLKY145.
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Consent for Publication
The patient understood the report and signed informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work is supported by the Jiangsu Provincial Natural Science Foundation for Youth, Health International (Regional) Exchange Support Program of Jiangsu Province, Jiangsu Provincial Health Commission General Project (H2023040), the Top Talent Support Program for young and middle-aged people of Wuxi Health Committee (HB2023086), the Wuxi Municipal Health Commission (Q202167), and Wuxi Taihu Talent Project (WXTTP2021).
Disclosure
The authors declare no conflict of interest.
References
1. Wei Y, Cao YP, Yang XL, et al. Frailty syndrome and its influencing factors in elderly inpatients. Fudan University J Med Sci. 2018;45(4):496–502.
2. Ma Q, Li R, Wang L, et al. Temporal trend and attributable risk factors of stroke burden in China, 1990-2019: an analysis for the global burden of disease study 2019. Lancet Public Health. 2021;6(12):e897–e906. doi:10.1016/S2468-2667(21)00228-0
3. Noguchi M, Kubo H, Kanai M, et al. Relationship between pre-stroke frailty status and short-term functional outcome in older patients with acute stroke-A mediation analysis. Arch Gerontol Geriatr. 2021;94:104370. doi:10.1016/j.archger.2021.104370
4. Bao Q, Huang X, Wu X, et al. Implications of frailty in acute ischemic stroke receiving endovascular treatment: systematic review and meta-analysis. Aging Clin Exp Res. 2023;35(5):969–978. doi:10.1007/s40520-023-02383-1
5. Kilkenny MF, Phan HT, Lindley RI, et al. Utility of the hospital frailty risk score derived from administrative data and the association with stroke outcomes. Stroke. 2021;52(9):2874–2881. doi:10.1161/STROKEAHA.120.033648
6. Vahedi A, Eriksdotter M, Ihle-Hansen H, et al. Cognitive impairment in people with physical frailty using the phenotype model: a systematic review and meta analysis. Int J Geriatr Psychiatry. 2022;37(11). doi:10.1002/gps.5822
7. Yang F, Li N, Yang L, et al. Association of pre-stroke frailty with prognosis of elderly patients with acute cerebral infarction: a cohort study. Front Neurol. 2022;13:855532. doi:10.3389/fneur.2022.855532
8. He H, Liu M, Li L, et al. The impact of frailty on short-term prognosis in discharged adult stroke patients: a multicenter prospective cohort study. Int J Nurs Stud. 2024;154:104735. doi:10.1016/j.ijnurstu.2024.104735
9. Yang JJ, Li F, Liu GW, et al. Research progress on frailty assessment in stroke patients. Chin Nurs Res. 2023;37(21):3878–3885.
10. Hoogendijk EO, Afilalo J, Ensrud KE, et al. Frailty: implications for clinical practice and public health. Lancet. 2019;394(10206):1365–1375. doi:10.1016/S0140-6736(19)31786-6
11. Huang YN, Wang XY, Chen YR, et al. Research progress on frailty in stroke patients. Chin Nurs Manage. 2023;23(2):282–286.
12. Wang X, Hu J, Wu D. Risk factors for frailty in older adults. Medicine. 2022;101(34):e30169. doi:10.1097/MD.0000000000030169
13. Burton JK, Stewart J, Blair M, et al. Prevalence and implications of frailty in acute stroke: systematic review & meta-analysis. Age Ageing. 2022;51(3). doi:10.1093/ageing/afac064
14. Huang YN, Yan FH, Wang XY, et al. Prevalence and risk factors of frailty in stroke patients: a meta-analysis and systematic review. J Nutr Health Aging. 2023;27(2):96–102. doi:10.1007/s12603-023-1879-z
15. Zhang KL, Xue R. Multidimensional frailty status and influencing factors in middle-aged and elderly stroke patients. Chinese J Geriatric Care Med. 2025;23(3):82–87.
16. Song J, Zhou D, Li J, et al. The causal relationship between sarcopenia-related traits and ischemic stroke: insights from univariable and multivariable Mendelian randomization analyses. CNS Neurosci Ther. 2024;30(5):e14759. doi:10.1111/cns.14759
17. Zhang XY, Zhang L, Sui RB. Construction of a frailty prediction model for elderly stroke patients based on Logistic regression and artificial neural network. Military Nursing. 2023;40(2):10–14,9.
18. Chen RQ, Wu JX, Shen XS. Study on the minimal clinically important difference of the Chinese version of Fugl-Meyer motor function assessment scale. Acta Universitatis Med Anhui. 2015;50(4):519–522.
19. Downs S. The berg balance scale. J Physiother. 2015;61(1):46. doi:10.1016/j.jphys.2014.10.002
20. Sun Y, Sun Y, Shi JJ. Development of the modified extended Barthel index and its reliability and validity in stroke patients. Chin J Phys Med Rehabil. 2024;46(9):769–775.
21. Folstein MF, Folstein SE, Mchugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
22. Creavin ST, Wisniewski S, Noel-Storr AH, et al. Mini-mental state examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst Rev. 2016;2016(1):Cd011145. doi:10.1002/14651858.CD011145.pub2
23. Wu C, Dagg P, Molgat C. A pilot study to measure cognitive impairment in patients with severe schizophrenia with the montreal cognitive assessment (MoCA). Schizophr Res. 2014;158(1–3):151–155. doi:10.1016/j.schres.2014.07.006
24. Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32(1):50–55. doi:10.1111/j.2044-8341.1959.tb00467.x
25. Hamilton M. Development of a rating scale for primary depressive illness. Br J Soc Clin Psychol. 1967;6(4):278–296. doi:10.1111/j.2044-8260.1967.tb00530.x
26. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–56. doi:10.1093/gerona/56.3.M146
27. Chinese Society of Neurology, Chinese Stroke Society. Chinese guidelines for primary prevention of cerebrovascular diseases 2019. Chin J Neurol. 2019;52(9):684–709.
28. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Hypertension. 2018;71(6):1269–1324. doi:10.1161/HYP.0000000000000066
29. De Boer IH, Bangalore S, Benetos A, et al. Diabetes and hypertension: a position statement by the American diabetes association. Diabetes Care. 2017;40(9):1273–1284. doi:10.2337/dci17-0026
30. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
31. Wang S, Zhu H, Pan L, et al. Systemic inflammatory regulators and risk of acute-on-chronic liver failure: a bidirectional mendelian-randomization study. Front Cell Dev Biol. 2023;11:1125233. doi:10.3389/fcell.2023.1125233
32. Renedo D, Acosta JN, Koo AB, et al. Higher hospital frailty risk score is associated with increased risk of stroke: observational and genetic analyses. Stroke. 2023;54(6):1538–1547. doi:10.1161/STROKEAHA.122.041891
33. Zhang X, Yang L, Jin Z, et al. Frailty index is positively associated with stroke risk in nationally representative cohorts from the United States and China. Sci Rep. 2025;15(1):28440. doi:10.1038/s41598-025-14116-7
34. Kanai M, Noguchi M, Kubo H, et al. Pre-stroke frailty and stroke severity in elderly patients with acute stroke. J Stroke Cerebrovasc Dis. 2020;29(12):105346. doi:10.1016/j.jstrokecerebrovasdis.2020.105346
35. Li J, Wan J, Wang H. Role of frailty in predicting outcomes after stroke: a systematic review and meta-analysis. Front Psychiatry. 2024;15:1347476. doi:10.3389/fpsyt.2024.1347476
36. Hassan EB, Phu S, Warburton E, et al. Frailty in Stroke-A narrated review. Life. 2021;11(9). doi:10.3390/life11090891
37. Wang J, Leung KS, Chow SK, et al. Inflammation and age-associated skeletal muscle deterioration (sarcopaenia). J Orthop Translat. 2017;10:94–101. doi:10.1016/j.jot.2017.05.006
38. Palmer K, Vetrano DL, Padua L, et al. Frailty syndromes in persons with cerebrovascular disease: a systematic review and meta-analysis. Front Neurol. 2019;10:1255. doi:10.3389/fneur.2019.01255
39. Taylor-Rowan M, Cuthbertson G, Keir R, et al. The prevalence of frailty among acute stroke patients, and evaluation of method of assessment. Clin Rehabil. 2019;33(10):1688–1696. doi:10.1177/0269215519841417
40. Li YJ, Chen R. Research progress on brain structural and functional network alterations in post-stroke motor dysfunction. Chinese J Cerebrovascular Dis. 2022;16(4):280–283.
41. Lee EY, Na Y, Cho M, et al. Clinical factors associated with balance function in the early subacute phase after stroke. Am J Phys Med Rehabil. 2022;101(3):203–210. doi:10.1097/PHM.0000000000001856
42. Kwak D, Thompson LV. Frailty: past, present, and future? Sports Med Health Sci. 2021;3(1):1–10. doi:10.1016/j.smhs.2020.11.005
43. Richter EA, Hargreaves M. Exercise, GLUT4, and skeletal muscle glucose uptake. Physiol Rev. 2013;93(3):993–1017. doi:10.1152/physrev.00038.2012
44. Angulo J, El Assar M, Álvarez-Bustos A, et al. Physical activity and exercise: strategies to manage frailty. Redox Biol. 2020;35:101513.
45. Kusec A, Milosevich E, Williams OA, et al. Long-term psychological outcomes following stroke: the OX-CHRONIC study. BMC Neurol. 2023;23(1):426. doi:10.1186/s12883-023-03463-5
46. Shinohara T, Saida K, Miyata K, et al. The balance function is associated with frailty in community-dwelling older women. Int J Rehabil Res. 2021;44(1):51–56. doi:10.1097/MRR.0000000000000453
47. Corral-Pérez J, Mier A, Vázquez-Sánchez M, et al. Multidimensional associations of physical performance, balance, wellness and daily activities with frailty in older adults with coexisting frailty and diabetes. J Clin Nurs. 2024.
48. Fan X, Xia Y, Xu S, et al. A narrative review of interventions for post-stroke frailty: current advances and future directions. Front Neurol. 2025;16:1592797. doi:10.3389/fneur.2025.1592797
49. Chen MM, Wang T, You M, et al. Prevalence and influencing factors of cognitive frailty in hospitalized elderly stroke patients. Pract J Cardiac Cerebral Pneumal Vascular Dis 2025;33(10):109–114.
50. Jia W, Zhou Y, Zuo L, et al. Effects of brain atrophy and altered functional connectivity on poststroke cognitive impairment. Brain Res. 2024;1822:148635.
51. Aravindhna K, Morgan K, Mat S, et al. Cognitive frailty and its association with depression, anxiety and stress during the COVID-19 pandemic among older adults in the transforming cognitive frailty into later-life self-sufficiency (AGELESS) study. Psychogeriatrics. 2023;23(6):1071–1082. doi:10.1111/psyg.13031
52. Hu YT, Hu XW. Correlation analysis of frailty syndrome with cognitive impairment and depression in elderly inpatients. Chin J Gen Pract. 2022;20(11):1913–5,86.
53. Han J, Wang JQ, Wang Y, et al. Status and correlation between physical frailty and cognitive function in community-dwelling adults aged 75 and above. Fudan University J Med Sci. 2021;48(4):494–502,544.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Study on the Association Between Dietary Habits, Patterns and Frailty of the Elderly: A Cross-Sectional Survey from Communities in China
Yang J, Wang A, Shang L, Sun C, Jia X, Hou L, Xu R, Wang X
Clinical Interventions in Aging 2022, 17:1527-1538
Published Date: 13 October 2022
Influence of Acupuncture and Other Clinical Factors on the Recovery of Limb Motor Function in Patients After Stroke: A Retrospective Study
Wu B, Ding Y, Peng M, Wang X, Li Y, Cheng X
Journal of Multidisciplinary Healthcare 2023, 16:463-474
Published Date: 21 February 2023
Systemic Inflammation Response Index as a Predictor of Stroke Risk in Elderly Patients with Hypertension: A Cohort Study
Cai X, Song S, Hu J, Wang L, Shen D, Zhu Q, Yang W, Luo Q, Hong J, Li N
Journal of Inflammation Research 2023, 16:4821-4832
Published Date: 24 October 2023
Effects of Anticoagulant Therapy and Frailty in the Elderly Patients with Atrial Fibrillation
Ding J, Sun Y, Zhang K, Huang W, Tang M, Zhang D, Xing Y
Clinical Interventions in Aging 2024, 19:247-254
Published Date: 14 February 2024
Effect of Continuous Positive Airway Pressure on Incident Frailty in Elderly Patients with Obstructive Sleep Apnea: A Study Based on Propensity Score Matching
Xue X, Zhao LB, Zhao Z, Xu WH, Cai WM, Chen SH, Li TJ, Nie TY, Rui D, Qian XS, Liu L
Clinical Interventions in Aging 2024, 19:255-263
Published Date: 16 February 2024