Back to Journals » Journal of Pain Research » Volume 18
Moving Beyond One-Size-Fits-All: Charting a Path to Personalized Nonpharmacological and Noninvasive Chronic Pain Management
Authors Xie Q ![]() , Goldberg SB, Jacobson N, Rakel D, Quanbeck A
, Goldberg SB, Jacobson N, Rakel D, Quanbeck A
Received 17 September 2025
Accepted for publication 18 December 2025
Published 31 December 2025 Volume 2025:18 Pages 7335—7349
DOI https://doi.org/10.2147/JPR.S568016
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ryan D'Souza
Qiang Xie,1– 3 Simon B Goldberg,2,3 Nora Jacobson,4,5 David Rakel,1 Andrew Quanbeck1
1Department of Family Medicine and Community Health, University of Wisconsin – Madison, Madison, WI, USA; 2Department of Counseling Psychology, University of Wisconsin – Madison, Madison, WI, USA; 3Center for Healthy Minds, University of Wisconsin – Madison, Madison, WI, USA; 4Institute for Clinical and Translational Research, University of Wisconsin – Madison, Madison, WI, USA; 5School of Nursing, University of Wisconsin – Madison, Madison, WI, USA
Correspondence: Qiang Xie, Department of Counseling Psychology, University of Wisconsin-Madison, 335 Education Building, 1000 Bascom Mall, Madison, WI, 53706, USA, Tel +1 608-421-9632, Email [email protected]
Abstract: One-size-fits-all opioid treatment for chronic pain may undermine treatment effectiveness and cause adverse effects. We explore personalized nonpharmacological and noninvasive chronic pain treatment as a promising approach to minimize these risks and optimize outcomes for each patient. Our paper introduces the definition of personalized treatment, emphasizes the significance of intervention personalization, and outlines strategies for inter- and intra-patient personalization in chronic pain management. We also discuss empirical studies on personalized chronic pain treatment. Research has shown a variety of strategies for personalizing nonpharmacological and noninvasive chronic pain treatment. These strategies have demonstrated the potential to improve effectiveness. However, many critical scientific questions remain unanswered. To fully harness the potential of personalized nonpharmacological and noninvasive chronic pain treatment, future research should conduct robust clinical trials and meta-analyses comparing personalized and non-personalized chronic pain interventions, examine diverse personalization approaches, incorporate ecological momentary assessment into outcomes assessment, leverage digital technologies, engage patients in treatment design, and assess factors influencing the implementation of personalized chronic pain treatment.
Keywords: chronic pain, persistent pain, personalized intervention, precision medicine, personalized medicine
Introduction
Chronic pain is commonly defined as pain lasting or recurring for more than 3 to 6 months.1 Chronic pain is a pervasive health challenge that detrimentally impacts individuals and society. According to the Centers for Disease Control and Prevention (CDC), approximately one in five adults in the United States (US) experienced chronic pain between 2019 and 2021.2 The significance of chronic pain is multifaceted. Beyond the physical suffering it inflicts, it is associated with diminished quality of life, impaired functioning in work and social life, and emotional distress.3–5 On the societal level, chronic pain imposes substantial economic burdens through healthcare expenses and lost productivity.6 Considering the individual suffering and societal impact inflicted by chronic pain, there is an imperative to develop effective interventions for its management.
Historically, physicians have often used opioid-based treatments as a uniform solution to treat chronic pain.7 Opioids may provide short-term relief for chronic pain.8 However, excessive reliance on opioids has been linked to a spectrum of adverse consequences, including the risk of opioid misuse, dependence, addiction, and overdose deaths.9–11 These outcomes not only exact a devastating toll on individuals and their families but also incur substantial economic costs.12 Furthermore, opioids are not universally effective for all patients experiencing chronic pain. In the case of specific chronic pain conditions, such as neuropathic pain and fibromyalgia, the evidence supporting the benefits of opioids for pain relief is limited,13 and in some instances (eg, osteoarthritis), there is evidence indicating that opioids may actually worsen outcomes.14
In recognition of the negative consequences of such a one-size-fits-all approach, there has been a burgeoning exploration of alternative, evidence-based interventions in chronic pain management.15,16 These interventions, such as psychotherapies and mind-body interventions, seek to help individuals manage chronic pain while mitigating the potential downsides of prolonged opioid use.15,16 In addition, personalized interventions for chronic pain that tailor interventions to the specific needs and characteristics of each patient have emerged as a promising approach to minimizing the risks associated with the over-reliance on opioids and optimizing treatment effects for each patient.17–19 As Margo McCaffery’s definition of pain highlights, “pain is whatever the person who experiences it says it is, existing whenever he/she says it does”. This patient-centered understanding reinforces the importance of individualized approaches in chronic pain management, ensuring that treatment strategies are aligned with the unique experiences and needs of each patient.20
Despite its potential, personalized nonpharmacological and noninvasive chronic pain management, has not yet been fully harnessed in clinical research and practice. A recent meta-analytic review focusing on interdisciplinary multimodal chronic pain treatment studies revealed that 81% of these studies included low levels of tailoring, primarily involving some form of personalized treatment goal setting. However, only 8% of these studies incorporated high-level tailoring, featuring fully individualized intervention strategies and treatment intensity.21 While levels of opioid prescribing have dropped in recent years, opioid prescribing remains prevalent in chronic pain treatment despite the associated health risks.22 This has occurred even though the CDC advised against considering opioids as a first-line therapy and recommended prioritizing non-opioid treatments over opioids for chronic pain.23 This trend reflects a broader issue in healthcare; a study revealed that only 54.9% of American adults receive the recommended healthcare.24 This critical gap in both research and practice, coupled with the potential benefits of highly personalized chronic pain management, necessitates a closer examination of personalized interventions within the context of chronic pain.
The current paper explores personalized nonpharmacological and noninvasive chronic pain management as a means to optimize the efficacy of interventions for chronic pain. We pursue the following three objectives:
- Introduce the conceptual foundations and motivation behind personalized treatment, as well as promising strategies for intervention personalization.
- Discuss chronic pain management as a candidate for a personalized approach, including the importance of personalized chronic pain management and empirical studies on personalized nonpharmacological and noninvasive chronic pain interventions.
- Discuss key future directions for research on personalized nonpharmacological and noninvasive chronic pain management.
Intervention Personalization in Healthcare
What is Intervention Personalization?
Intervention personalization is a broad concept involving processes of tailoring interventions to individuals according to their internal or environmental characteristics, intending to optimize treatment effectiveness, minimize potential adverse effects, or both.25–28 The personalization of interventions can involve both healthcare system-initiated treatment tailoring (eg, clinicians providing interventions based on patients’ unique characteristics) and collaborative treatment customization between patients and the healthcare system. Intervention personalization can be achieved across various aspects, such as the content, frequency, duration, sequencing, and timing of interventions.27,28 Intervention personalization can operate at two levels. At the inter-patient level, each patient receives individualized interventions specifically tailored to their unique characteristics compared to other patients.29 At the intra-patient level, intervention personalization involves the ongoing adjustment of interventions throughout the treatment to meet the evolving needs of each patient.30 In this section, we briefly discuss the conceptualization and history of intervention personalization in physical and mental health, respectively.
Intervention personalization, in the realm of physical health, is often termed personalized medicine. Personalized medicine marks a paradigm shift in healthcare, departing from the traditional one-size-fits-all approach.25 According to the US Food and Drug Administration, personalized medicine recognizes each patient as a unique individual shaped by complex interactions among genetic, environmental, and lifestyle factors.26 Personalized medicine aims to “match the right treatments at the right dosages for each individual patient at the right time”.26 The core element of personalized medicine is to categorize patients with a certain disease into distinct subgroups based on their genetic or biological characteristics and provide tailored medical treatments to these groups to optimize treatment benefits or minimize the adverse effects of treatment.29 The advancement in personalized medicine can be attributed to the breakthroughs in genomics, medical technology, and interdisciplinary research. The turn of the 21st century brought groundbreaking discoveries regarding genetic variants driving disease mechanisms.31 In the contemporary landscape, rapid strides in genomics, coupled with progress in computational biology, medical imaging, and regenerative medicine, have provided the essential tools for robust personalized treatment.29
In contrast to physical health conditions, the genetic or biological mechanisms underlying mental health conditions are often less well-defined; many genetic variations have been found in severe mental illnesses, and genetic variants are non-specifically associated with various mental disorders.32 Consequently, intervention personalization in mental health is less focused on delivering tailored treatments to subgroups with specific genetic or biological traits.27 Rather, it is often a multifaceted process that encompasses the consideration of numerous biopsychosocial factors. Evidence-based practice, proposed by the American Psychological Association, recognizes the significance of tailoring psychological interventions based on individual patient characteristics, culture, and preferences for treatment.33 Evidence-based practice recognizes that patients sharing the same psychiatric diagnosis can exhibit significant variations in etiology, prognosis, and factors sustaining psychopathological conditions. It acknowledges that client characteristics such as comorbidities, personality traits, developmental stage, motivation for change, and personal values can significantly impact treatment outcomes.33
Why is Intervention Personalization Important?
Fostering Patient Engagement
Theoretical frameworks, such as self-determination theory, posit that individuals are more likely to be engaged and motivated when their psychological needs for autonomy (sense of volition and control over one’s own actions), competence (sense of efficacy and mastery), and relatedness (sense of meaningful connections and relationships) are met.34 Intervention personalization, by considering patients’ unique biopsychosocial characteristics, preferences, and cultural backgrounds, may inherently address needs for autonomy and competence and thus foster patients’ engagement in treatment. Specifically, intervention personalization may enhance patients’ autonomy by involving them in decisions about their treatment plans and allowing treatment choices that resonate with their needs and preferences. It may also contribute to enhanced competence by tailoring interventions to individual’s capabilities.
Similarly, perspectives from behavioral economics also support the significance of intervention personalization in fostering patient engagement. Behavioral economic principles posit that human beings have limited cognitive resources and processing capabilities and that decision-making is susceptible to various cognitive biases.35 One widely recognized cognitive bias in behavioral economics is the endowment effect, which suggests that people tend to value things more highly when they perceive them as their own.36 Patients may feel a stronger sense of “ownership” over their treatment by involving them in the process of developing personalized treatment plans. According to the endowment effect, this may increase patients’ treatment engagement, as they see the treatment as something valuable and integral to their well-being.
Research on psychological interventions supports these theoretical perspectives, showing that interventions aligned with participants’ values, preferences, and needs may enhance engagement in the interventions.37,38 A meta-analysis on psychotherapy indicated that patients receiving their preferred treatments were half as likely to drop out relative to those who did not.39 In a randomized controlled trial (RCT) on mobile health treatment for promoting physical activity, personalized goal setting, based on participants’ self-reported capabilities and goals, was found to increase engagement in physical activities compared to the intervention arm with generic goals from national guidelines.40 Conversely, lack of intervention personalization seemed to be a reason for participants to drop out of interventions.41 Intervention personalization may be particularly critical in chronic conditions, where long-term engagement in interventions is vital for the successful management of health concerns.
Optimizing Treatment Effectiveness
As noted above, intervention personalization operates on the fundamental recognition that patients, even with similar diagnoses, exhibit substantial variability in their biopsychosocial characteristics. This heterogeneity profoundly influences treatment responses. For physical health conditions, tailoring interventions to align with these individual characteristics could optimize treatment efficacy by directly addressing the unique biological mechanisms of each patient. This perspective is supported by empirical evidence across various medical domains. For instance, in oncology, personalized cancer therapies using specific biomarkers for treatment selection were associated with improved response rates, prolonged progression-free survival and overall survival, and lower treatment-related death compared to non-personalized treatments.42
For mental health concerns, the aptitude-treatment interaction framework posits that the response to a particular psychological treatment depends on the individual’s characteristics (aptitude). In other words, individuals with certain characteristics could more readily benefit from certain treatment situations theoretically.43 Correspondingly, intervention personalization could optimize treatment efficacy by tailoring treatments to individuals’ characteristics. Indeed, empirical research has shown that patients with certain characteristics, such as an insecure attachment style, tend to exhibit better treatment outcomes from specific forms of psychotherapy (eg, those focused on interpersonal relationships).44 Moreover, a recent meta-analysis on RCTs has suggested that psychological interventions tailored to individual patient characteristics lead to more favorable outcomes compared to standardized treatments.45
Minimizing Adverse Effects
Intervention personalization can also be crucial for minimizing the adverse effects of treatment. Without personalization, treatments risk being applied uniformly across diverse patient profiles, neglecting the inherent variability in how individuals respond to interventions. In the realm of medical treatments such as pharmacotherapy, the importance of genetic variations in drug metabolism has been well-documented.46 Failure to consider these variations can lead to adverse reactions, as individuals with different genetic makeup can metabolize drugs differently. Correspondingly, empirical evidence in personalized medicine showcases instances where tailoring medical treatments based on genetic information significantly reduces the occurrence of adverse reactions.47
This principle extends into psychological interventions. Individuals undergoing psychological interventions exhibit significant variability in their psychological makeup, life experiences, and coping styles. In a standardized or generic approach, certain therapeutic techniques or strategies that work well for some individuals may be counterproductive or distressing for others. For example, meditation-based interventions in general are beneficial for improving mental health.48 However, there is a small proportion of meditation practitioners who reported meditation-related adverse effects (eg, traumatic re-experiencing, functional impairment), and practitioners with childhood adversity experiences (eg, abuse) have an elevated risk of experiencing meditation-related adverse effects.49 This underscores the potential for personalized psychological interventions to minimize the risk of inadvertently worsening psychological distress.
How to Personalize Interventions?
In this section, we discuss approaches for intervention personalization.27,28 Consistent with our conceptualization of intervention personalization, we broadly categorize personalization approaches at two levels: inter-patient personalization (ie, assigning tailored interventions based on the characteristics of individual patients compared to other patients) and intra-patient personalization (ie, adapting interventions during treatment to meet each patient’s evolving needs). It is important to acknowledge that our discussion represents a selection of prominent strategies and is not intended to provide an exhaustive list of strategies. In Table 1, we provide a summary of these intervention personalization strategies.
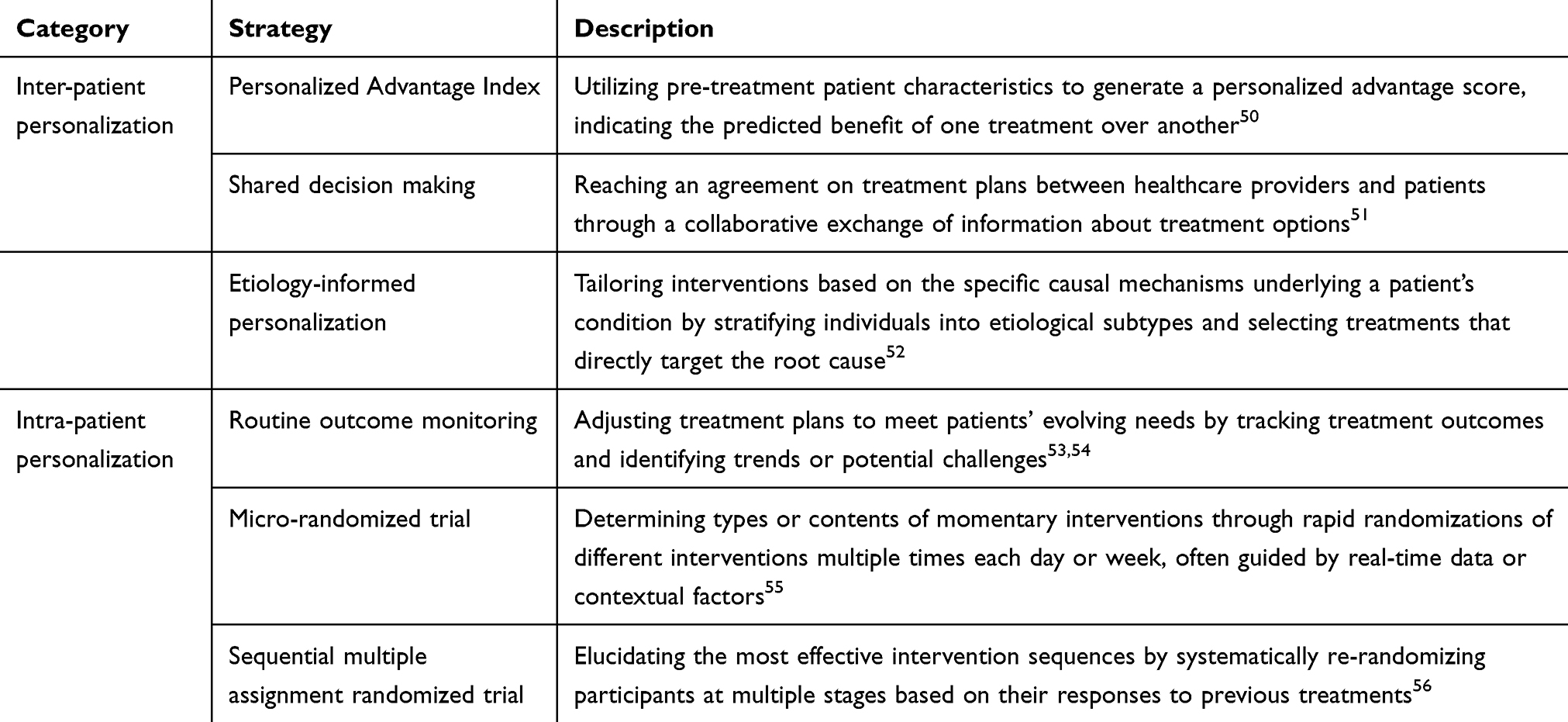 |
Table 1 Intervention Personalization Strategies |
Inter-Patient Intervention Personalization
Several strategies aim to personalize intervention strategies at the inter-patient level with the recognition of individual variability among patients. The Personalized Advantage Index (PAI) is a statistical algorithm utilizing pre-treatment patient characteristics, such as demographic information and symptom severity, to determine which treatment is likely to be more advantageous for a given patient.50 PAI was originally developed by DeRubeis et al’s randomized clinical trial to predict the relative efficacy of cognitive behavioral therapy (CBT) versus medications for major depressive disorder.50 In this trial, DeRubeis et al found relevant patient characteristics that could predict treatment outcomes, such as age, employment status, baseline symptom severity, presence of comorbid personality disorder, and number of stressful events. They developed predictive models for each patient using data from other patients to ensure the prediction was unbiased. Using these models, they estimated the expected end-of-treatment depressive symptoms for each treatment option with the input of each patient’s characteristics. By calculating the difference between the expected outcomes of different treatments for each patient, PAI indicated the treatment most likely to yield the best results for each patient. Research suggests that patients receiving their PAI-indicated “optimal” treatment had superior treatment outcomes compared to those assigned to PAI-non-indicated treatment (“non-optimal” treatment).57,58 These findings demonstrated the potential of PAI in guiding personalized treatment selection.
Shared decision making is a collaborative approach to personalized treatment selection according to diverse needs of different patients.51 Unlike PAI, shared decision making does not rely solely on statistical algorithms; instead, it emphasizes a partnership between the patient and the healthcare provider through collaborative decision-making. Shared decision making involves a comprehensive exchange of information between the healthcare provider and the patient, where treatment options, including potential benefits and risks, are thoroughly discussed. Through discussions about various options and potential outcomes, a joint agreement on the treatment plan is reached.51 Shared decision making often utilizes decision support tools such as informational materials to facilitate understanding of treatment options. Emphasizing patient values and preferences, shared decision making ensures that the patient’s lifestyle, goals, and concerns are integral to the decision-making process.59 Evidence from RCTs suggested that shared decision making increased patient satisfaction and engagement.60–62
Etiology-informed personalization is a strategy that tailors clinical interventions based on the specific causal mechanisms underlying an individual patient’s condition.52 By stratifying patients according to etiological profiles, this approach selects intervention types that directly target each patient’s root cause of conditions.52 This strategy has been applied in multiple domains. For instance, pain can be classified into nociceptive, neuropathic, or nociplastic types based on its underlying etiology.63 Nociceptive pain arises from tissue damage, inflammation, and degeneration; neuropathic pain results from nerve injury or damage; and nociplastic pain reflects a sensitized nervous system without clear tissue or nerve damage.63 Correspondingly, certain treatments are specific to a given pain phenotype; for example, neurodynamic mobilizations for neuropathic pain target the underlying neural pathology.64 Other treatment approaches, such as pain education and exercise therapy, may be applicable across different pain types, but their content and delivery should be adapted to the underlying pain mechanism.64 Similarly, in the management of childhood obesity, an etiology-based personalized intervention model has been proposed to customize nutritional, physical activity and behavioral components according to each child’s unique causal factors for obesity;65 and in asthma, delineating distinct inflammatory endotypes (phenotypes linked to underlying biology) allows clinicians to choose targeted therapies matched to the patient’s disease mechanism.66
Intra-Patient Intervention Personalization
Beyond personalizing intervention strategies at the inter-person level, some approaches adapt interventions during treatment. Routine outcome monitoring is an intervention personalization strategy that involves regularly measuring patients’ well-being, symptoms, and functioning throughout treatment. By systematically tracking these outcomes, clinicians can identify trends or potential challenges in a patient’s progress, allowing for timely adjustments to treatment plans to meet each patient’s needs.53,54 Meta-analytic evidence suggested that the use of routine outcome monitoring in psychotherapy was associated with improved outcomes compared to treatment-as-usual.53
Micro-randomized trials are a trial design offering a dynamic and contextually responsive approach to personalizing interventions. Micro-randomized trials involve rapid randomizations of different interventions multiple times each day or week, often guided by real-time data or contextual factors.55 This approach allows for determining the momentary interventions that patients need and are receptive to, in real time and real-world settings. Micro-randomized trials are particularly relevant in the context of mobile health interventions, where real-time delivery of appropriate interventions in moments when individuals need support is assumed to enhance effectiveness.30
In complex and longer-term interventions, which often involve a combination of multiple treatments, tailoring the order and timing of these interventions to individual needs emerges as a critical facet of intervention personalization. Sequential multiple assignment randomized trial (SMART) can be useful in discerning the most effective order of interventions, as well as which follow-up interventions are most effective for non-responders to the initial interventions.56 In a SMART design, participants undergo initial randomization to distinct treatments. Following this phase, adaptive decisions are made based on individual responses, leading to subsequent randomization to different follow-up treatments. This adaptive process iterates through various stages, allowing for the tailoring of interventions based on individual responses.56 For example, in a SMART design evaluating interventions for children with attention-deficit/hyperactivity disorder, participants were initially randomized into groups receiving either behavioral parent training and teacher consultation or extended-release methylphenidate. Those who did not respond sufficiently to the initial treatment were re-randomized into groups receiving increased dose/intensity of the initial treatment or adding the other treatment option.67 The results showed that for non-responders to behavioral interventions at the first stage, increasing the intensity of behavioral interventions at the second stage produced better outcomes than adding pharmacological treatments. However, for non-responders to medication at the first stage, the second-stage interventions did not show significant differences in outcomes.67
Chronic Pain Management as a Candidate for a Personalized Approach
What Makes Personalization Crucial in Chronic Pain Management?
Inter-Patient Variability in Pain Etiologies, Contributing Factors, and Pain Experiences
Chronic pain is not a singular entity but an umbrella term encompassing a multitude of conditions with different etiologies.1 For instance, chronic musculoskeletal pain like symptomatic osteoarthrosis is characterized by the wear and tear of joints, bones, muscles, or associated soft tissues; chronic neuropathic pain is caused by nerve damage or dysfunction.1 The distinct etiologies and pathophysiologies characterizing different pain conditions highlight the need for tailored approaches that address the unique origins and physiological processes to ensure effective chronic pain management.
Moreover, interactions among various psychosocial factors, such as gender, age, race/ethnicity, and pain catastrophizing contribute to the unique experiences of chronic pain across different patients.68 Personality traits may play a role in the use of coping strategies and the effect of coping strategies for patients with chronic pain. In one study conducted on patients with rheumatoid arthritis,69 researchers found that emotional expression was associated with lower pain in those with lower extroversion levels but demonstrated the opposite effect in patients with higher extroversion.69 According to this finding, encouraging low-extroversion patients to engage in emotional expression may help improve their pain outcomes. In contrast, emotional expression interventions may be unhelpful or even harmful for high-extroversion patients. Thus, it is important to tailor interventions to the psychosocial characteristics (eg, personality traits) of each patient to optimize treatment effectiveness while minimizing potential adverse effects.
The spectrum of chronic pain also extends across varying degrees of severity and functional impairment.2 This heterogeneity requires personalized interventions that account for both the intensity of pain and its functional repercussions. For instance, consider a patient experiencing moderate pain due to osteoarthritis. This patient faces challenges in performing routine activities like walking and climbing stairs. A personalized intervention for them might involve a combination of tailored exercises to improve joint mobility and biofeedback to enhance their awareness and control over physiological responses contributing to pain. In contrast, another patient with neuropathic pain might endure more intense pain sensations but maintain relatively unaffected daily functioning. In this case, a personalized intervention could prioritize mindfulness or CBT techniques, targeting the psychological aspects of pain experiences (eg, pain catastrophizing) and coping strategies. Conversely, applying one-size-fits-all treatment approaches without aligning them with the specific pain severities and functional impacts may undermine treatment effectiveness.
Intra-Patient Variability in Pain Experiences and Coping Strategies
Intra-patient variability further underscores the importance of personalized chronic pain treatment. Research showed that pain experiences (eg, pain intensity) and the use of coping strategies in patients with chronic pain can fluctuate on both daily and momentary levels.70,71 For instance, momentary pain intensity, along with pain-related emotional and cognitive symptoms, was found to increase steadily throughout the day in patients with multiple sclerosis.70 Kim et al demonstrated that both daily pain intensity and pain acceptance showcased significant intra-person variability in patients with spinal cord injury and chronic pain.71 Moreover, daily pain acceptance was found to be associated with improved daily pain interference, social engagement, depressive symptoms, and positive affect and well-being.71 Individualizing chronic pain interventions becomes important to accommodate these fluctuations. A one-size-fits-all approach may miss opportunities to try potentially effective interventions or overburden participants in circumstances when they do not need support. Personalized interventions, on the other hand, can dynamically adapt to the changing nature of pain experiences and coping strategies, offering tailored strategies only when participants require them.30 For example, based on the findings of Kim et al, interventions may selectively prompt pain acceptance strategies on days when patients exhibit lower pain acceptance to potentially improve symptoms, well-being, and functioning. Such personalized interventions have the potential not only to enhance the effectiveness of interventions but also to boost engagement and alleviate the burden on patients.
Treatment Response Heterogeneity
Nonpharmacological and noninvasive interventions have garnered attention for their potential to improve outcomes related to chronic pain with minimal risks.72 Various interventions, such as CBT, mindfulness-based interventions (MBIs), and biofeedback, address the psychological, behavioral, or physical aspects of chronic pain. These interventions have demonstrated efficacy in mitigating pain severity and enhancing functionality among patients with chronic pain.16,73,74
However, treatment response heterogeneity is evident in these interventions. A specific therapeutic approach that proves efficacious for one patient may not yield similar results for another. For instance, an RCT involving patients (n = 256) with chronic pain showed that patients with fewer interpersonal problems related to pain coping, higher expectations for treatment effect, greater disease severity, older age, and higher education levels benefited more from CBT compared with other patients.75 Patient psychological characteristics were also found to predict the effect of MBIs. Research on patients with chronic pain revealed that greater levels of attachment avoidance (ie, perceiving others as unreliable or unavailable when being distressed) were associated with more substantial reductions in pain intensity following participation in MBIs.76 These variations highlight the heterogeneity in treatment responses among patients with different demographics and psychological characteristics, supporting the importance of intervention personalization for chronic pain.
Moreover, a specific therapeutic approach that proves efficacious in improving certain pain-related symptoms may not yield similar results for other symptoms. In their meta-analysis of 167 RCTs on patients with fibromyalgia, Kundakci et al found that MBIs and CBT could improve disease-specific quality of life, pain, sleep, and depression compared to usual care while showing no impact on fatigue. In contrast, mind-body physical exercises were found to reduce fatigue but were not effective in improving disease-specific quality of life.77 These findings underscore the importance of providing targeted interventions to address the specific symptoms associated with chronic pain.
Personalized Nonpharmacological and Noninvasive Chronic Pain Treatment Studies
In 1991, Fry and Wong published one of the early studies on personalized nonpharmacological and noninvasive treatment for chronic pain.78 In this study, elderly patients (n = 69) with chronic pain reported their styles of coping with chronic pain. Patients who demonstrated a tendency for problem- and emotion-focused coping were paired with problem- and emotion-focused pain management training, respectively. The remaining patients received mixed interventions randomly chosen from problem- and emotion-focused training. The findings revealed significantly greater improvements in pain severity, anxiety, adjustment, and satisfaction in groups with tailored interventions relative to the group receiving non-tailored interventions.
In tandem with the growing emphasis on intervention personalization in the broader scientific literature, there has been a rising number of empirical studies on personalized interventions for chronic pain. In the following sections, we discuss some studies to demonstrate diverse strategies for personalizing nonpharmacological and noninvasive chronic pain treatment. We focus on nonpharmacological and noninvasive approaches because they represent accessible and low-risk strategies that can be implemented across diverse chronic pain populations. While our emphasis is on these modalities, we acknowledge that pharmacological and/or invasive treatments (eg, interventional pain management) can also be personalized based on pain etiology and individual characteristics.79
Inter-Patient Personalized Nonpharmacological and Noninvasive Chronic Pain Treatment
Van Koulil et al examined the efficacy of personalized treatment relative to a waitlist control in patients (n = 158) with fibromyalgia. Patients in the personalized treatment condition received 16-session CBT and exercise training focused on addressing pain avoidance or pain persistence tailored to their cognitive-behavioral patterns. The treatment condition was found to significantly improve both physical and psychological functioning from pre- to post-treatment and 6-month follow-up compared to the waitlist control.80
Lehtola et al conducted an RCT comparing the efficacy of specific movement control exercises (personalized) and general exercises (non-personalized) in patients (n = 70) with non-specific low back pain. General exercises focused on abdominal and paraspinal muscles without specific deep muscle engagement, aiming to improve overall physical function and confidence in spine use. In contrast, specific movement control exercises emphasized monitoring the precision of the lumbar spine position. These exercises specifically targeted a trunk movement direction, addressing the presumed lack of control contributing to low back pain. The study found that the specific movement control exercises group showed superior improvement in disability at 12-month follow-up compared to the general exercises group.81
De Groef et al developed and pilot-tested a personalized eHealth intervention delivering pain science education and self-management strategies for breast cancer survivors with chronic pain.82 The program included 22 interactive sessions tailored through a decision-tree algorithm to reflect each participant’s responses to questions. For example, only participants who indicated they received chemotherapy were shown the education on chemotherapy-related pain. Using a mixed-method pilot design with 29 women, the authors assessed feasibility, acceptability, and preliminary efficacy over a six-week period with follow-up at three months. Qualitative findings emphasized that the program was helpful and easy to use but best positioned as an adjunct to comprehensive care. Quantitative analyses indicated significant improvements in pain-related functioning, physical functioning, quality of life, and symptoms of hyperalgesia and allodynia, with no changes in pain intensity or emotional outcomes.
In a multicenter cluster RCT, Koppenaal et al investigated the short-term effectiveness of “e-Exercise LBP”, a stratified blended physiotherapy intervention integrating a smartphone app with face-to-face care.83 The study involved 208 patients with nonspecific low back pain, with the blended care group stratified according to their risk of developing persistent pain. In particular, the intensity, duration, and psychosocial focus of interventions in the blended care group were tailored to patients’ determined risk level. The control group received standard face-to-face physiotherapy without the use of a web-based application or a priori risk stratification. While both groups showed clinically relevant improvements, the study found no significant difference in the primary outcome of physical functioning at the 3-month follow-up. However, the stratified blended physiotherapy group achieved significant improvements in fear-avoidance beliefs and self-reported adherence to home exercises compared to the control. Additionally, patients at high risk of developing persistent pain experienced significantly better physical functioning with the blended intervention.
Intra-Patient Personalized Nonpharmacological and Noninvasive Chronic Pain Treatment
Somers et al aimed to optimize pain management in women (n = 327) with breast cancer by evaluating varying dose sequences of Pain Coping Skills Training (PCST).84 Participants were initially randomized to receive either a full course (5 sessions, PCST-Full) or a brief version (1 session, PCST-Brief). Responders (≥30% pain reduction) were re-randomized to a maintenance dose or no dose, while non-responders were re-randomized to an increased or maintenance dose. At the 6-month follow-up, all PCST dose sequences showed sustained pain reduction, with sequences involving PCST-Full, either as an initial or secondary dose, exhibited the most durable pain reduction at the 6-month follow-up. Conversely, sequences starting with PCST-Brief, followed by PCST-Brief Maintenance or no dose, had the least durable pain reduction. These results highlight the importance of tailoring intervention sequences for effective pain management. For instance, patients who do not respond to an initial PCST-Brief may benefit from an increased dose later, rather than maintenance or no dose, to achieve more durable pain reduction.
In an RCT, Piette et al compared artificial intelligence-assisted CBT for chronic pain (AI-CBT-CP, personalized group) to therapist-delivered CBT-CP in patients (n = 278) with chronic back pain.85 Both groups received CBT-CP for 10 weeks. The therapist-delivered CBT-CP group had weekly 45-minute telephone sessions. In the AI-CBT-CP group, patients provided daily reports on pain severity, mood, sleep, step counts, CBT skill use, self-efficacy, and progress toward behavioral goals. The AI engine in this group determined whether patients received a 45- or 15-minute synchronous telephone session or a personalized asynchronous voice message each week based on these reports. At the 6-month follow-up, more patients in the AI-CBT-CP group showed clinically significant improvements in pain-related disability and pain intensity relative to the therapist-delivered group. Patients in the AI-CBT-CP group also completed more treatment weeks and had less therapist interaction time.
Critical Evaluation of Personalized Nonpharmacological and Noninvasive Chronic Pain Treatment Studies
Across inter-patient personalization studies reviewed, inter-patient personalization was generally associated with improvements in physical functioning and psychological outcomes, though in some cases these benefits were limited to specific subgroups (eg, high-risk patients). Across these studies, tailoring was based upon cognitive-behavioral patterns,80 motor control impairments,81 prior treatment experiences,82 and risk of developing chronic pain.83 A strength of these studies was their grounding in theoretical or mechanistic models. Etiology-informed personalization was most closely reflected in studies that matched interventions to presumed psychological or biomechanical mechanisms.80,81 PAI and shared decision making were not implemented in any of the studies reviewed. In terms of methodological rigor, two studies were well-powered RCTs,80,83 one used a smaller RCT design,81 and one was a pilot study without a control group.82 Among the reviewed studies, only Lehtola et al directly isolated the effect of personalization by comparing tailored movement control exercises to non‑tailored general exercises; the remaining studies did not compare tailored and non-tailored versions of the same intervention, making it difficult to determine whether observed effects were attributable to personalization or to the intervention more broadly.
Across the intra-patient personalization studies reviewed, personalization was associated with improved outcomes in pain-related disability and intensity, while also enhancing treatment efficiency and engagement. Personalization was achieved through dynamic adaptation of intervention dose or delivery modality and intensity in response to patient progress or daily data.84,85 These approaches align with the intra-patient personalization strategies discussed earlier, particularly the SMART design and approaches conceptually similar to routine outcome monitoring. A strength of both studies was their clearly defined adaptation protocols and adequate sample sizes.84,85 However, neither study employed micro-randomized designs to test moment-to-moment intervention delivery.84,85 Together, these studies highlight the potential of intra-patient personalization to improve both clinical outcomes and scalability, while pointing to future directions for greater temporal precision.
Future Research Directions
We believe that personalized nonpharmacological and noninvasive chronic pain treatment has the potential to enhance treatment engagement, optimize treatment effectiveness, and minimize potential adverse effects. To harness the potential of personalized chronic pain treatment, below we propose several future research directions (See Table 2 for a summary).
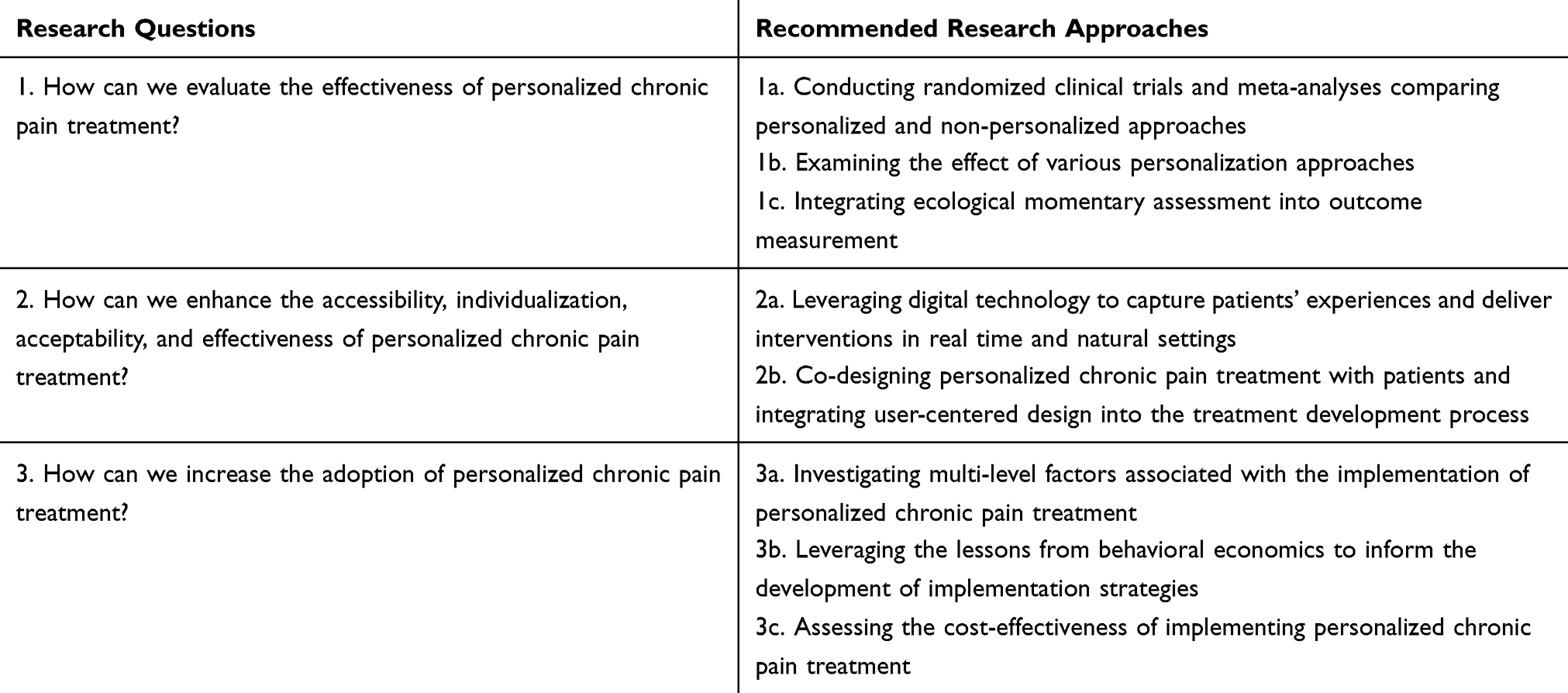 |
Table 2 Recommended Future Research Directions |
An important research question revolves around the effectiveness of personalized chronic pain treatment. Theoretically, personalization holds the promise to optimize treatment effectiveness. However, existing literature falls short of providing a definitive answer to this inquiry. RCTs demonstrated that incorporating personalized interventions alongside standard care or treatment-as-usual might yield incremental benefits for chronic pain management.86,87 However, empirical evidence regarding the effectiveness of personalized chronic pain interventions over non-personalized approaches appears inconclusive.81,88 Future well-powered randomized clinical trials and comprehensive meta-analyses comparing personalized and non-personalized interventions are needed to establish the evidence base of personalized nonpharmacological and noninvasive chronic pain treatment.
Moreover, there is a compelling need for a rigorous investigation into the effectiveness of various personalization approaches in chronic pain treatment. Moving beyond what personalized interventions work to uncovering how and when to deploy them most effectively, as well as determining the optimal intensity for each patient, is crucial for advancing personalized chronic pain treatment. This exploration will offer valuable insights into tailoring interventions to individual needs in various ways, thus optimizing their impact on chronic pain management. Additionally, incorporating multiple personalization strategies may enhance individualization and flexibility in chronic pain treatment. For example, shared decision-making can be utilized to select personalized chronic pain interventions for individual patients at the pre-treatment stage.51 This can be followed by routine outcome monitoring to adapt treatment approaches throughout treatments according to patients’ evolving needs.53,54
Another promising avenue for future research lies in integrating ecological momentary assessment into outcome measurement. Retrospective assessments, while valuable, are susceptible to recall bias and may not capture the nuanced, dynamic nature of chronic pain experiences over time.70 In contrast, ecological momentary assessment, with its real-time data collection, offers a more fine-grained understanding of patients’ pain experiences, coping strategies, and responses to interventions.70,71 Future studies may explore how integrating ecological momentary assessment into outcome measurement can potentially contribute to a more accurate and comprehensive evaluation of the impact of personalized chronic pain treatment.89
Future studies may embrace digital technologies to facilitate intervention personalization. As mentioned earlier, pain experiences (eg, pain intensity) and the use of coping strategies in patients with chronic pain can fluctuate on both daily and momentary levels.70,71 Advanced technologies, such as smartphones and wearable devices, allow for capturing the fluctuations in a patient’s pain experiences, the use of coping strategies, and the effect of interventions through real-time self-reports and passive data collection.70,71,90 Moreover, in contrast to the traditional weekly support provided by evidence-based treatments like MBIs and CBT for chronic pain, technology-delivered interventions can integrate support into patients’ daily lives. Just-in-time adaptive interventions, an example of this integration, may provide tailored types and amounts of support to patients with chronic pain based on their contextual and internal states in real time.30,91 For instance, if a patient encounters heightened pain interference in their daily life, a smartphone-delivered, timely pain acceptance strategy can be prompted through just-in-time adaptive interventions to help them reduce pain interference.71 With advancements in real-time data collection and analysis techniques, just-in-time adaptive interventions and other technology-based interventions hold significant potential to enhance the accessibility, individualization, and effectiveness of personalized nonpharmacological and noninvasive chronic pain treatment.
It is important to involve patients as key stakeholders in designing personalized chronic pain treatments. Patients with chronic pain often grapple with feelings of isolation and a sense of not being heard or believed within healthcare systems.92 Co-designing personalized nonpharmacological and noninvasive chronic pain treatment with patients may not only enhance the relevance, cultural sensitivity, and effectiveness of interventions but also promote a sense of ownership, connection, and trust among patients. Future research endeavors can benefit from integrating methodologies such as user-centered design into the intervention development process. Key steps in user-centered design, including identifying users and their needs, rapidly iterating interventions based on user feedback, simplifying interventions, and aligning interventions with specific contexts, have the potential to bolster patient engagement and optimize the effectiveness of personalized nonpharmacological and noninvasive chronic pain treatment.93
Future research endeavors may examine the factors influencing the implementation of personalized nonpharmacological and noninvasive interventions for chronic pain. Implementation science frameworks, such as the Consolidated Framework for Implementation Research, may provide a structured approach for systematically understanding the multi-level factors influencing the adoption and sustainability of personalized chronic pain treatments in real-world clinical settings.94 Future studies may explore the role of intervention complexity, patient needs, and perspectives of healthcare providers, clinic directors, and policymakers in the implementation of personalized nonpharmacological and noninvasive chronic pain treatment. Such efforts will ultimately inform targeted implementation strategies at different levels (eg, at the policy level, increasing investment in integrative medicine characterized by holistic and patient-centered care).95
Principles from behavioral economics may also provide valuable insights into examining the facilitators and barriers associated with the implementation of personalized nonpharmacological and noninvasive chronic pain treatment.96 As discussed earlier, behavioral economics operates under the assumption that individuals have limited cognitive resources and processing capabilities and that human decision-making is susceptible to various cognitive biases.35 Examples of such biases include the status quo bias, wherein individuals tend to default to their current state rather than embrace changes even when changes may be objectively better, and aversion to uncertainty, which reflects a preference for known risks over uncertain ones. Personalized nonpharmacological and noninvasive chronic pain treatment, departing from conventional, non-personalized approaches like opioid-centric treatments, may encounter the activation of cognitive biases during their implementation, mirroring challenges faced by other innovations.97 Future research may leverage lessons from behavioral economics to inform the development of implementation strategies that effectively promote the adoption and sustainment of personalized nonpharmacological and noninvasive chronic pain treatment.96
Moreover, it is important to assess the cost-effectiveness of implementing personalized nonpharmacological and noninvasive chronic pain treatment. This economic evaluation recognizes that the implementation cost of personalized interventions may be context-specific and influenced by factors such as specific features of the interventions, the population being served, and the broader healthcare system supporting the delivery of the interventions. As an integral facet of implementation science, evaluating the cost-effectiveness of implementing personalized nonpharmacological and noninvasive chronic pain treatment may provide insights into the practicality and sustainability of integrating these interventions into routine clinical practice and guide healthcare decision-makers in resource allocation.98 Overall, unraveling and addressing the implementation factors will be pivotal in ensuring the widespread and impactful deployment of personalized approaches for chronic pain management.
In conclusion, this paper addresses intervention personalization in general healthcare and specifically in the context of chronic pain management. It outlines a future research roadmap, urging robust clinical trials and meta-analyses, exploration of diverse personalization approaches, integration of ecological momentary assessment, adoption of cutting-edge digital technologies, patient co-design, and examination of implementation factors. We hope that future studies can advance highly personalized nonpharmacological and noninvasive chronic pain management to optimize treatment effectiveness and minimize adverse effects by pursuing these research directions.
Funding
QX was supported by grant R01 AA024150 (NIAAA). SBG was supported by the National Center for Complementary and Integrative Health Grants K23AT010879 and R24AT012845. NJ was supported by R01DA055527-01A1 (NIDA) and R01AA024150-01A1 (NIAAA). AQ was supported by R01DA055527-01A1 (NIDA), R01AA024150-01A1 (NIAAA), and R01DA047279-01 (NIDA). The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of any funding parties.
Disclosure
AQ has a shareholder interest in CHESS Health, a small business that markets a digital health application for substance use disorder to the addiction treatment field, and provides consulting on digital health implementation through the NIATx Foundation. The remaining authors declare no conflicts of interest with respect to the research, authorship, or publication of this article.
References
1. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–1007. doi:10.1097/j.pain.0000000000000160
2. Rikard SM, Strahan AE, Schmit KM, GPJr G. Chronic pain among adults — United States, 2019–2021. MMWR Morb Mortal Wkly Rep. 2023;72(15):379–385. doi:10.15585/mmwr.mm7215a1
3. Hadi MA, McHugh GA, Closs SJ. Impact of chronic pain on patients’ quality of life: a comparative mixed-methods study. J Patient Exp. 2019;6(2):133–141. doi:10.1177/2374373518786013
4. Angst F, Benz T, Lehmann S, et al. Extended overview of the longitudinal pain-depression association: a comparison of six cohorts treated for specific chronic pain conditions. J Affect Disord. 2020;273:508–516. doi:10.1016/j.jad.2020.05.044
5. Dueñas M, Ojeda B, Salazar A, Mico JA, Failde I. A review of chronic pain impact on patients, their social environment and the health care system. J Pain Res. 2016;9:457–467. doi:10.2147/JPR.S105892
6. Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13(8):715–724. doi:10.1016/j.jpain.2012.03.009
7. Jones MR, Viswanath O, Peck J, Kaye AD, Gill JS, Simopoulos TT. A brief history of the opioid epidemic and strategies for pain medicine. Pain Ther. 2018;7(1):13–21. doi:10.1007/s40122-018-0097-6
8. Ballantyne JC, Shin NS. Efficacy of opioids for chronic pain: a review of the evidence. Clin J Pain. 2008;24(6):469–478. doi:10.1097/AJP.0b013e31816b2f26
9. Inoue K, Ritz B, Arah OA. Causal effect of chronic pain on mortality through opioid prescriptions: application of the front-door formula. Epidemiology. 2022;33(4):572–580. doi:10.1097/EDE.0000000000001490
10. Kolodny A, Courtwright DT, Hwang CS, et al. The prescription opioid and heroin crisis: a public health approach to an epidemic of addiction. Annu Rev Public Health. 2015;36(1):559–574. doi:10.1146/annurev-publhealth-031914-122957
11. Boscarino JA, Rukstalis M, Hoffman SN, et al. Risk factors for drug dependence among out-patients on opioid therapy in a large US health-care system. Addiction. 2010;105(10):1776–1782. doi:10.1111/j.1360-0443.2010.03052.x
12. Florence C, Luo F, Rice K. The economic burden of opioid use disorder and fatal opioid overdose in the United States, 2017. Drug Alcohol Depend. 2021;218:108350. doi:10.1016/j.drugalcdep.2020.108350
13. Gaskell H, Moore RA, Derry S, Stannard C. Oxycodone for neuropathic pain and fibromyalgia in adults. Cochrane Database Syst Rev. 2014;(6):CD010692. doi:10.1002/14651858.CD010692.pub2
14. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, Hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578–1589. doi:10.1016/j.joca.2019.06.011
15. Nicol AL, Hurley RW, Benzon HT. Alternatives to opioids in the pharmacologic management of chronic pain syndromes: a narrative review of randomized, controlled, and blinded clinical trials. Anesth Analg. 2017;125(5):1682–1703. doi:10.1213/ANE.0000000000002426
16. Williams de ACC, Fisher E, Hearn L, Eccleston C. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst Rev. 2020. doi:10.1002/14651858.CD007407.pub4
17. Collins FS, Varmus H. A new initiative on precision medicine. New Eng J Med. 2015;372(9):793–795. doi:10.1056/NEJMp1500523
18. McCracken LM. Personalized pain management: is it time for process-based therapy for particular people with chronic pain? Eur J Pain. 2023;27(9):1044–1055. doi:10.1002/ejp.2091
19. Edwards RR, Schreiber KL, Dworkin RH, et al. Optimizing and accelerating the development of precision pain treatments for chronic pain: IMMPACT review and recommendations. J Pain. 2023;24(2):204–225. doi:10.1016/j.jpain.2022.08.010
20. McCaffery M. Nursing Practice Theories Related to Cognition, Bodily Pain, and Man-Environment Interactions. University of California Print. Office; 1968.
21. Elbers S, Wittink H, Konings S, et al. Longitudinal outcome evaluations of interdisciplinary multimodal pain treatment programmes for patients with chronic primary musculoskeletal pain: a systematic review and meta-analysis. Eur J Pain. 2022;26(2):310–335. doi:10.1002/ejp.1875
22. Mikosz CA, Zhang K, Haegerich T, et al. Indication-specific opioid prescribing for US patients with medicaid or private insurance, 2017. JAMA Network Open. 2020;3(5):e204514. doi:10.1001/jamanetworkopen.2020.4514
23. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain — United States, 2022. MMWR Recomm Rep. 2022;71(No. RR–3):1–95. doi:10.15585/mmwr.rr7103a1
24. McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348(26):2635–2645. doi:10.1056/NEJMsa022615
25. Jørgensen JT. Twenty years with personalized medicine: past, present, and future of individualized pharmacotherapy. Oncologist. 2019;24(7):e432–e440. doi:10.1634/theoncologist.2019-0054
26. U.S. Food and Drug Administration. Focus area: individualized therapeutics and precision medicine. 2022. Available from: https://www.fda.gov/science-research/focus-areas-regulatory-science-report/focus-area-individualized-therapeutics-and-precision-medicine.
27. Ng MY, Weisz JR. Annual research review: building a science of personalized intervention for youth mental health. J Child Psychol Psychiatry. 2016;57(3):216–236. doi:10.1111/jcpp.12470
28. Stumpp NE, Sauer-Zavala S. Evidence-based strategies for treatment personalization: a review. Cognitive Behav Pract. 2022;29(4):902–913. doi:10.1016/j.cbpra.2021.10.004
29. Hamburg MA. Paving the way for personalized medicine: FDA’s role in a new era of medical product development. 2013. Available from: https://www.fdanews.com/ext/resources/files/10/10-28-13-Personalized-Medicine.pdf.
30. Nahum-Shani I, Smith SN, Spring BJ, et al. Just-in-time adaptive interventions (JITAIs) in mobile health: key components and design principles for ongoing health behavior support. Ann Behav Med. 2018;52(6):446–462. doi:10.1007/s12160-016-9830-8
31. Claussnitzer M, Cho JH, Collins R, et al. A brief history of human disease genetics. Nature. 2020;577(7789):179–189. doi:10.1038/s41586-019-1879-7
32. Uher R, Zwicker A. Etiology in psychiatry: embracing the reality of poly‐gene‐environmental causation of mental illness. World Psychiatry. 2017;16(2):121–129. doi:10.1002/wps.20436
33. American Psychological Association. Presidential task force on evidence-based practice. evidence-based practice in psychology. Am Psychol. 2006;61(4):271–285. doi:10.1037/0003-066X.61.4.271
34. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55:68–78. doi:10.1037/0003-066X.55.1.68
35. Thaler RH. Behavioral economics: past, present, and future. Am Econ Rev. 2016;106(7):1577–1600. doi:10.1257/aer.106.7.1577
36. Ericson KMM, Fuster A. The endowment effect. Annu Rev Econ. 2014;6:555–579. doi:10.1146/annurev-economics-080213-041320
37. Borghouts J, Eikey E, Mark G, et al. Barriers to and facilitators of user engagement with digital mental health interventions: systematic review. J Med Internet Res. 2021;23(3):e24387. doi:10.2196/24387
38. Schubart JR, Stuckey HL, Ganeshamoorthy A, Sciamanna CN. Chronic health conditions and internet behavioral interventions: a review of factors to enhance user engagement. CIN. 2011;29(2):81. doi:10.1097/NCN.0b013e3182065eed
39. Swift JK, Callahan JL. The impact of client treatment preferences on outcome: a meta-analysis. J Clin Psychol. 2009;65(4):368–381. doi:10.1002/jclp.20553
40. Nuijten R, Gorp PV, Khanshan A, et al. Evaluating the impact of adaptive personalized goal setting on engagement levels of government staff with a gamified mHealth tool: results from a 2-month randomized controlled trial. JMIR mHealth and uHealth. 2022;10(3):e28801. doi:10.2196/28801
41. Fernández-álvarez J, Díaz-García A, González-Robles A, Baños R, García-Palacios A, Botella C. Dropping out of a transdiagnostic online intervention: a qualitative analysis of client’s experiences. Internet Intervent. 2017;10:29–38. doi:10.1016/j.invent.2017.09.001
42. Schwaederle M, Zhao M, Lee JJ, et al. Impact of precision medicine in diverse cancers: a meta-analysis of phase ii clinical trials. J Clin Oncol. 2015;33(32):3817–3825. doi:10.1200/JCO.2015.61.5997
43. Snow RE. Aptitude-treatment interaction as a framework for research on individual differences in psychotherapy. J Consult Clin Psychol. 1991;59(2):205–216. doi:10.1037/0022-006X.59.2.205
44. Levy KN, Kivity Y, Johnson BN, Gooch CV. Adult attachment as a predictor and moderator of psychotherapy outcome: a meta-analysis. J Clin Psychol. 2018;74(11):1996–2013. doi:10.1002/jclp.22685
45. Nye A, Delgadillo J, Barkham M. Efficacy of personalized psychological interventions: a systematic review and meta-analysis. J Consult Clin Psychol. 2023;91(7):389–397. doi:10.1037/ccp0000820
46. Pinto N, Dolan ME. Clinically relevant genetic variations in drug metabolizing enzymes. Curr Drug Metab. 2011;12(5):487–497. doi:10.2174/138920011795495321.
47. Swen JJ, Wouden van der CH, Manson LE, et al. A 12-gene pharmacogenetic panel to prevent adverse drug reactions: an open-label, multicentre, controlled, cluster-randomised crossover implementation study. Lancet. 2023;401(10374):347–356. doi:10.1016/S0140-6736(22)01841-4
48. Goldberg SB, Riordan KM, Sun S, Davidson RJ. The empirical status of mindfulness-based interventions: a systematic review of 44 meta-analyses of randomized controlled trials. Perspect Psychol Sci. 2022;17(1):108–130. doi:10.1177/1745691620968771
49. Goldberg SB, Lam SU, Britton WB, Davidson RJ. Prevalence of meditation-related adverse effects in a population-based sample in the United States. Psychother Res. 2022;32(3):291–305. doi:10.1080/10503307.2021.1933646
50. DeRubeis RJ, Cohen ZD, Forand NR, Fournier JC, Gelfand LA, Lorenzo-Luaces L. The personalized advantage index: translating research on prediction into individualized treatment recommendations. a demonstration. PLoS One. 2014;9(1):e83875. doi:10.1371/journal.pone.0083875
51. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
52. Wang RC, Wang Z. Precision medicine: disease subtyping and tailored treatment. Cancers. 2023;15(15):3837. doi:10.3390/cancers15153837
53. Lambert MJ, Whipple JL, Kleinstäuber M. Collecting and delivering progress feedback: a meta-analysis of routine outcome monitoring. Psychotherapy. 2018;55(4):520–537. doi:10.1037/pst0000167
54. Barkham M, De Jong K, Delgadillo J, Lutz W. Routine Outcome Monitoring (ROM) and feedback: research review and recommendations. Psychother Res. 2023;33(7):841–855. doi:10.1080/10503307.2023.2181114
55. Qian T, Walton AE, Collins LM, et al. The microrandomized trial for developing digital interventions: experimental design and data analysis considerations. Psychol Meth. 2022;27(5):874–894. doi:10.1037/met0000283
56. Kidwell KM, Almirall D. Sequential, multiple assignment, randomized trial designs. JAMA. 2023;329(4):336–337. doi:10.1001/jama.2022.24324
57. van Bronswijk SC, DeRubeis RJ, Lemmens LHJM, et al. Precision medicine for long-term depression outcomes using the personalized advantage index approach: cognitive therapy or interpersonal psychotherapy? Psychol Med. 2021;51(2):279–289. doi:10.1017/S0033291719003192
58. Senger K, Schröder A, Kleinstäuber M, Rubel JA, Rief W, Heider J. Predicting optimal treatment outcomes using the personalized advantage index for patients with persistent somatic symptoms. Psychother Res. 2022;32(2):165–178. doi:10.1080/10503307.2021.1916120
59. Stiggelbout AM, Pieterse AH, De Haes JCJM. Shared decision making: concepts, evidence, and practice. Patient Educ Couns. 2015;98(10):1172–1179. doi:10.1016/j.pec.2015.06.022
60. Hess EP, Hollander JE, Schaffer JT, et al. Shared decision making in patients with low risk chest pain: prospective randomized pragmatic trial. BMJ. 2016;355:i6165. doi:10.1136/bmj.i6165
61. Loh A, Simon D, Wills CE, Kriston L, Niebling W, Härter M. The effects of a shared decision-making intervention in primary care of depression: a cluster-randomized controlled trial. Patient Educ Couns. 2007;67(3):324–332. doi:10.1016/j.pec.2007.03.023
62. Bieber C, Müller KG, Blumenstiel K, et al. A shared decision-making communication training program for physicians treating fibromyalgia patients: effects of a randomized controlled trial. J Psychosom Res. 2008;64(1):13–20. doi:10.1016/j.jpsychores.2007.05.009
63. Cao B, Xu Q, Shi Y, et al. Pathology of pain and its implications for therapeutic interventions. Sig Transduct Target Ther. 2024;9(1):155. doi:10.1038/s41392-024-01845-w
64. Nijs J, De Baets L, Hodges P. Phenotyping nociceptive, neuropathic, and nociplastic pain: who, how, & why? Braz J Phys Ther. 2023;27(4):100537. doi:10.1016/j.bjpt.2023.100537
65. Motevalli M, Drenowatz C, Tanous DR, Khan NA, Wirnitzer K. Management of childhood obesity—time to shift from generalized to personalized intervention strategies. Nutrients. 2021;13(4):1200. doi:10.3390/nu13041200
66. Gonzalez-Uribe V, Romero-Tapia SJ, Castro-Rodriguez JA. Asthma phenotypes in the era of personalized medicine. J Clin Med. 2023;12(19):6207. doi:10.3390/jcm12196207
67. Pelham WE, Fabiano GA, Waxmonsky JG, et al. Treatment sequencing for childhood ADHD: a multiple-randomization study of adaptive medication and behavioral interventions. J Clin Child Adolesc Psychol. 2016;45(4):396–415. doi:10.1080/15374416.2015.1105138
68. Fillingim RB. Individual differences in pain: understanding the mosaic that makes pain personal. Pain. 2017;158(Suppl 1):S11–S18. doi:10.1097/j.pain.0000000000000775
69. Newth S, DeLongis A. Individual differences, mood, and coping with chronic pain in rheumatoid arthritis: a daily process analysis. Psychol Health. 2004;19(3):283–305. doi:10.1080/0887044042000193451
70. Kratz AL, Murphy SL, Braley TJ. Ecological momentary assessment of pain, fatigue, depressive, and cognitive symptoms reveals significant daily variability in multiple sclerosis. Arch Phys Med Rehabil. 2017;98(11):2142–2150. doi:10.1016/j.apmr.2017.07.002
71. Kim S, Whibley D, Williams DA, Kratz AL. Pain acceptance in people with chronic pain and spinal cord injury: daily fluctuation and impacts on physical and psychosocial functioning. J Pain. 2020;21(3):455–466. doi:10.1016/j.jpain.2019.08.014
72. Skelly AC, Chou R, Dettori JR, et al. Noninvasive Nonpharmacological Treatment for Chronic Pain: A Systematic Review Update. Agency for Healthcare Research and Quality (US); 2020.
73. Hilton L, Hempel S, Ewing BA, et al. Mindfulness meditation for chronic pain: systematic review and meta-analysis. Ann Behav Med. 2017;51(2):199–213. doi:10.1007/s12160-016-9844-2
74. Sielski R, Rief W, Glombiewski JA. Efficacy of biofeedback in chronic back pain: a meta-analysis. IntJ Behav Med. 2017;24(1):25–41. doi:10.1007/s12529-016-9572-9
75. Broderick JE, Keefe FJ, Schneider S, et al. Cognitive behavioral therapy for chronic pain is effective, but for whom? Pain. 2016;157(9):2115. doi:10.1097/j.pain.0000000000000626
76. Johannsen M, O’Toole MS, O’Connor M, Jensen AB, Zachariae R. Clinical and psychological moderators of the effect of mindfulness-based cognitive therapy on persistent pain in women treated for primary breast cancer – explorative analyses from a randomized controlled trial. Acta Oncologica. 2017;56(2):321–328. doi:10.1080/0284186X.2016.1268713
77. Kundakci B, Kaur J, Goh SL, et al. Efficacy of nonpharmacological interventions for individual features of fibromyalgia: a systematic review and meta-analysis of randomised controlled trials. Pain. 2022;163(8):1432. doi:10.1097/j.pain.0000000000002500
78. Fry PS, Wong PTP. Pain management training in the elderly: matching interventions with subjects’ coping styles. Stress Med. 1991;7(2):93–98. doi:10.1002/smi.2460070207
79. Smith H, Youn Y, Guay RC, Laufer A, Pilitsis JG. The role of invasive pain management modalities in the treatment of chronic pain. Med Clin. 2016;100(1):103–115. doi:10.1016/j.mcna.2015.08.011
80. van Koulil S, van Lankveld W, Kraaimaat FW, et al. Tailored cognitive-behavioural therapy and exercise training improves the physical fitness of patients with fibromyalgia. Ann Rheum Dis. 2011;70(12):2131–2133. doi:10.1136/ard.2010.148577
81. Lehtola V, Luomajoki H, Leinonen V, Gibbons S, Airaksinen O. Sub-classification based specific movement control exercises are superior to general exercise in sub-acute low back pain when both are combined with manual therapy: a randomized controlled trial. BMC Musculoskelet Disord. 2016;17(1):135. doi:10.1186/s12891-016-0986-y
82. De Groef A, Evenepoel M, Van Dijck S, et al. Feasibility and pilot testing of a personalized eHealth intervention for pain science education and self-management for breast cancer survivors with persistent pain: a mixed-method study. Supp Care Cancer. 2023;31(2):119. doi:10.1007/s00520-022-07557-7
83. Koppenaal T, Pisters MF, Kloek CJ, Arensman RM, Ostelo RW, Veenhof C. The 3-month effectiveness of a stratified blended physiotherapy intervention in patients with nonspecific low back pain: cluster randomized controlled trial. J Med Internet Res. 2022;24(2):e31675. doi:10.2196/31675
84. Somers TJ, Winger JG, Fisher HM, et al. Behavioral cancer pain intervention dosing: results of a sequential multiple assignment randomized trial. Pain. 2023;164(9):1935–1941. doi:10.1097/j.pain.0000000000002915
85. Piette JD, Newman S, Krein SL, et al. Patient-centered pain care using artificial intelligence and mobile health tools: a randomized comparative effectiveness trial. JAMA Int Med. 2022;182(9):975–983. doi:10.1001/jamainternmed.2022.3178
86. Ferwerda M, van Beugen S, van Middendorp H, et al. A tailored-guided internet-based cognitive-behavioral intervention for patients with rheumatoid arthritis as an adjunct to standard rheumatological care: results of a randomized controlled trial. Pain. 2017;158(5):868. doi:10.1097/j.pain.0000000000000845
87. Sandal LF, Bach K, Øverås CK, et al. Effectiveness of app-delivered, tailored self-management support for adults with lower back pain-related disability: a selfBACK randomized clinical trial. JAMA Intern Med. 2021;181(10):1288–1296. doi:10.1001/jamainternmed.2021.4097
88. Marcuzzi A, Nordstoga AL, Bach K, et al. Effect of an artificial intelligence–based self-management app on musculoskeletal health in patients with neck and/or low back pain referred to specialist care: a randomized clinical trial. JAMA Network Open. 2023;6(6):e2320400. doi:10.1001/jamanetworkopen.2023.20400
89. Overton M, Ward S, Swain N, et al. Are ecological momentary assessments of pain valid and reliable? A systematic review and meta-analysis. Clin J Pain. 2023;39(1):29. doi:10.1097/AJP.0000000000001084
90. Mohr DC, Zhang M, Schueller SM. Personal sensing: understanding mental health using ubiquitous sensors and machine learning. Annu Rev Clin Psychol. 2017;13:23–47. doi:10.1146/annurev-clinpsy-032816-044949
91. Xie Q, Amo V, Nahum-Shani I, Goldberg SB. Using digital technology to increase integration of meditation into daily life: the case for meditation-based ecological momentary interventions. J Technol Behav Sci. 2025. doi:10.1007/s41347-025-00568-1
92. Allvin R, Fjordkvist E, Blomberg K. Struggling to be seen and understood as a person – chronic back pain patients’ experiences of encounters in health care: an interview study. Nurs Open. 2019;6(3):1047–1054. doi:10.1002/nop2.290
93. Lyon AR, Koerner K. User-centered design for psychosocial intervention development and implementation. Clin Psychol. 2016;23(2):180–200. doi:10.1111/cpsp.12154
94. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):50. doi:10.1186/1748-5908-4-50
95. Maizes V, Rakel D, Niemiec C. Integrative medicine and patient-centered care. Explore. 2009;5(5):277–289. doi:10.1016/j.explore.2009.06.008
96. Quanbeck A, Hennessy RG, Park L. Applying concepts from “rapid” and “agile” implementation to advance implementation research. Implement Sci Commun. 2022;3(1):118. doi:10.1186/s43058-022-00366-3
97. Stewart RE, Beidas RS, Last BS, et al. Applying NUDGE to inform design of EBP implementation strategies in community mental health settings. Adm Policy Ment Health. 2021;48(1):131–142. doi:10.1007/s10488-020-01052-z
98. Saldana L, Ritzwoller DP, Campbell M, Block EP. Using economic evaluations in implementation science to increase transparency in costs and outcomes for organizational decision-makers. Implement Sci Commun. 2022;3(1):40. doi:10.1186/s43058-022-00295-1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Randomized, Double-Blind, Placebo-Controlled Trial to Evaluate the Therapeutic Effect of Magnesium-L-Threonate Supplementation for Persistent Pain After Breast Cancer Surgery
Ni Y, Deng F, Yu S, Zhang J, Zhang X, Huang D, Zhou H
Breast Cancer: Targets and Therapy 2023, 15:495-504
Published Date: 25 July 2023
Awareness and Predictors of the Use of Bioinformatics in Genome Research in Saudi Arabia
Alomair L, Abolfotouh MA
International Journal of General Medicine 2023, 16:3413-3425
Published Date: 11 August 2023