Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Role of Community Pharmacist in Asthma Management: Knowledge, Attitudes and Practice
Authors Jarab AS ![]() , Al-Qerem W
, Al-Qerem W ![]() , Alzoubi KH
, Alzoubi KH ![]() , Almomani N, Abu Heshmeh SR
, Almomani N, Abu Heshmeh SR ![]() , Mukattash TL
, Mukattash TL ![]() , Al Hamarneh YN, Al Momany EM
, Al Hamarneh YN, Al Momany EM ![]()
Received 28 September 2023
Accepted for publication 13 December 2023
Published 3 January 2024 Volume 2024:17 Pages 11—19
DOI https://doi.org/10.2147/JMDH.S442396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Anan S Jarab,1– 3 Walid Al-Qerem,4 Karem H Alzoubi,5,6 Nadeen Almomani,1 Shrouq Riad Abu Heshmeh,1 Tareq L Mukattash,1 Yazid N Al Hamarneh,7 Enaam M Al Momany8
1Department of Clinical Pharmacy, Faculty of Pharmacy, Jordan University of Science and Technology, Irbid, Jordan; 2College of Pharmacy, Al Ain University, Abu Dhabi, United Arab Emirates; 3AAU Health and Biomedical Research Center, Al Ain University, Abu Dhabi, United Arab Emirates; 4Department of Pharmacy, Al-Zaytoonah University of Jordan, Amman, Jordan; 5Department of Pharmacy Practice and Pharmacotherapeutics, University of Sharjah, Sharjah, United Arab Emirates; 6Faculty of Pharmacy, Jordan University of Science and Technology, Irbid, Jordan; 7Department of Pharmacology, University of Alberta, Edmonton, AB, Canada; 8Department of Clinical Pharmacy and Pharmacy Practice, Faculty of Pharmaceutical Sciences, The Hashemite University, Zarqa, Jordan
Correspondence: Enaam M Al Momany, Department of Clinical Pharmacy and Pharmacy Practice, Faculty of Pharmaceutical Sciences, The Hashemite University, Zarqa, Jordan, Email [email protected]
Purpose: To investigate knowledge, attitude, and practice of asthma management counseling and the perceived barriers by community pharmacists.
Methods: This cross-sectional study was conducted on 416 community pharmacists using an online-based questionnaire. The questionnaire included five parts that assessed socio-demographics and medical references used to seek drug-related information, pharmacists’ knowledge (7 items), attitudes (5 items), practice (22 items) and the barriers for the provision of asthma management counseling (10 items). Binary logistic regression was conducted to find the variables that were significantly and independently associated with knowledge, attitude and asthma management counseling practice.
Results: Increased years of experience was associated with decreased knowledge (OR = 0.918, 95% Cl (0.869:0.970), P = 0.002) and less positive attitude toward asthma management (OR = 0.876, 95% Cl. (0.821:0.935), P < 0.001), while working in independent community pharmacy (OR = 2.097, 95% Cl. (1.273:3.454), P = 0.004) and increased awareness of asthma management guidelines (OR = 1.60, 95% CI. (1.044:2.453), P = 0.031) increased the odds of being in the high knowledge group. In contrast, increasing the daily number of pharmacy visitors OR = 1.009, 95% Cl. (1.001:1.016), P = 0.024) and having a pharmacy degree (OR = 2.330, 95% Cl. (1.256:4.326), P = 0.007) increased the odds of having a positive attitude. Male pharmacists (OR = 0.553, 95% Cl. (0.350:0.873), P = 0.011) and having bachelor in pharmacy (OR = 0.354, 95% Cl. (0.179:0.700), P = 0.003) decreased the odds of being in the high practice group. On the other hand, increased awareness of asthma management guidelines tripled the odds of being in the high practice group (OR = 3.067, 95% Cl. (1.964:4.787), P < 0.001).
Conclusion: The current study findings offer valuable insights into the gaps in knowledge, attitude, and practice of asthma management counseling among community pharmacists, as well as the barriers and factors that impede the provision of these services. These insights serve as a guide for developing future strategies aimed at enhancing the role of pharmacists in asthma care.
Keywords: pharmacist, asthma, knowledge, attitude, counseling, practice
Introduction
Asthma is a common airway disease of children and adults that is marked by chronic airway inflammation and narrowing.1,2 In the Eastern Mediterranean Region, asthma prevalence in adults is 8% according to the World Health Organization.3 In Jordan, asthma prevalence was estimated to be at 10% among the elderly,4 2.38% among schoolchildren,5 and 6.2% among high school students.6
The control of asthma has been reported to be low in many countries.1,2,7,8 In a large-scale investigation of adult asthma control in the Middle East and North Africa, less than 30% of asthmatics were controlled with about 42% being uncontrolled.7 Similar results were reported in a previous study conducted in Northern Jordan,9 while in Southern Jordan, asthma control among adults was documented to be 45.2%.10 The high proportion of uncontrolled asthmatic patients increases its burden, which can be mitigated by proper management including follow up and effective education, measures that basically can occur in the primary healthcare settings including community pharmacies.11
Pharmacists can play a significant role in the management of chronic diseases including asthma.12 Due to their clinical expertise, pharmacists are well-equipped to educate asthmatic patients about their medical condition, explain the functionality of asthma medications, demonstrate correct inhalation techniques, address any concerns regarding potential side effects, and promote adherence to prescribed therapies. This positions them uniquely to contribute to optimal clinical outcomes for individuals with asthma.13 A randomized controlled clinical trial showed that a structured evidence-based pharmacist-delivered asthma management service significantly enhanced patients’ medication use, inhaler technique, and quality of life.14 The present study aimed to highlight several aspects related to real-life asthma management, namely the roles of Jordanian pharmacists in relation to their evidence-based up-to-date knowledge, their attitudes toward asthma management, and the practices of the proper use of inhaler devices and asthmatic patient care. In addition, it provides valuable insights into the perceived pharmacists’ barriers for providing asthma management counseling.
Methods
Study Design and Participants
This cross-sectional study was conducted among community pharmacists in Jordan in the period from December 2022 through March 2023 using a convenient sampling technique. Pharmacists were eligible to be included in the study if they graduated from universities recognized by the Ministry of Higher Education and received permission to practice as community pharmacists by the Ministry of Health and the Jordanian Pharmaceutical Association. Pharmacists who agreed to participate in the study were asked to sign an informed consent form.
Study Instruments
After extensive review of the related literature,15–17 the current self-administered, online survey was developed. The survey started with a small paragraph, which described the study objective and assured the confidentiality of the study findings. The questionnaire comprised of five main sections: Socio-demographic information of the community pharmacists, items related to medical references used to seek drug-related information, pharmacists’ knowledge about asthma management (7 items), pharmacists’ attitude towards asthma management (5 items), asthma management practice (22 items) and the barriers for the provision of asthma management (10 items). In both attitude and barriers scale, the participants were asked to show the level of agreement on a 5-Likert scale from strongly disagree to strongly agree. In the 22-item practice section, the pharmacists were asked to indicate how frequently they provide each service on a 5-point Likert scale ranging from never to always. These points were summed to calculate subscale scores of the instrument. An expert panel of different background, that is, a pulmonologist, general physician, and two pharmacy professors examined the questionnaire for face and content validity. Ten community pharmacists participated in a pilot test to evaluate clarity, relevance, and completion time. The final data analysis did not contain any of the data collected during the pilot test. Cronbach’s alpha test was conducted to evaluate the internal consistency of the survey scales including knowledge (0.52), attitude (0.70), practice (0.913) and the barriers (0.80).
Statistical Analysis
Statistical analyses were performed using SPSS version 28. Categorical variables were presented as frequencies and percentages, and continuous variables as medians (25–75 percentiles). Cronbach’s alpha test was conducted to assess the internal consistency of the survey domains including knowledge, attitudes, practice, and barriers. Except for knowledge, were acceptable value ≥0.5 as lower values are expected in binary data, acceptable internal consistency was determined at Cronbach’s alpha ≥0.7. The participants were categorized into high/low groups in the knowledge, attitude, and practice point after considering the median value as a cut point. Binary logistic regression was conducted to explore the variables associated with knowledge, attitude, and practice domains. Significance was determined at p-value <0.05.
Results
The present study enrolled 416 pharmacists (51.7% female); the median age was 28 (26–37) years. Most of the enrolled participants had bachelor’s degree of pharmacy (84.7%), did not have postgrad degree (70.2%) and had internet connection. The median for the daily average of patients served was 35 (25–50) and the median for the daily average prescriptions was 10 (7–20). Other socio-demographics are presented in Table 1.
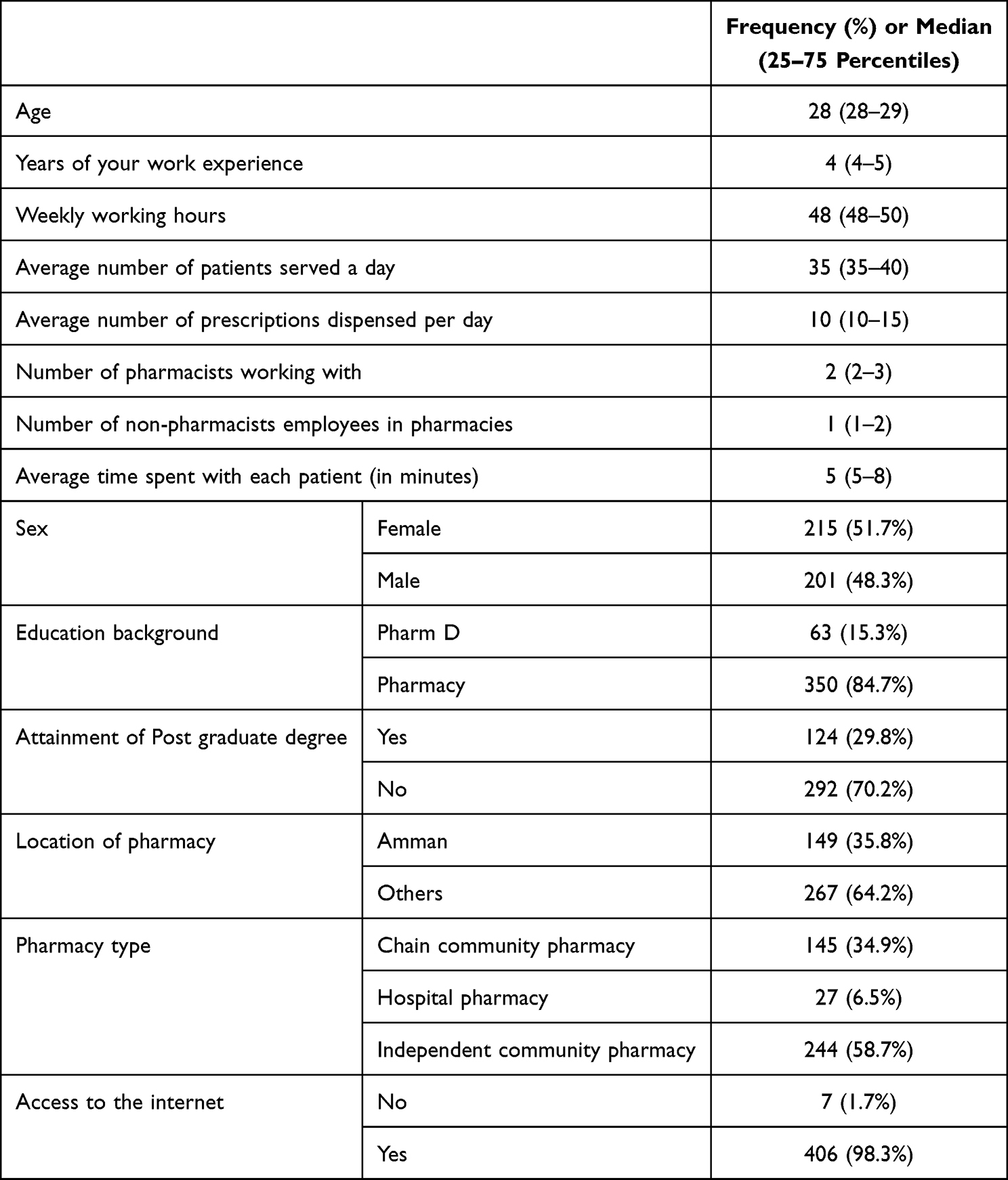 |
Table 1 Sociodemographic Characteristics of the Study Participants (n = 416) |
Figure 1 illustrates the source of information reported by the enrolled participants for asthma management. The most used source of information was the internet (80.3%) followed by Lexicomp (39.4%), while the least used one was Martindale (1.9%). Ten pharmacists reported that they did not use any source of information for asthma management.
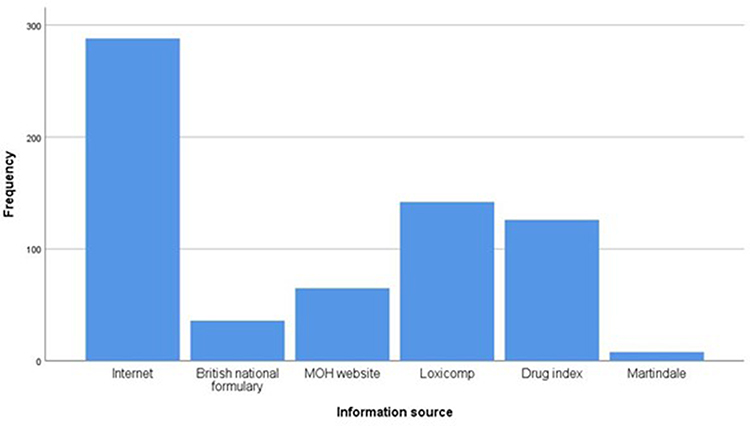 |
Figure 1 Sources of information for asthma management. |
The median of the actual knowledge score was 4 (4–5) out of a maximum possible score of 7. Accordingly, 42.9% of the participants were in the low knowledge group, while 57.5% were in the high knowledge group. As shown in Table 2, 63.2% of the participants were familiar with the symptoms and treatment options of asthma, 54.3% were aware about the most recent asthma treatment guidelines, 51.2% were able to assess the severity of asthma and only 30.3% recognized the proper use of the peak flow meter. The participants reported poor knowledge regarding “SABA-only therapy raises the danger of life-threatening exacerbations and deaths due to asthma” (70.2%), “using Steroid inhalation can significantly affect child’s growth” (68%), and “To reduce the risk of infection transmission during epidemics, patients should avoid using nebulizers as much as possible” (66.1%).
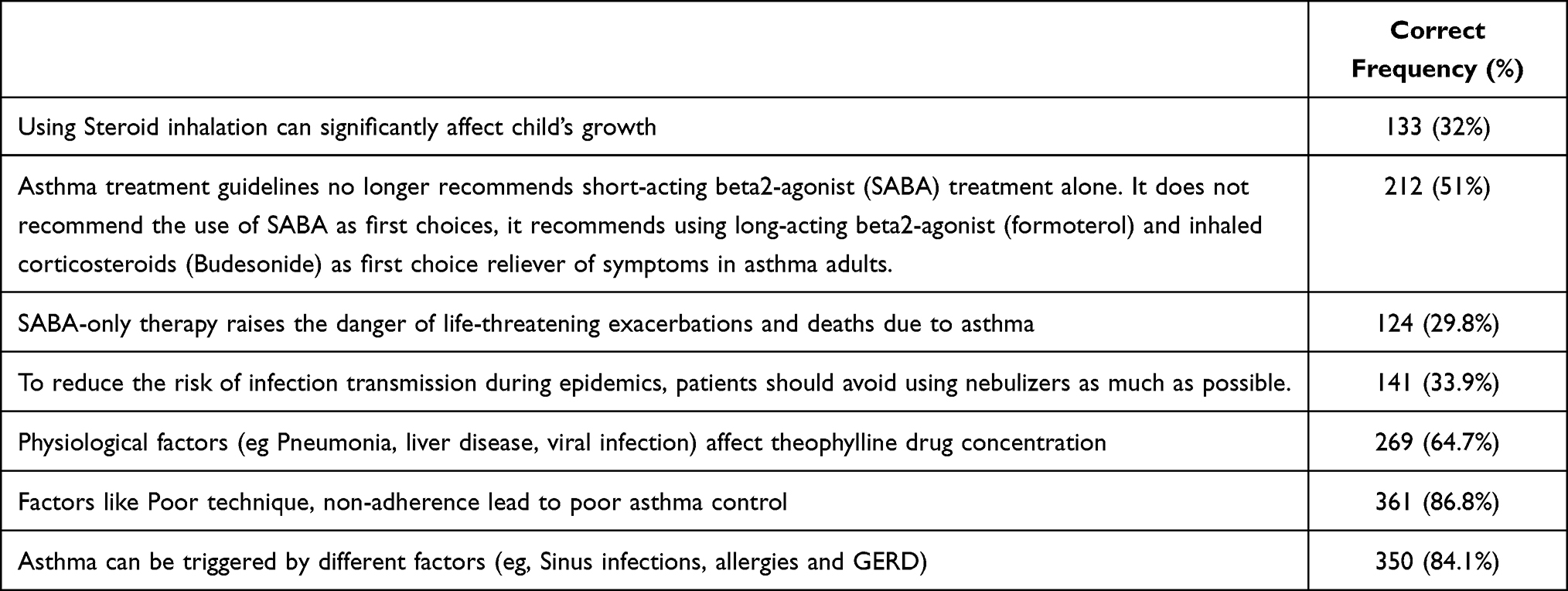 |
Table 2 Knowledge About Asthma Management (n = 416) |
As shown in Table 3, the median of the attitude score was 19 (19–20) out of maximum possible score of 25. Hence, 44.5% of the participants were in the low attitude group, while 55.5% were in the high attitude group. Except for the item “asthmatic patients may benefit from disease monitoring with peak flow meter” that had a median of three (3–4), all other items had a median of four (3–4).
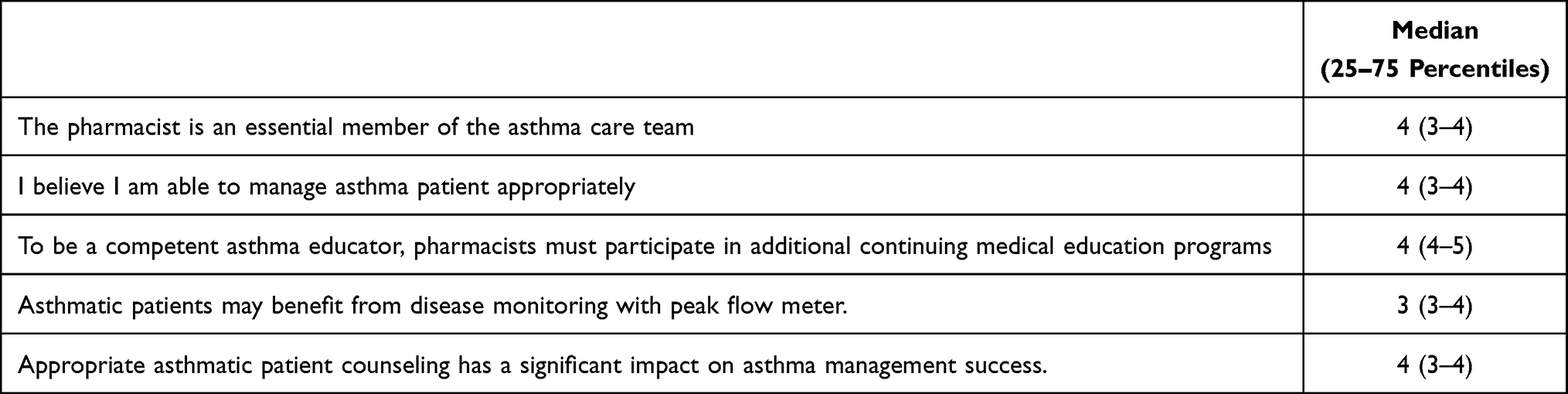 |
Table 3 Attitudes Toward Asthma Management and Counseling (n = 416) |
The median of the practice score was 76 (76–79) out of maximum possible score of 110. Accordingly, 45.2% of the participants were in the low practice group, while 54.8% were in the high practice group. As shown in Table 4, the most frequently provided instructions were “I advise asthmatic patients to take their inhaled corticosteroids on a regular basis” 4(3–4), and “I advise asthmatic patients to consult me before discontinuing any medication” 4 (3–4). On the other hand, the least frequently provided instruction was scheduling a follow-up visit for asthma patients who have been under control for the last 3 months 2 (1–3). As shown in Table 5, all the reported barriers for providing asthma management at the community pharmacy had a median of three.
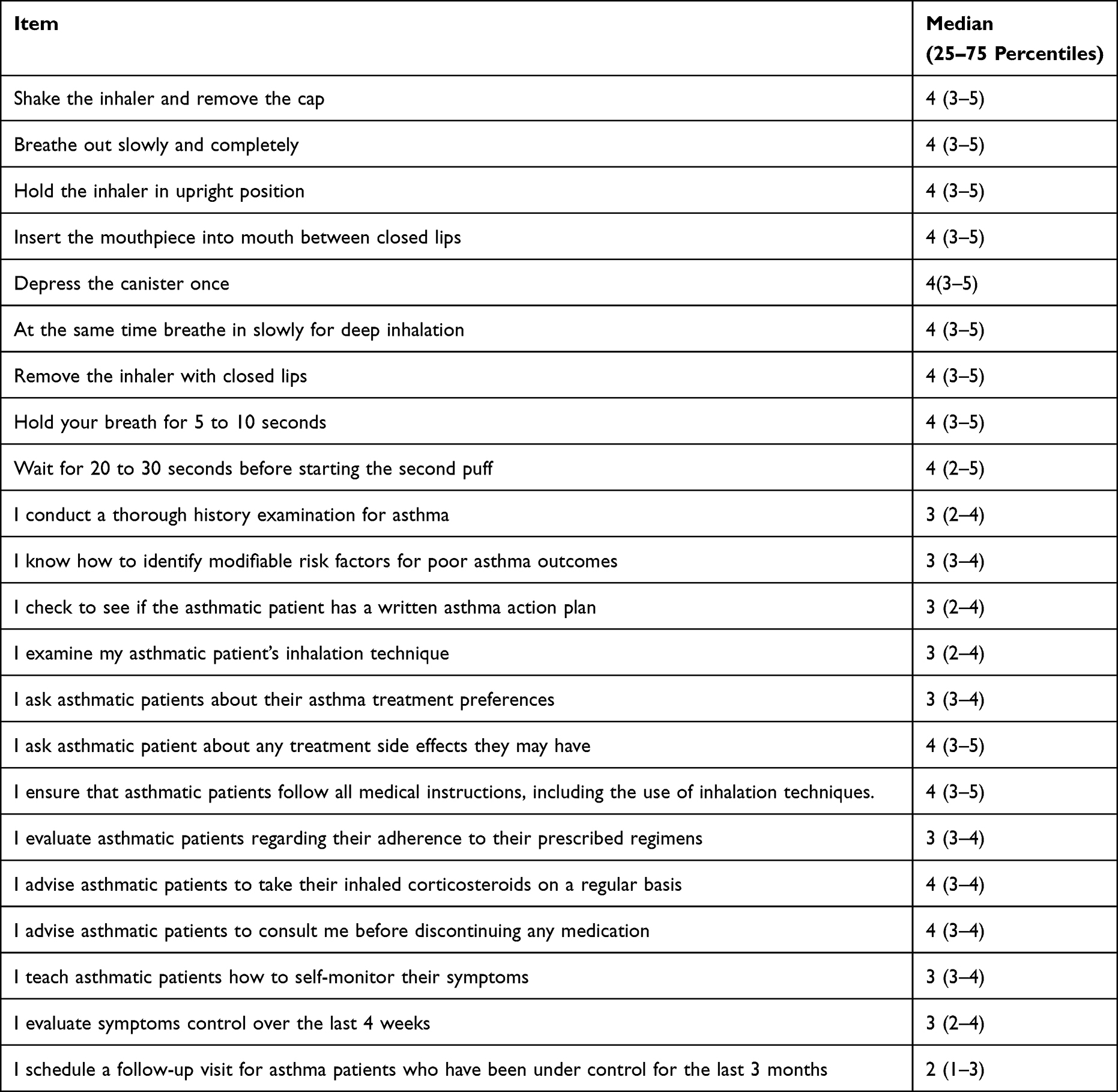 |
Table 4 Practice of Asthma Management Counseling (n = 416) |
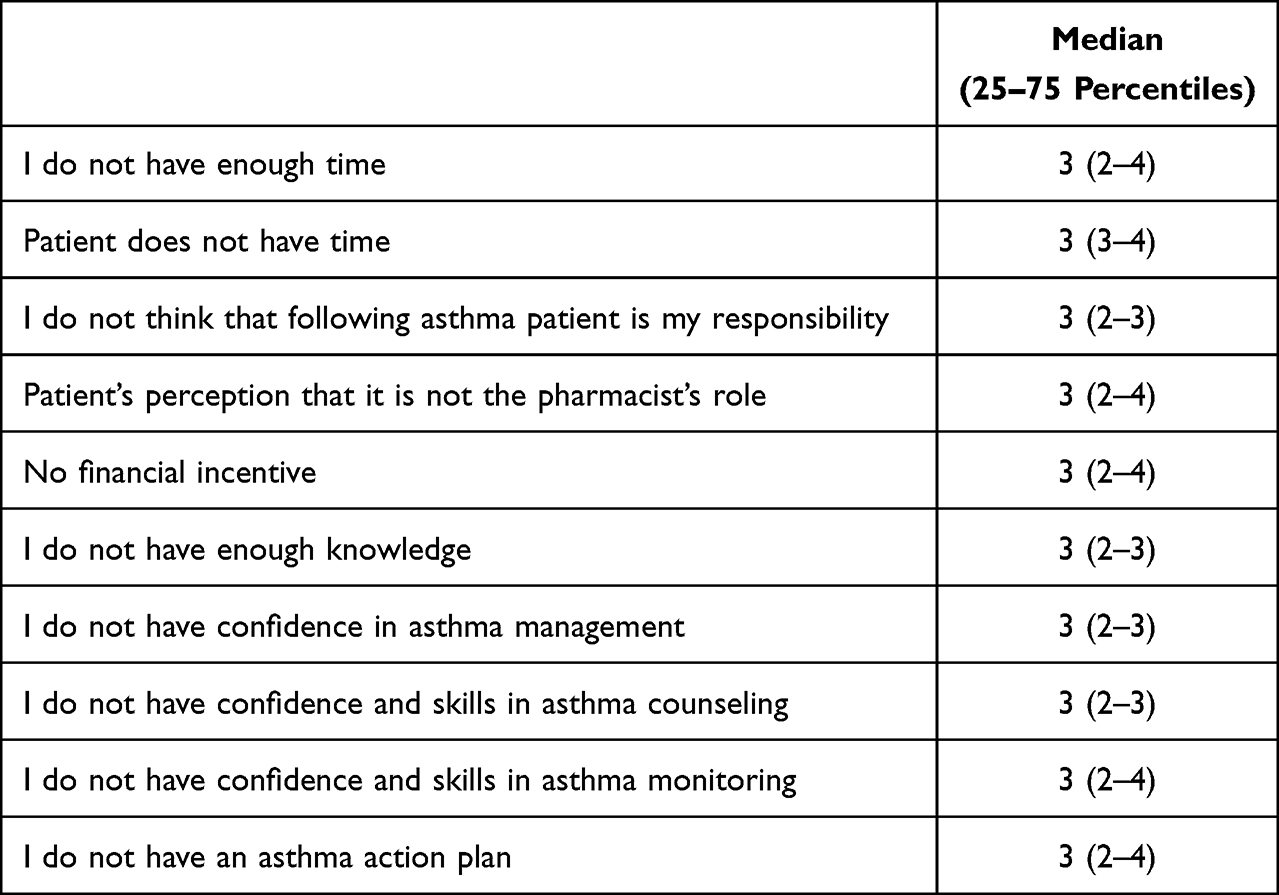 |
Table 5 Barriers for Providing Asthma Management Counseling (n = 416) |
Regression analysis showed that pharmacists with higher years of experience had significantly less odds to be in the high knowledge group (OR = 0.918, 95% Cl (0.869:0.970), P = 0.002), while working in independent community pharmacy doubled the odds of being in the high knowledge group (OR = 2.097, 95% Cl. (1.273:3.454), P = 0.004). Having high awareness of asthma management guidelines significantly increased the odds of being in the high knowledge group (OR = 1.60, 95% CI. (1.044:2.453), P = 0.031). Increased years of experience significantly decreased the odds of having positive attitude toward asthma management (OR = 0.876, 95% Cl. (0.821:0.935), P < 0.001). In contrast, increasing the daily number of pharmacy visitors significantly increased the odds of having positive attitude (OR = 1.009, 95% Cl. (1.001:1.016), P = 0.024). Furthermore, having a pharmacy degree doubled the odds of being in the high attitude group when compared to those who had a Pharm D degree (OR = 2.330, 95% Cl. (1.256:4.326), P = 0.007). Results also showed that male pharmacists tended to provide less asthma management instructions to their patients when compared to females (OR = 0.553, 95% Cl. (0.350:0.873), P = 0.011). Moreover, having bachelor in pharmacy decreased the odds of being in the high practice group when compared with Pharm D holders (OR = 0.354, 95% Cl. (0.179:0.700), P = 0.003), while pharmacists with improved awareness of asthma management guidelines significantly tripled the odds of being in the high practice group (OR = 3.067, 95% Cl. (1.964:4.787), P < 0.001).
Discussion
The study pharmacists demonstrated poor knowledge in different aspects of asthma management. Similarly, earlier studies reported poor pharmacists’ knowledge, skills, and confidence in asthma management which was an obstacle to effectively intervene in patient care.18–22 The sub-optimal pharmacists’ knowledge could be attributed to the traditional pharmacists’ role of dispensing medications without focus on providing patient-centered care.23 Moreover, the insufficient utilization and limited diversity of information sources might have also contributed to this knowledge gap observed in our study. Based on these findings, it is crucial to reorient the role of pharmacists from a mere focus on medication dispensing to providing patient-centered care. This involves actively engaging with patients, conducting comprehensive medication reviews, offering education on asthma management techniques, and addressing patients’ concerns and inquiries. Furthermore, it is essential to encourage pharmacists to diversify their sources of information to stay updated with the latest evidence-based practices in asthma management.
Although more than half of the pharmacists showed a positive attitude towards asthma counseling, the majority did not recognize the benefit of peak flow meter in terms of asthma monitoring. In earlier studies, pharmacists reported low levels of peak flow meter use for asthmatic patients monitoring.13,24 Other studies showed that pharmacists were not having peak flow meters in their workplace.25,26 Furthermore, our study revealed that only 50.5% of the pharmacists felt confident in managing asthma patients appropriately. These findings underscore the need for targeted education and training programs aimed at enhancing pharmacists’ attitudes towards asthma management.
Results revealed poor counseling practice in the majority of asthma management items, particularly in terms of elaborating asthma treatment preferences and scheduling a follow-up visit for patients who have been under control for the past 3 months. One explanation suggests that pharmacists might provide more focus on patients with new prescriptions than monitoring patients with refills in terms of medications’ counseling and education and follow-up.27–29 In addition, pharmacists might believe that their role in patient care is summarized in providing medication information and so their focus would be on new prescriptions rather than therapy monitoring and follow-up, or elaborating asthma treatment preferences.30 Previous research found that asthmatic patients who experience discordant relationships with their physicians exhibit markedly poorer asthma control compared to those with concordant relationships.31 This highlights the need for developing tailored strategies to smooth the relationship between patients and different healthcare providers, including doctors and pharmacists. Such strategies should include a patient-centered approach in counseling sessions that actively involves patients in making treatment decisions and takes into account their preferences, worries, and aspirations. Open lines of communication between patients and medical professionals, proactive and frequent discussions regarding treatment options and possible side effects, and clearing up any misunderstandings or doubts are also crucial.
Lack of time by the patients, lack of incentives for pharmacists, and unavailable asthma action plan were the most reported barriers for asthma counseling in the present study. Reported barriers in the literature included pharmacists’ insufficient knowledge, skills, and confidence, lack of proper education and training, time constraints to provide effective pharmaceutical care, and lack of financial incentives.19–21,24,32,33 Furthermore, most of the pharmacists in a Canadian study did not talk to patients about asthma action plan.27 The perceived low values in asthma action plan by healthcare professionals explained why these plans were not kept updated.34,35
Pharmacists working in single pharmacies showed better knowledge about asthma management when compared to pharmacists working in hospital or chain pharmacies. The single pharmacy is usually a locally owned family business where pharmacists tend to care more about the customers who are probably in the neighborhood. On the other hand, pharmacists with more years of experience were less likely to have high knowledge or positive attitude towards asthma counseling. The knowledge of pharmacists with longer years of experience may not be up-to-date, particularly in terms of recent treatment guidelines due to the lack of continuous education and training, a factor that was positively associated with asthma knowledge in this study, which might also have affected their attitudes towards asthma counseling in the current study. On the other hand, pharmacy is a noble profession, which provides services that improve health and well-being, and so the increased number of pharmacy visitors may have encouraged the staff positive attitude. As Pharm D graduates are more clinically oriented, pharmacy graduates reported less counseling practice in the present study. However, this inferiority might have developed the sense of competition, which stimulated them to improve clinical skills and competencies, which might have contributed to the high attitude reported by Pharmacy graduates in the present study. Lastly, factors that suggest a high level of asthma care practice were being highly aware of asthma management guidelines, and being a female pharmacist. Female pharmacists’ perceived superiority in asthma management practice might be attributed to various factors. One such factor is communication skills, as female pharmacists may possess an inherent ability to establish effective communication and provide comprehensive counseling to their patients.36 Another contributing factor could be the greater job satisfaction reported by females working in healthcare sectors.37 Higher job satisfaction levels may foster a more positive attitude and motivation, resulting in increased dedication to providing comprehensive services, including asthma management.
Strengths and Weaknesses
The study included a large number of community pharmacists, increasing the reliability and generalizability of the findings. In addition, the research questionnaire employed a thorough approach, covering a wide range of areas, including knowledge, attitudes, practices, and perceived barriers. This allows for a more in-depth understanding of the factors influencing asthma management counseling. The assessment of barriers, in particular, holds paramount importance for developing targeted interventions. By utilizing multivariate regression analysis to determine variables associated with practice, attitude, and knowledge, the study goes beyond simple evaluation and produces more reliable and robust findings. On the other hand, the cross-sectional design utilized in this study limits the ability to establish causation. Furthermore, the reliance on self-reported data from pharmacists may introduce social-desirability bias. Moreover, the use of an online-based questionnaire could lead to selection bias because it might draw participants who are more adept at technology or who have a particular interest in the subject, which could affect how representative the study sample is.
Conclusion
The current findings highlight specific areas in community pharmacists’ knowledge, attitude, and asthma counseling practice that need improvement. To tackle these areas effectively, it is crucial to involve pharmacists in educational and training programs that focus on asthma care. Moreover, the development and implementation of continuing education programs that equip the pharmacists with the most updated asthma management guidelines, treatment options, and counseling techniques.
Ethics Approval
The research meets the ethical guidelines and adhere to the legal requirements of Jordan. This research activity has been exempted from full application for ethical approval (Reference No.: COP/AREC/AD/30) by AAU Research Ethical Committee).
Acknowledgments
The authors wish to thank the Deanship of Research at Jordan University of Science and Technology for sponsoring this research work. The authors also thank all the community pharmacists who completed the study questionnaire.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Deanship of Research at Jordan University of Science and Technology supported this work [Research Grant Number: 20220508].
Disclosure
The authors declare no conflicts of interest in this work.
References
1. 2022 GINA Main Report - Global Initiative for Asthma - GINA. Available from: https://ginasthma.org/gina-reports/.
2. World Health Organization. Asthma; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/asthma.
3. Global Asthma Network. The Global Asthma Report 2022. Int J Tuberc Lung Dis. 2022;26(1):1–104. doi:10.5588/ijtld.22.1010
4. The Hashemite Kingdom of Jordan. High Council of Health. The National Strategy for Health Sector in Jordan 2015–2019; 2015.
5. Nour A, Alsayed AR, Basheti I. Prevalence of asthma amongst schoolchildren in Jordan and staff readiness to help. Healthcare (Switzerland). 2023;11(2):1–9. doi:10.3390/healthcare11020183
6. Al-sheyab NA, Alomari MA. Prevalence, associated factors, and control level of asthma symptoms among adolescents in Northern Jordan. Int J Adolesc Med Health. 2020;32(3). doi:10.1515/ijamh-2017-0159
7. Tarraf H, Al-Jahdali H, Al Qaseer AH, et al. Asthma control in adults in the Middle East and North Africa: results from the ESMAA study. Respir Med. 2018;138:64–73. doi:10.1016/j.rmed.2018.03.024
8. Al-Qerem W, Jarab A, Abu Heshmeh SR, Ling J. Variables associated with asthma control among adult patients. J Asthma. 2023;60(7):1290–1298. doi:10.1080/02770903.2022.2144351
9. Almomani BA, Al-Sawalha NA, Samrah SM, Gamble JM, Al Momani MA. Asthma insights from Jordan: cross-sectional observational study. J Asthma. 2016;53(4):349–355. doi:10.3109/02770903.2015.1121493
10. Albataineh E, Al-Zayadneh E, Al-Shagahin H, AL Soloman A, Altarawneh A, Aldmour I. Asthma Control and Its Predictive Factors in Adult Asthma Patients. J Clin Med Res. 2019;11(12):807–817. doi:10.14740/jocmr4021
11. Turcotte C, Fénélon-Dimanche R, Lemière C, et al. Development of a community pharmacy-based intervention for patients with uncontrolled asthma. Explor Res Clin Soc Pharm. 2022;7:100167. doi:10.1016/j.rcsop.2022.100167
12. Akour A, Elayeh E, Tubeileh R, Hammad A, Ya'Acoub R, Al-Tammemi AB. Role of community pharmacists in medication management during COVID-19 lockdown. Pathog Glob Health. 2021;115(3):168–177. doi:10.1080/20477724.2021.1884806
13. Bridgeman MB, Wilken LA. Essential role of pharmacists in asthma care and management. J Pharm Pract. 2021;34(1):149–162. doi:10.1177/0897190020927274
14. Serhal S, Saini B, Bosnic-Anticevich S, et al. A targeted approach to improve asthma control using community pharmacists. Front Pharmacol. 2021;12:1–16. doi:10.3389/fphar.2021.798263
15. Khan TM, Azhar S. A study investigating the community pharmacist knowledge about the appropriate use of inhaler, Eastern Region AlAhsa, Saudi Arabia. Saudi Pharm J. 2013;21(2):153–157. doi:10.1016/j.jsps.2012.07.004
16. Paravattil B, Kheir N, Yousif A. Utilization of simulated patients to assess diabetes and asthma counseling practices among community pharmacists in Qatar. Int J Clin Pharm. 2017;39(4):759–768. doi:10.1007/s11096-017-0469-8
17. Alghadeer SM, Mayet AY, Babelghaith SD, et al. Evaluation of knowledge and attitude towards asthma care in hospital and community pharmacy settings at central Saudi Arabia. Int J Green Pharm. 2015;9(4):S79–S85.
18. Nguyen TS, Nguyen TLH, Van Pham TT, et al. Effectiveness of a short training program for community pharmacists to improve knowledge and practice of asthma counselling – a simulated patient study. Respir Med. 2018;144:50–60. doi:10.1016/j.rmed.2018.10.003
19. Gemicioglu B, Borekci S, Can G. Investigation of knowledge of asthma and inhaler devices in pharmacy workers. J Asthma. 2014;51(9):982–988. doi:10.3109/02770903.2014.928310
20. Kritikos V, Reddel H, Bosnic-Anticevich S. Pharmacists’ perceptions of their role in asthma management and barriers to the provision of asthma services. Int J Pharm Pract. 2010;18(4):209–216. doi:10.1211/ijpp.18.04.0005.x
21. Casset A, Meunier-Spitz M, Rebotier P, et al. Asthma management and inhalation techniques among community pharmacists in 2009: a comparison with the 1999 survey. J Asthma. 2014;51(9):964–973. doi:10.3109/02770903.2014.936446
22. Nduka S, Anetoh M, Amorha K, Henry O, Okonta M. Use of simulated patient approach to assess the community pharmacists′ knowledge of appropriate use of metered dose inhaler. J Basic Clin Pharm. 2016;7(4):116. doi:10.4103/0976-0105.189435
23. Nazer LH, Tuffaha H. Health care and pharmacy practice in Jordan. Can J Hosp Pharm. 2017;70(2):150–155. doi:10.4212/CJHP.V70I2.1649
24. Said ASA, Hussain N, Kharaba Z, Al Haddad AHI, Abdelaty LN, Hussein RRS. Knowledge, attitude, and practice of pharmacists regarding asthma management: a cross-sectional study in Egypt. J Pharm Policy Pract. 2022;15(1):38. doi:10.1186/s40545-022-00436-w
25. Amorha KC, Idoko KE, Okonta MJ, Ukwe CV. Knowledge and practice of the global initiative for asthma report among community pharmacists in a Nigerian state. Pan Afr Med J. 2020;37(83):1–11. doi:10.11604/pamj.2020.37.83.18897
26. Banh HL, Ahmadi E, Cave A. Are peak flow meters readily available in community pharmacies? Can Pharm J. 2016;149(4):216–218. doi:10.1177/1715163516651278
27. Guirguis LM. Assessing the knowledge to practice gap: the asthma practices of community pharmacists. Can Pharm J. 2018;151(1):62–70. doi:10.1177/1715163517742162
28. Puspitasari HP, Aslani P, Krass I. A review of counseling practices on prescription medicines in community pharmacies. Res Soc Adm Pharm. 2009;5(3):197–210. doi:10.1016/j.sapharm.2008.08.006
29. Kaae S, Mygind A, Saleem S. A characterization of the current communication patterns in Danish community pharmacies – an observational study. Res Soc Adm Pharm. 2013;9(6):958–964. doi:10.1016/j.sapharm.2012.10.003
30. Guirguis LM, Chewning BA. Role theory: literature review and implications for patient-pharmacist interactions. Res Soc Adm Pharm. 2005;1(4):483–507. doi:10.1016/j.sapharm.2005.09.006
31. Matsunaga K, Hamada K, Oishi K, Yano M, Yamaji Y, Hirano T. Factors associated with physician-patient discordance in the perception of asthma control. J Allergy Clin Immunol Pract. 2019;7(8):2634–2641. doi:10.1016/j.jaip.2019.04.046
32. Aburuz S, Al-Ghazawi M, Snyder A. Pharmaceutical care in a community-based practice setting in Jordan: where are we now with our attitudes and perceived barriers? Int J Pharm Pract. 2012;20(2):71–79. doi:10.1111/j.2042-7174.2011.00164.x
33. Akram W, Ijaz N, Ahmad H, Jamshaid M, Ismail NE. Barriers to the provision of asthma services and perceived practice towards asthma management among urban community pharmacists in Selangor, Malaysia. Braz J Pharm Sci. 2018;54(4). doi:10.1590/s2175-97902018000417324
34. Ring N, Booth H, Wilson C, et al. The ‘vicious cycle’ of personalised asthma action plan implementation in primary care: a qualitative study of patients and health professionals’ views. BMC Fam Pract. 2015;16(1):145. doi:10.1186/s12875-015-0352-4
35. Charrois T, Newman S, Sin D, Senthilselvan A, Tsuyuki RT. Improving asthma symptom control in rural communities: the design of the Better Respiratory Education and Asthma Treatment in Hinton and Edson study. Control Clin Trials. 2004;25(5):502–514. doi:10.1016/j.cct.2004.07.004
36. Hansen JW. Science explains why women are better at communicating than men; September 10, 2014. Available from: https://www.linkedin.com/pulse/20140910124447-15318179-science-explains-why-women-are-better-at-communicating-than-men.
37. Berlin G, Darino L, Greenfield M, Starikova I. Women in the healthcare industry; June 7, 2019. Available from: https://www.mckinsey.com/industries/healthcare/our-insights/women-in-The-healthcare-industry.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Managing Pain in Low Resource Settings: Healthcare Professionals’ Knowledge, Attitude and Practice Regarding Pain Management in Western Nepal
Thapa P, KC B, Lee SWH, Dujaili JA, Gyawali S, Mohamed Ibrahim MI, Alrasheedy AA
Journal of Pain Research 2022, 15:1587-1599
Published Date: 2 June 2022
Knowledge, Attitudes, and Practices Regarding Ergonomic Hazards Among Healthcare Workers in a Saudi Government Hospital

ALHazim SS, Al-Otaibi ST, Herzallah NH
Journal of Multidisciplinary Healthcare 2022, 15:1771-1778
Published Date: 24 August 2022
Critical Care Nurses’ Knowledge, Attitudes, and Practices Regarding Pressure Injury Treatment: A Nationwide Cross-Sectional Survey
Li J, Zhu C, Liu Y, Song B, Jin J, Liu Y, Wen X, Cheng S, Wu X
Risk Management and Healthcare Policy 2022, 15:2125-2134
Published Date: 16 November 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024