Back to Journals » Clinical Interventions in Aging » Volume 21
Malnutrition, Frailty, and High Fall Risk in Older Adults: Examining Their Interactive Effects in a Cross-Sectional Study
Authors Wen H, Liang H ![]() , Mao Q, Yang S
, Mao Q, Yang S ![]() , Yuan X
, Yuan X
Received 17 March 2026
Accepted for publication 26 June 2026
Published 9 July 2026 Volume 2026:21 609884
DOI https://doi.org/10.2147/CIA.S609884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Honghong Wen,1,2 Heting Liang,1 Qingyun Mao,2 Shaoting Yang,2 Xiaoli Yuan1
1Department of Nursing, Affiliated Hospital of Zunyi Medical University, Zunyi, Guizhou, People’s Republic of China; 2Faculty of Nursing, Zunyi Medical University, Zunyi, Guizhou, People’s Republic of China
Correspondence: Xiaoli Yuan, Email [email protected]
Background: Falls are a major public health concern for older adults, impacting health. Frailty and malnutrition are widely studied variables closely linked to fall risk. While the individual links of these factors with fall risk are known, their combined effects and quantitative relationships remain poorly understood. This study aimed to explore the interactive effects of malnutrition and frailty on fall risk among older adults.
Methods: This study involved the recruitment of 13,970 older adults from 10 communities, who were assessed using the frailty score, the Mini-Nutritional Assessment Scale, and the STEADI tool. Multiplicative interactions were calculated through logistic regression. Additive interactions were evaluated using the relative excess risk (RERI), attribution ratio (AP), and synergy index (SI).
Results: 24.1% of participants were identified as having high fall risk. Frailty and malnutrition each independently correlate with fall risk. Compared with participants who were non-frail and well-nourished, those with coexisting frailty and malnutrition had significantly higher odds of high fall risk (OR = 15.83, 95% CI: 11.77– 21.28). A significant multiplicative interaction between frailty and malnutrition was confirmed (OR = 1.064, 95% CI: 1.047– 1.082). Significant positive additive interaction was also identified: RERI = 1.58 (95% CI: 0.19– 2.96), AP = 0.10 (95% CI: 0.01– 0.19), and SI = 1.18 (95% CI: 1.02– 1.36).
Conclusion: Frailty and malnutrition are correlated with high fall risk in older adults, with a modest positive interaction observed between the two conditions, offering empirical support for the development of comprehensive fall prevention and management strategies.
Keywords: older adults, frailty, malnutrition, falls, interaction
Background
With the accelerated global aging process, maintaining and enhancing the quality of life for older adults has emerged as a critical issue in public health. Among the various health problems affecting this demographic, falls represent a prevalent and serious form of unintentional injury. Falls not only directly elevate the risk of disability and mortality but also significantly undermine quality of life.1,2 Studies indicate that approximately 26.5% of older adults worldwide experience at least one fall annually; in China, the incidence of falls among individuals aged 60–79 years has reached 10.5%, with this rate trending upward as age increases.3,4 Consequently, preventing falls has become a pivotal challenge in the health management of older adults.5 In existing research related to the prevention of falls among older adults, some scholarshave applied the STEADI tool to specialized assessment of fall risk in older adults. Standardized, systematic screening and stratified evaluation enable accurate identification of high-risk groups and development of targeted management plans. It effectively compensates for the one-sidedness and subjectivity of traditional empirical assessments, ultimately achieving a significant reduction in the actual incidence of falls among older adults.6 Thereby, it prevents a series of adverse outcomes such as disability, decline in quality of life, and increased medical burdens caused by falls, substantially enhancing older adults’health management efficacy and conserving public health resources.
Frailty is a geriatric syndrome characterized by reduced physiological reserve, multisystem functional decline, and increased vulnerability.7,8 The primary physiological changes it induces include loss of muscle mass, decreased muscle strength, balance control disorders, and abnormal gait.9,10 These functional impairments directly compromise the body’s capacity to initiate emergency responses and regulate movements during sudden external events, such as navigating slippery surfaces, abrupt changes in posture, or avoiding obstacles. Concurrently, frailty significantly diminishes coordination in daily activities, thereby being a key factor associated with falls among older adults. A study11 conducted on older adults residing in Chinese communities substantiated this assertion, revealing a significant positive correlation between frailty scores and fall risk. Specifically, for each 1-point increase in frailty scores, the risk of falls escalated by 53% (OR = 1.53, 95% CI: 1.41–1.66). Another study12 revealed that among individuals with both frailty and myasthenia, the incidence of falls reached 67.9%, significantly exceeding the rates observed in the frailty-only group (60%) and the myasthenia-only group (59.2%). The coexistence of these conditions elevates the risk of falls to several times that associated with a single factor (adjusted OR = 20.45, 95% CI: 6.02–46.69). This finding suggests that frailty does not occur in isolation.13 Its relationship with falls arises not only from the direct effects of physiological degeneration but may also involve additional factors linked to frailty, such as malnutrition and the presence of multiple comorbidities. Moreover, an increasing body of evidence14 suggests that frailty is not an inevitable aspect of aging but rather a modifiable condition that can be reversed or delayed through targeted interventions. Consequently, elucidating the characteristics and mechanisms underlying the association between frailty and fall risk in the elderly holds significant clinical importance and practical value for developing precise and effective fall prevention strategies.
Malnutrition represents a prevalent and often overlooked health issue among the elderly, with its association with falls and fall risk corroborated by numerous studies.15,16 Research conducted by Biggin K et al17 has demonstrated that malnutrition, characterized by deficiencies in protein, vitamin D, and calcium, can adversely affect muscle mass and strength in older adults. This decline directly compromises gait stability and balance regulation, making it increasingly challenging for individuals to maintain homeostasis during postural changes or external disturbances. Furthermore, another study18 revealed a significant gender difference in fall risk after controlling for confounding variables such as age, body mass index (BMI), and muscle strength. Additionally, micronutrient deficiencies associated with malnutrition, including vitamin B12, can impair neurotransmitter synthesis,19 subsequently affecting memory and attention in older adults. This impairment diminishes their capacity to anticipate environmental risks and respond to emergencies. More importantly, malnutrition can also induce or perpetuate a low-grade systemic inflammatory state within the body. This chronic inflammatory microenvironment accelerates muscle protein breakdown, inhibits synthesis, and hampers tissue repair.20 Consequently, this pathological process undermines skeletal muscle health, leading to sarcopenia and osteoporosis, which significantly heightens the risk of falls and fractures.
Notably, Malnutrition and frailty frequently coexist in the elderly population.21,22 This association is not coincidental; rather, it results from the physiological degeneration of multiple systems within the aging body, the interplay of pathological conditions, and alterations in behavioral patterns. Consequently, this phenomenon has garnered significant attention from researchers in geriatrics and lifestyle medicine. A cohort study23 focused on community-dwelling elderly individuals elucidated the combined effect of these two conditions on fall risk, revealing that the incidence of falls among those with comorbidities was markedly higher than that among individuals with a single disease or those who were healthy. A follow-up study after orthopedic surgery in older adults24 identified the combination of frailty and malnutrition was independently associated with major postoperative complications, with its predictive value surpassing that of any single indicator. Clinical studies concentrating on intervention25,26 have preliminarily demonstrated that lifestyle modifications, including optimized protein and vitamin D intake alongside resistance and balance training, can effectively address the comorbidity of malnutrition and frailty, thereby reducing the risk of falls among older adults. In addition, fall risk in older adults is multifactorial, involving medication burden, orthostatic hypotension, visual impairment, vestibular/balance disorders, peripheral neuropathy, and other geriatric syndromes.27 This further indicates that malnutrition and frailty may exert a interaction via multisystem pathological changes, which together mediate the elevated fall risk among older adults. However, most studies have primarily examined European and American populations, focusing on the qualitative relationship between frailty and malnutrition concerning fall risk. Quantitative analysis regarding the combined multiplicative and additive effects of these factors on falls remains scarce. Therefore, this study seeks to quantitatively assess the multiplicative and additive interactions of frailty and malnutrition in older individuals, clarify their interactive characteristics, and offer empirical support for developing tailored comorbidity management approaches for the older adults.
Research Design and Methods
Study Design and Participants
This study adopted a cross-sectional design. From October 2022 to September 2023, a convenience sampling method was used to recruit older adults aged 60 years and above from Zunyi City, Guizhou Province, China. The inclusion criteria were as follows: (1) aged ≥ 60 years; (2) clear consciousness and ability to communicate normally; (3) provision of informed consent and voluntary participation. The exclusion criteria included: (1) a history of severe mental illness or severe cognitive impairment that prevented effective communication; (2) presence of acute critical conditions (including shock, respiratory failure, acute heart failure, acute myocardial infarction, stroke, etc.) that made it impossible to participate in the survey; (3) acute exacerbation of chronic diseases or terminal stage of illness (expected lifespan < 3 months).
By reviewing the literature,28 we identified that the prevalence of falls among older adults in China is approximately 19.3%. With a 95% confidence level (Z = 1.96) and a margin of error ( ) of 0.01, the minimum required sample size was calculated to be 5, 987. To account for potential design effects and to ensure sufficient statistical power for complex subgroup and interaction analyses, a final sample of 13, 970 participants was included.
) of 0.01, the minimum required sample size was calculated to be 5, 987. To account for potential design effects and to ensure sufficient statistical power for complex subgroup and interaction analyses, a final sample of 13, 970 participants was included.

Research Instruments
General Information Questionnaire
This questionnaire primarily collected sociodemographic and other relevant data, including: gender, age, BMI, education level, marital status, number of children, type of residence area, living arrangement, alcohol consumption, smoking status, social activities, physical exercise, and social support.
Activity of Daily Living Scale
We used the Barthel Index (BI) to evaluate the activities of daily living of older adults. This scale was developed to assess older adults’ self-care abilities.29 It covers a range of basic daily activities including using the toilet, dressing, and bathing. The total score of the scale ranges from 0 to 100, and a higher score indicates a higher level of functional independence. According to the standard cut-off values: a score above 60 points means the participant has basic self-care ability; scores between 40 and 59 points indicate the need for partial assistance; scores between 20 and 39 points mean significant assistance is required; a score below 20 points represents complete dependence on others. Previous studies30 have confirmed that this scale has good reliability and validity when applied to older adult populations.
Frailty Scale (FRAIL)
This scale was developed by Morley JE et al31 in 2012 as a simple and practical tool for assessing frailty status in older adults; it consists of 5 questions: fatigue, difficulty climbing stairs, difficulty walking 500 meters, having more than 5 diseases, and weight loss exceeding 3 kilograms. A score of 1 is given for a “yes” response and 0 for a “no” response, with a total score ranging from 0 to 5. A score of 0 indicates no frailty, 1 to 2 points indicate pre-frailty, and 3 points or more indicate frailty. This scale has been shown to have good reliability and validity in previous studies.32
Mini Nutritional Assessment Short-Form (MNA-SF)
This tool is used for the rapid screening of malnutrition risk in older adults and consists of 6 items,33 which assess weight loss, BMI, mobility, acute stress, neuropsychological problems, and appetite, respectively. The total score ranges from 0 to 14 points, and can be divided into three categories based on cut-off values: a score of 12–14 points indicates good nutritional status, 8–11 points indicates malnutrition risk, and 0–7 points indicates malnutrition. This short form has been shown to have good reliability and validity in other studies,34 can be completed in approximately 3–5 minutes, and is suitable for various settings.
Stopping Elderly Accidents, Deaths & Injuries (STEADI)
Fall risk was screened using the Chinese version of the STEADI initiative’s self-assessment questionnaire.35 This 12-item dichotomous (yes/no) tool scores the first two items 2 points each and the remaining ten 1 point each, for a total of 14. A score ≥ 4 indicates high fall risk, and the scale has demonstrated good reliability and validity in Chinese older adults.35
Survey Methods
Data were collected via questionnaire by five trained staff using a standardized protocol. After detailed explanation and obtaining informed consent, participants completed the survey independently. For those unable to self-report, staff administered the questionnaire verbally. Assistance was provided throughout to ensure comprehension. We distributed a total of 14, 256 questionnaires in this study and ultimately retrieved 13, 970 valid ones, with a questionnaire recovery rate of 98.0%.
Statistical Analysis
Data entry and processing were performed using SPSS 29.0 and Excel. Between-group comparisons of fall risk across different demographic characteristics were conducted using chi-square tests or t-tests, as appropriate. Two logistic regression models were constructed: Model 1 was unadjusted, while Model 2 controlled for demographic and other confounding variables. The dependent variable was high risk of falls (no = 0, yes = 1). Independent variables included nutritional status (with normal nutrition as the reference) and frailty level (with non - frailty as the reference). Collinearity diagnostics were conducted for all independent variables in the logistic regression models, including frailty score, MNA-SF score and relevant covariates. All variance inflation factor (VIF) values were below 2.5, which demonstrated the absence of serious multicollinearity among predictors. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were reported.
Furthermore, an interaction term (frailty × malnutrition) was introduced into Model 2. For multiplicative interaction analysis, the FRAIL score and MNA-SF total score were treated as continuous variables. A multiplicative interaction was considered statistically significant if the 95% CI of the OR for the interaction term did not include 1.
The Andersson Excel tool was used to assess additive interaction effects. We calculated and reported the relative excess risk due to interaction (RERI), attributable proportion due to interaction (AP), and synergy index (SI). Nutritional status and frailty status were converted into categorical variables for this analysis. In general, a significant additive interaction is identified when the 95% confidence intervals (CIs) of RERI and AP do not contain 0, and the 95% CI of SI does not contain 1. The significance level was set at P < 0.05.
Regarding missing data, participants with any missing information on the variables included in the logistic regression models (ie., frailty, nutritional status, and all covariates) were excluded from the multivariate analyses. Given the large sample size and low overall missing rate in this field survey, no data imputation was performed.
Results
Baseline Characteristics
The study included 13, 970 older adults (7, 084 males). The prevalence of high fall risk, frailty, and malnutrition was 24.1% (n = 3, 371), 14.0% (n = 1, 950), and 3.4% (n = 480), respectively. As shown in Table 1, results revealed significant differences (P < 0.05) between fall risk and age, sex, marital status, education, residence, number of children, smoking, alcohol use, social activities, physical exercise, and social support.
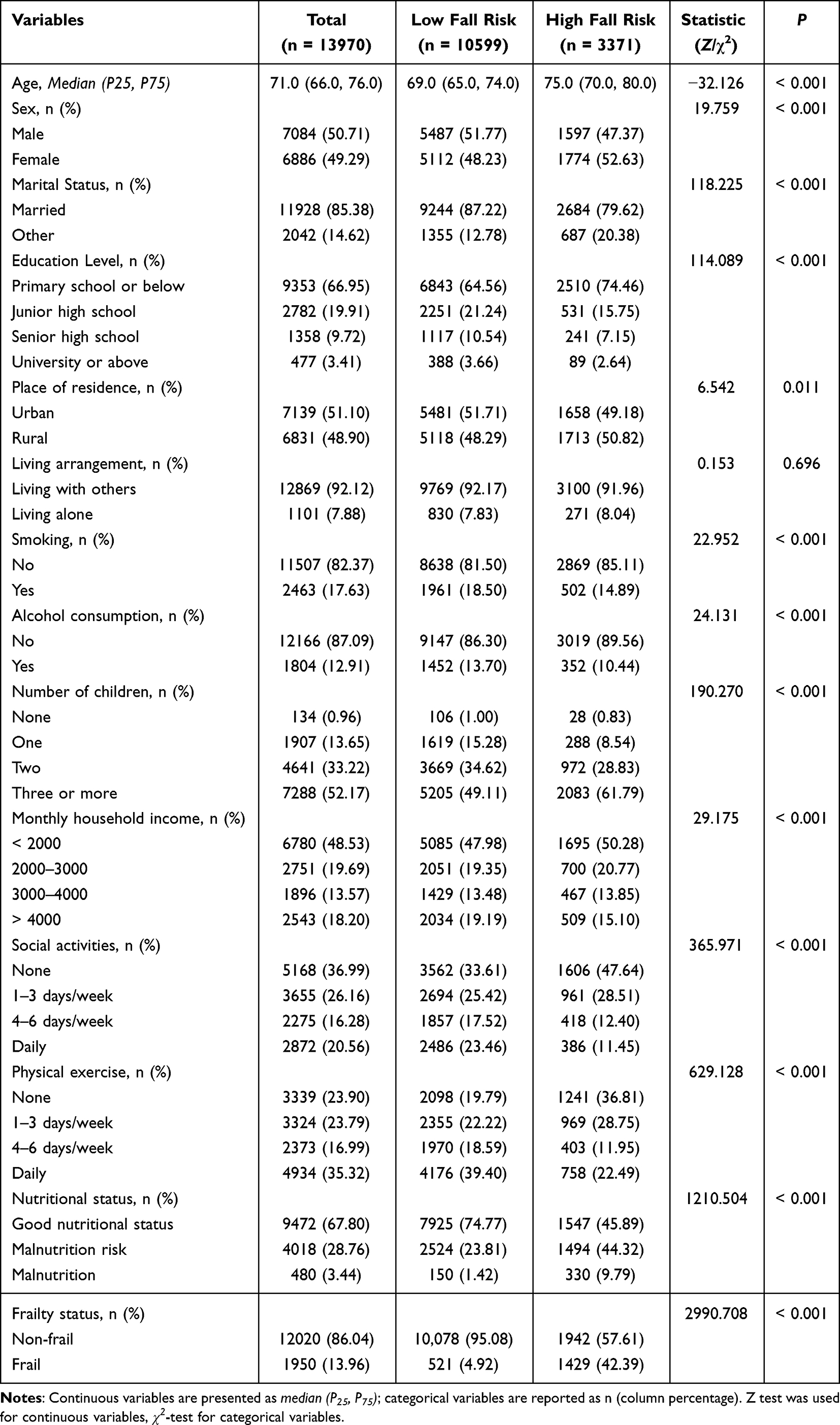 |
Table 1 Comparative Analysis of Baseline Characteristics |
Correlations Among Frailty, Nutritional Status, and Falls Risk in Older Adults
In univariable logistic regression, both frailty and malnutrition were significantly associated with falls (P < 0.001). These associations persisted in a multivariable model adjusted for age, sex, education, marital status, number of children, residence, income, smoking, alcohol use, social activities, and physical exercise (Table 2).
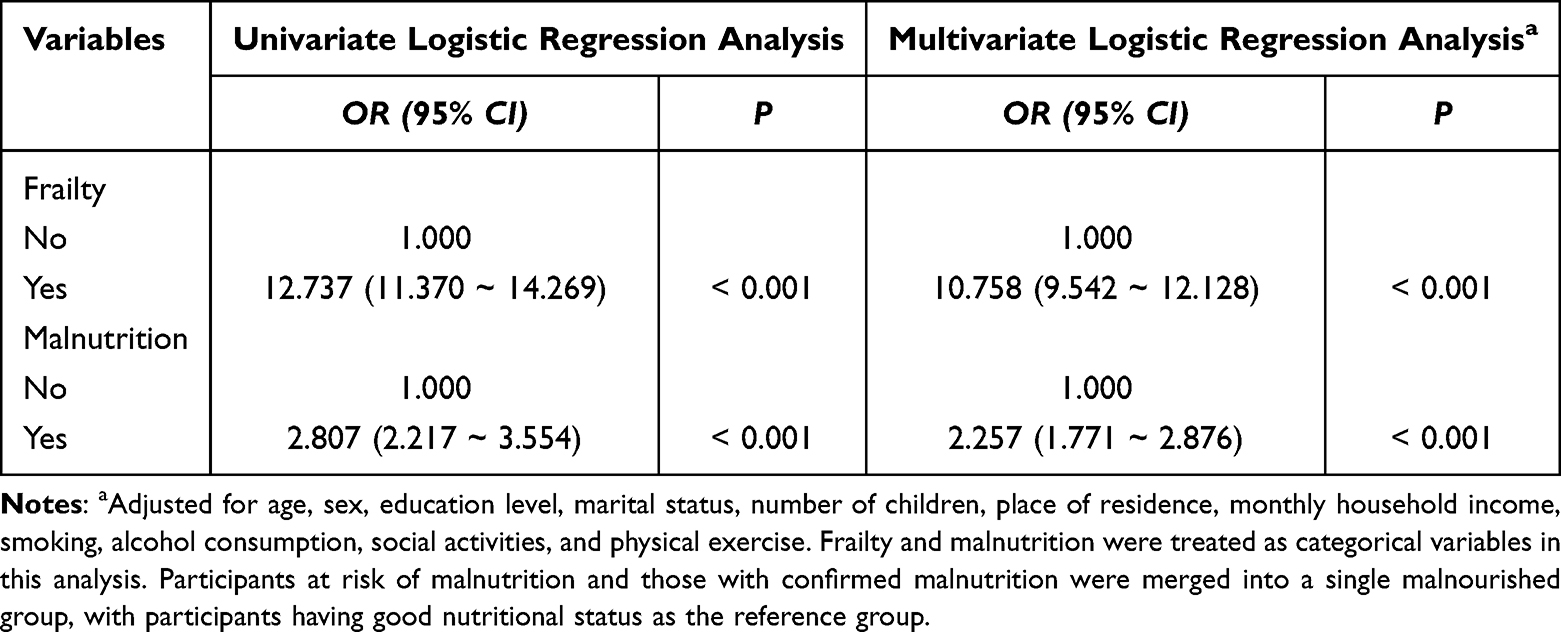 |
Table 2 Logistic Regression Analysis of Frailty, Malnutrition, and Falls in Older Adults |
Interaction Effects
Multiplicative Interaction Between Frailty and Malnutrition
Logistic regression models assessed the multiplicative interaction between frailty and malnutrition on fall risk. All confounding variables were determined in advance by multinomial logistic regression and included as covariates (Detailed results in Supplementary Table 1). The unadjusted model (Model 1) showed significant main effects for frailty and malnutrition, and a significant interaction term (all P < 0.05). In the adjusted model (Model 2, controlling for sociodemographic and lifestyle factors), the main effects and the multiplicative interaction remained statistically significant (Table 3, P < 0.05).
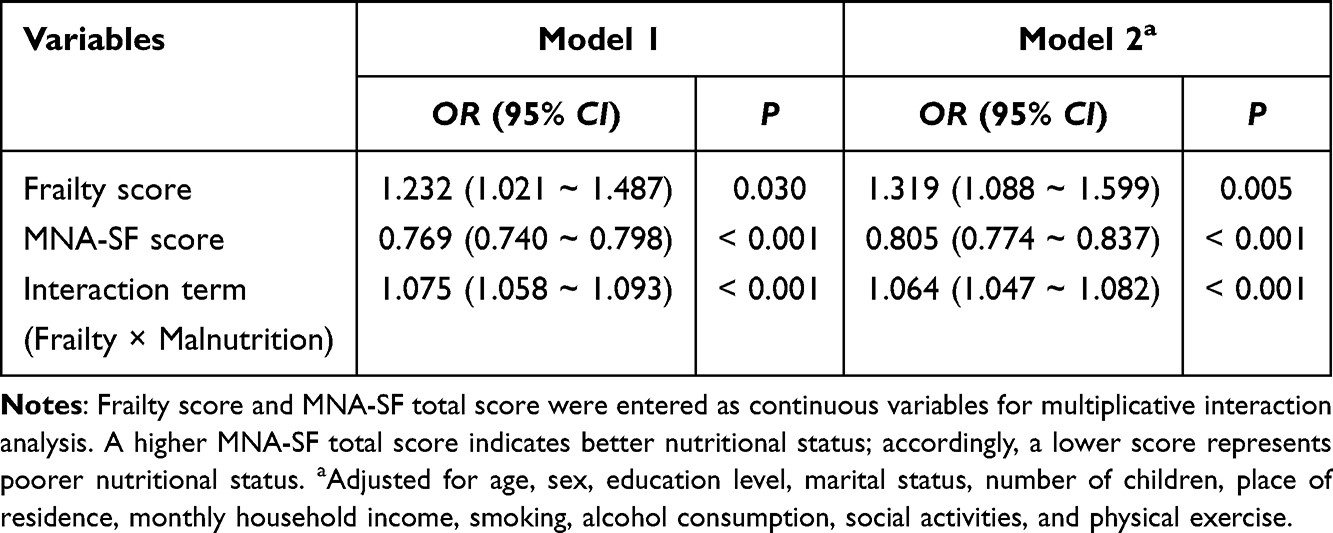 |
Table 3 Multiplicative Effects of Frailty and Malnutrition on Fall Risk in Elderly Adults |
Additive Interaction Effects Between Frailty and Malnutrition
Additive interaction was assessed by including frailty and malnutrition as dummy variables in regression models, using robust and well-nourished participants as the reference. In unadjusted analyses, the odds ratios (ORs) for falls were substantially elevated for malnutrition alone, frailty alone, and their combination. These associations remained significant after adjustment for sociodemographic and lifestyle factors (Table 4). Measures of additive interaction (RERI, AP, SI) were calculated with 95% CI. The interaction indices for Model 1, namely RERI, AP, and SI, had OR (95% CI) values of 2. 572 (0.804–4.340), 0.117 (0.037–0.197), and 1.23 (1.05–1.44), respectively. For Model 2, the estimated measures of additive interaction were RERI = 1.575 (95% CI: 0.192–2.958), AP = 0.099 (95% CI: 0.012–0.186), and SI = 1.18 (95% CI: 1.02–1.36). These results indicate that the coexistence of frailty and malnutrition significantly increases the risk of falls, demonstrating a statistically significant but modest positive additive interaction.
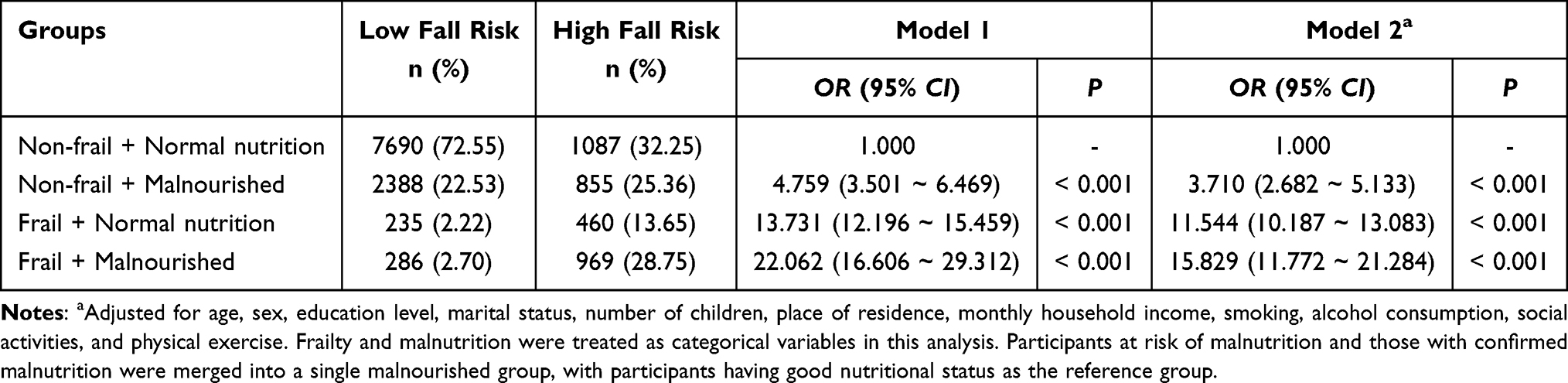 |
Table 4 Additive Effects of Frailty and Malnutrition on Fall Risk in Older Adults |
Discussion
Distribution and Demographic Characteristics of Populations at High Risk of Falls
This study show that among the enrolled older adults, 24.1% are at high risk of falls. This proportion is close to the previously reported 26.5%36 but higher than the 14.3% fall prevalence among community-dwelling older adults in China reported by Wang et al37 This may be closely related to assessment tools and sample characteristics. On the one hand, this study utilized the Chinese version of the STEADI tool for assessment. On the other hand, the research included participants from medical institutions, communities, and senior care facilities. Older adults in these environments often present with advanced age, multiple chronic conditions, and complex medication regimens, which collectively raise the overall risk profile. In addition, this study also found that multiple sociodemographic and behavioral factors, such as age, gender, educational level, social activities, and physical exercise, are significantly associated with the fall risk of older adults, this is consistent with the conclusions of previous studies.38 Among them, the mean age of older adults in the high fall-risk group (75.0 years) was significantly higher than that in the low fall-risk group (69.0 years). This suggests that age-related declines in physiological functions, such as reduced gait stability,39 muscle mass loss,40 and diminished sensorimotor integration ability,41 may be directly associated with falls. The phenomenon that females have a higher fall risk than males may be associated with the accelerated decline in bone mineral density and muscle mass resulting from decreased estrogen levels after menopause.42 Accordingly, older adults in communities, elderly care facilities and medical institutions face a relatively higher risk of falls. The formulation of fall prevention and control strategies should comprehensively take into account sociodemographic and behavioral factors. By implementing personalized risk screening and targeted health interventions, this study provides practical references for developing a scientific and efficient fall prevention and control system for the older adults.
Independent Associations of Frailty, Malnutrition, and Fall Risk
Findings of this study indicated that after adjusting for multiple confounding factors including age and gender, both frailty and malnutrition were independently associated with screened high fall risk among older adults. Specifically, frail older adults had a 10.758-fold higher risk of falling compared with non-frail individuals (adjusted OR = 10.758, 95% CI: 9.542–12.128), which was higher than the 3.43 - fold risk reported by Jiang et al11 In addition to the advanced age, heavy comorbidity burden of the study population, construct and item overlap across assessment scales is another critical factor contributing to the relatively high effect sizes observed in our study. The FRAIL scale for frailty includes items regarding difficulty climbing stairs and walking long distances, which evaluate lower-limb function, walking ability and balance. These functional domains also constitute the core components of the STEADI fall risk assessment tool. Repeated measurement of physical dysfunction by the two instruments introduces measurement bias and overestimates the strength of the association between frailty and fall risk. Although collinearity diagnostics ruled out severe multicollinearity among variables, it cannot eliminate systematic bias resulting from overlapping measurement domains. Objectively, this limitation only overestimates the strength of associations to a certain extent. Future studies may adopt multiple approaches such as stratified analysis and sensitivity analysis to further control the interference caused by scale overlap and achieve more accurate estimation of effect sizes. For malnourished older adults, their fall risk was 2.257 times that of those with normal nutritional status (adjusted OR = 2.257, 95% CI: 1.771–2.876), a slight increase over the 1.978-fold risk documented by Meijers et al,43 which also points to population-specific differences in the fall-inducing effect of malnutrition From the perspective of independent association mechanisms, frailty may mainly affect the physiological reserve of older adults, leading to muscle loss, decreased balance ability, abnormal gait, and cognitive decline, while also reducing their ability to respond to unexpected events, thereby being independently associated with elevated fall risk. Malnutrition may reduce muscle protein synthesis, decrease bone strength, and affect neuromuscular function, leading to insufficient muscle strength and increased skeletal fragility in older adults. It may also be accompanied by symptoms such as anemia and fatigue, further impairing older adults’ mobility and balance, and ultimately being independently associated with higher fall risk. The pathways of their effects are independent and each has its own focus. Both influence fall risk in older adults by affecting core physiological functions (such as mobility, balance, and emergency responses). This characteristic of independent association provides important support for the development of targeted prevention and control measures, suggesting that healthcare professionals need to pay attention to the assessment and management of both.
The Interaction Between Frailty and Malnutrition and Its Association with Fall Risk
Findings of this study further demonstrated that, with older adults who were non-frail and had normal nutritional status as the reference, the presence of frailty or malnutrition alone was associated with an increased fall risk by 11.544-fold and 3.710-fold, respectively (adjusted ORs), which were higher than the values reported by Yang et al44 In contrast, the concurrent presence of both conditions led to a marked increase in fall risk by 15.829-fold. The interaction indicators also show that the relative excess risk due to interaction (RERI) is 1.575 (95% CI: 0.192–2.958), the attributable proportion (AP) is 0.099 (95% CI: 0.012–0.186), and the synergy index (SI) is 1.18 (95% CI: 1.02–1.36). These results indicated that frailty and malnutrition produce more than a simple additive independent effect, presenting a statistically significant but modest positive additive interaction, which is consistent with the trend observed by Larissa Amorim Almeida et al45 in community-dwelling older adults. However, this study firstly quantifies the magnitude and attributable proportion of the additive interaction between frailty and nutritional status on the risk of falls in older adults through different combinations of frailty and nutritional status. In addition, the coefficient of the interaction term frailty × malnutrition in logistic regression is also significantly positive, indicating that a multiplicative interaction exists in terms of relative risk. The coexistence of the two models is not contradictory, but rather reveals the interplay of frailty and malnutrition on the risk of falls in the older adults from both the “excess case” and “relative risk” dimensions. The potential mechanisms of these two interactions may can be attributed in state of frailty, older adults may experience inadequate nutritional intake due to decreased physical activity and impaired digestive and absorptive functions, which exacerbates malnutrition; in turn, malnutrition may accelerates the frailty process by reducing muscle synthesis and lowering physiological reserves, creating a vicious cycle of frailty, malnutrition and progressive functional decline, which is correlated with elevated fall risk. Quantifying this attributable proportion provides a new perspective for understanding the public health significance of these interactions. Future research could use methods based on marginal structural models or interaction dose-response surface approaches to further quantify the absolute risk difference and population attributable risk under different frailty-nutrition combination states. This would help more precisely identify high-risk subgroups and provide more refined quantitative evidence for comprehensive fall prevention interventions for older adults.
Conclusions and Limitations
This cross-sectional analysis explored multiplicative and additive interactions between frailty, malnutrition and high fall risk among older adults. Statistically significant modest positive interactions were identified between frailty and malnutrition. Older adults with concurrent frailty and malnutrition presented higher odds of high fall risk. The findings highlight the value of multi-dimensional assessment of frailty and nutritional status when conducting fall risk screening for older adults. However, this study still has certain limitations: first, the cross-sectional design cannot clarify the causal relationship between frailty, malnutrition, and falls. Future studies need to track the dynamic changes of the three through prospective cohort studies to verify the temporal sequence of their interaction; second, the sample comes from Zunyi City, Guizhou Province, China, which may be influenced by regional economic conditions, medical resources, and other factors, leading to potential bias; third,we adjusted for conventional confounders including sex and physical exercise, but did not measure and include several well-recognized fall risk factors: orthostatic hypotension, burden of anticholinergic and sedative medications, vestibular and balance disorders, visual impairment, and peripheral neuropathy. The exclusion of these key indicators may lead to residual confounding and compromise the accuracy of effect estimates. Future studies should collect these clinical indicators to achieve more comprehensive confounding adjustment.
Data Sharing Statement
The datasets generated and analysed during the current study are not publicly available due the data needs further analysis, but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study has been reviewed and approved by the Ethics Review Committee of the Affiliated Hospital of Zunyi Medical University (Ethics Review No.: KLL2022 - 814), and was conducted in accordance with the principles outlined in the Declaration of Helsinki. Each participant freely consented to participate in the study and provided informed consent.
Acknowledgment
We acknowledge all the participants and research staff for their valuable contributions to this study.
Author Contributions
All authors have made substantial contributions to the conception, design, conduct, data acquisition, analysis and interpretation of this work. All participated in drafting and critically revising the manuscript, approved the final published version, agreed to submit the article to this journal, and take full accountability for all aspects of the work.
Individual contributions of each author are listed as follows: WH: Conceptualization, Data Curation, FormalAnalysis, Methodology, Validation, Visualization, Writing - Original Draft, Writing - Review & Editing. LH: Data Curation, Investigation,Validation, Writing - Review & Editing. MQ: Data Curation, Investigation,Writing - Review & Editing. YS: Data Curation, Investigation,Writing - Review & Editing. YX: Funding Acquisition, Project Administration, Supervision, Writing - Original Draft, Writing - Review & Editing.
Funding
This work was supported by the China National Key Research and Development Program (Grant No. 2020YFC2008500), the Medical Research Joint Fund for High-Quality Development of Health in Guizhou Province in 2024 (Grant No. 2024GZYXKYJJXM0163), and the Guizhou Provincial Science and Technology Planning Project (Grant No. CXTD [2023] 028).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Baek W, Min A, Ji Y, Park CG, Kang M. Impact of activity limitations due to fear of falling on changes in frailty in Korean older adults: a longitudinal study. Sci Rep. 2024;14(1):19121. doi:10.1038/s41598-024-69930-2
2. Pillay J, Gaudet LA, Saba S, et al. Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences. Syst Rev. 2024;13(1):289. doi:10.1186/s13643-024-02681-3
3. Salari N, Darvishi N, Ahmadipanah M, Shohaimi S, Mohammadi M. Global prevalence of falls in the older adults: a comprehensive systematic review and meta-analysis. J Orthop Surg Res. 2022;17(1):334. doi:10.1186/s13018-022-03222-1
4. Jiarong Z, Jingjing W, Chaoqun F, Xu Z, Qiang F. Current status and correlated factors of fall risk among Chinese elderly aged 60-79:A 2024 nationwide cross-sectional analysis. Med J Of Peking Union Med Coll Hosp. 2025;16(3):606–11. doi:10.12290/xhyxzz.2025-0227
5. Organization WH. Step Safely: Strategies for Preventing and Managing Falls Across the Life-Course. Geneva: Bulletin WHOAT; 2021.
6. Lin CC, Meardon S, O’Brien K. The predictive validity and clinical application of stopping elderly accidents, deaths & injuries (STEADI) for fall risk screening. Adv Geriatr Med Res. 2022;4(3). doi:10.20900/agmr20220008
7. Doody P, Lord JM, Greig CA, Whittaker AC. Frailty: Pathophysiology, theoretical and operational Definition(s), impact, prevalence, management and prevention, in an increasingly economically developed and ageing world. Gerontology. 2023;69(8):927–945. doi:10.1159/000528561
8. Jung HW. Frailty as a clinically relevant measure of human aging. Ann Geriatr Med Res. 2021;25(3):139–140. doi:10.4235/agmr.21.0106
9. Geriatrics Society CMAECoCJoG, Beijing, China. Chinese expert consensus on prevention of frailty in the elderly(2022). Chinese J Geriatrics. 2022;41(5):503–511. doi:10.3760/cma.j.issn.0254-9026.2022.05.001
10. Li S, Yuan X, Jiang Z, Yang X, Zhao X, Liang H, Wang C. Association of self-reported visual and hearing impairment and their interaction with frailty in the elderly. Practical Geriatrics. 2024;38(4):343–347.
11. Jiang L, Ding S, Wang J. The association between frailty and falls among individuals aged 60 years and older residing in community settings and experiencing hip fractures in China: a cross-sectional study. Aging Male. 2025;28(1):2442571. doi:10.1080/13685538.2024.2442571
12. Ghorbanzadeh M, Bakhtiari A, Hajian-Tilaki K, Abbaszadeh-Amirdehi M. Association of multidimensional frailty and dynapenia with fall risk in older adults. BMC Geriatr. 2025;25(1):442. doi:10.1186/s12877-025-06097-z
13. Yang ZC, Lin H, Jiang GH, et al. Frailty is a risk factor for falls in the older adults: a systematic review and meta-analysis. J Nutr Health Aging. 2023;27(6):487–595. doi:10.1007/s12603-023-1935-8
14. Serra-Prat M, Fortuny Borsot A, Burdoy E, Lavado Cuevas À, Muñoz Ortiz L, Cabré M. Frailty reversal and its main determinants: a population-based observational and longitudinal study. Fam Med Comm Health. 2025;13(2). doi:10.1136/fmch-2024-003250
15. Mziray M, Nowosad K, Śliwińska A, Chwesiuk M, Małgorzewicz S. Malnutrition and fall risk in older adults: a comprehensive assessment across different living situations. Nutrients. 2024;16(21). doi:10.3390/nu16213694
16. Eckert C, Gell NM, Wingood M, Schollmeyer J, Tarleton EK. Malnutrition risk, rurality, and falls among community-dwelling older adults. J Nutr Health Aging. 2021;25(5):624–627. doi:10.1007/s12603-021-1592-8
17. Biggin K, Marian IR, Lamb SE, et al. Mobility and strength training with and without protein supplements for pre-frail or frail older adults with low protein intake: the Maximising Mobility and Strength Training (MMoST) feasibility randomised controlled trial protocol. NIHR Open Res. 2023;3:62. doi:10.3310/nihropenres.13507.2
18. Binkley N, Sempos CT, Borchardt G, et al. Association of standardized serum 25-hydroxyvitamin D with falls in post-menopausal women. Osteoporos Int. 2025;36(2):255–264. doi:10.1007/s00198-024-07310-2
19. Mithal A, Bonjour JP, Boonen S, et al. Impact of nutrition on muscle mass, strength, and performance in older adults. Osteoporos Int. 2013;24(5):1555–1566. doi:10.1007/s00198-012-2236-y
20. Massironi S, Viganò C, Palermo A, et al. Inflammation and malnutrition in inflammatory bowel disease. Lancet Gastroenterol Hepatol. 2023;8(6):579–590. doi:10.1016/s2468-1253(23)00011-0
21. Norazman CW, Adznam SN, Jamaluddin R. Malnutrition as key predictor of physical frailty among malaysian older adults. Nutrients. 2020;12(6). doi:10.3390/nu12061713
22. Verlaan S, Ligthart-Melis GC, Wijers SLJ, Cederholm T, Maier AB, de Van der Schueren MAE. High prevalence of physical frailty among community-dwelling malnourished older adults-a systematic review and meta-analysis. J Am Med Dir Assoc. 2017;18(5):374–382. doi:10.1016/j.jamda.2016.12.074
23. Esquivel MK. Nutritional assessment and intervention to prevent and treat malnutrition for fall risk reduction in elderly populations. Am J Lifestyle Med. 2018;12(2):107–112. doi:10.1177/1559827617742847
24. Kwan KY, Ho M, Chau PH, Chan CH, Tang RLM, Yip PSF. Associations of food insecurity with geriatric syndromes in the economically deprived community-dwelling Chinese older adults: the mediating role of malnutrition risk. Eur Geriatr Med. 2025;doi:10.1007/s41999-025-01337-2
25. Dent E, Daly RM, Hoogendijk EO, Scott D. Exercise to prevent and manage frailty and fragility fractures. Curr Osteoporos Rep. 2023;21(2):205–215. doi:10.1007/s11914-023-00777-8
26. Yoshimura Y, Matsumoto A, Inoue T, Okamura M, Kuzuya M. Protein supplementation alone or combined with exercise for sarcopenia and physical frailty: a systematic review and meta-analysis of randomized controlled trials. Arch Gerontol Geriatr. 2025;131:105783. doi:10.1016/j.archger.2025.105783
27. Colón-Emeric CS, McDermott CL, Lee DS, Berry SD. Risk assessment and prevention of falls in older community-dwelling adults: a review. JAMA. 2024;331(16):1397–1406. doi:10.1001/jama.2024.1416
28. Kang N, Yu H, Lu X, Zhang Y, Chen G. A meta-analysis of the incidence of falls in the elderly in China. Chin J Evid Based Med. 2022;22(10):1142–1148.
29. Wade DT, Collin C. The barthel ADL index: a standard measure of physical disability? Int Disabil Stud. 1988;10(2):64–67. doi:10.3109/09638288809164105
30. Leung SO, Chan CC, Shah S. Development of a Chinese version of the modified barthel index-- validity and reliability. Clin Rehabil. 2007;21(10):912–922. doi:10.1177/0269215507077286
31. Morley JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging. 2012;16(7):601–608. doi:10.1007/s12603-012-0084-2
32. Sha S, Xu Y, Chen L. Loneliness as a risk factor for frailty transition among older Chinese people. BMC Geriatr. 2020;20(1):300. doi:10.1186/s12877-020-01714-5
33. Rubenstein LZ, Harker JO, Salvà A, Guigoz Y, Vellas B. Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF). J Gerontol a Biol Sci Med Sci. 2001;56(6):M366–72. doi:10.1093/gerona/56.6.m366
34. Vellas B, Guigoz Y, Garry PJ, et al. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition. 1999;15(2):116–122. doi:10.1016/s0899-9007(98)00171-3
35. Yaling L, Fu D. Translation of a fall risk self-assessment tool of the STEADI Toolkit: testing reliability and validity in the elderly. J Nurs Sci. 2020;35(9):84–87. doi:10.3870/j.issn.1001-4152.2020.09.084
36. AlSumadi M, AlAdwan M, AlSumadi A, Sangani C, Toh E. Inpatient falls and orthopaedic injuries in elderly patients: a retrospective cohort analysis from a falls register. Cureus. 2023;15(10):e46976. doi:10.7759/cureus.46976
37. Xiaojun W, Yang X, Yuanyuan Z, Yanxia G. Meta-analysis on the incidence of falls among the elderly in Chinese community. Chin Evid Based Nurs. 2020;6(11):1149–1154. doi:10.12102/j.issn.2095-8668.2020.11.003
38. Lee YC, Chang SF, Kao CY, Tsai HC. Muscle strength, physical fitness, balance, and walking ability at risk of fall for prefrail older people. Biomed Res Int. 2022;2022:4581126. doi:10.1155/2022/4581126
39. Nascimento MM, Gouveia ÉR, Gouveia BR, et al. Associations of gait speed, cadence, gait stability ratio, and body balance with falls in older adults. Int J Environ Res Public Health. 2022;19(21). doi:10.3390/ijerph192113926
40. de Almeida Nagata C, Hamu T, Pelicioni PHS, Durigan JLQ, Garcia PA. Influence of lower limb isokinetic muscle strength and power on the occurrence of falls in community-dwelling older adults: a longitudinal study. PLoS One. 2024;19(4):e0300818. doi:10.1371/journal.pone.0300818
41. Freire I, Seixas A. Effectiveness of a sensorimotor exercise program on proprioception, balance, muscle strength, functional mobility and risk of falls in older people. Front Physiol. 2024;15:1309161. doi:10.3389/fphys.2024.1309161
42. H S, Bhagavan VKR, Maharjan N. Relationship between Ankle Range of Motion (ROM), muscle strength, balance, and fall risk in postmenopausal women: a pilot study. Int J Sci Healthcare Res. 2021;6(3):291–297. doi:10.52403/ijshr.20210751
43. Meijers JM, Halfens RJ, Neyens JC, Luiking YC, Verlaan G, Schols JM. Predicting falls in elderly receiving home care: the role of malnutrition and impaired mobility. J Nutr Health Aging. 2012;16(7):654–658. doi:10.1007/s12603-012-0010-7
44. Fan Y, Shuang W, Hai Q, et al. Effect of frailty syndrome on falls in Chinese elderly diabetics in the communities: a prospective cohort study. Chin J Epidemiol. 2018;39(6):776–780. doi:10.3760/cma.j.issn.0254-6450.2018.06.016
45. Almeida LA, Dantas B, Rocha KPM, et al. Nutritional, cognitive, and functional deficits, frailty, and quality of life associated with fall risk in community-dwelling older adults: a cross-sectional study conducted in Brazil. J Prim Care Community Health. 2025;16:21501319251341742. doi:10.1177/21501319251341742
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Combined Vision and Hearing Impairment is Associated with Frailty in Older Adults: Results from the West China Health and Aging Trend Study
Zhao Y, Ding Q, Lin T, Shu X, Xie D, Gao L, Yue J
Clinical Interventions in Aging 2022, 17:675-683
Published Date: 2 May 2022
Intrinsic Capacity Declines with Elevated Homocysteine in Community-Dwelling Chinese Older Adults
Lin S, Wang F, Zheng J, Yuan Y, Huang F, Zhu P
Clinical Interventions in Aging 2022, 17:1057-1068
Published Date: 7 July 2022
Risk of Falls in HIV-Infected Patients on Antiretroviral Therapy and Its Associated Factors
Wahyudi ER, Putri RF, Yunihastuti E, Shatri H
HIV/AIDS - Research and Palliative Care 2022, 14:355-363
Published Date: 2 August 2022
An Easy-to-Implement Clinical-Trial Frailty Index Based on Accumulation of Deficits: Validation in Zoster Vaccine Clinical Trials

Andrew MK, Matthews S, Kim JH, Riley ME, Curran D
Clinical Interventions in Aging 2022, 17:1261-1274
Published Date: 19 August 2022
Recognition and Management of Hospital-Acquired Sepsis Among Older General Medical Inpatients: A Multi-Site Retrospective Study
Barker N, Scott IA, Seaton R, Mehta N, Kalke VR, Redpath L
International Journal of General Medicine 2023, 16:1039-1046
Published Date: 21 March 2023