")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Risk of Falls in HIV-Infected Patients on Antiretroviral Therapy and Its Associated Factors
Authors Wahyudi ER, Putri RF, Yunihastuti E , Shatri H
Received 25 April 2022
Accepted for publication 22 July 2022
Published 2 August 2022 Volume 2022:14 Pages 355—363
DOI https://doi.org/10.2147/HIV.S372204
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Edy Rizal Wahyudi, Rizki Febriani Putri, Evy Yunihastuti, Hamzah Shatri
Department of Internal Medicine, Faculty of Medicine Universitas Indonesia – Cipto Mangunkusumo Hospital, Jakarta, Indonesia
Correspondence: Evy Yunihastuti, Email [email protected]
Purpose: Fall is one of the geriatric syndromes and a significant public health concern, which causes potentially severe consequences among the elderly. Geriatric syndromes are common among PLHIV and affect younger age than the general population. This study attempted to identify the risk of falls in PLHIV on antiretroviral therapy (ART) and its related factors among older adults with HIV infection.
Methods: This cross-sectional study was conducted from December 2019 to May 2020 among PLHIV aged ≥ 40 years who received ART for at least 6 months in HIV Integrated Clinic, Cipto Mangunkusumo Hospital, Jakarta. Bivariate and multivariate analyses were performed using Poisson regression with robust estimator using STATA version 12.0.
Results: A total of 102 participants mainly consisted of males (83.3%) with a median age of 45 (IQR 5) years. The risk of fall was detected in 52% of these participants. PLHIV who have history of falls, current CD4 below 200 cells/mm3, and pre-frail–frail status were associated with an increased risk of falls in the future. An LPV/r-based regimen was found to be a protective factors of risk of falls among PLHIV.
Conclusion: History of falls, current CD4 below 200 cells/mm3, and pre-frail and frail status were identified as factors associated with a greater risk of fall among PLHIV.
Keywords: falls, HIV, frailty, antiretroviral, geriatric
Introduction
As a result of the widespread use of antiretroviral therapy (ART), people living with HIV (PLHIV) can live longer, survive into older age, and are now approaching the life expectancy of the general population.1 PLHIV are thought to manifest accelerated aging with an earlier occurrence of many aging diseases than expected.2,3 Geriatric syndromes are common among PLHIV, and they are affected at a younger age than the general population.4,5 However, the therapy also increases the risk of several comorbidities, such as cardiovascular and bone disease.6,7 PLHIV have a greater chance of injurious falls or fractures due to low bone density, low body weight, neuropathy, neurocognitive impairment, and frailty.8 Falls is one of the geriatric syndromes and is a significant public health concern with potentially severe consequences.9 Falls can result in a severe injury that leads to disability, hospitalization, limitations to activity, and increased mortality risk.10
In the previous study, 54% of PLHIV were diagnosed with at least two geriatric syndromes, and 26% of them reported at least one fall in the last 12 months.4 The fall rate among middle-aged PLHIV (45–65 years) on effective ART paralleled with non-infected elderly population aged 65 years or older.3 The prevalence of falls among PLHIV has been shown to vary from 18% to 41%.11,12 The fear of falling again among older adults who have a history of falls is associated with poor quality of life, developed frailty, and depression, which leads to physical inactivity and weakness that can exacerbate the underlying fall risk.8
Several factors that are known to increase the risk of falls in PLHIV are older age,11,13,14 pre-existing comorbidities and complication,3,4,13,14 lower body mass index,8 polypharmacy,3,14 depression status,3 neurocognitive impairment,8,13 frailty,4,8,11 neuropathy,3,8 and medication adherence.14 As the number of older adults living with HIV continues to rise because of enhanced survival and life expectancy, the impact of falls and fall-related complications has become increasingly relevant. Due to unique HIV-related characteristics, this study aimed to get the prevalence and identify the risk of falls in PLHIV on ART and the related factors of falls to reduce the rate of falls, or even prevent them, among older adults with HIV infections.
Methods
Study Design
This cross-sectional study was conducted from December 2019 to May 2020.
Study Setting
This study was conducted at HIV/AIDS Integrated Outpatient Clinic – Cipto Mangunkusumo Hospital, a national referral hospital that provides multidisciplinary HIV care in accordance with the Indonesian national guideline of HIV/AIDS infection.
Study Participants
Eligible criteria for this study were all PLHIV aged ≥40 years who received ART for at least 6 months in the HIV/AIDS Integrated Outpatient Clinic at Cipto Mangunkusumo Hospital. The exclusion criteria were refusal to participate in this study, physical disabilities that caused difficulties with walking or inability to walk and/or use their dominant hand, and participants with incomplete data. Of the 156 participants screened for eligibility in this study, 54 were declared not eligible due to refusal or inability to walk or use a hand-grip dynamometer due to disability. Thus, 102 participants completed the study procedures and were included in the final analysis.
Sampling Procedures
PLHIV who came to the clinic for regular control were invited to join the study. It was not based on the medical record, and the screening was done daily to seek potential participants aged a minimum of 40 years who had taken ART for at least 6 months by the researchers. We consecutively screened the patients until the minimum sample size was achieved. The minimum sample size was counted by using the two population proportion formula. No incentive was given to the participant in this study.
Measures
The socio-demographic information collected included age, gender, marital status, occupational status, and educational level, habitual history such as smoking status and alcohol consumption. Clinical HIV/AIDS information included HIV transmission routes, body mass index (BMI), duration of HIV/AIDS diagnosis and ART, recent and nadir CD4 cell count, latest HIV-RNA viral load, ART withdrawal history, opportunistic infection history such as tuberculosis and central nervous system (CNS) infection, comorbidities (cardiac, lung, liver, and kidney disease, diabetes mellitus, and malignancy), fall history, polypharmacy, type of ART, depression status, the severity of peripheral neuropathy, frailty and dementia status. The outcome of this study is to get the prevalence the risk of fall and to identify the risk of falls in PLHIV on ART and its related factors.
Depression status was measured using the Indonesian version of the Beck Depression Inventory (BDI)-II questionnaire. This tool has been reported as an adequate measurement of depressive symptoms among PLHIV and has been translated into Indonesian with good validity and reliability, with a Cronbach’s alpha of 0.9.15 The questionnaire used had a 21-item self-reported inventory that asked participants to rate each item based on the severity of depression symptoms they felt during the past week. The test covers cognitive (eg, thought of past failure), emotional/affective (eg, sadness), and somatic/vegetative (eg, tiredness or fatigue) symptoms. Each response is scored on a scale from 0 (not) to 3 (severe). The scores for each Indo-BDI-II item were combined to give a total score that indicated the severity of depression. Scores of 0–13 points were categorized as symptomatic, 14–19 points as mild depression, 20–28 points as moderate depression, and 29–63 points as severe depression.16 Ginting et al showed that the receiver operating characteristic (ROC) curve indicated that the cut-off point of the Indo BDI-II questionnaire for a mild severity of depression in the Indonesian population should be 17. In this study, we used scores below 17 points as considered not at risk of depression.15
The Toronto Clinical Scoring System (TCSS) was used to measure the severity of peripheral neuropathy. This system was first adopted for screening diabetic peripheral neuropathy by a research group in Toronto. The TCSS consists of three parts: symptoms score, reflex score, and sensory test score. The maximum score is 19 points that divided into four categories. Scores of 0–5 points were interpreted as no peripheral neuropathy, 6–8 points as mild peripheral neuropathy, 9–11 points as moderate peripheral neuropathy, and 12–19 as severe peripheral neuropathy.17
Fried et al defined the phenotypes of frailty using five criteria: unintentional weight loss, exhaustion, reduced physical activity, slowness of walking speed, and weakness in grip strength.18 Weight loss was defined as a loss of 4.5 kg or >5% body weight in the previous year. To measure exhaustion and reduced physical activity, participants were asked several questions such as “How often did you feel that every activity that you did are tiring?” and “How often did you feel that you could not do any activity due to your tiredness?”. The optional responses for those questions are almost always (5–7 days), often (3–4 days), sometimes (1–2 days), or none/rarely (<1 day in a week). The slowness of walking speed and weakness of handgrip strength were objectively measured by observing walking speed across a distance of 15 feet (4.57 meters) and employing the Jamar Hydraulic Hand Dynamometer. The slowness of walking speed were defined when time of ≥7 second (men with a height of ≤173 cm or women with a height of ≤159 cm) or ≥6 second (men with a height of >173 cm or women with a height of >159 cm), while the diagnosis of the weakness of handgrip strength was stratified based on gender and BMI. The weakness of handgrip strength was defined if ≤29 kg grip strength in ≤24 kg/m2, ≤30 kg in 24.1 kg/m2, and ≤32 kg in >28 kg/m2 for male, while ≤17 kg in ≤23 kg/m2, ≤17.3 kg in 23.1–26 kg/m2, ≤18 kg in 26.1–29 kg/m2, and ≤21 kg in >29 kg/m2 for female. Items meeting the criteria for frailty were scored as 1. Then, each item was calculated as a score to define the stages of frailty by Fried et al. A score of 0 points means the participant is robust or not frail, 1–2 points is considered pre-frail, and 3–5 points is frail.19
The Time Up and Go (TUG) is a tool for screening the risk of falls in inpatient and community settings. In this test, participants are timed while they rise from an armchair (seat height ±46 cm), walk a distance of 3 meters, then turn and walk back to the chair and sit down again. Each participant did these tests twice. The first time was a trial to become familiar with the test, and the second was the actual test. During the TUG test, the participants wore their regular footwear and used any customary walking that was necessary.20 A score ≥13.5 seconds is used as a cut-off point to identify those at risk of falls in the community. A faster time means the participant has a better functional performance.21 However, reported cut-off values vary from 10 to 33 seconds in previous literature.22,23 In this study, a score ≥10.0 seconds was used to identify those who had a risk of falls.
The guided Mini-Cog test was used for dementia screening in this study. The Mini-Cog test has two components: a three-word recall task to assess memory and a clock drawing test to assess cognitive function, language, visual-motor skills, and executive function. In the first part, which is the three-word recall task, the scoring system is based on the correct recall of 0–3 words (1 point per word), while the clock drawing test is scored as normal or abnormal. A positive Mini-Cog test result indicates a possible diagnosis of dementia, whereas a negative test result indicates a lack of dementia. A positive test result is a delayed word recall score of 0 out of 3 or a score of 1–2 with an abnormal clock drawing test result. A negative test result is a score of 3 on the delayed word recall or a score of 1–2 with a normal clock drawing test result.24
Statistical Analysis
Data were analyzed using STATA version 12.0 (StataCorp, College Station, TX, USA). Bivariate and multivariate analyses were performed using Poisson regression with a robust estimator to determine the factors associated with the risk of falls among Indonesian PLHIV. Descriptive characteristics were summarized with mean and standard deviation (SD) or median and interquartile range (IQR Q1-Q3) for continuous variables and frequency with percentage for categorical variables. We entered all bivariate correlates (p<0.25) into multivariate analyses using Poisson regression with a robust estimator test. The results are presented as prevalence ratio (PR) and 95% confidence intervals (95% CI). The level of significance was set at p<0.05.
Ethical Considerations
This study was approved by the Health Research Ethics Committee, Faculty of Medicine, Universitas Indonesia–Cipto Mangunkusumo Hospital (0702/UN2.F1/ETIK/2018). After explaining the study procedures and purpose, all participants who agreed to participate signed the informed consent form. All data obtained guaranteed confidentiality. All procedures in this study were conducted in accordance with the Declaration of Helsinki, as revised in 2013.
Results
Socio-Demographic and Clinical Characteristic of HIV Infection
Most of the participants were male (83.3%) with a median age of 45 (IQR 43–48) years. The mean of HIV diagnosis and ART use duration was 99.9 months (8.3 years) and 93.8 months (7.8 years), respectively. Intravenous drug use (IVDU) (41.2%) was the most transmission route of HIV infection, followed by multiple sexual partners (39.2%), and men who have sex with men (MSM) (18.6%). More than half of the participants had well-suppressed HIV-RNA viral load (60.8%) with the median of current and nadir CD4 counts were 495.5 (IQR 368.8–729.8) and 71.5 (IQR 26.0–246.5) cells/mm3, respectively (Table 1).
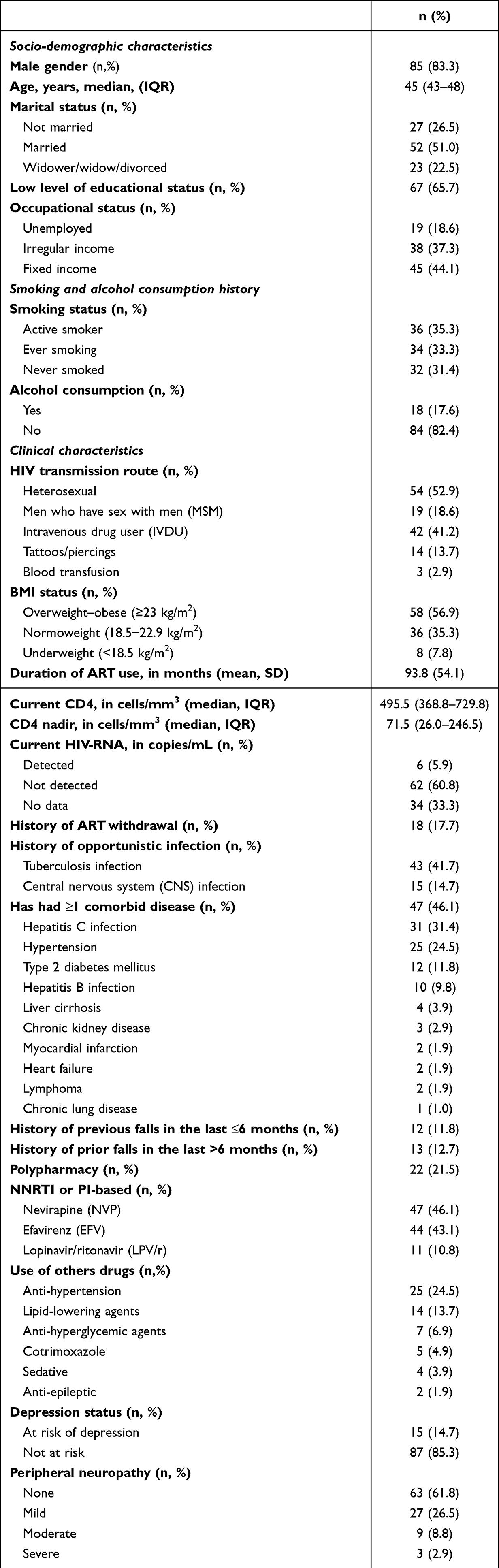 |
Table 1 Characteristics of Study Participants (n=102) |
Prevalence and Factors Associated with Risk of Falls in PLHIV
In this study, the risk of fall was detected in 52% of the participants. PLHIV with a pre-frail and frail status based on Fried criteria had 2.4-fold higher risk of fall than PLHIV with robust status. PLHIV with current CD4 <200 cells/mm3 had 1.6-fold, while history of falls in the past was found to have a 1.4-fold greater risk of fall in the future. However, age, peripheral neuropathy, and dementia did not significantly relate to the risk of fall. This study also showed that use of a PI-based regimen is a protective factor against falls among PLHIV. Nutritional status and comorbidities were not associated with the risk of falls among PLHIV in our study (Table 2).
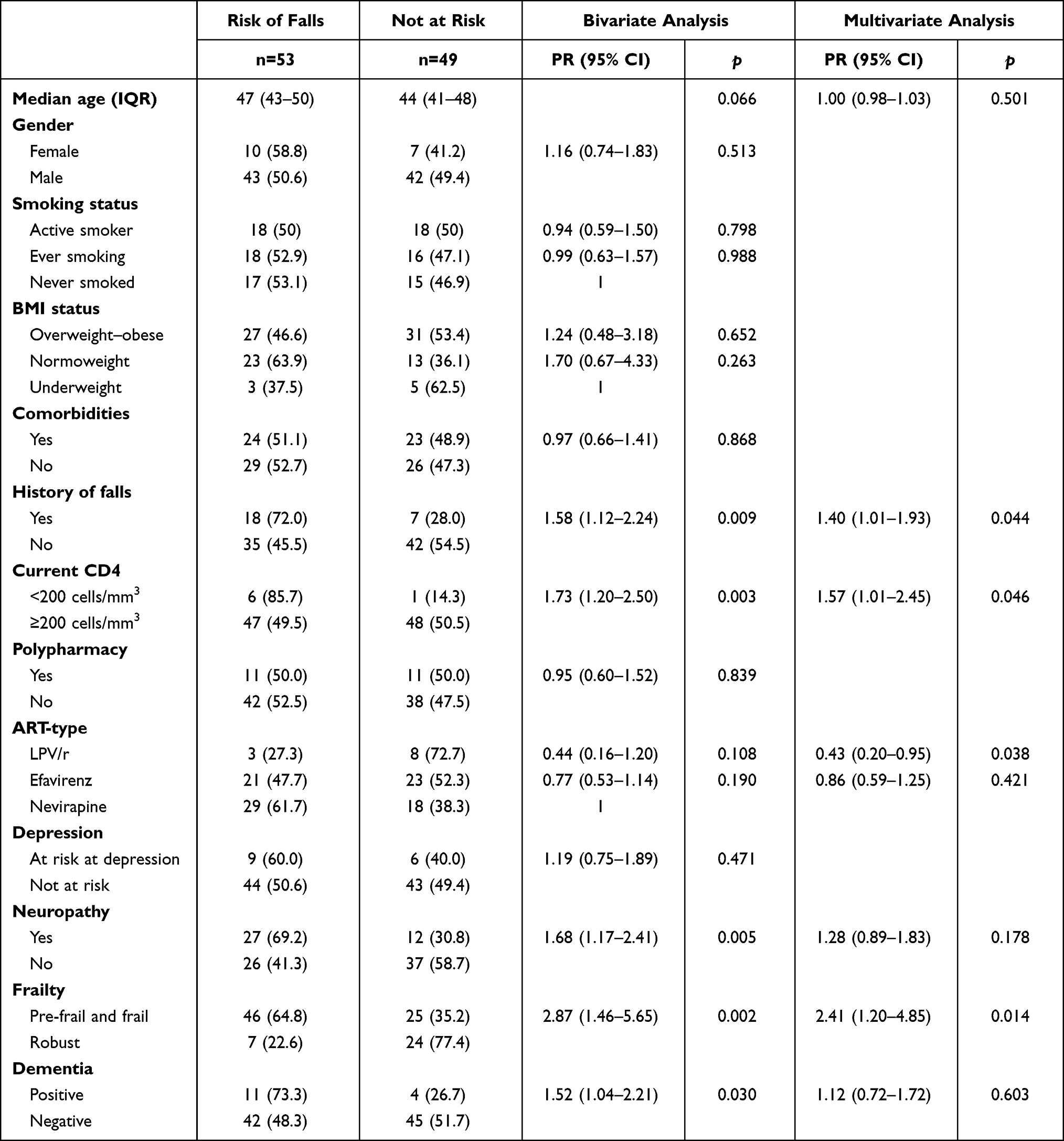 |
Table 2 Factors Associated with the Risk of Falls in PLHIV |
Discussion
In this study, less than one-fourth of the participants were female. This result was in line with the real situation in Indonesia, the number of the woman above 15 years living with HIV is 190,000 of 540,000 PLHIV.25 The factors related to the risk of falls in PLHIV there are history of falls, a current CD4 <200 cells/mm3, and have pre-frail and frail status.
First, a history of falls was associated with the risk of falls among PLHIV. Berner et al showed that 34% of PLHIV have a history of fall in the past year, both single fall or multiple falls. The most common reasons reported for falling were tripping (41.2%), dizziness (29.4%), and slipping (11.8%).26
Second, our study reported that current CD4 count less than 200 cells/mm3 was associated with a higher risk of falls among PLHIV. We suggest it is because the lower CD4 count in PLHIV will tend to get a higher risk of opportunistic infection that can lead to the frailty condition. In some cases, low CD4 counts may be associated with increased HIV-RNA viral load levels that impaired neuromotor performance, and even low levels of the detectable virus have been associated with higher immune activation levels, virological failure, and poorer clinical outcomes.27,28 Our finding was different from other previous studies that showed there is no association with CD4 count with risk of falls among PLHIV.8
The last factor associated with the risk of falls among PLHIV is a pre-frail–frail status. The results of this study are in line with the findings of Erlandson et al, who reported that frailty status increases the 9.5-fold risk of falls among PLHIV, and a one-point decrease in Fried criteria increased the 3.1-fold risk of fall.3 Another study also reported that pre-frail and frail status increased 1.5-fold and 2.4-fold risk of single falls among PLHIV, compared with robust participants; however, this study stated that these findings were not statistically significant.11 The other reason for the strong association of frailty status and falls is that PLHIV in our study has multimorbidities that affect their risk of falls through different mechanisms, such as balance impairment, neuropathy, polypharmacy, and weakness. Determining frailty as a factor associated with the risk of falling is essential because frailty can be modified, although perhaps not ultimately returned to normal state. Intervention targeting frailty is expected to minimize the risk of falls. Currently, there is no management guidelines regarding the pre-frail or frail status of PLHIV. A review of existing literature indicates that nutritional improvement by assessing nutritional status and individual needs and programmed physical exercise can improve frailty status.29
In our study, we also found that the use of a PI-based regimen was the protective factor of falls in PLHIV. This is the most interesting because it has not been previously reported in low-middle-income countries (LMIC). We assumed this is because the PI-based regimen has a lower penetrating effect on the central nervous system (CNS) or peripheral nervous system toxicity compared to other ART. This result was similar to the prior study in high-income countries (HIC) that showed PI-based regimen has a protective effect of falls among PLHIV.8 The higher CNS penetration score (CPE Score) means that the ARV drugs have good penetration into the cerebrospinal fluid (CSF). A higher CPE score is likely to have a greater neurocognitive improvement due to higher effectiveness in suppressed viral replication in the CNS and reduced neurotoxins and neuro-inflammation production.30–36 An LPV/r has a lower CPE score compared to NVP, but it has the same score as EFV. In our study, an EFV has a protective factor of risk of falls, but not statistically significant. We hypothesized that the higher CPE score will increase the risk of CNS adverse effects and peripheral nervous system toxicity that lead to a greater risk of falls among PLHIV.
Falls in PLHIV can result in as serious consequences that can increase the morbidity and mortality. The fall prevalence in our sample can thus not be generalized to the population of PLHIV in Indonesia. However, this study showed us that the risk of fall among PLHIV is high. Assessment of the risk of falls screening among PLHIV is important to prevent the fall incident in the future.
Limitations
This study does have some limitations. First, recall bias may affect the accuracy of self-reported questionnaires, and participants may also have given inaccurate information during data collection. In addition, this study is limited by its cross-sectional design, meaning that the definitive cause and effect associations cannot be determined. The fall prevalence in our sample can thus not be generalized to the population of PLHIV in Indonesia. The gender bias can also affect the result of this study because more than third-quarter of total participants were male.
Conclusion
The risk of falls is common among PLHIV. History of falls, current CD4 counts below 200 cells/mm3, and pre-frail and frail status were identified as factors related to a higher risk of falls among PLHIV. Therefore, it is important for clinicians to increase the awareness of the risk of falling and conduct the risk of fall screening among PLHIV to reduce morbidity and mortality due to falls-related.
Data Sharing Statement
The data could be obtained by request to author’s email ([email protected]).
Consent for Publication
Written informed consent for publication can be obtained from all participants.
Acknowledgments
We thank all the patients who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no competing interests for this study.
References
1. Samji H, Cescon A, Hogg RS, et al. Closing the gap: increases in life expectancy among treated HIV-positive individuals in the United States and Canada. PLoS One. 2013;8(12):e81355. doi:10.1371/journal.pone.0081355
2. Deeks SG. Immune dysfunction, inflammation, and accelerated aging in patients on antiretroviral therapy. Top HIV Med. 2015;17(4):118–123.
3. Erlandson KM, Allshouse AA, Jankowski CM, et al. Risk factors for falls in HIV-infected persons. J Acquir Immune Defic Syndr. 2012;61(4):484–489. doi:10.1097/QAI.0b013e3182716e38
4. Greene M, Covinsky KE, Valcour V, et al. Geriatric syndromes in older HIV-infected adults. J Acquir Immune Defic Syndr. 2015;69(2):161–167. doi:10.1097/QAI.0000000000000556
5. Desquilbet L, Jacobson LP, Fried LP, et al. HIV-1 infection is associated with an earlier occurrence of a phenotype related to frailty. J Gerontol a Biol Sci Med Sci. 2007;62(11):1279–1286. doi:10.1093/gerona/62.11.1279
6. Freiberg MS, Chang -C-CH, Kuller LH, et al. HIV infection and the risk of acute myocardial infarction. JAMA Intern Med. 2013;173(8):614–622. doi:10.1001/jamainternmed.2013.3728
7. Brown TT, Qaqish RB. Antiretroviral therapy and the prevalence of osteopenia and osteoporosis: a meta-analytic review. AIDS. 2006;20:2165–2174. doi:10.1097/QAD.0b013e32801022eb
8. Erlandson K, Plankey M, Springer G, et al. Fall frequency and associated factors among men and women with or at risk for HIV infection*. HIV Med. 2016;17(10):740–748. doi:10.1111/hiv.12378
9. Drewes J, Ebert J, Langer PC, Kleiber D, Gusy B. Comorbidities and psychosocial factors as correlates of self-reported falls in a nationwide sample of community-dwelling people aging with HIV in Germany. BMC Public Health. 2021;21(1):1544. doi:10.1186/s12889-021-11582-2
10. Ayoung-Chee P, McIntyre L, Ebel BE, Mack CD, McCormick W, Maier RV. Long-term outcomes of ground-level falls in the elderly. J Trauma Acute Care Surg. 2014;76(2):498–503. doi:10.1097/TA.0000000000000102
11. Tassiopoulos K, Abdo M, Wu K, et al. Frailty is strongly associated with increased risk of recurrent falls among older HIV-infected adults. AIDS. 2017;31(16):2287–2294. doi:10.1097/QAD.0000000000001613
12. John MD, Greene M, Hessol NA, et al. Geriatric assessments and association with VACS index among HIV-infected older adults in San Francisco. J Acquir Immune Defic Syndr. 2016;72(5):534–541. doi:10.1097/QAI.0000000000001009
13. Deandrea S, Lucenteforte E, Bravi F, Foschi R, La Vecchia C, Negri E. Risk factors for falls in community-dwelling older people: a systematic review and meta-analysis. Epidemiology. 2010;21:658–668. doi:10.1097/EDE.0b013e3181e89905
14. Ruiz MA, Reske T, Cefalu C, Estrada J. Falls in HIV-infected patients: a geriatric syndrome in a susceptible population. J Int Assoc Provid AIDS Care. 2013;12(4):266–269. doi:10.1177/2325957413488204
15. Ginting H, Näring G, van der Veld WM, Srisayekti W, Becker ES. Validating the Beck Depression Inventory-II in Indonesia’s general population and coronary heart disease patients. Int J Clin Heal Psychol. 2013;13:235–242. doi:10.1016/S1697-2600(13)70028-0
16. Lipps GE, Lowe GA, De La Haye W, et al. Validation of the Beck Depression Inventory II in HIV-positive patients. West Indian Med J. 2010;59(4):374–379.
17. Yang Z, Chen R, Zhang Y, et al. Scoring systems to screen for diabetic peripheral neuropathy. Cochrane Database Syst Rev. 2014;3:1–31.
18. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):146–157. doi:10.1093/gerona/56.3.M146
19. Wulunggono W, Yunihastuti E, Shatri H, Wahyudi ER, Ophinni Y. Frailty among HIV-1 infected adults under antiretroviral therapy in Indonesia. Curr HIV Res. 2019;17(3):204–213. doi:10.2174/1570162X17666190828143947
20. Podsiadlo D, Richardson S. The timed “up & go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
21. Rose DJ, Jones CJ, Lucchese N. Predicting the probability of falls in community-residing older adults using the 8-foot up-and-go: a new measure of functional mobility. J Aging Phys Act. 2002;10:466–475. doi:10.1123/japa.10.4.466
22. Thomas JI, Lane JV. A pilot study to explore the predictive validity of 4 measures of falls risk in frail elderly patients. Arch Phys Med Rehabil. 2005;86:1636–1640. doi:10.1016/j.apmr.2005.03.004
23. Arnold CM, Faulkner RA. The history of falls and the association of the timed up and go test to falls and near-falls in older adults with Hip osteoarthritis. BMC Geriatr. 2007;7:17. doi:10.1186/1471-2318-7-17
24. Seitz DP, Chan CC, Newton HT, et al. Mini-Cog for the diagnosis of Alzheimer’s disease dementia and other dementias within a primary care setting. Cochrane Database Syst Rev. 2018;2018(2):1–41.
25. World Health Organization. Indonesia: HIV country profile 2021. World Health Organization; 2022. Available from: https://cfs.hivci.org/.
26. Berner K, Strijdom H, Essop MF, Webster I, Morris L, Louw Q. Fall history and associated factors among adults living with HIV-1 in the Cape Winelands, South Africa: an exploratory investigation. Open Forum Infect Dis. 2019;6(10):1–7. doi:10.1093/ofid/ofz401
27. Berner K, Morris L, Baumeister J, Louw Q. Objective impairments of gait and balance in adults living with HIV-1 infection: a systematic review and meta-analysis of observational studies. BMC Musculoskelet Disord. 2017;18:325. doi:10.1186/s12891-017-1682-2
28. Antinori A, Lepri AC, Ammassari A, et al. Low-level viremia (LLV) ranging from 50 to 500 copies/mL is associated to an increased risk of AIDS events in the Icona Foundation Cohort. In:
29. Han CY, Miller M, Yaxley A, Baldwin C, Woodman R, Sharma Y. Effectiveness of combined exercise and nutrition interventions in prefrail or frail older hospitalised patients: a systematic review and meta-analysis. BMJ Open. 2020;10:e040146. doi:10.1136/bmjopen-2020-040146
30. de Oliveira Rodrigues R, de Carvalho PG, de Arruda ÉAG, et al. Interleukin-10 gene polymorphism (−1082G/A) and allergy to efavirenz in patients infected with human immunodeficiency virus. Braz J Infect Dis. 2014;18(4):445–448. doi:10.1016/j.bjid.2014.01.009
31. Spudich S. HIV and neurocognitive dysfunction. Curr HIV/AID Rep. 2013;10:235–243. doi:10.1007/s11904-013-0171-y
32. Cross HM, Combrinc M, Joska J. HIV-associated neurocognitive disorders: antiretroviral regimen, central nervous system penetration effectiveness, and cognitive outcomes. S Afr Med J. 2013;103(10):758–762. doi:10.7196/SAMJ.6677
33. Cysique L, Vaida F, Letendre S, et al. Dynamics of cognitive change in impaired HIV-positive patients initiating antiretroviral therapy. Neurology. 2009;73(5):342–348. doi:10.1212/WNL.0b013e3181ab2b3b
34. de Almeida SM. Cognitive impairment and major depressive disorder in HIV infection and cerebrospinal fluid biomarkers. Arq Neuropsiquiatr. 2013;71(9–B):689–692. doi:10.1590/0004-282X20130152
35. Letendre S, Ellis R, Ances B, McCutchan J. Neurologic complications of HIV disease and their treatment. Top HIV Med. 2010;18(2):45–55.
36. Cysique LA, Waters EK, Brew BJ. Central nervous system antiretroviral efficacy in HIV infection: a qualitative and quantitative review and implications for future research. BMC Neurol. 2011;11:148. doi:10.1186/1471-2377-11-148
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.