Back to Journals » Journal of Hepatocellular Carcinoma » Volume 11
Lymphocyte-to-C Reactive Protein Ratio is an Independent Predictor of Survival Benefits for Hepatocellular Carcinoma Patients Receiving Radiotherapy
Authors Shi Z ![]() , Zhu S, Jin Y, Qi L, Zhou M, Zhou Z
, Zhu S, Jin Y, Qi L, Zhou M, Zhou Z ![]() , Zhang J
, Zhang J ![]() , Liu B, Shen J
, Liu B, Shen J ![]()
Received 29 November 2023
Accepted for publication 23 January 2024
Published 8 February 2024 Volume 2024:11 Pages 305—316
DOI https://doi.org/10.2147/JHC.S452424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Gerber
Zhan Shi,1,* Sihui Zhu,2,* Yuncheng Jin,1 Liang Qi,1 Mingzhen Zhou,1 Ziyan Zhou,1 Juan Zhang,1 Baorui Liu,1 Jie Shen1
1Department of Oncology, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University & Clinical Cancer Institute of Nanjing University, Nanjing, Jiangsu Province, 210008, People’s Republic of China; 2The Comprehensive Cancer Centre of Nanjing International Hospital, Medical School of Nanjing University, Nanjing, Jiangsu Province, 210008, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jie Shen; Baorui Liu, Department of Oncology, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University & Clinical Cancer Institute of Nanjing University, Nanjing, Jiangsu Province, 210008, People’s Republic of China, Fax +86-025-83106666, Email [email protected]; [email protected]
Background: Stereotactic body radiotherapy (SBRT) has emerged as an alternative approach for patients with hepatocellular carcinoma (HCC), and we aim to find potential prognostic biomarkers for HCC patients who received SBRT.
Methods: In this study, we retrospectively analyzed HCC patients who underwent SBRT in our institution from January 2018 to December 2022. The inflammatory parameters, along with baseline patients’ characteristics were collected to elucidate the potential relationship with survival benefits and liver toxicities.
Results: Overall, 35 patients were enrolled in our study. For the efficacy population (25 patients who underwent SBRT for primary liver lesions), the objective response rate (ORR) and disease control rate (DCR) were 60% and 100%, respectively. The median progression-free survival (PFS) was 9.9 months [95% confidence interval (CI) 5.6– 14.1 months], and the median overall survival (OS) was 18.5 months (95% CI 14.2– 22.8 months). We further confirmed that higher baseline lymphocyte-C-reactive protein ratio (LCR) (≥ 2361.11) was positively related to both longer PFS (12.0 vs 4.3 months, P = 0.002) and OS (21.9 vs 11.4 months, P = 0.022). Moreover, patients with diabetes and higher alpha-fetoprotein (AFP) (≥ 400 ng/mL) were also found to be associated with worse OS. The most common hepatotoxicity was elevated gamma-glutamyl transferase (GGT) (84.0%).
Conclusion: In conclusion, for patients with inoperable HCC, SBRT resulted in satisfactory local control, survival benefits, and acceptable liver toxicity. Pre-radiotherapy LCR might be an independent and readily available predictor for survival, which facilitates us to find the most appropriate treatment options.
Keywords: hepatocellular carcinoma, stereotactic body radiotherapy, lymphocyte-C-reactive protein ratio, survival, liver toxicity
Introduction
Liver cancer represents the sixth most common malignancy and third lethal cancer-related mortality worldwide,1 with an estimated 1.4 million new cases and 1.3 million deaths in 2040,2 in which, hepatocellular carcinoma (HCC) is the most common form. Notably, the aetiology, diagnosis, treatment, and survival have changed during the past decade.3 Surgical resection, liver transplantation, and local radiofrequency ablation (RFA) are the preferred treatment regimens for early-stage HCC patients. The following locoregional therapies, such as transarterial chemoembolization (TACE), hepatic artery infusion chemotherapy (HAIC), and external beam radiotherapy (EBRT) have become the mainstays for intermediate HCC cases. Additionally, systemic targeted therapy and immunotherapy have shown promising antitumor activity for those who were not candidate for surgery or locoregional interventions.4 Dual immune-checkpoint inhibitors were also confirmed to be effective and well-tolerance.5 More recently, camrelizumab (an anti-programmed cell death protein-1 [PD-1] antibody) plus rivoceranib (an anti-angiogenic tyrosine-kinase inhibitor) showed encouraging survival benefits for unresectable HCC.6
Currently, EBRT, especially for stereotactic body radiotherapy (SBRT), has emerged as an alternative approach to intermediate and advanced HCC, with the advantage of higher precision of radiation delivery, and less toxicity to the surrounding normal tissues,7 even for those who diagnosed with Barcelona clinical liver cancer (BCLC) stage-C, palliative SBRT is an effective and safe treatment modality.8 Previous studies have demonstrated the high efficacy and well-tolerance of SBRT alone for the treatment of primary liver cancer, as well as extrahepatic metastases.9,10 In addition, the Phase 3 clinical trial of NRG/RTOG 1112 reported that SBRT followed by sorafenib prolonged the survival benefits for HCC patients.11 More recently, Chen et al found that SBRT plus sintilimab (the PD-1 inhibitor) achieved outstanding progression-free survival (PFS) and objective response rate (ORR) for patients with recurrent or oligometastatic HCC.12 However, there are no convenient and effective biomarkers to predict the efficacy and safety of HCC patients receiving radiotherapy until now.
Cancer-related inflammation is now regarded as a hallmark of cancer and is known to promote the occurrence, development, and progression of cancers. Radiotherapy has been shown to transform immunologically “cold” tumors into “hot” by stimulating the release of inflammatory mediators, increasing immune cell infiltration, and promoting immunogenicity.13 Currently, various inflammatory indicators are found to be associated with the inflammation status, and the efficacy and safety of anti-cancer treatment.14,15 To our knowledge, there is currently a lack of studies on the potential prognostic indicators for HCC patients who underwent SBRT. Therefore, we conducted this retrospective study to confirm the efficacy and safety of SBRT in patients with moderate and advanced-stage HCC, and further evaluated the relationship between the peripheral blood indicators and treatment outcomes.
Patients and Methods
Patients
This was a retrospective study of HCC patients receiving radiotherapy from January 2018 to December 2022 at our institution. All procedures were conducted with the approval of the Ethics Committee of Nanjing Drum Tower Hospital and following the Declaration of Helsinki. Only patients who signed the consent and met the following criteria were included in this study: Age ≥ 18 years; pathologically or clinically diagnosed with HCC; Child-Pugh class A or B; BCLC stage of B-C; SBRT for primary liver lesions or metastatic bone lesions; Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0–1; no prior radiotherapy to the liver; sufficient liver, renal, cardiac, hematologic, and coagulation function; had at least one measurable lesion; underwent imaging assessments both before and after the administration of radiotherapy. The exclusion criteria were as follows: multiple extrahepatic metastases; abnormal liver or renal function; discontinued therapy; serious comorbidity; without imaging examinations; lack of baseline clinicopathological data; or cessation of follow-up.
Clinical Data
The following laboratory data, including neutrophil count, lymphocyte count, platelet count, monocyte count, serum C‐reactive protein, and albumin levels were collected. The platelet-to-lymphocyte ratio (PLR, platelet count/lymphocyte count), neutrophil-to-lymphocyte ratio (NLR, neutrophil count/lymphocyte count), lymphocyte‐to-C reactive protein ratio [LCR, lymphocyte count (10^9/L) × 10^4 /CRP (mg/L)], lymphocyte-to-monocyte ratio (LMR, lymphocyte count/monocyte count), C-reactive protein-to-albumin ratio [CAR, CRP (mg/L)/albumin (g/L)], and systemic immune-inflammation index (SII, platelet count × neutrophil count/lymphocyte count) were then calculated according to former data. The related data on liver function were also retrieved before and after radiotherapy.
Radiotherapy
For patients without extrahepatic metastasis, the gross tumor volume (GTV) was regarded as the primary tumor lesion and the vascular tumor thrombus according to each phase of computed tomography (CT) and/or magnetic resonance imaging (MRI), the clinical target volume (CTV) was set by the expansion of 3–5 mm margin around the intrahepatic GTV, considering the subclinical disease extension, the planning target volume (PTV) was created by the CTV + 5 mm, depending on the setup error, respiration control, and organ motion. Additionally, we created the planning gross tumor volume (PGTV) as the GTV with a 3 mm uniform expansion to deliver higher radiation doses to tumor lesions. The target doses to PTV were 24–30 Gy/8-10 fractions, and the doses to PGTV were increased to 40–50 Gy/8-10 fractions. The surrounding normal organs and uninvolved liver dose constraints were determined according to the ASTRO guideline.7 Patients with bone metastases were treated based on previous reports.16,17
Evaluation and Follow-Up
Tumor response was evaluated with enhanced CT and/or MRI before and one month after radiotherapy, and then followed every three months according to the response evaluation criteria in solid tumors (RECIST) version 1.1, including complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). Survival benefits were assessed by PFS and overall survival (OS). Liver toxicities were evaluated by the Common Terminology Criteria of Adverse Events (CTCAE) version 5.0.
Statistical Analysis
All statistical analyses were performed with SPSS software version 22.0 and the R programs. The optimal cutoff values for PLR, NLR, LCR, LMR, CAR, and SII were determined using R software and the receiver operating characteristic (ROC) curve. The Wilcoxon signed-rank test was used to compare the changes in inflammatory parameters before and after radiotherapy. The relationships between peripheral blood markers and tumor response were assessed by the chi-square test and Fisher’s exact test. PFS and OS were estimated using the Kaplan–Meier method. Univariate and multivariate Cox regression analyses were performed to find the independent factors for survival and adverse events, the results were presented as hazard ratio (HR) and 95% confidence interval (CI). P < 0.05 was considered significant.
Results
Patient Characteristics
The flow diagram of this study is shown in Figure 1. From January 2018 to December 2022, 588 patients with primary liver cancer underwent treatment at our institution, of which, 416 patients were diagnosed with HCC. Among HCC patients, 90 received radiotherapy, and 25 patients who underwent SBRT for primary liver lesions were included in the efficacy population. Table 1 shows the baseline characteristics of the study population. The median duration of follow-up was 16.0 months (range 4.6–66.9 months). Of the 35 patients, 25 received radiotherapy for intrahepatic lesions, and another 10 received palliative radiotherapy for bone. The median age of our study population was 58 years (range 33–77 years). Twenty-nine patients (82.9%) were male. Twenty-one patients had an ECOG PS of 0. Most patients were diagnosed with chronic hepatitis B virus infection (91.4%) and cirrhosis (60.0%). Six and twelve patients had diabetes and hypertension, respectively. Portal vein thrombosis (PVT) was found in 11 patients. Alpha-fetoprotein (AFP) ≥ 400 ng/mL was observed in 16 patients (45.7%). About 60.0% of patients had a larger tumor size (≥5.0 cm) when they underwent SBRT for primary liver lesions. In this study, 10 patients were categorized as BCLC stage B, while 25 patients were categorized as BCLC stage C. Among the efficacy population who received SBRT for primary liver lesions, 15 out of 25 patients (60.0%) had advanced-stage disease (BCLC class C).
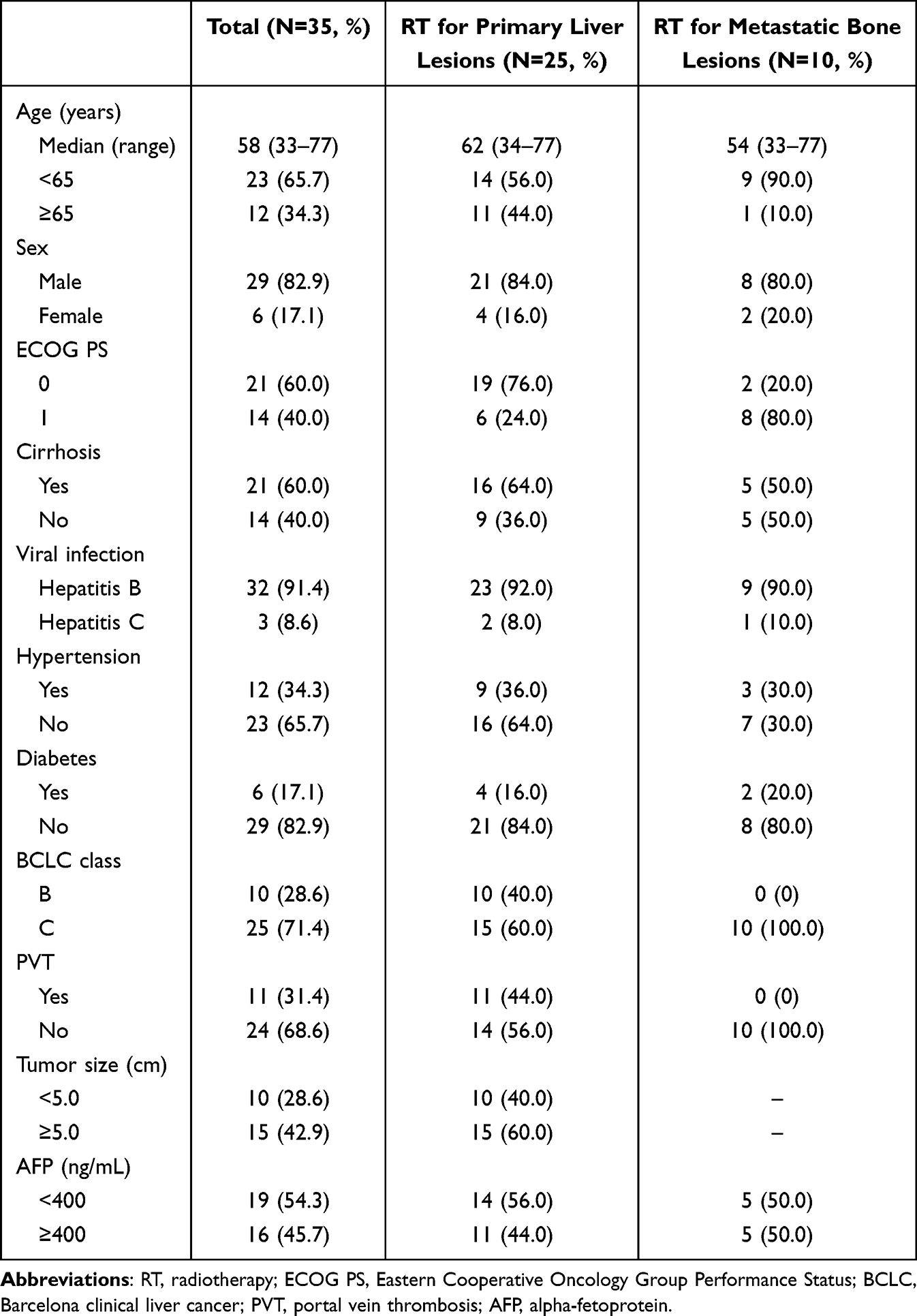 |
Table 1 Patient Baseline Characteristics |
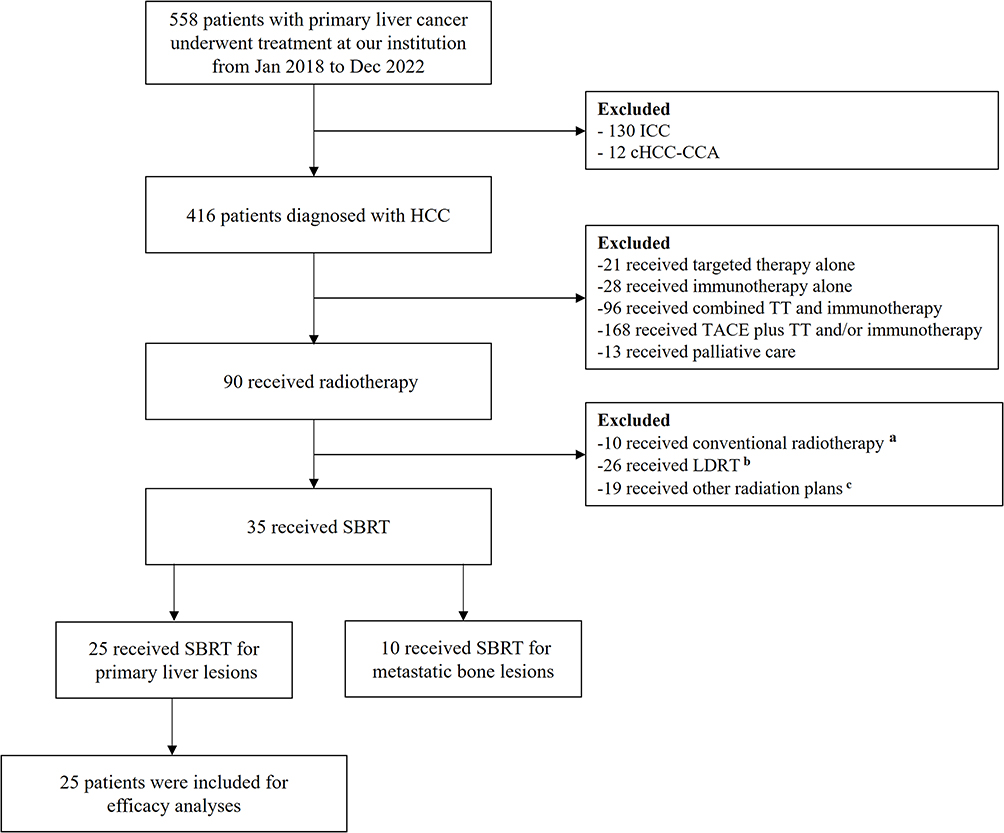 |
Figure 1 Flowchart of the recruitment process. aPTV 50 Gy in 25 fractions, five consecutive days per week; bPTV 15–24 Gy in 3 fractions, three consecutive days; cPTV 18 Gy/6 fractions, or 45 Gy/3 fractions. Abbreviations: ICC, intrahepatic cholangiocarcinoma; cHCC-CCA, combined hepatocellular-cholangiocarcinoma; HCC, hepatocellular carcinoma; TT, targeted therapy; TACE, transarterial chemoembolization; LDRT, low-dose radiotherapy; SBRT, stereotactic body radiation therapy; PTV, planning target volume; PGTV, planning gross tumor volume. |
Changes in Inflammatory Markers
Changes in PLR, NLR, LMR, LCR, CAR, and SII between pre- and post-radiotherapy are shown in Supplementary Figure 1. PLR was significantly increased (P < 0.0001) in patients who underwent radiotherapy for primary liver lesions, and similar results were also observed in NLR and SII. Furthermore, LCR and LMR were significantly reduced compared to pre-radiotherapy (LCR:P = 0.001; LMR: P < 0.0001). In addition, we analyzed the parameter changes in HCC patients with bone metastases who received radiotherapy, and found that the previous inflammatory indices (PLR, NLR, LMR, LCR, and SII) had no significant difference after radiotherapy, only the CAR decreased significantly (P = 0.043) (Supplementary Figure 2). To better identify the valuable parameter, we calculated the optimal cut-off values of the biomarkers using ROC curves. As shown in Supplementary Figure 3, the cut-off values for PLR, NLR, LCR, LMR, CAR, and SII were set to 97.34, 1.95, 2361.11, 4.74, 0.10, and 348.87, respectively. The area under the curve (AUC) values for NLR and LCR were higher than other indicators (NLR: 0.750; LCR: 0.733).
Analysis of PFS by Inflammatory Markers
Of the 35 HCC patients included in our study, 10 patients were excluded because their targeted bone lesions were not measurable according to RECIST 1.1 criteria, and an additional 25 patients with measurable intrahepatic lesions were included in the efficacy population. As shown in Figure 2, the median PFS was 9.9 months (95% CI 5.6–14.1 months). By the univariate and multivariate analysis, we confirmed that patient suffering from higher LCR (≥2361.11) was an independent predictor for PFS (12.0 vs 4.3 months, HR = 0.229, 95% CI 0.088–0.595, P = 0.002) (Table 2 and Figure 2).
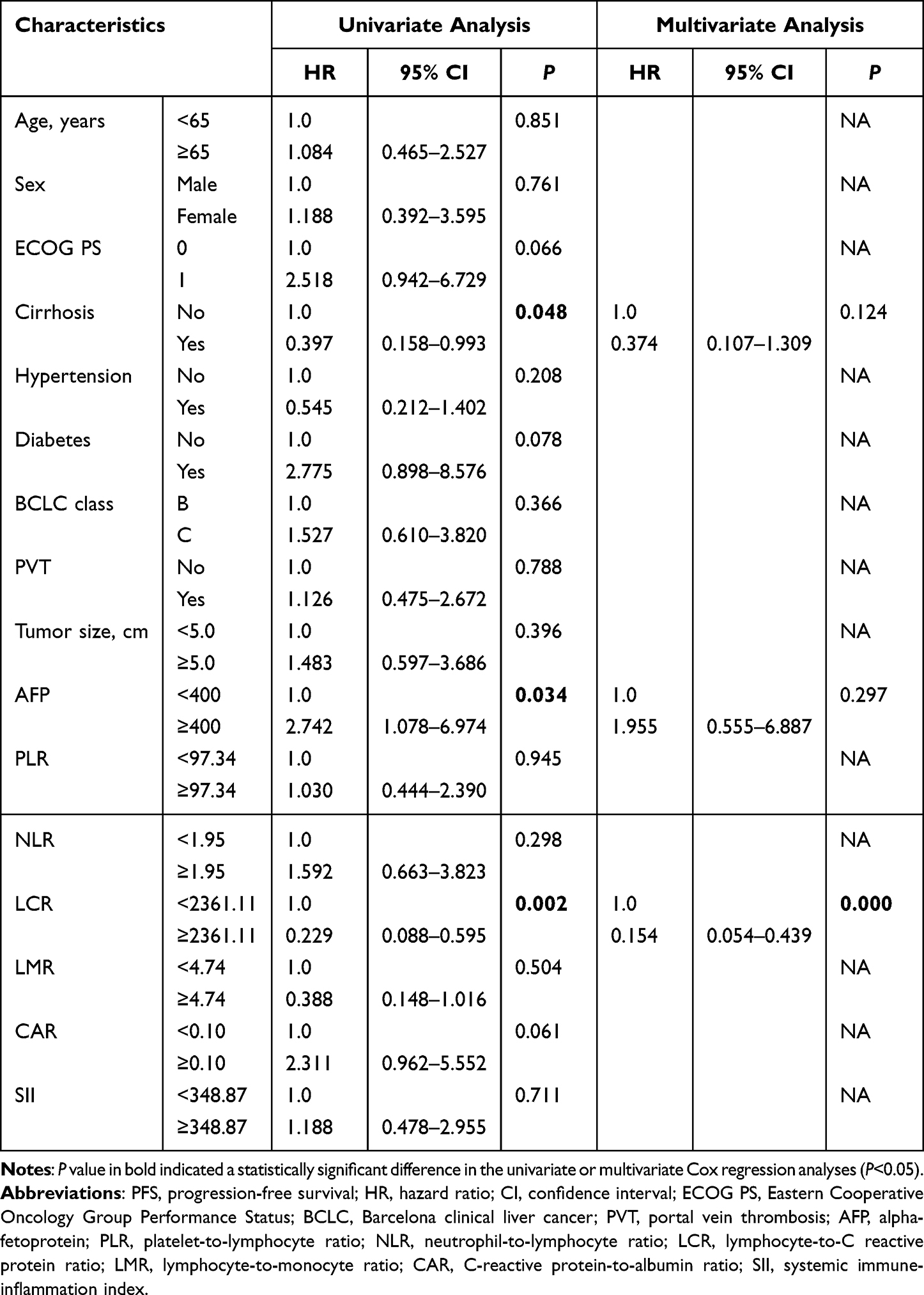 |
Table 2 Uni- and Multivariate Analyses for PFS |
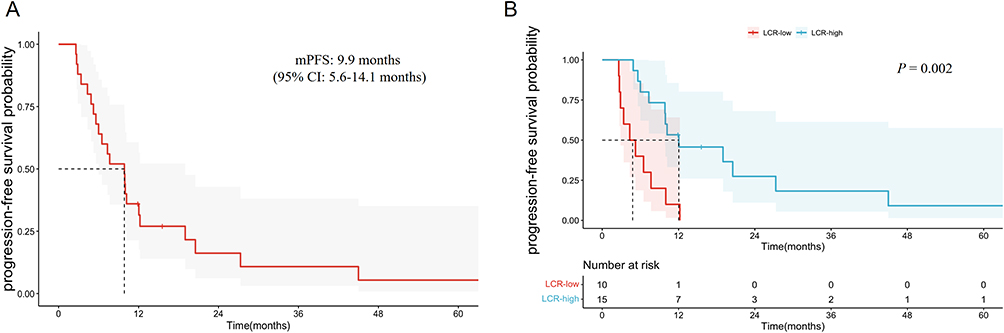 |
Figure 2 Kaplan–Meier curves for PFS (A), and stratified by LCR (B). Abbreviations: PFS, progression-free survival; LCR, lymphocyte‐to-C reactive protein ratio. |
Analysis of OS by Inflammatory Markers
In the efficacy population, the median OS was 18.5 months (95% CI 14.2–22.8 months), and 6 patients were alive at the last follow-up (Figure 3A). We then analyzed the association between inflammatory factors and overall survival benefit (Table 3). By univariate Cox regression analysis, we found that the following characteristics, including diabetes, AFP ≥ 400 ng/mL, LCR < 2361.11, LMR < 4.74, and without cirrhosis were negative prognostic predictors for OS. Furthermore, the multivariate analysis was performed, and the results suggested that patients with higher LCR (≥2361.11) achieved longer OS compared with the lower LCR group (21.9 vs 11.4 months, HR 0.310, 95% CI 0.114–0.844, P = 0.022). Two years after treatment, there were 1 (10.0%) and 6 (40.0%) patients were still alive in the lower and higher LCR group, respectively. Furthermore, elevated AFP (≥400 ng/mL) was significantly associated with worse OS (15.8 vs 28.3 months, HR 4.148, 95% CI 1.336–12.878, P = 0.014), and patients with diabetes also had a shorter survival time (10.5 vs 21.9 months, HR 4.258, 95% CI 1.273–14.245, P = 0.019) (Figure 3B–D).
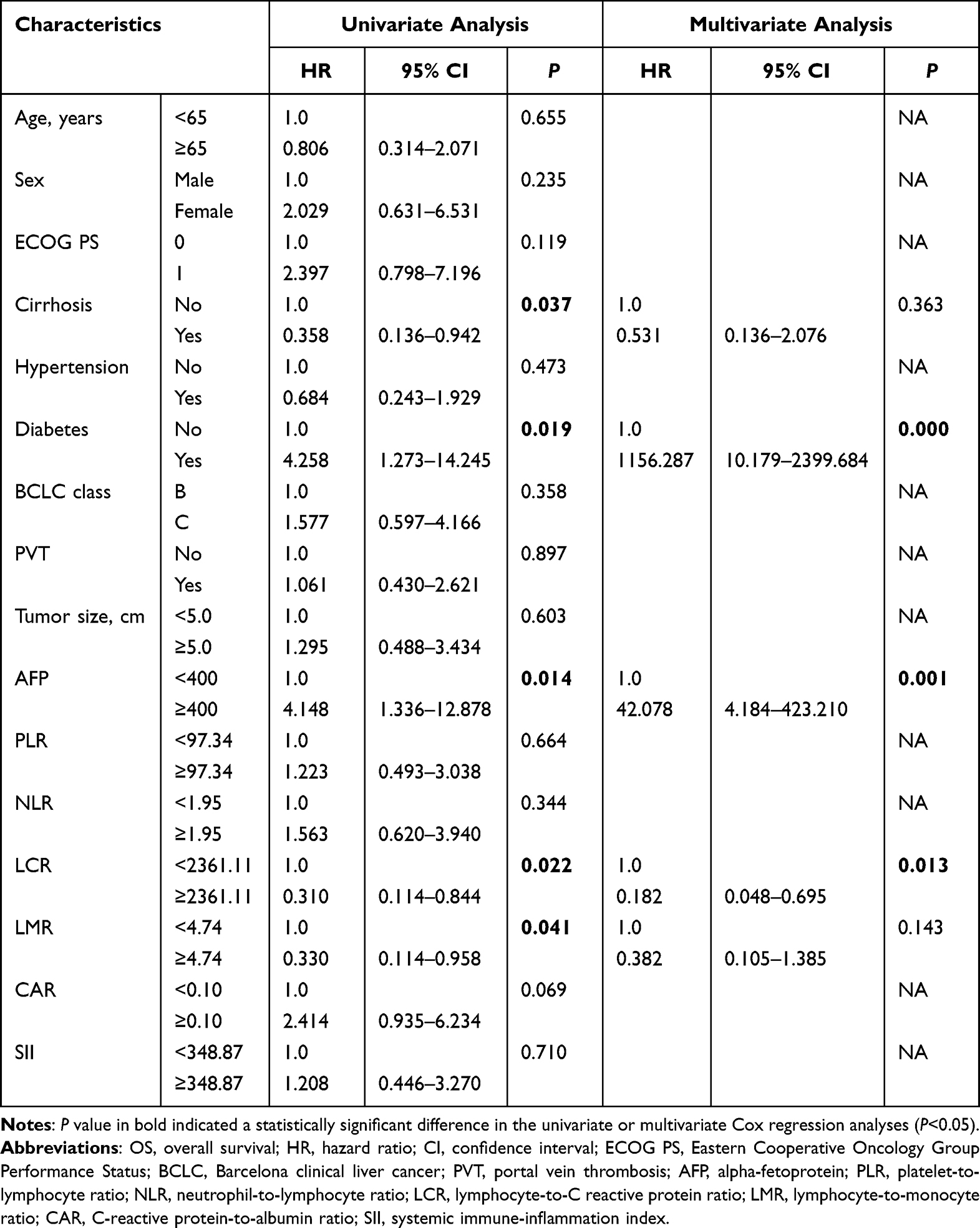 |
Table 3 Uni- and Multivariate Analyses for OS |
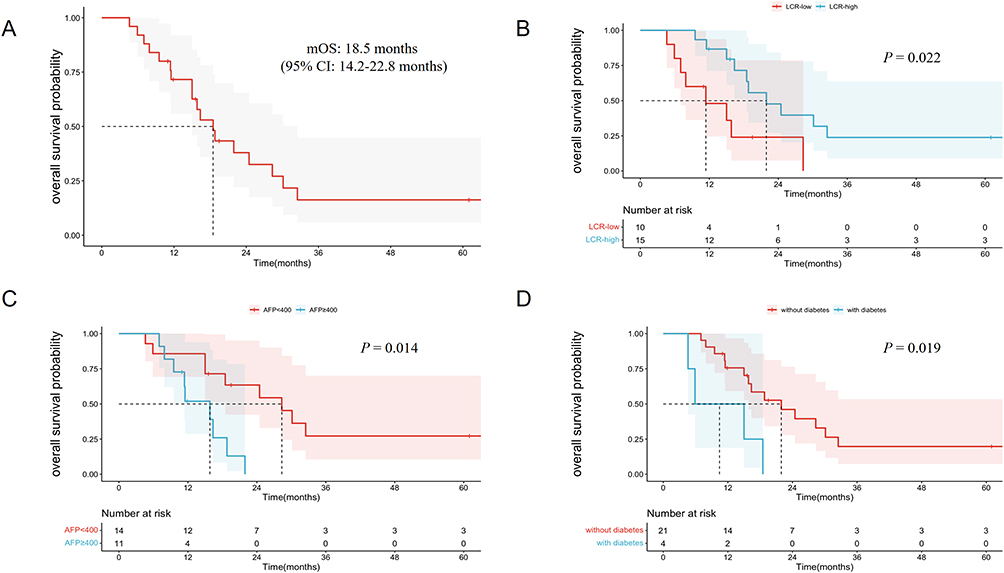 |
Figure 3 Kaplan–Meier curves for OS (A), and stratified by LCR (B), AFP (C), and diabetes (D). Abbreviations: OS, overall survival; LCR, lymphocyte‐to-C reactive protein ratio; AFP, alpha-fetoprotein. |
Tumor Response
As shown in Supplementary Table 1 and Supplementary Figure 4, 15 patients achieved the radiologic partial response, and 10 had stable disease on treatment with radiotherapy. The ORR and DCR were 60.0% and 100%, respectively. Patients with higher PLR, LCR, LMR, and lower CAR achieved better objective response rates compared to the control group (PLR: 69.2% vs 50.0%, P = 0.428; LCR: 66.7% vs 50.0%, P = 0.442; LMR: 66.7% vs 56.3%, P = 0.691; CAR: 66.7% vs 53.8%, P = 0.688), although no statistical significance was observed.
Liver Toxicity
Overall, there were no treatment-related deaths or radiation-induced liver disease (RILD) in the three months following radiation therapy. The most common hepatotoxicities were an increase in gamma-glutamyl transferase (GGT) (84.0%) and a decrease in albumin (44.0%). Nine patients (40.0%) showed an elevated alanine aminotransferase (ALT). In addition, the main severe toxicity (grade ≥ 3) was the higher GGT value (Supplementary Table 2). All hepatic toxicities were well tolerated and improved with symptomatic treatment. We further assessed the relationship between inflammatory biomarkers and liver toxicity, but there were no independent predictors for the adverse events (Supplementary Figure 5).
Discussion
This study presents the promising tumor response, survival benefits, and tolerable toxicity of radiotherapy in patients with intermediate and advanced-stage HCC. Additionally, it identified LCR as a significant independent prognostic factor for HCC patients undergoing radiotherapy for the first time.
As one of the most lethal malignancies, HCC results in poor survival due to the lack of effective treatment regimens. Either surgery or radiofrequency is only available for early-stage liver cancer. TACE and HAIC are now effective locoregional therapies for patients with intermediate-stage HCC.18 The RATIONALE-301 study demonstrated that single-agent tislelizumab had better and durable treatment responses compared to sorafenib as the initial treatment for HCC.19 Combining immunotherapy with targeted therapy has also emerged as a promising approach.20 As reported by the IMbrave150 clinical trial,21 atezolizumab plus bevacizumab resulted in superior survival benefits compared to sorafenib for unresectable HCC patients (median OS: 19.2 vs 3.4 months, descriptive P < 0.001; median PFS: 6.9 vs 4.3 months, descriptive P < 0.001). Another phase 3 study, CARES-310, revealed that the combination of camrelizumab and rivoceranib significantly improved the median PFS (5.6 vs 3.7 months) and OS (22.1 vs 15.2 months) versus sorafenib alone,6 these findings provided more novel and effective treatment modalities for HCC patients. However, local recurrences after curative treatment and distant metastasis to bone, lung, and lymph nodes are the main reasons for treatment failure.4,22 SBRT is a safe and effective alternative treatment regimen compared to TACE for HCC patients with either 1–2 tumors23 or medium-sized (3–8 cm) tumors.24 A single-arm, Phase 2 study showed that sequential TACE and SBRT followed by an anti-programmed cell death ligand-1 (PD-L1) drug achieved promising outcomes for patients with locally advanced HCC. The ORR was 67%, and the DCR was 70%. Additionally, the rates of local control at 6, 12, and 24 months were 98%, 92%, and 92%, respectively.25 SBRT was also confirmed to be associated with lower recurrence rates than RFA in unresectable Asian HCC patients (20.1% vs 27.9%, P < 0.001).26 The STRSPH trial demonstrated acceptable toxicities and promising survival benefits of SBRT for previously untreated solitary HCC that is not amenable to curative treatment options.27 Our previous study also showed a high local control rate of 100% and survival rate of 43% at 2 years with hypofractionated radiotherapy (PTV 50 Gy/10 fractions) using helical tomotherapy.28 In the current study, 25 patients underwent radiotherapy with a PTV dose of 24–30 Gy/8-10 fractions and a PGTV dose of 40–50 Gy/8-10 fractions to the primary liver lesions, and all patients achieved disease control, and no severe liver toxicity occurred during treatment, even for patients with poorer baseline liver function of Child-Pugh class B, who were reported to have a higher risk of RILD,29 further confirming the high efficacy and safety of SBRT with our radiation treatment plan.
The development of HCC is often related to chronic inflammation and subsequent liver cirrhosis caused by persistent hepatitis B virus (HBV) or hepatitis C virus (HCV) infection. Shalapour e reported that chronic inflammation induced the accumulation of immunoglobulin-A-producing (IgA+) cells, that directly inhibited the activation of CD8+ T lymphocytes (CTLs), and further promoted the development of HCC.30 Inflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α) and interleukin (IL)-6, as well as their downstream targets, have been shown to mediate the inflammation-associated HCC.31 Accumulating evidence suggests that inflammation-based markers are closely associated with the treatment response and adverse events for different treatment regimens, including HCC.32–34 In which, CRP is widely used to reflect the inflammatory status of cancers, peripheral lymphocytes play a vital role in host cell-mediated cytotoxic immunity against infection and tumors. The combination of CRP levels along with lymphocyte count, both LCR and CLR have also been reported to correlate with prognosis in several cancers, such as colorectal and gastric cancer.35,36 In terms of HCC, high LCR was found to be a predictor for better overall survival, as well as recurrence-free survival after liver resection.37 Recently, Lo et al found that pre-treatment NLR could be a valuable marker to predict the survival and hepatotoxicity in HCC patients treated with stereotactic ablative radiation therapy (SART).34 However, no related study about the relationship between LCR and radiotherapy for HCC has been reported yet. In the current study, we first observed a significant decrease in LCR after radiotherapy compared with baseline (median: 3448.28 vs 1538.46, P = 0.001), and found that high LCR was associated with prolonged PFS (12.0 vs 4.3 months, P = 0.002) and OS (21.9 vs 11.4 months, P = 0.022), the Cox regression analyses further demonstrated its role as an independent prognostic predictor for HCC patients receiving radiotherapy.
Diabetes is a risk factor for the development of HCC, it has been validated to activate inflammatory cascades through the generation of pro-inflammatory cytokines and reactive oxygen species, leading to genomic instability, cell proliferation, and inhibition of cell apoptosis, thereby promoting hepatocarcinogenesis.38 In our results, it is interesting to note that the history of diabetes was negatively related to the OS, whereas no significance was observed about the PFS. As one of the most common tumor markers, AFP-positive HCC (APHC) accounts for about 75%, of those who had less cytotoxic T cells and more suppressive tumor immune microenvironment (TIME).39 In our study, over 40% of patients experienced elevated levels of AFP (≥400 ng/mL), they had worse PFS and OS compared to lower AFP group (mPFS: 5.6 vs 10.2 months, P = 0.028; mOS: 15.8 vs 28.3 months, P = 0.014), the multivariate Cox regression analysis further confirmed AFP was an independent prognostic factor for OS, which was consistent with previous findings.40
In terms of radiotherapy safety, the most common liver toxicity was the elevated GGT (84.0%), and only one patient had severe elevated GGT, there was no death or treatment interruption during radiotherapy, which might be partially associated with the residual normal liver volume was above 700 mL in our radiation plan. We further analyzed the relationship between inflammatory indices and liver toxicity, and found no statistical significance, which reminds us to explore more potential markers to predict the adverse events.
This study has several limitations. Firstly, it was a single-center, retrospective study, which could lead to selection bias. Secondly, the sample size was small, and the conclusion needs to be further confirmed by larger cohorts. Thirdly, some confounding factors, such as medication usage, immune system status, and comorbidities, could potentially impact the results of the inflammatory index. In addition, the heterogeneity of treatment regimens prior to radiotherapy might be associated with the outcome.
In conclusion, our study confirmed the high efficacy and good tolerability of radiotherapy in patients with intermediate and advanced-stage HCC and, for the first time, demonstrated the association between LCR and survival benefit after SBRT. The predictive and prognostic potential of LCR should be further confirmed by prospective studies with larger sample sizes in the future.
Abbreviations
HCC, hepatocellular carcinoma; SBRT, stereotactic body radiotherapy; LCR, lymphocyte‐to-C reactive protein ratio; PLR, platelet-to-lymphocyte ratio; NLR, neutrophil-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; CAR, C-reactive protein-to-albumin ratio; SII, systemic immune-inflammation index; PFS, progression-free survival; OS, overall survival.
Data Sharing Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
All procedures performed in this study involving human participants were in accordance with the guidelines of the Ethics Committee of Nanjing Drum Tower Hospital and with the 1964 Helsinki Declaration. Patients treated in our hospital will be informed of the potential research use of personal information. Only patients who agreed with and signed the consent were included in our study.
Acknowledgments
The authors thank the patients for their participation in the current study.
Funding
The study was supported by the National Natural Science Foundation of Nanjing University of Chinese Medicine (No. XZR2023075); The Hospital Management Research of Jiangsu Province (No. JSYGY-3-2023-618); and Medical Science and Technology Development Foundation of Nanjing (No. YKK22095).
Disclosure
All authors declare no conflicts of interest related to this manuscript.
References
1. Sung H, Ferlay J, Siegel RL. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. doi:10.3322/caac.21660
2. Rumgay H, Arnold M, Ferlay J, et al. Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol. 2022;77:1598–1606. doi:10.1016/j.jhep.2022.08.021
3. Garuti F, Neri A, Avanzato F, Gramenzi A. The changing scenario of hepatocellular carcinoma in Italy: an update. Liver Int. 2021;41:585–597. doi:10.1111/liv.14735
4. Brown ZJ, Tsilimigras DI, Ruff SM, et al. Management of hepatocellular carcinoma: a review. JAMA Surg. 2023;158:410–420. doi:10.1001/jamasurg.2022.7989
5. Kudo M. Durvalumab plus tremelimumab in unresectable hepatocellular carcinoma. Hepatobiliary Surg Nutr. 2022;11:592–596. doi:10.21037/hbsn-22-143
6. Qin S, Chan SL, Gu S, et al. Camrelizumab plus rivoceranib versus sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised, open-label, international phase 3 study. Lancet. 2023;402:1133–1146. doi:10.1016/S0140-6736(23)00961-3
7. Apisarnthanarax S, Barry A, Cao M, et al. External beam radiation therapy for primary liver cancers: an ASTRO clinical practice guideline. Pract Radiat Oncol. 2022;12:28–51. doi:10.1016/j.prro.2021.09.004
8. Sharma D, Thaper D, Kamal R, Yadav HP. Role of palliative SBRT in Barcelona clinic liver cancer-stage C hepatocellular carcinoma patients. Strahlenther Onkol. 2023;199:838–846. doi:10.1007/s00066-023-02065-x
9. Lewis S, Dawson L, Barry A, et al. Stereotactic body radiation therapy for hepatocellular carcinoma: from infancy to ongoing maturity. JHEP Rep. 2022;4:100498. doi:10.1016/j.jhepr.2022.100498
10. Nguyen QN, Chun SG, Chow E, et al. Single-fraction stereotactic vs conventional multifraction radiotherapy for pain relief in patients with predominantly nonspine bone metastases: a randomized phase 2 trial. JAMA Oncol. 2019;5:872–878. doi:10.1001/jamaoncol.2019.0192
11. Dawson L, Winter K, Knox J, et al. NRG/RTOG 1112: randomized Phase III study of sorafenib vs. stereotactic body radiation therapy (SBRT) followed by sorafenib in hepatocellular carcinoma (HCC). J Clin oncol. 2023;41:489. doi:10.1200/JCO.2023.41.4_suppl.489
12. Chen YX, Yang P, Du SS, et al. Stereotactic body radiotherapy combined with sintilimab in patients with recurrent or oligometastatic hepatocellular carcinoma: a Phase II clinical trial. World J Gastroenterol. 2023;29:3871–3882. doi:10.3748/wjg.v29.i24.3871
13. McLaughlin M, Patin EC, Pedersen M, Wilkins A. Inflammatory microenvironment remodelling by tumour cells after radiotherapy. Nat Rev Cancer. 2020;20:203–217. doi:10.1038/s41568-020-0246-1
14. Qiu X, Shi Z, Tong F, et al. Biomarkers for predicting tumor response to PD-1 inhibitors in patients with advanced pancreatic cancer. Hum Vaccin Immunother. 2023;19:2178791. doi:10.1080/21645515.2023.2178791
15. Yamamoto T, Kawada K, Bagnato VS, Romero MP. Inflammation-related biomarkers for the prediction of prognosis in colorectal cancer patients. Int J Mol Sci. 2021;23:22. doi:10.3390/ijms23010022
16. Erler D, Brotherston D, Sahgal A, et al. Local control and fracture risk following stereotactic body radiation therapy for non-spine bone metastases. Radiother Oncol. 2018;127:304–309. doi:10.1016/j.radonc.2018.03.030
17. Oldenburger E, Brown S, Willmann J, et al. ESTRO ACROP guidelines for external beam radiotherapy of patients with complicated bone metastases. Radiother Oncol. 2022;173:240–253. doi:10.1016/j.radonc.2022.06.002
18. Llovet JM, De Baere T, Kulik L, et al. Locoregional therapies in the era of molecular and immune treatments for hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2021;18:293–313. doi:10.1038/s41575-020-00395-0
19. Qin S, Kudo M, Meyer T, et al. Tislelizumab vs sorafenib as first-line treatment for unresectable hepatocellular carcinoma: a phase 3 randomized clinical trial. JAMA Oncol. 2023;9:1651–1659. doi:10.1001/jamaoncol.2023.4003
20. Stefanini B, Ielasi L, Chen R. TKIs in combination with immunotherapy for hepatocellular carcinoma. Expert Rev Anticancer Ther. 2023;23:279–291. doi:10.1080/14737140.2023.2181162
21. Cheng AL, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76:862–873. doi:10.1016/j.jhep.2021.11.030
22. Vogel A, Meyer T, Sapisochin G, et al. Hepatocellular carcinoma. Lancet. 2022;400:1345–1362. doi:10.1016/S0140-6736(22)01200-4
23. Sapir E, Tao Y, Schipper MJ, et al. Stereotactic body radiation therapy as an alternative to transarterial chemoembolization for hepatocellular carcinoma. Int J Radiat Oncol Biol Phys. 2018;100:122–130. doi:10.1016/j.ijrobp.2017.09.001
24. Shen PC, Chang WC, Lo CH, et al. Comparison of stereotactic body radiation therapy and transarterial chemoembolization for unresectable medium-sized hepatocellular carcinoma. Int J Radiat Oncol Biol Phys. 2019;105:307–318. doi:10.1016/j.ijrobp.2019.05.066
25. Chiang CL, Chiu KWH, Chan KSK, et al. Sequential transarterial chemoembolisation and stereotactic body radiotherapy followed by immunotherapy as conversion therapy for patients with locally advanced, unresectable hepatocellular carcinoma (START-FIT): a single-arm, phase 2 trial. Lancet Gastroenterol Hepatol. 2023;8:169–178. doi:10.1016/S2468-1253(22)00339-9
26. Kim N, Cheng J, Jung I, et al. Stereotactic body radiation therapy vs. radiofrequency ablation in Asian patients with hepatocellular carcinoma. J Hepatol. 2020;73:121–129. doi:10.1016/j.jhep.2020.03.005
27. Kimura T, Takeda A, Sanuki N, et al. Multicenter prospective study of stereotactic body radiotherapy for previously untreated solitary primary hepatocellular carcinoma: the STRSPH study. Hepatol Res. 2021;51:461–471. doi:10.1111/hepr.13595
28. Shen J, Yan J, Zhu S, et al. The efficacy and safety of hypofractionated radiation therapy with tomotherapy for advanced or recurrent hepatocellular carcinoma. Front Oncol. 2021;11:559112. doi:10.3389/fonc.2021.559112
29. D’Avola D, Granito A, Torre-Aláez M, Piscaglia F. The importance of liver functional reserve in the non-surgical treatment of hepatocellular carcinoma. J Hepatol. 2022;76:1185–1198. doi:10.1016/j.jhep.2021.11.013
30. Shalapour S, Lin XJ, Bastian IN, et al. Inflammation-induced IgA+ cells dismantle anti-liver cancer immunity. Nature. 2017;551:340–345. doi:10.1038/nature24302
31. Ishtiaq SM, Arshad MI, Khan JA. PPARγ signaling in hepatocarcinogenesis: mechanistic insights for cellular reprogramming and therapeutic implications. Pharmacol Ther. 2022;240:108298. doi:10.1016/j.pharmthera.2022.108298
32. Valero C, Lee M, Hoen D, et al. Pretreatment neutrophil-to-lymphocyte ratio and mutational burden as biomarkers of tumor response to immune checkpoint inhibitors. Nat Commun. 2021;12:729. doi:10.1038/s41467-021-20935-9
33. Chan SL, Wong LL, Chan KA, et al. Development of a novel inflammation-based index for hepatocellular carcinoma. Liver Cancer. 2020;9:167–181. doi:10.1159/000504252
34. Lo CH, Lee HL, Hsiang CW, et al. Pretreatment neutrophil-to-lymphocyte ratio predicts survival and liver toxicity in patients with hepatocellular carcinoma treated with stereotactic ablative radiation therapy. Int J Radiat Oncol Biol Phys. 2021;109:474–484. doi:10.1016/j.ijrobp.2020.09.001
35. Ruan GT, Xie HL, Zhang HY, et al. Association of systemic inflammation and low performance status with reduced survival outcome in older adults with cancer. Clin Nutr. 2022;41:2284–2294. doi:10.1016/j.clnu.2022.08.025
36. Matsunaga T, Saito H, Fukumoto Y, et al. The prognostic impact of the lymphocyte-to-C-reactive protein ratio in patients with unresectable or recurrent advanced gastric cancer treated with first- and second-line treatment. Surg Today. 2023;53:940–948. doi:10.1007/s00595-022-02638-w
37. Utsumi M, Inagaki M. Preoperative lymphocyte-to-C-reactive protein ratio predicts hepatocellular carcinoma recurrence after surgery. Ann Surg Treat Res. 2022;103:72–80. doi:10.4174/astr.2022.103.2.72
38. Yang JD, Ahmed F, Mara KC, et al. Diabetes is associated with increased risk of hepatocellular carcinoma in patients with cirrhosis from nonalcoholic fatty liver disease. Hepatology. 2020;71:907–916. doi:10.1002/hep.30858
39. He H, Chen S, Fan Z, et al. Multi-dimensional single-cell characterization revealed suppressive immune microenvironment in AFP-positive hepatocellular carcinoma. Cell Discov. 2023;9:60. doi:10.1038/s41421-023-00563-x
40. Riaz A, Ryu RK, Kulik LM, et al. Alpha-fetoprotein response after locoregional therapy for hepatocellular carcinoma: oncologic marker of radiologic response, progression, and survival. J Clin Oncol. 2009;27:5734–5742. doi:10.1200/JCO.2009.23.1282
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Delayed Hepatocellular Carcinoma Recurrence After Liver Transplantation: Comprehensive Clinical Characterization of Case Series
Wong TH, Ho CM, Hsu HH, Wu YM, Ho MC, Lee PH, Hu RH
Journal of Hepatocellular Carcinoma 2022, 9:1081-1091
Published Date: 17 October 2022
Prognostic Significance of Hemoglobin, Albumin, Lymphocyte and Platelet (HALP) Score in Hepatocellular Carcinoma
Zhou J, Yang D
Journal of Hepatocellular Carcinoma 2023, 10:821-831
Published Date: 2 June 2023
A Novel Four-Gene Signature Based on Nonsense-Mediated RNA Decay for Predicting Prognosis in Hepatocellular Carcinoma: Bioinformatics Analysis and Functional Validation
Zhao J, Wang C, Zhao L, Zhou H, Wu R, Zhang T, Ding J, Zhou J, Zheng H, Zhang L, Kong T, Zhou J, Hu Z
Journal of Hepatocellular Carcinoma 2024, 11:747-766
Published Date: 23 April 2024
Portal Venous and Hepatic Arterial Coefficients Predict Post-Hepatectomy Overall and Recurrence-Free Survival in Patients with Hepatocellular Carcinoma: A Retrospective Study
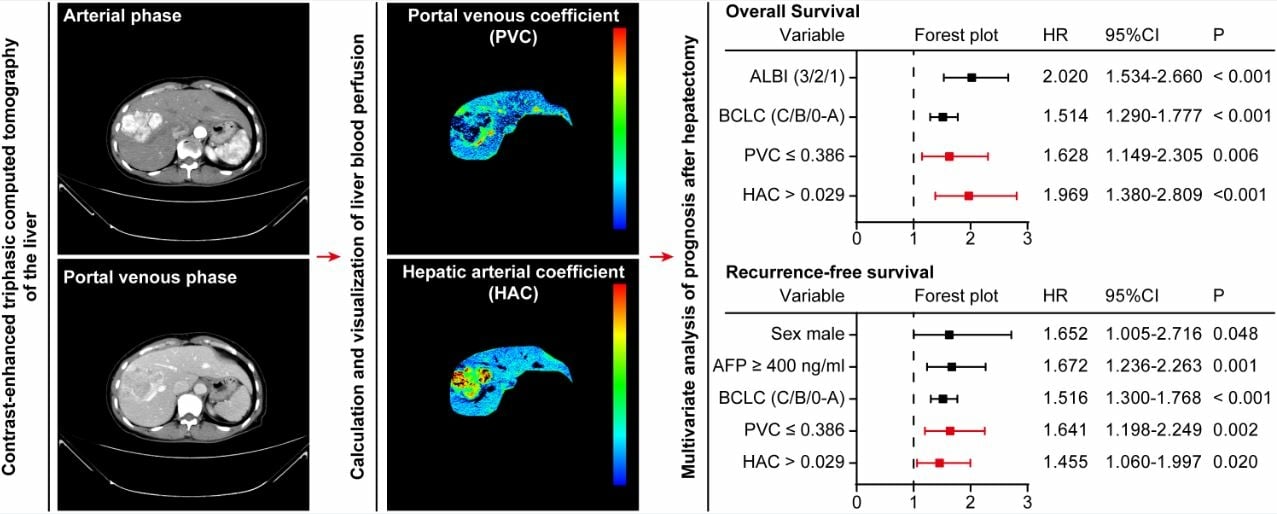
Li YK, Wu S, Wu YS, Zhang WH, Wang Y, Li YH, Kang Q, Huang SQ, Zheng K, Jiang GM, Wang QB, Liang YB, Li J, Lakang Y, Yang C, Li J, Wang JP, Kui X, Ke Y
Journal of Hepatocellular Carcinoma 2024, 11:1389-1402
Published Date: 9 July 2024
Comparative Performance of Stereotactic Body Radiotherapy and Lenvatinib in Unresectable Hepatocellular Carcinoma Complicated by Portal Vein Tumor Thrombosis: A Propensity Score-Matched Cohort Analysis
Huang J, Liu FC, Yang Y, Yuan SX, Gu FM, Jiang BG, Pan ZY
Journal of Hepatocellular Carcinoma 2026, 13:589137
Published Date: 15 June 2026