Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Lurasidone in Schizophrenia Management: A Comprehensive 12-Week Post-Marketing Surveillance Study in Chinese Patients
Authors Wei YM, Yang XD, Wang CS ![]() , Wang LL, Deng HL, Sang H, Xue AL, Zhu DM, Li-YM, Liu XJ, Li H, Shen YF
, Wang LL, Deng HL, Sang H, Xue AL, Zhu DM, Li-YM, Liu XJ, Li H, Shen YF ![]()
Received 12 December 2025
Accepted for publication 18 February 2026
Published 12 March 2026 Volume 2026:22 588526
DOI https://doi.org/10.2147/NDT.S588526
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Yu-mei Wei,1 Xiao-dong Yang,2 Chuan-sheng Wang,3 Li-li Wang,4 Huai-li Deng,5 Hong Sang,6 Ai-lan Xue,7 Dao-min Zhu,8 You-ming Li,9 Xue-jun Liu,10 Hai-yun Li,11 Yi-feng Shen1 On behalf of post-market surveillance investigators
1Shanghai Mental Health Center, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2Department of Psychiatry, Shandong Provincial Mental Health Center, Jinan, Shandong, People’s Republic of China; 3The Second Affiliated Hospital of Xinxiang Medical University, Xinxiang, Henan, People’s Republic of China; 4Department of Psychiatry, Tianjin Mental Health Center, Tianjin Anding Hospital, Tianjin, People’s Republic of China; 5Department of Psychiatry, Shanxi Mental Health Center (Taiyuan Mental Hospital), Taiyuan, Shanxi, People’s Republic of China; 6Department of Psychiatry, Changchun Sixth Hospital, Changchun, Jilin, People’s Republic of China; 7Department of Psychiatry, Zhuzhou Third Hospital, Zhuzhou, Hunan, People’s Republic of China; 8Department of Sleep Disorders, Affiliated Psychological Hospital of Anhui Medical University, Hefei Fourth People’s Hospital, Anhui Mental Health Center, Hefei, Anhui, People’s Republic of China; 9Department of Medical Equipment, Ganzhou Third People’s Hospital, Ganzhou, Jiangxi, People’s Republic of China; 10Department of Mental Psychology, Hunan Brain Hospital (Hunan Second People’s Hospital), Changsha, Hunan, People’s Republic of China; 11Sumitomo Pharma (China) Co., Ltd, Shanghai, People’s Republic of China
Correspondence: Yi-feng Shen, Email [email protected]
Objective: To evaluate the safety and effectiveness of lurasidone in Chinese patients with schizophrenia in a 12-week post-marketing study.
Methods: This 12-week, multicenter, prospective, open-label, single-arm study included schizophrenia patients from 36 sites in Mainland China, who initiated lurasidone between September 2019 and December 2023. Adverse events (AEs) and adverse drug reactions (ADRs) were primary safety endpoints. Other safety assessments included extrapyramidal symptoms (EPS) and weight gain. Effectiveness was evaluated using the Brief Psychiatric Rating Scale (BPRS) at baseline and week 12. Patients were also stratified to assess differences across ages.
Results: A total of 3170 patients were included in the Full Analysis Set (FAS) and 3178 in the Safety Set (SS). The mean daily lurasidone dose was 59.9± 20.93 mg. ADRs occurred in 7.9% of patients, with incidences of 8.1%, 8.9%, 5.9%, and 2.3% in the < 18, 18– 45, 45– 65, and > 65-year age groups, respectively. EPS was the most common ADR (3.2%), typically emerging in weeks 3– 4. Metabolic-related AEs occurred in 4.3% and 2.2% of patients with and without metabolic affecting agents. BPRS scores significantly improved at weeks 2/4, 6/8, and 12 compared with baseline (all P < 0.05): total score (− 8.9 ± 9.62, − 14.0 ± 12.16, − 17.5 ± 13.61), anxiety-depression (− 1.5 ± 2.37, − 2.5 ± 2.88, − 3.3 ± 3.31), anergia (− 1.5 ± 2.34, − 2.4 ± 2.83, − 3.1 ± 3.11), thought disturbance (− 2.4 ± 2.98, − 3.8 ± 3.72, − 4.7 ± 4.07), activation (− 1.2 ± 1.97, − 1.7 ± 2.38, − 2.1 ± 2.63), and hostility-suspiciousness (− 2.4 ± 2.81, − 3.6 ± 3.44, − 4.3 ± 3.76). In < 18 years group, BPRS total score also significantly decreased from 46.1± 15.10 at baseline to 26.3± 9.72 at week 12.
Conclusion: This real-world study demonstrated a favorable safety profile and significant clinical effectiveness of lurasidone in both adult and adolescent population with schizophrenia in China in real-world clinical settings, supporting its use across diverse patient populations.
Trial Registration: Shanghai Clinical Research Center for Mental Health (SCRC-MH) NCT04432688. URL: www.smhc.org.cn/.
Keywords: schizophrenia, lurasidone, safety, effectiveness, chinese population
Introduction
Schizophrenia is a severe mental disorder affecting approximately 23 million people worldwide, or 1 in 345 individuals (0.29%). 1 An epidemiological survey of mental illness conducted across 31 provinces and cities in China in 2013 showed that the lifetime prevalence of schizophrenia was 6 ‰.2 Schizophrenia is associated with considerable disability and can affect all aspects of life, resulting a loss of 3.48 million Disability Adjusted Life Years in China.1,3
Pharmacological treatment remains the cornerstone of schizophrenia management. According to current recommendations of international treatment guidelines, including those from the United States, Europe, and the World Psychiatric Association (WPA), second-generation (atypical) antipsychotics are generally recommended as first-line treatment.4 However, non‑adherence, which is strongly associated with an increased risk of relapse and psychiatric hospitalization, remains a major unmet need in schizophrenia.5 The CATIE study6 showed that as many as 64% to 82% of patients treated with second-generation (atypical) antipsychotics discontinued treatment within 18 months due to inadequate effectiveness, adverse effects (such as weight gain and metabolic problems), patient decisions, and other reasons. Among the identified risk factors for poor medication adherence, two are particularly influential: the safety profile of antipsychotics and the therapeutic alliance.5,7,8 Therefore, selecting agents that are both effective and well tolerated early in the treatment course is essential. Compared with first-generation antipsychotics, second-generation antipsychotics such as clozapine, olanzapine, risperidone, and quetiapine cause fewer extrapyramidal adverse reactions, but can cause adverse reactions such as metabolic syndrome, including weight gain and abnormal glucose and lipid metabolism, which significantly affect the safety, tolerability, and treatment adherence.4 In addition, transparent communication about medication risks and benefits, along with shared decision making, strengthens trust between patients, family members and healthcare providers. These practices enhance the therapeutic alliance and improve adherence, as recommended by guidelines.9,10
Lurasidone, a newer atypical antipsychotic, has been approved in multiple countries for the treatment of schizophrenia and has become one of major treatment choices in China following its approval in 2019. Lurasidone has high affinity for dopamine D2 and 5-HT2A receptors. Furthermore, its antagonism of 5-HT7 and partial agonism of 5-HT1A receptors may contribute to improvements in emotional and cognitive symptoms. Lurasidone has minimal or no affinity for histamine H1 and acetylcholine M1 receptors, as well as minimal affinity for 5-HT2C, thus causing fewer adverse effects such as weight gain and metabolic abnormalities.11 In addition, lurasidone has been shown to have minimal impact on prolactin levels and QTc.12
Extensive evidence has demonstrated the efficacy and safety of lurasidone in patients with schizophrenia.13,14 However, one study reported that Chinese individuals exhibit approximately 37% higher drug exposure compared to Western populations.15 Given the complexity of routine clinical settings, large-scale real‑world studies are needed to further evaluate lurasidone’s safety and effectiveness in diverse Chinese populations. A prospective, non-interventional, open-label, single-arm post-marketing surveillance (PMS) was conducted in Chinese patients with schizophrenia between 2019 and 2023.16 By enrolling a broad patient population under routine clinical settings, this study complements randomized controlled trials by addressing key limitations related to restricted eligibility criteria, standardized treatment regimens, limited sample sizes, and short follow‑up durations.17,18 Its interim analysis showed that lurasidone significantly improved symptoms in these patients, with a favorable safety profile.16 However, this interim analysis was based on 965 patients and primarily reflected overall treatment outcomes. Clinically meaningful differences such as tolerability across patient subgroups remain insufficiently characterized. Therefore, we analyzed the complete PMS dataset to provide a more comprehensive evaluation of lurasidone in real‑world settings, aiming to inform treatment regimen optimization, support shared decision-making, and strengthen the therapeutic alliance. Specifically, we examined the safety profile in different age groups, the chronological sequence of adverse drug reactions (ADRs) and how patients’ metabolic profiles were affected when lurasidone was used in combination with drugs known to significantly influence metabolism, such as olanzapine, clozapine, valproates and lithium.
Methods
Study Design and Treatment
This analysis represented the complete report of the PMS conducted from September 2019 to December 2023 across 36 sites in China, expanding upon the previously published interim analysis.16 All patients who met the inclusion criteria were included in the Full Analysis Set (FAS). The Safety Set (SS) consisted of patients who received at least one dose of treatment and had post-treatment safety data available. Patients were also stratified into 4 age groups: <18 years, 18–45 years, 45–65 years, and >65 years. The dosage of lurasidone was determined by the investigators based on clinical judgment. Treatment typically begins at 40 mg/d and can be increased to 80 mg/d based on the patient’s condition.19 All investigators received standardized protocol training prior to study initiation, with ongoing training as needed. This study was approved by the ethics committee of the leading site, Shanghai Mental Health Center (Approval No.: 2019–72) and was conducted in accordance with the Declaration of Helsinki. All participants signed informed consent prior to enrollment. For participants under 18 years, written informed consent was obtained from a parent or legal guardian.
Study Outcomes and Measurements
Adverse events (AEs, defined as any unfavorable medical occurrence reported after treatment initiation) and ADRs (defined as AEs for which a causal relationship with lurasidone was considered at least a reasonable possibility) assessed and reported by the investigators were used as primary safety endpoints. Other safety endpoints included the incidence of extrapyramidal symptoms (EPS), akathisia, the proportion of patients requiring concomitant EPS medications at week 12, and changes in weight from baseline at different visits. Effectiveness endpoints included changes from baseline in the total score of Brief Psychiatric Rating Scale (BPRS) at different visits. The BPRS is a psychometric tool specifically designed to evaluate clinical changes in individuals with schizophrenia.20 This comprehensive scale consists of 18 distinct items. The assessment was performed using a 7-point Likert-type scale, with item ratings ranging from 1 (“not present”) to 7 (“extremely severe”), for a total score range from 18 to 126, calculated by summing the scores of each item. The BPRS measures five primary psychopathological dimensions:21 anxiety-depression, anergia, thought disturbance, activation, and hostility-suspiciousness. Additionally, scores were computed based on the established 5-factor model structure of the instrument.
Statistical Analysis
Statistical analyses were conducted using SAS 9.4 software (SAS Institute, Cary, North Carolina). All statistical tests were two-tailed, and a P values less than or equal to 0.05 were considered statistically significant. For descriptive statistics, continuous data were described using the mean, standard deviation. Categorical data were described by frequency and percentage. Effectiveness endpoint data were analyzed using the last-observation-carried forward (LOCF) approach for the missing values.
Results
Demographic and Pathogenic Characteristics at Baseline
A total of 3,192 patients with schizophrenia were enrolled across 36 centers. After screening, 3,170 patients were included in FAS and 3,178 in SS. Among them, 2855 patients completed the full 12-week surveillance.
More than 60% of the 3178 patients were between 18 and 45 years old, with 6.6% younger than 18 years. The mean baseline BPRS total score was 43.9 ± 14.66 (Table 1).
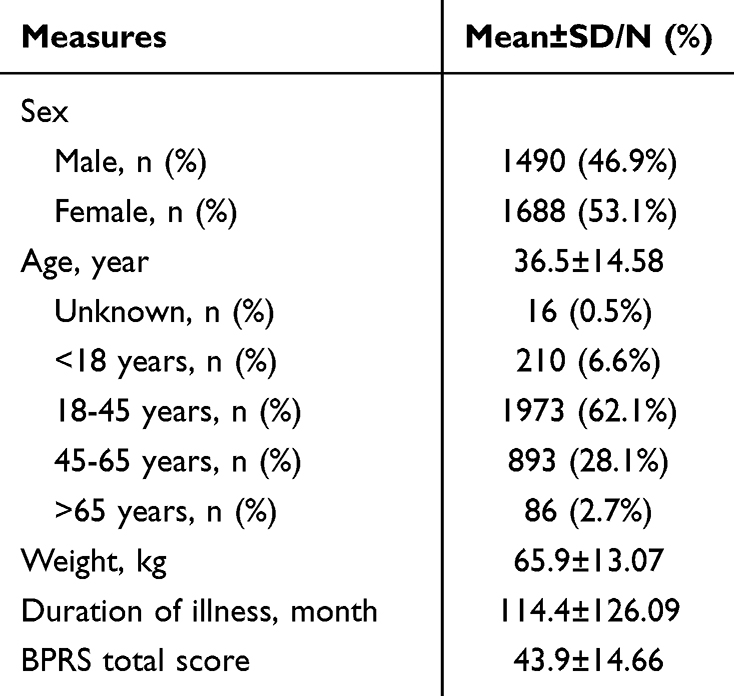 |
Table 1 Baseline Demographic Characteristics |
Medications
The average lurasidone exposure during the surveillance was 7137.2 mg, and the median duration of drug exposure was 85 days. The mean daily dose was 59.9±20.93 mg/d. By age, the mean daily doses of lurasidone in the <18, 18–45, 45–65, and >65-year groups were 63.5 ± 18.28, 60.9 ± 19.37, 56.0 ± 19.74, and 54.9 ± 20.90 mg/d, respectively. Most patients (2556/3170, 80.6%) initiated lurasidone at a dose of 40 mg/d.
A total of 1693 (53.3%) patients received polypharmacy during this surveillance. The most commonly used concomitant medications were oral antipsychotics (1251/3178, 39.4%), followed by sedative and hypnotic/therapeutic anti-EPS medication (332/3178, 10.4%), antidepressants and anxiolytics (183/3178, 5.8%), and mood stabilizer/antiepileptic drugs (129, 4.1%). Olanzapine was the most common concomitant medication (536, 16.9%), followed by clozapine (253, 8.0%), risperidone (211, 6.6%), and benzhexol (158/3178, 5.0%).
Safety Outcomes
A total of 370 of 3178 (11.6%) patients had AEs, including 2 patients (0.06%) with serious AEs. ADRs occurred in 250 patients (7.9%), accounting for 338 cases. One patient (0.03%) had a serious ADR. EPS was the most frequently reported ADR in this study (3.2%, 101/3178), and 14 patients (0.4%) withdrew from the surveillance due to EPS-related reactions (including akathisia, dystonia, extrapyramidal disorders, tremor, parkinsonism, etc). Chronologically, gastrointestinal disorders such as nausea and vomiting typically occurred early after initiation of lurasidone treatment, whereas weight gain tended to appear later. Nervous system disorders, including restlessness, dystonia, and other extrapyramidal symptoms, generally emerged during the third or fourth week of therapy (Figure 1 and Table 2).
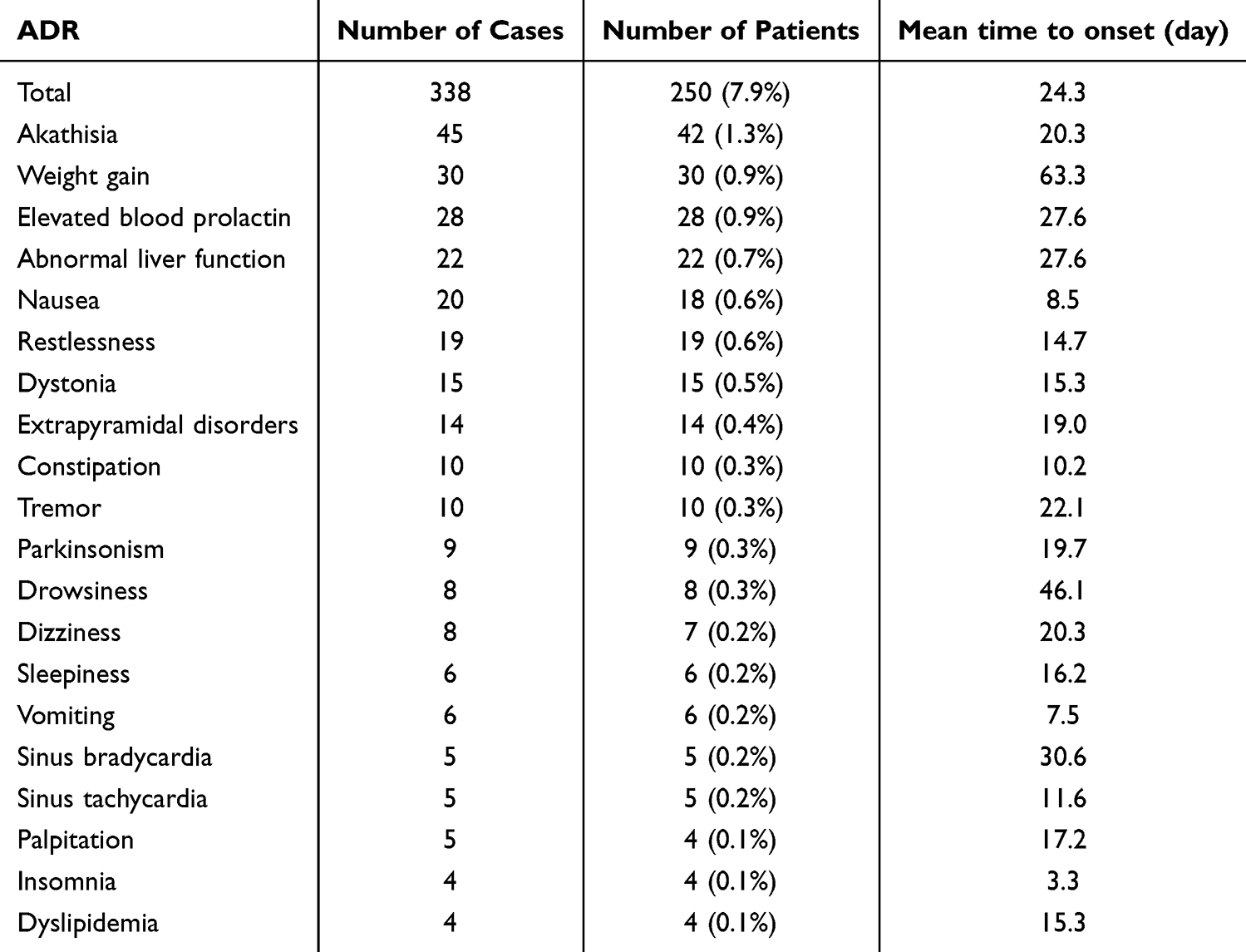 |
Table 2 The Incidence and Time to Onset of Major ADRs (>0.1%) |
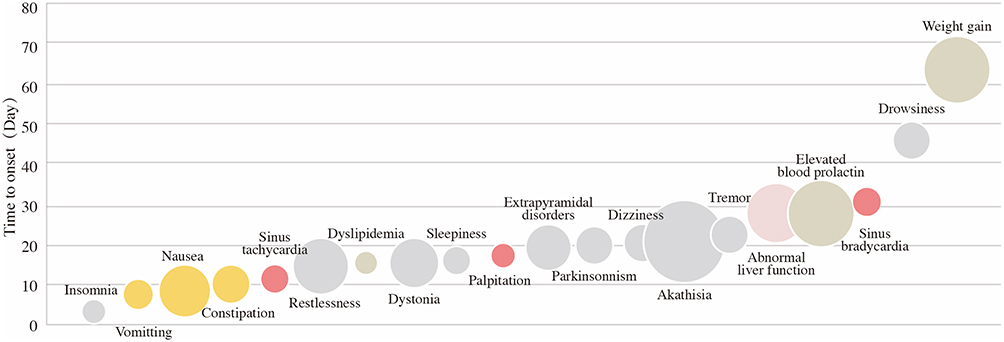 |
Figure 1 Time to onset of major ADRs during the surveillance (bubble size represents the incidence of ADRs, expressed as the percentage of patients experiencing at least one ADR). |
Incidences of ADRs in the <18, 18–45, 45–65, and >65-year age groups were 8.1% (17/210), 8.9% (175/1973), 5.9% (53/893), and 2.3% (2/86), respectively. A total of 210 children and adolescents (age range: 10–17 years) with schizophrenia were included in the SS. Among these pediatric patients, 21 (10.0%) experienced AEs and 17 (8.1%) experienced ADRs, most of which were mild in severity. No significant differences were found between the pediatric group and other age groups (P for <18 vs 18–45, 45–65, and >65 years group were 0.706, 0.248, and 0.066, respectively). The most frequently reported ADRs were EPS-related ADRs, abnormal liver function and weight gain (each 1.4%) in patients aged <18 years; EPS-related ADRs (3.8%) and weight gain and abnormal liver function (both 1.0%) in those aged 18–45 years; EPS-related ADRs (2.4%), elevated blood prolactin (1.0%), and weight gain (0.7%) in patients aged 45–65 years; and EPS-related ADRs and QT‑interval prolongation (both 1.2%) in patients aged >65 years.
Over the 12-week period, the overall mean weight change remains minimal, and only a small proportion of participants experienced a significant weight gain (≥7%). Given the favorable metabolic profile of lurasidone, we further estimated metabolic-related AEs in patients with and without concomitant use of medications known to substantially affect metabolic parameters (including glucose, cholesterol, triglycerides, body weight, BMI). Patients in the SS were stratified based on whether they concomitantly used olanzapine, clozapine, quetiapine, amitriptyline, mirtazapine, lithium and valproate.22 Approximately one third of patients (1082/3178, 34.0%) used metabolic affecting medications during surveillance. Among them, 4.3% (47/1082) experienced metabolic AEs, which was significantly higher than the incidence in patients without metabolic affecting agents (46/2096, 2.2%; P < 0.001).
Effectiveness Outcomes
Significant reductions were observed in the BPRS total score, as well as anxiety-depression, anergia, thought disturbance, activation, and hostility-suspiciousness subscores at weeks 2/4, 6/8, and 12 after treatment initiation compared with those before treatment (P<0.05) (Table 3).
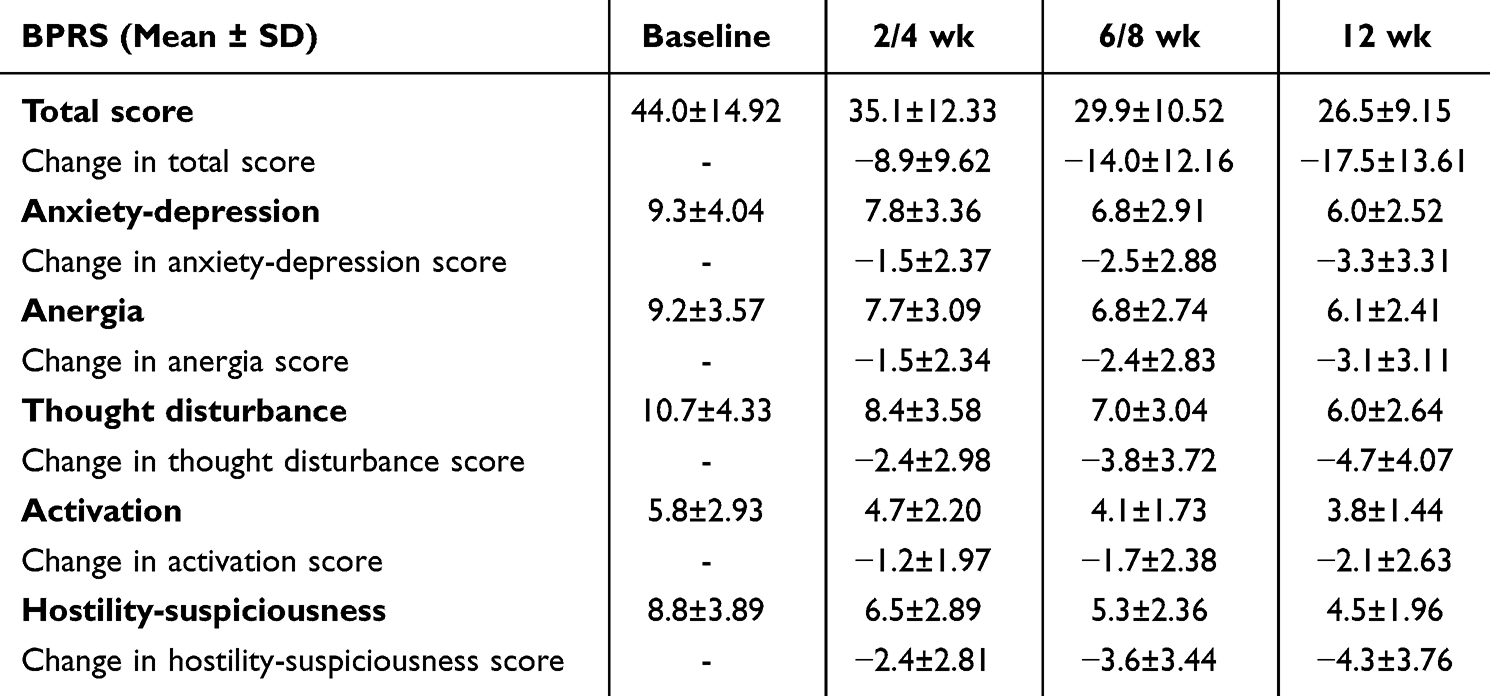 |
Table 3 Changes from Baseline to Week 12 in BPRS Scores |
Significant improvements were also observed in all age groups. BPRS total scores at baseline and week 12 for the <18, 18–45, 45–65, and >65-year groups were 46.1±15.10 to 26.3±9.72, 44.1±14.78 to 26.1±8.95, 43.0±14.24 to 27.3±9.41, and 42.1±15.10 to 27.2±9.44, respectively (all P < 0.001). Specifically, in pediatric patients, significant improvements were also seen in the total BPRS scores at each visit compared to baseline (all P < 0.001), with mean changes of −9.4 ± 9.16, −15.4 ± 12.04, and −20.3 ± 13.45 at weeks 2/4, 6/8, and 12, respectively.
Discussion
This study presents, for the first time, comprehensive real-world data from the largest cohort of patients with schizophrenia in China treated with lurasidone. It characterizes major ADRs and their time to onset, the ADR profile across different age groups, and potential interactions when lurasidone is combined with agents affecting metabolic function. While the interim analysis established the effectiveness and overall tolerability of lurasidone, the current complete analysis extends these observations through a larger cohort and age‑stratified assessments of safety and effectiveness. Moreover, the findings further support transparent communication and shared decision-making, thereby strengthening therapeutic alliances and facilitating optimized treatment strategies that enhance patient outcomes.
In this study, the daily dose of lurasidone was consistent with the dose range approved in China. Pharmacokinetic data indicate that the steady‑state plasma concentration of lurasidone in Chinese individuals is approximately 30–40% higher than that observed in Western populations,15 which supports the lower approved dose range in China (40–80 mg/d) and the lower mean daily dose used in this real-world study (59.9 ± 20.9 mg/day), compared with the higher approved dose ranges in Europe (37–148 mg/d) and the United States (40–160 mg/d).23,24 By age, the mean lurasidone dose in patients aged <18 years seemed relatively higher than that reported for the general population, which may reflect greater symptom severity in pediatric patients.25 In contrast, lower doses were commonly used in older adults, potentially due to age‑related functional decline in the dopaminergic system and increased susceptibility to adverse effects.26 In addition, elderly patients frequently receive concomitant medications for comorbid conditions; for example, commonly used calcium‑channel blockers such as verapamil and diltiazem are moderate CYP3A4 inhibitors and may increase lurasidone exposure,19 further supporting cautious dosing in this population.
Lurasidone demonstrated a favorable safety profile in this PMS, with no novel side effects identified. The most common AEs were consistent with previous evidence, although the incidence was relatively low.14,27,28 In a 6-week double-blind, placebo-controlled trials conducted in Asian patients from Japan, South Korea, Malaysia, and Taiwan, the most frequent treatment-emergent AEs in the lurasidone 40 mg/d, 80 mg/d and placebo groups were akathisia (7.3%, 10.4%, 3.3%), nausea (7.3%, 7.8%, 4.6%), insomnia (6.7%, 7.1%, 4.0%), nasopharyngitis (6.0%, 7.1%, 4.6%), and tremor (3.3%, 5.2%, 2.6%).28 Similarly, a randomized, double-blind, 6-week Phase III trial in Chinese patients reported the most frequent AEs in the lurasidone group were extrapyramidal disorder (17.0%), constipation (12.9%), nasopharyngitis (9.8%), insomnia (9.8%), akathisia (7.2%), anxiety (6.2%), and upper respiratory infection (5.2%).14 These lower AEs incidence observed in this study may be attributed to: 1) its open-label, non-interventional design; 2) flexible dosing regimen and administration times of lurasidone determined by the investigators based on clinical judgment; and 3) the larger sample size.
In this study, nausea and vomiting typically appeared early after receiving lurasidone. A pooled analysis of six Phase II/III, 6‑week randomized placebo‑controlled trials showed that the incidence of nausea was lowest in the 160 mg lurasidone group compared with the 120 mg and 80 mg groups, suggesting a dose‑related reduction.29 Both 5‑HT1A agonism and dopaminergic antagonism are known to mitigate nausea.30 Lurasidone has high affinity for dopamine D2 receptors and partial agonist activity at 5‑HT1A receptors.11 One hypothesis is that at lower serum lurasidone concentrations, partial agonism at 5‑HT1A receptors may provide insufficient activation of this pathway, resulting in nausea that is not adequately counterbalanced by dopamine antagonism. At higher serum concentrations, however, dose‑dependent dopamine D2-receptor antagonism becomes more prominent and may mitigate nausea associated with reduced 5‑HT1A activity. This mechanism may help explain the lower incidence of nausea observed with the 160 mg lurasidone dose.31 Since the 160 mg dose of lurasidone is not approved in China, administration with food, which increases lurasidone exposure, may be a practical strategy to alleviate nausea, as recommended in the prescribing information.19 Nervous system disorders, predominantly EPS, generally emerged by the third to fourth week of therapy in this PMS. These findings are consistent with reports for other oral second‑generation antipsychotics in analyses of the Japanese Adverse Drug Event Report database.32
The incidence of ADRs varied by age group in the PMS. Pharmacokinetic and pharmacodynamic responses to antipsychotics differ in pediatric and geriatric patients compared with mid-life adults, who may be more vulnerable to side effects.25,33 Although the <18 years group showed a trend toward higher ADR incidence, the difference did not reach statistical significance, potentially due to the relatively lower prevalence of polypharmacy in this population. In contrast, patients >65 years exhibited a relatively lower incidence of ADRs, which may be attributable to reduced lurasidone exposure. Although EPS were the most frequently reported ADRs overall, distinct age‑related patterns in other ADRs were observed in this study. Metabolic‑related ADRs occurred more frequently in younger patients, particularly those younger than 18 years, whereas QT‑interval prolongation was more commonly reported in patients older than 65 years, highlighting the relevance of age‑specific safety considerations. While advanced approaches such as therapeutic drug monitoring or pharmacogenetic testing may be informative in selected clinical contexts,34 our real‑world findings underscore the importance of pragmatic, age‑tailored safety surveillance in routine practice. Beyond vigilance for EPS across all age groups, longitudinal monitoring of body weight and metabolic parameters may be particularly pertinent in pediatric patients, whereas closer cardiovascular monitoring may be more relevant in geriatric populations.
A favorable metabolic profile was also confirmed in the PMS. AEs related to metabolic function was infrequent, even when lurasidone was combined with drugs known to significantly affect metabolic function. Several widely used psychotropic agents, including olanzapine, clozapine, quetiapine, amitriptyline, mirtazapine, lithium and valproate, are well recognized for their impact on metabolic parameters.35 Given that antipsychotic polypharmacy remains common in clinical practice and is often used prior to or instead of clozapine,36 lurasidone may represent a reasonable option for patients with metabolic risk factors, either as monotherapy or in combination with other agents.
In this study, lurasidone demonstrated effectiveness in both pediatric and adult patients, with symptomatic improvements observed as early as two weeks after treatment initiation. These findings are consistent with previous evidence observed in adolescents and adults with schizophrenia in other countries.13
This study has several limitations. First, its open‑label, non‑interventional, single‑arm design may introduce potential confounding and bias, and causal inferences could not be established. Second, the absence of a control group precludes direct comparison of safety outcomes with agents known to significantly affect metabolism. Third, the observation period was relatively short, meaning ADRs requiring longer exposure, such as weight gain, may have been underestimated. Future studies should prioritize long‑term evaluations and comparisons with other antipsychotics to further clarify lurasidone’s role in the management of schizophrenia.
Conclusion
This PMS study confirms that lurasidone is safe and effective for treating schizophrenia in Chinese patients in real-world clinical settings, across both adult and adolescent populations. Despite the relatively short follow‑up and lack of a comparator arm, it provides a detailed safety profile that facilitates treatment regimen optimization and strengthens therapeutic alliance, which in turn, improves compliance and prognosis of patients with schizophrenia. These findings provide valuable evidence for the clinical use of lurasidone in China and highlight its value as a treatment option with favorable safety and efficacy profile that can be tailored to diverse patient populations in China. The results also suggest the potential value of a pragmatic, age‑tailored monitoring approach in routine practice, with particular attention to possible drug–drug interactions, especially in geriatric patients with polypharmacy.
Data Sharing Statement
The data are not publicly available as we do not have permission from the data custodians or ethics approval to do so.
Informed Consent Statement
All patients provided informed consent.
Acknowledgment
The authors sincerely thank all the patients and their families, as well as the physicians and paramedical staff, for their participation in this study. Grateful acknowledgement is also given to the following research sites for their indispensable support in patient enrollment:
• The First Psychiatric Hospital of Harbin
• Daqing Third Hospital
• Hebei Mental Health Center
• Quzhou Third Hospital
• Fujian Energy General Hospital
• Fuzhou Shenkang Hospital
• The Fifth People’s Hospital of Zigong
• Hengyang Mental Health Center
• Jinzhou Kangning Hospital
• Liaoning Mental Health Center
• Xi’an Mental Health Center
• Xiangtan Mental Health Center
• Beijing Anding Hospital
• Dalian Seventh People’s Hospital
• Jilin Sixth People’s Hospital
• Changshu Mental Health Center
• Guangyuan Mental Health Center
• Tianshui Third People’s Hospital
• Yueqing Third People’s Hospital
• Suzhou Guangji Hospital
• Mianyang Third People’s Hospital
• Chengdu Fourth People’s Hospital
• Shanghai Xuhui District Mental Health Center
• Jiangxi Mental Health Center
• Zhejiang Xiaoshan Hospital
• Kailuan Mental Health Center
This study would not have been possible without their dedicated efforts.
Funding
Supported by Collaborative Innovation Center Project of Translational Medicine, Shanghai Jiaotong University School of Medicine, No. TM202116PT (2021–2023); Clinical Research Plan of SHDC, No. SHDC2022CRS032; and the Sumitomo Pharma (Suzhou) Co., Ltd.
Disclosure
The authors declare no Potential conflicts of interest in this work.
References
1. Schizophrenia. 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/schizophrenia.
2. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–10. doi:10.1016/S2215-0366(18)30511-X
3. Global health estimates: leading causes of DALYs. Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/global-health-estimates-leading-causes-of-dalys.
4. Zhao J, Shi S. Guidelines for schizophrenia prevention and treatment in china. 2015.
5. Velligan DI, Weiden PJ, Sajatovic M, et al. The expert consensus guideline series: adherence problems in patients with serious and persistent mental illness. J Clin Psychiatry. 2009;70(Suppl 4):1–46.
6. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209–1223. doi:10.1056/NEJMoa051688
7. Lieslehto J, Tiihonen J, Lähteenvuo M, et al. Primary nonadherence to antipsychotic treatment among persons with schizophrenia. Schizophr Bull. 2022;48(3):655–663. doi:10.1093/schbul/sbac014
8. Hamann J, Leucht S, Kissling W. Shared decision making in psychiatry. Acta Psychiatr Scand. 2003;107(6):403–409. doi:10.1034/j.1600-0447.2003.00130.x
9. McCutcheon RA, Pillinger T, Varvari I, et al. INTEGRATE: international guidelines for the algorithmic treatment of schizophrenia. Lancet Psychiatry. 2025;12(5):384–394. doi:10.1016/S2215-0366(25)00031-8
10. Keepers GA, Fochtmann LJ, Anzia JM, et al. The American psychiatric association practice guideline for the treatment of patients with schizophrenia. Am J Psychiatry. 2020;177(9):868–872. doi:10.1176/appi.ajp.2020.177901
11. Jaeschke RR, Sowa-Kućma M, Pańczyszyn-Trzewik P, et al. Lurasidone: the 2016 update on the pharmacology, efficacy and safety profile. Pharmacol Rep. 2016;68(4):748–755. doi:10.1016/j.pharep.2016.04.002
12. Pompili M, Verzura C, Trovini G, et al. Lurasidone: efficacy and safety in the treatment of psychotic and mood disorders. Expert Opin Drug Saf. 2018;17(2):197–205. doi:10.1080/14740338.2017.137998
13. Fiorillo A, Cuomo A, Sampogna G, et al. Lurasidone in adolescents and adults with schizophrenia: from clinical trials to real-world clinical practice. Expert Opin Pharmacother. 2022;23(16):1801–1818. doi:10.1080/14656566.2022.2141568
14. Feng Y, Shi J, Wang L, et al. Randomized, double-blind, 6-week non-inferiority study of lurasidone and risperidone for the treatment of schizophrenia. Psychiatry Clin Neurosci. 2020;74(6):336–343. doi:10.1111/pcn.12965
15. Huang CY, Lin SK. Therapeutic drug monitoring of lurasidone in patients with schizophrenia or bipolar disorder: a preliminary study. Psychiatry Clin Neurosci. 2022;76(12):674–675. doi:10.1111/pcn.13466
16. Wei YM, Wang XJ, Yang XD, et al. Safety and effectiveness of lurasidone in the treatment of Chinese schizophrenia patients: an interim analysis of post-marketing surveillance. World J Psychiatry. 2023;13(11):937–948. doi:10.5498/wjp.v13.i11.937
17. Rothwell PM. External validity of randomised controlled trials: “to whom do the results of this trial apply?”. Lancet. 2005;365(9453):82–93. doi:10.1016/S0140-6736(04)17670-8
18. Khaowroongrueng V, Kim TE, Park SI, et al. Application of real-world evidence to support FDA regulatory decision making. AAPS J. 2025;27(4):98. doi:10.1208/s12248-025-01082-1
19. Sumitomo Pharma America, Inc. Label for Lurasidone hydrochloride (Latuda). In: Sumitomo Pharma (Suzhou). Available from: https://www.sumitomo-pharma.com.cn/upload/product/1706217815043220823.pdf.
20. Overall J, Gorham D. The brief psychiatric rating scale. Psychol Reports. 1962;10:799–812. doi:10.2466/pr0.1962.10.3.799
21. Czobor P, Volavka J. Dimensions of the brief psychiatric rating scale: an examination of stability during haloperidol treatment. Compr Psychiatry. 1996;37:205–215. doi:10.1016/s0010-440x(96)90037-1
22. Correll CU, Detraux J, De Lepeleire J, De Hert M. Effects of antipsychotics, antidepressants and mood stabilizers on risk for physical diseases in people with schizophrenia, depression and bipolar disorder. World Psychiatry. 2015;14(2):119–136. doi:10.1002/wps.20204
23. Aziende CR. unite Angelini Francesco – a.C.R.A.F. S.p.A. Label for Lurasidone hydrochloride (Latuda). In: EMA. Available from: https://www.ema.europa.eu/en/documents/product-information/latuda-epar-product-information_en.pdf.
24. Sumitomo Pharma America, Inc. Label for Lurasidone hydrochloride (Latuda). In: FDA. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/200603s041lbl.pdf.
25. Abidi S, Mian I, Garcia-Ortega I, et al. Canadian guidelines for the pharmacological treatment of schizophrenia spectrum and other psychotic disorders in children and youth. Can J Psychiatry. 2017;62(9):635–647. doi:10.1177/0706743717720197
26. Uchida H, Mamo DC, Mulsant BH, et al. Increased antipsychotic sensitivity in elderly patients: evidence and mechanisms. J Clin Psychiatry. 2009;70(3):397–405. doi:10.4088/JCP.08r04171
27. Caccia S, Pasina L, Nobili A. Critical appraisal of lurasidone in the management of schizophrenia. Neuropsychiatr Dis Treat. 2012(8):155–168. doi:10.2147/NDT.S18059
28. Higuchi T, Ishigooka J, Iyo M. Lurasidone in the treatment of schizophrenia: results of a double-blind, placebo-controlled trial in Asian patients. Asia Pac Psychiatry. 2019;11(2):e12352. doi:10.1111/appy.12352
29. Citrome L. Lurasidone for the acute treatment of adults with schizophrenia: what is the number needed to treat, number needed to harm, and likelihood to be helped or harmed? Clin Schizophr Relat Psychoses. 2012;6(2):76–85. doi:10.3371/CSRP.6.2.5
30. Kenward H, Pelligand L, Savary-Bataille K, et al. Nausea: current knowledge of mechanisms, measurement and clinical impact. Vet J. 2015;203(1):36–43. doi:10.1016/j.tvjl.2014.10.007
31. Kolli V, Walia A, Kinnan S. Food matters: reduction of lurasidone-induced nausea with meals. Prim Care Companion CNS Disord. 2019;21(2):18l02343. doi:10.4088/PCC.18l02343
32. Ebina T, Iwamoto K, Ando M, et al. Second-generation antipsychotic-induced dystonia: analysis using the Japanese Adverse Drug Event Report (JADER) database. Psychiatry Clin Neurosci. 2025;79(3):117–124. doi:10.1111/pcn.13785
33. Gebauer EM, Lukas A. Prescriptions of antipsychotics in younger and older geriatric patients with polypharmacy, their safety, and the impact of a pharmaceutical-medical dialogue on antipsychotic use. Biomedicines. 2022;10(12):3127. doi:10.3390/biomedicines10123127
34. Hart XM, Gründer G, Ansermot N, et al. Optimisation of pharmacotherapy in psychiatry through therapeutic drug monitoring, molecular brain imaging and pharmacogenetic tests: focus on antipsychotics. World J Biol Psychiatry. 2024;25(9):451–536. doi:10.1080/15622975.2024.2366235
35. Sepúlveda-Lizcano L, Arenas-Villamizar VV, Jaimes-Duarte EB, et al. Metabolic adverse effects of psychotropic drug therapy: a systematic review. Eur J Investig Health Psychol Educ. 2023;13(8):1505–1520. doi:10.3390/ejihpe13080110
36. Højlund M, Köhler-Forsberg O, Gregersen AT, et al. Prevalence, correlates, tolerability-related outcomes, and efficacy-related outcomes of antipsychotic polypharmacy: a systematic review and meta-analysis. Lancet Psychiatry. 2024;11(12):975–989. doi:10.1016/S2215-0366(24)00314-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of Lurasidone 80 mg in Patients with Schizophrenia: Results of an Open-Label, 12-Week Extension Study
Miura I, Watabe K, Sakaguchi R, Okamoto K, Maruyama H
Neuropsychiatric Disease and Treatment 2022, 18:2627-2637
Published Date: 9 November 2022
Effectiveness and Safety of Radiofrequency Thermocoagulation Treatment Guided by Computed Tomography for Infraorbital Neuralgia Following Failed Conservative Treatment: A Retrospective Study
Sun Z, Liu L, Liu H, Luo F
Journal of Pain Research 2023, 16:1005-1015
Published Date: 21 March 2023
Effectiveness and Safety of a Fixed-Dose Combination of Valsartan and Rosuvastatin (Rovatitan® Tablet) in Patients with Concomitant Hypertension and Hyperlipidemia: An Observational Study
Lee KJ, Ryu JK, Cho YH, Shin WY, Kim JS, Yoon YW, Jang JY, Kim WH, Beom JW, Kang SM
Drug Design, Development and Therapy 2023, 17:1047-1062
Published Date: 6 April 2023
Real-World Safety and Effectiveness of Omalizumab in Moderate to Severe Allergic Asthma Patients in China: A Post-Authorization Study
Su N, Zhi L, Liu F, Wang Y, Zhang Q, Liu X, Wang X, Hao G, Zhang X, Hu Q, Ligueros-Saylan M, Uddin A, Yang J, Liang T, Ding L, Li R, Wang C
Journal of Asthma and Allergy 2023, 16:625-636
Published Date: 19 June 2023
Clinical Utility of Long-Acting Injectable Risperidone in Schizophrenia and Bipolar I Disorder: A Review of Clinical Studies
Bartoli F, Cavaleri D, Riboldi I, Capogrosso CA, Carrà G
Psychology Research and Behavior Management 2025, 18:1455-1469
Published Date: 17 June 2025