Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Longitudinal Spirometric Trajectory from Normal Lung Function to PRISm and COPD in a Population-Based Korean Cohort
Authors Kang SY ![]() , Roh S
, Roh S ![]() , Yeo IH, Ko YK, Oh JY
, Yeo IH, Ko YK, Oh JY ![]() , Gim JA
, Gim JA ![]()
Received 13 January 2026
Accepted for publication 7 May 2026
Published 16 May 2026 Volume 2026:21 595625
DOI https://doi.org/10.2147/COPD.S595625
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Sun Young Kang,1,* Sanghyun Roh,2,* In Hwan Yeo,2 Young Kyung Ko,3 Jee Youn Oh,3 Jeong-An Gim1,2
1Institute for Molecular Metabolism Innovation, Soonchunhyang University, Asan, Republic of Korea; 2Department of Medical Science, Soonchunhyang University, Asan, Republic of Korea; 3Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Korea University Guro Hospital, Seoul, Republic of Korea
*These authors contributed equally to this work
Correspondence: Jee Youn Oh, Email [email protected] Jeong-An Gim, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) develops through heterogeneous lung-function trajectories, but the longitudinal role of preserved ratio impaired spirometry (PRISm) in progression toward COPD remains unclear.
Objective: We aimed to characterize long-term spirometric trajectories and transitions from normal spirometry to PRISm or COPD in a population-based cohort.
Patients and Methods: We analyzed data from the Ansan–Ansung cohort of the Korean Genome and Epidemiology Study. Among medication-free participants with normal baseline spirometry who had classifiable spirometry across seven examinations over approximately 12 years, longitudinal trajectories of forced expiratory volume in 1 second (FEV1, % predicted) and the FEV1/FVC ratio were evaluated. Participants were classified into normal maintenance, PRISm, or COPD trajectory groups using a clinically interpretable, rule-based approach. Because post-bronchodilator measurements were not available across all examinations, COPD was operationally defined using pre-bronchodilator spirometry as FEV1/FVC < 0.70.
Results: Lung-function decline followed heterogeneous trajectories rather than a single linear pathway. Among 1,753 participants, 1,658 (94.6%) remained normal, 21 (1.2%) developed PRISm, and 74 (4.2%) progressed to COPD. Most individuals who developed COPD did so without a preceding sustained PRISm phase. In descriptive baseline comparisons, the COPD trajectory showed greater smoking exposure, higher blood pressure, and more pronounced central adiposity, whereas PRISm was more closely associated with wheeze-related respiratory symptoms and lower baseline lung function. In multivariable logistic regression, older age and current smoking were the strongest independent predictors of progression to COPD.
Conclusion: Progression toward COPD in the general population is heterogeneous, and PRISm is not an obligatory precursor to COPD. Longitudinal spirometric assessment may provide clinically relevant insights beyond single time-point classification in the general population.
Plain Language Summary: Why was the study done?
COPD does not develop in the same way in everyone. Preserved ratio impaired spirometry (PRISm) has been proposed as an early stage of COPD, but its long-term role remains uncertain. This study examined how lung function changes over time and whether PRISm always leads to COPD.
What did the researchers do?
We studied Korean adults from the general population who had normal lung function at baseline. Lung function was measured seven times over about 12 years using spirometry. We tracked each person’s lung-function pattern over time and grouped participants according to their long-term trajectories.
What did the researchers find?
Lung-function change was heterogeneous. Most participants remained normal, some developed PRISm, and a smaller group developed COPD. Many individuals who developed COPD did so without a sustained PRISm phase. The COPD trajectory was more strongly associated with older age and smoking, and descriptively showed less favorable baseline clinical profiles, whereas PRISm was more closely associated with wheeze-related symptoms and lower baseline lung function.
What do these results mean?
PRISm is not always a necessary step before COPD. Repeated spirometry over time may provide more useful information than a single test for identifying people at risk of COPD and for understanding different pathways of disease development.
Keywords: COPD, PRISm, KoGES, longitudinal study, spirometry
Introduction
Chronic obstructive pulmonary disease (COPD) is a major global health burden, affecting more than 300 million individuals worldwide and remaining a leading cause of morbidity and mortality.1 The disease is characterized by persistent airflow limitation and progressive structural changes in the airways and lung parenchyma. Importantly, lung-function impairment often begins years before a clinical diagnosis is established, highlighting the need to identify early lung-function patterns associated with subsequent disease development and progression.1–3 In line with this concept, the recent Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2023 report redefined COPD as a heterogeneous disease encompassing symptoms, structural abnormalities, and underlying risk factors, emphasizing the importance of early identification and risk stratification.2
Spirometry remains the cornerstone of COPD diagnosis and monitoring, with forced expiratory volume in one second (FEV1) and the FEV1/forced vital capacity (FVC) ratio serving as key indicators of airflow obstruction.3,4 Beyond the conventional spirometric definition of COPD based on a reduced FEV1/FVC ratio, increasing attention has been directed toward individuals with preserved FEV1/FVC but reduced FEV1 (<80% predicted), a spirometric pattern known as preserved ratio impaired spirometry (PRISm).5 PRISm has been consistently associated with respiratory symptoms, cardiometabolic comorbidities, and increased mortality, indicating that it represents a clinically meaningful lung-function phenotype rather than a benign spirometric variant.4–6 Recent large-scale analyses further reported that PRISm is associated with mortality risks comparable to those observed in COPD and exhibits a substantial population-level prevalence.7
Longitudinal evidence has highlighted the heterogeneity of PRISm. Analyses from the COPDGene study demonstrated that individuals with PRISm frequently transition to normal spirometry or overt airflow obstruction and experience mortality risks similar to those of moderate COPD.8 These findings established PRISm as an important phenotype that must be considered in studies of COPD development and lung-function trajectories. Given the inherently longitudinal nature of COPD, several studies have proposed PRISm as a potential transitional or “pre-COPD” state, suggesting a stepwise progression from normal lung function to PRISm and subsequently to COPD.8 Supporting this hypothesis, a population-based Korean study reported that individuals with PRISm exhibited a significantly increased risk of developing COPD compared with those with normal spirometry.9
However, accumulating evidence suggests that PRISm does not represent a uniform or obligatory precursor to COPD.10 Although previous studies have demonstrated diverse transitions involving PRISm, the longitudinal pathways linking normal lung function, PRISm, and COPD remain incompletely understood. In particular, it remains unclear whether PRISm represents a transitional stage toward COPD or an independent trajectory with distinct clinical characteristics. In a general population cohort from Denmark, PRISm was associated with increased risks of cardiovascular and respiratory hospitalization and mortality, while exhibiting diverse longitudinal trajectories, including transition from normal spirometry to PRISm, persistent PRISm, and reversion to normal spirometry.11 Similarly, a Japanese community-based cohort study demonstrated that PRISm was associated with increased risks of all-cause mortality, cardiovascular mortality, and incident airflow limitation compared with normal spirometry.12 Together with recent reviews, these findings highlight substantial heterogeneity within PRISm, encompassing distinct comorbidity profiles and variable longitudinal outcomes, including stable PRISm, reversion to normal spirometry, and direct progression from normal lung function to COPD without a sustained PRISm phase.10–13
This concept of heterogeneous disease pathways is further supported by landmark longitudinal studies demonstrating that COPD can arise through distinct lung-function trajectories, determined not only by the rate of FEV1 decline but also by the level of lung function attained earlier in life.14 These observations underscore the importance of trajectory-based approaches and baseline phenotypic characterization in advancing the understanding of COPD development beyond cross-sectional spirometric classification.
Despite growing interest in lung-function trajectories, long-term population-based evidence examining spirometric trajectories and PRISm-related transitions remains limited, particularly in Asian populations.9 The Korean Genome and Epidemiology Study (KoGES), with repeated standardized spirometry over approximately 12 years, provides a unique opportunity to investigate these longitudinal patterns in a large population-based cohort. Therefore, using repeated spirometric data across seven examinations, this study aimed to characterize long-term lung-function trajectories and transitions from normal spirometry to PRISm or COPD, and to examine baseline demographic, lifestyle, and clinical factors associated with progression to COPD.
Materials and Methods
Study Population
This study used data from the Ansan–Ansung cohort of the Korean Genome and Epidemiology Study (KoGES), a population-based prospective cohort that enrolled 10,030 adults aged 40–69 years between 2001 and 2002. Participants underwent standardized health examinations, including spirometry, at baseline and at subsequent follow-up visits conducted at approximately 2-year intervals over a total follow-up period of approximately 12 years.
Among the total cohort, 9,783 participants had classifiable baseline spirometry. For longitudinal trajectory analyses, we first identified participants with classifiable spirometry across all seven examinations (baseline plus six follow-up visits). We then restricted the main analytic cohort to participants with normal baseline spirometry who followed prespecified monotone target trajectories and had no baseline history of ≥3-month medication use. To address potential misclassification due to reversible airway disease, we additionally performed sensitivity analyses excluding participants with asthma-related baseline indicators, including physician-diagnosed asthma, current asthma treatment, current use of asthma medication or inhalers, and recent asthma medication use. Invalid or extreme spirometric values were excluded according to predefined data-cleaning rules before trajectory construction. After applying these criteria, 1,753 participants were included in the final analytic cohort (Figure 1).
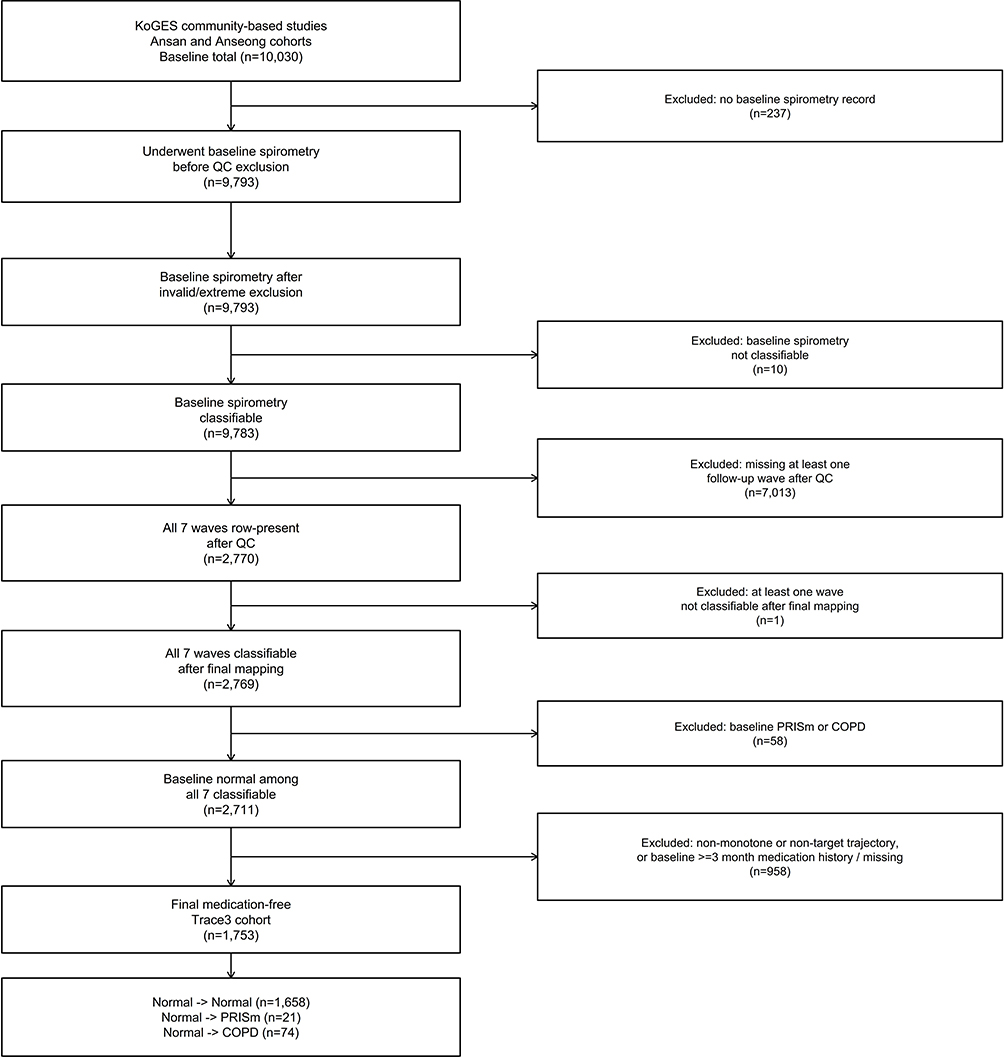 |
Figure 1 Study flow. Flow diagram of participant selection for the longitudinal spirometry analysis across seven examinations in the KoGES cohort. |
This study was conducted using bioresources from the National Biobank of Korea, Korea Disease Control and Prevention Agency (KBN-2024-045). All participants provided written informed consent. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Soonchunhyang University (IRB No. 2024–05-049).
Spirometry Assessment and Classification
Spirometry was performed by trained technicians using standardized equipment (Vmax®, SensorMedics, Yorba Linda, CA, USA) in accordance with the American Thoracic Society and European Respiratory Society (ATS/ERS) guidelines.4,5 All measurements followed standardized KoGES protocols, including routine calibration and quality control procedures consistent with ATS/ERS recommendations.
Because post-bronchodilator measurements were not available across all examinations, COPD was operationally defined using pre-bronchodilator spirometry as FEV1/FVC < 0.70. Accordingly, COPD in this study refers to a spirometrically defined category based on pre-bronchodilator measurements. Forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) were measured at each examination, and percent predicted values were calculated using Korean reference equations. At each examination, participants were classified into one of three spirometric categories based on contemporaneous measurements:
- Normal: FEV1 ≥ 80% predicted and FEV1/FVC ≥ 0.70
- PRISm: FEV1 < 80% predicted and FEV1/FVC ≥ 0.70
- COPD: FEV1/FVC < 0.70
This classification scheme was applied consistently across all seven examinations and served as the basis for constructing individual longitudinal lung-function trajectories.
Longitudinal Spirometric Trajectories
Longitudinal spirometric trajectories were evaluated by tracking changes in spirometric categories across the seven examination time points. Individual-level trajectories of FEV1 (% predicted) and FEV1/FVC were visualized using line plots to illustrate within-person longitudinal changes. In addition, population-level distributions of spirometric measurements at each examination were assessed to examine temporal shifts in lung-function patterns over follow-up. The primary objective was to determine whether lung-function decline followed a single linear pathway (eg., normal → PRISm → COPD) or whether multiple heterogeneous trajectories existed.
Definition of Spirometric Trajectory Groups
Spirometric trajectory groups were defined based on spirometric status observed across all seven examinations. To ensure a uniform starting point for trajectory analyses, only participants classified as having normal spirometry at baseline were included.
Participants were categorized into three clinically relevant trajectory groups:
- Normal maintainers (Normal to Normal; NN): remained normal at all examinations
- PRISm trajectory group (Normal to PRISm; NP): participants whose baseline spirometry was normal, whose final examination was classified as PRISm, whose first PRISm classification occurred after baseline, and whose spirometric status remained PRISm from the first PRISm classification through the final examination without meeting COPD criteria.
- COPD trajectory group (Normal to COPD; NC): participants whose baseline spirometry was normal, whose final examination was classified as COPD, whose first COPD classification occurred after baseline, and whose spirometric status remained COPD from the first COPD classification through the final examination; PRISm before the first COPD classification was allowed.
Participants with non-monotone patterns, including reversion from PRISm or COPD to normal spirometry or oscillating classifications across examinations, were not assigned to NN, NP, or NC and were excluded from the final target-trajectory cohort. A clinically interpretable, rule-based approach was adopted rather than model-based methods (eg., latent class trajectory modeling) to preserve transparency and clinical relevance. However, this approach may not fully capture the complexity of longitudinal trajectories and may be more limited than model-based methods.
Age-stratified analyses were additionally performed using <60 versus ≥60 years to evaluate potential age-related differences in trajectory patterns.
Statistical Analysis
To evaluate potential selection bias, baseline characteristics were compared between participants included in the final analysis and those excluded from the final analytic cohort based on the prespecified analytic pipeline. Baseline demographic, clinical, and lifestyle variables were compared across trajectory groups. Continuous variables were expressed as mean ± standard deviation and compared using the Kruskal–Wallis test, while categorical variables were compared using Fisher’s exact test. For post hoc pairwise comparisons, p-values were adjusted using the Benjamini–Hochberg false discovery rate (FDR). Statistical significance was defined as a two-sided p-value < 0.05. All analyses were conducted using R software (version 4.5.2).
In addition, multivariable logistic regression analyses were performed to evaluate associations between baseline demographic, smoking-related, and cardiometabolic factors and transition to the COPD trajectory. The primary regression model compared the COPD trajectory group (NC) with the normal-maintainer group (NN). Odds ratios for age are reported per 1-year increase, and odds ratios for triglyceride are reported per 10 mg/dL increase. Baseline spirometric variables were not included in the primary model because the aim was to evaluate non-spirometric demographic, lifestyle, and cardiometabolic correlates of trajectory progression, and because trajectory membership was itself defined using repeated spirometric measures. Because the number of events in the PRISm trajectory group was small, NP versus NN analyses were treated as exploratory.
Results
Subject Classification by Spirometry
A total of 1,753 participants were included in the final analytic cohort. Of these, 1,658 (94.6%) remained in the normal-maintainer group, 21 (1.2%) entered the PRISm trajectory, and 74 (4.2%) entered the COPD trajectory. Among the 74 participants in the COPD trajectory, 70 progressed directly to COPD without a preceding PRISm phase, whereas 4 exhibited PRISm prior to the first COPD classification (Table 1).
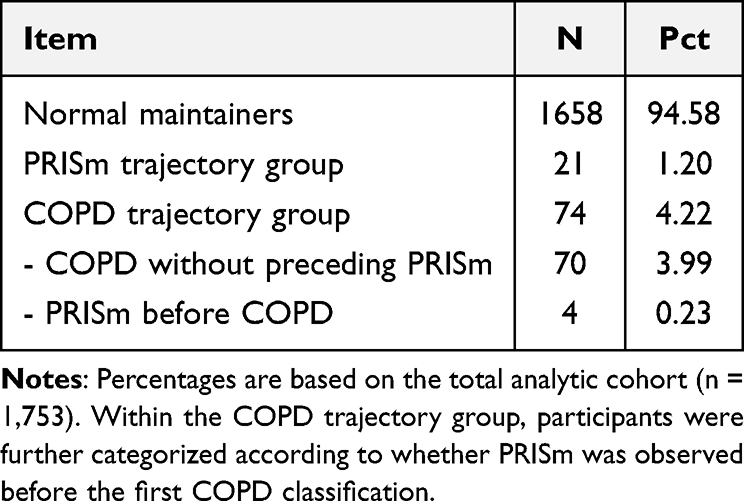 |
Table 1 Distribution of Spirometric Trajectory Groups |
Baseline characteristics of included and excluded participants are presented in Supplementary Table S1. Among 9,783 participants with classifiable baseline spirometry, 1,753 were included in the final analytic cohort and 8,030 were excluded. Compared with excluded participants, those included in the final analytic cohort were younger, had lower smoking exposure, and had better baseline lung function. In particular, baseline FEV1/FVC was 75.34 ± 1.54 in the included group and 74.41 ± 1.92 in the excluded group, suggesting a degree of selection toward a relatively healthier analytic subset.
The mean age at baseline was 48.04 ± 6.77 years and increased to 59.82 ± 6.79 years at the seventh examination. Body mass index remained relatively stable over time, whereas lung-function indices declined. Mean FEV1/FVC decreased from 75.34 ± 1.54 at baseline to 72.87 ± 1.68 at the final examination. At baseline, all participants were classified as having normal spirometry; at the seventh examination, 21 participants were classified as PRISm and 74 met the criteria for COPD (Table 2).
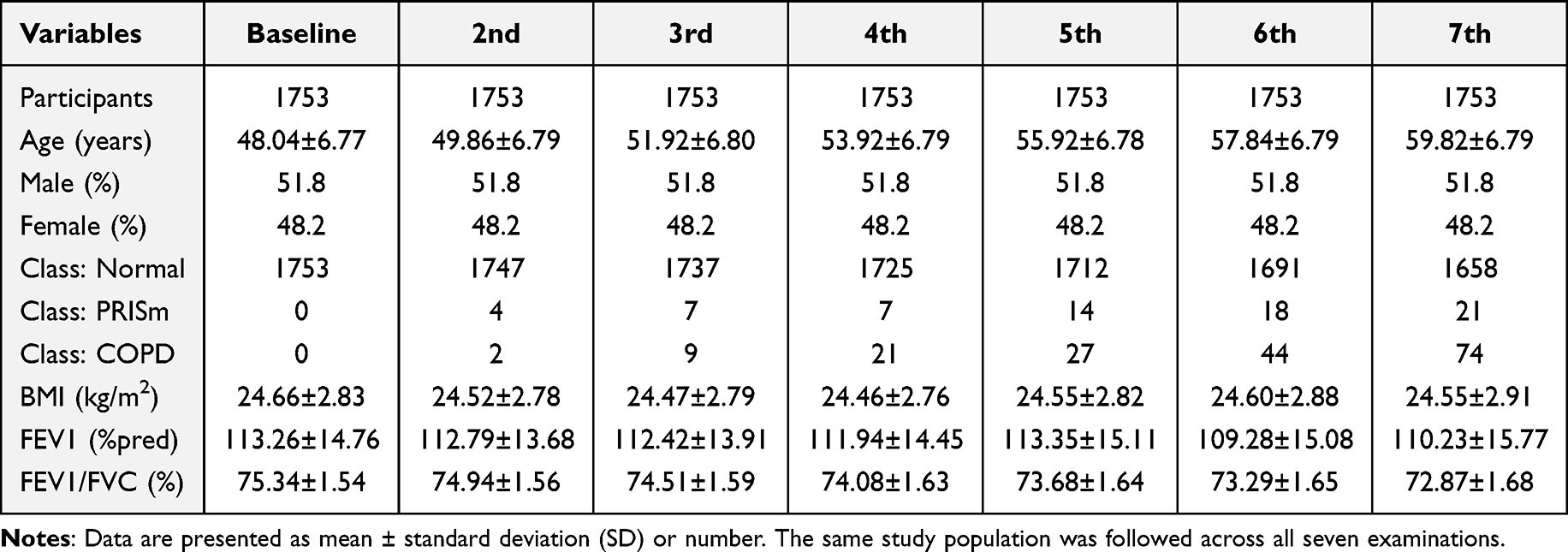 |
Table 2 Longitudinal Summary Across Seven Examinations |
Spirometry-Based Longitudinal Trace of Lung Function
All 1,753 participants in the final analytic cohort were included in the longitudinal trajectory analysis. Individual-level trajectories of FEV1 (% predicted) and FEV1/FVC are shown in Figure 2. Substantial inter-individual variability in longitudinal lung-function patterns was observed across spirometric trajectory groups.
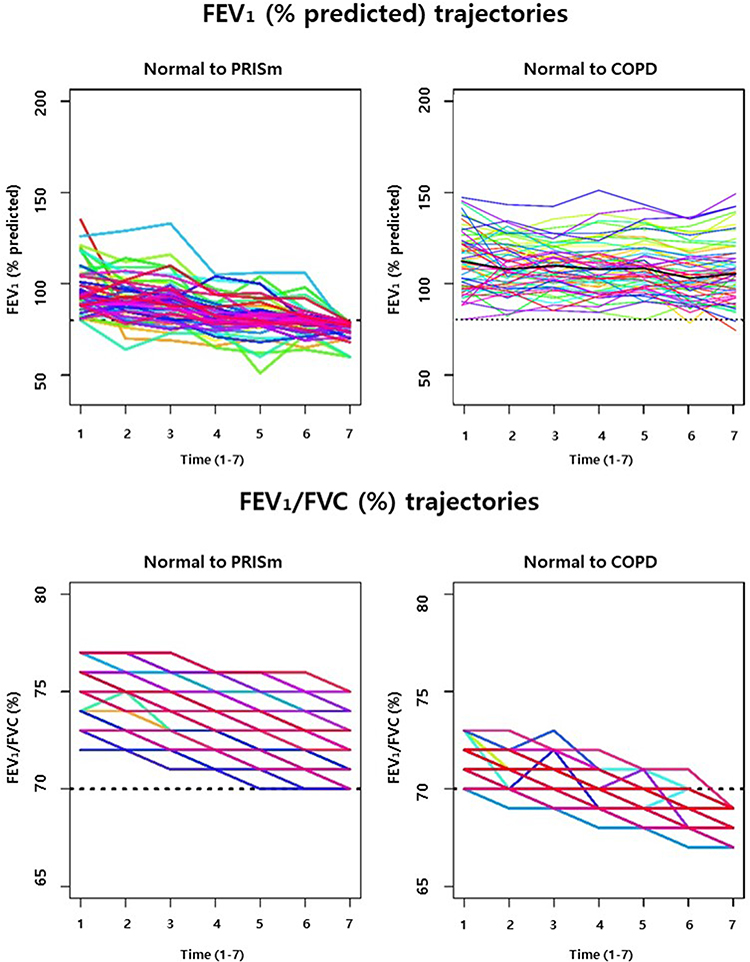 |
Figure 2 Individual-level longitudinal trajectories of lung function. Individual trajectories of FEV1 (% predicted) (top) and FEV1/FVC (%) (bottom) across seven spirometry examinations in participants assigned to the PRISm or COPD trajectory groups. Each colored line represents one participant. Dashed horizontal lines indicate the thresholds for PRISm (FEV1 = 80% predicted) and COPD (FEV1/FVC = 70%). |
Trajectories of FEV1 (% predicted) varied widely among individuals. Participants in the PRISm trajectory group (NP) generally exhibited gradual declines in FEV1%pred, although the magnitude and slope of decline differed across individuals. In the COPD trajectory group (NC), FEV1 decline patterns were heterogeneous, with some individuals showing early and rapid decline and others remaining relatively stable for several years before later deterioration. Several individuals met COPD criteria without preceding PRISm classification.
In contrast, FEV1/FVC trajectories showed a more consistent downward pattern among participants who developed COPD. In both the NC group and individuals transitioning from PRISm to COPD, FEV1/FVC values declined over time, with most individuals crossing the diagnostic threshold of 0.70 during follow-up.
Population-level distributions of spirometric measurements at each examination are shown in Figure 3. Over successive follow-up visits, the proportion of participants classified as COPD increased, whereas the proportion classified as PRISm remained relatively stable across examinations.
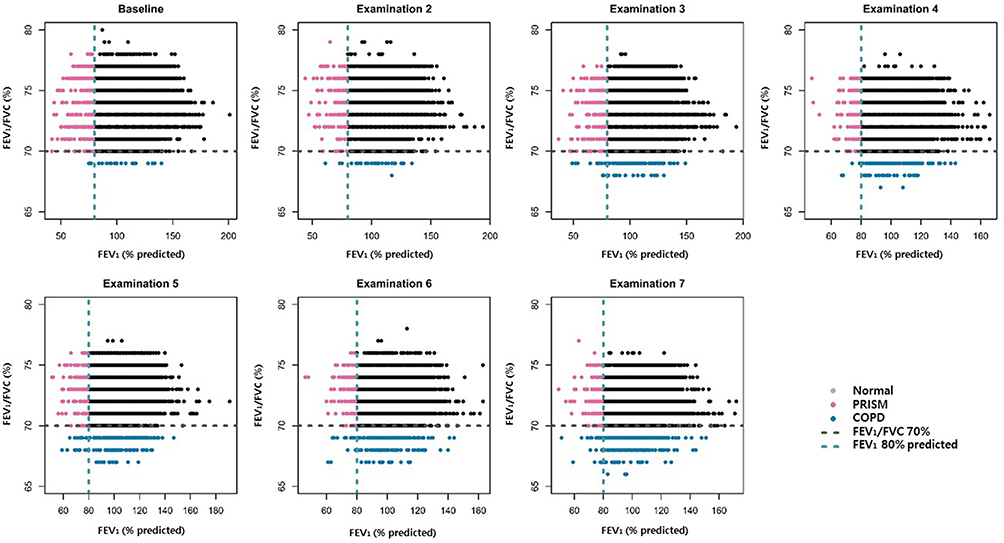 |
Figure 3 Population distribution across time points. Scatter plots show the joint distribution of FEV1 (% predicted) and FEV1/FVC (%) at baseline and six follow-up examinations. The dashed horizontal line indicates the threshold for COPD (FEV1/FVC = 70%), and the dashed vertical line indicates the threshold for PRISm (FEV1 = 80% predicted). Colors represent spirometric categories. |
Comparison of Clinical Characteristics According to Spirometric Trajectory Groups
Baseline clinical characteristics according to spirometric trajectory groups are presented in Table 3. Compared with NN, the NC group showed higher waist circumference, waist-to-hip ratio, blood pressure, current drinking, and smoking exposure in descriptive baseline comparisons. Baseline FEV1/FVC was also substantially lower in NC than in NN, whereas baseline FEV1 (% predicted) was lower in NP than in NN.
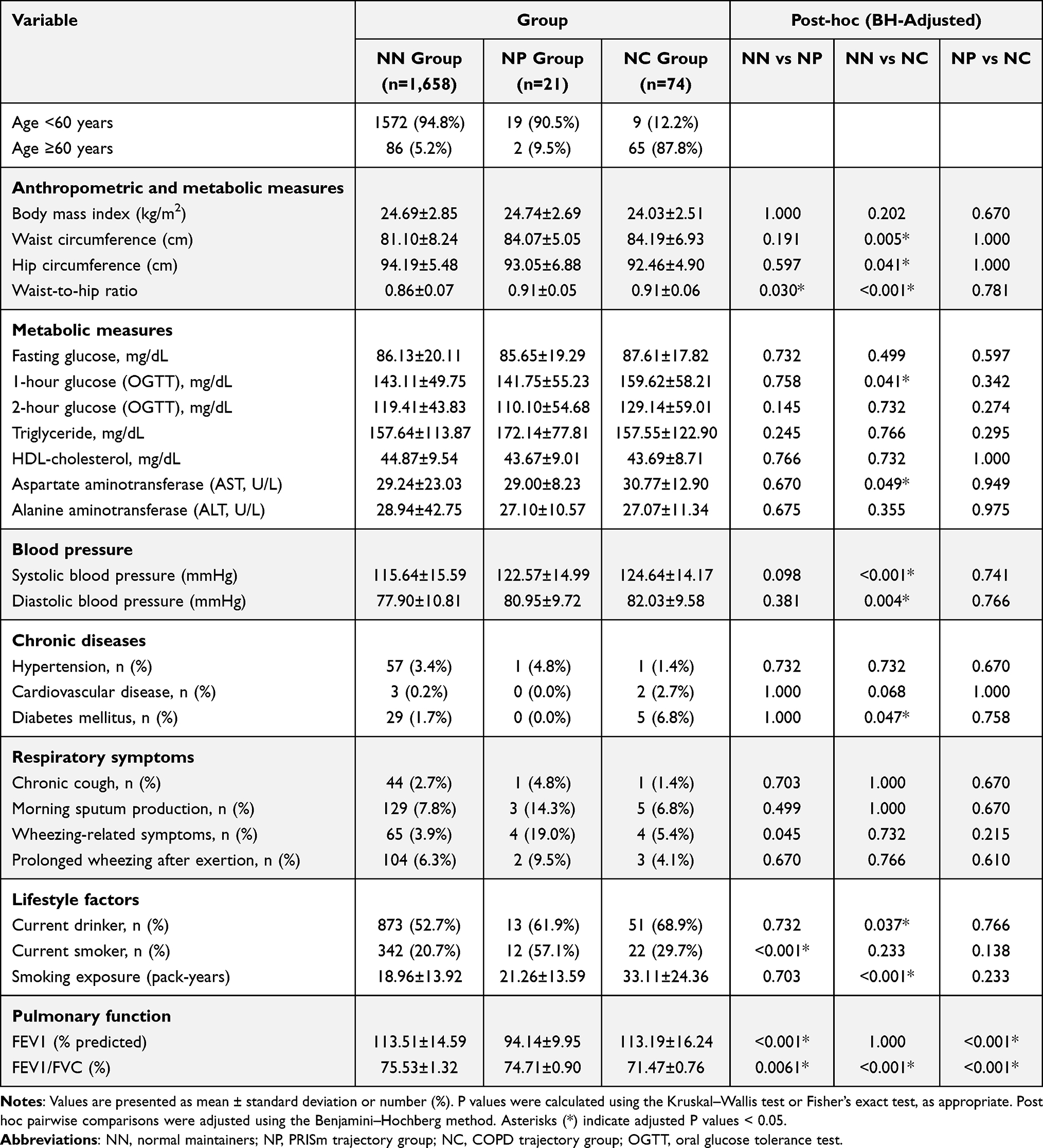 |
Table 3 Baseline Clinical Characteristics Across Spirometric Trajectory Groups |
Participants in the NP group were primarily characterized by wheeze-related respiratory symptoms, current smoking, and lower baseline FEV1 (% predicted). After adjustment for multiple comparisons, most baseline clinical characteristics did not differ significantly between the NP and NC groups, indicating substantial overlap in baseline profiles.
Logistic Regression Analysis of Trajectory Progression
Multivariable logistic regression analysis comparing the NC and NN groups is presented in Table 4. Older age (per 1-year increase; OR 1.45, 95% CI 1.36–1.55, p < 0.001) and current smoking (OR 7.49, 95% CI 3.37–16.61, p < 0.001) were strongly associated with increased odds of progression to the NC trajectory. In contrast, baseline cardiometabolic components, including waist circumference, systolic blood pressure, fasting glucose, and HDL cholesterol, were not independently associated with NC progression after adjustment. Triglyceride showed only a borderline association when expressed per 10 mg/dL increase (OR 0.97, 95% CI 0.94–1.00, p = 0.047). Because the number of NP events was small, regression analyses for NP versus NN were treated as exploratory and are not presented in detail.
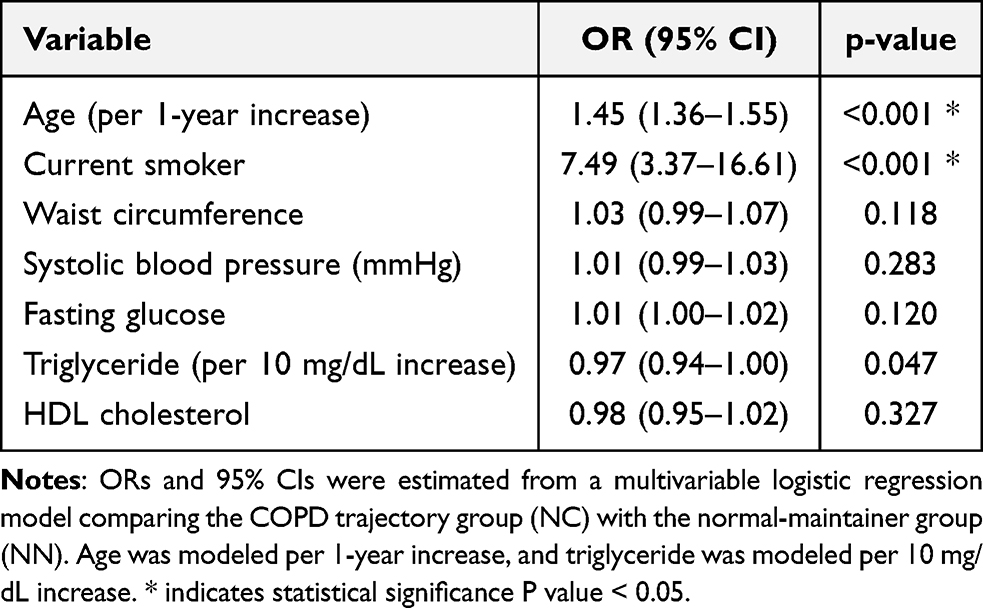 |
Table 4 Multivariable Logistic Regression Analysis for COPD Trajectory (NN vs NC) |
Discussion
This study characterized long-term spirometric trajectories and their clinical correlates using seven repeated spirometry assessments conducted at approximately 2-year intervals over a total follow-up period of approximately 12 years in a community-based Korean cohort. By focusing on within-person spirometric transitions rather than cross-sectional phenotypes, we identified heterogeneous patterns of lung-function change and examined differences in baseline clinical profiles across clinically meaningful trajectory groups. The extended follow-up duration and repeated standardized spirometry represent key strengths of this study and provide rare longitudinal evidence from an Asian population.9,15
Our trajectory analysis suggests that progression toward COPD does not follow a single linear pathway. Although some individuals exhibited transitions involving PRISm, most participants in the COPD trajectory progressed without a preceding sustained PRISm phase. Because non-monotone patterns, including reversions to normal spirometry, were not assigned to NN, NP, or NC in the final target-trajectory cohort, the present results should be interpreted as reflecting monotone target trajectories rather than the full spectrum of transient longitudinal variability.6,11,13
Interpretation of these trajectories should be grounded in spirometric definitions.4–6 In the present analysis, COPD was operationally defined using pre-bronchodilator spirometry as FEV1/FVC < 0.70, whereas PRISm was defined by reduced FEV1 in the presence of a preserved FEV1/FVC ratio. Within this framework, although FEV1 (% predicted) exhibited marked inter-individual variability over time, progression to COPD necessarily involved crossing the FEV1/FVC threshold used in our analysis. In contrast, PRISm classification appeared variably across examinations, reinforcing that PRISm and COPD represent distinct spirometric states rather than uniform sequential disease stages.4–6
This interpretation is consistent with prior longitudinal studies reporting substantial heterogeneity within PRISm, including stability, reversion to normal spirometry, and progression to COPD in only a subset of individuals.6,8,11,13,16 Together with evidence from large population-based cohorts, our findings challenge a simplified “normal → PRISm → COPD” paradigm and support the concept of multiple spirometric trajectories in the general population.9 In the UK Biobank cohort, for example, only a minority of individuals with PRISm progressed to COPD, while a substantial proportion reverted to normal spirometry over time.17
Clinical comparisons across trajectory groups further highlighted differences in baseline risk profiles. Participants in the COPD trajectory showed greater central adiposity, higher blood pressure, heavier smoking exposure, and more frequent current drinking than normal maintainers. These descriptive differences are broadly consistent with prior epidemiologic evidence linking smoking and cardiometabolic burden with COPD risk and progression.14,18,19 However, in multivariable logistic regression analysis, age and current smoking remained the most robust factors associated with progression to the COPD trajectory, whereas most cardiometabolic components did not retain independent associations after adjustment. These findings suggest that metabolic abnormalities may reflect shared risk profiles rather than direct causal determinants of COPD.
From a clinical perspective, an important observation was that most baseline clinical variables did not differ significantly between the PRISm and COPD trajectory groups after correction for multiple comparisons, indicating substantial overlap in baseline profiles. However, wheezing-related respiratory symptoms were more prominent among individuals in the PRISm trajectory group, distinguishing PRISm as a symptom-dominant phenotype despite preserved airflow ratios. This pattern suggests that PRISm represents a clinically relevant state characterized by wheeze-related symptoms and lower baseline lung function, rather than a uniform precursor to COPD. This interpretation is consistent with prior longitudinal and population-based studies reporting that PRISm is frequently associated with respiratory symptoms and metabolic vulnerability while demonstrating heterogeneous progression patterns.6,8,10,12 Metabolic abnormalities were more frequently observed among participants in trajectories associated with COPD; however, these findings should be interpreted as associations rather than evidence of causality. Taken together with the regression results, our data suggest that smoking exposure is a more consistent predictor of progression, whereas metabolic abnormalities may mark a higher-risk clinical profile without demonstrating strong independent effects.
These findings have important epidemiologic and clinical implications. PRISm should not be uniformly interpreted as a “pre-COPD” state. Instead, risk stratification may benefit from incorporating respiratory symptoms, central adiposity, smoking exposure, and longitudinal spirometric follow-up rather than relying on single time-point classification. Moreover, the observation that COPD can develop without a sustained PRISm phase highlights the limitations of cross-sectional spirometry and supports the value of repeated lung-function assessment in population-based prevention strategies.
From a public health perspective, our results reinforce the importance of smoking prevention and cessation as central strategies for reducing progression to COPD. At the same time, adverse metabolic profiles may help identify individuals with a higher-risk clinical background, even if their independent effects were attenuated after adjustment. Integrated approaches addressing both pulmonary and systemic health may therefore still be relevant in populations undergoing rapid demographic and metabolic transitions, such as those in East Asia.9
Several limitations warrant consideration. First, COPD was defined using pre-bronchodilator spirometry, which may have led to misclassification of reversible airway obstruction, such as asthma. Although participants with asthma-related baseline features and medication history were excluded during construction of the final analytic cohort, some misclassification cannot be entirely ruled out. Second, because COPD was classified using a fixed FEV1/FVC ratio rather than the lower limit of normal, age-related misclassification remains possible. In age-stratified analyses, direct transitions from normal spirometry to COPD were strongly concentrated in older participants, particularly in the ≥60 baseline age group, suggesting that aging may partly contribute to this pattern. Third, because the final analytic cohort was defined through a prespecified trajectory-analysis pipeline, including classifiable spirometry across all seven examinations, baseline normal spirometry, and additional analytic restrictions, some selection bias cannot be excluded. In particular, excluded participants were older, had greater smoking exposure, and had poorer baseline lung function than those included in the final analysis. Thus, the analytic sample may represent a relatively healthier subset of participants who were available for repeated long-term follow-up, and generalizability should be interpreted with caution. Fourth, although model-based trajectory methods can identify latent patterns, we adopted a clinically grounded rule-based classification to enhance interpretability and consistency with spirometric thresholds commonly used in clinical and epidemiologic practice. Nevertheless, transient spirometric variability may still have influenced some group assignments. Fifth, the relatively small number of participants in the PRISm trajectory group may have limited statistical power to detect subtle differences between PRISm and COPD trajectories after correction for multiple comparisons. Finally, clinical comparisons were primarily descriptive, and residual confounding cannot be excluded. Future studies incorporating longitudinal causal modeling and imaging-based phenotyping may further clarify mechanisms underlying heterogeneous spirometric trajectories.
Despite these limitations, the long follow-up duration with repeated spirometry provides valuable insight into spirometric transitions and their clinical correlates in a community-based Korean cohort. Our findings add to growing evidence that progression toward COPD is heterogeneous and underscore the importance of longitudinal approaches in respiratory epidemiology.1,5
Conclusion
In this population-based cohort, repeated spirometry revealed heterogeneous longitudinal patterns of lung-function change. Under the pre-bronchodilator spirometric framework used in this study, some individuals met criteria for COPD without a sustained PRISm phase, whereas PRISm showed variable longitudinal courses. Trajectories associated with COPD were more frequently accompanied by greater smoking exposure and adverse cardiometabolic profiles, whereas PRISm was characterized by lower baseline lung function and more wheeze-related symptoms, with limited evidence of a broadly adverse metabolic profile. These findings highlight the value of longitudinal spirometric assessment for understanding heterogeneous pathways toward COPD and for improving risk stratification in the general population.
Data Sharing Statement
The data used in this study are available from the corresponding author upon reasonable request, subject to the policies of the Korean Genome and Epidemiology Study (KoGES) and the Korea Disease Control and Prevention Agency (KDCA).
Ethics Approval and Informed Consent
This study was conducted using bioresources from the National Biobank of Korea, Korea Disease Control and Prevention Agency. All participants provided written informed consent. The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Soonchunhyang University (IRB No. 2024-05-049).
Acknowledgments
The authors thank the participants and staff of the Korean Genome and Epidemiology Study (KoGES) for their valuable contributions.
Author Contributions
Sun Young Kang conceived the study, designed the analysis, and drafted the manuscript. Sanghyun Roh contributed to methodology and visualization. In Hwan Yeo contributed to data preprocessing and statistical analysis. Young Kyung Ko contributed to data management and quality control. Jee Youn Oh and Jeong-An Gim contributed to project administration and critical revision of the manuscript. All authors made a significant contribution to the work reported; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article was submitted; and agreed to be accountable for all aspects of the work.
Funding
This research was supported by the Global Learning & Academic Research Institution for Master’s–PhD Students and Postdocs (G-LAMP) Program of the National Research Foundation of Korea (NRF), funded by the Ministry of Education (No. RS-2025-25441283), and by an NRF grant funded by the Korean government (MSIT) (No. 2022R1C1C1009250).
Disclosure
The authors have no conflicts of interest to declare for this study.
References
1. Mirza S, Clay RD, Koslow MA, Scanlon PD. COPD guidelines: a review of the 2018 GOLD report. Mayo Clin Proc. 2018;93(10):1488–13. doi:10.1016/j.mayocp.2018.05.026
2. Agustí A, Celli BR, Criner GJ, et al. Global Initiative for chronic obstructive lung disease 2023 report. Arch Bronconeumol. 2023;59(5):326–333. doi:10.1016/j.arbres.2023.03.002
3. Lin CH, Cheng SL, Chen CZ, Chen CH, Lin SH, Wang HC. Current progress of COPD early detection: key points and novel strategies. Int J Chron Obstruct Pulmon Dis. 2023;18:1511–1524. doi:10.2147/COPD.S420640
4. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
5. Stanojevic S, Kaminsky DA, Miller MR, et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J. 2022;60(1):2101499. doi:10.1183/13993003.01499-2021
6. Huang J, Li W, Sun Y, et al. Preserved ratio impaired spirometry (PRISm): a global epidemiological overview, radiographic characteristics, comorbid associations, and differentiation from chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2024;19:753–764. doi:10.2147/COPD.S442345
7. Cadham CJ, Drucker AM, Wise RA, et al. The prevalence and mortality risks of PRISm and COPD: a population-based cohort study. Am J Respir Crit Care Med. 2024;209(8):912–921. doi:10.1164/rccm.202310-1783OC
8. Wan ES, Fortis S, Regan EA, et al. Longitudinal phenotypes and mortality in preserved ratio impaired spirometry in the COPDGene study. Am J Respir Crit Care Med. 2018;198(11):1397–1405. doi:10.1164/rccm.201801-0142OC
9. Jo YS, Rhee CK, Kim SH, Lee H, Choi JY. Spirometric transition of at-risk individuals and risks for progression to chronic obstructive pulmonary disease in the general population. Arch Bronconeumol. 2024;60(10):634–642. doi:10.1016/j.arbres.2024.05.033
10. Fortis S. The clinical spectrum of PRISm. Am J Respir Crit Care Med. 2022;206(7):769–771. doi:10.1164/rccm.202205-0965ED
11. Marott JL, Ingebrigtsen TS, Çolak Y, Vestbo J, Lange P. Trajectory of preserved ratio impaired spirometry: natural history and long-term prognosis. Am J Respir Crit Care Med. 2021;204(8):910–920. doi:10.1164/rccm.202102-0517OC
12. Washio Y, Sakata S, Fukuyama S, et al. Risks of mortality and airflow limitation in Japanese individuals with preserved ratio impaired spirometry. Am J Respir Crit Care Med. 2022;206(5):563–572. doi:10.1164/rccm.202110-2302OC
13. Wijnant SRA, De Roos E, Kavousi M, et al. Trajectory and mortality of preserved ratio impaired spirometry: the Rotterdam Study. Eur Respir J. 2020;55(1):1901217. doi:10.1183/13993003.01217-2019
14. Lange P, Celli B, Agustí A, et al. Lung-function trajectories leading to chronic obstructive pulmonary disease. N Engl J Med. 2015;373(2):111–122. doi:10.1056/NEJMoa1411530
15. Leem AY, Park B, Kim YS, Chang J, Won S, Jung JY. Longitudinal decline in lung function: a community-based cohort study in Korea. Sci Rep. 2019;9(1):13614. doi:10.1038/s41598-019-50165-z
16. Xu H, Li Y, Wang J, et al. Associated factors and pulmonary function outcomes of preserved ratio impaired spirometry: a longitudinal cohort study. Respir Res. 2025;26(1):45. doi:10.1186/s12931-025-03012-3
17. Higbee DH, Granell R, Smith GD, Dodd JW. Prevalence, risk factors, and clinical implications of preserved ratio impaired spirometry: a UK Biobank cohort analysis. Lancet Respir Med. 2022;10(2):149–157. doi:10.1016/S2213-2600(21)00357-7
18. Sin DD, Man SF. Chronic obstructive pulmonary disease as a risk factor for cardiovascular morbidity and mortality. Proc Am Thorac Soc. 2005;2(1):8–11. doi:10.1513/pats.200404-017MS
19. Fabbri LM, Rabe KF. From COPD to chronic systemic inflammatory syndrome? Lancet. 2007;370(9589):797–799. doi:10.1016/S0140-6736(07)61383-X
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Influences of Two FEV1 Reference Equations (GLI-2012 and GIRH-2017) on Airflow Limitation Classification Among COPD Patients
Wei D, Wang Q, Liu S, Tan X, Chen L, Tu R, Liu Q, Jia Y, Liu S
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2053-2065
Published Date: 2 September 2022
Prevalence of Chronic Obstructive Pulmonary Disease in an Urban Area. Changes in COPD Ten Years on

García Castillo E, Alonso Pérez T, Peláez A, Pérez González P, Soriano JB, Ancochea J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2431-2441
Published Date: 29 September 2022
The Relationship Between BMI and Lung Function in Populations with Different Characteristics: A Cross-Sectional Study Based on the Enjoying Breathing Program in China
Tang X, Lei J, Li W, Peng Y, Wang C, Huang K, Yang T
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2677-2692
Published Date: 18 October 2022
The Impact of Lung Function Parameters on Sleep Among Aboriginal Australians – A Polysomnography and Spirometry Relationship Study
Howarth T, Ben Saad H, Heraganahally SS
Nature and Science of Sleep 2023, 15:449-464
Published Date: 9 June 2023
Prevalence and Associated Factors of Chronic Obstructive Pulmonary Disease Among Adults in Neno District, Malawi: A Cross-Sectional Analytical Study
Zaniku HR, Connolly E, Aron MB, Matanje BL, Ndambo MK, Talama GC, Munyaneza F, Ruderman T, Rylance J, Dullie LW, Lalitha R, Banda NPK, Muula AS
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:389-401
Published Date: 5 February 2024