Back to Journals » Nature and Science of Sleep » Volume 15
The Impact of Lung Function Parameters on Sleep Among Aboriginal Australians – A Polysomnography and Spirometry Relationship Study
Authors Howarth T ![]() , Ben Saad H
, Ben Saad H ![]() , Heraganahally SS
, Heraganahally SS ![]()
Received 1 March 2023
Accepted for publication 22 May 2023
Published 9 June 2023 Volume 2023:15 Pages 449—464
DOI https://doi.org/10.2147/NSS.S409883
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Timothy Howarth,1– 3 Helmi Ben Saad,4 Subash S Heraganahally1,5,6
1Darwin Respiratory and Sleep Health, Darwin Private Hospital, Darwin, Northern Territory, Australia; 2Department of Technical Physics, University of Eastern Finland, Kuopio, Finland; 3College of Health and Human Sciences, Charles Darwin University, Darwin, Northern Territory, Australia; 4Faculté de Médecine de Sousse, Hôpital Farhat HACHED de Sousse, Laboratoire de recherche “Insuffisance Cardiaque” (LR12SP09), Université de Sousse, Sousse, Tunisia; 5Department of Respiratory and Sleep Medicine, Royal Darwin Hospital, Darwin, Northern Territory, Australia; 6College of Medicine and Public Health, Flinders University, Adelaide, South Australia, Australia
Correspondence: Subash S Heraganahally, Email [email protected]; [email protected]
Background: Sleep disorders such as obstructive sleep apnoea (OSA) are known to overlap significantly with airway diseases in various populations. This study assessed the relationship between lung function parameters against polysomnography (PSG) and continuous positive airway pressure (CPAP) adherence data amongst an Aboriginal Australian population.
Methods: Patients who undertook both a diagnostic PSG and spirometry were included. Restrictive, obstructive, and mixed impairments were assessed via global lung function initiative (GLI-2012, ATS/ERS) criteria/guidelines. PSG and CPAP data were evaluated between patients with or without spirometry impairments.
Results: Of the total 771 patients, 248 had PSG and spirometry data available (52% female, 44% remote residents, 78% obese). The majority (89%) had OSA (51% severe), 95 (38%) were observed to have a restrictive impairment, and 31 (13%) had an obstructive or mixed impairment on spirometry. Compared to patients with no spirometric impairment, those with restrictive or obstructive/mixed impairments demonstrated significantly lower sleep efficiency (median 84% vs 79% and 78%), higher apnoea-hypopnea index (AHI) during rapid eye movement (REM) sleep (median 32 vs 52 and 55 events/hour), reduced REM oxygen saturation (SpO2) (median 94.0% vs 92.0% and 92.5%) and reduced adherence to CPAP therapy (median 39% vs 22% and 17%). Differences in sleep efficiency, REM AHI, and NREM SpO2 held for patients with obstructive/mixed impairments in multivariate modelling.
Conclusion: Aboriginal Australian patients with OSA have a higher concurrent lung function’ impairment. Spirometric impairment appears to negatively influence sleep efficiency, nocturnal SpO2 and CPAP adherence. This may have substantial implications for OSA management among Aboriginal Australians.
Keywords: COPD, CPAP, first nations, OSA, sleep apnoea, spirometry
Plain Language Summary
The existence of Aboriginal people in the Northern Australian continent dates back to 65,000 years (Clarkson et al. Human occupation of northern Australia by 65,000 years ago. Nature 2017). The First Australians had belief in dreaming and fostered dreaming as an avenue for advocating moral, human behaviour and culture. Aboriginal elders have also identified that sleep is an important aspect of wellbeing and that lack of quality sleep could have a critical effect on spirituality, connection to the land, country, and kinship. However, similar to Indigenous populations globally, a history of colonisation and dispossession of country has resulted in ongoing intergenerational trauma and disadvantage, moreover, adaptation to demanding modern world and culture has resulted in contemporary health inequities. Indigenous Australians have a higher burden of lung/breathing disorders in comparison to non-Indigenous Australians. However, no studies have examined the impact of sleep in the presence or absence or its interrelationship with lung/breathing disorders in Aboriginal people. This study for the first time assessed sleep health profile and its relationship to lung function/breathing amongst adult Aboriginal Australians in Northern Australia and has demonstrated that presence of abnormal lung function/breathing could have an impact on several sleep-related domains, more specifically during rapid eye movement sleep and in overall sleep efficiency. Hence, it is reasonable to speculate that improving lung function/breathing would result in better sleep in Aboriginal people.
Introduction
The Australian Aboriginal population experiences a higher prevalence of chronic airway diseases than their non-Aboriginal peers.1 Emerging literature highlights the high prevalence of chronic obstructive pulmonary disease (COPD), bronchiectasis, and asthma, among other complex and comorbid conditions, as well as reduced lung function in the absence of objective evidence of disease.2–12 Presence of chronic airway diseases and reduced lung function have been noted to significantly increase the risk of, and overlap with sleep disorders such as obstructive sleep apnoea (OSA), in turn leading to adverse bi-directional health effects resulting in significantly worse outcomes.13–15 Yet, despite the enhanced risk of, and greater potential sequelae from sleep-related disorders, limited literature exists regarding the prevalence of sleep disorders and sleep health outcomes among the Aboriginal Australian population.16,17 Furthermore, common tools to assess sleep health outcomes such as the Epworth sleepiness scale (ESS) have shown limited validity among Aboriginal Australians.18 Limited evidence in the literature suggests a heightened prevalence of both insomnia and inadequate sleep and sleep disordered breathing in this population.17,19–24
Numerous previous studies have utilised spirometry to predict or identify the association between lung function and sleep health parameters.15,25–30 Forced expiratory volume in one second (FEV1) was reported to be both a strong predictor of OSA,15,25 and strongly susceptible to decline over time among patients with OSA.26 However, other studies have shown limited correlation between spirometry parameters and sleep-related breathing disorders.27–29 Furthermore, there is a considerable range of spirometric abnormalities defined and identified across studies and regions, with restrictive or obstructive impairments among patients with OSA recorded as 10% and 40% in India,27 73% and 16% in Algeria,31 and 12% and 18% in Portugal.25 Further complicating matters, differing definitions of spirometric impairment have been utilised across studies.25–30,32
The applicability of these studies to the Aboriginal Australian adult population, who have a significant prevalence of chronic airway diseases and lung function impairment, is doubtful. Of additional concern is the gold standard treatment of OSA via continuous positive airway pressure (CPAP) therapy, for which adherence is noted to be low,31 may be impacted by the presence of airway diseases33 – especially those, such as bronchiectasis for which a productive cough is a common symptom. Hence, it is crucial to assess the association of spirometric parameters to polysomnographic (PSG) outcomes among the Aboriginal Australian adult population. We hypothesised that presence and type of lung function abnormality either; normal, restrictive, obstructive or mixed impairments would have an influence on sleep, as assessed on PSG, including long-term adherence to CPAP therapy. Therefore, in this study, we aimed to assess the prevalence of spirometric impairment among Aboriginal Australian patients referred for a PSG, the potential bidirectional associations between OSA severity and lung function impairment, and the association between lung function impairments and CPAP adherence among adult Aboriginal patients in the Top End Health Service (TEHS) region of the Northern Territory (NT) of Australia.
Methods
Setting and Ethical Approval
This study was conducted at the respiratory and sleep service at the Royal Darwin Hospital and Darwin respiratory and sleep health (DRSH)/Darwin Private Hospital based in the TEHS region of the NT of Australia. This study is a part of a larger project assessing factors influencing and implications of lung function parameters in Aboriginal Australians, inclusive of study participants from our previous reports.10,19,34,35 The project was approved by the Human Research Ethics Committee of the NT, TEHS and Menzies School of Health Research (Reference no: Human Research Ethics Committee 2019–3445) and was conducted according to the Declaration of Helsinki. As the study was retrospective in nature, individual patients' consent or consent to review their medical records was waived by the research committee. Patient data confidentiality was ensured for all patients involved in this study.
Study Patient Inclusion & Data Collection
All adult patients (>18 years) who self-identified as of Aboriginal and/or Torres Strait Islander descent who underwent a diagnostic PSG at DRSH between 2012 and 2020 and had spirometry recorded in the same time period were included in this study. Data for patients with a failed diagnostic sleep study, those with failed spirometry and those with missing data, were excluded from the final analysis. Patients were referred to specialist respiratory and sleep service for further assessment by general practitioners, primary health care or other specialist practitioners based on clinical judgment for the presence of either sleep or respiratory disorders.
Prior to undergoing a diagnostic PSG, all patients completed a detailed questionnaire providing self-reported Aboriginal status, age, sex, smoking status, usual place of residence, and subjective daytime sleepiness via ESS.36 Place of usual residence was coded according to the Australian Statistical Geography Standard (ASGS) (ASGS-3: outer regional, AGSG-4: remote, ASGS-5: very remote).37 Anthropometric measures of height, weight and neck circumference were collected prior to the sleep study. Body mass index (BMI) was calculated in a normal fashion and categorised as underweight (<18.5 kg/m2), normal weight (≥18.5 and <25 kg/m2), overweight (≥25 and <30 kg/m2) or obese (≥30 kg/m2). Patients’ electronic medical records (EMRs) and radiology reports where available were checked for presence of comorbid COPD.10
Patients underwent a diagnostic PSG either as a level-1 in-lab monitored sleep study or as an unmonitored ambulatory level-2 study following an initial consultation and as per the discretion of the treating respiratory/sleep physician. PSG parameters utilised for this analysis included total sleep time (TST), sleep latency, rapid eye movement (REM) latency, wake after sleep onset (WASO), sleep efficiency (with low sleep efficiency defined as sleep efficiency <80%), percentage of total sleep time spent in non-REM (NREM) stage 1, 2, 3 or REM sleep, arousal indexes [total (TAI), respiratory (RAI), spontaneous (SAI)], apnoea/hypopnoea index (AHI) in total and for both REM and NREM sleep, with presence of OSA defined as an AHI >5 events/hour, and further broken down into mild (AHI 5–15), moderate (AHI 15–30), or severe (AHI >30), and oxygen saturations (SpO2) averages in total and for each of REM, NREM, and wake stages in addition to absolute nadir. Further details regarding PSG testing protocol as per recommended guidelines are available from a previous report from our centre.19
Spirometry tests were performed via a portable single-breath carbon monoxide diffusing capacity device “EasyOne Pro®, ndd Medical Technologies (Medizintechnik).” Only spirometry results that were graded as acceptable and repeatable38 were included in the analysis. For the purposes of this study and in the absence of specific spirometric norms for Aboriginal Australians, the predicted values were calculated using the Global lung function initiative data (GLI-2012) (other/mixed ethnicity).39 Parameters assessed were FEV1, forced vital capacity (FVC), FEV1/FVC ratio, bronchodilator responsiveness (BDR, defined as per updated 2022-international criteria as a change of ≥10% in percent predicted values of FEV1 or FVC), as per ATS/ERS guidelines.40 Further details on spirometry testing are described in our previous reports.4,7,8,10,11,34,35,41,42
Four spirometry impairments were defined on the basis of post-bronchodilator (BD) values:40
- Restrictive impairment: post-BD FVC < lower limit of normal (LLN) in the absence of an obstructive impairment.
- Obstructive impairment: post-BD FEV1/FVC < LLN in the absence of a restrictive impairment.
- Mixed impairment: presence of both obstructive and restrictive impairments.
- Normal spirometry: absence of both obstructive and restrictive impairments.
In cases where the patient had multiple diagnostic PSGs or spirometries, the PSG and spirometry with the shortest time lag between were selected for analysis.
CPAP Data
In our centre, patients with moderate or severe OSA are offered CPAP therapy, or in the case of mild OSA patients with cardiovascular comorbidities, including in the presence of arterial hypertension. Patients may either undertake an in-lab CPAP titration or an un-monitored auto-positive airway pressure (APAP) trial, and if the patient accepts therapy, they are offered a further home trial for 4–8 weeks. At the end of this trial period, patients who are assessed to be adapting and adherent to CPAP (via assessment of downloaded data from the CPAP device) are eligible for a health department funded CPAP device.43 For the current study, device data were downloaded and information on usage (up to maximum 180 days) was utilised to determine the percentage of nights with use, average nightly hours of use (on nights with device use), percentage of nights with at least 4 hr of use and adherence which was defined as 70% of nights with at least 4 hr of use.31,44
Statistical Methods
Data were not normally distributed as tested on Shapiro–Wilks and thus reported as median (interquartile range (IQR)). Differences in demographic and clinical parameters between patients with and without OSA were tested via Kruskal–Wallis rank sum test for continuous parameters, and chi-square test for categorical parameters or Fishers exact test in instances where categories contained less than 10 participants. Differences in PSG outcomes between spirometry impairments (normal spirometry vs restrictive impairment vs obstructive/mixed impairment) and differences in spirometry parameters by OSA severity (mild vs moderate vs severe) were tested via quantile regression for continuous parameters, logistic regression for binary parameters, and ordered logistic regression for step outcomes. Multivariate quantile or logistic regression models adjusted for age, sex, BMI, remoteness (ASGS-3, −4 or −5) and smoking status were utilised to identify the effect of spirometry impairments on PSG outcomes, with results reported as beta (95% confidence interval (95% CI)) or odds ratio (OR), utilising “normal spirometry” as the reference. Alpha was set to 0.05 throughout, and all analyses were conducted in STATA IC 15 (StataCorp Texas).
Results
Study Participants and Clinical Data
A total of 771 adult Aboriginal patients were identified to have undergone a diagnostic PSG in the study timeframe, of whom 294 had spirometry available. Excluding patients with a failed diagnostic sleep study (n=14, 5%), those with failed spirometry (n=21, 7%) and those with missing data (n=16, 5%) resulted in 248 patients for analysis, of whom the majority (89%, n=221) had OSA (Figure 1). Most patients were female (52%), resided in outer regional areas (56%) and were classified as obese (78%). The median time between PSG and spirometry was 22 days (IQR 3, 173), and the majority of patients (72%) had their PSG prior to the spirometry. There were significant differences in proportion of females, weight, BMI, neck circumference and ESS between patients with OSA and those without, such that patients with OSA were male, heavier, had a larger neck circumference and a greater ESS (Table 1). Baseline data for PSG and spirometry parameters are shown in Supplementary File A. Half of the cohort had no spirometry impairment identified (n=122, 49%), just over one-third (38%, n=95) showed a restrictive impairment, while isolated obstructive or mixed impairments were rare, occurring in 3% (n=7) and 10% (n=24) of patients, respectively. Hence, subsequent analyses merged obstructive and mixed impairments into a single group.
 |
Table 1 Demographic and Clinical Profile of Study Patients by Obstructive Sleep Apnoea (OSA) Presence |
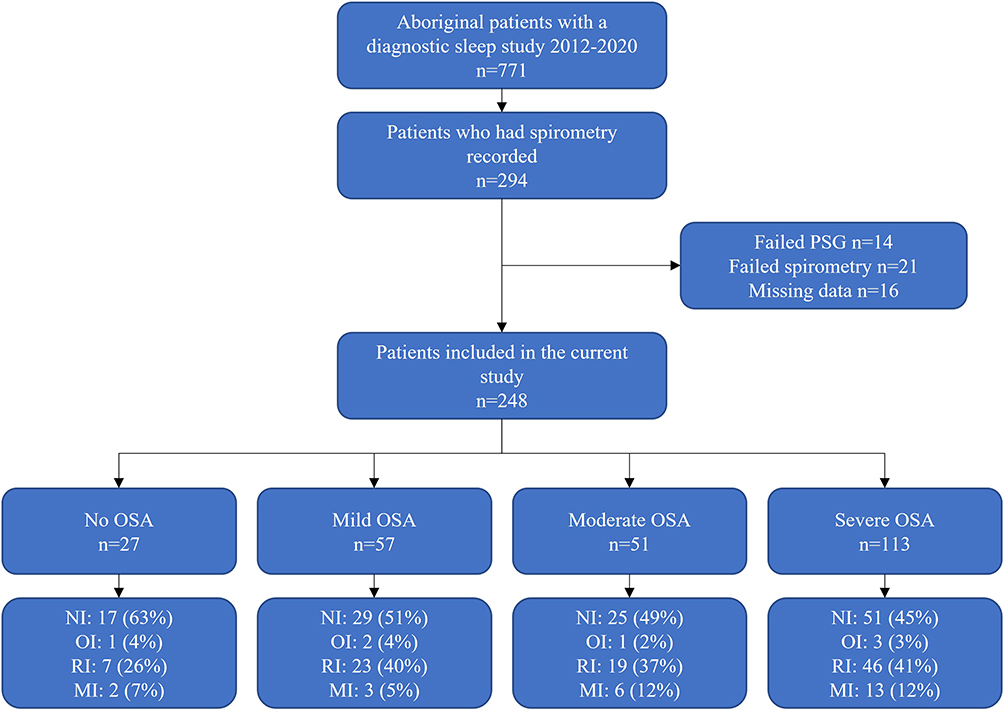 |
Figure 1 Flow chart of patient inclusion, OSA severity categorisation and spirometry impairment. Abbreviations: MI, Mixed impairment; NI, No impairment; OI, Obstructive impairment; OSA, obstructive sleep apnoea; PFT, Pulmonary function test; PSG, Polysomnography; RI, Restrictive impairment. |
Spirometry Parameters by OSA Severity
Among patients with no OSA, and those with mild, moderate or severe OSA, there were limited differences in spirometry parameters (Table 2). Post-BD percent predicted values for FVC were significantly reduced among severe OSA patients compared to no-OSA patients (beta 0.11 (95% CI 0.02, 0.2)), with a decreasing trend evident from no-OSA to mild to moderate to severe OSA (medians 88, 82, 79 and 77%, respectively). This decreasing trend was also seen for FEV1 (medians 90, 82, 81 and 78%, respectively, from no- to severe OSA), and the proportion of patients with no spirometry impairment (63, 51, 49 and 45%, respectively); however, these differences did not reach statistical significance. In multivariate regression models, no significant differences were noted between mild, moderate or severe OSA patients compared to no-OSA patients for any parameters (Figure 2).
 |
Table 2 Spirometry Parameters Split by Presence and Severity of Obstructive Sleep Apnoea (OSA) |
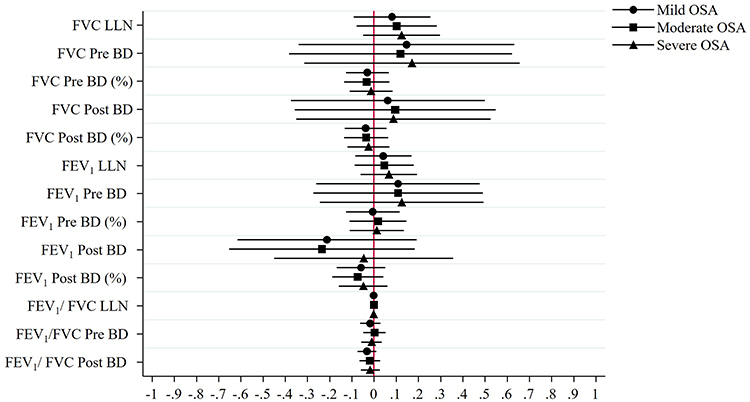 |
Figure 2 Coefficients plot of multivariate regression effects showing effect of severity of OSA compared to no OSA baseline on spirometry parameters. Abbreviations: BD, bronchodilator; FEV1, Forced expiratory volume in 1 s; FVC, Forced vital capacity; LLN, Lower limit of normal; OSA, obstructive sleep apnoea. |
Polysomnography Parameters by Spirometry Impairment
Patients with a restrictive impairment showed significantly reduced sleep efficiency (beta 5.8% (95% CI 0.7, 10.9)) compared to patients with no spirometry impairment, while patients with obstructive/mixed impairments showed significantly increased odds of recording low sleep efficiency (OR 2.3 (95% CI 1, 5.2)) (Table 3). Both patients with restrictive impairment and those with obstructive/mixed impairments showed significantly increased REM AHI (beta 19.8 events/hour (95% CI 4.8, 34.8) and 22.7 events/hour (95% CI 0.4, 45.1), respectively), which corresponded to a significant reduction in REM sleep percentage and REM sleep SpO2 among those with a restrictive impairment (beta 5.4% (95% CI 2.5, 8.3) and 2% (95% CI 0.1, 3.9), respectively), yet not among those with obstructive/mixed impairments (2.8% (95% CI −1.5, 7.2) and 2% (95% CI −0.7, 4.7), respectively). Total average and NREM SpO2 were significantly reduced among patients with obstructive/mixed impairments (2% (95% CI 0.1, 3.9) and 2% (95% CI 0.2, 3.8), respectively), though not among patients with a restrictive impairment.
 |
Table 3 Polysomnography (PSG) Parameters by Normal Spirometry, Restrictive or Obstructive/Mixed Impairments on Spirometry |
Among patients who used CPAP for >30 days, the percentage of days with at least 4 hr of CPAP use was significantly lower among patients with a restrictive impairment compared to patients with normal spirometry (beta 33.9% (95% CI 8.6, 59.3)). Although there was a lower proportion of patients with restrictive or obstructive/mixed impairments adherent to CPAP compared to those with no impairment, this did not reach statistical significance.
Multivariate Regression Modelling of Polysomnography Parameters by Spirometry
In multivariate regression models, patients with obstructive/mixed impairments had significantly increased odds of having low sleep efficiency compared to patients with no impairment (OR 2.6 (95% CI 1, 6.4)), while patients with a restrictive impairment showed no significant difference (Table 4). The previously noted changes in REM sleep percentage, AHI and SpO2 among patients with a restrictive impairment (Table 3) were fully attenuated in the multivariate models, as was the difference in percentage of nights with at least 4 hours of CPAP use. Among patients with obstructive/mixed impairments; however, there remained a significant increase in REM AHI (beta 20.7 events/hour (95% CI 2.8, 38.6)), borderline reductions in SpO2 while awake or in REM (1% (95% CI −0.1, 2.1) and 2% (95% CI −0.2, 4.6), respectively), and significant reductions in SpO2 total average and during NREM (beta 1.6% (95% CI 0.3, 3) and 2.1% (95% CI 0.4, 3.9), respectively).
 |
Table 4 Quantile Regression (Continuous Parameters) and Logistic Regression (Binary Parameters) for the Effects of Restrictive or Obstructive/Mixed Impairments of Spirometry Against the Reference of “Normal” Spirometry, Adjusting for Age, Sex, Body Mass Index, Remoteness and Smoking Status |
When assessing lung function parameters as continuous predictors (FVC, FEV1 & FEV1/FVC) we noted some different patterns of results when compared to the previous assessment by impairment category (Figure 3). One unit increases in both FVC and FEV1 were associated with significantly reduced WASO (median −16.7 and −21.5 min, respectively) and significantly increased sleep efficiency (3% and 4.2%, respectively). Both were also significantly associated with increased SpO2 in NREM sleep and borderline increases in total average and nadir values. NREM SpO2 was the only outcome significantly influenced by changes in FEV1/FVC (beta 7.45% (95% CI 2.15, 12.74)), with all other FEV1/FVC outcomes showing significantly larger confidence intervals than either FVC or FEV1 alone.
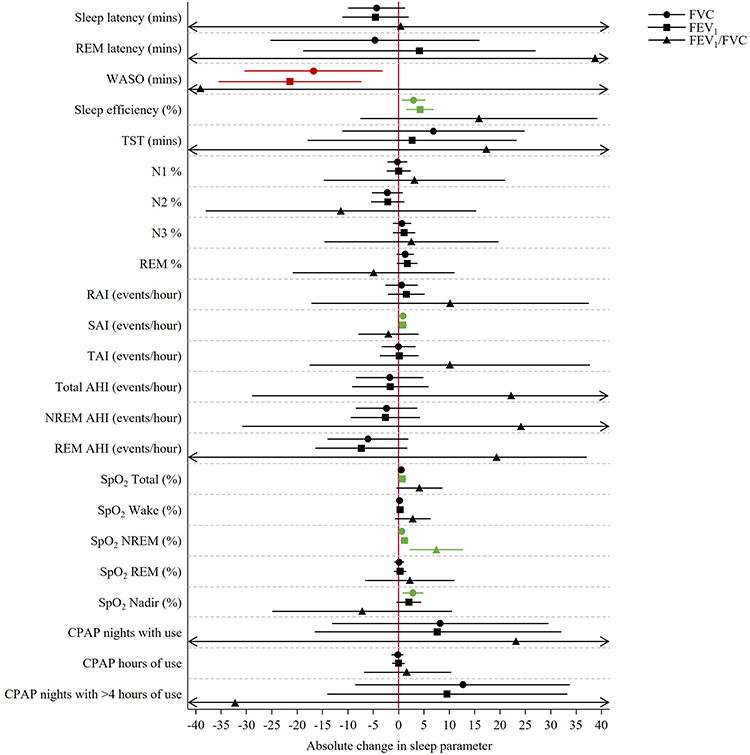 |
Figure 3 Coefficients plot of multivariate regression effects for one unit change in FVC, FEV1 & FEV1/FVC. Abbreviations: AHI; apnoea-hypopnoea index; CPAP, Continuous positive airway pressure FEV1, Forced expiratory volume in 1 s; FVC, Forced vital capacity; N1/2/3, Non-REM stage 1/2/3; RAI, Respiratory arousal index; REM, Rapid eye movement; SAI, Spontaneous arousal index; SpO2, oxygen saturation; TAI, Total arousal index; TST, Total sleep time, WASO, Wake after sleep onset. |
Discussion
To the best of the authors’ knowledge, this is the first study to assess spirometry parameters in relation to PSG findings among an adult Aboriginal Australian population and demonstrated several key findings:
- Restrictive ventilatory abnormality was the most common spirometric impairment in the presence of OSA.
- Presence of ventilatory impairment has a negative influence on sleep efficiency.
- REM sleep stages are particularly affected by the presence of ventilatory impairment.
- Presence or absence of spirometric impairments may help to predict CPAP adherence.
The Aboriginal Australian population has a high prevalence of chronic airway diseases and experiences significantly greater and earlier morbidity and mortality as sequelae from them than non-Aboriginal populations.2,3,6,8–11,17,34,35,42,45 The recognised potential for overlap between pulmonary function parameters and sleep disordered breathing is reflected in the relatively high proportion (38%) of patients who had been referred for a spirometry among the PSG patient cohort. The prevalence of spirometric impairment was high, as reported in previous publications from this region,4,7,8,34 with half (51%) of the patients with spirometry available recording an impairment. Among those patients with OSA, a restrictive impairment was the most common, present in 40% of patients while obstructive or mixed impairments were present in 3% and 10%, respectively. Overall, 33% of patients with OSA in the current study had evidence of COPD/OSA overlap (via either an existing COPD diagnosis or evidence of obstructive impairment on spirometry), which is in the middle of the range previously reported among OSA patients.46,47
In addition to COPD, literature also shows evidence for significant nocturnal symptoms among patients with bronchiectasis,48–50 with the prevalence of OSA particularly increased among patients with comorbid COPD & bronchiectasis.51 Although bronchiectasis was not reported in the current study, among Aboriginal Australian children in the NT, the incidence of bronchiectasis has been reported to be the highest seen worldwide,52 and among Aboriginal Australian adults with COPD in the NT, comorbid bronchiectasis is seen in about 30%.6,10,34,53,54 In this population, bronchiectasis has been associated with restrictive impairment on spirometry,54 and a restrictive impairment was common in the current study. Overall, the frequency of spirometric impairments was similar to what has been reported among Algerian or Indian patients,27,32 and significantly higher than what has been reported among European and non-Aboriginal Australian patients.25,55 Additionally, patients in the current study had mean 48 years of age, similar to small studies from Algeria,32 India27 and Serbia,28 yet significantly younger than European studies.25,26,46,56
Previous reports have shown that up to 40% of patients with COPD could experience disturbed sleep, particularly during REM sleep – with greater awakenings and micro-arousals, significantly disrupting sleep architecture.57,58 Indeed, in the current study 52% of restrictive and 60% of obstructive/mixed impairment patients had a sleep efficiency of less than 80%, and in multivariate adjusted models, the odds of having low sleep efficiency were significantly heightened (OR 2.6). Moreover, in line with previous research, we found significantly greater impacts of obstructive impairments on REM sleep compared to NREM sleep.57 In REM sleep, patients with obstructive/mixed impairments experienced a median 21 events/hour (AHI) more than patients with no impairment, while in NREM sleep there was a median difference of 8 events/hour. Despite this, SpO2 in both REM and NREM sleep was a median 2% lower among patients with obstructive/mixed impairments.
Patients with COPD/OSA overlap syndrome have been reported to have significantly worse outcomes than patients who have either OSA or COPD alone.26,57,59,60 As such, adherence to CPAP therapy is essential for patients with potential overlap syndrome and has been associated with improvements in quality of life, daytime symptoms of COPD, reduced hospitalisations, exacerbations and mortality.61–65 A novel aspect of the current study was the assessment of CPAP usage among patients with differing spirometric impairments. Among patients with more than 30 days of CPAP-use, those who had a restrictive impairment recorded at least 4 hr of use on a median 13% of nights, while those with no impairment did so on a median 44% of nights, and the overall adherence rate among patients with any spirometric impairment was nearly half that of patients with no impairment (21 vs 39%). These differences were attenuated in multivariate modelling, which is likely largely due to the difference in residence remoteness between patients with and without spirometric impairments44 – as 28% of no impairment patients resided in remote areas compared to 67% and 57% of patients with restrictive or obstructive spirometric impairments resided in remote/rural locality (Supplementary File B). Challenges associated with remoteness appear to be a major barrier to adherence, as identified in a recent study from our centre among Aboriginal Australian patients on CPAP, within which 21% were identified to be adherent to therapy, of whom the majority (84%) resided in outer regional areas.44 Regardless, out of the entire cohort in the current study, only 78 patients were able to have CPAP adherence assessed, which dramatically reduces the power for the multivariate modelling. Among patients with respiratory/ventilatory impairment, it has been noted that some patients may have difficulty in acclimatising, potentially due to experiencing the perception of asphyxiation and breathing impairment when first introduced to CPAP therapy.33,66 Among Aboriginal Australian patients with COPD, symptoms of cough, wheeze and sputum production are particularly prevalent and thus may present as a barrier to CPAP use.33,67 Our study findings indicate that in the combined presence of a higher burden of respiratory comorbidities alongside significant spirometry impairment among remote residing Aboriginal population may hamper long-term adherence to CPAP therapy. Hence, improving lung function may have bi-directional benefits for both respiratory and sleep related outcomes.
In the Australian context, only a single previous study (a conference abstract), involving a predominantly non-Aboriginal cohort was identified, which had a similar number of patients who undertook both a PSG and spirometry.55 In contrast to our study, the majority of patients had normal spirometry (63%), and obstruction was the predominant spirometric impairment identified (19%). Moreover, an association between FVC, FEV1 and total AHI among patients with an obstructive impairment was observed. This may indicate that the interplay between ventilatory function to sleep manifests differently among Indigenous in comparison to non-Indigenous patients. Nevertheless, in the absence of similar data published in any other Indigenous population, it is hard to generalise our study findings for other Indigenous populations in Australia or globally. Hence, further studies among populations with high risk of COPD/OSA overlap, or populations with high prevalence of respiratory comorbidities,68,69 are warranted to further explore the clinical parameters and outcomes of lung function impairment coupled with sleep-disordered breathing.
Study Limitations
The current study was conducted in the TEHS region of the NT, and as such may not be generalizable to other regions. In the absence of Aboriginal Australian specific reference norms for spirometry, the classification of patients into restrictive, obstructive or mixed impairments of spirometry has not been validated, as is highlighted by the significant presence of restrictive disease, and the low percent predicted values of FVC and FEV1. In addition, the current study did not utilise total lung capacity, which is necessary to confirm restrictive impairments. We also did not have data on current therapeutic interventions for the management of respiratory disease, including interventions such as domiciliary oxygen therapy. Although most patients had spirometry recorded within 1 month of their sleep study, for some patients the lag between spirometry and PSG was quite large, with potential for hospitalisations, medication changes or other significant changes in health between the two time points, including if CPAP therapy was initiated prior to spirometry test. Finally, spirometry was not available or performed in all patients who underwent a diagnostic PSG. Nonetheless, this is the first study to report on the relationship of lung function parameters to sleep study data in an Indigenous population, and there is room for prospective research.
Conclusions
Aboriginal Australian patients with OSA show a high prevalence of spirometry impairments. Restrictive impairments are the most common; however, obstructive/mixed impairments were associated with greater deficits in sleep outcomes. Presence of spirometry impairment may interact with remoteness to lower CPAP adherence in this population. As such, these findings may have substantial implications for the management of sleep disorders, including OSA, in this population.
Abbreviations
AHI, Apnoea-hypopnoea index; APAP, Automatic positive airway pressure; ASGS, Australian statistical geographical standard; BD, Bronchodilator; BDR, Bronchodilator responsiveness; BMI, Body mass index; CI, Confidence interval; COPD, Chronic obstructive pulmonary disease; CPAP, Continuous positive airway pressure; DRSH, Darwin respiratory and sleep health; EMR, Electronic medical record; ESS, Epworth sleepiness scale; FEV1, Forced expiratory volume in 1 s; FVC, Forced vital capacity; GLI, Global lung function initiative; GOLD, Global initiative for chronic obstructive lung disease; IQR, Interquartile range; LLN, Lower limit of normal; NREM, Non-rapid eye movement; N1/2/3, Non-rapid eye movement stage 1/2/3; NT, Northern Territory; OR, Odds ratio; OSA, Obstructive sleep apnoea; PFT, Pulmonary function test; PSG, Polysomnography; RAI, Respiratory arousal index; REM, Rapid eye movement; SAI, Spontaneous arousal index; SpO2, Oxygen saturation; TAI, Total arousal index; TEHS, Top-end health service; TST, Total sleep time; WASO, Wake after sleep onset.
Ethics Approval and Informed Consent
The project was approved by the Human Research Ethics Committee of the NT, TEHS and Menzies School of Health Research (Reference no: Human Research Ethics Committee 2019-3445) and was conducted according to the Declaration of Helsinki. As the study was retrospective in nature, individual consent was not required and was waived by the research committee.
Acknowledgment
We sincerely thank Ms. Ara Joy Perez from DRSH, Darwin Private Hospital, Darwin, Australia, for her invaluable contribution towards this study, including our other sleep/respiratory technologists at DRSH; Mr Mark Ramirez, Mr Jessie Crespo and Ms Bianca Al-Dossary, for their help with this study. We also extend our sincere appreciation to our Aboriginal health workers, especially Mr Izaak Thomas (Australian Indigenous Luritja descendent) from the respiratory chronic respiratory disease co-ordination division in approving this research addressing much-needed data in the diagnosis and management of adult Indigenous patients with respiratory disorders and for the appropriateness and respect in relation to the Indigenous context represented in this study.
Author Contributions
All authors have made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. Have drafted or written, or substantially revised or critically reviewed the article. Have agreed on the journal to which the article will be submitted. Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. Agree to take responsibility and be accountable for the contents of the article.
Disclosure
All authors declare no conflicts of interest for this study.
References
1. Australian Institute of Health and Welfare. Australian Burden of Disease Study: Impact and Causes of Illness and Death in Aboriginal and Torres Strait Islander People 2018. Canberra: AIHW; 2022.
2. Heraganahally SS, Ghimire RH, Howarth T, Kankanamalage OM, Palmer D, Falhammar H. Comparison and outcomes of emergency department presentations with respiratory disorders among Australian indigenous and non-indigenous patients. BMC Emerg Med. 2022;22:11. doi:10.1186/s12873-022-00570-3
3. Heraganahally SS, Silva SAMS, Howarth TP, Kangaharan N, Majoni SW. Comparison of clinical manifestation among Australian Indigenous and non‐indigenous patients presenting with pleural effusion. Intern Med J. 2022;52(7):1232–1241. doi:10.1111/imj.15310
4. Heraganahally SS, Howarth T, White E, Sorger L, Biancardi E, Ben Saad H. Lung function parameters among Australian aboriginal ‘apparently healthy’ adults: an Australian caucasian and Global Lung Function Initiative (GLI-2012) various ethnic norms comparative study. Expert Rev Respir Med. 2021;15:833–843. doi:10.1080/17476348.2021.1847649
5. Heraganahally SS, Wasgewatta SL, McNamara K, et al. Chronic obstructive pulmonary disease in aboriginal patients of the Northern Territory of Australia: a landscape perspective. Int J Chron Obstruct Pulmon Dis. 2019;14:2205–2217. doi:10.2147/COPD.S213947
6. Heraganahally SS, Wasgewatta SL, McNamara K, et al. Chronic obstructive pulmonary disease with and without bronchiectasis in Aboriginal Australians: a comparative study. Intern Med J. 2020;50:1505–1513. doi:10.1111/imj.14718
7. Howarth T, Saad HB, Perez AJ, Atos CB, White E, Heraganahally SS. Comparison of diffusing capacity of carbon monoxide (DLCO) and total lung capacity (TLC) between indigenous Australians and Australian caucasian adults. PLoS One. 2021;16(4):e0248900. doi:10.1371/journal.pone.0248900
8. Sze DF, Howarth TP, Lake CD, Ben Saad H, Heraganahally SS. Differences in the spirometry parameters between indigenous and non-indigenous patients with COPD: a matched control study. Int J Chron Obstruct Pulmon Dis. 2022;17:869–881. doi:10.2147/COPD.S361839
9. Seyedshahabedin MM, Howarth TP, Mo L, Biancardi E, Heraganahally SS. Flexible bronchoscopy indications and outcomes between indigenous and non-indigenous patients in the Northern Territory of Australia. Int Med J. 2022. doi:10.1111/imj.15865
10. Heraganahally SS, Howarth TP, Sorger L. Chest computed tomography findings among adult Indigenous Australians in the Northern Territory of Australia. J Med Imaging Radiat Oncol. 2022;66:337–344. doi:10.1111/1754-9485.13295
11. Heraganahally SS, Howarth TP, Lloyd A, White E, Veale A, Ben Saad H. The prevalence of bronchodilator responsiveness ‘asthma’ among adult indigenous Australians referred for lung function testing in the top end Northern Territory of Australia. J Asthma Allergy. 2022;15:1305–1319. doi:10.2147/JAA.S376213
12. Kruavit A, Fox M, Pearson R, Heraganahally S. Chronic respiratory disease in the regional and remote population of the Northern Territory top end: a perspective from the specialist respiratory outreach service. Aust J Rural Health. 2017;25:275–284. doi:10.1111/ajr.12349
13. McNicholas WT. Chronic obstructive pulmonary disease and obstructive sleep apnea: overlaps in pathophysiology, systemic inflammation, and cardiovascular disease. Am J Respir Crit Care Med. 2009;180:692–700. doi:10.1164/rccm.200903-0347PP
14. Lee R, McNicholas WT. Obstructive sleep apnea in chronic obstructive pulmonary disease patients. Curr Opin Pulm Med. 2011;17:79–83. doi:10.1097/MCP.0b013e32834317bb
15. Zhang P, Chen B, Lou H, et al. Predictors and outcomes of obstructive sleep apnea in patients with chronic obstructive pulmonary disease in China. BMC Pulm Med. 2022;22:16. doi:10.1186/s12890-021-01780-4
16. Blunden S, Yiallourou S, Fatima Y. Sleep health and its implications in First Nation Australians: a systematic review. Lancet Reg Health West Pac. 2022;21:100386. doi:10.1016/j.lanwpc.2022.100386
17. Heraganahally SS, Rajaratnam B, Silva SAAS, et al. Obstructive sleep apnoea and cardiac disease among aboriginal patients in the Northern Territory of Australia. Heart Lung Circ. 2021;30:1184–1192. doi:10.1016/j.hlc.2021.01.007
18. Benn E, Wirth H, Short T, Howarth T, Heraganahally SS. The Top End Sleepiness Scale (TESS): a new tool to assess subjective daytime sleepiness among indigenous Australian adults. Nat Sci Sleep. 2021;13:315–328. doi:10.2147/NSS.S298409
19. Heraganahally SS, Kruavit A, Oguoma VM, et al. Sleep apnoea among Australian aboriginal and non-aboriginal patients in the Northern Territory of Australia—a comparative study. Sleep. 2020;43(3):zsz248. doi:10.1093/sleep/zsz248
20. Woods CE, McPherson K, Tikoft E, et al. Sleep disorders in aboriginal and torres strait islander people and residents of regional and remote Australia. J Clin Sleep Med. 2015;15:1263–1271. doi:10.5664/jcsm.5182
21. Yiallourou SR, Maguire GP, Carrington MJ. Sleep quantity and quality and cardiometabolic risk factors in Indigenous Australians. J Sleep Res. 2021;30:e13067. doi:10.1111/jsr.13067
22. Macniven R, Richards J, Gubhaju L, et al. Physical activity, healthy lifestyle behaviors, neighborhood environment characteristics and social support among Australian aboriginal and non-aboriginal adults. Prev Med Rep. 2016;3:203–210. doi:10.1016/j.pmedr.2016.01.006
23. LaGrappe D, Massey L, Kruavit A, et al. Sleep disorders among Aboriginal Australians with Machado-Joseph disease: quantitative results from a multiple methods study to assess the experience of people living with the disease and their caregivers. Neurobiol Sleep Circadian Rhythm. 2022;12:100075. doi:10.1016/j.nbscr.2022.100075
24. Mehra S, Ghimire RH, Mingi JJ, et al. Gender differences in the clinical and polysomnographic characteristics among Australian Aboriginal patients with obstructive sleep apnea. Nat Sci Sleep. 2020;12:593–602. doi:10.2147/NSS.S258330
25. Santos MA, Aguiar M, Sacramento V, et al. Obstructive sleep apnea severity and lung function. Eur Respir J. 2018;52(62):A2522.
26. Emilsson ÖI, Sundbom F, Ljunggren M, et al. Association between lung function decline and obstructive sleep apnoea: the ALEC study. Sleep Breath Schlaf Atm. 2021;25:587–596. doi:10.1007/s11325-020-02086-1
27. Mehfooz N, Siraj F, Shabir A, et al. Spirometric abnormalities in patients with sleep-related breathing disorders. J Fam Med Prim Care. 2021;10:1009–1014. doi:10.4103/jfmpc.jfmpc_1018_20
28. Vukoja M, Milicic D, Bokan A, et al. Lung function in patients with obstructive sleep apnoea. ERJ Open Res. 2017;3(1):14.
29. Ashraf M, Shaffi SA, BaHammam AS. Spirometry and flow-volume curve in patients with obstructive sleep apnea. Saudi Med J. 2008;29:198–202.
30. Rouatbi S, Ghannouchi I, Kammoun R, Ben Saad H. The ventilatory and diffusion dysfunctions in obese patients with and without obstructive sleep apnea-hypopnea syndrome. J Obes. 2020;10:8075482. doi:10.1155/2020/8075482
31. Rotenberg BW, Murariu D, Pang KP. Trends in CPAP adherence over twenty years of data collection: a flattened curve. J Otolaryngol Head Neck Surg J. 2016;45(1):43. doi:10.1186/s40463-016-0156-0
32. Martani M, Bourahli MK, Bougrida M, Ben Saad H. Plethysmographic data and profile of North-African patients with severe obstructive sleep apnea treated with continuous positive airway pressure. Expert Rev Respir Med. 2021;15:267–275. doi:10.1080/17476348.2021.1823834
33. Woods C, Usher K, Kerr L, Ferns J, Maguire G. Barriers and enablers to successful uptake of Continuous Positive Airway Pressure (CPAP) treatment for obstructive sleep apnoea for aboriginal and torres strait islander people. J Sleep Disord Treat Care. 2016;5:1–7.
34. Heraganahally SS, Howarth T, Mo L, Sorger L, Ben Saad H. Critical analysis of spirometric patterns in correlation to chest computed tomography among adult Indigenous Australians with chronic airway diseases. Expert Rev Respir Med. 2021;15:1229–1238. doi:10.1080/17476348.2021.1928496
35. Heraganahally SS, Howarth T, Sorger L, Ben Saad H. Sex differences in pulmonary function parameters among Indigenous Australians with and without chronic airway disease. PLoS One. 2022;17:2. doi:10.1371/journal.pone.0263744
36. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14:540–545. doi:10.1093/sleep/14.6.540
37. Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS): volume 5—remoteness structure, 2011. ABS cat. no. 1270.0.55.005. Canberra: Australian Bureau of Statistics; 2013.
38. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319–338. doi:10.1183/09031936.05.00034805
39. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40:1324–1343. doi:10.1183/09031936.00080312
40. Stanojevic S, Kaminsky DA, Miller M, et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J. 2022;60(1):2101499. doi:10.1183/13993003.01499-2021
41. Heraganahally S, Howarth TP, White E, Ben Saad H. Implications of using the GLI-2012, GOLD and Australian COPD-X recommendations in assessing the severity of airflow limitation on spirometry among an Indigenous population with COPD: an Indigenous Australians perspective study. BMJ Open Respir Res. 2021;8:e001135. doi:10.1136/bmjresp-2021-001135
42. Heraganahally SS, Ponneri TR, Howarth TP, Saad HB. The effects of inhaled airway directed pharmacotherapy on decline in lung function parameters among Indigenous Australian adults with and without underlying airway disease. Int J Chron Obstruct Pulmon Dis. 2021;16:2707–2720. doi:10.2147/COPD.S328137
43. Heraganahally SS, Kerslake C, Issac S, et al. Outcome of public hospital-funded continuous positive airway therapy device for patients with obstructive sleep apnoea: an Australian perspective study. Sleep Vigil. 2020;4:195–204. doi:10.1007/s41782-020-00114-4
44. Heraganahally SS, Howarth TP, Perez AJ, et al. Acceptability, adaptability and adherence to CPAP therapy among aboriginal Australians with OSA - “The A5 study”. Sleep Med. 2023;102:147–156. doi:10.1016/j.sleep.2022.12.024
45. Heraganahally SS, Mortimer N, Howarth T, et al. Utility and outcomes among Indigenous and non-Indigenous patients requiring domiciliary oxygen therapy in the regional and rural Australian population. Aust J Rural Health. 2021;29:918–926. doi:10.1111/ajr.12782
46. Shawon MSR, Perret JL, Senaratna CV, Lodge C, Hamilton GS, Dharmage SC. Current evidence on prevalence and clinical outcomes of co-morbid obstructive sleep apnea and chronic obstructive pulmonary disease: a systematic review. Sleep Med Rev. 2017;32:58–68. doi:10.1016/j.smrv.2016.02.007
47. McNicholas WT. COPD-OSA overlap syndrome: evolving evidence regarding epidemiology, clinical consequences, and management. Chest. 2017;152:1318–1326. doi:10.1016/j.chest.2017.04.160
48. Borekci S, Hacoğlu Y, Musellim B. Investigation of obstructive sleep apnea in adult non-cystic fibrosis bronchiectasis patients. Eur Respir J. 2019;54(63):A631.
49. Erdem E, Ersu R, Karadag B, et al. Effect of night symptoms and disease severity on subjective sleep quality in children with non-cystic-fibrosis bronchiectasis. Pediatr Pulmonol. 2011;46:919–926. doi:10.1002/ppul.21454
50. Faria Júnior NS, Urbano JJ, Santos IR, et al. Evaluation of obstructive sleep apnea in non-cystic fibrosis bronchiectasis: a cross-sectional study. PLoS One. 2017;12:10. doi:10.1371/journal.pone.0185413
51. Yang X, Tang X, Cao Y, et al. The bronchiectasis in COPD-OSA overlap syndrome patients. Int J Chron Obstruct Pulmon Dis. 2020;15:605–611. doi:10.2147/COPD.S243429
52. Chang AB, Masel JP, Boyce NC, Wheaton G, Torzillo PJ. Non-CF bronchiectasis: clinical and HRCT evaluation. Pediatr Pulmonol. 2003;35:477–483. doi:10.1002/ppul.10289
53. Howarth T, Heraganahally SS, Heraganahally SS. Bronchiectasis among adult first nations Indigenous people - a scoping review. Curr Respir Med Rev. 2022;19:36–51.
54. Howarth TP, Gahreman D, Saad HB, Ng L, Heraganahally SS. Correlation of spirometry indices to chest radiology in the diagnosis of chronic airway disease among regional and rural Indigenous Australians. Intern Med J. 2023. doi:10.1111/imj.16023
55. Wang D, Smith D, Huang H, Murray N, Thomas PS. Spirometry to identify moderate to severe obstructive sleep apnea. Am J Respir Crit Care Med. 2020;201:A4142–A4142.
56. Bednarek M, Plywaczewski R, Jonczak L, Zielinski J. There is no relationship between chronic obstructive pulmonary disease and obstructive sleep apnea syndrome: a population study. Respir Int Rev Thorac Dis. 2005;72:142–149.
57. McNicholas WT, Verbraecken J, Marin JM. Sleep disorders in COPD: the forgotten dimension. Eur Respir Rev. 2013;22:365–375. doi:10.1183/09059180.00003213
58. Rennard S, Decramer M, Calverley PMA, et al. Impact of COPD in North America and Europe in 2000: subjects’ perspective of confronting COPD international survey. Eur Respir J. 2002;20:799–805. doi:10.1183/09031936.02.03242002
59. Budhiraja R, Siddiqi TA, Quan SF. Sleep disorders in chronic obstructive pulmonary disease: etiology, impact, and management. J Clin Sleep Med. 2015;11:259–270. doi:10.5664/jcsm.4540
60. Luyster FS, Wang J, Sciurba FC, Bon J. Longitudinal associations between sleep disturbance and disease severity in patients with COPD. Sleep Sci Pract. 2020;4:12. doi:10.1186/s41606-020-00046-y
61. Martinez S, Sullivan J, Pasquale C, et al. Effect of two interventional strategies on improving continuous positive airway pressure adherence in existing COPD and obstructive sleep apnea patients: the O2VERLAP study. Chronic Obstr Pulm Dis. 2022;9:394–412. doi:10.15326/jcopdf.2022.0293
62. Jaoude P, Kufel T, El-Solh AA. Survival benefit of CPAP favors hypercapnic patients with the overlap syndrome. Lung. 2014;192:251–258. doi:10.1007/s00408-014-9555-z
63. Stanchina ML, Welicky LM, Donat W, Lee D, Corrao W, Malhotra A. Impact of CPAP use and age on mortality in patients with combined COPD and obstructive sleep apnea: the overlap syndrome. J Clin Sleep Med. 2013;9:767–772. doi:10.5664/jcsm.2916
64. Sterling KL, Pépin J-L, Linde-Zwirble W, et al. Impact of positive airway pressure therapy adherence on outcomes in patients with obstructive sleep apnea and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2022;206:197–205. doi:10.1164/rccm.202109-2035OC
65. Wang TY, Lo YL, Lin SM, et al. Obstructive sleep apnoea accelerates FEV1 decline in asthmatic patients. BMC Pulm Med. 2017;17(1):55. doi:10.1186/s12890-017-0398-2
66. Sullivan J, Pasquale C, Clark B, et al. Outcomes important to patients diagnosed with both COPD and sleep apnea: findings from the O2VERLAP study focus groups. Chronic Obstr Pulm Dis. 2022;9:45–54. doi:10.15326/jcopdf.2021.0268
67. Pal A, Howarth TP, Rissel C, et al. COPD disease knowledge, self-awareness and reasons for hospital presentations among a predominately Indigenous Australian cohort: a study to explore preventable hospitalisation. BMJ Open Resp Res. 2022;9:e001295. doi:10.1136/bmjresp-2022-001295
68. Heraganahally SS, Howarth TP, Issac S, et al. Exploring the appropriateness of prescribing practice of inhaled pharmacotherapy among Aboriginal Australians in the Top End Northern Territory of Australia – a retrospective cohort study. BMJ Open Resp Res. 2023;10:e001508. doi:10.1136/bmjresp-2022-001508
69. Lindfield M, Howarth TP, Perez AJ, et al. Obstructive sleep apnoea in Aboriginal Australians: polysomnographic outcomes and symptom perception post-CPAP implementation. Sleep Adv. 2023;4:1. doi:10.1093/sleepadvances/zpad015
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Influences of Two FEV1 Reference Equations (GLI-2012 and GIRH-2017) on Airflow Limitation Classification Among COPD Patients
Wei D, Wang Q, Liu S, Tan X, Chen L, Tu R, Liu Q, Jia Y, Liu S
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2053-2065
Published Date: 2 September 2022
Prevalence of Chronic Obstructive Pulmonary Disease in an Urban Area. Changes in COPD Ten Years on

García Castillo E, Alonso Pérez T, Peláez A, Pérez González P, Soriano JB, Ancochea J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2431-2441
Published Date: 29 September 2022
Different Case Finding Approaches to Optimise COPD Diagnosis: Evidence from the RADICALS Trial
Alotaibi N, Borg BM, Abramson MJ, Paul E, Zwar N, Russell G, Wilson S, Holland AE, Bonevski B, Mahal A, George J
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1543-1554
Published Date: 20 July 2023
Prevalence and Associated Factors of Chronic Obstructive Pulmonary Disease Among Adults in Neno District, Malawi: A Cross-Sectional Analytical Study
Zaniku HR, Connolly E, Aron MB, Matanje BL, Ndambo MK, Talama GC, Munyaneza F, Ruderman T, Rylance J, Dullie LW, Lalitha R, Banda NPK, Muula AS
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:389-401
Published Date: 5 February 2024
Reliability of Pulmonary Function Tests in Patients with Chronic Obstructive Pulmonary Disease
Arslan F, Şen E, Şirin B, Köktürk N, Ulubay G, Aydogan Eroglu S, Gemicioglu B, Sönmez Ö, Şerifoğlu İ, Dilektasli AG, Öztürk Şahin B, Doğan İ, Gürhan N, Günen H, Ensen N
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:554115
Published Date: 21 January 2026