")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Prevalence of Chronic Obstructive Pulmonary Disease in an Urban Area. Changes in COPD Ten Years on
Authors García Castillo E , Alonso Pérez T, Peláez A , Pérez González P, Soriano JB, Ancochea J
Received 10 June 2022
Accepted for publication 9 September 2022
Published 29 September 2022 Volume 2022:17 Pages 2431—2441
DOI https://doi.org/10.2147/COPD.S377140
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Russell
Elena García Castillo,1– 4 Tamara Alonso Pérez,1– 4 Adrián Peláez,1– 3 Patricia Pérez González,1,2,4 Joan B Soriano,1– 3 Julio Ancochea1– 4
1Pulmonary Department, Hospital Universitario La Princesa, Instituto de Investigación Sanitaria La Princesa, Madrid, Spain; 2School of Medicine, Universidad Autónoma de Madrid (UAM), Madrid, Spain; 3Centro de Investigación Biomédica en Red de Enfermedades Respiratorias (CIBERES), Instituto de Salud Carlos III, Madrid, Spain; 4Cátedra UAM-GSK “Respira Vida”, Madrid, Spain
Correspondence: Elena García Castillo, Pulmonology Department, Hospital Universitario La Princesa, C/ Diego de León, 62, Madrid, CP: 28006, Spain, Tel +34 91 520 22 77, Fax +91-520-26-72, Email [email protected]
Purpose: The prevalence of Chronic obstructive pulmonary disease (COPD) in Spain has been evaluated in the last ten years by EPISCAN in 2007 and EPISCAN II in 2017. This study describes changes in the prevalence of COPD in an urban region of Spain in the last 10 years, its risk factors and underdiagnosis.
Patients and Methods: Participants from the Autonomous Community of Madrid (Spain) were selected from both studies up to the age of 80 years. A descriptive analysis of their sociodemographic and clinical characteristics, as well as by gender, was conducted. COPD was defined by a post-bronchodilator ratio < 0.70.
Results: The prevalence of COPD in the Autonomous Community of Madrid increased non-significantly from 11.0% (95% CI: 8.9– 13.5%) to 12.1% (95% CI: 9.6– 15.1, p=0.612). However, the prevalence by gender showed an increase in women (5.6% to 14.7%, p< 0.001) and a decrease in men (17.6% to 9.8%, p=0.08). Underdiagnosis was reduced from 81.0% to 67.9% (p=0.006), although with greater underdiagnosis in women (86.4% in EPISCAN and 100% in EPISCAN II). Smoking was higher in men than in women in EPISCAN (31.2% vs 23.0%, p< 0.01) but with no differences by gender in EPISCAN II (25.5% men vs 26.0% women, p=0.146). Age, smoking, low BMI, and a sedentary lifestyle were consistently associated with COPD.
Conclusion: In 10 years in Madrid, there have been no changes in the global prevalence of COPD, but there have been important changes in women, with an increase in its prevalence, smoking habit and underdiagnosis.
Keywords: COPD, prevalence, Madrid, spirometry
Introduction
Chronic obstructive pulmonary disease (COPD) is a major health problem, which has gone from being the fifth leading cause of death in the world in the 1990s to the third leading cause of death today. In 2019, COPD caused 3.2 million deaths globally, and this number could increase to 4.4 million by 2040.1
Because of the major impact it has on morbidity, mortality, and related healthcare spending, it is particularly important to determine the prevalence of the disease periodically. So far, a large body of research has been published on this subject, albeit with major differences in the methodologies used, the diagnostic criteria established, and the geographical framework, making it difficult to establish comparisons between the different studies.2 This major variability is reflected in studies such as PLATINO3 carried out in different Latin American cities, with rates of prevalence ranging from 7.8% to 19.7%, or the BOLD study,4 carried out in several continents, which also revealed broad variability in prevalence rates in the different participating countries.
In Spain, the prevalence of the disease has been evaluated through three major population-based epidemiological studies, IBERPOC,5 EPISCAN6 and EPISCAN II.7 The last two have the advantage of having been carried out with the same methodology, protocol, and ten years apart. A direct comparison of the final results of the two studies has revealed increased prevalence, the broad geographical variability of the results, and the significant underdiagnosis of the disease. In EPISCAN II, Madrid was the only region of Spain in which a higher prevalence of COPD is detected among women than men. Although the prevalence of the disease in women is known to be increasing, this regional peculiarity has not been described in other epidemiological studies in the West.8 Therefore, we believe that it may be of interest to know not only the prevalence of the disease, but also the trend observed in the disease in one of the most populated urban regions of Spain, in order to evaluate whether the prevention and treatment strategies applied in the healthcare setting are the right ones and whether there are opportunities for improvement.
Therefore, the objective of our study has been to determine changes in the prevalence of COPD in the region of Madrid over the 10-year period between the two EPISCAN surveys, risk factors for COPD, and the percentage of underdiagnosis of this disease.
Materials and Methods
EPISCAN and EPISCAN II are two observational, population-based, multi-centre, national epidemiological studies, conducted in 2007 and 2017, respectively. The methodology of both studies has been published previously, with the main characteristics summarised in Table 1.9,10 EPISCAN was conducted in eleven centres in Spain with the participation of two teaching hospitals in the region of Madrid: Hospital Universitario de La Paz and Hospital Universitario de La Princesa. The first EPISCAN study randomly selected participants aged between 40 and 80 years old, using two-stage stratified sampling according to the areas closest to the participating centres. EPISCAN II was carried out ten years later with the inclusion of nineteen hospitals, but just one from the Region of Madrid, the Hospital Universitario la Princesa, but with the same sample size. In the case of EPISCAN II, there was no upper age limit, applying two-stage stratified sampling according to the areas closest to the hospitals.
Forced spirometry with bronchodilator test was performed using a pneumotachograph according to standardized procedures and reference values indicated in Table 1. Different guidelines used in both studies were comparable. Each spirometry was reviewed, and only spirograms that met acceptability and reproducibility criteria were included.
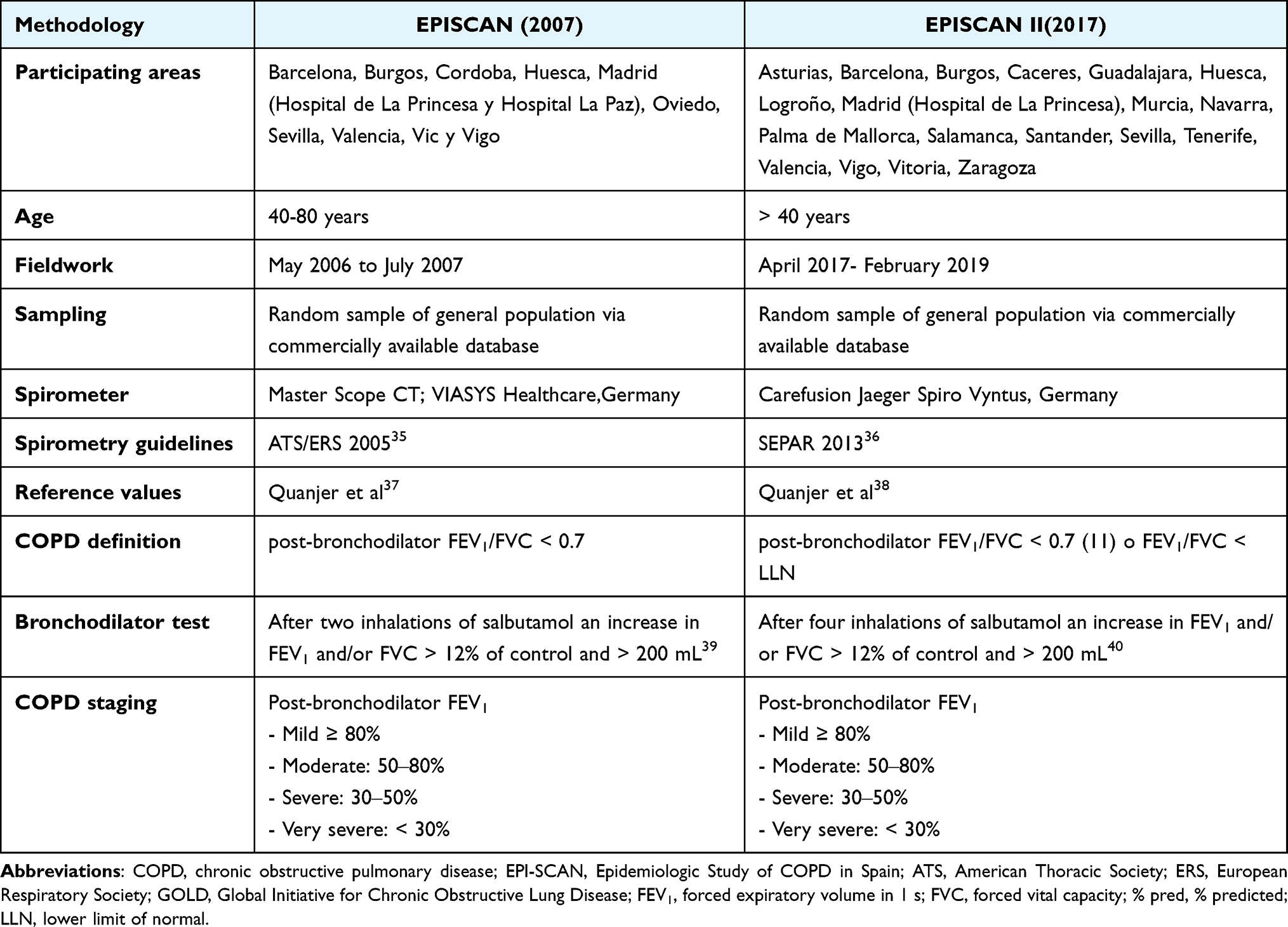 |
Table 1 Comparison of Study Designs Used in 2007 and 2017 |
As shown in Table 1, the definitions of COPD were the same.11 Similarly, both studies classified participants according to the lower limit of normal (LLN)12 to minimise potential false-negatives in the younger population and false-positives in the older population.13 Identical questions were asked about previous medical diagnoses compatible with COPD, pharmacological treatments used, and clinical questionnaires were applied to determine underdiagnosis of the disease.
Both studies were approved by their respective ethics committees, and all participants signed informed consent. In order to carry out this sub-study, participants from the Region of Madrid were analysed from the primary databases. The two data sets were then merged by matching the identical variables and discarding those that did not match or had a different definition. The recommendations of the STROBE declaration for observational studies have been followed in the preparation of the study.14 The study has also been approved by the scientific committees of EPISCAN and EPISCAN II, and has been carried out under the researcher’s own initiative and without any funding. Flowchart of the study is shown in Figure 1 Supplementary Material.
Statistical Analysis
An initial descriptive comparative analysis was made between the main sociodemographic characteristics and clinical variables of both studies, as well as by gender. Because EPISCAN II included patients with a different age range than EPISCAN, only those participants within the same age range (40–80 years) were included in the comparative analysis. so that both populations were as similar as possible. The mean and standard deviation (SD) of the quantitative variables were calculated, using the Shapiro–Wilk and Kolmogorov–Smirnov tests to confirm the normality of the continuous variables. Homoscedasticity was verified using Levene’s test.15 When the distributions were normal and homoscedastic, a parametric test (t-test) was performed, and when one of these two assumptions was not met, a non-parametric test (Mann–Whitney-Wilcoxon test) was performed. In the case of qualitative variables, proportions were compared using the χ2 test or Fisher’s exact test, whenever necessary. Prevalences were calculated as percentages with a 95% CI.
Risk factors for COPD were analysed using a crude and multivariate logistic regression model. In addition, a mediation analysis was conducted for each study (EPISCAN and EPISCAN II) with the dependent variable COPD prevalence and the independent variable gender, using smoking status (smokers and ex-smokers) as a mediator. In all comparisons, p <0.05 was considered statistically significant. All analyses were performed using R (R Development Core Team, 2015) statistical software.
Results
The main demographic characteristics and clinical variables of the participants in the 2007 and 2017 studies are compared in Table 2. The subgroup of EPISCAN II participants aged 40 to 80 is shown in a separate column, with all of the study comparisons made with this subgroup. Compared with the participants in the first EPISCAN survey, EPISCAN II participants were found to have a higher mean age (56.9 ± 10.7 vs 58.7 ± 9.4 years), a higher percentage of male participants, taller, lower body mass index, and a higher level of education (p<0.05). No statistically significant differences were found in terms of occupation or smoking habits, although the mean number of pack-years was significantly higher among EPISCAN II participants (31.5 ± 22.7 pack-years vs 27.1 ± 22.4 pack-years, p=0.001). With regard to lung function, small significant differences were observed in the post-bronchodilator forced expiratory volume measurements.
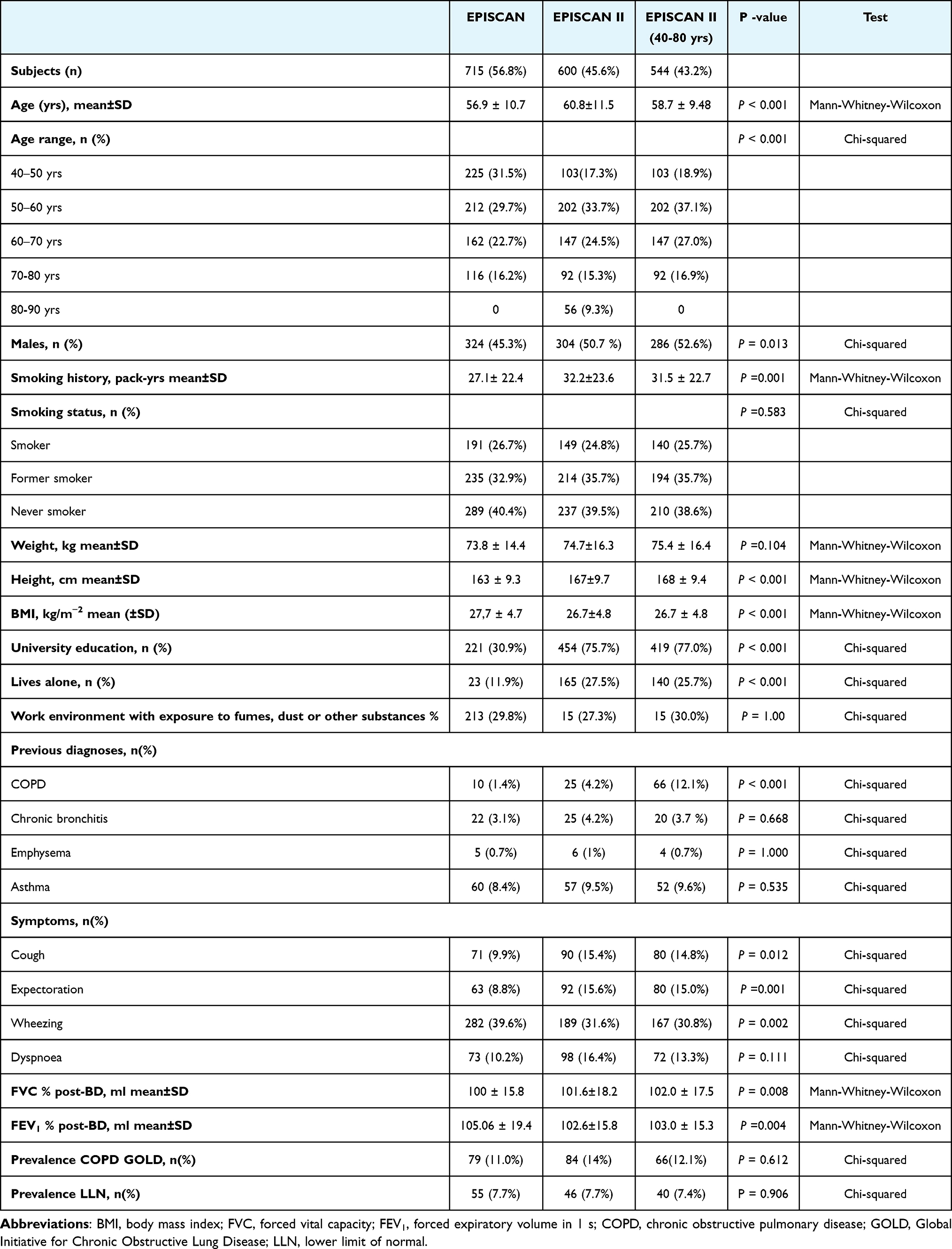 |
Table 2 Demographic and clinical characteristics of participants in 2007 and 2017 in the Community of Madrid |
The overall prevalence of COPD in the region of Madrid according to GOLD showed no statistically significant differences, although a numerical increase of 1.1 percentage points was observed: 11% (CI 95%: 8.9–13.5%) in EPISCAN, compared to 12.1% (95% CI: 9.6–15.1%) in EPISCAN II, not statistically significant (p = 0.612). The percentages when estimating prevalence by LLN were very similar: 7.7% (CI 95%: 5.9–9.8) in EPISCAN compared to 7.4% in EPISCAN II (95% CI: 5.4–9.8), p = 0.906.
However, when analysing prevalence changes by gender, marked differences were found with an increase in prevalence among women from 5.6% to 14.7% (p < 0.001) and a decrease among men from 17.6% to 9.8% (p = 0.008). Similarly, according to LLN, prevalence among women increased from 4.9% to 9.7% (p<0.025) and among men it decreased from 11.1% to 5.2% (p<0.014) (Figure 1). The characteristics of the participants in both studies analysed from a gender perspective is shown in Table 1 Supplementary Material.
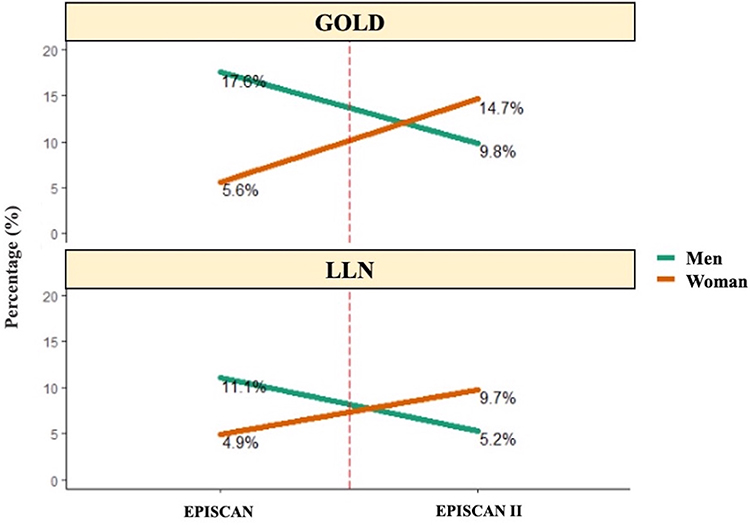 |
Figure 1 Changes in COPD prevalence from 2007 to 2017, by sex in Madrid. Abbreviations: GOLD, Global Initiative for Chronic Obstructive Lung Disease; LLN, lower limit of normal. |
Evaluating these changes by age group (Figure 2), EPISCAN shows an increase in the prevalence of COPD among men, both by GOLD (p <0.001) and by LLN (p <0.002). In EPISCAN II, there was also an increase in prevalence with age according to the GOLD criteria (p < 0.013) and according to LLN (p = 0.06), except in the age group of 50 to 59 years old, when there was a small decrease in prevalence. With regard to women, EPISCAN also showed an upward trend, although not as significant according to the GOLD criteria (p =0.406), being particularly worrying among younger age groups. According to LLN, the highest percentage of prevalence was observed in the first age group, with a subsequent decrease (p = 0.958). In EPISCAN II, the trend with age is not so clear, with a small decrease in the group aged 60 to 69 years and a subsequent upward swing in the older age brackets according to GOLD (p=0.181) and according to LLN (p=0.264).
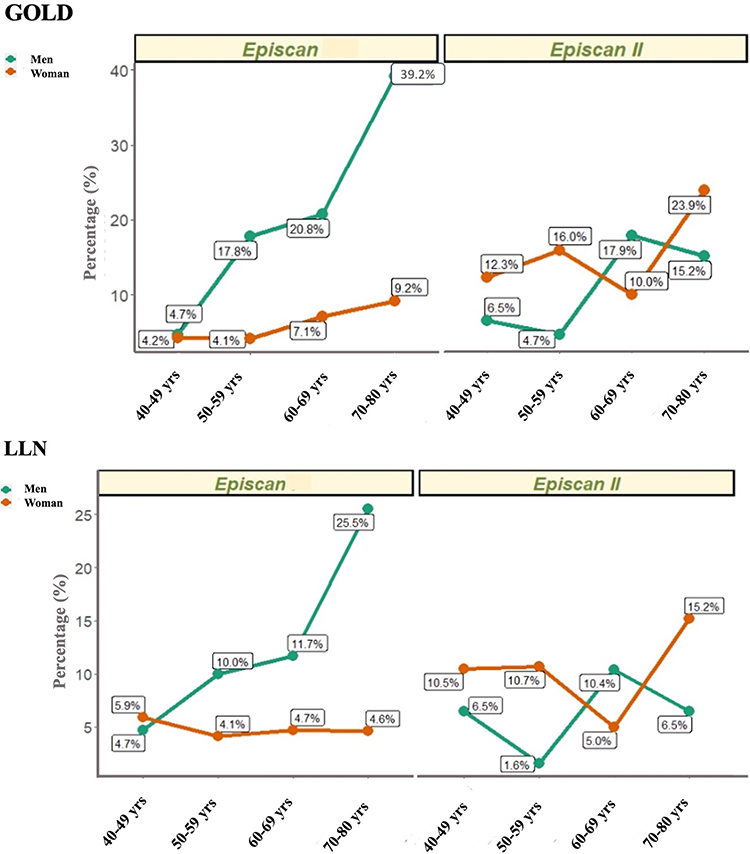 |
Figure 2 Changes in COPD prevalence from 2007 to 2017, by sex and age in Madrid. Abbreviations: GOLD, Global Initiative for Chronic Obstructive Lung Disease; LLN, lower limit of normal. |
In terms of comparison of smoking habits, there were no statistically significant differences between the two studies, although there were differences found according to the analysis by gender (Figure 3). In EPISCAN, a lower percentage of smokers was found among women compared to men (23.0% vs 31.2%, p < 0.01), but in EPISCAN II, this proportion was equal for both genders (26.0% vs 25.5%, p =0.146). Also, in EPISCAN, the percentage of non-smokers was significantly higher among women than men (51.9% vs 26.5%, p<0.001), decreasing significantly and balancing out in EPISCAN II (36.7% vs 40.7%, p = 0.518).
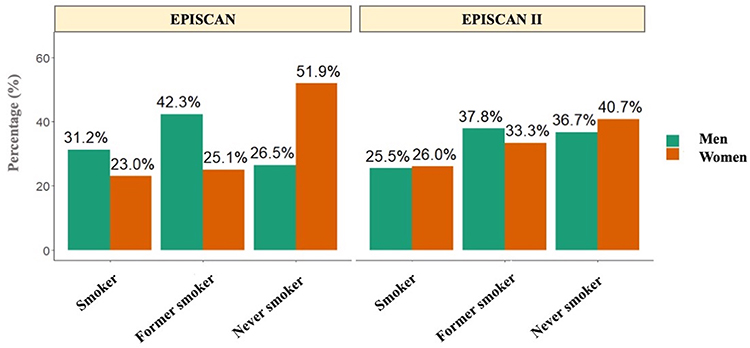 |
Figure 3 Smoking habits by sex in EPISCAN and EPISCAN II subjects. |
In addition, a mediation analysis showed that gender (female) on COPD diagnosis was fully mediated by smoking habit (smoker or former smoker). However, in EPISCAN II, compared to EPISCAN, regression coefficient between gender and smoking habit decreased and was not significant, fact that might suggest a gender changed in smoking habit (Figure 2 Supplementary Material).
The global underdiagnosis of COPD based on the criteria proposed by GOLD decreased from 81% in EPISCAN to 67.9%% in EPISCAN II (p =0.006). Underdiagnosis according to LLN also showed a decrease although not as striking as it is according to GOLD criteria (74.5% EPISCAN vs 69.6% EPISCAN II). When analysing these data by gender, clear differences were again found. Among women, an increase in underdiagnosis was observed, reaching 100% in EPISCAN II (p=0.046), and among men a non-significant percentage decrease was found (78.9% vs 67.9%, p=0.085).
For all the EPISCAN data as a whole, we analysed the variables associated with the presence of COPD (Table 3). In the bivariate analysis, age over 60, male gender, smoking, lack of education, BMI <21, and a sedentary lifestyle were associated with an increased risk of COPD. In the multivariate analysis, the direction and magnitude of the associations were maintained except for the level of education.
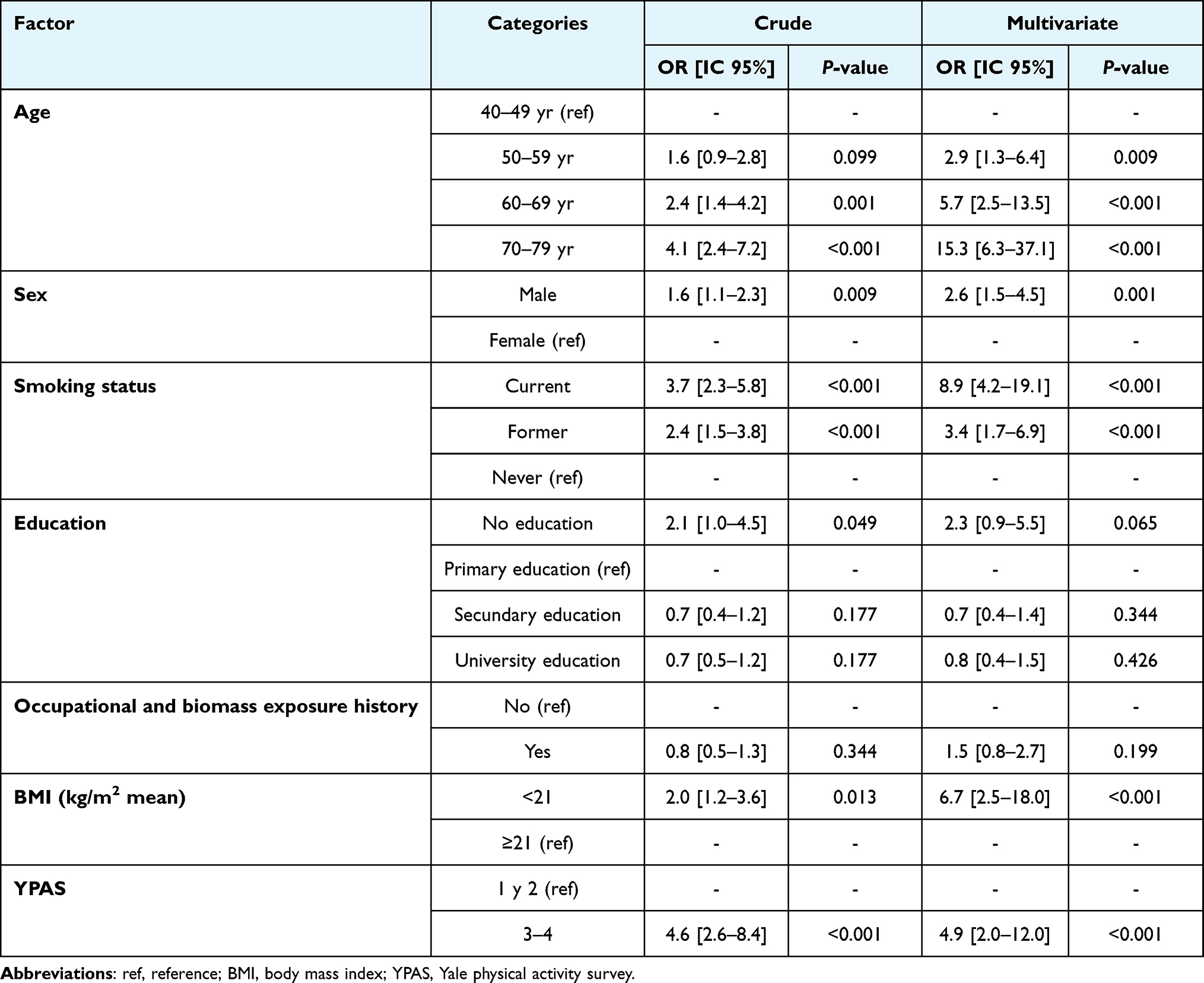 |
Table 3 Factors associated with COPD |
Finally, we performed the same analysis splitting by study (Table 2 Supplementary Material) and gender (Table 3 Supplementary Material) variables to show how the risk factors differ between EPISCAN and EPISCAN II and between women and men. In the bivariate analysis for study, gender and occupational and biomass exposure history showed a different direction and magnitude between EPISCAN and EPISCAN II, which only gender differed, also for multivariate analysis. While, in the bivariate and multivariate analyses for gender analysis, university education and occupational and biomass exposure history, showed a different direction and magnitude between genders.
Discussion
The results of this study have shown that the overall prevalence of COPD in the population aged 40 to 80 in the region of Madrid did not undergo any major changes between 2007 and 2017, and there has been a non-statistically significant increase from 11% to 12.1%. However, these similar figures at the global level, mask important differences that emerge when analysed from a gender perspective: among women, a significant increase in prevalence and underdiagnosis has been observed, while among men the trend has been the opposite, with a decrease in prevalence and no differences in underdiagnosis. Age, smoking, and low weight of participants have been the most associated risk factors for the disease.
Disease prevalence has been defined on the basis of spirometric criteria as in other epidemiological studies.9,10,16 It is well known that prevalence may vary according to the spirometric criteria used, with higher percentages obtained according to GOLD among older and younger participants. The definition of COPD in our study was established according to the GOLD criteria in order to draw comparisons with most epidemiological studies published to date. However, prevalence according to LLN has also been evaluated, with younger participants (40–50 years) presenting a higher prevalence of this disease defined by this criterion than by the fixed post-bronchodilator ratio established by GOLD.17,18
In the region of Madrid prevalence of COPD only increase 1.1 percentage points between 2007 and 2017. It could be because the geographical setting, population, design and methodology of EPISCAN and EPISCAN II was very similar, unlike other epidemiological studies carried out in this regard. Prevalence has been higher than the national average published in EPISCAN II7 and unlike in previous studies in which there appeared to be a downward trend.16 There are possible factors that have been previously described in the literature that could explain this higher prevalence.19–21 The first of these is smoking, with the prevalence of smokers in Madrid being higher than the national average observed in EPISCAN II.7 Another factor to be taken into account is environmental pollution and the urban area where the study was carried out. The Hospital Universitario de la Princesa is located in the city centre, in an urban environment under the direct influence of road traffic and, therefore, with greater exposure to environmental pollution than other regions included in EPISCAN II.
The influence of these factors has also been analysed as a possible explanation of the slight increase in prevalence in the region itself between the two studies, with smoking habits being very similar in 2007 and 2017. With regard to environmental pollution, the levels analysed by the different automatic measurement stations as part of Madrid City Council’s air quality monitoring network were similar between the two studies. The levels of suspended particles (PM10 and PM2.5, particles smaller than 10 and 2.5 microns, respectively) fell slightly between 2007 and 2017, but in contrast, despite legislative changes in this area in recent years, in 2017 there was a notable increase in levels of nitrogen dioxide pollution (N02) influenced by prevailing weather conditions and possibly by a surge in traffic. Although the two EPISCAN participating centres have a different geographical location, the measurements published by the stations closest to the two hospitals did not show any major differences.22,23
In relation to the analysis by gender, there has been an important change in the tendency of the disease that had been detected in previous years. In EPISCAN II study, Madrid was the only region where prevalence among women exceeded the level among men. The systematic review published by Ntritsos et al8 found an overall prevalence among women of 6.2% with clear geographical variations, reaching up to 8.4% in urban populations. This factor, together with a greater smoking habit, ageing and higher socioeconomic status among women in Madrid in 2017, could explain this higher prevalence detected in the region. Additionally, mediation analysis using smoking habit as mediator, dependent variable COPD prevalence and the independent variable gender showed that COPD diagnosis was fully mediated by smoking habit (smoker or former smoker) and a gender change in smoking habit between EPISCAN and EPISCAN II which could be related to the increased prevalence of COPD in the female gender.
Changes have also been observed in relation to smoking by gender. Among men, the number of smokers has declined in line with the downward trend detected since the late 80s. In contrast, the percentage of smokers has increased in women and is higher than men, even among participants in the lowest age bracket, which is more worrying. This phenomenon is consistent with previous reports on changes in tobacco use in Spain and other developed countries where, due to the fact that women are taking up smoking at a younger age, the difference in habit between the two genders has narrowed.24 It is known that tobacco use among women is influenced by socioeconomic status, with higher prevalence figures in countries with higher per capita income. In Europe, in 2018, the prevalence of women smokers was 19%, the highest in the world, with the overall prevalence being 9%25 and a higher percentage detected in our study in 2017. This phenomenon may be due to the fact that in Madrid a decrease in the prevalence of smoking in women was detected up to 2014. From that year onwards, consumption increased again, and it is in the population subgroup aged 45–60 that this sustained increase has been evident, due to the fact that the cohorts of young smokers from the 1980s and 1990s have now reached this age bracket.26 The greater susceptibility of women to tobacco smoke is well known, with a higher impact on the deterioration of lung function in women, even with lower cumulative consumption and at younger ages.27,28 This phenomenon could explain why in our study, despite the lower PYI (pack-year index) in women, the prevalence of the disease has been higher than among men.
The underdiagnosis of COPD is similar in both studies: 73% in EPISCAN and 74.7%% in EPISCAN II, which could reflect a stagnation in the diagnosis of the disease and the inadequacy of strategies to modify it. This problem is even more pronounced among women. Our study found that although women reported a higher percentage of symptoms (cough, expectoration, and dyspnoea) than men, none of the participants included in the 2017 study with obstructive spirometry had a previous diagnosis of COPD. For this reason, the rate of underdiagnosis among women reached 100%. This difference in underdiagnosis by gender has been demonstrated in previous studies, especially in European cohorts,29 with several causes associated with this high level of underdiagnosis. The perception of the disease as a pathology associated with men, the high level of public ignorance surrounding the disease, and the anxiety and depression that sometimes lead to a different perception of dyspnoea among women are several of the factors described.30,31
Older age, smoking, a sedentary lifestyle, and especially BMI < 21 are the variables that present a more consistent association with COPD. This relationship has already been described in previous studies, and the important role of malnutrition in these patients is known with underweight individuals with lower lung function compared to those with higher BMI ranges.32,33 A possible explanation for this inverse correlation between BMI and lung function decline is the increasing resting energy consumption, non-respiratory skeletal muscle atrophy due to decreased peripheral oxygen availability and systemic inflammation.
One of the limitations of our study is the establishment of a COPD diagnosis by means of spirometric criteria. The clinical diagnosis of the disease is based on risk exposure, clinical criteria, and bronchial obstruction34 since the potential causes of non-reversible spirometric obstruction are different. However, to date all epidemiological studies are based on spirometric criteria, which have been used in EPISCAN, EPISCAN II and GOLD, in order to compare their results. Another limitation is the small sample size, having focused the study on a single region and an urban setting. As strengths, it should be noted that, by comparing studies conducted in the same geographical region using practically the same methodology, it has been possible to eliminate the major variability that exists in most of the studies carried out so far.
In conclusion, the prevalence of COPD in the Region of Madrid has not varied significantly in the ten-year period between the EPISCAN and EPISCAN II surveys, although there has been a change in the trend of the disease, with a higher prevalence, underdiagnosis and increased smoking among women in recent years. That is why greater efforts should be made to improve diagnosis, promote awareness of the disease, and implement greater measures to prevent and control smoking, especially among women.
Ethics Approval
The study was approved by the Ethics Committee of the Hospital La Princesa (Madrid). Register number: 2899. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Acknowledgments
We thank the staff and participants in EPI-SCAN and EPISCAN II studies and the scientific committee of both studies. We particularly thank Mónica Sarmiento and Neus Canal (IMS Health Economics and Outcomes Research, Barcelona, Spain) for the monitoring and data management of the studies. We also sincerely thank the scientific committee of IBERPOC: Sobradillo V, Jiménez CA, Gabriel R. Viejo JL, Masa JF, Fernández-Faue L, Villasante C.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The EPI-SCAN study was funded by an unrestricted grant from GlaxoSmithKline Spain. EPISCAN II was a sponsored study from GlaxoSmithKline Spain registered in ClinicalTrials.gov Identifier: NCT01122758. All sponsors played no role in the study design, data collection, data analysis, data interpretation, or writing the original reports.
Disclosure
EGC has received speaker fees from GlaxoSmithKline, Chiesi and Pfizer. TAP has received speaker fees from AstraZeneca, GlaxoSmithKline, Chiesi, Novartis and Pfizer. JA has received company training fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline and Novartis and speaker fees from AstraZeneca, GlaxoSmithKline, Boehringer Ingelheim, Roche and Faes Farma. All other authors declare no conflicts of interest in this work.
References
1. Soriano JB, Kendrick PJ, Paulson KR; GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
2. Blanco I, Diego I, Bueno P, Casas-Maldonado F, Miravitlles M. Geographic distribution of COPD prevalence in the world displayed by Geographic Information System maps. Eur Respir J. 2019;54(1):1900610. doi:10.1183/13993003.00610-2019
3. Menezes AMB, Perez-Padilla R, Jardim JB, et al. Chronic obstructive pulmonary disease in five Latin American cities (the PLATINO study): a prevalence study. Lancet. 2005;366(9500):1875–1881. doi:10.1016/S0140-6736(05)67632-5
4. Buist AS, McBurnie MA, Vollmer WM, et al. International variation in the prevalence of COPD (The BOLD Study): a population-based prevalence study. Lancet. 2007;370(9589):741–750. doi:10.1016/S0140-6736(07)61377-4
5. Sobradillo V, Miravitlles M, Jiménez CA, et al. Epidemiological study of chronic obstructive pulmonary disease in Spain (IBERPOC): prevalence of chronic respiratory symptoms and airflow limitation. Arch Bronconeumol. 1999;35(4):159–166. doi:10.1016/S0300-2896(15)30272-6
6. Miravitlles M, Soriano JB, Garcia-Rio F, et al. Prevalence of COPD in Spain: impact of undiagnosed COPD on quality of life and daily life activities. Thorax. 2009;64(10):863–868. doi:10.1136/thx.2009.115725
7. Soriano JB, Alfageme I, Miravitlles M, et al. Prevalence and determinants of COPD in Spain: EPISCAN II. Arch Bronconeumol. 2021;57(1):61–69. doi:10.1016/j.arbres.2020.07.024
8. Ntritsos G, Franek J, Belbasis L, et al. Gender-specific estimates of COPD prevalence: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2018;13:1507–1514. doi:10.2147/COPD.S146390
9. Ancochea J, Badiola C, Duran-Tauleria E, et al.. The EPI-SCAN Survey to Assess the Prevalence of Chronic Obstructive Pulmonary Disease in Spanish 40-to-80-Year-Olds: Protocol Summary Arch Bronconeumol. 2009;45(1):41–47. doi:10.1016/j.arbres.2008.06.001
10. Alfageme I, de Lucas P, Ancochea J, et al. 10 years after EPISCAN: a new study on the prevalence of COPD in Spain -A summary of the EPISCAN II protocol. Arch Bronconeumol. 2019;55(1):38–47. doi:10.1016/j.arbres.2018.05.011
11. Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532–555. doi:10.1164/rccm.200703-456SO
12. Pellegrino R. Interpretative strategies for lung function tests. Eur Respir J. 2005;26(5):948–968. doi:10.1183/09031936.05.00035205
13. Swanney MP, Ruppel G, Enright PL, et al. Using the lower limit of normal for the FEV1/FVC ratio reduces the misclassification of airway obstruction. Thorax. 2008;63(12):1046–1051. doi:10.1136/thx.2008.098483
14. STROBE. Strengthening the reporting of observational studies in epidemiology. Available at: https://www.strobe-statement.org/.
15. Sokal RR, Rohlf FJ. Biometry: The Principles and Practice of Statistics in Biological Research.
16. Soriano JB, Ancochea J, Miravitlles M, et al. Recent trends in COPD prevalence in Spain: a repeated cross-sectional survey 1997–2007. Eur Respir J. 2010;36(4):758–765. doi:10.1183/09031936.00138409
17. Alabi FO, Alkhateeb HA, DeBarros KM, et al. The heterogeneity of COPD patients in a community-based practice and the inadequacy of the global initiative for chronic obstructive lung disease criteria: a real-world experience. Chronic Obstr Pulm Dis J COPD Found. 2021;8(3):396–407. doi:10.15326/jcopdf.2021.0229
18. Liu S, Zhou Y, Liu S, et al. Clinical impact of the lower limit of normal of FEV1/FVC on detecting chronic obstructive pulmonary disease: a follow-up study based on cross-sectional data. Respir Med. 2018;139:27–33. doi:10.1016/j.rmed.2018.04.011
19. Rabe KF, Watz H. Chronic obstructive pulmonary disease. Lancet. 2017;389(10082):1931–1940. doi:10.1016/S0140-6736(17)31222-9
20. Raherison C, Girodet P-O. Epidemiology of COPD. Eur Respir Rev. 2009;18(114):213–221. doi:10.1183/09059180.00003609
21. Boldo E, Querol X. [New European policies for air pollution control: A step forward in improving public health?].Gac Sanit. 2014;28(4):263–266. doi:10.1016/j.gaceta.2014.04.003
22. Ecologists in Action, Air quality in the city of Madrid; 2017. Available at: https://www.ecologistasenaccion.org/35593/2017-aumenta-la-contaminacion-del-aire-madrid/.
23. Report of the General Directorate of Quality, Control and Environmental Evaluation. Department of Air Quality. Air quality. Daily data years 2001 to 2021. Available at: https://www.mambiente.madrid.es/opencms/calaire/Publicaciones/memoria_2007.html.
24. Feliu A, Martínez C, Fernández E. Lights and shadows for public health: A critical analysis of the tobacco legislation in Spain. Gac Sanit. 2022;36(1):48–52. doi:10.1016/j.gaceta.2021.07.001
25. WHO global report on trends in prevalence of tobacco use 2000–2025, Tercera edición. Geneva, Switzerland: World Health Organization; 2019. ISBN: 978-92-4-000003-2.
26. Epidemiology Service. Results of the Comprehensive Smoking Surveillance System (VITa). Report 2021. Available from: https://www.comunidad.madrid/sites/default/files/doc/sanidad/epid/informe_tabaco_vita_2021.pdf.
27. Alonso T, Sobradillo P, de Torres JP. Chronic obstructive pulmonary disease in Women. Is it Different? Arch Bronconeumol. 2017;53(4):222–227. doi:10.1016/j.arbres.2016.10.008
28. Jenkins C. Differences between men and women with chronic obstructive pulmonary disease. Clin Chest Med. 2021;42(3):443–456. doi:10.1016/j.ccm.2021.06.001
29. Ho T, Cusack RP, Chaudhary N, Satia I, Kurmi OP. Under- and over-diagnosis of COPD: a global perspective. Breathe. 2019;15(1):24–35. doi:10.1183/20734735.0346-2018
30. Soriano JB, Calle M, Montemayor T, Álvarez-Sala JL, Ruiz-Manzano J, Miravitlles M. The General Public's Knowledge of Chronic Obstructive Pulmonary Disease and Its Determinants: Current Situation and Recent Changes. Arch Bronconeumol. 2012;48(9):308–315. doi:10.1016/j.arbres.2012.04.008
31. Jia G, Lu M, Wu R, Chen Y, Yao W. Gender difference on the knowledge, attitude, and practice of COPD diagnosis and treatment: a national, multicenter, cross-sectional survey in China. Int J Chron Obstruct Pulmon Dis. 2018;13:3269–3280. doi:10.2147/COPD.S176173
32. Cabrera López C, Juliá Serdá G, Cabrera Lacalzada C, et al. Prevalence of Chronic Obstructive Pulmonary Disease in the Canary Islands. Archivos de bronconeumologia. 2014;50(7):272–277. doi:10.1016/j.arbres.2013.12.006
33. Keogh E, Mark Williams E. Managing malnutrition in COPD: a review. Respir Med. 2021;176:106248. doi:10.1016/j.rmed.2020.106248
34. Miravitlles M, Soler-Cataluña JJ, Calle M, et al. Spanish Guidelines for Management of Chronic Obstructive Pulmonary Disease (GesEPOC) 2017. Pharmacological Treatment of Stable Phase Arch Bronconeumol. 2017;53(6):324–335. doi:10.1016/j.arbres.2017.03.018
35. Miller MR. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
36. García-Río F, Calle M, Burgos F, et al. Spirometry Arch Bronconeumol. 2013;49(9):388–401. doi:10.1016/j.arbres.2013.04.001
37. Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault J-C. Lung volumes and forced ventilatory flows. Eur Respir J. 1993;6(16):5–40. doi:10.1183/09041950.005s1693
38. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324–1343. doi:10.1183/09031936.00080312
39. Celli BR, MacNee W, Agusti A, et al. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23(6):932–946. doi:10.1183/09031936.04.00014304
40. Brusasco V. Coming together: the ATS/ERS consensus on clinical pulmonary function testing. Eur Respir J. 2005;26(1):1–2. doi:10.1183/09031936.05.00034205
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.