Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Lobar Yttrium-90 Radioembolization with BSA-Based Dosimetry for Unresectable Hepatocellular Carcinoma: Baseline Vascularity Predicts Responders to the Combination with Targeted Therapy or Immune Checkpoint Inhibition
Authors Lüdemann WM ![]() , Kahn J, Herzler P, Collettini F, Savic LJ
, Kahn J, Herzler P, Collettini F, Savic LJ ![]() , Mohr R
, Mohr R ![]() , Fehrenbach U, Auer TA
, Fehrenbach U, Auer TA ![]() , Gebauer B, Amthauer H, Wieners G
, Gebauer B, Amthauer H, Wieners G
Received 6 August 2025
Accepted for publication 19 December 2025
Published 3 March 2026 Volume 2025:12 Pages 1—13
DOI https://doi.org/10.2147/JHC.S553808
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hop Tran Cao
Willie M Lüdemann,1 Johannes Kahn,2 Paul Herzler,3 Federico Collettini,1 Lynn J Savic,1 Raphael Mohr,4 Uli Fehrenbach,1 Timo Alexander Auer,1 Bernhard Gebauer,1 Holger Amthauer,3 Gero Wieners5
1Department of Diagnostic and Interventional Radiology, Charité Universitätsmedizin, Berlin, Germany; 2Department of Diagnostic and Interventional Radiology, Health and Medical University Potsdam, Potsdam, Germany; 3Department of Nuclear Medicine, Charité Universitätsmedizin, Berlin, Germany; 4Department of Hepatology and Gastroenterology, Charité Universitätsmedizin, Berlin, Germany; 5Department of Radiology, Medical University Lausitz-Carl Thiem, Cottbus, Germany
Correspondence: Willie M Lüdemann, Email [email protected]
Objective: This retrospective study investigates the benefit of combining lobar radioembolization (TARE), performed using a body surface area (BSA) dose prescription model, with targeted therapy (TT) in hepatocellular carcinoma (HCC), and aims to identify predictors of response through contrast-enhanced MRI tumour volumetry.
Methods: Ninety-two HCC patients who underwent TARE at our center between 10/2008 and 01/2022 and a baseline MRI within 60 days prior to TARE as well as follow-up MRI were included. Pre- and post-treatment target lesion volumes were measured as total-tumour-volume (TTV) and enhancing-tumour-volume (ETV). Kaplan-Meier analysis, Log rank tests, and Cox regression were used to assess the impact of clinical and imaging variables on time to target lesion progression and overall survival.
Results: The mean patient age was 65 (SD 10) years; 67 patients had liver cirrhosis. Median overall survival (mOS) was 13 months (95% CI 11– 16). A baseline ETV/TTV ratio > 50% was associated with a median ETV reduction of 41% versus a 61% increase in those with low vascularity (p< 0.001), and a longer time to target lesion progression (28 vs 3 months, p=0.002). Of 45 patients receiving TT, 21 were treated within 2 months before TARE. In this subgroup with pre-interventional TT, high vascularity correlated with significantly improved mOS (> 17 vs 6 months, p=0.027), while no survival difference was observed in other cohorts.
Conclusion: High baseline vascularization may help identify patients who benefit from conventional lobar TARE and a narrowly timed combination with TT in terms of mOS, suggesting synergistic effects in patients not eligible for resection or ablation.
Plain Language Summary: QUESTION: In unresectable hepatocellular carcinoma (HCC), does baseline vascularity identify patients who benefit from combining conventional lobar radioembolization with targeted therapy?
PERTINENT FINDINGS: In this retrospective single-center study of 92 HCC patients, those with baseline tumor arterial vascularity > 50% demonstrated significantly better MR-morphologic response and improved median overall survival when targeted therapy was administered within two months before radioembolization.
IMPLICATIONS FOR PATIENT CARE: Elevated baseline vascularity may identify unresectable HCC patients who benefit from combined radioembolization and targeted therapy, suggesting synergistic effects in patients not eligible for resection or ablation.
Keywords: carcinoma, hepatocellular, survival analysis, radioembolization, targeted therapy, sorafenib
Introduction
Transarterial radioembolization (TARE) using high-energy beta-emitting Yttrium-90 or Holmium-166 microspheres is a locoregional therapy for patients with unresectable hepatocellular carcinoma (HCC) or liver metastases.1 Certain HCC subgroups may benefit more from TARE and potential combinations with targeted therapy (TT), warranting further study.
HCC is the third-leading cause of tumor-related death worldwide, with 60–70% diagnosed at intermediate or advanced stages, often unsuitable for surgery or ablation.2,3 Modern immunotherapies have revolutionized the treatment of these patients, and intra-arterial therapies are increasingly being investigated as potential combination partners.4 The Phase 3 SIRveNIB and SARAH trials confirmed TARE’s safety and efficacy but showed no survival advantage over sorafenib.5,6 The likewise negative randomized controlled SORAMIC trial compared the combination of TARE and sorafenib to sorafenib monotherapy.7 The DOSISPHERE trial demonstrated that the conventional BSA-based dosimetry employed in these trials was flawed and resulted in insufficient tumor doses, yielding lower response and survival rates compared to personalized dosimetry using Technetium-99m macroaggregated albumin SPECT/CT.8 Advancements in computational capacities allowed for the volumetric assessment of tumour volumes and relative vascularization, reflective of tumour biology and susceptibility to intraarterial therapies.9–11 To date, these techniques have not been applied in subgroup analyses of the aforementioned negative RCTs employing BSA-based dosimetry to identify predictors of response to TARE at sublethal doses, including the particularly noteworthy SORAMIC trial, given its combination therapy design. Recently published data and ongoing Phase II and III trials such as EMERALD-Y90, ROWAN or EMERALD-1 are encouraging and highlight the great potential of combining transarterial therapies with TT and immunotherapy. However, the precise degree of transarterial damage required to elicit specific systemic or biological effects is still unknown.12–17
In a prior study with unresectable HCC patients treated with TARE before 2017 we explored baseline vascularity as predictor of devascularization in a multivariable prediction model.18 In an extended cohort, we now aim to investigate the interaction between high baseline vascularity and the timing of TT in relation to target lesion progression and overall survival.
Materials and Methods
Study Cohort
This retrospective single-institution cohort study was approved by the institutional review board at Charité Universitätsmedizin Berlin, Germany (EA4/002/18). The requirement for written informed consent was waived by the ethics committee. All therapies were endorsed by an interdisciplinary tumour board in accordance with current recommendations. All patients who underwent their first TARE session between 10/2008 and 02/2022 were evaluated for inclusion. Exclusion criteria were missing baseline MRI in a 60-day timeframe before radioembolization, missing follow up MRI between day 60 and 90 afterwards or poor imaging quality not amenable to segmentation. The patient selection process is presented as a flowchart in Figure 1.
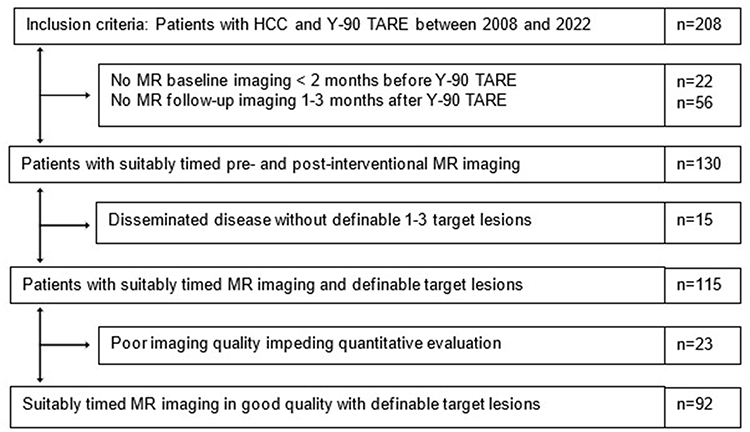 |
Figure 1 Inclusion criteria. Abbreviations: HCC, hepatocellular carcinoma; TARE, transarterial radioembolization. |
TARE Protocol
Interventions were performed by board-certified radiologists using Yttrium-90 resin microspheres (SIR-Spheres®) based on BSA dosimetry according to a standard protocol (supplement 1). Dose reduction was considered for lung shunt fractions between 10% and 20% or if the lung dose approached 30 Gy, as recommended by current guidelines.19 There was no dose reduction performed for patients with signs of liver cirrhosis.
Imaging Technique
Every patient received cross-sectional imaging before and after TARE. MRI was performed with a 1.5 T (Siemens Avanto or Aera) imaging unit. A phased-array torso coil and 0.1 mL per kilogram body weight of intravenous dinatriumgadoxetat (Eovist/Primovist, Bayer Healthcare) were used. The MRI protocol included breath-hold unenhanced and CE T1-weighted 3D fat-suppressed spoiled gradient-echo imaging (section thickness, 2.5 mm; receiver bandwidth, 64 kHz; flip angle, 10°) in the arterial phase (delay of 15 seconds after bolus tracking), portal venous phase (delay of 70 seconds), the delayed phase (delay 3 minutes) and the hepatobiliary excretion phase (delay of 20 minutes after administration). Arterial phase was used for segmentation.
Quantitative and Semi-Quantitative MRI Analysis
A semi-automated quantification software (Philips IntelliSpace Portal V 8.0) was used. Accuracy and reproducibility were previously demonstrated, measurements were performed by two independent readers.9,20 A signal intensity greater than two standard deviations than the average signal intensity measured within a region of interest (ROI) of 10 x 10×10 mm in the musculus erector spinae was defined as arterial vascularization. A maximum of three dominant lesions were analyzed, combined as surrogate total tumour volume (TTV) and enhancing tumour volume (ETV) and segmented at baseline and follow-up. The measurements are given in milliliters. The ETV/TTV ratio served as a vascularity surrogate. Response was evaluated with quantitative European Association for the Study of the Liver (qEASL) criteria, defined as ≥65% reduction in ETV.20 Lesion-specific time to progression was evaluated using the Liver Imaging Reporting and Data System Treatment Response Algorithm (LI-RADS TRA) from the American College of Radiology CT/MRI LI-RADS v2024.21 Lesion-specific progression was rated for mass-like enhancement which was new or increased over time after TARE.
Additional Systemic Therapy
Type and timing of additional TT with multikinase inhibitors and treatment with immune checkpoint inhibitors (ICI) were analyzed. If systemic therapies were initiated within two months before TARE they were labeled pre-interventional TT.
Statistical Analysis
All statistical analyses were conducted with IBM SPSS STATISTICS, version 25 (IBM Corporation, Armonk, NY, USA). Normally distributed, continuous data are presented with mean and standard deviation and compared with the two-sample t-test. Agreement between the two readers was measured with the Pearson correlation coefficient (PCC) statistic. Non-normally distributed data are expressed as median and interquartile range (IQR) and compared with the Mann–Whitney U-test or the Wilcoxon signed-rank test. Survival is reported as median with a 95% confidence interval and was analyzed with the Cox proportional hazard model, Kaplan-Meier curves and the Log rank test. For systemic therapies initiated after TARE, exposure was modeled as a time-dependent covariate in Cox regression to avoid immortal-time bias. Overall survival (OS) was defined from the date of the first TARE session until death. Patients who were either lost to follow-up or alive at the end-of-observation date were censored. Regression coefficients, hazard ratios (HR) and odds ratios (OR) as well as p-values are presented. Multivariable models were built to assess for confounding, variable selection was guided by clinical relevance and univariable statistical significance. As this is an explorative study, no adjustment for multiple testing was applied. Thus, a p-value < 0.05 was considered significant, but is to be interpreted cautiously.
Results
Patient Characteristics
Out of 208 HCC patients treated with TARE from 2008 to 2022, 92 were included in the final analysis after excluding 78 with missing MRIs and 15 with disseminated disease or poor-quality imaging (Figure 1 and Table 1). The median MRI follow-up interval was 77 days (range 32–175 days; interquartile range (IQR) 42 days). The predominantly male cohort had a mean age of 65.3 years, 67% (62/92) were BCLC stage B, 73% (67/92) had liver cirrhosis, 30% (28/92) had portal vein tumour thrombosis. All patients had an Eastern Cooperative Oncology Group (ECOG) performance status 0–1. The mOS was 13 months (95% CI 11–16) and TT was administered to 45 patients before or after TARE. 78% (35/45) received sorafenib, and 16% received ICIs or combinations (Table 2). Pre-interventional TT within 2 months was given to 21 patients, there was no statistical difference in baseline variables between with or without pre-interventional TT. In all cases, baseline MRI was performed after initiation of TT. In the last five years of the observation period, the rate of prior ablation increased from 26% to 49% (p=0.047), with mOS increasing from 11 months (95% CI 7.3–14.7) to 20.8 months (95% CI 10.5–15.5) (p=0.024) (supplement 2).
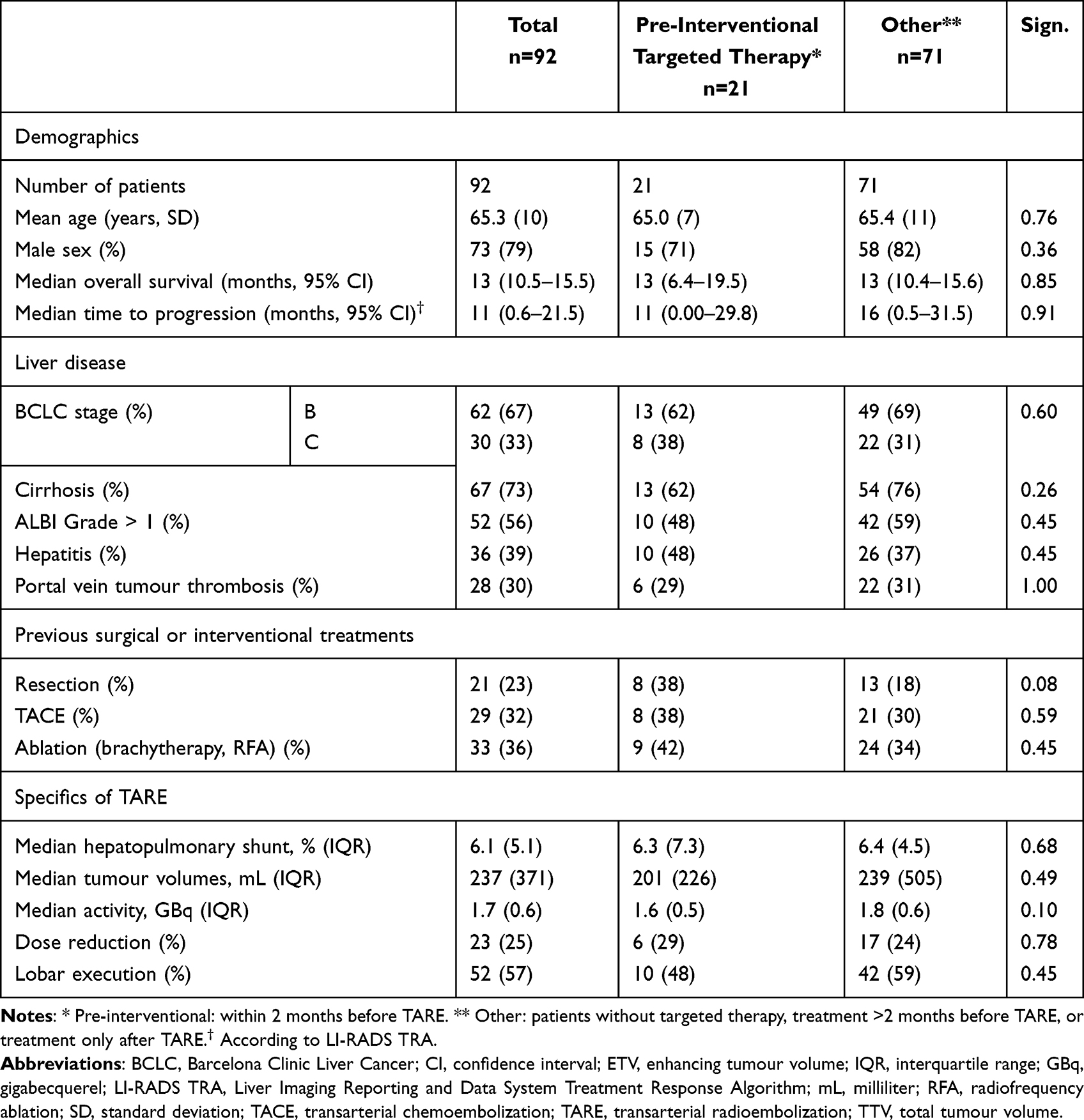 |
Table 1 Patient Characteristics |
 |
Table 2 Type and Timing of Targeted Therapy |
MRI Tumor Segmentation at Baseline and 3 Months After Treatment
To approximate TTV and ETV on contrast-enhanced MRI, up to three dominant lesions were measured in 92 patients (Table 3). An example of baseline and follow-up segmentations can be found in the supplements section (supplement 3). The agreement of two readers was high with a PCC > 0.93 for all measurements. Baseline median TTV was 167 mL (IQR 319 mL) and ETV was 69 mL (IQR 179 mL), with a median ETV/TTV ratio of 71% (IQR 62%). 56/92 patients (61%) had an ETV/TTV ratio >50% and there was no significant difference between cohorts with or without pre-interventional TT. In patients with baseline ETV/TTV >50%, ETV decreased by a median of 41% (IQR 67%), while those with ETV/TTV <50% showed a median ETV increase of 61% (IQR 221%) (p<0.001). These findings were consistent across the peri-interventional TT and the remaining cohorts (Figure 2a). The proportion of patients with high baseline vascularity increased over time—from 42% (22/53) between 2008–2016 to 87% (34/39) in the last five years of the observation period (p<0.001) (supplement 2).
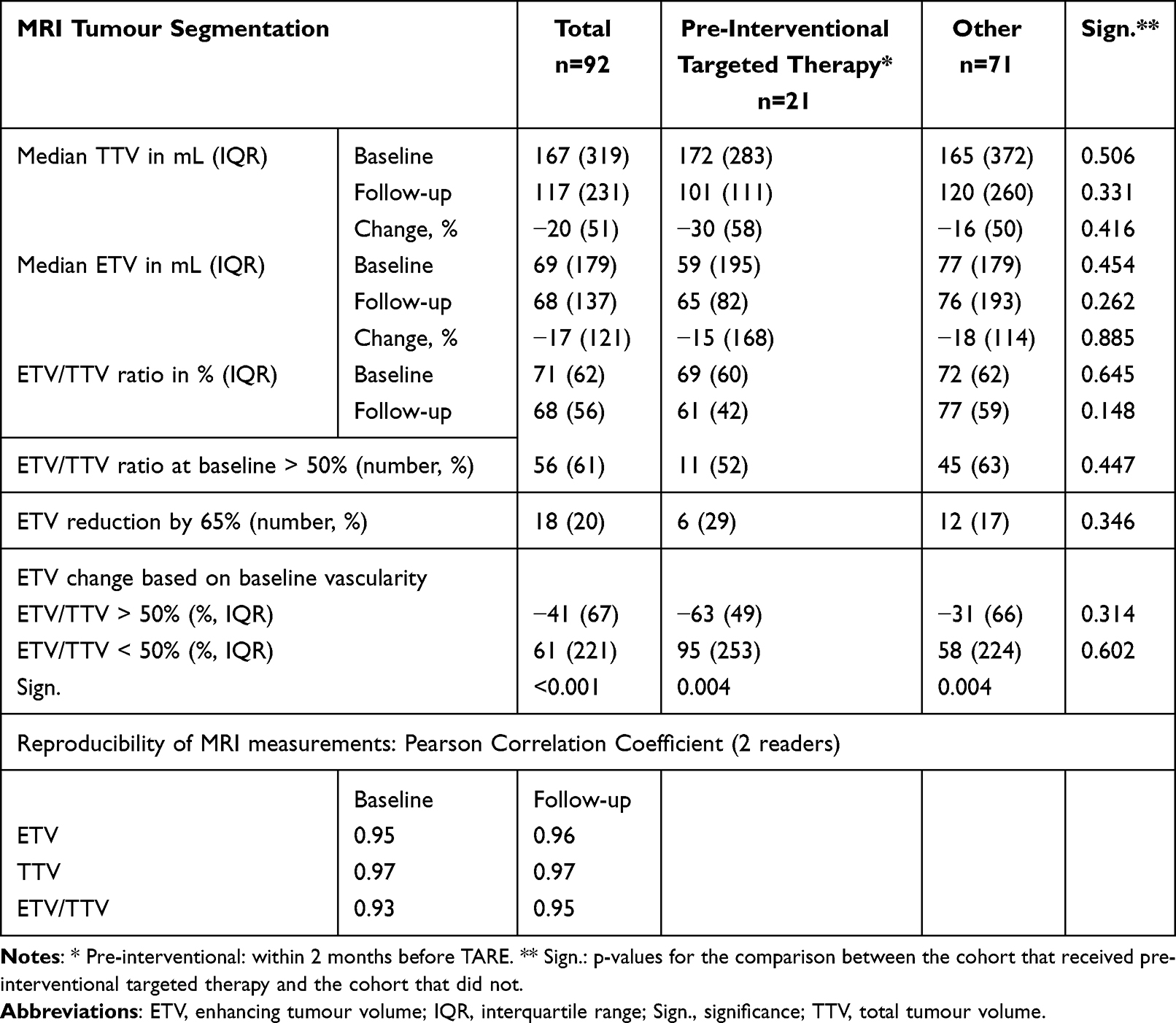 |
Table 3 Tumour Segmentation |
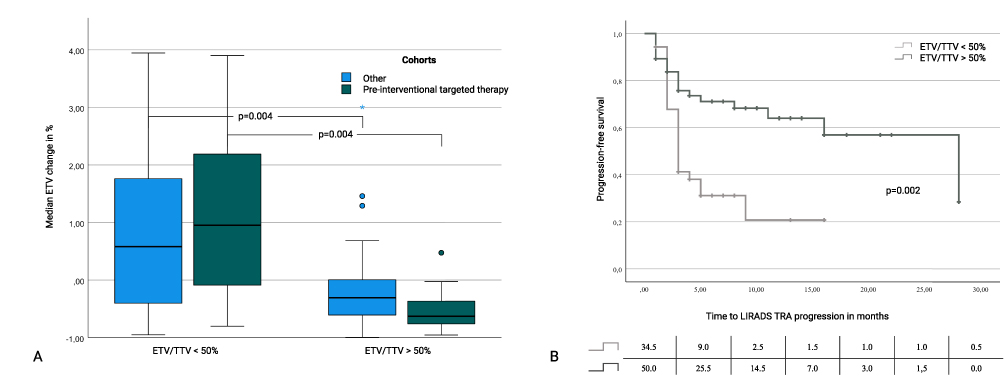 |
Figure 2 Baseline vascularization, change in enhancing tumour volume and time to progression. (A) Box plots show a significant difference in median enhancing tumour volume (ETV) change after radioembolization based on baseline vascularity (ETV/TTV < or >50%). No significant differences were observed between subgroups with or without pre-interventional targeted therapy (TT). The asterisk indicates an outlier greater three times the interquartil range from the nearest quartile. (B) Kaplan-Meier curves of lesion-based time to progression (per Liver Imaging Reporting and Data System Treatment Response Algorithm, LI-RADS TRA) comparing subgroups with or without pre-interventional targeted therapy. Kaplan–Meier curves were truncated at 30 months due to sparse numbers at risk thereafter. |
Predictors of Time to Target Lesion Progression
All consecutive follow-up MRIs were reviewed for target lesion progression according to LI-RADS TRA criteria. Patients were censored if no target lesion progression was seen on the last available imaging which was the case in 12/36 patients for ETV/TTV < 50% and 37/56 patients for ETV/TTV > 50% respectively (49/92 patients). Hence, patients with high baseline vascularity more frequently succumbed to their disease without documented progression of the target lesion on the last available imaging. In univariable Cox regression, high baseline vascularity was significantly associated with reduced risk of target lesion progression per LI-RADS TRA. As a continuous variable, ETV/TTV showed an HR of 0.23 (p=0.002); dichotomized at 50%, the HR was 0.40 (p=0.004). Neither pre-interventional TT nor other clinical, demographic, or imaging variables had a significant effect, and results were consistent regardless of TT status (supplement 4). Median time to progression was 11.0 months (95% CI, 0.6–21.5) for the whole cohort. Patients with ETV/TTV >50% had a significantly longer median time to progression of 28.0 months (95% CI 11.0–45.1) versus 3.0 months for poorly vascularized lesions (p=0.002) (Figure 2b).
Predictors of Patient Survival in Patients with Pre-Interventional Targeted Therapy
Univariable Cox regression showed that an ALBI grade >1 was associated with a significantly increased hazard of death (HR = 2.35) in the entire cohort and remained significant in both subcohorts. Treatment after 2017 significantly reduced the HR by 0.53 and 0.50 in the whole cohort and the sub-cohort without pre-interventional TT respectively (Table 4 and supplement 5). In patients who received pre-interventional TT, univariable Cox regression revealed prior TACE to significantly increase the hazard ratio (HR) by 3.11 (p=0.040). BCLC status, tumour burden, age and liver reserve affect both TACE allocation and survival, limiting its interpretability. ETV/TTV, both as continuous variable and dichotomized at 50%, significantly reduced the HR to 0.12 (p=0.034) and 0.31 (p=0.039) respectively. A ≥65% reduction in ETV lowered the HR to 0.20 (p=0.038). No significant predictors were identified in patients who did not receive TT or treatment outside the specified time frame. To adjust for confounding, BCLC stage, age, ALBI score, tumour volume as calculated for TARE dosimetry, calendar period, and an ETV/TTV ratio >50% were analyzed in a multivariable Cox regression model. In both the entire cohort as well as the cohort without pre-interventional TT, ALBI grade > 1 significantly increased the HRs whereas treatment after 2017 decreased the HR. In the pre-interventional TT cohort, an ETV/TTV > 50% was associated with a significant reduction in HR (p=0.046); however, due to the small number of events relative to covariates, these results should be interpreted cautiously, as overfitting may have produced unstable estimates, pseudoseparation and reduced power (Table 5). Kaplan-Meier analysis demonstrated a mOS >17 months for patients with pre-interventional TT and an ETV/TTV >50%, versus 6 months for those with low baseline vascularity (p=0.027) (Table 6). No survival difference by vascularity was observed in patients without pre-interventional TT (Figure 3) who had a mOS of 11 months (95% CI 7.3–14.7). Patients who received post-interventional TT had the longest mOS of 23.4 months (95% CI 20.3–26.6) (Table 6), with potential survivorship bias. Time-dependent Cox regression revealed no statistically significant association of survival and later administration of TT (Table 4). Inclusion of patients with targeted therapy within two months after TARE improved the separation of the survival curves for high and low baseline vascularity (supplement 6).
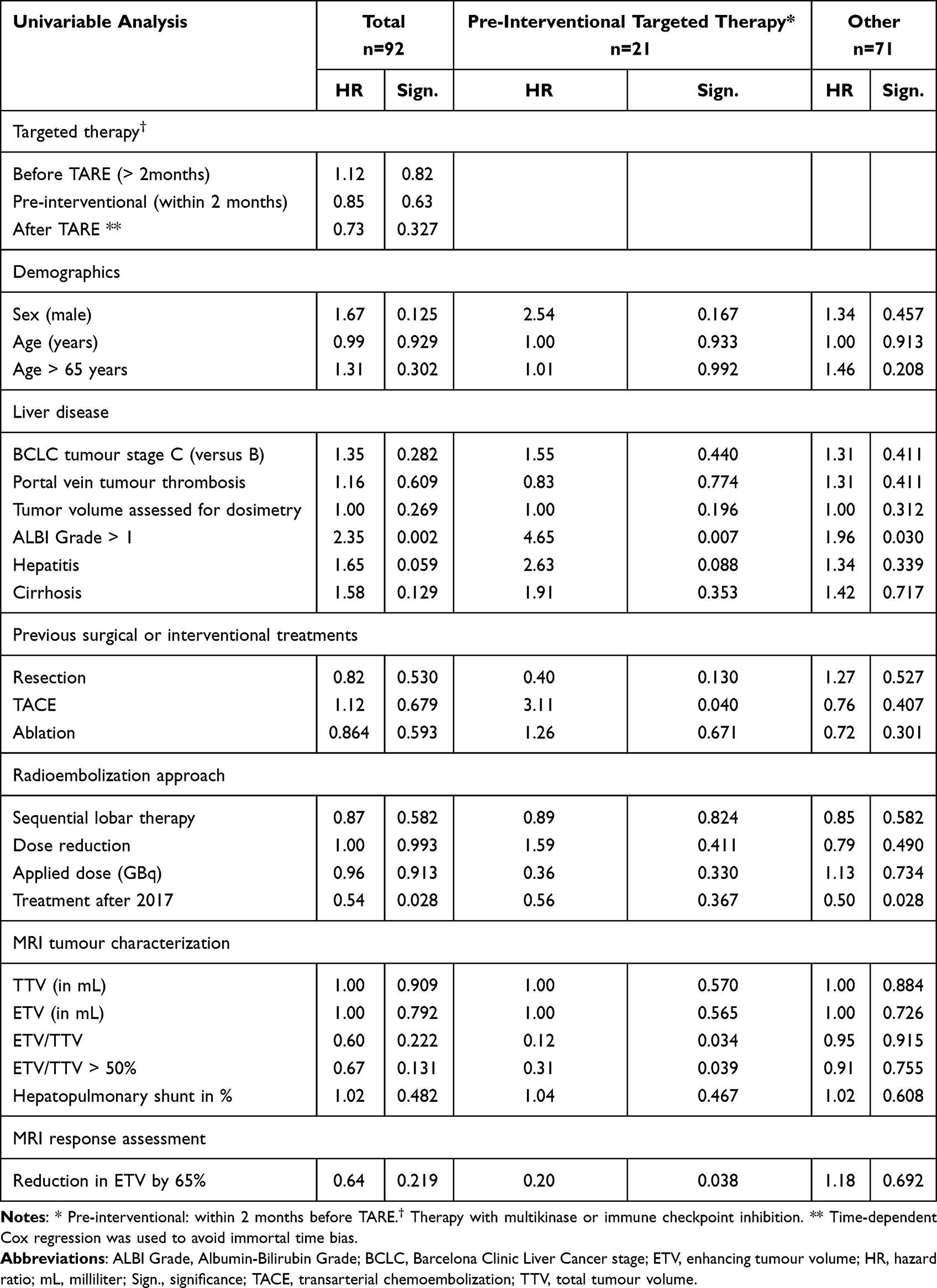 |
Table 4 Univariable Cox Regression Analysis by Timing of Targeted Therapy |
 |
Table 5 Multivariable Cox Regression Analysis by Timing of Targeted Therapy |
 |
Table 6 Time to Target Lesion Progression and Median Overall Survival |
 |
Figure 3 Impact of baseline vascularity in patients with or without pre-interventional targeted therapy. Kaplan Meier curves of survival in patients with low or high ratio of enhancing to total tumour volume (ETV/TTV) < or >50%. (A) In patients who did not receive pre-interventional TT, no significant impact of baseline vascularity was seen. (B) In patients who received TT within two months before TARE, survival was significantly higher in patients with high baseline vascularity (p=0.027). The adjusted numbers at risk are given at the beginning of the interval. |
Discussion
In this retrospective, single-center study of 92 patients with unresectable HCC treated with TARE using the BSA dose model, arterial baseline vascularity greater than 50% was associated with a median ETV reduction of 41%, compared to a 61% increase in patients with low baseline vascularity (p<0.001). High baseline vascularity was also significantly associated with prolonged time to target lesion progression. OS was significantly reduced in patients with reduced liver reserve and longer in patients treated after 2017. Among patients who received TT—primarily sorafenib—within two months prior to TARE, high baseline vascularity was associated with a significantly longer mOS of over 17 months compared to 6 months (p=0.027).
Stratifying patients by an ETV/TTV ratio above or below 50% identifies cohorts that either consistently reduce or continue growing their ETV after lobar TARE with conventional dosing, as previously shown.18 This likely reflects favorable tumor-to-liver dose distribution that translates into deterministic radiation damage in at least parts of the tumour and allows baseline vascularization to be used as a screening tool for potential response to lobar TARE. In our cohort, high baseline vascularity combined with pre-interventional TT was associated with improved mOS. This effect was neither observed in poorly vascularized tumors nor in well-vascularized tumors that received TT outside the predefined pre-interventional time frame, supporting the hypothesis of a synergistic interaction between TARE and TT. Pre-interventional TT did not significantly affect time to target lesion progression in our cohort, although our data do not support any speculation regarding potential out-of-field effects. TKIs may enhance TARE efficacy via anti-proliferative and anti-angiogenic mechanisms counteracting VEGFR and related pathways.22 With respect to ICI therapy, radiation can exert a powerful antitumor immune response and help overcome mechanisms of immunosuppression by remodeling the tumor microenvironment as well as increasing lymphocytic infiltration and recognition of tumor cells by T cells. This is why many recent and ongoing trials explore the benefit of administering ICI therapies after radiation.23 Nevertheless, other trials investigate the administration of ICI prior or concomitant to radiation therapy in order to investigate the impact of priming immunomodulatory effects which we might have encountered in our cohort.24 However, no control group that received TT only was included, which might yield superior outcomes in highly vascular tumors as recent data suggest.25 Furthermore, prior systemic therapies likely reduced the measured baseline vascularity and thereby altered the apparent tumour biology. However, as most patients in our cohort underwent TARE due to non-response to TT, the extent of TT-induced devascularization was probably limited.
Our findings align with and potentially extend current treatment paradigms. The BSA method for activity calculation is conservative and has shown inferior outcomes compared to personalized dosimetry, as evidenced by the DOSISPHERE trial.8 Our proposed baseline ETV/TTV threshold identifies patients with unfavorable tumor biology for BSA dosing and may explain why large RCTs like SORAMIC failed to meet primary endpoints. In our cohort, patients with pre-interventional TT and high tumor vascularity had a significantly prolonged mOS (>17 months) compared to 6 months in poorly vascularized tumors (p=0.027), exceeding outcomes reported in the SARAH (9.9 months) and SORAMIC trials (11–12 months).6 In the period since 2016, when recruitment for SORAMIC ended, we saw an increase both in the share of highly vascularized tumours and mOS from 11 months (95% CI (7.3, 14.7)) to 20.8 months (95% CI (10.5, 15.5)) (p=0.024) (supplement 2). This change in treatment patterns and outcomes fits well with results from a recent meta-analysis, which investigated survival trends in sorafenib for unresectable HCC in 5525 patients.26 The authors likewise reported an increase in mOS from 9.78 months to 13.38 months in cohorts treated after 2015. This could in part explain our longer mOS with respect to the SORAMIC cohorts as for SORAMIC, biological tumour activity as measured by PET or tumour vascularity has not been part of the patient selection criteria and could potentially have been in the lower ranges that we saw in the beginning of our observation period. A 2021 meta-analysis with 632 patients reported a pooled mOS of 10.79 months after combination therapy of TARE and sorafenib but found no advantage over TARE alone.27 Similarly, a propensity score analysis of TARE plus sorafenib versus TARE alone found no significant difference.28 None of these studies used baseline vascularity as a predictor of lobar TARE or combined therapy efficacy, highlighting the originality of our approach.
Our findings impact retrospective analyses, response prediction, and the role of TARE with traditional BSA dosing in the era of personalized dosimetry. The ETV/TTV ratio is an accessible imaging biomarker that can be integrated into standard PACS systems and compared between MR and CT imaging using correction factors.29 Subgroup analyses of available high-quality data may uncover survival benefits of TKI combination therapy in highly vascularized tumors or cohorts treated solely with TKIs, aiding understanding of combination therapy effects. Similar considerations apply to checkpoint inhibitors, now first line treatment for advanced HCC with reported response rates of around 27% and 30% for the combination of Atezolizumab and Bevacizumab and dual CTLA4 and PD1/PDL1 blockade respectively.30,31 Reliable response prediction is an unmet clinical need with respect to treatment-related adverse events that cause drug discontinuation in 10–20% of patients.32,33 In a small heterogeneous HCC cohort, vascularity metrics have shown predictive value for ICI therapies.25 Personalized dosimetry has transformed TARE from palliative lobar treatment to segmental, ablative therapy with curative intent.34,35 Baseline ETV/TTV ratio calculation could identify patients benefitting from interaction effects of TARE and systemic therapy, in our cohort potentially 62% of patients. This would create a rationale for lobar TARE with significantly lower activity targets as for radiation ablation purposes, which could very well be achieved with conventional, workflow-efficient dose prescription regimen such as the BSA method and like that expand the applicability of TARE.
Limitations include the small, heterogeneous cohort over 14 years, variability in TT timing and type, and imaging protocols, especially before 2017. Both whole-liver and sequential TARE were performed. Prior systemic therapies likely reduced the measured baseline vascularity and thereby altered the apparent tumour biology. However, as most patients in our cohort underwent TARE due to non-response to TT, the extent of TT-induced devascularization was probably limited. The small number of patients treated with ICIs precluded meaningful subgroup analyses and limits the interpretability of related findings. Absence of Y90 dosimetry data impeded direct correlation with absorbed dose.
In conclusion, baseline vascularity—quantified by the ETV/TTV ratio—emerges as a promising imaging biomarker for predicting meaningful tumor response to conventional TARE. These findings may inform patient selection for TARE combined with TT administered in close temporal proximity and warrant validation in retrospective and prospective studies.
Abbreviations
ALBI grade, albumin-bilirubin grade; BSA, body surface area; CE, contrast enhanced; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; ETV, enhancing tumour volume; HCC, hepatocellular carcinoma; HR, hazard ratio; ICI, immune checkpoint inhibitor; IQR, interquartile range; LI-RADS TRA, Liver Imaging Reporting and Data System Treatment Response Algorithm; mOS, median overall survival; OR, odds ratio; PCC, Pearson correlation coefficient; TACE, transarterial chemoembolization; TARE, transarterial radioembolization; TT, targeted therapy; TTV, total tumour volume.
Funding
This study was not supported by any funding.
Disclosure
Prof. Gebauer reports lecture honoraria from Inari Medical, BAYER, CALYX, Boston Scientific, ICON, Terumo, SIRTex Medical, and Siemens Healthineers. Prof. Amthauer discloses advisory work for Novartis and lecture honoraria from Pfizer, Novartis, and SIRTex Medical. Dr. Auer received travel and lecture honoraria from Boston Scientific, BD, Bayer, SIRTex Medical, and IGEA. Dr. Savic reports grants from Guerbet, Berliner Krebsgesellschaft e.V., Charité 3R - Reduce, Refine, Replace and the Deutsche Forschungsgemeinschaft (DFG). Drs. Collettini and Wieners report lecture and travel honoraria from SIRTex Medical. The authors report no other conflicts of interest in this work.
References
1. Mazzaferro V, Sposito C, Bhoori S, et al. Yttrium-90 radioembolization for intermediate-advanced hepatocellular carcinoma: a Phase 2 study. Hepatology. 2013;57:1826–13. doi:10.1002/hep.26014
2. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229–263. doi:10.3322/caac.21834
3. Park JW, Chen M, Colombo M, et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE Study. Liver Int. 2015;35:2155–2166. doi:10.1111/liv.12818
4. Foerster F, Wiesmann L, Bark P, Galle PR. Pioneering precision: the evolution of immunotherapy for hepatocellular carcinoma. Hepatology. 2025. doi:10.1097/HEP.0000000000001554
5. Chow PKH, Gandhi M, Tan SB, et al. SIRveNIB: selective internal radiation therapy versus sorafenib in asia-pacific patients with hepatocellular carcinoma. J Clin Oncol. 2018;36:1913–1921. doi:10.1200/JCO.2017.76.0892
6. Vilgrain V, Pereira H, Assenat E, et al. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): an open-label randomised controlled phase 3 trial. Lancet Oncol. 2017;18:1624–1636. doi:10.1016/S1470-2045(17)30683-6
7. Ricke J, Klumpen HJ, Amthauer H, et al. Impact of combined selective internal radiation therapy and sorafenib on survival in advanced hepatocellular carcinoma. J Hepatol. 2019;71:1164–1174. doi:10.1016/j.jhep.2019.08.006
8. Garin E, Tselikas L, Guiu B, et al. Personalised versus standard dosimetry approach of selective internal radiation therapy in patients with locally advanced hepatocellular carcinoma (DOSISPHERE-01): a randomised, multicentre, open-label phase 2 trial. Lancet Gastroenterol Hepatol. 2021;6:17–29. doi:10.1016/S2468-1253(20)30290-9
9. Chapiro J, Duran R, Lin M, et al. Identifying staging markers for hepatocellular carcinoma before transarterial chemoembolization: comparison of three-dimensional quantitative versus non-three-dimensional imaging markers. Radiology. 2015;275:438–447. doi:10.1148/radiol.14141180
10. Chapiro J, Lin M, Duran R, Schernthaner RE, Geschwind JF. Assessing tumor response after loco-regional liver cancer therapies: the role of 3D MRI. Expert Rev Anticancer Ther. 2015;15:199–205. doi:10.1586/14737140.2015.978861
11. Chapiro J, Wood LD, Lin M, et al. Radiologic-pathologic analysis of contrast-enhanced and diffusion-weighted MR imaging in patients with HCC after TACE: diagnostic accuracy of 3D quantitative image analysis. Radiology. 2014;273:746–758. doi:10.1148/radiol.14140033
12. He AR, Toskich B. The ROWAN study: safety and efficacy of transarterial radioembolization with Y-90 glass microspheres and the STRIDE regimen in hepatocellular carcinoma. J Clin Oncol. 2023;41(4_suppl):Tps622–Tps622. doi:10.1200/JCO.2023.41.4_suppl.TPS622
13. Lencioni R, Kudo M, Erinjeri J, et al. EMERALD-1: a phase 3, randomized, placebo-controlled study of transarterial chemoembolization combined with durvalumab with or without bevacizumab in participants with unresectable hepatocellular carcinoma eligible for embolization. J Clin Oncol. 2024;42:Lba432–Lba432. doi:10.1200/JCO.2024.42.3_suppl.LBA432
14. Salem R, Noonan A, Ben S, et al. Emerald-Y90: a phase 2 study to evaluate transarterial radioembolization (Tare) followed by durvalumab (D) and Bevacizumab (B) for the treatment of participants (pts) with unresectable hepatocellular carcinoma (Uhcc) eligible for embolization. Hepatology. 2024;80:1.
15. Zeng H, Zhou CY, Chen XJ, et al. Comparison of the efficacy and safety of selective internal radiotherapy and sorafenib alone or combined for hepatocellular carcinoma: a systematic review and Bayesian network meta-analysis. Clin Exp Med. 2023;23:2141–2150. doi:10.1007/s10238-023-00997-3
16. Yeo YH, Liang J, Lauzon M, et al. Immunotherapy and transarterial radioembolization combination treatment for advanced hepatocellular carcinoma. Am J Gastroenterol. 2023;118:2201–2211. doi:10.14309/ajg.0000000000002467
17. Peng ZW, Fan WZ, Zhu BW, et al. Lenvatinib combined with transarterial chemoembolization as first-line treatment for advanced hepatocellular carcinoma: a Phase III, randomized clinical trial (LAUNCH). J Clin Oncol. 2023;41:
18. Ludemann W, Kahn J, Pustelnik D, et al. Yttrium-90 radioembolization for unresectable hepatocellular carcinoma: predictive modeling strategies to anticipate tumor response and improve patient selection. Eur Radiol. 2022;32:4687–4698. doi:10.1007/s00330-022-08585-x
19. Busse NC, Al-Ghazi MSAL, Abi-Jaoudeh N, et al. AAPM medical physics practice guideline 14.a: yttrium-90 microsphere radioembolization. J Appl Clin Med Physics. 2024;25:e14157.
20. Chapiro J, Duran R, Lin M, et al. Early survival prediction after intra-arterial therapies: a 3D quantitative MRI assessment of tumour response after TACE or radioembolization of colorectal cancer metastases to the liver. Eur Radiol. 2015;25:1993–2003. doi:10.1007/s00330-015-3595-5
21. Aslam A, Chernyak V, Miller FH, et al. CT/MRI LI-RADS 2024 update: treatment response assessment. Radiology. 2024;313:e232408. doi:10.1148/radiol.232408
22. Qin S, Li A, Yi M, Yu S, Zhang M, Wu K. Recent advances on anti-angiogenesis receptor tyrosine kinase inhibitors in cancer therapy. J Hematol Oncol. 2019;12:27. doi:10.1186/s13045-019-0718-5
23. Sangro B, Sarobe P, Hervas-Stubbs S, Melero I. Advances in immunotherapy for hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2021;18:525–543. doi:10.1038/s41575-021-00438-0
24. Zhang Z, Liu X, Chen D, Yu J. Radiotherapy combined with immunotherapy: the Dawn of cancer treatment. Signal Transduct Target Ther. 2022;7:258.
25. Sobirey R, Matuschewski N, Gross M, et al. Tumor response assessment in hepatocellular carcinoma treated with immunotherapy: imaging biomarkers for clinical decision-making. Eur Radiol. 2024;35(1):73–83. doi:10.1007/s00330-024-10955-6
26. Tan DJH, Tang ASP, Lim WH, et al. Survival trends in sorafenib for advanced hepatocellular carcinoma: a reconstructed individual patient data meta-analysis of randomized trials. Liver Cancer. 2023;12:445–456. doi:10.1159/000529824
27. Facciorusso A, Paolillo R, Tartaglia N, et al. Efficacy of combined transarterial radioembolization and sorafenib in the treatment of hepatocarcinoma: a meta-analysis. Dig Liver Dis. 2022;54:316–323. doi:10.1016/j.dld.2021.06.003
28. Facciorusso A, Bargellini I, Cela M, Cincione I, Sacco R. Comparison between Y90 radioembolization plus sorafenib and Y90 radioembolization alone in the treatment of hepatocellular carcinoma: a propensity score analysis. Cancers. 2020;13:12. doi:10.3390/cancers13010012
29. Luedemann WM, Geisel D, Gebauer B, et al. Comparing HCC arterial tumour vascularisation on baseline imaging and after lipiodol cTACE: how do estimations of enhancing tumour volumes differ on contrast-enhanced MR and CT? Eur Radiol. 2020;30:1601–1608. doi:10.1007/s00330-019-06430-2
30. Finn RS, Qin SK, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. New Engl J Med. 2020;382:1894–1905. doi:10.1056/NEJMoa1915745
31. Abou-Alfa GK, Chan SL, Kudo M, et al. Phase 3 randomized, open-label, multicenter study of tremelimumab (T) and durvalumab (D) as first-line therapy in patients (pts) with unresectable hepatocellular carcinoma (uHCC): HIMALAYA. J Clin Oncol. 2022;40:40. doi:10.1200/JCO.21.00105
32. Yau T, Kang YK, Kim TY, et al. Efficacy and safety of nivolumab plus ipilimumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib: the CheckMate 040 randomized clinical trial. JAMA Oncol. 2020;6:e204564. doi:10.1001/jamaoncol.2020.4564
33. Cheng AL, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76:862–873. doi:10.1016/j.jhep.2021.11.030
34. Kim E, Sher A, Abboud G, et al. Radiation segmentectomy for curative intent of unresectable very early to early stage hepatocellular carcinoma (RASER): a single-centre, single-arm study. Lancet Gastroenterol Hepatol. 2022;7:843–850. doi:10.1016/S2468-1253(22)00091-7
35. Salem R, Gordon AC, Mouli S, et al. Y90 radioembolization significantly prolongs time to progression compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology. 2016;151:1155–1163e1152. doi:10.1053/j.gastro.2016.08.029
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Curative-Intent Treatments on Hepatocellular Carcinoma Survival in Alcohol-Related Cirrhosis: A Nationwide Study
Kraglund F, Villadsen GE, Jepsen P
Clinical Epidemiology 2023, 15:39-48
Published Date: 6 January 2023
Modified Patent Hemostasis Strategy Based on the Platelet Counts for Transradial Access Chemoembolization in Patients with Hepatocellular Carcinoma: A Prospective Single-Center Study
Luo YG, Zhang XW, Tsauo JW, Li Y, Li JG, Peng Q, Li YW, Sun W, Zhao H, Li X
Journal of Hepatocellular Carcinoma 2023, 10:687-695
Published Date: 21 April 2023
Efficacy of Atezolizumab Plus Bevacizumab Combined with Transarterial Chemoembolization for Unresectable Hepatocellular Carcinoma: A Real-World Study
Shen X, Zhang JX, Liu J, Liu S, Shi HB, Cheng Y, Zhang QQ, Yin GW, Zu QQ
Journal of Hepatocellular Carcinoma 2024, 11:1993-2003
Published Date: 21 October 2024