Back to Journals » Clinical Epidemiology » Volume 15
Effects of Curative-Intent Treatments on Hepatocellular Carcinoma Survival in Alcohol-Related Cirrhosis: A Nationwide Study
Authors Kraglund F ![]() , Villadsen GE, Jepsen P
, Villadsen GE, Jepsen P ![]()
Received 12 October 2022
Accepted for publication 2 December 2022
Published 6 January 2023 Volume 2023:15 Pages 39—48
DOI https://doi.org/10.2147/CLEP.S393118
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor H Sorensen
Frederik Kraglund,1 Gerda Elisabeth Villadsen,1 Peter Jepsen1,2
1Department of Hepatology and Gastroenterology, Aarhus University Hospital, Aarhus, Denmark; 2Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark
Correspondence: Frederik Kraglund, Email [email protected]
Purpose: The aim of curative-intent treatment for hepatocellular carcinoma (HCC) is to restore the patients’ survival to what it would have been, had they not developed HCC. We examined the chances of such ‘statistical cure’ from HCC in patients with cirrhosis due to alcohol-related liver disease (ALD cirrhosis).
Patients and Methods: Using nationwide Danish healthcare registries, all patients with ALD cirrhosis who were treated for HCC in 2004– 2018 were identified and included in cohorts based on initial HCC treatment. We used cure fraction analyses to estimate the chance of being statistically cured by each HCC treatment.
Results: We included 1087 patients with HCC due to ALD cirrhosis, of whom 51 (4.7%) were treated with resection and 215 (19.8%) were treated with ablation. The cure fraction, ie the fraction of patients who experienced no excess mortality from HCC, was 31.8% (95% CI: 0.0− 67.5) following resection and 22.9% (95% CI: 2.6− 43.2) following ablation. In patients who were still alive five years after the initial HCC treatment, the likelihood of having been statistically cured at that time was 69.0% after resection and 60.2% after ablation. For both treatments, a 90% chance of having been statistically cured was reached after seven years.
Conclusion: Based on cure fraction analyses, resection for HCC statistically cures 31.8% of patients with HCC and underlying ALD cirrhosis, while ablation statistically cures 22.9% of patients. Seven years after curative-intent treatments for HCC, surviving patients are 90% likely to be statistically cured of HCC. This information is valuable to patients and the clinicians caring for them.
Keywords: carcinoma, hepatocellular, liver diseases, alcoholic, hepatectomy, catheter ablation
Plain Language Summary
Using Danish, nationwide registries, we studied the probability of being cured by curative-intent treatments for primary liver cancer in patients with cirrhosis due to alcohol-related liver disease. In 2004–2018, liver resection cured around one third of patients with liver cancer due to alcohol-related liver disease, and catheter ablation cured around one fourth of patients.
Introduction
Hepatocellular carcinoma (HCC) is the 5th commonest cancer and the 3rd leading cause of cancer-related death globally.1 Most patients with HCC have cirrhosis, and in Denmark, one-half of patients with HCC have underlying cirrhosis due to alcohol-related liver disease (ALD cirrhosis).2 In addition to a high mortality from HCC, these patients have a very high mortality due to other causes, such as liver failure or non-HCC comorbidities.3 That high mortality due to other causes must be accounted for when evaluating the effectiveness of curative-intent HCC treatments, because HCC treatments cannot be expected to reduce it.
Statistical cure is a useful measure in evaluating the effectiveness of HCC treatments because it accounts for non-HCC mortality. The ‘net survival’ and the ‘cure fraction’ are different, but equally valid measures of statistical cure and, thereby, treatment effectiveness.4,5 Recently, the cure fraction following resection for HCC was estimated at 26.3% in a multinational cohort of mixed HCC etiology.6 However, an estimate of the cure fraction for HCC treatments other than resection and liver transplantation has not previously been published, nor has an etiology-specific estimate.
The aim of curative-intent HCC treatments is to restore the patients’ survival to what it would have been, had they not developed HCC. Analyses of statistical cure measure the extent to which that aim is fulfilled, and it is of obvious importance to both patients and clinicians to know whether the purportedly curative treatments for HCC are in fact curative.
In this nationwide descriptive study, we aimed to estimate the net survival and cure fraction of curative-intent resection and ablation for HCC in patients with ALD cirrhosis.
Patients and Methods
Setting
This descriptive, registry-based study was conducted in the Danish population of 5,781,190 people (1 January 2018). All Danish citizens have free, tax-supported access to general practitioners and hospital care. The personal identification number (CPR-number) issued to all Danish citizens at birth or immigration allows linkage of all national registries. The CPR registry records the vital status of all citizens with complete follow-up until death or emigration. The National Patient Registry contains data on hospital contacts since 1977 including International Classification of Diseases (ICD) codes, Danish Classification of Surgical Procedures and Therapies codes, and administrative codes. Since 1996, all surgical procedures have been registered as NOMESCO Classification of Surgical Procedures (NCSP) codes.7 The Danish Cancer Registry contains data on all incident cases of cancer in Denmark since 1943, including TNM-stage from 2004 onwards,8 and the Danish Register of Causes of Death records all immediate, supplementary, and underlying causes of death by ICD codes.9 Regarding clinical care, treatment and follow-up of HCC is conducted according to Danish guidelines based on The European Association for the Study of the Liver (EASL) guidelines.10
Study Population
Using the National Patient Registry and the Danish Cancer Registry, the study population was defined as all Danish citizens treated for HCC in 2004–2018 who also had an ALD cirrhosis diagnosis code from a hospital contact any time between 1 January 1980 and the date of the first HCC treatment. The inclusion period was restricted to 2004–2018 for two reasons. First, to increase HCC treatment homogeneity throughout the study period, and second, because the Danish Cancer Registry was modernized in 2004 to include TNM-stage. All HCC treatments were identified using the National Patient Registry. Thus, we identified all NCSP codes for liver resection, radiofrequency and microwave ablation of pathological liver tissue, liver transplantation, and transarterial chemoembolisation (TACE) or selective internal radiation therapy (SIRT) of the liver. Similarly, using codes for non-surgical treatment, we identified treatment with Sorafenib, Regorafenib, stereotactic body radiation therapy (SBRT), and palliative treatment. Additionally, we identified referrals to oncology and palliative medicine and recorded decisions to not offer HCC treatment due to the health of the patient. To check whether all HCC treatment codes were accounted for, we screened all treatment codes received by the patients with HCC in the year prior to and in the year following the HCC diagnosis. Baseline cirrhosis decompensation was defined as any of the following procedures or diagnoses prior to the first HCC treatment: ascites drainage; treatment of gastric or esophageal varices; or diagnosis of ascites, spontaneous bacterial peritonitis, variceal bleeding, or hepatorenal syndrome.
Treatment Cohorts
The patients were included in separate curative-intent treatment cohorts based on their first HCC treatment. When a patient received both ablation and TACE within two days, the first treatment was defined as a combination therapy of ablation and TACE. We defined five curative-intent treatment cohorts: resection, ablation, ablation plus TACE, SBRT, and transplantation. Patients in the ablation plus TACE, SBRT, and transplantation cohorts and patients whose first HCC treatment was life-prolonging (TACE, SIRT, and Sorafenib) or best supportive care (palliative treatment, referral without further treatment, and no recorded treatments) were enumerated for completeness, but not included in the net survival analyses. The patients were followed from the date of their first treatment until death, and surviving patients were censored on 31 December 2019. To evaluate clinical follow-up, all CT and MR scans of the liver from the initial treatment date until the end of follow-up were enumerated. All registry-codes used to define the study population and the treatment cohorts are listed in Supplementary Table S1.
Cure Models
The ‘statistical cure fraction’ is the proportion of patients who do not experience excess mortality from HCC. Therefore, it is defined solely by survival time. There is no standard method to estimate the chances of being statistically cured by curative-intent treatment. For that reason, we used three different methods: cause-specific survival analysis, relative survival ratio analysis, and cure fraction analysis.
- In cause-specific survival analysis, deaths from causes other than HCC are censored, meaning that the analysis measures the survival probability that would be observed if – hypothetically – death from non-HCC causes were impossible.
- In relative survival ratio analysis, net survival is estimated as a ratio between the observed survival and the expected survival for patients with HCC.
- Cure fraction analysis models the relative survival using expected survival estimates and computes the cure fraction, which is the predicted relative survival probability at the time when the predicted relative survival function plateaus.5 The expected survival is based on controls who are identical to the patients with HCC, except they did not develop HCC (see below for further details).
Cause of Death
The Danish Register of Causes of Death contains up to 12 codes recorded by the on-duty physician detailing the cause of death: one underlying cause (obligatory), two supplementary causes, one immediate cause, and eight non-causal supplementary diseases. To minimize misclassification, one of the authors (FK) determined whether a given death was caused by HCC by manual inspection of all recorded cause of death codes. Briefly, a death was classified as HCC-related if HCC was recorded as either the underlying, a supplementary, or the immediate cause of death, except when the codes suggested an acute event, which was likely not caused by HCC (eg acute myocardial infarction).
Lifetable of Expected Survival
Calculations of the relative survival ratio and the cure fraction rely on estimates of expected survival for patients with HCC, ie, the survival they would have experienced had they not developed HCC. The expected survival was based on a lifetable of 1-year survival probabilities that could be combined to compute expected survival beyond one year. The 1-year survival probabilities were computed from each day after ALD cirrhosis diagnosis, within strata defined by sex, attained 5-year age group, attained 5-year calendar period, cirrhosis decompensation any time prior to the initial HCC treatment (yes/no), and whether the first ALD cirrhosis diagnosis was given during acute admission (yes/no). The 1-year survival probabilities were computed using the Kaplan-Meier estimator, and they were based on the source population of all patients diagnosed with ALD cirrhosis in 1980–2018 in Denmark.
Statistical Analysis
The cause-specific survival was calculated using the Kaplan-Meier estimator, treating deaths from causes other than HCC as censoring events, so that we estimated the mortality that would be observed if, hypothetically, deaths from causes other than HCC could not occur.11 To compute the expected life-years lost due to HCC in the cause-specific survival setting, we generated pseudo-values to fit a generalized linear model of lost life-years.12 The relative survival ratio was calculated using the Ederer I method.13 Thus, the observed survival of a given HCC-treated patient was continually matched to his/her expected survival probability.
The cure fraction was estimated using a mixture model,5 and expected cumulative mortality hazards were derived from the lifetable of expected survival probabilities. The choice of survival distribution for modelling the cure fraction was based on Akaike information criteria and visual inspection of Cox-Snell residuals.14 The probability of being statistically cured at a given time after treatment was derived from the cure fraction models. The number of clinical follow-up CT and MR liver scans were calculated as the number of scans per person-year per year.
Results
We identified 1087 patients with underlying ALD cirrhosis treated for incident HCC in 2004–2018. Of these, 290 (27%) received curative-intent treatments (resection: 51, ablation: 215, transplantation: 13, ablation plus TACE: 5, SBRT: 6), 214 (20%) received life-prolonging treatments, and the remaining 538 (54%) received best supportive care. Baseline characteristics of the patients receiving curative-intent treatments are listed along with follow-up time and overall survival estimates in Table 1. Briefly, the 10-year overall survival was 10.5% (95% confidence interval [CI]: 2.5−25.2) after resection and 6.0% (95% CI: 2.1−13.0) after ablation (Supplementary Figure S1), and the overall survival was not statistically significantly different between the resection and ablation cohorts (Log rank test, p = 0.25). For reference, the 10-year overall survival was 58.6% (95% CI: 26.7−80.6) after transplantation. Patients who received resection had higher TNM stages than patients who received ablation (Table 1). Regarding clinical follow-up, patients treated with resection received an average of three CT or MR liver scans during the first year of follow-up, while patients treated with ablation received an average of four scans. In both cohorts, the average number of MR and CT liver scans gradually decreased over the following 10 years (Supplementary Figure S2).
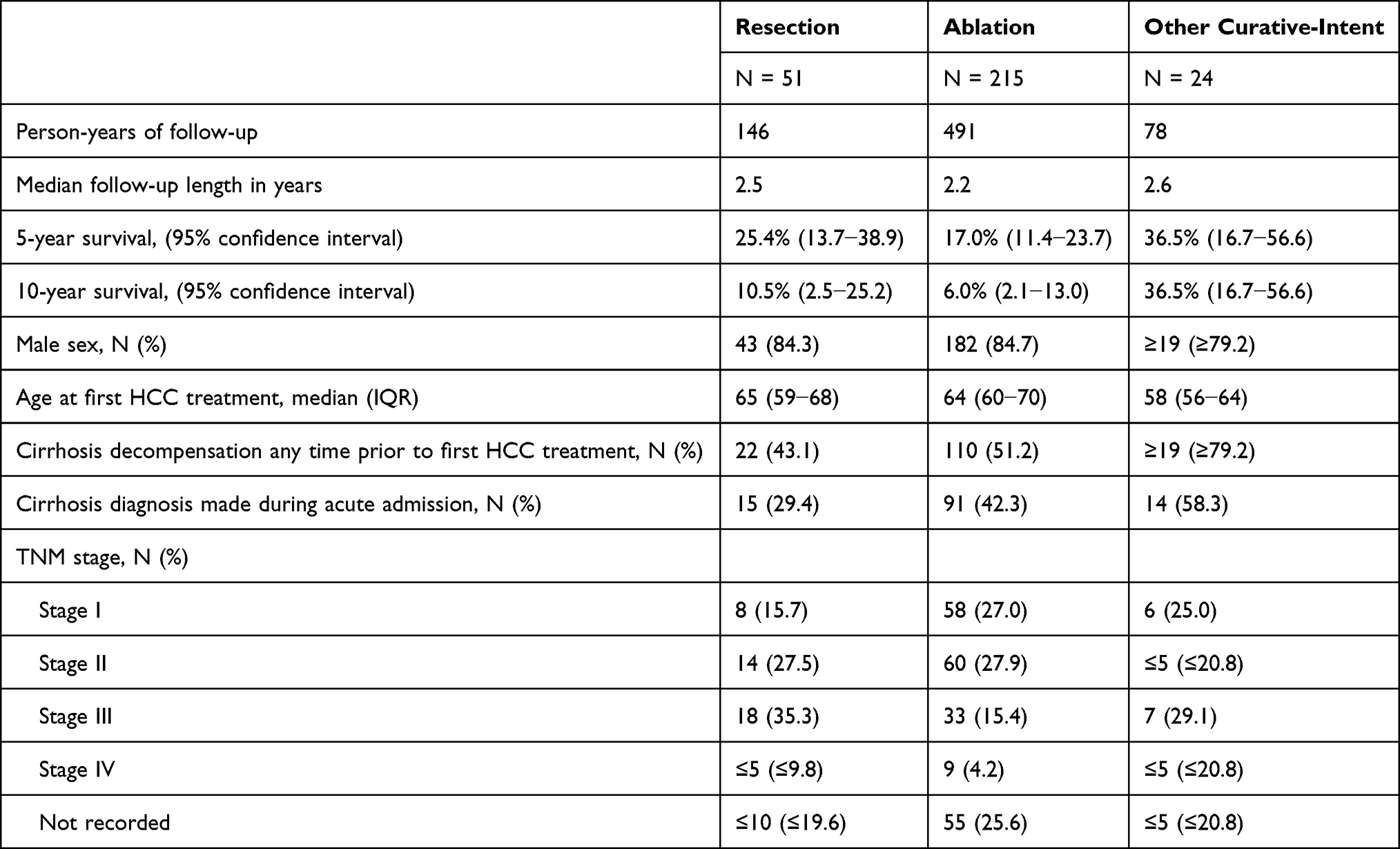 |
Table 1 Follow-Up Time, Overall Survival, and Baseline Characteristics of the Treatment Cohorts |
Cause-Specific Survival
The cause-specific survival describes the proportion of patients who would be alive if, hypothetically, death from causes other than HCC were literally impossible. The cause-specific survival following resection was 43.6% (95% CI: 25.6−60.2) after 5 years and 34.9% (95% CI: 15.5−55.1%) after 10 years (Figure 1). Over 10 years after resection for HCC, an average of 3.6 life-years (95% CI: 2.4−4.7) were lost due to HCC. Death from HCC occurred more frequently following ablation, and the cause-specific survival was 39.0% (95% CI: 29.1−48.7) after 5 years and 17.1% (95% CI: 6.2−32.5%) after 10 years (Figure 1). Over 10 years after ablation for HCC, an average of 4.1 life-years (95% CI: 3.5−4.7) were lost due to HCC. The causes of death of patients in the resection and ablation cohorts are listed in Supplementary Table S2.
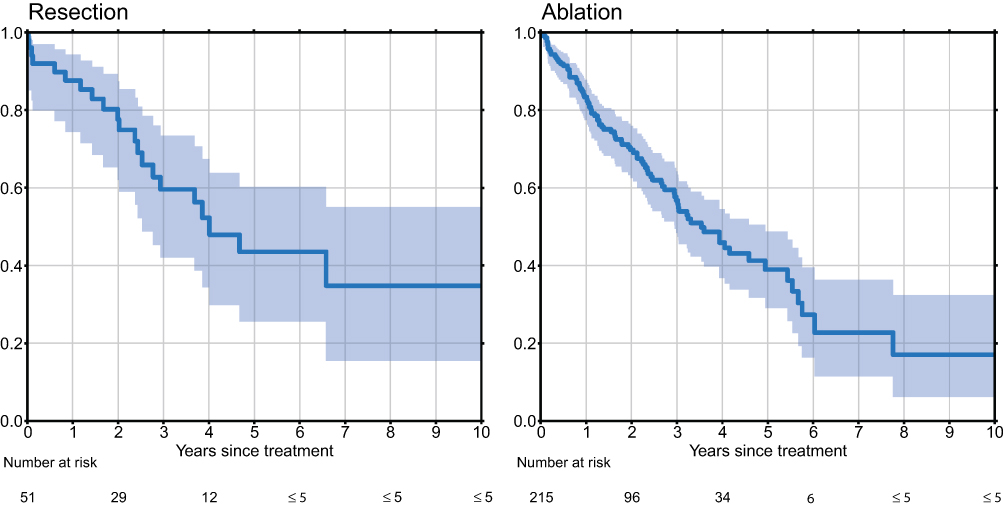 |
Figure 1 The cause-specific survival in the resection and ablation cohorts. Left: resection, right: ablation. The cause-specific survival is the survival probability observed in a hypothetical world where death from non-HCC causes is literally impossible. Consequently, the cause-specific survival is 100% if treatment eliminates the risk of death from HCC, and it is 0% if everybody dies from HCC despite treatment. |
Relative Survival
The relative survival ratio describes the patients’ survival relative to what it would have been, had they not developed HCC. The relative survival ratio following resection was 54.4% (95% CI: 29.4−83.2) after 5 years and 40.1% (95% CI: 9.3−97.8%) after 10 years. Following ablation, it was 40.0% (95% CI: 26.7−55.5) after 5 years and 32.0% (95% CI: 10.9−69.5%) after 10 years (Figure 2).
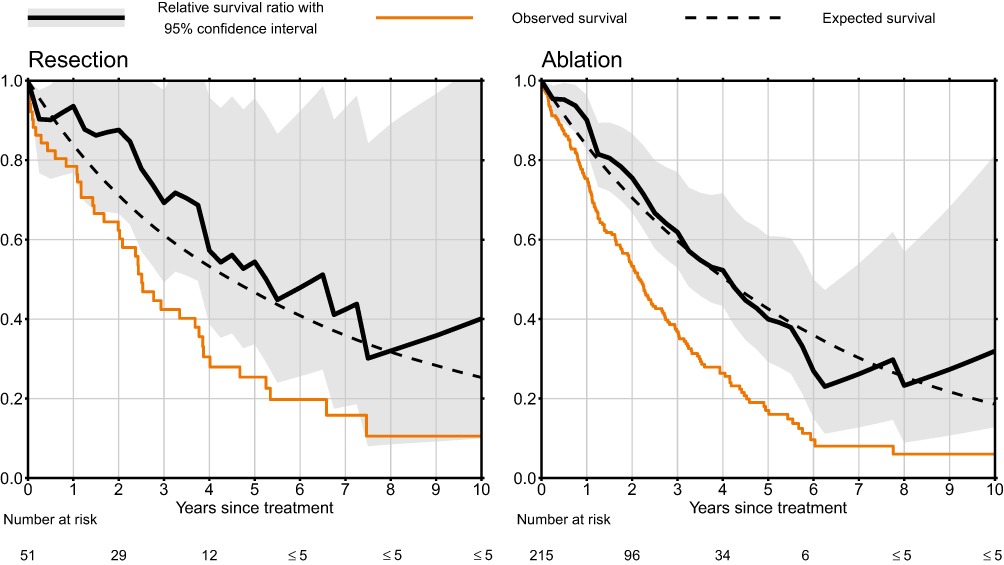 |
Figure 2 The relative survival ratio, observed survival, and expected survival in the resection and ablation cohorts. Left: resection, right: ablation. |
Cure Fraction
The cure fraction represents the chance of experiencing no excess mortality despite having HCC. The cure fraction was 31.8% (95% CI: 0−67.5) after resection and 22.9% (95% CI: 2.6−43.2) after ablation. The likelihood of being statistically cured increased with increasing time since treatment, and the patients who were still alive after five years had by that time achieved a 69.0% (after resection) or 60.2% (after ablation) likelihood of statistical cure. For both resection and ablation, a 90% likelihood of being statistically cured was achieved after seven years (Figure 3). There was a high level of agreement between the three cure models: the cause-specific survival, the relative survival ratios, and the predicted relative survival function derived from the cure fraction model (Figure 4).
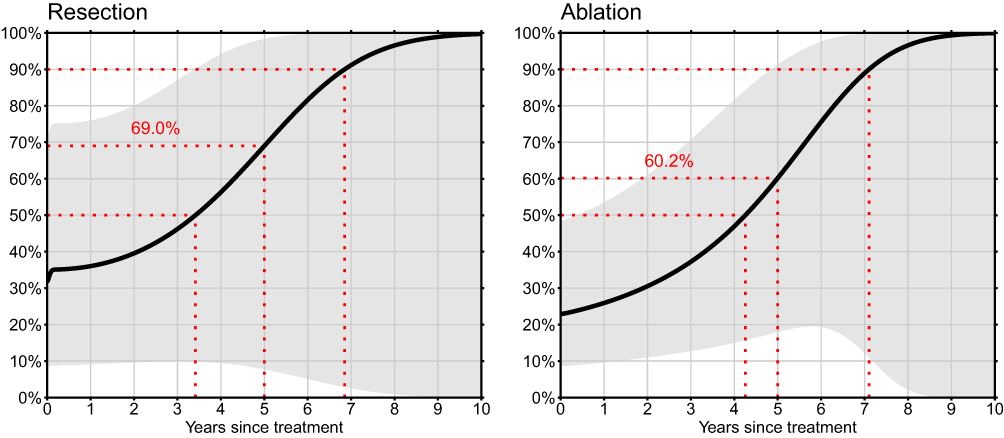 |
Figure 3 The probability of being statistically cured of HCC over time since the first treatment, conditional on surviving. The grey areas represent 95% confidence intervals. The three dotted red lines mark the time to reach a statistical cure probability of 50% and 90% along with the statistical cure probability reached after five years. |
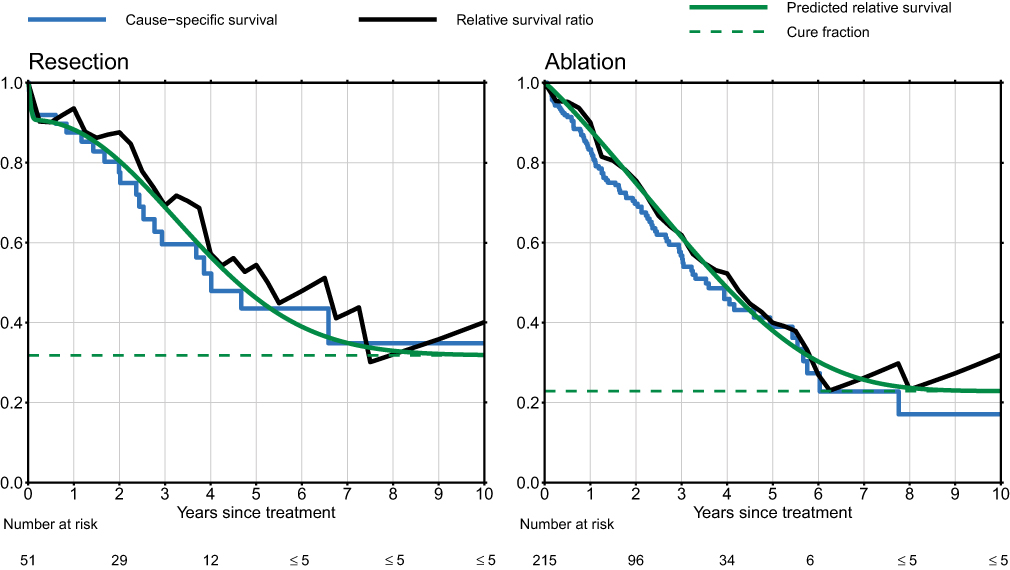 |
Figure 4 Visual comparison of the three cure models. Cause-specific survival, relative survival ratio, and cure fraction predicted relative survival following resection (left) and ablation (right). |
Discussion
Patients with HCC have a high mortality, and this is particularly true if they also have ALD cirrhosis. HCC surveillance is recommended by international guidelines because it can allow an earlier HCC diagnosis with a better chance of curative treatment. In this nationwide study, we confirmed that resection and ablation offer a chance of statistical cure, but they are far from perfect. Based on this nationwide study, we estimate that resection statistically cures 31.8−40.1% of patients with HCC due to ALD cirrhosis, while ablation statistically cures 17.1−32.0%. Seven years after curative-intent treatment for HCC, surviving patients are 90% likely to be statistically cured of HCC. This is a clinically relevant message to patients. Of note, it was not our purpose to determine whether resection or ablation is the better treatment for HCC. Our estimates of the chance of a statistical cure apply only to patients who, according to the EASL guidelines, are eligible for the treatment in question. Specifically, it should not be inferred that patients who were truly treated with ablation would have had a better prognosis if they had instead been treated with resection.
Very little is known about the curative potential of curative-intent treatments for HCC. What is known is that resection or ablation for HCC is associated with a low recurrence-free survival. Thus, the 5-year recurrence risk following resection has been reported as upward of 70%,15 and the 5-year recurrence-free survival following ablation has been estimated at around 25%.16,17 However, it is impossible to derive the treatment effectiveness from these measures − especially in patients with ALD cirrhosis who have an initially low overall survival. The cure fraction is important to consider because, unlike overall and recurrence-free survival, it measures what is gained by curative-intent HCC treatments. This knowledge may better guide clinicians and patients in HCC treatment decisions.
Based on the cause-specific analyses, the 10-year probability of surviving HCC was 34.9% following resection and 17.1% following ablation. Since cause-specific survival analyses rely on cause of death data, the main limitation of this method is misclassification of the causes of death.18 All death certificates must contain at least the underlying cause of death registered by the on-duty physician, and while this provides complete data, it does not ensure validity or reproducibility.9 The consistency of the results across the three methods to estimate cure fraction provides some reassurance that we adjudicated causes of death reliably.
The relative survival ratio was 40.1% following resection and 32.0% following ablation, and based on the predicted relative survival functions, the cure fraction was 31.8% following resection and 22.9% following ablation. The main limitation of relative survival ratio and cure fraction analyses is the validity of the expected survival probabilities. Patients who develop HCC have a much higher mortality than the general population, because 80% of them have underlying cirrhosis,19 so using a general population lifetable for this study, while possible, would result in heavily biased estimates.20 We circumvented this issue by using a lifetable derived from the same single-etiology study population as the HCC treatment cohorts. That is a strong point of our study. Furthermore, we stratified the expected survival probabilities by the strongest predictors of survival. Cucchetti and colleagues recently estimated the cure fraction following resection for HCC at 26.3% (95% CI: 21.7–30.8) in a cohort of patients with HCC irrespective of etiology.6 Although comparable, this estimate is lower than any of our cure model estimates. This difference in estimates is likely explained by two significant study design differences. First, Cucchetti and colleagues modelled the disease-free survival of patients with HCC, effectively equating HCC recurrence with death. We chose to model the overall survival because HCC recurrence does not equate death, and because death following HCC recurrence may not be caused by HCC. Second, Cucchetti’s expected survival rates were derived from a mixed-etiology cohort of health insurance beneficiaries from the American SEER database,21,22 and those beneficiaries likely had a better survival probability than the population that give rise to the patients with HCC.
Previous studies have found discrepancies between the net survival estimation methods.4,23 It is a strong point of our study that the methods yielded highly consistent results, as it indicates that we succeeded in minimizing the bias introduced by misclassification and invalid expected survival probabilities. Notably, the three methods are distinctly different; they require different data, different assumptions, and they have different limitations and strengths. Because of this, the methods can be used to triangulate the “true” probability of being statistically cured by curative-intent treatment for HCC. Thus, the results presented in the present study are not significantly dependent on the choice of net survival analysis method.
Our study was restricted to patients with ALD cirrhosis in Denmark. This was done to increase the validity of the expected survival probabilities, but it came at the cost of smaller cohorts, statistical imprecision, and uncertainty whether our findings generalize to other settings and other cirrhosis etiologies. Another downside of this restriction is the small number of liver transplantations, which prevented the analysis of the net survival following liver transplantation. Of note, a study from 2018 estimated the cure fraction following liver transplantation irrespective of HCC-etiology at 74.1% (inter-quartile range: 62.6–83.1) using disease-free survival and expected survival rates from the general population.24 Based on these and our results, patients receiving liver transplantation for HCC have the best chances of statistical cure by far.
Valid analyses require valid data, and while the Danish healthcare registries provide nationwide, prospectively collected data with complete follow-up, the reliance on registry codes is a potential limitation of this study. The Danish Cancer Registry had an estimated completeness of 95–97% in 1997,25 and it has likely improved since then, owing to the modernization of the registry in 2004–2008.8 In the National Patient Registry, the positive predictive value (PPV) of codes for ALD cirrhosis recorded in 1985–1989 was estimated at 92.4% with a completeness of 93.2%.26 The specific treatment codes used in this study have not previously been validated, but codes for gastrointestinal surgery generally have a very high validity.27,28 In the present study, multiple codes were used to define the cohorts, which increases the PPV of the individual codes. For instance, the a priori probability of receiving liver resection is obviously much higher in patients with HCC than in the general population, and because of this, the PPV of the code is also much higher. A limitation of the registry data is the lack of information on known predictors of survival, ie BCLC stage comprising tumor size, performance status, liver function (eg Child-Pugh classification), alpha fetoprotein (AFP),29 and des-gamma-carboxy prothrombin (DCP).30
As evidenced by the number of control CT and MR scans performed during clinical follow-up, Danish patients with HCC are treated and followed in accordance with the current EASL guidelines, and therefore, the results of this study apply to countries adhering to these guidelines. Regarding transportability of the results to other HCC-etiologies, studies comparing different HCC-etiologies have shown that patients with chronic viral hepatitis have a higher risk of HCC-recurrence following resection.31,32 This implies that our results are not applicable to patients with HCC due to chronic viral liver disease.
With this study, we have demonstrated the utility of using multiple cure models to triangulate the probability of statistical cure after curative-intent HCC treatments. The results of this study illustrate that curative-intent treatments do statistically cure a substantial proportion of patients of HCC despite the low overall survival. This conclusion is important to patients and to the clinicians who care for them. Additionally, our estimates may be important for discussions about the duration of follow-up after HCC treatment; our findings indicate that seven years of clinical follow-up is required to ensure a 90% likelihood that the patient is statistically cured. The estimates may also be important for discussions about HCC surveillance among patients with ALD cirrhosis. The goal of surveillance is to identify HCCs while they can still be treated with curative intent. We have shown that those treatments do in fact statistically cure some patients, thus providing a rationale for HCC surveillance, but we have also shown that curative-intent treatment of HCC is inferior to primary prevention of HCC, the goal of which is to prevent chronic liver disease and subsequent development of HCC.10 Our findings may provide inputs to simulation studies modelling the effect of HCC surveillance on HCC-related mortality, and they may also provide inputs to policy discussions about the merits of primary and secondary prevention of HCC.
Conclusion
In conclusion, the probability of being statistically cured by curative-intent treatment for HCC due to ALD cirrhosis was 31.8–40.1% for resection and 17.1−32.0% for ablation. The probability of having been statistically cured gradually increased over time, and after seven years, surviving patients were 90% likely to be statistically cured of HCC.
Abbreviations
HCC, hepatocellular carcinoma; ALD cirrhosis, cirrhosis due to alcohol-related liver disease; ICD, International Classification of Diseases; NCSP, NOMESCO Classification of Surgical Procedures; EASL, The European Association for the Study of the Liver; TACE, transarterial chemoembolisation; SIRT, selective internal radiation therapy; SBRT, stereotactic body radiation therapy; MR, magnetic resonance imaging; CT, computed tomography; CI, confidence interval; PPV, positive predictive value.
Data Sharing Statement
The data used in this study cannot be made publicly available according to Danish law. Access to data from the Danish healthcare registries can be applied for via https://sundhedsdatastyrelsen.dk/da/forskerservice.
Ethics Approval and Informed Consent
This study was approved by the National Board of Health and by the Danish Data Protection Agency (Journal No. 1-16-02-321-19). According to the Danish law, approval from the Danish Committee on Health Research Ethics was not necessary. Since this is a register-based study, written consent was not required.
Consent for Publication
All content in this manuscript is original, and all authors have seen and agreed to the publication of the final draft.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Peter Jepsen was supported by a grant from the Novo Nordisk Foundation (NNF18OC0054612). The funding organization was not involved in the design and conduct of the study, or in the decision to submit the manuscript for publication. All other authors report no financial support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL., et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 71(3):209. doi:10.3322/caac.21660
2. Akinyemiju T, Abera S, Ahmed M; Collaboration GBoDLC. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level: results From the Global Burden of Disease Study 2015. JAMA Oncol. 2017;3(12):1683–1691. doi:10.1001/jamaoncol.2017.3055
3. Deleuran T, Vilstrup H, Jepsen P. Decreasing Mortality Among Danish Alcoholic Cirrhosis Patients: a Nationwide Cohort Study. Am J Gastroenterol. 2016;111(6):817–822. doi:10.1038/ajg.2016.107
4. Makkar N, Ostrom QT, Kruchko C, Barnholtz-Sloan JS. A comparison of relative survival and cause-specific survival methods to measure net survival in cancer populations. Cancer Med. 2018;7(9):4773–4780. doi:10.1002/cam4.1706
5. Lambert PC, Thompson JR, Weston CL, Dickman PW. Estimating and modeling the cure fraction in population-based cancer survival analysis. Biostatistics. 2007;8(3):576–594. doi:10.1093/biostatistics/kxl030
6. Cucchetti A, Zhong J, Berhane S, et al. The chances of hepatic resection curing hepatocellular carcinoma. J Hepatol. 2020;72(4):711–717. doi:10.1016/j.jhep.2019.11.016
7. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/clep.S91125
8. Gjerstorff ML. The Danish Cancer Registry. Scand J Public Health. 2011;39(7 Suppl):42–45. doi:10.1177/1403494810393562
9. Helweg-Larsen K. The Danish Register of Causes of Death. Scand J Public Health. 2011;39(7 Suppl):26–29. doi:10.1177/1403494811399958
10. EASL Clinical Practice. Guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
11. Sarfati D, Blakely T, Pearce N. Measuring cancer survival in populations: relative survival vs cancer-specific survival. Int J Epidemiol. 2010;39(2):598–610. doi:10.1093/ije/dyp392
12. Kragh Andersen P, Pohar Perme M. Pseudo-Observations in Survival Analysis Research report, 08/12
13. Hakulinen T, Seppä K, Lambert PC. Choosing the relative survival method for cancer survival estimation. Eur J Cancer. 2011;47(14):2202–2210. doi:10.1016/j.ejca.2011.03.011
14. McLachlan GJ, McGiffin DC. On the role of finite mixture models in survival analysis. Stat Methods Med Res. 1994;3(3):211–226. doi:10.1177/096228029400300302
15. Hartke J, Johnson M, Ghabril M. The diagnosis and treatment of hepatocellular carcinoma. Semin Diagn Pathol. 2017;34(2):153–159. doi:10.1053/j.semdp.2016.12.011
16. Lee DH, Lee JM, Lee JY, et al. Radiofrequency Ablation of Hepatocellular Carcinoma as First-Line Treatment: long-term Results and Prognostic Factors in 162 Patients with Cirrhosis. Radiology. 2014;270(3):900–909. doi:10.1148/radiol.13130940
17. Facciorusso A, Del Prete V, Antonino M, et al. Post-recurrence survival in hepatocellular carcinoma after percutaneous radiofrequency ablation. Digestive Liver Dis. 2014;46(11):1014–1019. doi:10.1016/j.dld.2014.07.012
18. Schaffar R, Rachet B, Belot A, Woods L. Cause-specific or relative survival setting to estimate population-based net survival from cancer? An empirical evaluation using women diagnosed with breast cancer in Geneva between 1981 and 1991 and followed for 20 years after diagnosis. Cancer Epidemiol. 2015;39(3):465–472. doi:10.1016/j.canep.2015.04.001
19. Jepsen P, Andersen MW, Villadsen GE, Ott P, Vilstrup H. Time-trends in incidence and prognosis of hepatocellular carcinoma in Denmark: a nationwide register-based cohort study. Liver Int. 2017;37(6):871–878. doi:10.1111/liv.13340
20. Bright CJ, Brentnall AR, Wooldrage K, Myles J, Sasieni P, Duffy SW. Errors in determination of net survival: cause-specific and relative survival settings. Br J Cancer. 2020;122(7):1094–1101. doi:10.1038/s41416-020-0739-4
21. Cho H, Klabunde CN, Yabroff KR, et al. Comorbidity-Adjusted Life Expectancy: a New Tool to Inform Recommendations for Optimal Screening Strategies. Ann Intern Med. 2013;159(10):667–676. doi:10.7326/0003-4819-159-10-201311190-00005
22. Mariotto AB, Wang Z, Klabunde CN, Cho H, Das B, Feuer EJ. Life tables adjusted for comorbidity more accurately estimate noncancer survival for recently diagnosed cancer patients. J Clin Epidemiol. 2013;66(12):1376–1385. doi:10.1016/j.jclinepi.2013.07.002
23. Tan KS, Eguchi T, Adusumilli PS. Reporting net survival in populations: a sensitivity analysis in lung cancer demonstrates the differential implications of reporting relative survival and cause-specific survival. Clin Epidemiol. 2019;11:781–792. doi:10.2147/CLEP.S210894
24. Pinna AD, Yang T, Mazzaferro V, et al. Liver Transplantation and Hepatic Resection can Achieve Cure for Hepatocellular Carcinoma. Ann Surg. 2018;268(5):868–875. doi:10.1097/sla.0000000000002889
25. Storm HH, Michelsen EV, Clemmensen IH, Pihl J. The Danish Cancer Registry--history, content, quality and use. Dan Med Bull. 1997;44(5):535–539.
26. Vestberg K, Thulstrup AM, Sørensen HT, Ottesen P, Sabroe S, Vilstrup H. Data quality of administratively collected hospital discharge data for liver cirrhosis epidemiology. J Med Syst. 1997;21(1):11–20.
27. Kjærgaard J, Clemmensen IH, Thomsen BL, Storm HH. Validity of diagnoses of and operations for nonmalignant gynecological conditions in the Danish National Hospital Registry. J Clin Epidemiol. 2002;55(2):137–142. doi:10.1016/S0895-4356(01)
28. Harboe KM, Anthonsen K, Bardram L. Validation of data and indicators in the Danish Cholecystectomy Database. Int J Qual Health Care. 2009;21(3):160–168. doi:10.1093/intqhc/mzp009
29. Chen HL, Chen YH, Du L, Song YP, Zhu B. Elevated serum alpha-fetoprotein levels are associated with poor prognosis of hepatocellular carcinoma after surgical resection: a systematic review and meta-analysis. Arab J Gastroenterol. 2021;22(1):12–22. doi:10.1016/j.ajg.2020.09.004
30. Lee S, Rhim H, Kim YS, Kang TW, Song KD. Post-ablation des-gamma-carboxy prothrombin level predicts prognosis in hepatitis B-related hepatocellular carcinoma. Liver Int. 2016;36(4):580–587. doi:10.1111/liv.12991
31. Utsunomiya T, Shimada M, Kudo M, et al. A Comparison of the Surgical Outcomes Among Patients With HBV-positive, HCV-positive, and Non-B Non-C Hepatocellular Carcinoma: a Nationwide Study of 11,950 Patients. Ann Surg. 2015;261(3):513–520. doi:10.1097/SLA.0000000000000821
32. Marasco G, Colecchia A, Colli A, et al. Role of liver and spleen stiffness in predicting the recurrence of hepatocellular carcinoma after resection. J Hepatol. 2019;70(3):440–448. doi:10.1016/j.jhep.2018.10.022
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Modified Patent Hemostasis Strategy Based on the Platelet Counts for Transradial Access Chemoembolization in Patients with Hepatocellular Carcinoma: A Prospective Single-Center Study
Luo YG, Zhang XW, Tsauo JW, Li Y, Li JG, Peng Q, Li YW, Sun W, Zhao H, Li X
Journal of Hepatocellular Carcinoma 2023, 10:687-695
Published Date: 21 April 2023
Efficacy of Atezolizumab Plus Bevacizumab Combined with Transarterial Chemoembolization for Unresectable Hepatocellular Carcinoma: A Real-World Study
Shen X, Zhang JX, Liu J, Liu S, Shi HB, Cheng Y, Zhang QQ, Yin GW, Zu QQ
Journal of Hepatocellular Carcinoma 2024, 11:1993-2003
Published Date: 21 October 2024
Lobar Yttrium-90 Radioembolization with BSA-Based Dosimetry for Unresectable Hepatocellular Carcinoma: Baseline Vascularity Predicts Responders to the Combination with Targeted Therapy or Immune Checkpoint Inhibition
Lüdemann WM, Kahn J, Herzler P, Collettini F, Savic LJ, Mohr R, Fehrenbach U, Auer TA, Gebauer B, Amthauer H, Wieners G
Journal of Hepatocellular Carcinoma 2025, 12:1-13
Published Date: 3 March 2026