Back to Journals » International Journal of Women's Health » Volume 18
Latent Profile Analysis and Predictors of Positive Psychological Capital in Patients Undergoing in vitro Fertilization-Embryo Transfer
Authors Yan Y, Ma Y, Xu L, Lv Y, Zhang X, Yu G
Received 14 March 2026
Accepted for publication 27 June 2026
Published 10 July 2026 Volume 2026:18 602396
DOI https://doi.org/10.2147/IJWH.S602396
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Yuying Yan, Ya Ma, Lidan Xu, Yuehong Lv, Xin Zhang, Gelin Yu
Department of Reproductive Endocrinology, Women’s Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuying Yan, Department of Reproductive Endocrinology, Women’s Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310000, People’s Republic of China, Tel +8613750882607, Email [email protected]
Purpose: To explore the classification characteristics of positive psychological capital in patients undergoing in vitro fertilization-embryo transfer (IVF-ET), and to analyze the differences in characteristics of different categories of positive psychological capital in women undergoing IVF-ET.
Methods: A total of 602 patients undergoing IVF-ET were selected using convenience sampling from the outpatient clinic of the Department of Reproductive Endocrinology at a tertiary Grade A obstetrics and gynecology hospital in mainland China between July 2025 and November 2025. On the day of embryo transfer, a general demographic questionnaire, the Kessler Psychological Distress Scale (K10), and the Positive Psychological Capital Questionnaire (PPQ) were administered. Latent profile analysis (LPA) was conducted to explore the potential classes of positive psychological capital in patients undergoing IVF-ET, and univariate analysis and multivariate logistic regression analysis were employed to identify the factors associated with these latent profiles.
Results: The positive psychological capital of IVF-ET patients could be categorized into three latent classes: the low psychological capital group (21.6%), the moderate psychological capital group (45.7%), and the high psychological capital group (32.7%). Multivariate logistic regression analysis results showed that age < 35 years (OR = 0.534, 95% CI: [0.316, 0.902], P < 0.05) and psychological distress (OR = 0.942, 95% CI: [0.911, 0.975], P < 0.05) were independent predictors of belonging to Class 2 compared to Class 1. Similarly, for Class 3 vs. Class 1, age < 35 years (OR = 0.361, 95% CI: [0.205, 0.637], P < 0.05) and psychological distress (OR = 0.857, 95% CI: [0.819, 0.897], P < 0.05) were significant predictors. Specifically, younger age (< 35 years) and higher psychological distress positively predicted the likelihood of being in the reference class (Class 1), indicating they are risk factors for lower positive psychological capital.
Conclusion: The positive psychological capital of IVF-ET patients can be categorized into three latent profiles. Clinical healthcare professionals should pay particular attention to patients who are younger (< 35 years) and experience higher levels of psychological distress, as they are more likely to exhibit lower levels of positive psychological capital. Tailored psychological screening and supportive strategies are recommended for these specific subgroups to potentially mitigate their psychological burden.
Keywords: IVF-ET, positive psychological capital, psychological distress, latent profile analysis, related factors
Introduction
In recent years, with changes in lifestyle, the impact of environmental factors, and the intensifying trend of late marriage and childbearing, infertility has become a global public health issue, severely threatening human reproductive health.1 As the most effective assisted reproductive technology (ART), in vitro fertilization and embryo transfer (IVF-ET) has been widely applied in clinical practice. However, IVF-ET is not only a complex medical technology but also a lengthy and uncertain treatment process, in which patients often endure immense psychological stress. Beyond the general burden of infertility, IVF-ET patients face unique and specific psychological challenges. The treatment is characterized by invasive medical procedures, strict daily regimens, and the recurrent trauma of potential implantation failure, which deprive patients of a sense of control over their own bodies and life trajectories.2 Studies3 indicate that IVF-ET patients generally suffer from varying degrees of anxiety and depression; these negative psychological states not only reduce the patients’ quality of life but may also affect treatment outcomes through neuroendocrine mechanisms.
Furthermore, the psychological well-being of IVF-ET patients cannot be separated from the broader context of their family and social environments. Furthermore, the psychological well-being of IVF-ET patients is inextricably linked to the broader context of their family and socio-cultural environments. Within the cultural context that emphasizes family traditions, childbearing is not merely an individual desire but a core familial obligation. Patients often endure immense intergenerational pressure from extended family members regarding lineage continuation.4 Simultaneously, the dynamic of the partner relationship is significantly strained; the shared burden of treatment decisions, financial costs, and the emotional rollercoaster of waiting for pregnancy test results can either unify or fracture the couple’s bond.5 These specific socio-cultural pressures and interpersonal dynamics significantly exacerbate the psychological vulnerability of IVF-ET patients.
Traditional psychological research has mostly focused on patients’ negative psychological states, such as anxiety and depression. However, with the rise of positive psychology, scholars have gradually shifted their attention to exploring individual positive psychological resources.6 Positive psychological capital refers to a positive psychological state exhibited by an individual during the process of growth and development, primarily consisting of four dimensions: self-efficacy, resilience, hope, and optimism. Among them, optimism refers to the tendency to make positive attributions and cognitions regarding past, present, and future events, and to maintain a positive psychological outlook over the long term; hope refers to the psychological process in which an individual steadfastly pursues goals and achieves them through agency and pathways thinking; resilience refers to the ability of an individual to adjust themselves in the face of adversity and setbacks, turning passivity into initiative to achieve recovery and growth; self-efficacy refers to the cognitive state in which an individual holds confidence in their ability to successfully complete a task when facing challenges or specific tasks, and is capable of positive self-assessment.7 While traditional positive psychology literature largely draws from general populations, the theory of positive psychological capital is of critical importance for IVF-ET patients specifically. According to the Conservation of Resources (COR) Theory, individuals strive to obtain, retain, and protect their resources.8 IVF-ET is a process characterized by continuous resource depletion, draining patients’ physical, emotional, and financial reserves. In this context, positive psychological capital serves as a vital internal resource reservoir: self-efficacy empowers patients to persevere through invasive procedures, hope sustains them through uncertain waiting periods, resilience facilitates recovery from failed cycles, and optimism helps reframe setbacks. Mobilizing these positive resources is essential to resist stress and prevent the psychological depletion triggered by treatment.9 Relevant studies indicate that the enhancement of positive psychological capital can promote effective coping with stressors and psychological adaptation in women undergoing IVF-ET,10 and positive psychological capital is closely related to psychological distress and fertility stress.11,12
However, due to the long duration and high uncertainty of IVF-ET treatment, patients are highly prone to falling into a vicious cycle of “resource loss.” Although our previous research has identified the latent profiles of alexithymia—a negative psychological trait—in this population,13 the heterogeneity of positive psychological resources remains unexplored. Currently, research on the positive psychological capital of IVF-ET patients remains scarce. Existing latent characteristic analyses of positive psychological capital primarily focus on non-IVF-ET populations, such as college students and cancer patients,14,15 while studies specifically targeting IVF-ET patients are rare. Therefore, exploring the latent characteristics of positive psychological capital in IVF-ET patients helps to fill the current research gap. Furthermore, in studies regarding the psychological status of IVF-ET patients, conventional practices are mostly limited to analyzing based on total or dimensional scores.16 Most existing studies lack in-depth exploration beyond simple statistical scoring of scales; they fail to deeply investigate the latent characteristics of positive psychological capital, thereby failing to fully account for the heterogeneity of this population. This, in turn, hinders clinical healthcare professionals from promptly adopting targeted interventions to promote patients’ mental health.
Latent profile analysis (LPA) is an individual-centered research method. Based on similar response patterns of observed variables, this method classifies the population into latent subgroups with distinct characteristics, thereby providing a basis for developing precise intervention strategies for different subgroups.17 In summary, exploring the latent characteristics and individual specificity of positive psychological capital in IVF-ET patients holds significant clinical implications for improving patients’ mental health and reproductive outcomes. Therefore, this study intends to employ latent profile analysis to identify the latent classes of positive psychological capital in IVF-ET patients and to deeply analyze their associated factors. By identifying patient subgroups with different psychological characteristics, this study aims to provide an empirical basis for clinical healthcare professionals to formulate differentiated psychological support strategies, and to offer references for targeted interventions aimed at enhancing patients’ positive psychological capital and alleviating psychological distress.
Materials and Methods
Research Subject
This study was conducted in Zhejiang Province, mainland China, from July 2025 to November 2025. The study participants were selected from a tertiary Grade A obstetrics and gynecology hospital. The inclusion criteria were: (1) age ≥20 years (in accordance with the legal marriage age regulations in mainland China, ie., not earlier than 22 years for males and 20 years for females); (2) married women; (3) suffering from infertility and undergoing IVF-ET treatment with the first embryo transfer; and (4) possessing basic literacy and communication skills, and able to complete the electronic questionnaire independently. The exclusion criteria were: (1) those with comorbid severe somatic diseases or a history of psychiatric disorders; and (2) those who canceled the transfer cycle. In addition, referring to relevant literature suggesting the minimum sample size (n=200) for latent profile analysis (LPA) modeling,18 the sample size of this study met the statistical requirements.
Tools
General Information Questionnaire
The General Information Questionnaire was designed by the research team to collect the demographic characteristics and clinical data of the subjects. The content mainly includes: ① Demographic characteristics: age, residence, education level, occupation, per capita monthly household income, and marital status; ② Clinical characteristics: cause of infertility, type of infertility, duration of infertility, source of semen, ART technology method, controlled ovarian stimulation protocol, number of oocytes retrieved, number of high-quality embryos, and number of embryos transferred; ③ Reproductive history: pregnancy history and history of abortion.
Positive Psychological Capital Questionnaire
This scale was originally developed by Luthans et al19 in 2007, and was later adapted by Zhang Kuo et al8 in 2008. It is primarily used to assess the level of an individual’s positive psychological resources, which refers to the positive psychological state possessed by the individual during growth, work, and when handling life challenges. It consists of 26 items divided into four dimensions: self-efficacy, resilience, hope, and optimism. The scale uses a 7-point Likert scoring method, and all items are positively scored; higher scores indicate a better level of positive psychological capital. This scale has demonstrated favorable construct validity and internal consistency reliability in Chinese populations, with Cronbach’s α coefficients for the subscales ranging from 0.77 to 0.92,8 and confirmatory factor analysis supports the rationality of psychological capital as a higher-order factor.5 Notably, the scale has been directly employed in Chinese assisted reproductive populations. Wu et al11 used the Psychological Capital Questionnaire among 185 hospitalized patients with ovarian hyperstimulation syndrome (OHSS) during IVF-ET cycles, reporting a mean psychological capital score of (120.05 ± 18.92) and acceptable internal consistency, further supporting its utility in this clinical context. In this study, the Cronbach’s α coefficient of the scale was 0.932.
The Kessler Psychological Distress Scale (K10)
This scale was originally developed by Kessler and Mroczek20 at the University of Michigan in 1992. It was introduced to China by Xu Lingzhong et al21 in 2005, followed by translation and cultural adaptation to form the Chinese version of the K10 scale. It is primarily used to assess the frequency and severity of psychological symptoms, such as anxiety and depression, experienced by individuals in the past 30 days. A 5-point Likert scoring method is adopted, with a total score ranging from 10 to 50 points; higher scores indicate more severe psychological distress in the patient. Based on the total score, psychological status is classified into four levels: (1) 10–15 points, indicating good mental health; (2) 16–21 points, indicating fair mental health; (3) 22–29 points, indicating poor mental health; and (4) 30–50 points, indicating severe mental health problems. The Chinese version of the K10 has demonstrated good reliability and validity in various Chinese populations. Wang et al22 validated the K10 in a large sample of 8602 Chinese healthcare professionals, reporting a Cronbach’s α of 0.952 and confirming a two-factor structure. Notably, the K10 has been directly employed in Chinese infertility populations. Jiang et al23 used the K10 among 595 Chinese women with infertility undergoing IVF-ET and reported a Cronbach’s α of 0.87, further supporting its utility in this clinical context. In this study, the Cronbach’s α coefficient of the scale was 0.932.
Data Collection
Data were collected via convenience sampling through offline on-site surveys at the hospital’s reproductive center by uniformly trained researchers from July to November 2025. We first explained the study’s purpose, significance, and confidentiality principles in detail to subjects who met the inclusion criteria. After obtaining written informed consent, we guided them to complete the questionnaires independently using pen and paper. All baseline questionnaires were administered to the participants prior to the embryo transfer procedure on the transfer day. Following the procedure, patients were followed up, and clinical pregnancy outcomes were assessed 30 to 35 days post-embryo transfer. A clinical pregnancy was defined as the presence of a gestational sac in the uterine cavity confirmed by transvaginal ultrasound.24 During the completion process, we answered non-leading questions regarding the items and immediately checked the questionnaires for completeness to ensure there were no omissions or errors. All completed questionnaires were verified on-site before collection, and data were entered into a database by two persons to ensure accuracy. A total of 638 questionnaires were distributed in this study. After excluding 36 invalid questionnaires with consistent answers, 602 valid questionnaires were finally recovered, yielding an effective response rate of 94.4%. This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Statistical Analysis
In this study, Mplus 8.3 software was used to perform latent profile analysis on the positive psychological capital of IVF-ET patients, and SPSS 25.0 software was used for general statistical data analysis. Using the items of the Positive Psychological Capital Questionnaire as observed indicators, latent profile models with 1 to 4 classes were sequentially constructed for fitting. Model fit evaluation indices included the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), sample-size adjusted BIC (aBIC), Entropy, the Lo-Mendell-Rubin Adjusted Likelihood Ratio Test (LMRT), and the Bootstrap Likelihood Ratio Test (BLRT). Smaller values for AIC, BIC, and aBIC indicate better model fit, balancing model accuracy and parsimony. Entropy measures the accuracy of classifying individuals into latent classes, ranging from 0 to 1; values closer to 1 indicate higher classification precision, and an Entropy ≥ 0.8 is generally considered acceptable LMRT and BLRT compare the fit of a model with k classes against a model with k‑1 classes; a statistically significant result (P < 0.05) indicates that the k‑class model fits significantly better than the k‑1 class model.25,26 Quantitative data conforming to a normal distribution were expressed as mean ± standard deviation (x ±s), while qualitative data were expressed as frequency and percentage (%). Intergroup comparisons were conducted using the Chi-square test (χ2 test) or Fisher’s exact probability method. Multivariate logistic regression analysis was performed using the optimal classification result from the latent profile analysis as the dependent variable and variables showing statistical significance in univariate analysis as independent variables. All tests set a two-sided significance level of α=0.05.
Results
Participant Characteristics
In this study, a total of 602 IVF-ET patients were included, with an average age of (32.99 ± 4.52) years. There were 392 cases (65.1%) younger than 35 years. Other detailed information is shown in Table 1. Additionally, the scores for positive psychological capital and psychological distress of IVF-ET patients are also presented in Table 2.
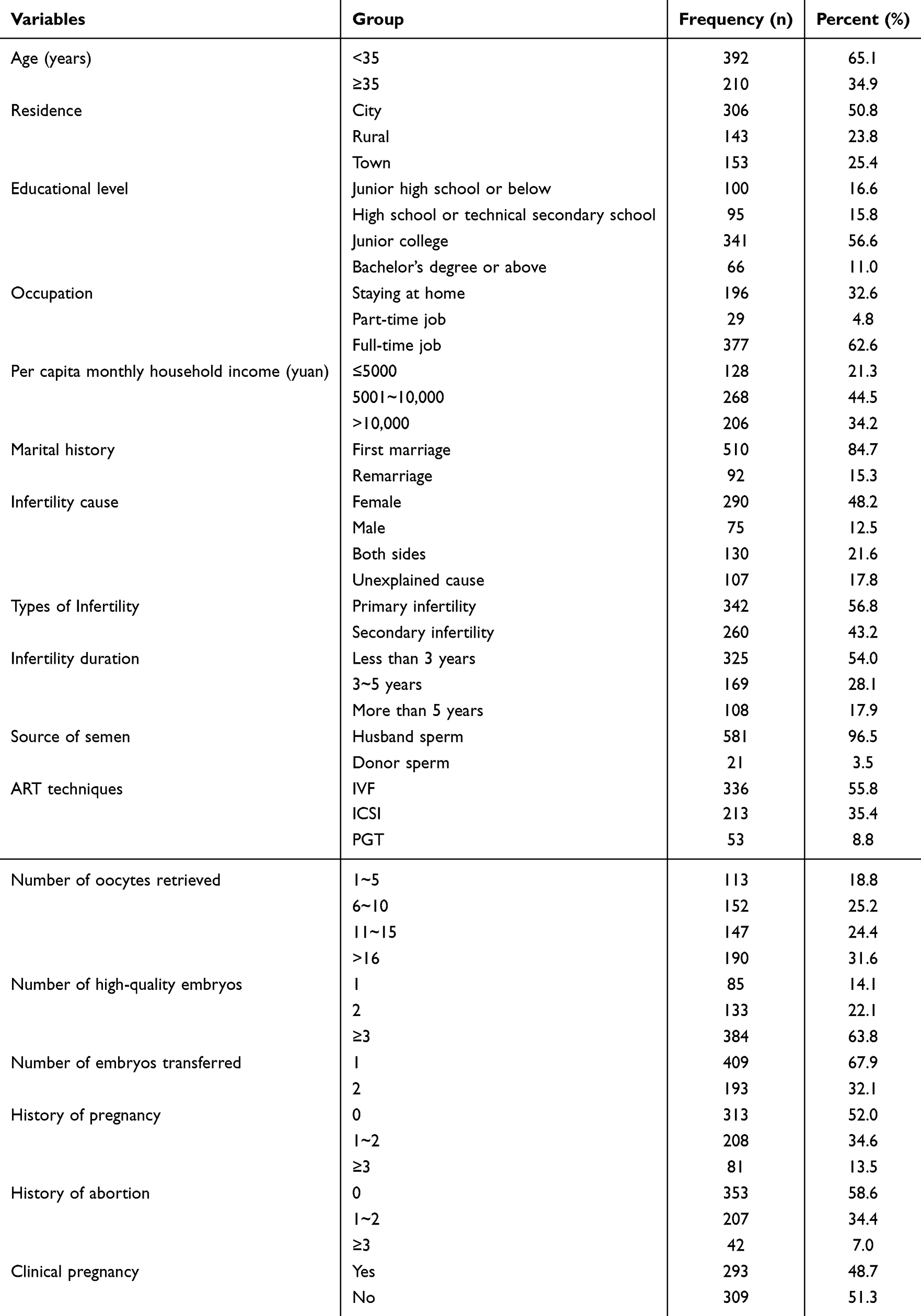 |
Table 1 General Information Questionnaire (N=602) |
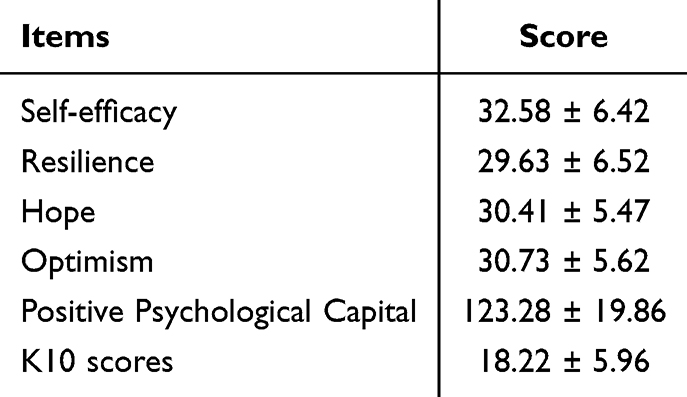 |
Table 2 Scores of Positive Psychological Capital and Psychological Distress in IVF-ET Patients (n=602, |

LPA of Positive Psychological Capital in IVF-ET Patients
LPA was performed based on the scores of the 26 items of the Positive Psychological Capital Scale, fitting a total of 1 to 4 models, as shown in Table 3. When the number of classes increased from 1 to 3, all information criteria (AIC, BIC, aBIC) decreased progressively, and both LMRT and BLRT were statistically significant (all P < 0.05), indicating that the 3‑class model was superior to the 2‑class model. When the number of classes was 4, although the AIC, BIC, and aBIC values continued to decrease slightly and the entropy was 0.925, the LMRT P‑value was not statistically significant (P > 0.05), suggesting that adding a fourth class did not significantly improve model fit. Therefore, based on the combined criteria (lower information criteria, entropy ≥ 0.8, significant LMRT and BLRT for the 3‑class solution, and non‑significant LMRT for the 4‑class solution), the 3‑class model was selected as the optimal latent profile model for positive psychological capital in IVF‑ET patients. The probabilities of IVF-ET patients in each category belonging to their corresponding latent categories were 0.215, 0.456, and 0.327, respectively, indicating that the 3-category latent profile model has high reliability. The latent profile plot was drawn based on the classification results of the three latent categories, as shown in Figure 1.
 |
Table 3 Latent Class Indicators of Positive Psychological Capital in IVF-ET Patients |
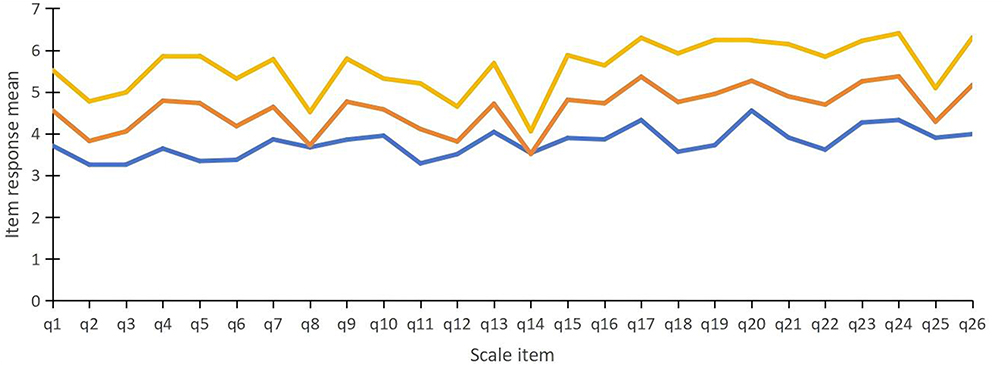 |
Figure 1 Characteristic distribution of three latent classes of positive psychological capital in IVF-ET patients. Notes: Blue represents Group C1 (Low psychological capital group, 21.6%); Orange represents Group C2 (Moderate psychological capital group, 45.7%); and yellow represents Group C3 (High psychological capital group, 32.7%). |
Figure 1 shows the item scores of positive psychological capital across the three categories. Among them, Class C1 consisted of 130 cases (21.6%). The positive psychological capital score for IVF-ET patients in this category was (97.86 ± 9.34), which was below the moderate level of positive psychological capital; therefore, this category of IVF-ET patients was named the “low psychological capital group.” Class C2 consisted of 275 cases (45.7%). The positive psychological capital score for IVF-ET patients in this category was (119.40 ± 7.36), which was between the low and high scoring groups and close to the median of the theoretical total score; therefore, this category of IVF-ET patients was named the “moderate psychological capital group.” Class C3 consisted of 197 cases (32.7%). The positive psychological capital score for IVF-ET patients in this category was (145.48 ± 11.45), which was significantly higher than the other two groups and close to the upper limit of the theoretical total score; therefore, this category of IVF-ET patients was named the “high psychological capital group.”
Comparison of General Data and Psychological Distress Characteristics Among Different Profiles of Positive Psychological Capital in IVF-ET Patients
The results of the univariate analysis are shown in Table 4. Differences in the distribution of the three latent profiles of positive psychological capital were statistically significant for age (χ2=12.094), place of residence (χ2=9.579), per capita monthly household income (χ2=14.981), duration of infertility (χ2=15.291), and history of pregnancy (χ2=11.995) (all P<0.05).
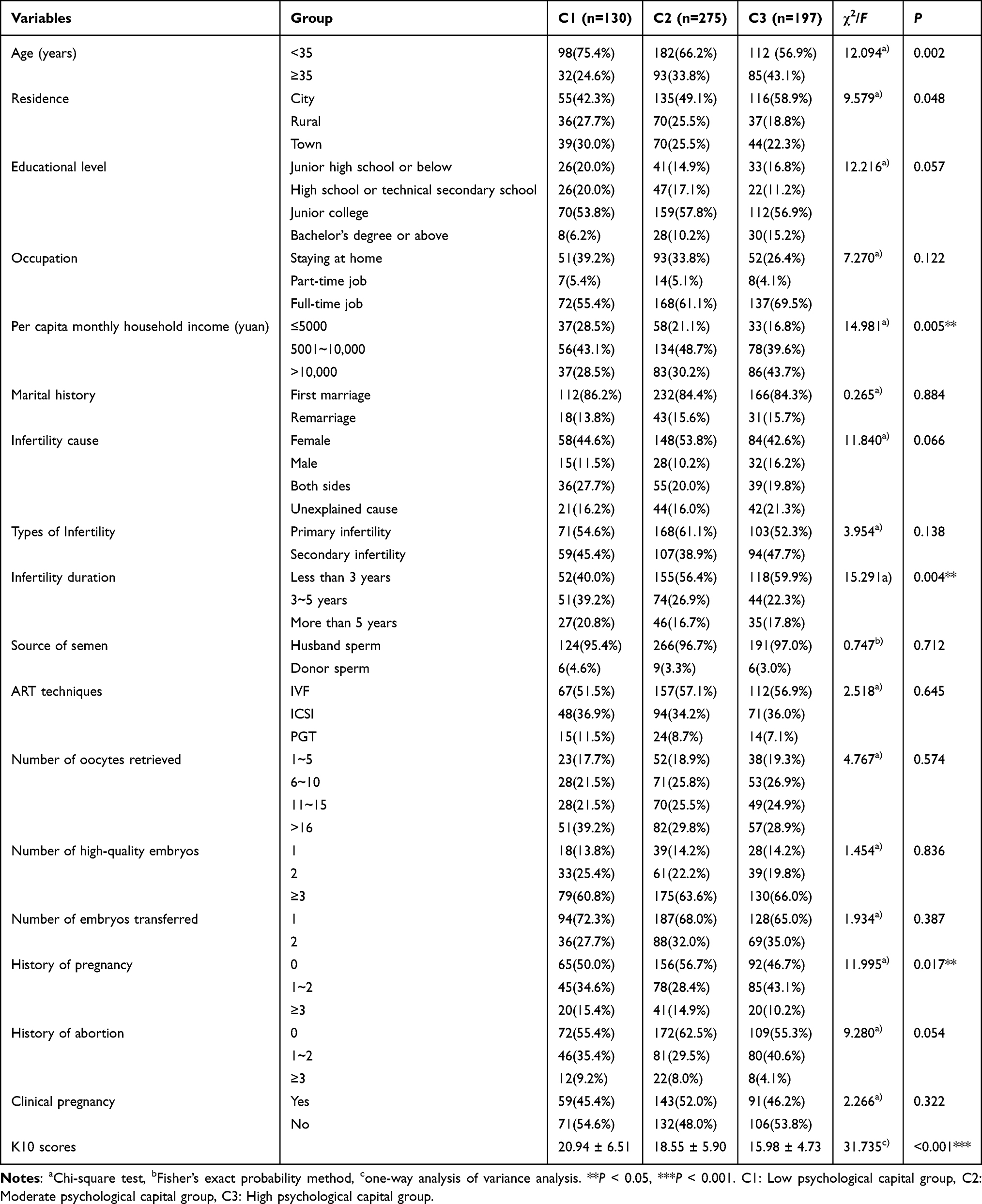 |
Table 4 Comparison of General Data and Psychological Distress Characteristics Among Different Profiles of Positive Psychological Capital in IVF-ET Patients |
Multivariate Analysis of Latent Profiles of Positive Psychological Capital in IVF-ET Patients
Taking the three latent profiles of positive psychological capital in IVF-ET patients as the dependent variable, with the low psychological capital group as the reference group, indicators with statistical significance in the univariate analysis were included as independent variables, and self-efficacy score was included as a covariate for multivariate Logistic regression analysis. The results are shown in Table 5. Comparing the “low psychological capital group” and the “moderate psychological capital group,” IVF-ET patients aged <35 years (OR=0.534) were more likely to fall into the “low psychological capital group” (P<0.05), while patients with lower psychological distress scale scores (OR=0.942) were more likely to fall into the “moderate psychological capital group” (P<0.05). Comparing the “low psychological capital group” and the “high psychological capital group,” IVF-ET patients aged <35 years (OR=0.361) were more likely to fall into the low psychological capital group (P<0.05), while patients with lower K10 scores (OR=0.857) were more likely to fall into the “high psychological capital group” (P<0.05).
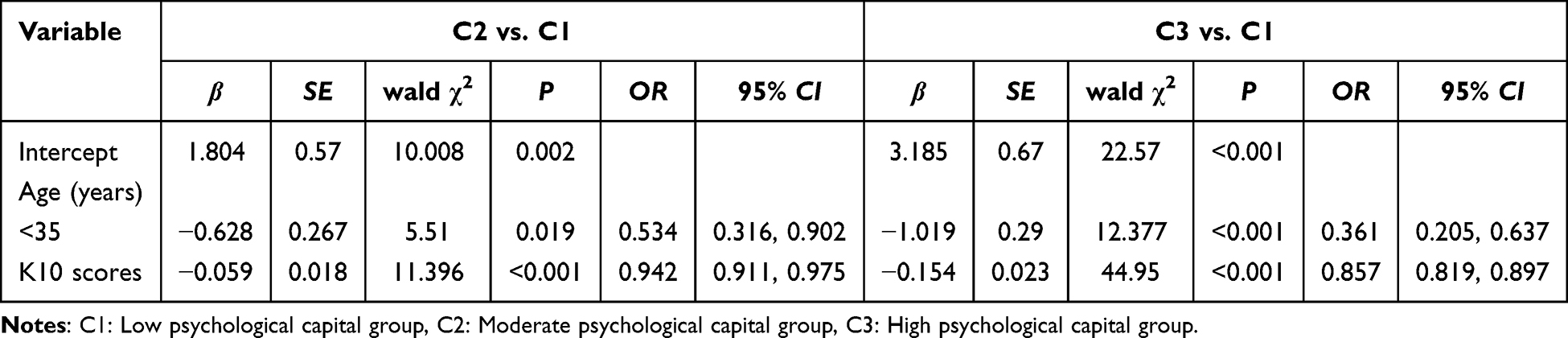 |
Table 5 Multiple Logistic Regression Analysis of Different Profiles of Positive Psychological Capital in IVF-ET Patients |
Discussion
This study investigated the current status of positive psychological capital among 602 IVF-ET patients, identified three subgroups using latent profile analysis, and further analyzed the key factors influencing these subgroups. This study provides a scientific reference and empirical evidence for targeted improvement of positive psychological capital in such patients.
Analysis of the Current Status of Positive Psychological Capital in IVF-ET Patients
The results showed that the positive psychological capital score of the 602 IVF-ET patients was (123.28 ± 19.86), which is at a moderate level. This is similar to the results (120.05 ± 18.92) of a survey conducted by Wu et al11 in 2023 on patients hospitalized for OHSS after IVF-ET in mainland China. As a serious iatrogenic complication of assisted reproductive technology, OHSS is often accompanied by severe abdominal pain, abdominal distension, and even dyspnea, causing patients to endure significant physiological suffering.27 The similarity in psychological capital levels between the sample of this study and the special group of hospitalized OHSS patients suggests that although the patients in this study did not experience serious complications such as hospitalization for OHSS, IVF-ET, as a long-term stressor characterized by uncertainty, invasive procedures, and excessive concern about reproductive outcomes, continuously consumes patients’ psychological resources. This status highlights that in clinical nursing, attention must be paid not only to physiological indicators but also to the assessment and cultivation of patients’ positive psychological resources. However, the fact that the positive psychological capital score of IVF-ET patients is at a moderate level indicates that these patients have not completely fallen into a psychological predicament. Despite bearing immense reproductive pressure, most patients still retain basic self-efficacy, hope, and resilience. This “moderate level” of psychological capital may provides a favorable foundation and an entry point for clinical intervention. It implies that patients’ psychological resources are not exhausted but are in a state “awaiting activation.” Given the current status of insufficient resource reserves on the day of transplantation, clinical nursing could focus on the “pre-transplantation preparation period” as a critical intervention window to implement immediate resource supplementation measures. Based on previous studies, targeted psychological interventions such as mindfulness therapy28 and dyadic coping29 might help patients tap into their potential psychological strength and possibly elevate their psychological capital from a moderate level to a higher level, which may in turn enhance their adaptability to cope with treatment challenges. However, because the present study did not assess post‑intervention changes, these suggestions remain hypothetical and require testing in future longitudinal or intervention studies.
In this study, the dimensions of positive psychological capital were ranked from highest to lowest as follows: self-efficacy, optimism, hope, and resilience. This differs from the ranking of self-efficacy, resilience, optimism, and hope found in other studies,30 with the discrepancy primarily manifesting in the relative lag of the resilience dimension. This finding suggests an association between long-term treatment pressure and lower resilience scores in this specific population, although causality cannot be inferred due to the cross-sectional design. Although patients still maintain high treatment expectations (optimism and hope), their psychological resilience system is relatively fragile, providing a theoretical basis for formulating targeted psychological intervention measures. In clinical practice, healthcare professionals may consider focusing on identifying and strengthening patients’ psychological resilience. While fully utilizing their higher self-efficacy and treatment expectations (optimism, hope) as intervention advantages, emphasis could be placed on helping patients build buffering mechanisms to cope with setbacks through targeted psychological counseling and resilience training,31 with the goal of enhancing their overall mental health level. Future research is needed to determine whether such interventions effectively improve resilience and clinical outcomes.
Positive Psychological Capital in IVF-ET Patients Can Be Categorized into Three Latent Classes
It is worth noting that our research team previously conducted a latent profile analysis focusing on alexithymia among IVF-ET patients.13 While both studies utilize LPA to explore the heterogeneity of psychological characteristics in this population, the current study extends our previous work by shifting the focus from negative psychological traits to positive psychological resources. Unlike alexithymia, which represents a deficit in emotional processing, positive psychological capital reflects a positive psychological state of development. This shift in perspective is significant because identifying distinct profiles of positive psychological capital allows for strength-based interventions aimed at enhancing resilience, rather than solely focusing on mitigating deficits. Furthermore, the predictors associated with positive psychological capital profiles in this study differ from those identified in the alexithymia study, providing a more comprehensive understanding of the psychological dynamics experienced by IVF-ET patients. Thus, the current study serves as a necessary complement to our previous findings, offering novel insights for positive psychological nursing interventions.
The results showed that there was significant individual heterogeneity in the positive psychological capital of IVF-ET patients, which could be classified into three latent categories. Among them, 197 IVF-ET patients (32.7%) belonged to the high psychological capital group, indicating that this population possessed abundant reserves of psychological resources. Based on their self-reported responses, they appeared to effectively regulate anxiety and stress during assisted reproduction treatment and actively cope with various challenges in the treatment process. A total of 275 IVF-ET patients (45.7%) belonged to the moderate psychological capital group, indicating that while this population possessed a certain degree of psychological adaptability, their optimistic attitude or resilience to stress might fluctuate when facing the repeatability and uncertainty of treatment, leaving considerable room for psychological improvement. Additionally, 130 IVF-ET patients (21.6%) belonged to the low psychological capital group, indicating that this population had low levels across all four dimensions of self-efficacy, optimism, hope, and resilience. They lacked internal motivation and buffering mechanisms to cope with difficulties and reported being highly prone to feelings of helplessness and frustration; this deficiency in psychological resources may be associated with lower treatment adherence and quality of life, although the cross-sectional design prevents causal conclusions. These findings suggest that clinical medical staff could consider identifying differences in psychological capital levels among different categories of IVF-ET patients as early as possible and potentially implement graded, personalized psychological nursing interventions aimed at enhancing the overall level of positive psychological capital in patients. Future longitudinal or intervention studies are needed to determine whether such targeted approaches lead to improved patient outcomes.
Based on these identified latent profiles, we propose the following potential strategies for tailored psychological interventions: (1) For the high psychological capital group, clinical staff could focus on maintenance and empowerment—providing minimal but supportive interventions to sustain their resilience and serve as role models for other patients. (2) For the moderate psychological capital group, targeted counseling approaches might aim to stabilize and elevate their psychological resources. Specific strategies such as group-based cognitive-behavioral therapy (CBT) sessions to address treatment-related uncertainty. (3) For the low psychological capital group, intensive and individualized psychological support may be considered. Recommended approaches could include one-on-one CBT tailored to infertility-related distress, psychoeducation to build hope and self-efficacy, stress management techniques, and regular emotional check-ins to prevent dropout. These patients might also benefit from referral to specialized mental health services when needed. In summary, clinical staff could consider identifying differences in psychological capital levels among different categories of IVF-ET patients as early as possible and potentially implement these graded, personalized psychological nursing interventions with the goal of enhancing the overall level of positive psychological capital in patients. However, because the present study is cross-sectional, the proposed interventions should be viewed as hypothesis-generating suggestions that require testing in future longitudinal or intervention studies before they can be recommended for routine clinical practice.
Related Factors of Latent Classes of Positive Psychological Capital in IVF-ET Patients
The results of this study indicated that age is a factor associated with the psychological capital of IVF-ET patients (P<0.05); that is, as the patient’s age decreases, the likelihood of being in the low psychological capital level is often higher. This finding initially appears counterintuitive, as younger patients typically have better physiological reserves and higher fecundity. However, this association can be explained by the specific psychosocial context of Chinese IVF-ET patients. This is consistent with the results of previous studies.32 From the perspective of the COR theory, younger patients often face multiple competing demands: many are in the early stages of their careers, experience greater work–treatment conflicts, and may have limited life experience to cope with repeated treatment failures. Additionally, in traditional Chinese culture, younger married women may encounter intense family pressure to conceive early, which paradoxically heightens their psychological vulnerability. To further explore this seemingly counterintuitive finding, future studies could examine whether factors such as work–family conflict, perceived social support, or fertility-related stigma mediate or moderate the relationship between age and psychological capital. Qualitative interviews with younger IVF-ET patients may also help elucidate the specific sources of distress. Although younger patients have the advantage in terms of physiological function, many of them are in the rising stage of their careers and face more severe conflicts between work and treatment. Furthermore, the contradiction between high expectations regarding the timing of fertility and the uncertainty of assisted reproduction exacerbates their psychological burden. Compared with older patients, the younger group is relatively lacking in life experience and psychological resilience. Thus, younger age is associated with a higher risk of low psychological capital, rather than being a protective factor. When facing treatment setbacks, they lack mature coping mechanisms, which is associated with lower self-efficacy and hope levels, corresponding to a state of lower psychological capital. Based on this finding, we suggest that clinical staff could prioritize younger patients for early psychological screening and intervention. For this high-risk group, the following evidence-based strategies may be considered: (1) At the beginning of the cycle or before transplantation, a 0–10 point Numeric Rating Scale (NRS) could be used for rapid psychological risk stratification combined with a brief assessment of work–family conflict.33 (2) For younger patients identified as high-risk, structured problem-solving therapy (PST) might be offered, which has been shown to effectively reduce distress and improve coping in fertility patients.34 (3) Mindfulness-based interventions delivered via mobile health applications may increase accessibility for this demographic. If implemented, these graded, evidence-supported interventions may help younger patients build psychological resources and potentially improve their treatment experience. However, because the present study is cross-sectional, the effectiveness of these suggested strategies requires testing in future longitudinal or intervention studies before they can be recommended for routine clinical practice.
The results of this study showed that, compared with the moderate and high psychological capital groups, IVF-ET patients with higher psychological distress scale scores were more likely to fall into the low psychological capital group. This is consistent with the research results of Zhou et al12 This finding indicates a negative association between psychological distress and psychological capital, aligning with the COR theory,34 which suggests that chronic emotional distress may be associated with depletion of cognitive and emotional resources, potentially reducing the capacity to maintain positive psychological states. Patients with infertility often face enormous psychological pressure and are commonly accompanied by anxiety, depression, fear, and worry about treatment failure.35 Psychological distress has been reported to affect nearly half of infertility patients.36 From the perspective of resource consumption, IVF-ET patients remain under prolonged treatment pressure, and symptoms of psychological distress may consume individual cognitive and emotional resources. Consequently, these patients might have fewer resources to sustain positive psychological capital, making them more likely to be classified into the low psychological capital group. However, due to the cross-sectional design of this study, we cannot determine the direction or causality of this association; it is possible that low psychological capital also increases vulnerability to psychological distress, or that the two mutually reinforce each other over time. This result suggests that clinical professionals, when selecting entry points for psychological intervention, could consider both reducing psychological distress and enhancing positive psychological capital. Based on existing evidence-based strategies, we suggest the following potential approaches: (1) routine screening for psychological distress, eg., using the K10, at the start of the IVF cycle, followed by referral to interventions such as cognitive-behavioral therapy (CBT) or mindfulness-based stress reduction (MBSR), which have been shown to reduce distress in fertility populations; (2) offering positive psychology interventions, eg., hope-building and resilience training, to directly enhance psychological capital; (3) implementing a stepped-care model that provides basic psychoeducation to all patients and more intensive, tailored support to those with elevated distress or low capital. However, because the present study is cross-sectional, these suggestions should be viewed as hypothesis-generating, and their effectiveness requires testing in future longitudinal or intervention studies. Future longitudinal studies are needed to examine the temporal dynamics between psychological distress and psychological capital and to test whether improving psychological capital is associated with improved clinical outcomes.
Cultural Considerations, Generalizability, and the Broader Psychosocial Context
The present study was conducted in mainland China, where cultural factors may influence patients’ psychological responses and the applicability of the Positive Psychological Capital Questionnaire. In traditional Chinese culture, fertility is closely linked to family continuity, filial piety, and marital stability, which can intensify the psychological burden of infertility. Compared with Western populations, Chinese IVF-ET patients may experience additional stigma, social pressure from extended family, and a greater sense of personal failure. These culturally shaped responses may affect how patients interpret Positive Psychological Capital Questionnaire items, particularly those related to self-efficacy and hope. Thus, while the Positive Psychological Capital Questionnaire has been validated in Chinese populations, Similarly, our three-profile structure and associated factors may not be directly generalizable to populations with different cultural norms or healthcare systems. Future cross-cultural studies are needed to determine whether similar profiles emerge elsewhere and whether tailored interventions require cultural adaptation.
Moreover, a recent comprehensive review by Ribeiro Neto et al37 highlights the emotional, social, and ethical challenges of infertility and ART. These findings align with our observation that many IVF-ET patients possess moderate to high levels of positive psychological capital, suggesting that psychological resources can buffer treatment-related distress. The review also reinforces the need for integrated mental health support that considers ethical, social, and emotional factors-a perspective that complements our proposal for tailored interventions based on positive psychological capital profiles. Incorporating this broader framework deepens understanding of the multifaceted psychological impacts of ART and supports the development of more comprehensive, patient-centered care models.37
Limitations
This study has certain limitations. First, the use of convenience sampling and a single-center design clearly limits the external validity of the findings. Due to time and geographical constraints, this cross-sectional survey was conducted only at a tertiary Grade A obstetrics and gynecology hospital in mainland China. This sampling method introduces potential biases, including selection bias and limited sample representativeness, which may restrict the generalizability of the research conclusions to a broader population. Second, there is significant selection bias in the study subjects. The included sample was mainly restricted to patients undergoing IVF-ET treatment and preparing for embryo transfer. Therefore, the results are difficult to generalize to the entire IVF-ET population, especially those who canceled their cycles due to failure to obtain transferable embryos, complications such as Ovarian Hyperstimulation Syndrome (OHSS), or early treatment failure. These negative events often have a major impact on the psychological state of patients, resulting in the psychological capital levels of the excluded groups potentially being significantly lower than those of the sample in this study; this is an important limitation of the current study. Furthermore, although our inclusion criteria specified “first embryo transfer,” we did not systematically collect detailed historical data regarding prior failed stimulation attempts or cycle cancellations. Given that these prior treatment burdens could profoundly impact patients’ psychological states, the absence of these IVF-specific variables may obscure the nuanced impact of previous treatment failures. Third, the cross-sectional design of this study inherently limits causal inferences. While we identified associations between various factors and positive psychological capital, we cannot determine causality or the direction of effects. Additionally, because psychological assessments were performed at a single time point on the day of embryo transfer, the findings may capture transient emotional responses related to that specific stage of treatment rather than entirely stable psychological characteristics. Fourth, this study relied entirely on self-report measures, which may introduce response biases such as social desirability bias, recall bias, and common method variance. These biases could potentially inflate or distort the observed relationships between variables, affecting the accuracy and reliability of the findings. Fifth, the study is currently exploratory and hypothesis-generating in nature. Although we did follow up on reproductive outcomes, the overall study design remains cross‑sectional. Consequently, we cannot draw causal conclusions about whether positive psychological capital influences subsequent clinical outcomes, which limits the immediate clinical applicability of our findings. Additionally, the absence of an external validation sample further constrains the generalizability of the results.
Given these limitations, future research should not only conduct multicenter, randomized sampling studies across different regions with longitudinal designs to track dynamic changes in positive psychological capital, but also implement intervention studies to test the effectiveness of tailored psychological support programs based on individual positive psychological capital profiles. Additionally, future studies should explore other potential influencing factors beyond those examined here, such as social support (eg., partner support, family support, peer support from other patients) and cultural beliefs (eg., attitudes toward assisted reproduction, filial piety expectations, or fertility-related stigma), which may moderate or mediate the relationships observed in this study. Incorporating these factors would provide a more comprehensive understanding of positive psychological capital in the IVF-ET population and inform the development of culturally sensitive, evidence-based psychological interventions. This would provide stronger evidence for promoting patient mental health.
Conclusion
The overall positive psychological capital of IVF-ET patients is at a moderate level, and there is significant heterogeneity within the group, which can be categorized into three latent classes: the low psychological capital group, the moderate psychological capital group, and the high psychological capital group. This finding indicates that while most patients possess certain psychological resources, a considerable proportion of patients (especially those in the low group) are in a state of depleted psychological resources and are in urgent need of attention. Age and psychological distress are key factors influencing the latent classification of positive psychological capital in IVF-ET patients. Clinical medical staff should use the dual indicators of age and psychological distress levels to early identify the high-risk population belonging to the “low psychological capital group,” and move away from the traditional “one-size-fits-all” intervention model to instead implement graded, categorized, and precise psychological intervention strategies. By focusing on alleviating patients’ psychological distress and enhancing their psychological resilience, the psychological environment for assisted reproduction can be effectively improved, thereby enhancing treatment outcomes and quality of life.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request but are not publicly available due to privacy and ethical restrictions.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from the Ethics Committee of Women’s Hospital, Zhejiang University School of Medicine (No. IRB-20250235-R). Written informed consent was obtained from all participants before the survey was conducted.
Acknowledgments
We are grateful to all the participants and researchers who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Medical and Health Science Program of Zhejiang Province (Grant No.2024KY1154 and Grant No.2025HY0492).
Disclosure
Yuying Yan and Ya Ma are-co-first authors for this study. The authors declare no conflicts of interest in this work.
References
1. Kitchen H, Aldhouse N, Trigg A, et al. A review of patient-reported outcome measures to assess female infertility-related quality of life. Health Qual Life Outcomes. 2017;15(1):86. doi:10.1186/s12955-017-0666-0
2. Ma J, Gao W, Li D. Recurrent implantation failure: a comprehensive summary from etiology to treatment. Front Endocrinol. 2023;13:1061766. doi:10.3389/fendo.2022.1061766
3. Zhou Y, Sun Z, Song J. Research progress on the impact of anxiety and depression on embryo transfer outcomes of in vitro fertilization. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2023;52(1):61–15. doi:10.3724/zdxbyxb-2022-0473
4. L GA, Slauson‐Blevins K, McQuillan J. The experience of infertility: a review of recent literature. Sociol Health Illness. 2010;32(1):140–162.
5. Bokek-Cohen Y, Turgeman-Lupo K, Miller N, Wiser A, Haikin‐Herzberger E. A holistic evaluation of multiple well-being dimensions in IVF patients and their spouses: a cross-sectional study informed by a dyadic approach. Int J Gynaecol Obstet. 2025;171(3):1408–1413. doi:10.1002/ijgo.70324
6. Kong L, Fang M, Ma T, et al. Positive affect mediates the relationships between resilience, social support and posttraumatic growth of women with infertility. Psychol Health Med. 2018;23(6):707–716. doi:10.1080/13548506.2018.1447679
7. Luthans F, Youssef C, Avolio B. Psychological Capital. New York: Oxford University Press; 2007.
8. Zhang K, Sai Z, Yinghong D. Positive psychological capital: measurement and relationship with mental health. Studies Psychol Behav. 2010;8(1):58–64.
9. Wu Y, Y HJ, Zhu J, et al. Psychological capital mediates the impact of psychological distress on fertility-related quality of life in IVF patients: a Cross-Sectional Study in China. doi:10.21203/rs.3.rs-6886103/v1
10. Song DN, Hu S, Pu CS, et al. Analysis of influencing factors on the trajectories of psychological symptom clusters in pregnant women with assisted reproductive technology and nursing. Chin J Nurs. 2025;60(10):1209–1216. doi:10.3761/j.issn.0254-1769.2025.10.009
11. Wu W, Zhou N, He Y. Correlation between fertility stress, psychological capital, and conjugal communication patterns in hospitalized patients with ovarian hyperstimulation syndrome during in vitro fertilization-embryo transfer cycles. Int J Womens Health. 2025;17:2819–2832. doi:10.2147/IJWH.S537423
12. Zhou H, Peng J, Wang D, et al. Mediating effect of coping styles on the association between psychological capital and psychological distress among Chinese nurses: a cross-sectional study. J Psychiatr Ment Health Nurs. 2017;24(2–3):114–122. doi:10.1111/jpm.12350
13. Yan Y, Xu L, Ma Y, et al. In vitro fertilization-embryo transfer patients with alexithymia and its influencing factors: a potential profile analysis. Int J Womens Health. 2025;17:5209–5221. doi:10.2147/IJWH.S552324
14. Li R, Zhou W, Wu J. Identifying the subtypes of psychological profiles in senior undergraduate nursing students and its relationship with academic performance: a latent class analysis. J Prof Nurs. 2021;37(4):757–764. doi:10.1016/j.profnurs.2021.04.011
15. Tao XQ, Wu QC, Wei X, et al. Fear of progression and its associated factors among patients with positive lung cancer screening results: a latent profile analysis. Nurs Health Sci. 2025;27(3):e70176. doi:10.1111/nhs.70176
16. Xu XF, My XUE, Lv GR, et al. Mediating effect of psychological capital on mindfulness and psychological distress among men in infertile couples. J Shandong Univ. 2019;57(2):105–109. doi:10.6040/j.issn.1671-7554.0.2018.955
17. Lönnqvist K, Sinervo T, Kaihlanen AM, et al. Psychosocial work characteristics and sleep quality among early career registered nurses: a cross-sectional latent profile analysis. BMC Health Serv Res. 2023;23(1):1020. doi:10.1186/s12913-023-09949-9
18. Nguena Nguefack HL, Pagé MG, Katz J, et al. Trajectory modelling techniques useful to epidemiological research: a comparative narrative review of approaches. Clin Epidemiol. 2020;12:1205–1222. doi:10.2147/CLEP.S265287
19. Luthans F, Avolio BJ, Avey JB, et al. Positive psychologicalcapital:measurement and relationship with performance andsatisfaction. Personnel Psychol. 2007;60(3):541–572. doi:10.1111/j.1744-6570.2007.00083
20. Kessler RC, Andrews G, Colpe LJ, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychological Medicine. 2002;32(6):959–976. doi:10.1017/S0033291702006074
21. Xu LZ, Wang JX, H S, et al. Application of Kessler 10 and its significance. Soft Sci Health. 2005;19(6):410–412. doi:10.6040/j.issn.1671-7554.0.2018.955
22. Wang Y, Zeng Z, Huang C, et al. Large-scale validation of the Kessler-10 Scale’s psychometric properties among healthcare professionals in China. General Hospital Psychiatry. 2025;94:112–117. doi:10.1016/j.genhosppsych.2025.02.017
23. Jiang Z, Hou S, Zhang Y, Zong L. The mediating and moderating effects of resilience on the relationship between sleep quality and psychological distress in Chinese women with infertility. BMC Women’s Health. 2024;24(1):192. doi:10.1186/s12905-024-03018-x
24. Nelen WL, van der Pluijm RW, Hermens RP, et al. The methodological quality of clinical guidelines of the European society of human reproduction and embryology (ESHRE). Hum Reprod. 2008;23(8):1786–1792. doi:10.1093/humrep/den120
25. Li M, Harring JR. Investigating approaches to estimating covariate effects in growth mixture modeling: a Simulation Study. Educ Psychol Meas. 2017;77(5):766–791. doi:10.1177/0013164416653789
26. da Silva Castanheira K, Zahedi N, Miočević M. Bayesian mediation analysis in trauma research. Psychol Trauma. 2024;16(1):149–157. doi:10.1037/tra0001439
27. Humaidan P, Quartarolo J, Papanikolaou EG. Preventing ovarian hyperstimulation syndrome: guidance for the clinician. Fertil Steril. 2010;94(2):389–400. doi:10.1016/j.fertnstert.2010.03.028
28. Shorey S, Ng ED. The efficacy of mindful parenting interventions: a systematic review and meta-analysis. Int J Nurs Stud. 2021;121:103996. doi:10.1016/j.ijnurstu.2021.103996
29. Brandão T, Schulz MS, Matos PM. Psychological intervention with couples coping with breast cancer: a systematic review. Psychol Health. 2014;29(5):491–516. doi:10.1080/08870446.2013.859257
30. Zhong ZK, Liu L, Zhou L, et al. Latent profile analysis of psychological capital among student nurses and its relationship with career support. Chongqing Med. 2025;54(05):1268–1270. doi:10.3969/j.issn.1671-8348.2025.05.041
31. Wang X, Yang M, Zhang Y, et al. How resilience mitigates depression after IVF-ET failure: a moderated mediation model of hope, social relations, and income in China. Int J Womens Health. 2025;17:3865–3879. doi:10.2147/IJWH.S549816
32. Liao L. Correlation Study on Positive Psychological Capital, Social Capital, and Health-Promoting Behaviors Among Elderly People in Nursing Homes in Xiangxi Region. Jishou University; 2025; doi:10.27750/d.cnki.gjsdx.2025.000655
33. Gana K, Jakubowska S. Relationship between infertility-related stress and emotional distress and marital satisfaction. J Health Psychol. 2016;21(6):1043–1054. doi:10.1177/1359105314544990
34. Hobfoll SE. Conservation of resources theory: its implication for stress, health, and resilience. The Oxford Handbook of Stress, Health, and Coping. 2011;127:147.
35. Hu L, Yuan Y, Li Y, et al. Prevalence and risk factors of negative emotions in infertile women: a systematic review and meta-analysis. Front Public Health. 2025;13:1701381.
36. Kong LH. Construction of Dyadic Interaction Model of Emotional Distress and Its Influencing Factors Among Infertile Couples[D]. Shandong University; 2017.
37. Ribeiro Neto B, Barreiro M, Tomé A, Vale-Fernandes E. Psychosocial aspects of infertility and the impact of assisted reproductive techniques - a comprehensive review. JBRA Assist Reprod. 2025;29(2):378–393. doi:10.5935/1518-0557.20250002
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Coping Profiles and Differences in Psychological Distress and Quality of Life in Clients Undergoing Assisted Reproductive Techniques: A Latent Profile Analysis
Bai J, Zheng J, Guo N, Dong Y, Wang K, Cheng C, Jiang H, Qian L
Journal of Multidisciplinary Healthcare 2024, 17:533-540
Published Date: 5 February 2024
Psychological-Symptom Mismatch Phenotypes and Their Clinical Implications in Patients with Chronic Obstructive Pulmonary Disease
Cai Y, Ren X, Wang K, Cheng H
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:593901
Published Date: 11 June 2026
Development and Validation of a Nomogram to Identify and Predict High-Distress Psychosocial Phenotypes in Tinnitus Patients: A Latent Profile Analysis
Xu X, Xiao S, Li X, Niu Y, Cen S, Chang Z, Liu C, Zhang L, Zhang X, Liu F
Psychology Research and Behavior Management 2026, 19:614795
Published Date: 26 June 2026