Back to Journals » Patient Preference and Adherence » Volume 20
Knowledge, Attitudes, and Practices on Antihypertensive Therapy Among Older Patients with Hypertension: Structural Equation Modeling Analysis
Authors Li S, Zhang H, Zhang J, Liu X
Received 29 April 2026
Accepted for publication 9 July 2026
Published 15 July 2026 Volume 2026:20 621042
DOI https://doi.org/10.2147/PPA.S621042
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Shenghua Li,1 Hao Zhang,1 Jinming Zhang,2 Xia Liu3
1General Practice Department, Shanghai Taikang Shenyuan Rehabilitation Hospital, Shanghai, People’s Republic of China; 2Rehabilitation Department, Shanghai Taikang Shenyuan Rehabilitation Hospital, Shanghai, People’s Republic of China; 3Pharmacy Department, Shanghai Taikang Shenyuan Rehabilitation Hospital, Shanghai, People’s Republic of China
Correspondence: Xia Liu, Pharmacy Department, Shanghai Taikang Shenyuan Rehabilitation Hospital, Shanghai, People’s Republic of China, Tel +86-13795397490, Email [email protected]
Purpose: This study aimed to examine the medication knowledge, attitudes, and practices (KAP) of older hypertensive patients regarding antihypertensive therapy and to confirm the theoretical relationships among these domains.
Patients and Methods: A cross-sectional study was conducted from July to October 2023 among older hypertensive patients to assess their KAP regarding antihypertensive therapy. Structural equation modeling (SEM) was employed to assess the relationships among the KAP dimensions.
Results: A total of 561 valid responses from older hypertensive patients were included in the final analysis (response rate 74.7%). Older hypertensive patients exhibited a moderate level of knowledge (median 24, IQR 22– 26), generally positive attitudes (median 23, IQR 19– 24), and practices (median 33, IQR 27– 37). SEM analysis revealed that knowledge directly influenced attitude (β=0.497, P< 0.001) and practice (β=0.331, P< 0.001). Attitude directly influenced practice (β=0.484, P< 0.001). Knowledge also indirectly influenced practice through its effect on attitudes (β=0.241, P< 0.001).
Conclusion: This study largely confirmed the expected KAP pathway in older hypertensive patients receiving antihypertensive therapy, showing that knowledge supports attitudes and, both directly and indirectly, influences practice. Although attitudes and practices were generally favorable, the moderate knowledge level and specific knowledge gaps suggest that targeted educational interventions remain necessary.
Keywords: knowledge, attitudes, practices, hypertension therapy, older patients with hypertension, cross-sectional study
Introduction
Hypertension is common among older adult patients, and the prevalence increases with age.1,2 Older adults and frail patients may be more likely to have medication adverse effects.3 Lower achieved systolic blood pressure (SBP) is associated with an increased risk of renal failure in patients >75 years old.4 Older hypertensive patients are more likely to have age-related diseases, which may be secondary (identifiable) causes of hypertension, such as chronic kidney disease, atherosclerotic renal artery stenosis, and hyperthyroidism.5,6
The pharmacological treatment of hypertension holds significant clinical importance in lowering blood pressure, preventing complications, and enhancing quality of life.3,7–9 However, medication management in hypertensive older adult patients can be influenced by various factors, including patients’ understanding of medications, their attitudes, and their adherence to prescribed treatment. In clinical practice, we often encounter questions such as whether patients comprehend the correct usage of medications, whether they are concerned about adverse effects, and whether they adhere to medication as prescribed. Hence, understanding the medication KAP of hypertensive older adult patients and the potential impact of these factors on treatment outcomes is crucial for developing more personalized and effective treatment strategies. Previous studies reported that hypertensive patients have a relatively adequate KAP toward their disease.10–13 Two studies from Nepal reported that the KAP of hypertensive patients using antihypertensive therapy needed to be improved.14,15 Still, these previous studies were not specifically performed in older adults, nor were they specific to antihypertensive therapy.
Previous studies have reported KAP related to hypertension in general patient populations, and a limited number have evaluated KAP among antihypertensive medication users. However, these studies have largely focused on hypertension-related knowledge in broader adult populations rather than medication-related KAP concerning antihypertensive therapy in older adults. Because older patients have distinct treatment goals, comorbidity profiles, and medication-related concerns, evidence specific to this population remains limited. Therefore, this study aimed to assess medication-related KAP regarding antihypertensive therapy among older Chinese patients with hypertension and to analyze the relationships among these domains using SEM. The results could help gain a better understanding of the medication management needs of hypertensive older patients, identify potential challenges, and provide valuable insights for improving clinical practices. Furthermore, by promoting appropriate medication use in hypertensive older patients, the results could help further reduce their cardiovascular risk, enhance their quality of life, and support the development of patient-centered public health policies.
Materials and Methods
Study Design and Participants
This study is reported following the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) checklist.16 This multi-center cross-sectional study was conducted from July 2023 to October 2023 in general communities in China. Convenience sampling was employed to recruit older hypertensive patients.
The study complies with the Declaration of Helsinki. The study was approved by the ethical review committee of Shanghai Taikang Shenyuan Rehabilitation Hospital. All subjects provided written informed consent before completing the questionnaire.
The inclusion criteria were 1) residents of Shanghai, Zhejiang, and Jiangsu aged 60 and above, and 2) a diagnosis of hypertension. The exclusion criteria were 1) recent severe acute physical illnesses that could affect the survey, such as acute cerebrovascular accidents, acute coronary syndrome, or acute infections, 2) surveys completed in less than 114 s (minimum time calculated based on single-choice questions) or more than 1800 s.10–15
Procedures
The questionnaire items were developed based on national and international hypertension guidelines3,7–9 and patient education materials, focusing on key concepts relevant to older adults (eg, blood pressure targets, lifestyle recommendations, and principles of antihypertensive drug use). To ensure that the content was understandable for older patients, the items were written in plain language, reviewed by a panel of cardiovascular and pharmacy experts, and pilot-tested in a group of 50 older hypertensive patients. Feedback from this pilot testing was used to refine wording and remove overly technical formulations before field administration. The overall reliability of the questionnaire was 0.829 (Cronbach’s α), which falls in the “good” range, indicating that the questionnaire has good internal consistency reliability.
The final questionnaire was in Chinese and comprised four dimensions: demographic information of the participants (15 questions), knowledge dimension (15 questions), attitude dimension (10 questions), and the practice dimension (10 questions). In the knowledge dimension, single-choice items (K1-K4 and K7-K10) were scored 1 point for correct responses and 0 points for incorrect ones. For the multiple-choice items (K5, K6, and K11-K14), all listed options were correct. Each option selected gave 1 point. For the special item (K15), selecting options A and C awarded 2 points, but selecting option B, regardless of A and C, was scored 0. Higher scores indicated better knowledge. The scores could range 6–39.
The attitude items were scored using Likert-5 scales. The positive items (A1 and A4) were scored from strongly agree=5 to strongly disagree=1. The negative items (A2, A3, A5, and A6) were scored from strongly agree=1 to strongly disagree=5. The open-ended items (A7-A10) were not scored and were analyzed qualitatively. Higher scores indicated a more positive attitude. The scores could range 6–30.
The practice items were scored using Likert-5 scales. The positive items (P1, P8, and P9) were scored from never=1 to always=5. The reverse-coded items (P2-P6) were scored from never=5 to always=1. The open-ended items (P7 and P10) were not scored and were analyzed qualitatively. Higher scores indicated a more positive attitude. The scores could range 8–40.17,18
An online questionnaire was constructed to facilitate data collection using the WeChat-based Questionnaire Star mini-program, and a QR code was generated for participants to access and complete the questionnaire through WeChat. Within each community, the survey was facilitated by on-site health care workers and community administrators. Residents who met the inclusion criteria and expressed interest in the study were screened for eligibility by trained investigators. Each IP address was limited to one submission, and all questions were mandatory to ensure the quality and completeness of the questionnaire results. An incomplete questionnaire could not be submitted. Subsequently, an Excel spreadsheet was exported from the Questionnaire Star platform. A team of researchers examined the integrity, internal consistency, and validity of all questionnaires.
Sample Size
The minimal sample size was estimated using Cochran’s sample size formula for survey studies:19
Where Z2 is the confidence coefficient, p is the proportion, and d is the margin of error. The sample size is maximized when p=0.5. A 95% confidence interval involves a Z-value of 1.96. The margin of error was assumed at 5%. Hence, a minimum of 384 participants were needed.
Statistical Analysis
The statistical analysis was performed using SPSS 26.0 (IBM Corp., Armonk, NY, USA). The distribution of the scores for each dimension was first tested for normality using the Kolmogorov–Smirnov test; all scores showed a skewed distribution. The continuous variables were presented as median (interquartile range) and analyzed using the Mann–Whitney U-test (two groups) or the Kruskal–Wallis H-test (more than two groups). The categorical data were presented as n (%) and analyzed using the chi-squared test. Correlation analysis of the dimension scores was performed using Spearman correlation. Univariate and multivariable logistic regression analyses were conducted with the dimension scores as dependent variables. Variables for inclusion in the multivariate regression analysis were selected based on variables with a P-value <0.1 from the univariable analyses. Structural equation modeling (SEM) was utilized to explore the relationships between KAP. P-values <0.05 were considered statistically significant.
Results
Characteristics of the Subjects
A total of 751 questionnaires were collected through collaboration with a large domestic older adult care organization in the Yangtze River Delta region (including Shanghai, Jiangsu, and Zhejiang provinces). Two questionnaires were excluded for being outside the answer timer, and 188 for logic errors such as reporting a duration of antihypertensive therapy but indicating not taking antihypertensive therapy, answering having hypertension but not taking medication, and then stating taking medication. Ultimately, 561 valid questionnaires were included in the analysis, yielding a valid questionnaire rate of 74.7%. Among them, 333 (59.4%) were aged 65–79 years, 313 (55.8%) were female. Older hypertensive patients exhibited a moderate level of knowledge (median 24, IQR 22–26), generally positive attitudes (median 23, IQR 19–24), and practices (median 33, IQR 27–37) (Table 1).
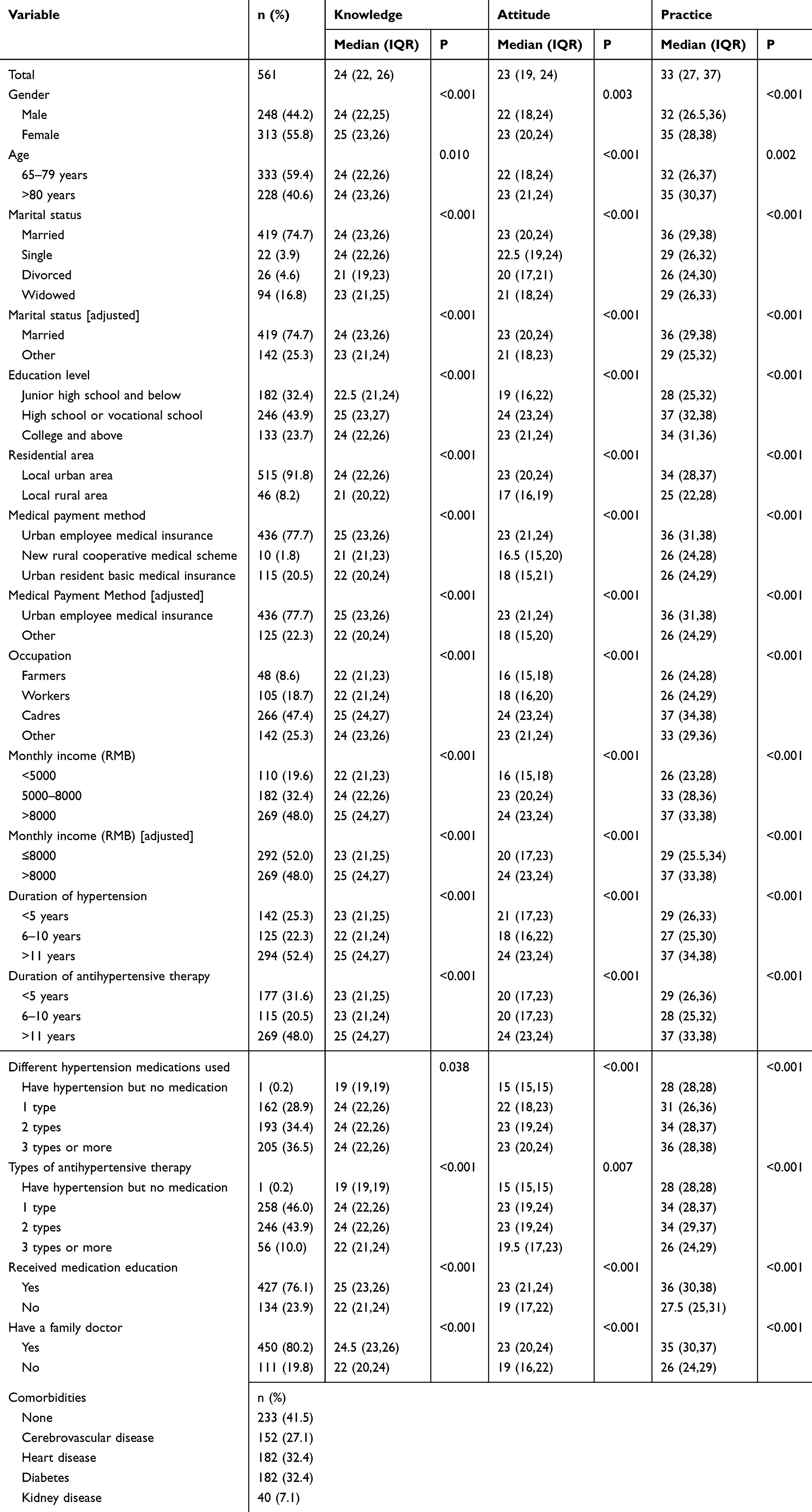 |
Table 1 Characteristics of the Participants |
Knowledge, Attitudes, and Practices Distribution
In the knowledge dimension, participant responses indicated that understanding of specific antihypertensive therapy could be enhanced. Specifically, knowledge concerning the fundamental treatment goal for older adults was limited, with 43.1% of respondents selecting the correct option of “lowering blood pressure to below 140/90 mmHg” (K8). Similarly, the understanding of lifestyle recommendations was not comprehensive, as only 34.9% correctly identified “intense physical activity” as an inappropriate change for hypertensive patients (K9). Furthermore, awareness of basic principles for antihypertensive drug use in older adults was moderate, with 65.2% correctly identifying that a “rapid” approach should be avoided (K10) (Table S1).
Regarding the attitudinal dimension, participants displayed overwhelmingly positive and well-informed beliefs about antihypertensive therapy. Specifically, a vast majority (n=513) recognized that hypertension is a dangerous but manageable disease (A1). This understanding was complemented by a strong belief in the necessity of lifelong treatment, with 427 participants agreeing that medication must be taken consistently for life (A4). Furthermore, confidence in the prescribed therapy was exceptionally high, as a combined 465 participants believed their current medication was effective in controlling their hypertension (A7). This proactive stance was further supported by the high willingness (n=445) to undergo regular follow-up and adjust their medication plan (A10) (Figure S1).
On the practice dimension, participants demonstrated largely positive behaviors, particularly in their commitment to medication adherence and following professional medical advice. Specifically, a combined majority of 74.5% reported that they “Always” (n=211) or “Often” (n=207) follow their doctor’s medication advice and instructions (P9). Furthermore, a high degree of understanding regarding the chronic nature of the condition was evident, as 68.9% (n=357) stated they “Never” stop taking medication even when they feel their blood pressure is under control (P6). This strong adherence was reinforced by the fact that the majority (n=308) reported “Never” having reduced the dosage or stopped medication without informing their doctor (P4) (Figure S2).
Correlations
Table 2 shows that the knowledge scores were correlated to the attitude (r=0.544, P<0.001) and practice (r=0.624, P<0.001) scores, while the attitude scores were correlated to the practice scores (r=0.643, P<0.001).
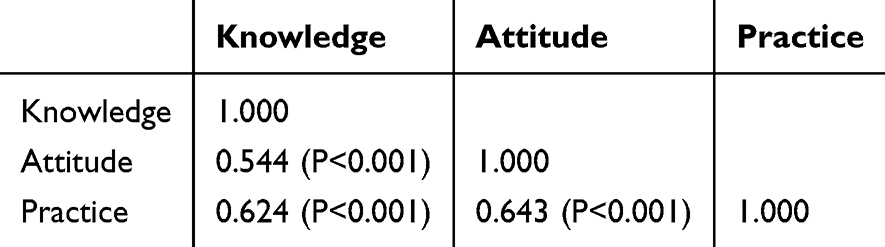 |
Table 2 Correlation Analysis |
Multivariable Analysis
Marital status other than married (OR=0.564, 95% CI: 0.343–0.925, P=0.023), rural area (OR=0.290, 95% CI: 0.111–0.757, P=0.011), other insurance (OR=0.558, 95% CI: 0.322–0.969, P=0.038), farmers (OR=0.244, 95% CI: 0.095–0.629, P=0.004), workers (OR=0.442, 95% CI: 0.238–0.821, P=0.010), higher income (OR=1.744, 95% CI: 1.111–2.736, P=0.016), antihypertensive medications for >11 years (OR=1.899, 95% CI: 1.142–3.159, P=0.013), and no medication education (OR=0.505, 95% CI: 0.303–0.843, P=0.009) were independently associated with the knowledge scores (Table S2).
High school education (OR=3.067, 95% CI: 1.641–5.730, P<0.001), other medical insurance (OR=0.320, 95% CI: 0.161–0.635, P=0.001), higher income (OR=2.034, 95% CI: 1.221–3.388, P=0.006), hypertension for >11 years (OR=3.983, 95% CI: 2.217–7.154, P<0.001), no medication education (OR=0.412, 95% CI: 0.229–0.742, P=0.003), and knowledge score >24 (OR=2.450, 95% CI: 1.445–4.156, P=0.001) were independently associated with the attitude scores (Table S3).
Marital status other than married (OR=0.447, 95% CI: 0.227–0.881, P=0.020), other medical insurance (OR=0.351, 95% CI: 0.143–0.861, P=0.022), workers (OR=0.217, 95% CI: 0.080–0.592, P=0.003), higher income (OR=2.317, 95% CI: 1.256–4.271, P=0.007), antihypertensive medication for 6–10 years (OR=0.288, 95% CI: 0.126–0.657, P=0.003), one current antihypertensive medication (OR=5.512, 95% CI: 1.694–17.939, P=0.005), two current antihypertensive medications (OR=3.947, 95% CI: 1.216–12.816, P=0.022), no family doctor (OR=0.257, 95% CI: 0.107–0.616, P=0.002), knowledge score >24 (OR=2.878, 95% CI: 1.546–5.359, P=0.001), and attitude score >23 (OR=5.945, 95% CI: 3.182–11.108, P<0.001) were independently associated with the practice scores (Table S4).
Structural Equation Modeling
The model (Figure 1) showed a root mean square error of approximation (RMSEA) of <0.001 (<0.080 is good), a standardized root mean square residual (SRMR) of <0.001 (<0.080 is good), a Tucker-Lewis index (TLI) of >0.999 (>0.800 is good), and a comparative factor index (CFI) of >0.999 (>0.800 is good). Knowledge directly influenced attitude (β=0.497, P<0.001) and practice (β=0.331, P<0.001). Attitude directly influenced practice (β=0.484, P<0.001). Knowledge also indirectly influenced practice through its effect on attitudes (β=0.241, P<0.001) (Table 3).
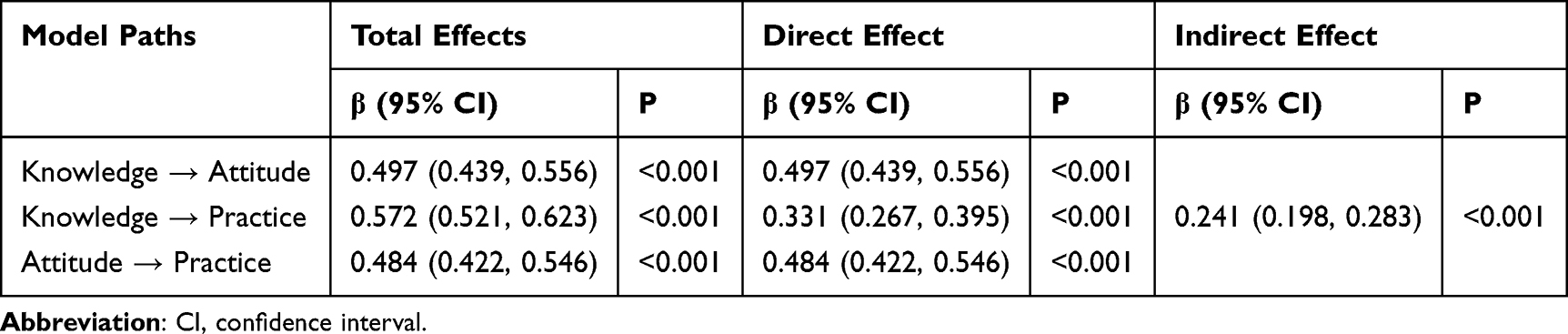 |
Table 3 SEM Analysis |
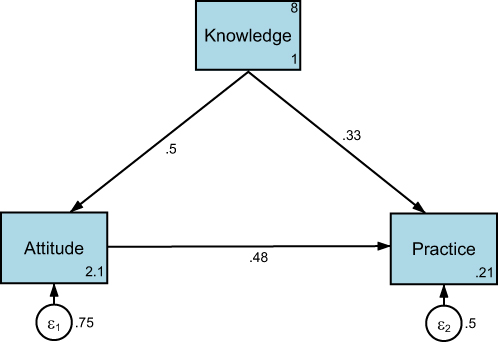 |
Figure 1 Structural equation modeling. |
Discussion
This cross-sectional study indicated that these older hypertensive patients exhibited generally positive attitudes and practices towards antihypertensive therapy, but possessed moderate knowledge levels. This suggests that while patients are generally willing and report adherence to medication regimens, gaps in their understanding may still exist. The study identified specific knowledge points that could be improved. Improving knowledge should also improve attitude and practice. A notable contribution of this study is that it examined medication-related KAP specifically among older Chinese patients with hypertension, a population less frequently investigated than general adult hypertensive populations. In addition, SEM was used to empirically test the hypothesized KAP pathway, providing quantitative support for the sequence in which knowledge influences attitudes and, directly and indirectly, practice. Although these findings are largely confirmatory, they extend the literature by contextualizing the KAP framework within antihypertensive therapy in older adults.
Previous studies reported that hypertensive patients had a relatively moderate to good KAP toward their disease,10–13 but these studies did not specifically examine the KAP toward antihypertensives. The present study showed relatively moderate knowledge but positive attitudes and proactive practices toward antihypertensive therapy among older adults. It is supported by Shrestha et al,14,15 who also showed moderate KAP toward antihypertensives among Nepalese with hypertension.
A core finding of this study is the strong positive correlation between the three dimensions of knowledge, attitude, and practice, which provides empirical support for the KAP theoretical model in the study population.18,20 It was further reinforced by the multivariate regression analysis, which showed that knowledge was an independent predictor of better attitudes and practices, and that positive attitudes were also strongly predictive of better practice. This sequence relationship (knowledge supports attitudes, attitudes drive practice) is crucial since it matches the KAP theoretical framework and suggests the validity of the constructs. Indeed, according to the KAP theory, knowledge is the basis for practice, and attitude is the driving force.18,20 It also directly responds to the study’s objectives and shows that the moderate level of knowledge observed in the study is not an isolated problem but a fundamental barrier to reaching ideal attitudes and practices. Therefore, the findings strongly suggest that knowledge enhancement, especially through targeted educational interventions, is not only necessary but also highly likely to have a cascading effect to improve patient attitudes and subsequent medication adherence. Although the present study did not directly measure where patients obtained their information, it is plausible that their knowledge of hypertension and antihypertensive therapy was shaped by routine physician consultations, pharmacist counseling, family doctor services, and community health education activities. Given that both prior medication education and having a family doctor were associated with higher KAP scores in this study, these channels likely play an important role in disseminating treatment-related information and could be leveraged to deliver more structured, patient-centered education on hypertension. Nevertheless, the results suggest that the points to be improved would include the goal of treating older adults with hypertension, the principles of antihypertensive drugs, the risk factors for hypertension, the classification of hypertension, the beneficial lifestyle changes, and the common side effects of antihypertensive drugs. Of note, a study revealed that community pharmacists had a poor KAP toward the education of patients with hypertension.21 Since community healthcare providers, including pharmacists, play an important role in patient education, continuing education activities should also target them. Future research should explicitly investigate the main sources and perceived credibility of hypertension-related information among older adults, including clinicians, pharmacists, media, and digital platforms. Such data would inform the design of targeted educational interventions that build on the most influential information channels to improve patients’ knowledge and, consequently, their attitudes and practices.
The study generally showed that a higher socioeconomic status (ie, higher education, higher income, cadres, living in urban areas, and having urban employee medical insurance) was associated with higher KAP dimension scores. It is supported by Svendsen et al,22 who showed that a higher socioeconomic status was associated with higher health literacy. Being married was also associated with a higher KAP, probably because spouses care for each other and share knowledge. Not having received medication education was also associated with lower KAP scores, which was expected. Therefore, this study suggests that older adults with hypertension and a lower socioeconomic status, who are not married, and who did not receive medication education should be targeted first by educational interventions.
From a clinical and public health perspective, the findings suggest that apparently favorable attitudes and self-reported practices may coexist with only moderate medication knowledge. The identification of specific knowledge deficiencies, particularly regarding treatment goals for older adults and principles of antihypertensive drug use, offers practical targets for patient education. Furthermore, the associations observed for lower socioeconomic status, lack of medication education, and absence of family doctor support may help clinicians and policymakers identify subgroups requiring more intensive support.
This study had limitations. Because of the cross-sectional design, the findings should be interpreted as descriptive and hypothesis-generating rather than causal. Therefore, while the results support the rationale for targeted educational strategies, interventional and longitudinal studies are needed before firm conclusions can be drawn regarding effects on clinical practice or outcomes. The participants were enrolled through convenience sampling, possibly introducing a selection bias. Especially, a core limitation is that the data were collected online through WeChat, likely over-representing affluent, educated, and digitally literate individuals. This method systematically excluded more vulnerable populations (eg, rural, lower socioeconomic status) who probably exhibit lower knowledge scores. Consequently, the reported “positive” attitudes and practices are likely an overestimation of the true situation in the general population of older adults. Future studies should also include the possibility of completing a paper questionnaire to cover a broader range of participants. The participants were also from a single geographical area, limiting generalizability. The questionnaire was designed by local investigators, limiting generalizability and exportability. The exploratory factor analysis suggested the presence of crossloading, but it is a common phenomenon in KAP surveys since knowledge, attitudes, and practices are not polarly independent in reality but closely interwoven. The use of an online questionnaire probably introduced a selection bias based on digital literacy and confidence in the use of digital tools. Finally, all KAP studies are susceptible to the social desirability bias, ie, the participants could answer what they know they should do or think instead of what they are really doing/thinking.23,24
Conclusions
This study showed that older Chinese patients with hypertension generally reported positive attitudes and practices regarding antihypertensive therapy, despite only moderate knowledge. SEM findings supported the expected KAP pathway, suggesting that knowledge may influence practice both directly and indirectly through attitudes. The identified knowledge gaps and vulnerable subgroups provide practical direction for future educational interventions, although these findings should be regarded as descriptive and hypothesis-generating because of the cross-sectional study design. Future research should focus on designing and evaluating such interventions, especially for at-risk groups, to improve medication knowledge, subsequently enhance attitudes and practices, and ultimately contribute to better clinical outcomes and quality of life for this vulnerable population.
Data Sharing Statement
All data generated or analyzed during this study are included in this article.
Ethics Approval and Consent to Participate
The study complies with the Declaration of Helsinki. The study was approved by the ethical review committee of Shanghai Taikang Shenyuan Rehabilitation Hospital (TKSY202307-01). All participants provided written informed consent before completing the questionnaire. All methods were performed in accordance with the relevant guidelines and regulations.
Consent for Publication
All participants provided written informed consent before completing the questionnaire.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the 2022 Taikang Health Investment Youth Medical Research Launch Fund. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Lloyd-Jones DM, Evans JC, Levy D. Hypertension in adults across the age spectrum: current outcomes and control in the community. JAMA. 2005;294(4):466–10. doi:10.1001/jama.294.4.466
2. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: executive Summary: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71(6):1269–1324. doi:10.1161/HYP.0000000000000066
3. Aronow WS, Fleg JL, Pepine CJ, et al. ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. Circulation. 2011;123(21):2434–2506. doi:10.1161/CIR.0b013e31821daaf6
4. McAlister FA, Zhang J, Tonelli M, Klarenbach S, Manns BJ, Hemmelgarn BR. The safety of combining angiotensin-converting-enzyme inhibitors with angiotensin-receptor blockers in elderly patients: a population-based longitudinal analysis. Cmaj. 2011;183(6):655–662. doi:10.1503/cmaj.101333
5. Setters B, Holmes HM. Hypertension in the Older Adult. Prim Care. 2017;44(3):529–539. doi:10.1016/j.pop.2017.05.002
6. Viera AJ, Neutze DM. Diagnosis of secondary hypertension: an age-based approach. Am Fam Physician. 2010;82(12):1471–1478.
7. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507–520. doi:10.1001/jama.2013.284427
8. Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021–3104. doi:10.1093/eurheartj/ehy339
9. Rabi DM, McBrien KA, Sapir-Pichhadze R, et al. Hypertension Canada’s 2020 Comprehensive Guidelines for the Prevention, Diagnosis, Risk Assessment, and Treatment of Hypertension in Adults and Children. Can J Cardiol. 2020;36(5):596–624. doi:10.1016/j.cjca.2020.02.086
10. Machaalani M, Seifeddine H, Ali A, Bitar H, Briman O, Chahine MN. Knowledge, Attitude, and Practice Toward Hypertension Among Hypertensive Patients Residing in Lebanon. Vasc Health Risk Manag. 2022;18:541–553. doi:10.2147/VHRM.S367187
11. Buang NFB, Rahman NAA, Haque M. Knowledge, attitude and practice regarding hypertension among residents in a housing area in Selangor, Malaysia. Med Pharm Rep. 2019;92(2):145–152. doi:10.15386/mpr-1227
12. Aubert L, Bovet P, Gervasoni JP, Rwebogora A, Waeber B, Paccaud F. Knowledge, attitudes, and practices on hypertension in a country in epidemiological transition. Hypertension. 1998;31(5):1136–1145. doi:10.1161/01.HYP.31.5.1136
13. Ralapanawa U, Bopeththa K, Wickramasurendra N, Tennakoon S. Hypertension Knowledge, Attitude, and Practice in Adult Hypertensive Patients at a Tertiary Care Hospital in Sri Lanka. Int J Hypertens. 2020;2020:4642704. doi:10.1155/2020/4642704
14. Shrestha S, Adhikari B, Poudel RS, et al. Knowledge, Attitude and Practice on Hypertension Among Antihypertensive Medication Users. JNMA J Nepal Med Assoc. 2016;55(204):86–92. doi:10.31729/jnma.2848
15. Shrestha J, Marasine NR, Lamichhane R, Marasini NR, Sankhi S. Attitude and self-care practice on hypertension among antihypertensive medication users in a tertiary care hospital Nepal. SAGE Open Med. 2021;9:20503121211040707. doi:10.1177/20503121211040707
16. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
17. Bf AL, Thirunavukkarasu A, Alsaidan AA, et al. Knowledge, attitude, and practice towards evidence-based medicine among Northern Saudi Primary Care Physicians: a cross-sectional study. Healthcare. 2022;10(11):2138.
18. Andrade C, Menon V, Ameen S, Kumar Praharaj S. Designing and Conducting Knowledge, Attitude, and Practice Surveys in Psychiatry: practical Guidance. Indian J Psychol Med. 2020;42(5):478–481. doi:10.1177/0253717620946111
19. Cochran WG. Sampling Techniques.
20. World Health Organization. Advocacy, communication and social mobilization for TB control: a guide to developing knowledge, attitude and practice surveys. 2022. Available from: http://whqlibdoc.who.int/publications/2008/9789241596176_eng.pdf.
21. Chen L, Liu Y, Xi X. Study of knowledge, attitude and practice regarding patient education in hypertension among community pharmacists in China. BMC Health Serv Res. 2022;22(1):1295. doi:10.1186/s12913-022-08686-9
22. Svendsen MT, Bak CK, Sorensen K, et al. Associations of health literacy with socioeconomic position, health risk behavior, and health status: a large national population-based survey among Danish adults. BMC Public Health. 2020;20(1):565. doi:10.1186/s12889-020-08498-8
23. Bergen N, Labonte R. “Everything Is Perfect, and We Have No Problems”: detecting and Limiting Social Desirability Bias in Qualitative Research. Qual Health Res. 2020;30(5):783–792. doi:10.1177/1049732319889354
24. Latkin CA, Edwards C, Davey-Rothwell MA, Tobin KE. The relationship between social desirability bias and self-reports of health, substance use, and social network factors among urban substance users in Baltimore, Maryland. Addict Behav. 2017;73:133–136. doi:10.1016/j.addbeh.2017.05.005
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes, and Practices Among Patients with Systemic Lupus Erythematosus Toward Disease Management and Biologic Therapy
Liu X, Song Y, Wan L, Du R
Journal of Multidisciplinary Healthcare 2024, 17:937-947
Published Date: 2 March 2024
Knowledge, Attitudes, and Practices Among Community Populations Toward Long COVID in China
He N, Tunala S, Wu R, Zhao C, Wuren T, Hushuud C
International Journal of General Medicine 2024, 17:4455-4463
Published Date: 1 October 2024
Knowledge, Attitudes, and Practices Regarding Swallowing Disorders Among General Practitioners
Zou M, Zhu X, Li J, Yu H, Guo P
International Journal of General Medicine 2025, 18:1555-1567
Published Date: 18 March 2025
Knowledge, Attitudes and Practices Toward Hypotension During Hemodialysis Among Nephrology and Hemodialysis Medical Staff: A Multi-Center Cross-Sectional Study
Cheng D, Xie L, Chu X, Bai Y, He T
Journal of Multidisciplinary Healthcare 2025, 18:5359-5369
Published Date: 28 August 2025
Knowledge, Attitudes, and Practices Toward Microvascular Decompression for Hemifacial Spasm Among Neurosurgeons: A Multicenter Cross-Sectional Study
Xu Y, Dong S, Zhao R, Liu J, Han P, Guo Y, Jiang R
Journal of Multidisciplinary Healthcare 2025, 18:8277-8291
Published Date: 27 December 2025