Back to Journals » Journal of Pain Research » Volume 18
Investigating Self-Reported Sensory Intolerance and Perceptual Ability Across Sensory Modalities in Fibromyalgia
Authors Shepherd H ![]() , Poliakoff E
, Poliakoff E ![]() , Brown CA, Brown RJ
, Brown CA, Brown RJ
Received 16 July 2025
Accepted for publication 27 October 2025
Published 21 December 2025 Volume 2025:18 Pages 6947—6961
DOI https://doi.org/10.2147/JPR.S551725
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Hayley Shepherd,1 Ellen Poliakoff,1 Christopher A Brown,2 Richard J Brown3
1Division of Psychology, Communication and Human Neuroscience, University of Manchester, Manchester, UK; 2Department of Psychology, University of Liverpool, Liverpool, UK; 3Division of Psychology and Mental Health, University of Manchester, Manchester, UK
Correspondence: Hayley Shepherd, Division of Psychology, Communication and Human Neuroscience, University of Manchester, Manchester, UK, Tel +44 7510904121, Email [email protected]
Purpose: Fibromyalgia has predominantly been classified as a condition of amplified pain processing associated with greater sensitivity to pain. Beyond disturbed pain processing, emerging evidence suggests that people with fibromyalgia experience intolerances (increased unpleasantness) across sensory modalities. Limited research, however, has investigated how discrimination and detection in different senses are affected in this group. Understanding how basic perception is affected in fibromyalgia has important implications for treatment and could lead to the development of new perceptual training interventions. This study used self-report methods to investigate how different aspects of sensory processing in fibromyalgia, including detection/discrimination and intolerance, are affected across modalities.
Patients and Methods: One hundred and eighty-eight people with fibromyalgia and 121 controls completed the Sensory Hypersensitivity Scale (intolerance) and the Sensory Perception Quotient (discrimination/detection) online.
Results: Pre-registered group comparisons revealed that the fibromyalgia group reported increased intolerance across all measured sensory modalities and an increased subjective perceptual ability (discrimination/detection) across all modalities except smell and taste. Exploratory cluster analysis identified three fibromyalgia subgroups. While one group reported low intolerance that was comparable to healthy controls, the remaining two groups primarily differed in their subjective perceptual ability with one group enhanced and the other reduced.
Conclusion: These findings suggest that there are heterogenous sensory features in fibromyalgia that point to the potential value of treatments focusing on non-pain perceptual processing for some people. Future research should investigate whether the higher subjective perceptual abilities reported by people with fibromyalgia are matched by superior objective perceptual ability.
Keywords: pain, fibromyalgia, perception, sensory modalities
Introduction
Fibromyalgia is a widespread chronic pain condition, estimated to affect 2.7% of the global population.1 In addition to chronic pain, the condition is accompanied by physical symptoms including chronic fatigue, stiffness and difficulty sleeping and is often comorbid with mental health conditions such as anxiety and depression.2 The modal view is that the condition reflects a sensitization of the central nervous system which is experienced as allodynia (pain perception in response to innocuous stimuli) and hyperalgesia (amplification of pain perception).2 Peripheral factors may also play a role, with a growing body of evidence suggesting that around 50% of people with fibromyalgia have small fiber pathology which may contribute to central sensitization.3 Despite this, the pathophysiology of fibromyalgia is poorly understood with no clear clinical biomarkers and there is a lack of universally effective treatments, reflecting the complex nature of the condition.4,5
As well as being more sensitive to touch and pain stimuli, many people with fibromyalgia also report increased sensitivity to sounds, visual stimuli and smells.6 The term “sensitivity” can mean different things, however. In Wilbarger and Cook,6 it was used to refer to how bothered participants were by sensory stimuli; we refer to this here as intolerance. In other settings, however, sensitivity refers to basic perceptual processes including detection and discrimination abilities. In the interest of clarity, in this paper we use the term increased intolerance to refer to increased ratings of unpleasantness in response to sensory stimuli or a reduction in the intensity of stimuli required to create an unpleasant or overwhelmed response. In contrast, we use the term perceptual ability to refer to detection and discrimination abilities.
In an experimental setting, increased intolerance in people with fibromyalgia has been reported across multiple sensory modalities including, vision, audition, touch, and olfaction.6–13 Using functional magnetic resonance imaging (fMRI), increased intolerance to different sensory modalities in people with fibromyalgia has been associated with altered brain activity, including reduced neural responses in early sensory cortices and increased responses in areas implicated in sensory integration.14 Evidence of increased intolerance to sensory stimuli across modalities has led to the suggestion that fibromyalgia may reflect a global disturbance in sensory processing, further supported by significant correlations between pain tolerance and tolerance in different modalities in this group.8
Individual differences in perceptual ability pertain to sensory detection (the ability to detect the presence of a stimulus) and discrimination (the ability to differentiate between stimuli on a given feature), both of which inform body representation.15 Using objective measures of perceptual ability, there is some evidence that people with fibromyalgia display decreased accuracy in detecting internal bodily sensations such as heartbeats (a measure of interoception).16 Similarly, using tactile acuity as a measure of discrimination ability, Martinez et al17 found that people with fibromyalgia require a greater distance between two tactile stimuli on the skin in order to correctly identify them as discrete points. Similar impairments have been shown in other aspects of tactile discrimination, including temporal discrimination.18 Importantly, these impairments have been found to correlate with self-reported pain intensity, suggesting that an increased intolerance to pain in fibromyalgia may be associated with impaired basic bodily perception in the pain and touch modalities. This fits with the Bayesian account of chronic pain, which suggests that noisy and imprecise bodily signals (bottom-up information) force the brain to rely on top-down information such as expectations to inform sensory experiences. This can result in the perception of an innocuous stimulus as painful, if this fits with an individual’s prior expectations.19,20
Understanding how intolerance and perceptual ability are affected in fibromyalgia is crucial for informing treatment of the condition, particularly given evidence suggesting that body perception training can be effective in reducing pain in chronic pain conditions, including fibromyalgia.21,22 A caveat of training as a treatment, however, is that its success is dependent on the source of imprecise bodily signals. For example, if small fiber pathology is present, improved perception through training may not be effective. If this is not the case and if impairments in perceptual processing extend to other modalities in fibromyalgia, then improving perception in one modality may have the potential to influence symptoms in another. If true, then training could potentially be administered using non-painful stimuli, which would have obvious clinical benefits such as being possible to administer remotely by the patient themselves. Currently, however, very few studies have investigated how detection and discrimination abilities are affected across modalities in people with fibromyalgia.
The overall aim of the current study was to investigate how people with fibromyalgia rate different aspects of their sensory processing, namely detection/discrimination and intolerance, across sensory modalities. Several self-report questionnaires have been developed to measure different aspects of sensory processing in clinical populations. These include the Sensory Perception Quotient (SPQ)23 and the Sensory Hypersensitivity Scale (SHS).12 The SPQ was designed to measure perceptual experiences other than emotional reactions to stimuli by asking about the person’s perceived discrimination and detection ability across five different sensory modalities in autistic adults (ie, touch, hearing, vision, smell and taste). In contrast, the SHS was designed to serve as a proxy measure for central sensitization and contains questions relating to greater perceived noxiousness of sensory stimuli (intolerance) across nine separate subscales (eg, allergies, heat, cold, light, pain, smell, hearing, taste and touch). In a fibromyalgia population (N = 44), intolerance was found to be greater relative to healthy controls across all modalities of the SHS, with the exception of hearing which did not reach significance.12
To address our aim, the current study compared people with fibromyalgia and healthy controls on both the SHS and SPQ, as measures of self-rated intolerance and subjective detection/discrimination ability across modalities respectively. For the SHS, it was predicted that people with fibromyalgia would report increased intolerance across modalities as previously reported. For the SPQ, it was predicted that the fibromyalgia group would report reduced subjective perceptual ability, that is, impaired detection/discrimination ability across modalities, in line with evidence of impaired basic perception in the touch modality.18 An exploratory analysis aimed to identify subgroups that show similar patterns of responses across questionnaires. As fibromyalgia presents with varied symptoms, subgrouping has the potential to help identify different underlying mechanisms that may play a role and lead to more tailored treatments.
It should be noted that a secondary aim of the study was to attempt to validate a new scale (containing questions from the SPQ and SHS) measuring three different aspects of perception (detection, discrimination and intolerance). See supplementary materials for the analysis which indicated that it was best to use the questionnaires in their original forms.
Materials and Methods
Design
The study contained one independent variable with two levels (the presence or absence of fibromyalgia). The main dependant variables consisted of scores on the SPQ23 and SHS for each modality.12 This consisted of five dependant variables for the SPQ and nine for the SHS.
Participants
Participants were 188 people with a self-reported diagnosis of fibromyalgia (178 females, 9 males and 1 participant who preferred not to say) with a mean age of 45.10 years (± 11.80, range 21–68). The average number of years since diagnosis was 7.14 (± 7.00, range less than 1 year- 51 years). The control group consisted of 121 participants (86 female, 32 male and 3 who preferred not to say) who self-reported that they did not suffer from a chronic pain condition. Chronic pain was defined as the self-reported presence of persistent pain in any part of the body for the last 3 months. The mean age of the control group was 31.60 years (±11.50, range 18–78). The fibromyalgia group were significantly older than the control group (W= 18310, p <0.001, r=0.515). There were significantly more females in the fibromyalgia group (X2 = 32.99, p <0.001). Participants were recruited through social media, online support groups and via the charity Fibromyalgia Action UK, using a link to the survey. For most participants there was no financial incentive to take part, however, a prize draw with a modest prize was later introduced to boost recruitment. The pre-registered sample size was 150 participants in each group and the stopping rule to end recruitment was 12 months after the date of launch or when the target sample size was reached. At 12-months, power calculations were run using G*Power which suggested that the collected sample size would give sufficient power to capture an effect size of 0.05 (small effect size) when α =0.05, β=0.20 for a two-tailed MANOVA test.24 Ethical approval was granted by the University of Manchester (University research ethics committee 5 2021–10,504-17,619).
Materials
The SPQ measures subjective detection and discrimination abilities across five separate sensory modalities (vision, hearing, touch, taste and smell). The questionnaire consists of 35 items (eg, “I would be able to distinguish different people by their smell”), taken from an earlier 92-item version. Participants are asked to indicate whether they strongly agree with each statement (score of zero), agree (score of 1), disagree (score of 2), or strongly disagree (score of 3). Lower scores represent higher subjective perceptual ability. The maximum possible total score participants could achieve was 105. The questionnaire has excellent internal reliability with a Cronbach’s alpha value of .93.23 The Cronbach’s alpha value for the total scale in the current study was .90 for the fibromyalgia group and .88 for the healthy controls (Cronbach’s alpha =0.90 for both groups together).
The SHS contains questions relating to increased noxiousness of sensory stimuli (intolerance) across nine subscales (allergies, heat, cold, light, pain, smell, hearing, taste and touch). Participants are presented with 25 statements (eg, “I am easily disturbed by high temperatures”), and are asked to indicate whether they strongly disagree (score of 1), disagree (score of 2), neutral/not sure (score of 3), agree (score of 4) and strongly agree (score of 5). Higher scores represent higher intolerance. The maximum total possible score was 125 (average of 5). The questionnaire has a Cronbach’s alpha value of .81.12 The Cronbach’s alpha value for the total scale in the current study was .83 for the fibromyalgia group and.82 for the healthy controls (Cronbach’s alpha =0.89 for both groups together).
For the purpose of addressing our secondary aim of validating a new scale containing questions from the SPQ and SHS, as the SPQ and SHS did not have an equal number of questions measuring detection/discrimination and intolerance for each modality, we added 25 items to the SPQ and three items to the SHS for the additional analyses to ensure that questions were more equally spread across modalities. This is reported in the supplementary material (Supplementary Tables 1–3).
To explore the relationship between physical symptom severity and scores on the SPQ and SHS, the Patient Health Questionnaire-15 (PHQ-15) was used as a measure of symptom reporting.25 This questionnaire consists of 15 somatic symptoms including pain and measures the overall tendency to be bothered by physical symptoms (ibid). Participants are required to rate how often they have been bothered by each symptom in the past 4 weeks. Responses include not bothered at all (score of 0), bothered a little (score of 1) or bothered a lot (score of 2). Greater scores indicate greater symptom reporting. The maximum possible total score was 30. The Cronbach’s alpha value for the total scale in the current study was .77 for the fibromyalgia group and .79 for the healthy controls (Cronbach’s alpha =0.90 for both groups together).
Fibromyalgia symptoms were measured using the Revised Fibromyalgia Impact Questionnaire (FIQR).26 This questionnaire measures the impact of fibromyalgia symptomatology in the past seven days. The questionnaire is divided into three main sections: function, overall impact and symptoms. In each section, participants are asked to rate statements on an 11-point scale (0–10), where 10 is the worst possible impact. The maximum possible total score was 100. The Cronbach’s alpha value for the total scale in the current study was .93 for the fibromyalgia group.
Procedure
All survey responses were collected and managed using RedCap electronic data capture tools27 hosted at the University of Manchester. Participants gave informed consent, completed demographic questions and were then asked to complete each questionnaire in the following fixed order: SPQ, SHS, PHQ-15; the FIQR was then completed by participants who reported a diagnosis of fibromyalgia. Attention checks were included throughout the questionnaires, consisting of four questions where participants were instructed to respond with a specified response (eg, respond strongly disagree for this question). Participants who failed to respond correctly on two or more attention questions were removed from the analysis.
Data Analysis
The pre-registration of this study can be found at https://osf.io/n4s9g. Deviations from the original plan are detailed in the supplementary material. R version 4.1.0 was used to analyze the data.28 Total scores were calculated for each modality on the SPQ and SHS. In line with the original papers, total scores for the SPQ were calculated by summing each individual item; for the SHS, total scores consisted of the average response across modalities. Attention check errors resulted in the removal of six fibromyalgia participants and three healthy controls.
A MANOVA was conducted for between-group comparisons for each of the five modalities on the SPQ. Pillai’s trace was used as the criterion for significance to maximise robustness given unbalanced sample sizes and some violations of normality in the fibromyalgia group.29 A significant result was followed by six ANOVAs (including an ANOVA for the total SPQ score), correcting for multiple comparisons using Bonferroni correction (α =0.0083). Two MANCOVAs were also conducted. The first included age and gender added as covariates, while the second also included the total score on the PHQ-15. Effect sizes were calculated using partial eta squared.
As the normality assumptions of MANOVA were violated for modality scores on the SHS, a Mann Whitney U-test was conducted for all nine modality scores as well as the total SHS score, using a Bonferroni corrected alpha score of α=0.005. Effect sizes were calculated using the r value.
To assess whether modality scores on each questionnaire could predict fibromyalgia severity (as measured by the FIQR), a simultaneous multiple linear regression was conducted. All five modality scores from the SPQ and all nine modality scores from the SHS were added as predictor variables, in addition to age. A separate regression equation was also constructed with SPQ total, SHS total and age added as predictor variables. Variance inflation factors (VIF) were checked for each predictor to ensure predictors were sufficiently uncorrelated.
Factor analyses on the adapted SHS and SPQ scales suggested that the scales were best used in their original form, without the inclusion of our additional items (see supplementary material and supplementary Tables 1–8).
Exploratory Analysis
A cluster analysis was conducted to explore the presence of subgroups in the data after finding that some of the data were unevenly distributed. An exploratory factor analysis was first conducted on the total sub-scores of each modality of the SPQ and SHS for both groups to aid interpretation of the underlying dimensions of the scales and to reduce the dimensionality of the data. Factors were extracted using principal factor analysis. Deciding the number of factors to retain was based on a combination of the visual inspection of scree plots, parallel analysis and the Kaiser criterion (Eigen values greater than 1). Promax rotation was used to aid interpretation of the factors based on the expectation that the factors would be correlated. As recommended by Tabachnick,30 variables with factor loadings lower than .32 were not interpreted. Factor scores were calculated using the factor scores function. Hierarchical clustering using Ward’s criterion was conducted on the factor scores to create a hierarchical tree. The number of clusters identified was based on the minimization of intra-cluster inertia and the visualization of elbow and silhouette plots. To enhance interpretation, data from both scales were standardized using min-max normalization and scores on the SPQ were reverse scored prior to the factor analysis.
ANOVAs were conducted to measure between-cluster differences on ages, factor scores and FIQR scores in the fibromyalgia group. Significant results were followed up with post-hoc tests using Tukey HSD corrected p values. ANCOVAs were also conducted with age and gender added as covariates.
A Kruskal Wallis test was used to measure between-cluster differences in scores on the PHQ-15. Significant results were followed up with three Mann Whitney U-tests using Bonferroni corrected p values.
Results
Hypothesis One – Subjective Perceptual Ability Will Be Reduced in the Fibromyalgia Group (Greater Scores on the SPQ)
Figure 1 displays raincloud plots for each SPQ modality and Figure 2 the total SPQ score. A MANOVA showed significant group differences for scores on the SPQ (F(1,307) = 23.34, p <0.001, partial eta squared =0.280). Follow-up univariate ANOVAs for each modality on the SPQ and the total SPQ score showed that the fibromyalgia group scored significantly lower (indicating higher subjective perceptual ability) in touch, hearing, vision and on the total SPQ score. No group differences were found for smell and taste (see Table 1). These findings therefore did not support our prediction that the fibromyalgia group would report reduced subjective perceptual ability. Group differences on the SPQ remained significant after controlling for age and gender (F(1,304) = 16.73, p <0.001, partial eta squared =0.220). Age (F(1,304) = 6.87, p <0.001, partial eta squared =0.100) and gender (F(2,304) = 2.90, p =0.001, partial eta squared =0.050) were both significant covariates. After adding PHQ-15 scores, group differences for the SPQ were no longer significant (F(1,303) = 1.79, p =0.115, partial eta squared =0.030). PHQ-15 scores (F(1,303) = 31.45, p <0.001, partial eta squared =0.340) and gender (F(1,307) = 1.99, p =0.033, partial eta squared =0.030) were both significant covariates within the second MANCOVA. A Mann Whitney U-test revealed that the fibromyalgia group had significantly higher PHQ-15 scores (Mdn= 19.00, range =28.00) than the healthy controls (Mdn= 7.00, range= 24.00; W= 21388, p <0.001, r=0.744; see Figure 2).
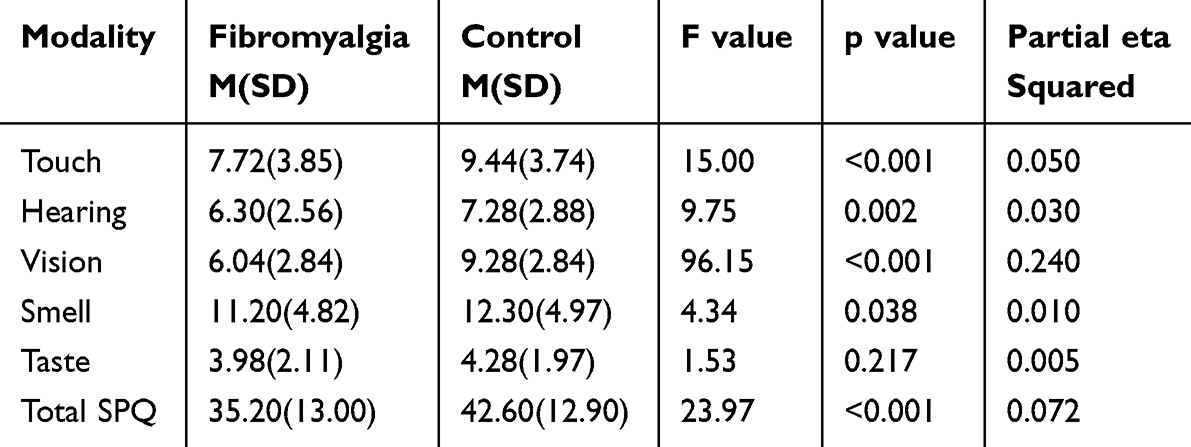 |
Table 1 Mean (Standard Deviation), F, p and Partial Eta Square Values for Comparisons on the SPQ |
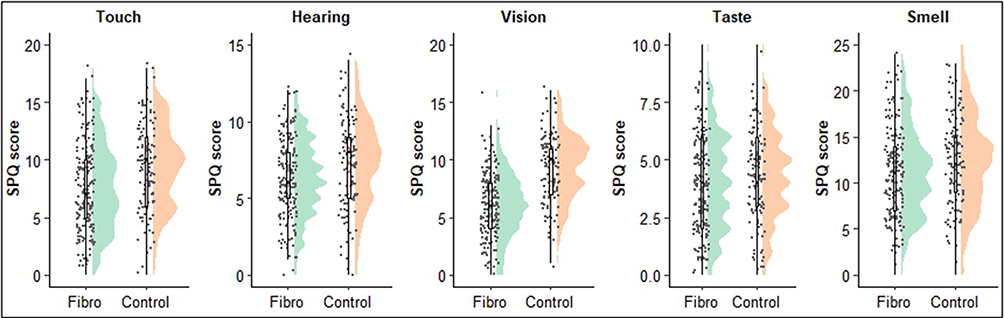 |
Figure 1 Raincloud plots for each SPQ modality. A lower score indicates higher subjective perceptual ability. Note: The distribution of the data for each group is shown in green and orange. Box plots represent the median and interquartile range with each point representing an individual participant. |
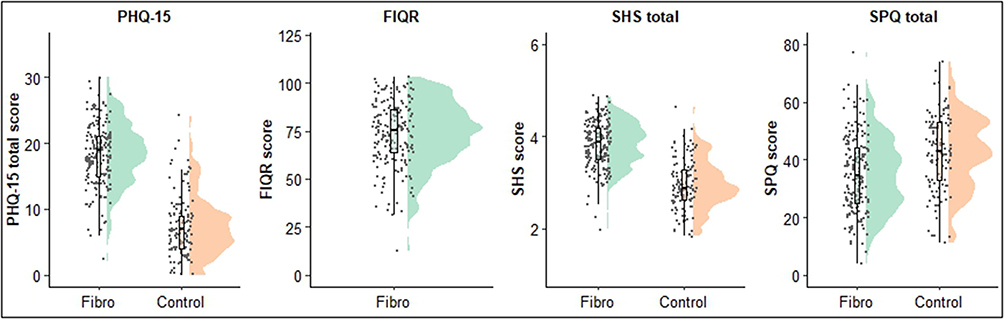 |
Figure 2 Raincloud plots for PHQ-15, FIQR, SHS total and SPQ total. |
Hypothesis Two – Self – Reported Intolerance Will Be Greater in the Fibromyalgia Group (Greater Scores on the SHS)
Figure 3 displays raincloud plots for each SHS modality and Figure 2 the total SHS score. Mann Whitney U-test comparisons for each SHS modality demonstrated that the fibromyalgia group had significantly higher responses for all modalities and the total SHS score (indicating greater intolerance; see Table 2). These findings therefore support our prediction that the fibromyalgia group would report increased intolerance across modalities.
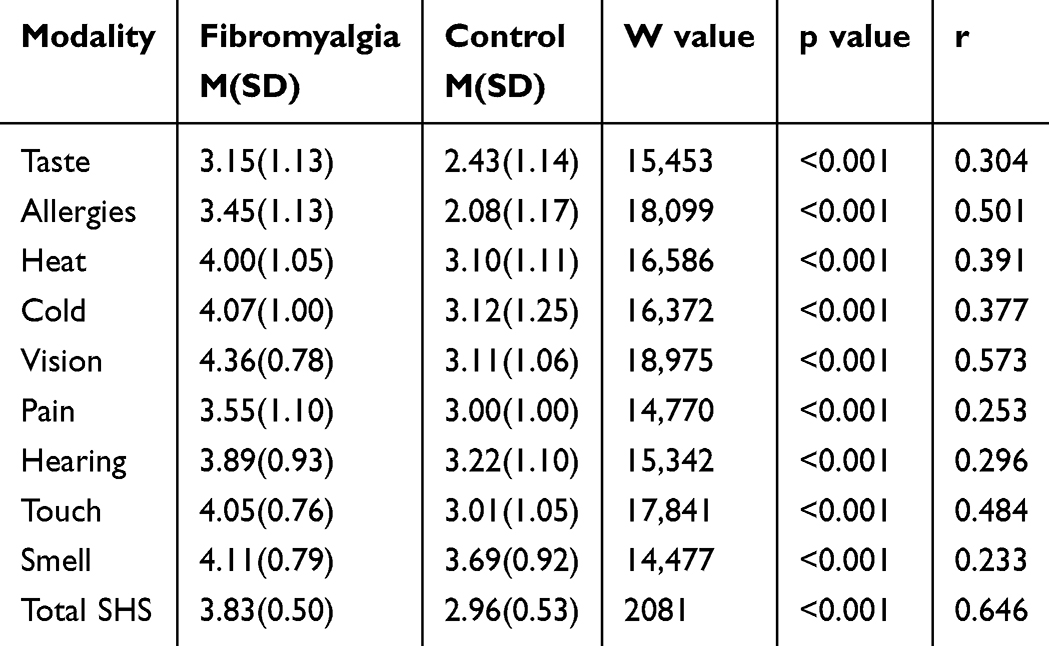 |
Table 2 Mean (Standard Deviation), W, p and r for All Comparisons on the SHS |
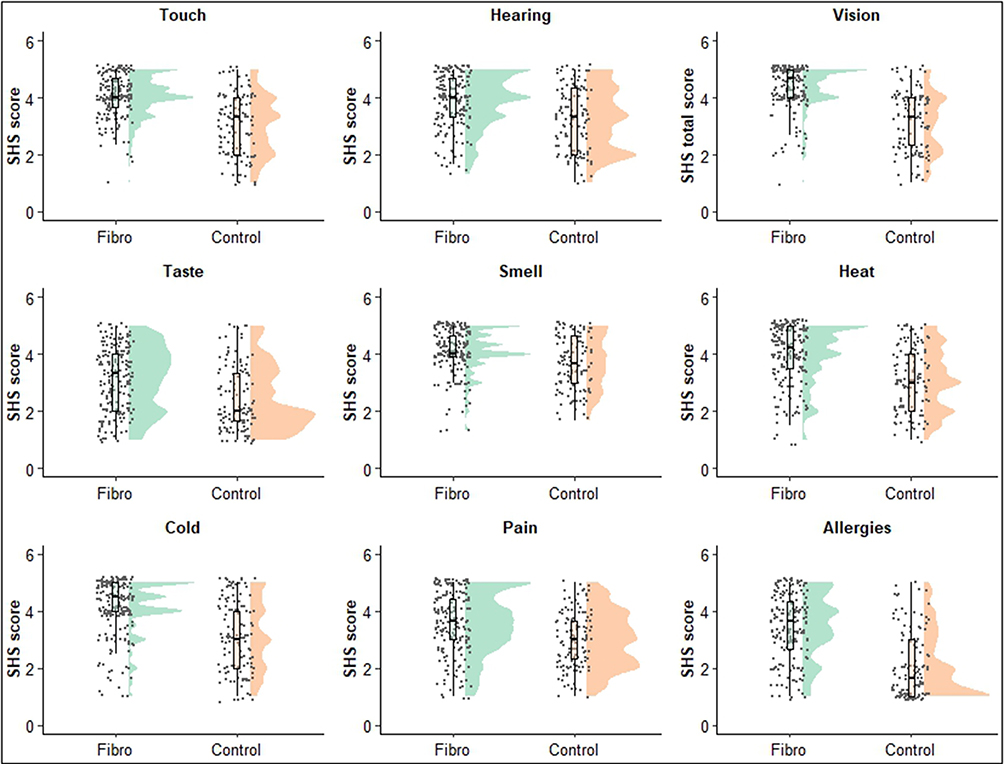 |
Figure 3 Raincloud plots for each SHS modality. Higher scores indicate greater intolerance. |
Multiple Regressions in the Fibromyalgia Group – Investigating the Relationship Between Questionnaire Variables and Fibromyalgia Severity
The regression model predicting fibromyalgia impact including scores for all modalities on the SPQ and SHS as predictor variables in addition to age was significant F(15,172) = 5.86, p <0.001, R2=0.338. SPQ hearing, SPQ vision, SHS hearing, SHS taste and SHS touch were found to be significant unique predictors of FIQR scores; all were positively associated with FIQR scores, with the exception of SPQ vision, which was negatively associated (VIF range 1.13–2.56). There is no clear explanation as to why SPQ vision shows the opposite pattern of results, however, low VIF values suggest that this is not due to multicollinearity. The remaining predictor variables were not significant (see Table 3). The regression model with total scores for the SHS and SPQ entered as predictor variables in addition to age was also significant F(3,184) = 18.84, p<0.001, R2=0.235. SHS total (t= 7.00, p<0.001, standardised b=0.49, Part2=0.204), was found to be the only significant unique predictor of the FIQR and was positively associated. SPQ total (t= 0.30, p=0.767, standardised b=0.02, Part2=0.001) and age (t= 1.13, p=0.258, standardised b=0.07, Part2=0.005) were not significant predictors (VIF range 1.02–1.18).
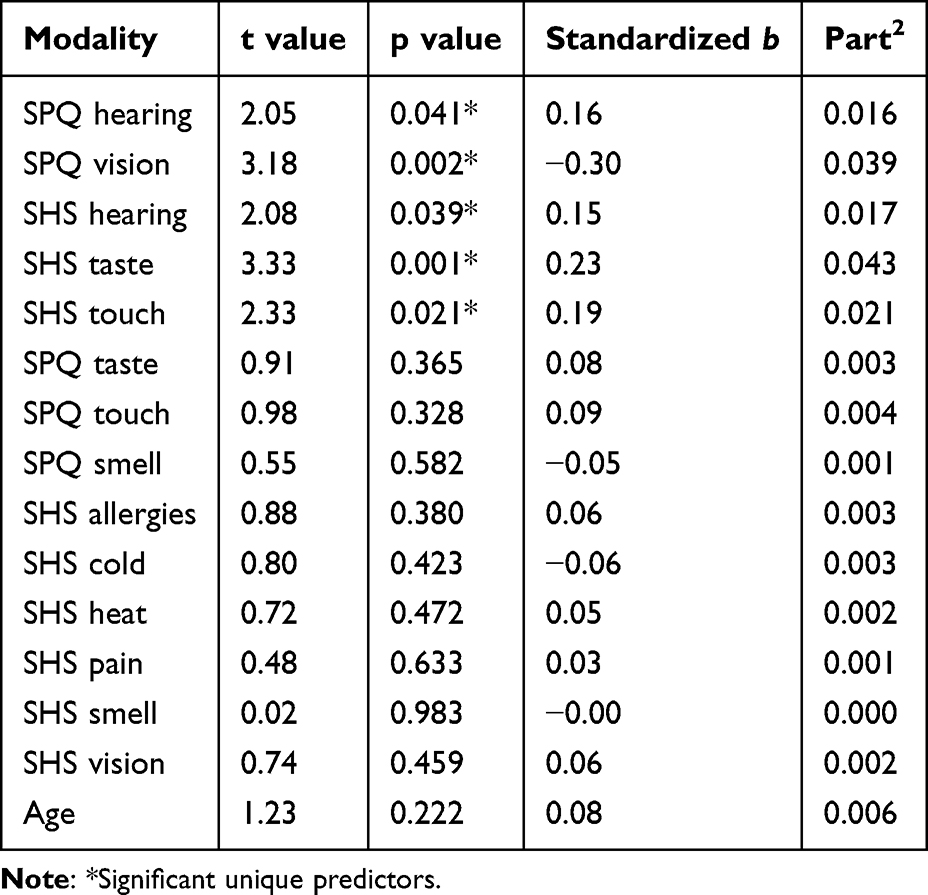 |
Table 3 t, p, Standardised b and Part2 for All Predictors in the Regression Model with All Modalities |
Exploratory Analysis
Factor Analysis – Investigating the Underlying Dimensions of the Scales
Exploratory factor analysis resulted in the identification of two factors, which explained 42% of the variance in the SPQ and SHS modality scores. Each of the SPQ modality variables and SHS smell positively loaded on factor one, which explained 22% of the variance. Each of the SHS modality variables apart from smell positively loaded on factor two, which explained 20% of the variance. See Figure 4 for a path diagram showing the factor loadings for each variable. Factor one appears to correspond to a measure of subjective perceptual ability while factor two corresponds to a measure of intolerance.
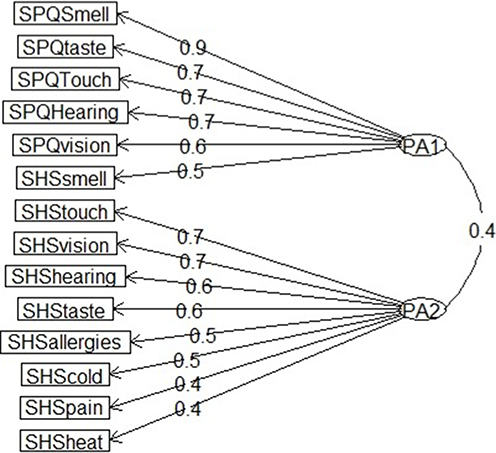 |
Figure 4 Factor loadings for each modality total score on the SPQ and SHS for the first two factors. |
Cluster Analysis – Exploring the Presence of Subgroups
Visual inspection of the dendrogram, elbow plot and silhouette plot suggested that four clusters was the optimal solution (see Figures 5a and b and supplementary Figures 1 and 2). Cluster one consisted primarily of healthy controls (92.5%), cluster two had sizable numbers of people with fibromyalgia (43%) and healthy controls (57%), and clusters three and four both consisted primarily of people with fibromyalgia (91% and 83.2% respectively; see Figure 5c for pie charts showing the breakdown of clusters for both groups.
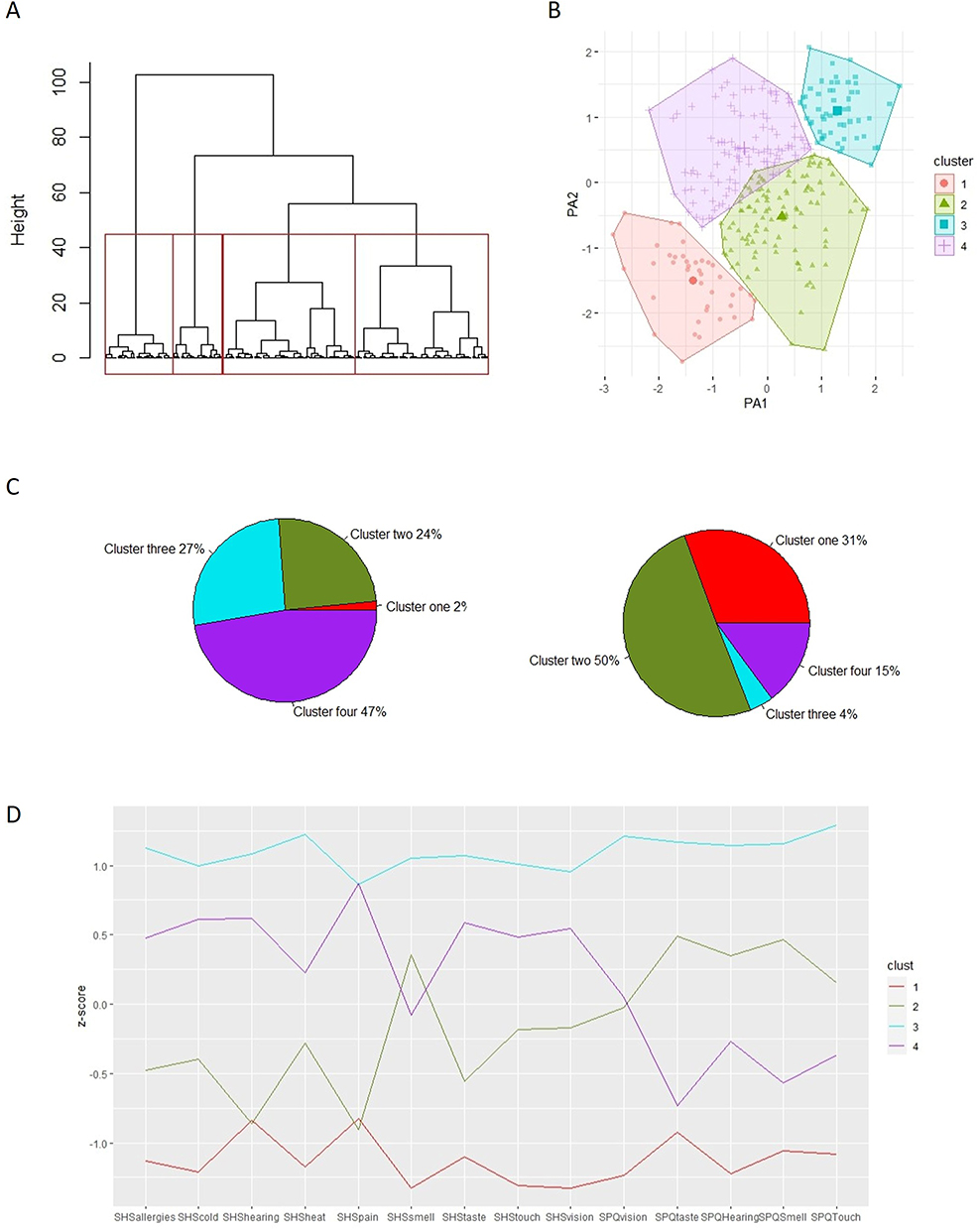 |
Figure 5 Results of the exploratory cluster analyses. Notes: 5A Dendrogram with four cluster solution highlighted in red. 5B Partitioning of the clusters on factor scores for factor one and two. 5C Pie charts showing the break-down of clusters for fibromyalgia sample (left) and control sample (right). 5D SHS modality and SPQ modality means for each cluster. |
A one-way ANOVA revealed between-cluster differences in ages (F (3,305) = 12.34, p<0.001, eta squared =0.108). Follow up post-hoc tests revealed that cluster one was significantly younger than clusters three (p=0.001, d=0.76) and four (p<0.001, d=0.72) and cluster two was significantly younger than clusters three (p<0.001, d=0.71) and four (p<0.001, d=0.67). There were no significant differences between the ages of clusters one and two (p=0.985, d=0.06) and three and four (p=0.991, d=0.05). There was an uneven spread of genders across clusters (X2(6) = 33.52, p <0.001). Descriptive statistics are in Table 4.
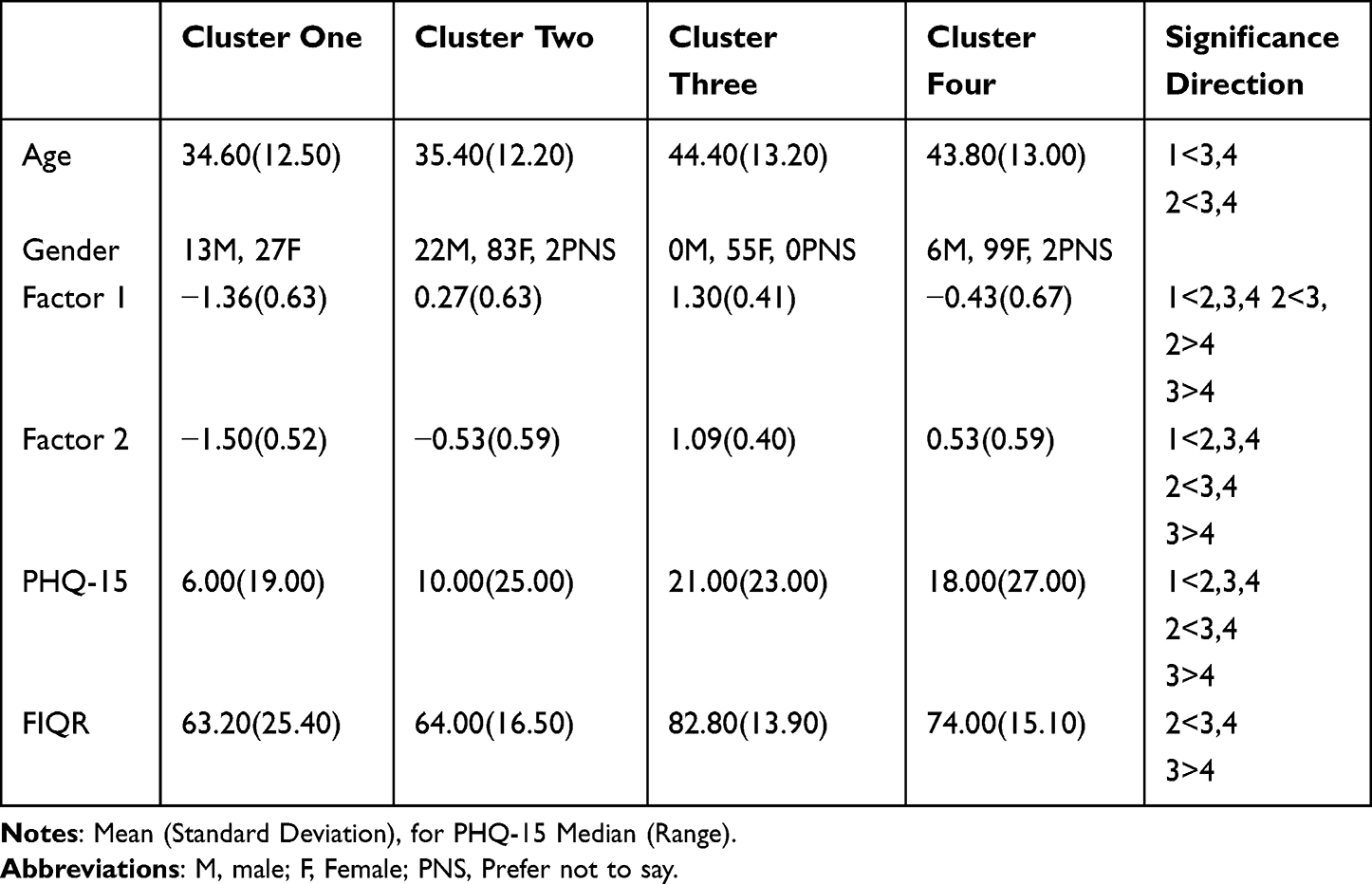 |
Table 4 Descriptive Statistics for Between Cluster Comparisons |
One-way ANOVAs revealed between-cluster differences on factor one (F (3,305) = 173.30, p<0.001, eta squared =0.630) and factor two (F (3,305) = 235.40, p<0.001, eta squared =0.700). For factor one, follow up post-hoc tests revealed that cluster one had significantly lower subjective perceptual ability than clusters two (p<0.001, d = 2.59), three (p<0.001, d =5.00) and four (p<0.001, d =1.43). Cluster two had significantly lower subjective perceptual ability than cluster three (p<0.001, d = 1.94), but higher than cluster four (p<0.001, d = 1.08). Finally, cluster three had significantly higher subjective perceptual ability than cluster four (p<0.001, d = 3.11). See Table 4 for descriptive statistics. Cluster differences for factor one remained significant after controlling for age and gender (F(3,302) = 173.90, p <0.001, partial eta squared =0.630). Age (F(1,302) = 0.19, p =0.665, partial eta squared <0.001) and gender (F(2,302) = 1.96, p =0.143, partial eta squared =0.004) were not significant covariates.
For factor two, post-hoc tests revealed that cluster one had significantly lower intolerance than clusters two (p<0.001 d = 1.74), three (p<0.001 d = 5.58) and four (p<0.001 d = 3.65). Cluster two had significantly lower intolerance than clusters three (p<0.001 d =3.21) and four (p<0.001 d =1.80). Finally, cluster three had significantly higher intolerance than cluster four (p<0.001 d =1.11). See Table 4 for descriptive statistics. Cluster differences for factor two remained significant after controlling for age and gender (F(3,302) = 240.19, p <0.001, partial eta squared =0.698). Gender was a significant covariate (F(2,302) = 3.88, p =0.022, partial eta squared =0.008), however, age was not significant F(1,302) = 1.43, p =0.233, partial eta squared =0.001). See Figure 5d for SHS modality and SPQ modality means for each cluster.
A Kruskal Wallis test revealed between-cluster differences on PHQ-15 scores (H (3)= 221.00 p <0.001, eta squared =0.410). Post-hoc tests demonstrated that cluster one scored significantly lower than clusters two (p <0.001, r =0.331), three (p <0.001, r =0.804) and four (p <0.001, r =0.635). Cluster two scored significantly lower than clusters three (p <0.001, r =0.635) and four (p <0.001, r =0.483) and cluster three scored significantly higher than cluster four (p <0.001, r =0.246; see Table 4 for descriptive statistics).
A one-way ANOVA revealed between-cluster differences on FIQR scores for people with fibromyalgia (F (3,184)= 12.57, p <0.001, eta squared =0.170). Post-hoc tests demonstrated that cluster two scored significantly lower than clusters three (p <0.001, d =1.23) and four (p =0.002, d =0.63) and cluster three scored significantly higher than cluster four (p =0.007, d =0.61; see Table 4 for descriptive statistics). As cluster one contained only a small number of people with fibromyalgia, post hoc comparisons were not conducted for this cluster. Cluster differences for scores on the FIQR remained significant after controlling for age and gender (F(3,181) = 12.44, p <0.001, partial eta squared =0.170). Age (F(1,181) = 0.31, p =0.576, partial eta squared =0.001) and gender (F(2,181) = 0.38, p =0.683, partial eta squared =0.003) were not significant covariates.
Discussion
The primary aim of the current study was to investigate how different aspects of subjective sensory processing, that is detection/discrimination and intolerance, are rated by people with fibromyalgia across different sensory modalities. Using the Sensory Hypersensitivity Scale (SHS),12 we found greater intolerance on all measured modalities in the fibromyalgia group, supporting our prediction that fibromyalgia is associated with increased sensory intolerance beyond the pain modality. Assessing perceived discrimination/detection abilities via the Sensory Perception Quotient, (SPQ)23 our findings showed that people with fibromyalgia reported enhanced subjective detection/discrimination abilities in touch, vision and audition, with no group differences in smell and taste. We therefore did not find support for our overall prediction that fibromyalgia would be associated with a self-reported impairment in basic perceptual ability across modalities.
Evidence of increased intolerance in the fibromyalgia group across all modality subscales replicates the findings of Dixon et al12 and extends this to include hearing, which did not reach significance in the previous study. The findings are also in line with experimental studies showing that people with fibromyalgia display a reduction in the intensity of a stimulus required to create an unpleasant or overwhelmed response in different sensory modalities.7 It is also consistent with evidence that people with fibromyalgia avoid certain sensory stimuli, for example bright lights.31 Evidence of increased intolerance across modalities further supports the notion that fibromyalgia may reflect a global disturbance in sensory processing, suggestive of a common underlying mechanism.
Our finding that people with fibromyalgia reported superior subjective discrimination and detection abilities in the touch, visual and hearing modality is at odds with recent evidence of impaired tactile discrimination and detection performance in this group.18,32 Only one recent study has used the SPQ in people with fibromyalgia and found superior subjective perceptual ability across sensory modalities relative to a non-fibromyalgia chronic pain group.31 Our study extends and builds on this by showing how sensory processing in fibromyalgia diverges from what would typically be expected in the general population.
Enhanced subjective perceptual ability in fibromyalgia is consistent with the generalized hypervigilance model of the condition, where a person with fibromyalgia is hypothesized to display heightened detection of sensory stimuli due to allocating more attentional resources towards potentially aversive stimuli.33 Objective evidence for hypervigilance in fibromyalgia is limited, however, casting doubt on this interpretation.34,35
An alternative explanation of our SPQ findings is that self-reported beliefs about basic perception do not reflect objective perceptual ability in fibromyalgia, at least for some participants. This explanation would be analogous to findings relating to interoception in fibromyalgia. Interoception refers to the detection of internal physiological changes and, according to one commonly cited model, encompasses three related constructs: interoceptive accuracy (objective measure of detection ability), sensibility (self-evaluated report of internal sensations) and awareness (meta-cognitive insight of ability).36 Findings have shown that while some people with fibromyalgia display reduced interoceptive accuracy,16 sensibility is increased,37 which may point to a discrepancy between objectively measured perceptual ability and the subjective experience of internal sensations in fibromyalgia. Further research is required to determine whether our finding of subjectively enhanced perception of external stimuli is similarly associated with objectively measured differences in perceptual ability.
The fact that taste and smell showed a different pattern of results on the SPQ to the other modalities may be because these are chemical senses which are processed, and therefore perceived, differently. Furthermore, smell and taste are argued to be the least dominant senses in humans,38 which may influence the degree of attention allocated towards them, affecting participants’ ratings of their perceptual ability in these modalities. As vision is suggested to be the most dominant sense, this may explain why the largest group difference was in this modality. In autistic adults, enhanced perceptual ability was reported across all modalities on the SPQ with the exception of smell, further suggesting that chemical senses are processed differently in terms of enhanced perception.23
An additional finding was that after controlling for symptom reporting (PHQ-15 scores), group differences on the SPQ were no longer present. This could be attributed to group differences being related to the tendency to experience and report somatic symptoms, which could be considered part of the wider fibromyalgia phenotype.39 In the literature on somatic symptom reporting, scores on measures like the PHQ-15 are often regarded as reflecting a trait-like tendency to experience and report disturbances in somatic awareness19 that may also be responsible for the elevated SPQ scores in our sample.
As an exploratory analysis, we conducted hierarchical clustering on factor scores for each of the subscales of the SPQ and the SHS. This enabled us to explore the underlying dimensions of both scales and investigate the presence of subgroups according to questionnaire responses. The exploratory factor analysis identified two underlying dimensions supporting our predictions that these questionnaires measure distinct underlying constructs (ie, intolerance and subjective perceptual ability). In a four-cluster solution, cluster one was predominantly made up of healthy controls and contained 31% of this sample who reported low intolerance and low subjective perceptual ability. Most people with fibromyalgia were spread across the other three clusters, which varied significantly in their self-reported intolerance and perceptual ability. Evidence of three distinct fibromyalgia groups supports the notion that people with fibromyalgia are heterogeneous with respect to perceptual processes. Particularly notable was a large cluster two comprising both healthy controls and people with fibromyalgia, pointing to normative perception in these participants. Most of the remaining participants with fibromyalgia were distributed across two clusters with increased intolerance to sensory stimuli across modalities, but which differed in subjective perceptual ability (cluster 3 rating themselves as having higher subjective perceptual ability and cluster 4 rating themselves as having lower subjective perceptual ability). Although caution is required when interpreting the findings of this analysis, they raise the possibility that different psychophysiological mechanisms contribute to symptom experience in different people with fibromyalgia. This should be explored in future research.
If the low subjective ability across sensory modalities reported by cluster four is matched by objectively poor performance, then this could support Bayesian accounts40 that implicate low perceptual precision as a key factor in the development of fibromyalgia. In contrast, the superior subjective perceptual ability reported by fibromyalgia participants in cluster three may be accounted for by hypervigilance towards external stimuli in this group.37 Within-group variability in the condition may explain the mixed findings in relation to hypervigilance in fibromyalgia more generally. A flare in fibromyalgia symptoms indicated by increased symptom reporting and increased scores on the FIQR in this cluster may also cause hypervigilance, resulting in enhanced subjective perceptual ability. However, experimental evidence that increased discrimination thresholds are correlated with the severity of fibromyalgia symptoms suggests that this explanation is unlikely.41 Furthermore, as the SPQ asks general questions about perceptual experiences, participants may be less likely to be influenced by their current state. An alternative explanation is that the heightened perceptual abilities reported by this group may be accounted for by exaggerated self-evaluation, resulting in a discrepancy between subjective and objective perceptual ability. Cluster three and four may therefore differ in terms of the accuracy of their perceptual self-awareness. Increased symptom reporting in cluster three may also suggest that reduced accuracy in self-awareness increases symptom severity. Similar findings have been reported in people with functional seizures where the discrepancy between objective and subjective measures of interoception positively predicted seizure frequency and dissociation.42 A similar pattern could indicate a role for impaired sensory meta-cognition in fibromyalgia, either as a cause or consequence of the condition. It should be noted that differences between the clusters may also be attributed to changes in the peripheral nervous system such as small fiber pathology.3 Another important question is the meaning behind the group of healthy controls classified as clusters three and four. Whether these findings are clinically interesting and highlight a risk of developing fibromyalgia or other functional symptoms remains to be seen and may be worth studying in the future.
Potential practical implications of these findings include the use of the SPQ and SHS questionnaires as a tool to identify distinct subgroups of fibromyalgia who might have different treatment needs, or people who may be a risk of developing fibromyalgia. Further research is first required, however, to untangle how subjective perceptual ability relates to objective perceptual ability in fibromyalgia and further investigate the presence of subgroups. Depending on the mechanism at play (eg Bayesian accounts, hypervigilance model) evidence of similar patterns of results across modalities in the current study could also suggests that improving perception in one modality may have the potential to reduce symptoms in a different modality. This would have clinical benefits as interventions could be designed around the most accessible and acceptable modality for patients. In general, the findings may also be used to raise awareness and improve education of how fibromyalgia can affect a person’s life beyond pain, affecting multiple sensory systems.
A strength of the study is that it begins to unpack how common usages of the term “sensitivity” may actually refer to different aspects of sensory processing. In the literature, sensitivity is frequently used as an umbrella term encompassing both tolerance and perceptual ability, which can lead to confusion regarding which construct is being measured and in the interpretation of findings. This is evident in Dorris et al’s31 study where increased sensitivity across modalities on the SPQ in fibromyalgia is interpreted as being an extension of an increased intolerance to pain. The findings of our factor analysis, which suggest that intolerance and subjective perceptual ability are distinct constructs, challenge this interpretation and suggest that future work should consider them separately.
A limitation of this study is that most questions in the SPQ are designed to measure increased perceptual ability as opposed to reduced perceptual ability. Higher scores on the SPQ may therefore represent the absence of superior perceptual ability rather than impaired perceptual ability itself. A recent revised method of scoring the SPQ which provides a separate score for hyposensitivity and hypersensitivity could help overcome this problem.43 An additional limitation of the study is that the SPQ and the SHS do not assess interoceptive modalities. It is therefore unclear whether people with fibromyalgia would also report increased intolerance and perceptual ability for interoceptive signals.
Conclusion
In conclusion, this study represents the first attempt to disentangle how both subjective perceptual ability and intolerance are affected in fibromyalgia across sensory modalities. Overall group comparisons showed that people with fibromyalgia report increased intolerance and increased subjective discrimination/detection ability in most measured modalities. While this supports the argument that fibromyalgia is associated with a global disturbance in sensory processing, findings of higher levels of subjective perceptual ability in fibromyalgia raises the question of how closely self-reported ability reflects objective ability. Exploratory cluster analysis revealed three distinct fibromyalgia subgroups warranting further investigation of fibromyalgia as a heterogenous condition, in which within-group differences should be considered when developing treatment strategies.
Abbreviations
fMRI, Functional Magnetic Resonance Imaging; PHQ-15, Patient Health Questionnaire 15; SHS, Sensory Hypersensitivity Scale; SPQ, Sensory Perception Quotient; FIQR, Revised Fibromyalgia Impact Questionnaire.
Data Sharing Statement
The data that support the findings of this study are openly available in the Open Science Framework at https://osf.io/27vfh/?view_only=ab4cdb907d4b4dafbb23f5ea9aa4c1c6.
Ethics Approval Statement
This study complies with the Declaration of Helsinki.
Ethical approval was granted by the University of Manchester (University research ethics committee 5 2021-10504-17619).
Consent was obtained by the study participants prior to study commencement.
Funding
This research was funded by a Versus Arthritis PhD Studentship award to HS (grant reference 22215).
Disclosure
The author(s) report no conflicts of interest in this work.
The abstract of this paper was presented at the Experimental Psychology Society meeting, Versus Arthritis Fellows meeting, The International British Neuroscience Association Festival of Neuroscience and the European Pain Federation as a poster presentation with interim findings. The poster’s abstract was published in The International BNA 2023 Festival of Neuroscience. Brain and Neuroscience Advances. 10.1177/23982128231180246 and the poster was published on the EPS website https://eps.ac.uk/wp-content/uploads/2022/12/Hayley-Shepherd.pdf.
References
1. Sarzi-Puttini P, Giorgi V, Marotto D, Atzeni F. Fibromyalgia: an update on clinical characteristics, aetiopathogenesis and treatment. Nat Rev Rheumatol. 2020;16(11):645–660. doi:10.1038/s41584-020-00506-w
2. Borchers AT, Gershwin ME. Fibromyalgia: a critical and comprehensive review. Clin Rev Allergy Immunol. 2015;49(2):100–151. doi:10.1007/s12016-015-8509-4
3. Sommer C, Üçeyler N. Small fiber pathology in fibromyalgia syndrome. Pain Rep Lippincott Williams Wilkins. 2024;10(1). doi:10.1097/PR9.0000000000001220
4. Jurado-Priego LN, Cueto-Ureña C, Ramírez-Expósito MJ, Martínez-Martos JM. Fibromyalgia: a review of the pathophysiological mechanisms and multidisciplinary treatment strategies. Biomed Multidisciplinary Digital Publishing Institute. 2024;12(7). doi:10.3390/biomedicines12071543
5. Russo M, Santarelli D, Georgius P, Austin PJ. A review of etiological biomarkers for fibromyalgia and their therapeutic implications. Pain Physician Am Soc Intervent Pain Physicians. 2024;27(8):495–506. doi:10.36076/ppj.2024.7.495
6. Wilbarger JL, Cook DB. Multisensory hypersensitivity in women with fibromyalgia: implications for well being and intervention. Arch Phys Med Rehabil. 2011;92(4):653–656. doi:10.1016/j.apmr.2010.10.029
7. McDermin AJ, Rollman GB, McCain GA. Generalized hypervigilance in fibromyalgia: evidence of perceptual amplification. Internation Association Study Pain. 1996;66:133–144.
8. Geisser ME, Glass JM, Rajcevska LD, et al. A psychophysical study of auditory and pressure sensitivity in patients with fibromyalgia and healthy controls. J Pain. 2008;9(5):417–422. doi:10.1016/j.jpain.2007.12.006
9. Hollins M, Harper D, Gallagher S, et al. Perceived intensity and unpleasantness of cutaneous and auditory stimuli: an evaluation of the generalized hypervigilance hypothesis. Pain. 2009;141(3):215–221. doi:10.1016/j.pain.2008.10.003
10. Schweinhardt P, Sauro KM, Bushnell MC. Fibromyalgia: a disorder of the brain? Neuroscientist. 2008;14(5):415–421. doi:10.1177/1073858407312521
11. Ten Brink AF, Proulx MJ, Bultitude JH. Validation of the Leiden visual sensitivity scale and visual discomfort scale in chronic pain conditions. Perception. 2021;50(5):399–417. doi:10.1177/03010066211005327
12. Dixon EA, Benham G, Sturgeon JA, Mackey S, Johnson KA, Younger J. Development of the Sensory Hypersensitivity Scale (SHS): a self-report tool for assessing sensitivity to sensory stimuli. J Behav Med. 2016;39(3):537–550. doi:10.1007/s10865-016-9720-3
13. Rafferty C, Ward J. Fibromyalgia is linked to increased subjective sensory sensitivity across multiple senses. Perception. 2024;53(4):276–286. doi:10.1177/03010066241234037
14. Lõpez-Solà M, Pujol J, Wager TD, et al. Altered functional magnetic resonance imaging responses to nonpainful sensory stimulation in fibromyalgia patients. Arthritis Rheumatol. 2014;66(11):3200–3209. doi:10.1002/art.38781
15. Haggard P, Taylor-Clarke M, Kennett S. Tactile perception, cortical representation and the bodily self. Curr Biol. 2003;13(5):170–173. doi:10.1016/s0960-9822(03)00115-5
16. Duschek S, Montoro CI, Reyes del paso GA. Diminished interoceptive awareness in fibromyalgia syndrome. Behav Med. 2017;43(2):100–107. doi:10.1080/08964289.2015.1094442
17. Martínez E, Guillen V, Buesa I, Azkue JJ. A distorted body schema and susceptibility to experiencing anomalous somatosensory sensations in fibromyalgia syndrome. Clin J Pain. 2019;35(11):887–893. doi:10.1097/AJP.0000000000000754
18. Gunendi Z, Polat M, Vuralli D, Cengiz B. Somatosensory temporal discrimination is impaired in fibromyalgia. J Clin Neurosci. 2019;60:44–48. doi:10.1016/j.jocn.2018.10.067
19. Van den Bergh O, Witthöft M, Petersen S, Brown RJ. Symptoms and the body: taking the inferential leap. Neurosci Biobehav Rev. 2017;74:185–203. doi:10.1016/j.neubiorev.2017.01.015
20. Hechler T, Endres D, Thorwart A. Why harmless sensations might hurt in individuals with chronic pain: about heightened prediction and perception of pain in the mind. Front Psychol. 2016;7:1–7. doi:10.3389/fpsyg.2016.01638
21. Moseley GL, Zalucki NM, Wiech K. Tactile discrimination, but not tactile stimulation alone, reduces chronic limb pain. Pain. 2008;137(3):600–608. doi:10.1016/j.pain.2007.10.021
22. Martínez E, Buesa I, Guillén V, Azkue J. Short-term improvements in the body schema can modulate pain perception in fibromyalgia syndrome Improvements in body schema modulates pain perception in FM syndrome. Clin Exp Rheumatol. 2022;40:1127–1135. doi:10.55563/clinexprheumatol/2vn0uh
23. Tavassoli T, Hoekstra RA, Baron-Cohen S. The Sensory Perception Quotient (SPQ): development and validation of a new sensory questionnaire for adults with and without autism. Mol Autism. 2014;5(1):1–10. doi:10.1186/2040-2392-5-29
24. Erdfelder E, Faul F, Buchner A. GPOWER: a general power analysis program. BehavRes Methods Instrum Comput. 1996;28(1):1–11. doi:10.3758/BF03203630
25. Kroenke K, Spitzer R, Williams J. The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms. Psychosom Med. 2002;64(2):258–266. doi:10.1097/00006842-200203000-00008
26. Bennett RM, Friend R, Jones KD, Ward R, Han BK, Ross RL. The revised fibromyalgia impact questionnaire (FIQR): validation and psychometric properties. Arthritis Res Ther. 2009;11(4):1–14. doi:10.1186/ar2783
27. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
28. R core team. R.
29. Ateş C, Kaymaz Ö, Kale HE, Tekindal MA. Comparison of test statistics of nonnormal and unbalanced samples for multivariate analysis of variance in terms of type-i error rates. Comput Math Methods Med. 2019;2019. doi:10.1155/2019/2173638
30. Tabachnick BG. Using Multivariate Statistics.
31. Dorris ER, Maccarthy J, Simpson K, McCarthy GM. Sensory perception quotient reveals visual, scent and touch sensory hypersensitivity in people with fibromyalgia syndrome. Frontiers in Pain Research. 2022;3. doi:10.3389/fpain.2022.926331
32. Augière T, Desjardins A, Paquette Raynard E, et al. Tactile detection in fibromyalgia: a systematic review and a meta-analysis. Frontiers in Pain Research. 2021;2(December):1–11. doi:10.3389/fpain.2021.740897
33. Duschek S, Werner NS, Limbert N, Winkelmann A, Montoya P. Attentional bias toward negative information in patients with fibromyalgia syndrome. Pain Med. 2014;15(4):603–612. doi:10.1111/pme.12360
34. Van Damme S, Van Hulle L, Spence C, Devulder J, Brusselmans G, Crombez G. Hypervigilance for innocuous tactile stimuli in patients with fibromyalgia: an experimental approach. Eur. J. Pain. 2015;19(5):706–714. doi:10.1002/ejp.593
35. Cardoso S, Fernandes C, Barbosa F. Emotional and attentional bias in fibromyalgia: a pilot ERP study of the dot-probe task. Neurol Ther. 2021;10(2):1079–1093. doi:10.1007/s40120-021-00287-8
36. Garfinkel SN, Seth AK, Barrett AB, Suzuki K, Critchley HD. Knowing your own heart: distinguishing interoceptive accuracy from interoceptive awareness. Biol Psychol. 2015;104:65–74. doi:10.1016/j.biopsycho.2014.11.004
37. Borg C, Emond FC, Colson D, Laurent B, Michael GA. Attentional focus on subjective interoceptive experience in patients with fibromyalgia. Brain Cogn. 2015;101:35–43. doi:10.1016/j.bandc.2015.10.002
38. Majid A, Roberts SG, Cilissen L, et al. Differential coding of perception in the world’s languages. Proc Natl Acad Sci U S A. 2018;115(45):11369–11376. doi:10.1073/pnas.1720419115
39. Wolfe F, Clauw DJ, Fitzcharles MA, et al. Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum. 2016;46(3):319–329. doi:10.1016/j.semarthrit.2016.08.012
40. Ongaro G, Kaptchuk TJ. Symptom perception, placebo effects, and the Bayesian brain. Pain. 2018;160(1):1. doi:10.1097/00006396-900000000-98882
41. Gunendi Z, Polat M, Cengiz B, Martínez-González LJ, Delgado-Fernández M, Álvarez-Cubero MJ. Somatosesnory temporal discrimination is impaired in fibromyalgia. Rheumatol Int. 2018;38(3):531–533. doi:10.1007/s00296-017-3896-x
42. Koreki A, Garfkinel SN, Mula M, et al. Trait and state interoceptive abnormalities are associated with dissociation and seizure frequency in patients with functional seizures. Epilepsia. 2020;61(6):1156–1165. doi:10.1111/epi.16532
43. Taylor E, Holt R, Tavassoli T, Ashwin C, Baron-Cohen S. Revised scored sensory perception quotient reveals sensory hypersensitivity in women with autism. Mol Autism. 2020;11(1). doi:10.1186/s13229-019-0289-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Western Medical Acupuncture Perception and Use for Pain Management Among Athletes: A Systematic Review
Chaabna K, Jithesh A, Cheema J, Aboughanem J, Mamtani R
Journal of Pain Research 2024, 17:357-366
Published Date: 26 January 2024
Motor Dysfunctions in Fibromyalgia Patients: The Importance of Breathing
Bordoni B, Escher AR
Open Access Rheumatology: Research and Reviews 2024, 16:55-66
Published Date: 7 March 2024