Back to Journals » Patient Preference and Adherence » Volume 17
Investigating the Effect of Adherence to Antipsychotic Therapy on the Length of Stay and Number of Hospitalizations in Patients with Schizophrenia – A Descriptive Analysis
Authors Barliana MI ![]() , Ramdini DA
, Ramdini DA ![]() , Afifah NN
, Afifah NN ![]() , Alfian SD
, Alfian SD ![]() , Sumiwi SA
, Sumiwi SA
Received 11 July 2023
Accepted for publication 20 October 2023
Published 1 November 2023 Volume 2023:17 Pages 2737—2747
DOI https://doi.org/10.2147/PPA.S430083
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Melisa Intan Barliana,1,2 Dwi Aulia Ramdini,3 Nadiya Nurul Afifah,1 Sofa Dewi Alfian,2,4 Sri Adi Sumiwi4
1Department of Biological Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jatinangor, Indonesia; 2Center of Excellence for Pharmaceutical Care Innovation, Universitas Padjadjaran, Jatinangor, Indonesia; 3Department of Pharmacy, Faculty of Medicine, Universitas Lampung, Bandar Lampung, Indonesia; 4Department of Pharmacology and Clinical Pharmacy Faculty of Pharmacy, Universitas Padjadjaran, Jatinangor, Indonesia
Correspondence: Melisa Intan Barliana, Department of Biological Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jl. Ir. Soekarno Km 21, Jatinangor, Sumedang, 45363, Indonesia, Email [email protected]
Background: Optimizing long-term outcomes in schizophrenia treatment requires effective pharmacological interventions. Medication adherence is known to influence clinical outcomes, yet there is a scarcity of studies examining its correlation with factors like Length of Stay (LOS) and re-hospitalization frequency. These outcomes are crucial indicators of how medication adherence affects overall patient well-being.
Purpose: This study aims to describe the effect of medication adherence on the length of stay (LOS) and number of hospitalizations in patients with schizophrenia.
Patients and Methods: A total of 157 subjects from the West Java Psychiatric Hospital were included in this cross-sectional retrospective study. Data, including demographics, comorbidities, duration of illness, antipsychotic adherence, LOS, and the number of hospitalizations, were collected from the patients’ medical records. All the data were analyzed using the Chi-Square (χ²) test with a significance level set at p < 0.05.
Results: Our findings showed that 88% of all schizophrenia inpatients were in the nonadherence group. The highest (40.7%) LOS (> 30 days) was found in the non-adherence group with discontinued therapy/stopped therapy group, while the highest percentage of patients with less than five hospitalizations was identified in the obedient and regular therapy group (94.4%). In the statistical results, we observed a significant association between therapy adherence (p = 0.043) and therapy regimen (p = 0.014) with gender. Additionally, the distinction between male and female schizophrenia patients demonstrated statistical significance (p = 0.000).
Conclusion: In this study, therapy adherence and therapy regimen were found to have a significant association with gender, as well as differences between the number of male and female schizophrenia patients that were statistically significant. While other variables may exhibit clinical associations, their statistical significance has not been fully depicted. The results of this study could be preliminary study for subsequent observational studies.
Keywords: adherence, antipsychotic, hospitalization, LOS, schizophrenia
Introduction
Schizophrenia is a psychosis, a mental disorder characterized by disruptions in thought processes, perceptions, emotions, sense of self, and social interactions, including language and behavior. In brief, schizophrenia is a chronic and severe illness affecting a large number of people, approximately 20 million, and it is one of the top 15 leading causes of disability worldwide.1,2 Furthermore, schizophrenia is also associated with increased mortality rates – as well as shortened lifespan that are reported to be two to four times higher than in the general population,3 rendering this disorder a serious threat.
Neurotransmission abnormalities, such as excess or deficiency of dopamine, serotonin, and glutamate, have provided the theoretical framework upon which the pathophysiology of schizophrenia is based. Furthermore, numerous studies have implicated aspartate, glycine, and gamma-aminobutyric acid in neurochemical imbalance of schizophrenia.4 Genetic factors also play a substantial role in the development of schizophrenia, a role that is both straightforward and incredibly complicated.5 Genetic studies, especially those on genetic polymorphism, have strongly suggested that many different genes increase the risk of developing schizophrenia.1 In addition, genetic polymorphism related to the therapeutic response of antipsychotics has been extensively studied.6–8
The goal of pharmacological and non-pharmacological treatment of schizophrenia is to improve symptoms, prevent potential relapse, and increase adaptive functioning so that patients can be integrated back into the community. Both types of treatment must be used to optimize long-term outcomes.9 The use of antipsychotics as a pharmacological therapy in schizophrenic patients is recommended by the American Psychiatric Association (APA) and other psychiatric associations. APA states that the use of antipsychotics should be monitored and observed for its subsequent effectiveness and side effects.3 The effectiveness of antipsychotic therapy can be evaluated by clinical response, which is influenced by various factors, including age, mode of onset of illness, gender, duration of psychosis, schizophrenia subtype, primary negative symptoms, signs of extrapyramidal or other side effects, genetic factors, and adherence to therapy.10–12 Failure to adhere to antipsychotic medication regimens results in prolonged antipsychotic treatment. Research indicates that individuals with moderate or light medication adherence have a 52% to 72% higher likelihood of being hospitalized for schizophrenia, with confidence intervals ranging from 30% to 75% and 49% to 100%, respectively, compared with the prolonged use of antipsychotic.13 Patients with schizophrenia switched to lurasidone experienced significantly fewer hospitalizations for all causes and mental health reasons, with comparable rates of schizophrenia-related hospitalization compared to those switched to quetiapine.14 Other study related to the increasing dose of antipsychotic does not give an impact on the decreased number of LOS and hospitalization. These findings align with previous research indicating that higher antipsychotic dosages do not provide clinical benefits. Optimized medication practices may offer positive effects, not only in managing schizophrenic symptoms but also in addressing violence in schizophrenic patients’.
In general, medication adherence improves clinical outcomes, thus adherence to antipsychotics is bound to improve outcomes in mental illnesses such as schizophrenia.15,16 Nonadherence to antipsychotic drugs can exacerbate negative symptoms and prognosis and increase the respective morbidity rates.16–20 Factors related to medication adherence involve age, substance abuse, poor insight, cognitive impairments, low level of education, minority ethnicity, poor therapeutic alliance, high intensity of delusional symptoms and suspiciousness, low socioeconomic status, and the development of an effective therapeutic relationship between patients and clinician/pharmacist.16–18 Besides, medication nonadherence also related to increased risk for relapse, extended length of stay (LOS) in hospital settings, and high risk for rehospitalization.21,22 A comparative study on oral versus long-acting injectable antipsychotics (LAIAs) stated that the actual type of antipsychotic, including its preparation form, affects patients’ compliance and therapy response, which is indicated by the number of rehospitalization events.23 The present study analyzed the adherence to antipsychotic therapy among schizophrenic patients and its association to LOS and the number of hospitalization events. We conducted a study to assess the impact of adherence to antipsychotic treatment on clinical outcomes, aiming to identify the primary factors associated with Length of Stay (LOS) and the frequency of hospitalizations. This study aimed to provide new insights into the relationship between medication adherence and these clinical parameters. This study therefore provides greater insight into the urgency of seeking antipsychotic compliance, especially among schizophrenia cases in Indonesia.
Materials and Methods
Study Design and Population
This is a nonexperimental, descriptive cross-sectional, and retrospective study among schizophrenia patients at the West Java Psychiatric Hospital (Rumah Sakit Jiwa Jawa Barat). A total of 305 data were collected from medical records data, including demographics, comorbidities, duration of illness, antipsychotic adherence, LOS, and the number of hospitalization events. The patients who met the inclusion criteria were 18–65 years old and diagnosed with schizophrenia spectrum disorder based on diagnostic and statistical manual of mental disorder IV (DSM IV). The data that are incomplete or cannot be traced and patients who have other psychiatric disease such as bipolar, depression, etc., would be excluded. A total of 157 patients are included in this study, as illustrated in Figure 1. All procedures and patient consent for reviewing medical records were waived by the Health Research Ethics Committee of Universitas Padjadjaran (No. 1127/UN6.C.10/PN/2017) due to the retrospective and anonymized nature of the study, in compliance with the Helsinki Declaration.
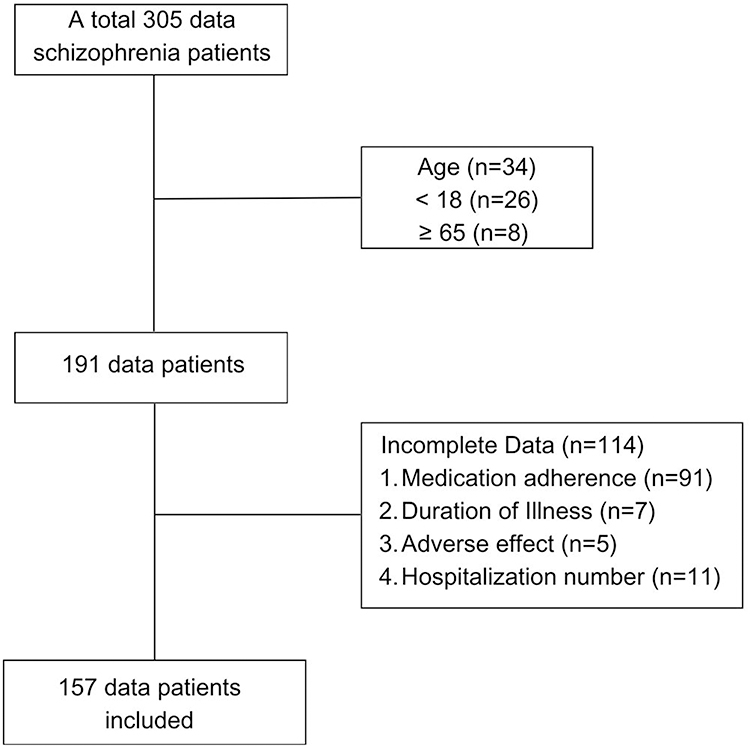 |
Figure 1 Research flowchart. |
Statistical Analysis
From this research, data on patient characteristics and clinical outcomes were obtained. To determine the relationship between patient characteristics and clinical outcomes, hypothesis testing was performed using the Chi-Square (χ²) test or the Fisher’s exact test for dichotomous data, and the Mann–Whitney U-test was used to assess the relationship between polytomous characteristic variables when the chi-square conditions were not met. The interpretation of the analysis results is based on the significance value (p-value). If the significance value is <0.05, it indicates a relationship between patient characteristics and clinical outcomes.
Results
Characterization of Patients Based on Medication Adherence
The majority of patients did not adhere to their medications (88.5%) (Table 1). The nonadherence group included patients with a history of discontinuing medication/drugs withdrawal or patients with medication-related issues, such as the development of adverse effects and accessibility to the therapy, which affected medication adherence. Many studies have investigated the association between medication adherence and the effectiveness of antipsychotic therapy. It has been known that adherence to an appropriate therapy is bound to increase the efficacy of the therapy and possibly reduce disease progression.24–26 Nevertheless, in this study, statistically significant differences were not found concerning the correlation between medication adherence and patient characteristics.
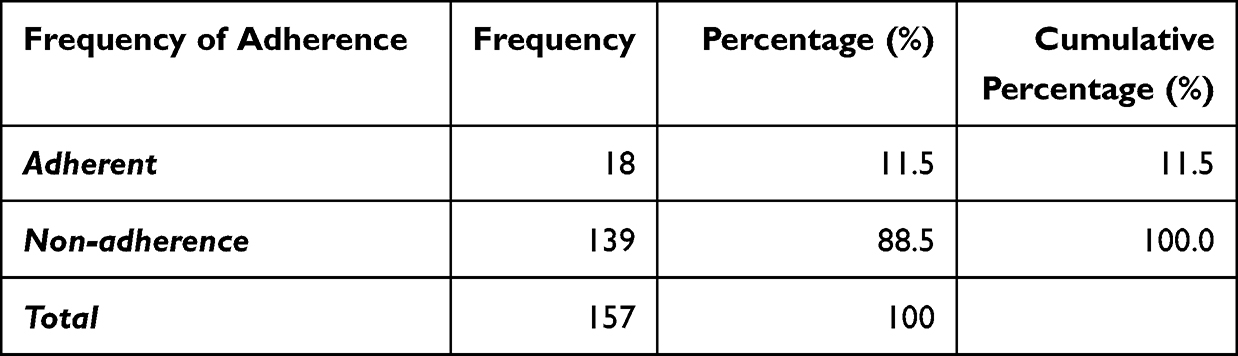 |
Table 1 Frequency of Medication Adherence |
Characterization of Patients Based on Gender
Males and females responded differently to medication adherence, including duration of the disease, age of onset, adverse side effects, LOS, and hospitalization events (Table 2). In addition, medication adherence between the two genders also has slight differences. The percentage of male patients was greater than females (70.1% vs 29.9%), and the majority of patients were over 20 years of age (95.7% and 95.5%, respectively) (Table 2). Most male patients had been diagnosed with schizophrenia less than 10 years (56.4%), whereas most female patients had been diagnosed less than 20 years (93.6%). Females were found to require less hospitalization time than men as indicated by the LOS (<30 days) among females and males (63.8% vs 60.0%). Meanwhile, the percentage of female patients with LOS of more than 30 days was 36.2% compared to 40.0% among males. In line with the LOS data, females had a lower number of rehospitalization events than men. More specifically, the percentage of female patients with less than five hospitalizations was greater compared to that among males (93.6 vs 90.9%), while hospitalization events of more than five times in females were lower than that in males (6.4% vs 9.1%). A relatively small number of patients (less than 10.0%) was identified to experience adverse effects, especially extrapyramidal syndrome (6.4% and 8.2% in females and males, respectively). Furthermore, discontinuation of therapy was more common among men than women (82.7% vs 68.1%), a finding which is consistent with the higher rate of adherence to therapy in females than in males (12.8% vs 10.9%), although the difference was small. In the statistical results, we observed a significant association between therapy adherence (p = 0.043) and therapy regimen (p = 0.014) with gender. Additionally, the distinction between male and female schizophrenia patients demonstrated statistical significance (p = 0.000).
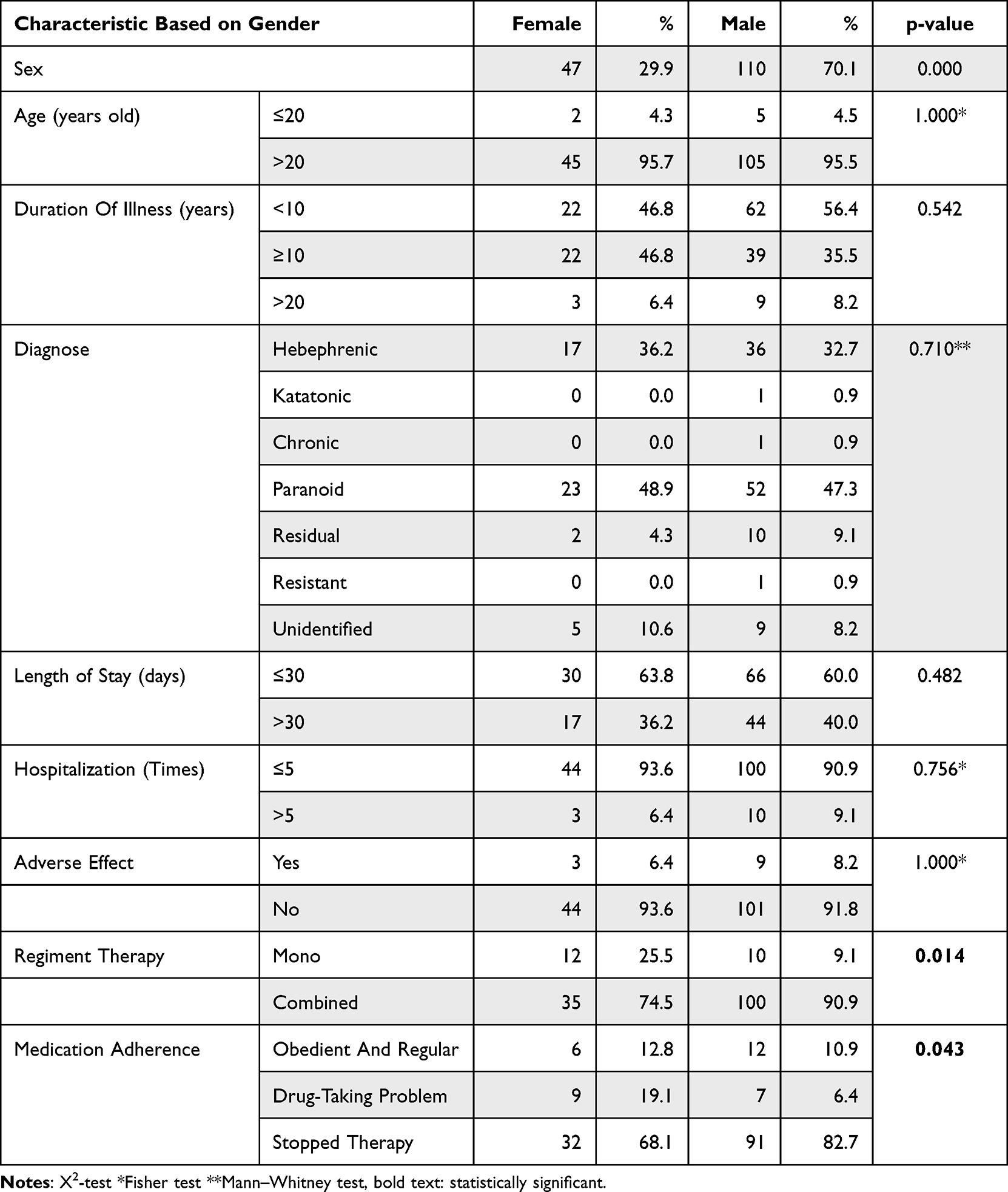 |
Table 2 Characteristic Based on Gender |
Characterization of Patients Based on Adherence
This study showed that medication adherence can be associated with several factors, including age, duration of illness, incidence of adverse effects, and regiment of therapy (Table 3). Although we did not find statistically significant associations between medication adherence and patient characteristics in this study, previous research has suggested that medication adherence to antipsychotics may indeed influence the length of stay (LOS) and the likelihood of rehospitalization events in individuals with schizophrenia. A high percentage of patients in all medication adherence categories was over 20 years of age (Table 3). In contrast, several parameters were found to affect medication adherence and the duration of illness, including the percentage of patients with obedient and regular medications, which decreased with increasing duration of illness (66.7% for <10 years, 22.2% for ≥10 years, and 11.1% for >20 years). Similarly, the percentage rate in the stopped therapy group decreased with the increasing duration of illness (56.1% for <10 years: 35.8% for ≥10 years, and 8.1% for >20 years). However, a distinct difference was found in the drug-taking group. The stopped therapy group had the highest percentage of patients with LOS > 30 days (40.7%). In addition, the obedient and regular therapy group had the highest percentage of patients with less than five hospitalization events (94.4%), whereas the stopped therapy group had the highest percentage of patients with more than five hospitalization events (8.9%). The drug-taking group had the highest percentage of adverse effect incidence (18.8%) followed by the stopped therapy group (7.3%), whereas there were no cases of adverse effect in the obedient and regular therapy group.
 |
Table 3 Patients Characteristic Based on Medication Adherence |
The Effect of Regiment Therapy on Clinical Outcomes
The monotherapy group had a higher percentage of LOS < 30 days than the combined therapy group (63.6% vs 60.7%) (Table 4). In addition, the monotherapy group had lower hospitalization rates than the combined therapy group (95.5% and 4.5% vs 91.1% and 8.9%). Meanwhile, the monotherapy group had zero cases of adverse effects, suggesting that all adverse effect cases occurred in the combined therapy group. It should be mentioned that the majority of patients who had been diagnosed with schizophrenia more than 10 years ago underwent a combined therapeutic approach rather than monotherapy (63.0% vs 45.5%). Our findings showed that patients with obedient and regular therapy had a smaller LOS (≤30 days) compared to the stopped therapy categories (61.1% vs 59.3%). Adherence to medication, not only to antipsychotic agents but also to almost all types of therapies, including antibiotics, has been known to influence clinical outcomes. The present study showed that the number of hospitalizations was higher on the stopped therapy group rather than the drug-taking and obedient or regular therapy groups (8.9%, 6.3%, and 5.6%, respectively). As mentioned before, adherence could be a predictor factor of 30-day hospital readmission events.
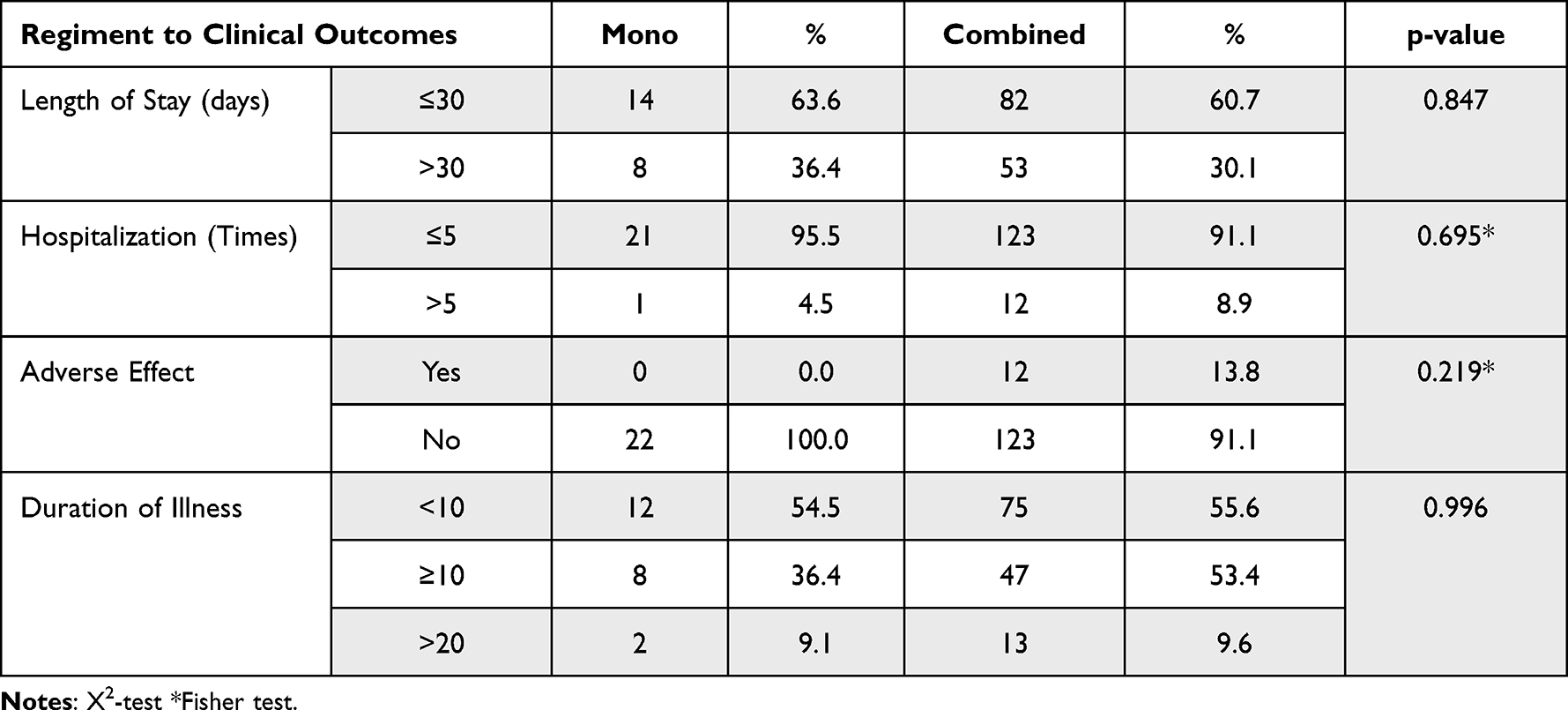 |
Table 4 Regiment Therapy and Clinical Outcomes |
Discussion
In general, mental illnesses require long-term therapy; thus, adherence to therapy has been recognized as a significant challenging aspect of the overall treatment.27,28 Basically, the use of long-term antipsychotic therapies can be explained by the provision of initial as well as maintenance therapy, of which the latter likely contributes to improving clinical practice and care for patients with psychotic diseases.29 Our findings are consistent with that statement and demonstrate that clinical outcomes tended to be worse in psychotic patients who had not received maintenance therapy. A large proportion of patients, ranging from 19.0% to 48.2%, were not on maintained therapy.30 The results of a meta-analysis study from 26 studies investigating the factors related to antipsychotic medication adherence and 17 studies investigating interventions to improve adherence in patients with psychosis spectrum disorders revealed that adherence to the antipsychotic agent was associated with the positive attitude shown by both patients and their families toward medication, family involvement, and illness insight. Consequently, it can be inferred that comprehensive intervention strategies should be designed to address factors associated with psychotropic medication nonadherence.31
Recent studies have shown that males and females have different prevalence rates, symptoms, onset, and clinical responses to psychiatric disease treatment, including schizophrenia.32–34 In addition, this study revealed statistically significant differences between male and female individuals diagnosed with schizophrenia (p = 0.000). Recent genetic studies have also suggested the presence of a significant sex-specific pathway in schizophrenia. Most of these studies indicate that genetic factors can influence the molecular pathogenesis of schizophrenia and can thus be considered a predictor of risk factors.35 The study found that gender influences the corresponding drug response through the amount of drug concentration related to the pharmacokinetic mechanism and the number of neurotransmitter receptors to which it can bind.10,36,37 Gender differences were also speculated to influence the pharmacokinetic process and predict the adverse reaction specifically in females. Furthermore, studies related to the influence of genetics on the risk of schizophrenia conducted in the UK found that 70.1% of patients with schizophrenia were males,10 which is consistent with the results of a previous review and meta-analysis studies stating that the incidence of schizophrenia was two to three times higher among males than females.38 Following the inclusion of all these studies (effect size: 49), the incidence risk ratio between men and women in terms of developing schizophrenia was 1.42 (95% confidence interval [CI], 1.30–1.56). In contrast, the incidence risk ratio was 1.31 (95% CI, 1.13–1.51) when studies that minimized selection biases were analyzed separately (effect size: 23) and 1.39 (95% CI, 1.15–1.68) when only high-quality studies were included (effect size: 11).39 The previous study concluded that the male sex is a major risk factor for more severe and therefore more easily recognizable forms of schizophrenia.39,40 Other previous studies also showed that genetic variations in Interferon gamma receptor 2 (IFGNR2) in the Tunisian population and Chromogranin B (CHGB) in the Korean population are significant risk factors for the development of schizophrenia in males.41,42 In the context of medication adherence, previous studies have shown that gender differences result in significant disparities between women and men regarding the intensity of their medication use, their adherence to prescribed medications, and their likelihood of receiving guideline-based drug therapy. Furthermore, with respect to the utilization of therapeutic regimens, it has been observed that women are more inclined towards combination therapies as compared to men.43 This aligns with the findings of our study, which identified statistically significant differences in medication adherence and therapy regimen based on gender.
Although schizophrenia can occur at any age, the age of onset is typically classified into two categories, before 20 years old or after 20 years old, based on the average onset of schizophrenia, which tends to be in the late teens to the early 20s for males and late 20s to early 30s for females. It is uncommon for schizophrenia to be diagnosed in people younger than 12 or older than 40.44,45 In the present study, we found that more than 95% patients with schizophrenia were over 20 years of age. In contrast, slightly more males than females were found to have an early onset at an age of less than 20 years (4.5% vs 4.3%, respectively).
A linear regression analysis of a Norwegian, multicenter, observational cohort demonstrated a trend towards shorter LOS when LOS was analyzed in patients after hospitalization with symptoms of schizophrenia who had been discharged alive (predicted mean difference −0.47, 95% CI (−1.02, 0.07), p = 0.081). In a competing risk analysis of LOS, the adherent group had a subdistribution hazard ratio (SHR) of 1.17 [95% CI (1.02, 1.34), p = 0.025] for discharge compared to the nonadherent group. Conclusions of adhering to antibiotic guidelines when treating infections in hospital inpatients were associated with favorable patient outcomes in terms of mortality and LOS.46 Another study on Parkinson's Disease stated that strict protocol adherence to the therapy could reduce LOS with a decrease in the actual/expected LOS ratio from 1.54 to 1.32 (p < 0.05).47 The dosage form is one of the factors that affect compliance. Some studies suggested that compliance could be maintained significantly more effectively when using injectable antipsychotics compared to oral antipsychotics. However, some studies stated that LOS was not statistically significantly reduced in patients receiving LAIAs following treatment with oral antipsychotics.23,47,48 Meanwhile, another study showed that LOS was associated with patients discharged from hospital [aOR: 3.65 (1.66–8.01), p = 0.001] and treatment for antipsychotic extrapyramidal side effects during hospitalization [aOR: 3.45 (1.32–9.03), p = 0.012]. Patients who had more interactions with medical providers during psychotic episodes prior to presentation at the unit were less likely to have a long LOS [aOR: 0.35 (0.16–0.76), p = 0.008].49 In addition to the association between medication adherence and LOS, adherence can also be used as a predictor factor of the 30-day hospital readmission, and thus to the number of hospitalization events in psychiatric patients.50 A study performed in Thailand demonstrated that 140 (24.1%) patients with schizophrenia had a significantly longer LOS rather than patients with optimal adherence (0.56 ± 2.64 days vs 0.06 ± 0.57 days; p < 0.01).51 The association between medication adherence and LOS has also been proved in several other diseases such as diabetes.52
Monotherapy versus combined therapy on antipsychotic treatment for schizophrenia has been widely studied. Monotherapy (single agent of SGA or FGA) versus combined therapy (SGA + FGA/ ECT/other agent) on antipsychotic treatment for schizophrenia has been widely studied. As per established algorithms, agents that used for schizophrenia are the Second Generation of Antipsychotics (SGAs) like aripiprazole, clozapine, olanzapine, quetiapine, risperidone, and ziprasidone, First Generation of Antipsychotics (FGAs) such as chlorpromazine, haloperidol, and fluphenazine, Electroconvulsive, and/or other agent such as mood stabilizer like lithium.53 Monotherapy has several advantages, including the ease of monitoring adverse side effects and medication adherence in patients. However, the availability of antipsychotic medications and their effectiveness on individuals can vary, indicating that not all patients can fully respond to a single antipsychotic drug. Consequently, prescription of a combination of antipsychotics might be necessary. A previous study showed that patients with low and intermediate adherence (combined therapy) had higher readmission rates compared to patients with high adherence (of 20.0% vs 9.3%, p = 0.005).50 In addition, the authors found that patients with low and intermediate medication adherence had an adjusted 2.54-fold higher odds of readmission compared to those in patients with high adherence (95% confidence interval [CI]: 1.32–4.90, p = 0.005). The model of predictive power, as measured by the c-statistic, improved from 0.65 to 0.70 after adding adherence.50 In the other case study performed in Thailand, patients with low adherence had the highest hospitalization rates (14 and 10 for all-cause and schizophrenia-related hospitalizations, respectively).51 Although that study does not provide a statistically clear picture regarding the association between adherence and hospitalization, the percentages obtained from our research study could be used as a predictor that adherence is indeed related to the hospitalization rates, an association that has already been verified in patients with cardiovascular or other diseases.54,55 Finally, even though our data has not been able to statistically described, our descriptive study confirmed the findings of a systematic review of prospective observational studies in that nonadherence to medication was associated with hospital admission.54
Drug-related factors such as the choice of medication, dosage, administration, and medical adherence are well recognized for their impact on clinical outcomes. Medical adherence is recognized as a factor that necessitates collaboration between healthcare providers and patients. The findings furnish pertinent insights into how both patient and hospital-related factors contribute to determining health status. These outcomes have the potential to guide improved targeting of mental health service policies and enhance the precision of information gathering and resource allocation.56
However, in addition to these drug-related factors, non-pharmacological elements, including psychosocial, environmental, and systemic factors such as education and economic status, can also influence Length of Stay (LOS) and re-hospitalization rates. A retrospective study conducted in China revealed the significance of these non-pharmacological factors in relation to the clinical outcomes of schizophrenia. This study represents the first attempt to investigate the influence of various factors, including biochemical indices, on the LOS for a specific mental disorder. Particularly noteworthy were the findings that marital status and Thyroid-Stimulating Hormone (TSH) levels were significantly associated with LOS in schizophrenia patients. These findings provide valuable reference points for LOS within the field of clinical psychiatry, potentially improving hospitalization management and the allocation of healthcare resources.57
Conclusion
In summary, this study suggests that the correlation between medication adherence to antipsychotic treatment in individuals with schizophrenia and both length of stay (LOS) and hospitalization numbers may exhibit clinical associations, but their statistical significance has not been definitively established. These findings provide a preliminary foundation for further observational studies to delve deeper into this relationship. Furthermore, our study has underscored the significance of gender differences within the schizophrenia population and demonstrated that gender is indeed associated with medication adherence. This adds to the growing body of knowledge regarding gender-specific factors influencing treatment adherence in individuals with schizophrenia. This information might encourage collaboration among healthcare professionals, including physicians, pharmacists, nurses, and social workers. Facilitate regular communication and information sharing to ensure a holistic approach to medication management.
Acknowledgments
We would like to express our sincere gratitude to all individuals who have contributed to the completion of this manuscript. A big thank you to Lanny Indah Permatasari, who provided us with statistical support for our manuscript in the midst of the peer review process. Foremost, all the West Java Psychiatric Hospital (Rumah Sakit Jiwa Jawa Barat) staff.
Funding
This research was funded by Grant-in-aids from Universitas Padjadjaran for MIB.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Schizophrenia. Available from: https://www.who.int/news-room/fact-sheets/detail/schizophrenia.
2. National Institute of Mental Health. Schizophrenia. Available from: https://www.nimh.nih.gov/health/topics/schizophrenia.
3. Keepers GA, Fochtmann LJ, Anzia JM, et al. The American psychiatric association practice guideline for the treatment of patients with schizophrenia. Am J Psychiatry. 2020;177(9):868–872. doi:10.1176/appi.ajp.2020.177901
4. Mueser KT, Jeste DV. Clinical Handbook of Schizophrenia. Guilford Press; 2011.
5. Howrigan DP, Rose SA, Samocha KE, et al. Exome sequencing in schizophrenia-affected parent–offspring trios reveals risk conferred by protein-coding de novo mutations. Nat Neurosci. 2020;23(2):185–193. doi:10.1038/s41593-019-0564-3
6. Vehof J, Burger H, Wilffert B, Al Hadithy A, Alizadeh BZ, Snieder H. Clinical response to antipsychotic drug treatment: association study of polymorphisms in six candidate genes. Eur Neuropsychopharmacol. 2012;22(9):625–631. doi:10.1016/j.euroneuro.2012.01.006
7. Li N, Cao T, Wu X, Tang M, Xiang D, Cai H. Progress in Genetic Polymorphisms Related to Lipid Disturbances Induced by Atypical Antipsychotic Drugs. Front Pharmacol. 2020;10:1669.
8. Hattori S, Suda A, Kishida I, et al. Effects of ABCB1 gene polymorphisms on autonomic nervous system activity during atypical antipsychotic treatment in schizophrenia. BMC Psychiatry. 2018;18(1):231. doi:10.1186/s12888-018-1817-5
9. Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A Pathophysiologic Approach. New York: McGraw-Hill Medical; 2014.
10. Reynolds GP. The pharmacogenetics of symptom response to antipsychotic drugs. Psychiatry Investig. 2012;9(1):1–7. doi:10.4306/pi.2012.9.1.1
11. Lieberman JA, Koreen AR, Chakos M, et al. Factors influencing treatment response and outcome of first-episode schizophrenia: implications for understanding the pathophysiology of schizophrenia. J Clin Psychiatry. 1996;57(Suppl 9):5–9.
12. Caqueo-Urízar A, Urzúa A, Mena-Chamorro P, Fond G, Boyer L. Adherence to antipsychotic medication and quality of life in Latin-American patients diagnosed with Schizophrenia. Patient Prefer Adherence. 2020;14:1595–1604. doi:10.2147/PPA.S265312
13. dosReis S, Johnson E, Steinwachs D, et al. Antipsychotic treatment patterns and hospitalizations among adults with schizophrenia. Schizophr Res. 2008;101(1–3):304–311. doi:10.1016/j.schres.2007.12.475
14. Newcomer JW, Ng-Mak D, Rajagopalan K, Loebel A. Hospitalization outcomes in patients with schizophrenia after switching to lurasidone or quetiapine: a US claims database analysis. BMC Health Serv Res. 2018;18(1):243. doi:10.1186/s12913-018-3020-2
15. Sendt KV, Tracy DK, Bhattacharyya S. A systematic review of factors influencing adherence to antipsychotic medication in schizophrenia-spectrum disorders. Psychiatry Res. 2015;225(1–2):14–30. doi:10.1016/j.psychres.2014.11.002
16. García S, Martínez-Cengotitabengoa M, López-Zurbano S, et al. Adherence to Antipsychotic Medication in Bipolar Disorder and Schizophrenic Patients: a Systematic Review. J Clin Psychopharmacol. 2016;36(4):355–371. doi:10.1097/JCP.0000000000000523
17. Byerly MJ, Nakonezny PA, Lescouflair E. Antipsychotic Medication Adherence in Schizophrenia. Psychiatric Clinics of North America. 2007;30(3):437–452. doi:10.1016/j.psc.2007.04.002
18. McCabe R, Bullenkamp J, Hansson L, et al. The therapeutic relationship and adherence to antipsychotic medication in schizophrenia. PLoS One. 2012;7(4):e36080. doi:10.1371/journal.pone.0036080
19. Novick D, Haro JM, Suarez D, Perez V, Dittmann RW, Haddad PM. Predictors and clinical consequences of non-adherence with antipsychotic medication in the outpatient treatment of schizophrenia. Psychiatry Res. 2010;176(2–3):109–113. doi:10.1016/j.psychres.2009.05.004
20. El-Mallakh P, Findlay J. Strategies to improve medication adherence in patients with schizophrenia: the role of support services. Neuropsychiatr Dis Treat. 2015;11:1077–1090. doi:10.2147/NDT.S56107
21. Bodén R, Brandt L, Kieler H, Andersen M, Reutfors J. Early non-adherence to medication and other risk factors for rehospitalization in schizophrenia and schizoaffective disorder. Schizophr Res. 2011;133(1–3):36–41. doi:10.1016/j.schres.2011.08.024
22. Zipursky RB, Menezes NM, Streiner DL. Risk of symptom recurrence with medication discontinuation in first-episode psychosis: a systematic review. Schizophr Res. 2014;152(2–3):408–414. doi:10.1016/j.schres.2013.08.001
23. Marcus SC, Zummo J, Pettit AR, Stoddard J, Doshi JA. Antipsychotic adherence and rehospitalization in schizophrenia patients receiving oral versus long-acting injectable antipsychotics following hospital discharge. J Managed Care Pharmacy. 2015;21(9):754–768. doi:10.18553/jmcp.2015.21.9.754
24. Yu W, Tong J, Sun X, et al. Analysis of Medication Adherence and Its Influencing Factors in Patients with Schizophrenia in the Chinese Institutional Environment. Int J Environ Res Public Health. 2021;18(9):4746. doi:10.3390/ijerph18094746
25. Goff DC, Hill M, Freudenreich O. Strategies for improving treatment adherence in schizophrenia and schizoaffective disorder. J Clin Psychiatry. 2010;71(SUPPL. 2):20–26. doi:10.4088/JCP.9096su1cc.04
26. Goff DC, Hill M, Freudenreich O. Treatment adherence in schizophrenia and schizoaffective disorder. J Clin Psychiatry. 2011;72(4):e13. doi:10.4088/JCP.9096tx6cc
27. Higashi K, Medic G, Littlewood KJ, Diez T, Granström O, De Hert M. Medication adherence in schizophrenia: factors influencing adherence and consequences of nonadherence, a systematic literature review. Ther Adv Psychopharmacol. 2013;3(4):200–218. doi:10.1177/2045125312474019
28. Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: a systematic review and meta-analysis. Syst Rev. 2020;9(1):17. doi:10.1186/s13643-020-1274-3
29. Marić NP, Andrić Petrović S, Jerotić S, et al. Maintenance phase treatment of psychotic disorders in outpatients from Serbia-focus on long-term benzodiazepine use) Maintenance phase treatment of psychotic disorders in outpatients from Serbia-focus on long-term benzodiazepine use Maintenance phase treatment of psychotic disorders in outpatients from Serbia-focus on long-term benzodiazepine use. Int J Psychiatry Clin Pract. 2020;24(3):315–321. doi:10.1080/13651501.2020.1767788
30. Peritogiannis V, Gogou A, Samakouri M. Very long-term outcome of psychotic disorders. Int J Social Psychiatry. 2020;66(7):633–641. doi:10.1177/0020764020922276
31. El Abdellati K, De Picker L, Morrens M. Antipsychotic Treatment Failure: a Systematic Review on Risk Factors and Interventions for Treatment Adherence in Psychosis. Front Neurosci. 2020;14:1019. doi:10.3389/FNINS.2020.531763/BIBTEX
32. Ayesa-Arriola R, de la Foz VOG, Setién-Suero E, et al. Understanding sex differences in long-term outcomes after a first episode of psychosis. Npj Schizophrenia. 2020;6(1):1–8. doi:10.1038/s41537-020-00120-5
33. Giordano GM, Bucci P, Mucci A, Pezzella P, Galderisi S. Gender Differences in Clinical and Psychosocial Features Among Persons With Schizophrenia: a Mini Review. Front Psychiatry. 2021;12:2430. doi:10.3389/FPSYT.2021.789179/BIBTEX
34. Pu C, Huang B, Zhou T, et al. Gender differences in the first-year antipsychotic treatment for Chinese first-episode schizophrenia. Neuropsychiatr Dis Treat. 2020;16:3145–3152. doi:10.2147/NDT.S280719
35. Seeman MV. The Pharmacodynamics of Antipsychotic Drugs in Women and Men. Front Psychiatry. 2021;12(April):1–7. doi:10.3389/fpsyt.2021.650904
36. Li R, Ma X, Wang G, Yang J, Wang C. Why sex differences in schizophrenia? J Transl Neurosci. 2016;1(1):37.
37. Franconi F, Campesi I. Sex and gender influences on pharmacological response: an overview. Expert Rev Clin Pharmacol. 2014;7(4):469–485. doi:10.1586/17512433.2014.922866
38. Iacono WG, Beiser M. Are males more likely than females to develop schizophrenia? Am J Psychiatry. 1992;149(8):1070–1074. doi:10.1176/ajp.149.8.1070
39. Al‐lssa I. Sex differences in the aetiology of schizophrenia. Applied Psychology. 1985;34(3):315–332. doi:10.1111/j.1464-0597.1985.tb01327.x
40. Sommer IE, Tiihonen J, van Mourik A, Tanskanen A, Taipale H. The clinical course of schizophrenia in women and men—a nation-wide cohort study. NPJ Schizophr. 2020;6(1):12. doi:10.1038/s41537-020-0102-z
41. Jemli A, Inoubli O, Trifa F, et al. IFNGR2 genetic polymorphism associated with sex-specific paranoid schizophrenia risk. Nord J Psychiatry. 2017;71(1):42–47. doi:10.1080/08039488.2016.1216595
42. Shin JG, Kim JH, Park CS, et al. Gender-specific associations between chgb genetic variants and schizophrenia in a Korean population. Yonsei Med J. 2017;58(3):619–625. doi:10.3349/ymj.2017.58.3.619
43. Manteuffel M, Williams S, Chen W, Verbrugge RR, Pittman DG, Steinkellner A. Influence of patient sex and gender on medication use, adherence, and prescribing alignment with guidelines. J Womens Health. 2014;23(2):112–119.
44. Rajji TK, Ismail Z, Mulsant BH. Age at onset and cognition in schizophrenia: meta-analysis. Br J Psychiatry. 2009;195(4):286–293. doi:10.1192/bjp.bp.108.060723
45. Stochl J, Whittier A, Wagner AP, et al. Association between developmental milestones and age of schizophrenia onset: results from the Northern Finland Birth Cohort 1966. Schizophr Res. 2019;208:228–234. doi:10.1016/j.schres.2019.02.013
46. Wathne JS, Harthug S, Kleppe LKS, et al. The association between adherence to national antibiotic guidelines and mortality, readmission and length of stay in hospital inpatients: results from a Norwegian multicentre, observational cohort study. Antimicrob Resist Infect Control. 2019;8:63. doi:10.1186/s13756-019-0515-5
47. Azmi H, Cocoziello L, Nyirenda T, et al. Adherence to a strict medication protocol can reduce length of stay in hospitalized patients with Parkinson’s Disease. Clin Park Relat Disord. 2020;3:100076. doi:10.1016/j.prdoa.2020.100076
48. Chou F, Reome E, Davis P. Impact on length of stay and readmission rates when converting oral to long-acting injectable antipsychotics in schizophrenia or schizoaffective disorder. Mental Health Clinician. 2016;6(5):254–259. doi:10.9740/mhc.2016.09.254
49. Barnett BS, Kusunzi V, Magola L, et al. Factors associated with long length of stay in an inpatient psychiatric unit in Lilongwe, Malawi. Soc Psychiatry Psychiatr Epidemiol. 2019;54(2):235–242. doi:10.1007/s00127-018-1611-1
50. Rosen OZ, Fridman R, Rosen BT, Shane R, Pevnick JM. Medication adherence as a predictor of 30-day hospital readmissions. Patient Prefer Adherence. 2017;11:801–810. doi:10.2147/PPA.S125672
51. Dilokthornsakul P, Thoopputra T, Patanaprateep O, Kongsakon R, Chaiyakunapruk N. Effects of medication adherence on hospitalizations and healthcare costs in patients with schizophrenia in Thailand. SAGE Open Med. 2016;4:205031211663702. doi:10.1177/2050312116637026
52. Pednekar P. Association of Medication Adherence with Hospital Utilization. J Manag Care Spec Pharm. 2020;26(9):1099–1108.
53. DiPiro JT, TRL, YGC, MGR, WBG, PLM. Pharmacotherapy: A Pathophysiologic Approach.
54. Mongkhon P, Ashcroft DM, Scholfield CN, Kongkaew C. Hospital admissions associated with medication non-adherence: a systematic review of prospective observational studies. BMJ Quality Safety. 2018;27(11):902 LP. doi:10.1136/bmjqs-2017-007453
55. Kim S, Shin DW, Yun JM, et al. Medication Adherence and the Risk of Cardiovascular Mortality and Hospitalization among Patients with Newly Prescribed Antihypertensive Medications. Hypertension. 2016;67(3):506–512. doi:10.1161/HYPERTENSIONAHA.115.06731
56. Smithnaraseth A, Seeherunwong A, Panitrat R, Tipayamongkholgul M. Hospital and patient factors influencing the health status among patients with schizophrenia, thirty days after hospital discharge: multi-level analysis. BMC Psychiatry. 2020;20(1):592. doi:10.1186/s12888-020-03001-4
57. Cheng P, Wang L, Xu L, Zhou Y, Zhang L, Li W. Factors Related to the Length of Stay for Patients With Schizophrenia: a Retrospective Study. Front Psychiatry. 2022;12:818254. doi:10.3389/fpsyt.2021.818254
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Interventions to Improve Medication Adherence in People with Schizophrenia: A Systematic Review
Cahaya N, Kristina SA, Widayanti AW, Green J
Patient Preference and Adherence 2022, 16:2431-2449
Published Date: 1 September 2022
Impact of COVID-19 Pandemic on Prescribing of Long-Acting Injectable Antipsychotics for Schizophrenia: Results from a United States Prescriber Survey
Zhdanava M, Starr HL, Totev TI, Lefebvre P, Shah A, Sheng K, Pilon D
Neuropsychiatric Disease and Treatment 2022, 18:2003-2019
Published Date: 7 September 2022
The Effect of Longer Dosing Intervals for Long-Acting Injectable Antipsychotics on Outcomes in Schizophrenia
Milz R, Benson C, Knight K, Antunes J, Najarian D, Lopez Rengel PM, Wang S, Richarz U, Gopal S, Kane JM
Neuropsychiatric Disease and Treatment 2023, 19:531-545
Published Date: 7 March 2023
Aripiprazole Plasma Concentrations Delivered from Two 2-Month Long-Acting Injectable Formulations: An Indirect Comparison
Harlin M, Chepke C, Larsen F, Bell Lynum KS, Chumki SR, Fitzgerald H, Such P, Madera-McDonough J, Yildirim M, Panni M, Saklad SR
Neuropsychiatric Disease and Treatment 2023, 19:1409-1416
Published Date: 8 June 2023
Xanomeline and Trospium Chloride Versus Placebo for the Treatment of Schizophrenia: A Post Hoc Analysis of Number Needed to Treat, Number Needed to Harm, and Likelihood to Be Helped or Harmed
Citrome L, Neugebauer NM, Meli AA, Kando J
Neuropsychiatric Disease and Treatment 2025, 21:761-773
Published Date: 5 April 2025