")
Back to Journals » Patient Preference and Adherence » Volume 16
Perceptions with Type 2 Diabetes Mellitus of the Value of Prescribed Medications Among Malaysian Adults: A Qualitative Study
Authors Lim MC , Hatah E , Lai KC, Buang A, Koay TJ, Sim WJY, Ng SC
Received 14 July 2022
Accepted for publication 1 November 2022
Published 29 November 2022 Volume 2022:16 Pages 3133—3142
DOI https://doi.org/10.2147/PPA.S382341
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ming Chiang Lim,1,2 Ernieda Hatah,3 Kay Chee Lai,1 Asdayati Buang,1,4 Tze Juin Koay,1 Wendy Jia Yii Sim,1 Suet Chee Ng1
1Pharmacy Department, Hospital Banting, Selangor, 42700, Malaysia; 2Pharmacy Department, Hospital Sultan Haji Ahmad Shah, Temerloh, 28000, Malaysia; 3Faculty of Pharmacy, Universiti Kebangsaan Malaysia, Kuala Lumpur, 50300, Malaysia; 4Pharmacy Department, Hospital Sultan Ismail Petra, Kelantan, 18000, Malaysia
Correspondence: Ernieda Hatah, Faculty of Pharmacy, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, Kuala Lumpur, 50300, Malaysia, Tel +603-9289 7328, Fax +603-2698 3271, Email [email protected]
Purpose: Previous studies show that customer loyalty and purchase intentions were influenced by perceived product value, but little is known about the factors that influence patients’ perceptions of the value of their subsidized prescriptions, when purchasing of medications were not required, and how these factors influence their medication adherence. Hence, this study aims to investigate perceptions of patients receiving subsidized medications regarding the value of their medication.
Patients and Methods: This qualitative study involved semi-structured, face-to-face interviews with patients diagnosed with type 2 diabetes mellitus at a government district hospital in Selangor state, Malaysia between June to September 2019. Using purposive sampling, patients were identified at an out-patient pharmacy during prescription refill. They were asked how they perceived the value of their medication. Interviews were audio recorded and then transcribed verbatim for thematic analysis.
Results: A total of thirty patients were interviewed. Patients’ perceptions on the value of medications were influenced by several factors such as trust, how the medications impact on their physical and social well-beings, and the perceived sacrificed made when the medications were procured and used. Perceptions on medication values were influenced by the recommendation received from someone they trust such as their doctors or significant others. It was also influenced by their perceptions of how the medication helps to improve their disease symptoms and affect their religious and social activities. Other factors include the perceived worth of the sacrifices made to access and use the medication.
Conclusion: Identifying factors that may influence patients’ perceived value of the medication may help improve healthcare practices.
Keywords: value, medication, adherence, subsidies
Plain Language Summary
Diabetes is a chronic condition that needs ongoing care and lifelong treatment. To ensure treatment effectiveness, adherence to medications is essential. Many factors could affect patients’ adherence towards medication, and this include the perceived value of the medication.
Semi-structured interviews were conducted with 30 patients with diabetes who received subsidized medications from a government district hospital to evaluate their perceived value of their medications. With patients’ consent, the interviews were audio-recorded and then transcribed verbatim for thematic analysis.
Patients with diabetes in the study setting were found to value their medications based on trust, perceived usefulness of the medication on their functional and social wellbeing, and sacrifices made to access and use the medications. The findings may help understand factors that are important in influencing patients’ perceived value of their medication, which in turn may aid in improving healthcare practices.
Introduction
Type 2 diabetes mellitus (T2DM) is a prevalent chronic condition that raises the risk of microvascular and macrovascular complications. It was estimated to cause 1.5 million deaths worldwide.1 Based on the National Health Morbidity Survey 2015, the prevalence of T2DM among adults in Malaysia has increased tremendously from 8.3% in 1996 to 22.5% in 2015.2 The number of people with diabetes in Malaysian population had doubled from 2 million in 2011 to 4.4 million in 2021.3 Many pharmacological treatment options are available for T2DM. However, treatment effectiveness is limited by patient’s non-adherence to medication. Previous studies reported only 50% of patients with T2DM adhered to their medications.4 Medication non-adherence may increase the likelihood of disease complications, resulting in higher healthcare costs. The International Diabetes Federation anticipated that the cost for diabetes management per person in 2021 would be USD 3048.00 or RM 13,523.98, potentially increasing countries’ economic burden.3
Medication adherence can be defined as “the extent to which a person’s behaviour in terms of taking medications corresponds with agreed recommendations from the healthcare provider”.5 Based on the World Health Organization (WHO), adherence is a multi-dimensional phenomenon that can be affected by multiple factors including socioeconomic, provider-patient/ healthcare system, condition, therapy and patient-related factors.5 In a previous study, socioeconomic factors such as medication cost was reported to influence medication adherence in patients with chronic diseases. Hsu et al found that over half of the hypertension patients in their study did not take their medication as prescribed due to the high cost of the medications.6 A systematic review also revealed that a reduction in patient cost-sharing such as lower co-payment and higher drug coverage and prescription caps were associated with better medication adherence.7 Nevertheless, contradictory findings were reported among underserved T2DM patients who received subsidized medications. A study found that, despite receiving the medication at no cost, patients’ adherence was poor at 56%.8 It is unknown if the medication non-adherence is related to the perceptions that lower-cost items are of lower quality, as reported in a previous study.9
A study among volunteers who were given a drink that purportedly helped their mental acuity in solving puzzles found their overall performance to be significantly lower when they had a discounted drink versus a regular-priced drink. The discounted price of the drink is thought to have generated assumptions that the product’s quality was inferior.10 In addition, a study among patients attending public hospitals in Malaysia found that patients underestimated or were unsure of the cost of their medication, despite it being clearly printed on the medication labels.11 It is unknown whether the underestimation of the medication cost was related to their perceived quality of the medication.
Besides medication costs, patients may appreciate and adhere to their medications if they valued the medications they receive.7 The perceived value of a product can be defined as a “consumer’s overall assessment of the utility of a product based on perceptions of what is received and what is given”.12 Value is affected by a product’s perceived quality and price, which in turn can be influenced by a product’s intrinsic attributes.13 Besides this simple and unidimensional measure of perceived value, extant literature has presented a multi-dimensional method that considers a variation in intangible, intrinsic, social, and emotional elements.14 A qualitative study among patients receiving subsidized medications in public hospitals in Malaysia shows that consumer’s perceived healthcare service quality is associated with their satisfaction.11 In other study, patients’ medication purchasing behaviour which may promote adherence to medication, was found to be influenced by patients’ perceptions of the benefit and value of the medication.15 A similar finding by Wong et al among White and Black veterans also reported that the willingness to pay for their medication, which promotes medication adherence, was influenced by the perceived value of medication.16 Nevertheless, previous studies have not explored factors that may influence perceptions of the value of the medications and healthcare services. Hence, this study aims to inquire of patients with diabetes their perceived value of subsidized medication received from public hospital in Malaysia and examine the factors that may influence it.
Materials and Methods
This qualitative study employed face-to-face semi-structured interviews with patients with T2DM attending a public hospital in Selangor, Malaysia between June and September 2019. The selected hospital is a district hospital that provides medical care to approximately 12,000 patients monthly in the out-patient clinics. The residents from the surrounding area were mainly Malay, Chinese and Indian, which were the three major ethnicities in Malaysia; they were fluent in either Malay or English or both languages.
Patients were identified at the out-patient pharmacy of the hospital while they filled their prescription of antidiabetic medications. Patients were invited to participate in the study if they were adults aged 18 years and above, able to speak and understand English or Malay languages, diagnosed with T2DM at least six months before the study, currently under follow-up at the diabetic clinic, and able to give informed consent. They were excluded from the study if they were diagnosed with other terminal illness such as end-stage cancer or human immunodeficiency virus, had any cognitive impairment such as Alzheimer’s disease or dementia, or had caretakers who were responsible for administering their medication. Purposive sampling, considering patients’ sociodemographic characteristics, disease condition, type of pharmacotherapy, and medication adherence status, were done for data triangulation to produce a maximum variation sample. The details on the criterion used for purposive sampling is provided in Supplementary File 1.
Before the interview, patients were explained the study purpose and were informed about their rights to participate in the study. If they agreed, they were asked to provide written informed consent included the publication of anonymized responses. Data on sociodemographic characteristics of the respondents were collected before the interview. Their confidentiality was assured by deidentifying individual data during the publication and presentation of study findings. Patients’ medication adherence levels were noted at the beginning of the interview by asking them to estimate their own medication-taking behavior, in terms of the percentage of doses that they may have missed over the past one month or the monthly frequency of when they were unable to follow the medication regime. Researchers then evaluated their response to determine the level of adherence. In this study, patients were classified in the “adherence” category if they claimed taking 80% or more of their medications.17
An interview guide was developed based on a review of previous studies.18–20 By applying the core conceptual model of consumption value theory and a multi-dimensional measure of perceived value, the interview guide included the following major dimensions of perceived value: functional, emotional, conditional, social, and perceived monetary and non-monetary sacrifices. This includes exploring patients’ perceptions on the value of medications such as medication effectiveness (functional), affective states before and after taking the medications (emotional), market choices or set of circumstances faced by the consumers such as side effects or any unwanted adverse reactions (conditional), social image (social value), perceived quality and price, the time, effort and energy required to receive or use their medications (monetary and non-monetary sacrifice) and any other potential input related to perceived value by the patients.12,18,21 Pilot interviews were conducted with three patients and the inputs obtained from these interviews were used to refine the topic guide (see topic guide in Supplementary File 2).
The interviews took place in the private counselling room at the outpatient pharmacy department and were conducted by trained interviewers AB, LKC, and KTJ, who are also pharmacists. The interviewers were trained by EH, who is an expert in qualitative studies to ensure that they possess sufficient knowledge, skills, and consistency when performing the interviews. No monetary incentives were offered to the patients who participated in the study; in terms of non-monetary incentives, they did not need to queue to get their prescription filled. The interviews were conducted in Malay or English, depending on patients’ preferences, and each interview lasted for approximately 30 to 40 minutes. Broad, open-ended questions were used during the interview and field notes were taken to capture some key points and observations. The interviews were tape-recorded with patients’ consent. Data collection ceased upon saturation of themes, such that there was no new theme emerging in two consecutive interviews. All interviewers did not have any affiliations or relationship with the participants.
All interviews were transcribed verbatim by individual interviewers and checked by WSJY and NSC, who listened to the recorded audio and reviewed the transcriptions. During the transcription, patients’ names and identifiers were removed to ensure confidentiality and reduce the risk of biases in the analysis. After the first few interviews, the research team gathered to discuss and compare their individual coding, which involved individual marking and categorizing key words, phrases, and texts to identify codes. A standardized coding scheme with definitions were then developed to ensure coding accuracy. If the interviewers found any new code, the team were informed and were provided with the example of quotes for consensus. LMC and EH then reviewed all the coding by referring to transcriptions, audio recordings, and field notes, to see whether there was any inconsistency in coding within or between the interviewers. The team met again when saturation of themes was perceived to be achieved by the individual interviewers. Any disagreements regarding the identified themes were resolved through consensus in which the majority of the team members agreed during the meeting. Content analysis was performed to identify the overarching themes using the thematic analysis methodology. Ethical approval for this study was sought from the National Medical Research Registry (NMRR) Ethics Community, National Institutes of Health (NIH) Malaysia with the reference number of NMRR-19-350-46328. This study was conducted in accordance with the principles of the Declaration of Helsinki and implemented relevant sections of the consolidated criteria for reporting qualitative research (COREQ) checklist.22
Results
A total of 30 patients were recruited in the study as the saturation of themes was achieved. The patients’ demographic characteristics are presented in Table 1. The median age (interquartile range) of the patients was 60.00 (15.25). There were 16 male and 14 female patients in the study. Majority of the patients had between two and four comorbidities including diabetes. The other common comorbidities experienced by the patients in this study were hypertension, dyslipidemia, and heart disease. Majority of the patients were diagnosed with diabetes for more than five years, had three medications for their illness, range between two and 11 types of medications and received oral hypoglycemic agents (OHA) as their treatment modalities. Most of them also had secondary school as their highest education level and had income of less than RM 3000 (USD 666.96) per month.
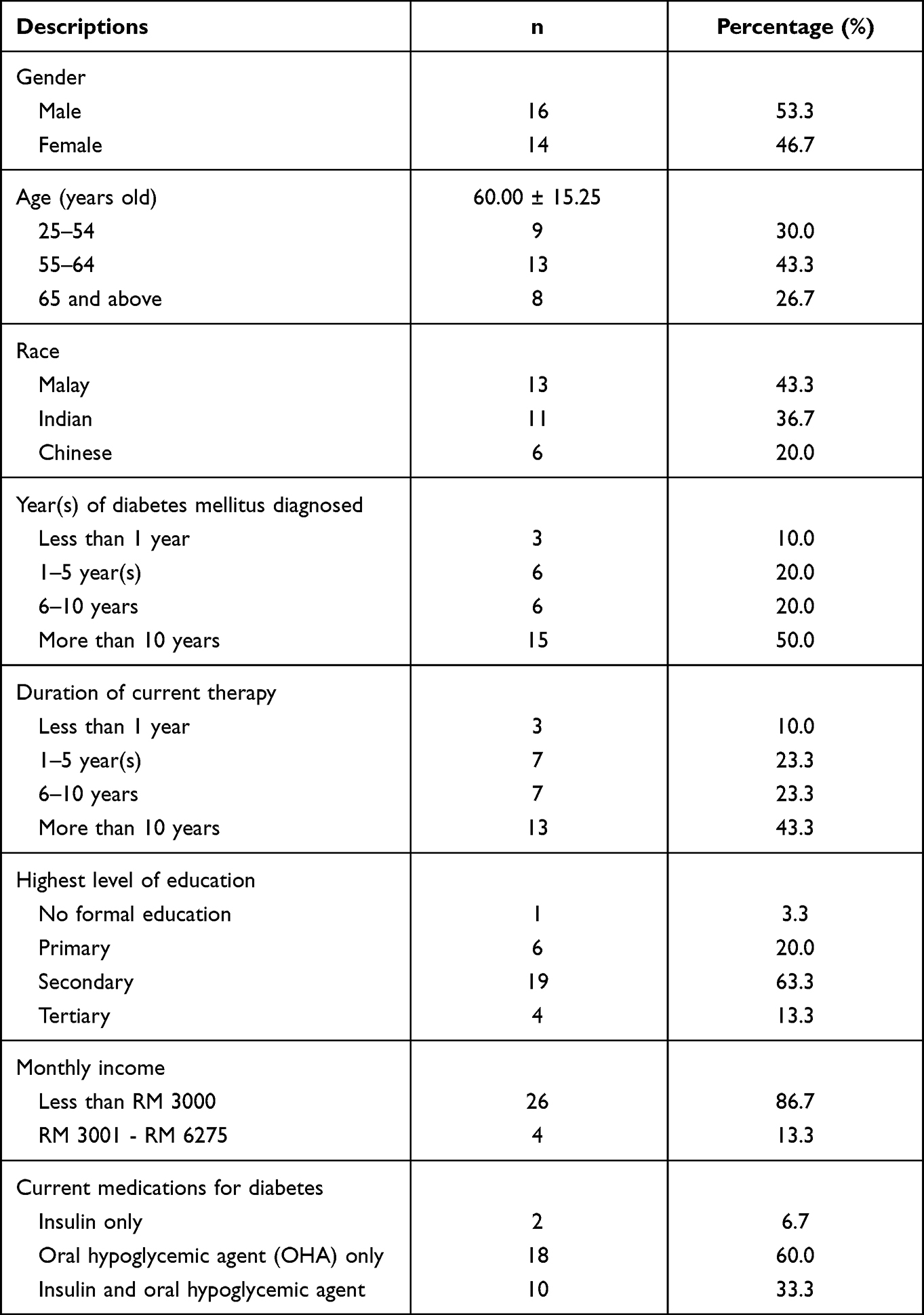 |
Table 1 Summary of Patients’ Demographic and Characteristics |
Several themes on patients’ perceptions of the value of their medications were found in the current study. These include trust, sacrifice, and impact of medications on patients’ physical and social well-being as summarized in Figure 1 Summary of Patients’ perception on medication value.
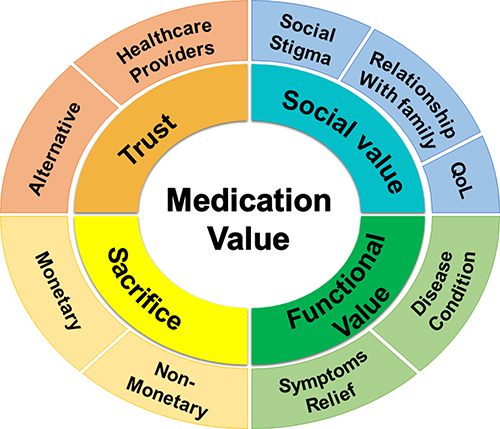 |
Figure 1 Summary of Patients’ perception on medication value. |
Perceived Value Through Trust
In the current study, “trust” was found to mediate the effect of patients’ perceived value on their treatment options. Patients were found to value or devalue their medication based on the recommendation received from someone they trust. This may include their doctor or significant others such as friends or family members. Patients who adhere to their prescribed medication valued their antidiabetic as they trust the choice made by their doctor were the best for them. Patients’ trust in healthcare providers was found to have developed based on the perceived credibility of the professional who prescribed the medications.
Depends on the advice from the doctor. I can’t decide it myself. They (the doctors) know better… (P17, Male, Adherence, OHA only)
I cannot simply stop taking the medications. I must listen to my doctor. If they told me I still have it (the health problem), it means that I must continue taking the medications. (P16, Male, Adherence, OHA and insulin)
The doctor knows my health problem well. I don’t mean that the other (treatment) option cannot be trusted, but I don’t know whether they will suit me or not. Since he (the doctor) has checked me, he knows which one will suit me better. I am afraid to try others (treatment option) as it may not suit me well’. (P15, Female, Adherence, OHA only)
On the other hand, trusting advice from people other than the doctor was found to mediate the patients’ perceived devaluation of their prescribed medication. Trust in a significant other’s recommendation was found to be influenced by the long-term relationship the patient has with them or if they have had similar experience in diabetes management. The perceived devaluation of the prescribed medication was more significant if the patients experience problems related to the medication such as side effects of the medication or if the medication did not achieve patients’ expectations. Others include that patient were afraid that they will develop over-dependency on the medication.
Oh, I don’t use the insulin - she (my sister) told me the insulin injection is not good for me (P6, Female, Non-adherence, OHA and insulin)
My aunty is also a patient with diabetes. She received the same medications as the one I received. She told me that by taking this (alternative treatment) my blood sugar level will be further reduced. So, I decided to try it (P29, Female, Non-adherence, OHA and insulin)
I took Chinese traditional preparation as well, so I took it 2 hours apart from my other medications. I would rather adjust the timing for my diabetes medication (metformin) for the traditional preparation (P6, Female, Non-adherence, OHA and insulin)
Perceived Value Through Impact on Physical and Social Well-Being
Patients were found to value or devalue their medication based on whether it helps to improve or reduce their physical or social well-being. This includes consideration of the medication’s effectiveness and side effects. Patients value their medication as it was perceived to improve the symptoms and disease condition, such as by improving their blood sugar level and quality of life, thereby enabling them to do their daily activities. They may devalue their medications if they feel that it does not help with their symptoms or worsen their quality of life.
I think the (prescribed) medication helps me because when I took it, my blood sugar level was 5.9 which is below than 10 (mmol/L) (P27, Male, Adherence, OHA only)
I feel better after taking the (prescribed) medications. I am not feeling tired anymore. (P18, Female, Adherence, Insulin only)
I felt I have less energy (after taking the medication) and yep more tired. (P11, Male, Non-adherence, OHA only)
I can’t sleep at night. The medication was supposed to help me to sleep but I can’t sleep. So, I do not take this (insulin injection) that frequent anymore (P12, Male, Non-adherence, Insulin only)
In terms of social well-being, patients value their medication as it allows them to do their religious activities and improves their social functioning with their family members and friends. This was perceived as control over the disease or symptoms.
Thank you to God that I was able to fast (during last Ramadhan). The medications somewhat also help me with my daily activities…praise to God. (P2, Female, Adherence, OHA only)
There is improvement in symptoms after I took the medications. If it doesn’t control, I may not be able to work and perhaps I may lose my job. This may interfere with my marriage as I cannot be the sole provider for the family (P1, Male, Adherence, OHA only)
If I didn’t take the medication, I will feel dizzy. I cannot stand and sit for more than 20 to 30 minutes or even speak long with my friends when we see each other (P20, Male, Non-adherence, OHA and Insulin)
Nevertheless, some of the patients devalue their medication as they feel that the medication had led to social stigma, distinguishing them from other members of a society or causing them to be disapproved socially. This was particularly evident especially among patients with insulin pen injection as stated in the following quotes:
I do not simply tell people that I have diabetes because they will talk bad or gossip behind me but yes sometimes, I just ignored them. (P29, Female, Non-adherence, OHA and insulin)
No, I can’t inject the insulin in front of my friends. I will only do it when I am at home. (P26, Female, Adherence, OHA and insulin)
Perceived Value Through Perceived Sacrifices
Patients who value the medication were found willing to sacrifice their money, effort, and time to be able to procure and use their medication as prescribed. This theme was commonly raised especially among patients who perceived the functional value of their medication. Patients felt that the effort, time, and money spent were worth their sacrifices as they were able to control their symptoms or disease. In addition, some patients value their subsidized prescribed medication in term of its monetary aspect as they get it for free or lower cost from the public health facilities. If they need to pay for their medication, some patients claimed that they may devalue the medication as they need to prioritize their expenditure over other things that may be more important such as food.
I don’t mind that I must travel and wait long to refill my medication. I think that it is worth the values that it gives me. I get it for free and I don’t need to spend my own pocket money to purchase it (from the community pharmacy) (P17, Male, Adherence, OHA only)
Some patients were also found to devalue their medications because of the sacrifices they or their significant others made to get the medications from the hospital. For example, some patients perceived that the time and effort spent to get the refilled medication from the hospital was not worth the value of the medications. Patients stated that it took their time away from work which may cause them to lose their income for that day. This is particularly important for some patients who have financial restrictions, or whose employers did not approve the time taken off from work. Some patients may devalue the medication as they may feel others need to make sacrifices for them, for example, when they need to rely on others for their medication refill.
I don’t think that it is worth my time. I must wait at least one to two hours to get my refilled medication and sometimes I just give up. (P13, Female, Adherence, OHA only)
My husband is working at night, so it is going to trouble him much to get the medication for me as I am afraid that he will be sleepy when driving (P29, Female, Non-adherence, OHA and insulin).
When he looked so tired, I felt sorry for asking him to accompany me to go for my follow up, so I decided not to go. (P29, Female, Non-adherence, OHA and insulin)
Some patients may also devalue their medication due to the perceived sacrifices that they had to undergo, such as controlling their diet and adhering to complex medication for long duration.
I don’t feel willing and happy to take my medications. Who will be happy if their medication is for lifelong? But yes, I must take it (P3, Female, Adherence, OHA only)
I feel stress as I must take my medication every day, but I have no option. (P2, Female, Adherence, OHA only)
Discussion
This qualitative study aimed to explore the potential factors influencing patients’ perception on the values of the subsidized medications. These patients’ perspective on the “values of medications” were examined based on the model of consumption value theory.18 Patients were found to value or devalue medications due to several factors. Based on the model of consumption value theory, values of products are categorized into five major dimensions - functional, social, emotional, epistemic, and conditional value. In the current study, patients were found to “value” their medication based on i) “trust”, ii) “how it impacts their physical and social well-being” and iii) “the perceived sacrifice that they underwent to obtain the medications”.
The patient’s “trust” in their medications or the healthcare professionals was found to influence the patient’s perceived value of the medications. On the other hand, patients devalue their prescribed medications if they trust alternative treatment and perceive it to help achieve their unmet expectations regarding the prescribed medication. This commonly occurs if patients had problems with their medication use, such as experiencing side effects or being too dependent on the medications. Patients may value the medication because they trust that the doctor’s choice was the best one for them. This trust in a healthcare professional’s decision may be associated with the power that the physician had in physician-patient relationship as reported by Friedman and Churchill (1987).23 Moreover, this may also be explained by the power-distance culture reported in Malaysia. In such a culture, people with lower authority usually follow and do not contradict the instructions or orders given by higher authorities such as doctors.24 Although shared decision making was encouraged between physician and patients, the non-readiness of both patients and healthcare practitioners hinders its implementation.25 Furthermore, since the patients in the current study were predominantly older, they were more likely to be devoted to and believe their doctors, as reported by Carter et al, this indicated that more senior patients were more inclined to trust their physicians because they were more conservative.26
Patients were also shown to value or devalue their medicine depending on the degree to which the drug affected their social and functional well-being. As the illness symptoms and condition improved, they value their medicine and feel motivated to take it. Motivation is a crucial component of behaviour change that may promote greater drug adherence which lead to better disease control.27 In terms of their social wellbeing, patients value their medicine because it enables them to practice their religious activities and strengthen their family ties. This was perceived to be connected to post-medication illness or symptom management. According to prior research by Aziz et al, patients appreciate their medicine since it affects their quality of life.11 Patients who participated in their study wished to maintain good health, avoid disease complications, and minimize disease symptoms so they could enjoy their social activities. This was also observed in the Wu et al’s study involving individuals with heart failure who exhibit a strong motivation to adhere to their medication regimens to remain healthy and have good quality of life.28
The current study also found several factors that may cause patients to devalue their medications. This applies if they believe that their medication did not help them perform better physically or if they encounter any side effects. Consumers frequently compare the advantages and compromises they must make to appreciate the value of the products. Consumers also frequently compare the expected value of the provided goods or services with the actual value to determine their level of satisfaction.29 According to reports, negative attitudes about medications are linked to notions about side effects and disruptions of lifestyle, as well as more esoteric concerns about long-term consequences and reliance.30 In addition, a patient may devalue their prescription if they believe that using it would differentiate them from other members of society or social stigma, which includes the strong disapproval of one’s actions by society. This was notably evidenced as some patients would not inject insulin in front of other people; a similar finding has been reported previously by Jha et al and Simon et al.31,32
Patients in the present study were also found to devalue their prescriptions if they were demotivated by the sacrifices they must make when taking the medications. Motivation can be defined as “the psychological forces or energies that impel a person towards a specific goal”.33 Patients are more likely to follow treatment plans if they feel that their disease is serious and will have major implications if untreated and that the drug will effectively treat their condition and avoid complications.33 Patients would feel ambivalent toward their drugs and would even devalue them if they were not convinced of their usefulness and were unable to overcome perceived obstacles or sacrifices such as food restrictions, complexity of prescription regimens, and a lack of drive for adherence.34 Nevertheless, in the current study, patients who value their prescribed medication were found to be prepared to make sacrifices in terms of their finances, time, and effort to use their medication as prescribed. For instance, patients may value their subsidized prescription medications because they believe it would lessen any potential financial sacrifice they may have to make if they had to pay for the medication out of pocket. Patients who valued the medication’s impact on their functional well-being were more prepared to forgo money for it, for example, if they had to buy it themselves, as well as the time and effort spent while refilling prescription at the hospital.
This study has several limitations. First, because we only included patients with diabetes in our study, extrapolating the findings to patients with other chronic illnesses is not possible. Second, since the study’s sampling technique focuses on enlisting patients who returned for prescription refills, the study may have overlooked the group that does not adhere to prescribed drugs and does not return for follow-up and prescription refills. These patients may offer a similar or different perceptions of the perceived value of the medications. Finally, despite the patients’ assurances that their answers would have no impact on their present clinical care, there was still a chance that they could have attempted to respond more positively while being interviewed by their healthcare providers and could have over-estimated their adherence level.
Conclusion
Patients’ perceptions of the value of their medications were shown to be influenced by trust, perceived sacrifice, and the effect of medications on their health and social well-being. The findings may aid in enhancing health care practices by fostering strong doctor-patient relationships, understanding the sacrifices patients make, and considering how the medicine impacts patients’ physical and social wellness. The perceived value of patients’ medications may affect their motivation and behavioral changes related to medication adherence; however, this may need to be further explored.
Abbreviations
T2DM, Type 2 diabetes mellitus; OHA, oral hypoglycemic agents.
Acknowledgments
We are grateful to all the patients who willingly involve in this study. We would like to thank the Director General of Health Malaysia for his permission to publish this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Fact sheets on Diabetes. Geneva: World Health Organization; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/diabetes.
2. Institute for Public Health (IPH), Ministry of Health (MOH) Malaysia. The National Health Morbidity Survey 2015: non-communicable diseases, risk factors & other health problems. Kuala Lumpur: Institute for Public Health (IPH), Ministry of Health (MOH) Malaysia; 2015. Available from: http://iku.moh.gov.my/images/IKU/Document/REPORT/nhmsreport2015vol2.pdf.
3. International Diabetes Federation (IDF). The IDF diabetes atlas. Belgium: International Diabetes Federation (IDF); 2021. Available from: https://diabetesatlas.org/idfawp/resource-files/2021/07/IDF_Atlas_10th_Edition_2021.pdf.
4. Ahmad NS, Ramli A, Islahudin F, Paraidathathu T. Medication adherence in patients with type 2 diabetes mellitus treated at primary health clinics in Malaysia. Patient Prefer Adherence. 2013;7:525–530. doi:10.2147/PPA.S44698
5. World Health Organization. Adherence to long-term therapies: evidence for action. Geneva: World Health Organization (WHO); 2003. Available from: http://www.who.int/chronic_conditions/adherencereport/en/.
6. Hsu J, Price M, Huang J, et al. Unintended consequences of caps on Medicare drug benefits. N Engl J Med. 2006;354(22):2349–2359. doi:10.1056/NEJMsa054436
7. Aziz H, Hatah E, Bakry MM, Islahudin F. How payment scheme affects patients’ adherence to medications? A systematic review. Patient Prefer Adherence. 2016;10:837–850. doi:10.2147/PPA.S103057
8. Bailey GR, Barner JC, Weems JK, et al. Assessing barriers to medication adherence in underserved patients with diabetes in Texas. Diabetes Educ. 2012;38(2):271–279. doi:10.1177/0145721711436134
9. Rao AR, Monroe KB. The moderating effect of prior knowledge on cue utilization in product evaluation. J Consum Res. 1988;15:253–264. doi:10.1086/209162
10. Shiv B, Carmon Z, Ariely D. Placebo effects of marketing actions: consumers may get what they pay for. J Mark Res. 2005;42(4):383–393. doi:10.1509/jmkr.2005.42.4.383
11. Aziz H, Hatah E, Bakry MM, Islahudin F, Hamdi NA, Wan IMP. Qualitative exploration of the modifiable factors for medication adherence among subsidised and self-paying patients in Malaysia. BMC Health Serv Res. 2018;18:605. doi:10.1186/s12913-018-3417-y
12. Zeithmal VA. Consumer perceptions of price, quality, and value: a means-end model and synthesis of evidence. J Mark. 1988;52(3):2–22. doi:10.1177/002224298805200302
13. Chang TZ, Wildt AR. Price, product information, and purchase intention: an empirical study. J Acad Mark Sci. 1994;22(1):16–27. doi:10.1177/0092070394221002
14. Sánchez-Fernández R, Ángeles M. The concept of perceived value: a systematic review of the research. Mark Theory. 2007;7(4):427–451. doi:10.1177/1470593107083165
15. Fuldeore MJ. Evaluating the Impact of Cost, Benefit and Value on Prescription Drug Purchasing Behavior [Dissertation]. Accra: Auburn University; 2005.
16. Wong ES, Maciejewski ML, Liu CF. Does the association between prescription differ by race? J Health Care Poor Underserved. 2013;24(3):1317–1330. doi:10.1353/hpu.2013.0152
17. Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:217047. doi:10.1155/2015/217047
18. Sheth JN, Newman BI, Gross BL. Why we buy what we buy: a theory of consumption values. J Bus Res. 1991;22(2):159–170. doi:10.1016/0148-2963(91)90050-8
19. Sweeney JC, Soutar GN. Consumer perceived value: the development of a multiple item scale. J Retail. 2001;77(2001):203–220. doi:10.1016/S0022-4359(01)00041-0
20. Demirgüneş BK. Relative importance of perceived value, satisfaction and perceived risk on willingness to pay more. Int Rev Manag Mark. 2015;5(4):211–220.
21. Shukla P. Effects of perceived sacrifice, quality, value, and satisfaction on behavioral intentions in the service environment. Serv Mark Q. 2010;31(4):466–484.
22. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
23. Friedman ML, Churchill GA. Using consumer perceptions and a contingency approach to improve health care delivery. J Consum Res. 1987;13(4):492–510. doi:10.1086/209083
24. Hatah E, Ping LK, Ali AM, Shah NM, Islahudin F. The influence of cultural and religious orientations on social support and its potential impact on medication adherence. Patient Prefer Adherence. 2015;2015(9):589–596. doi:10.2147/PPA.S79477
25. Lee YK, Ng CJ. The state of shared decision making in Malaysia. Z Evid Fortbild Qual Gesundhwes. 2017;123–124:66–68. doi:10.1016/j.zefq.2017.05.019
26. Carter F, Jambulingam T, Chitturi R. Determinants of perceived value of direct to consumer advertising for prescription drugs: do they vary by disease condition? J Mark Manag. 2015;3(2):1–10.
27. Tabor PA, Lopez DA. Comply with us: improving medication adherence. J Pharm Pract. 2004;17(3):167–181. doi:10.1177/0897190004264816
28. Wu JR, Moser DK, Chung ML, Lennie TA. Predictors of medication adherence using a multidimensional adherence model in patients with heart failure. J Card Fail. 2008;14(7):603–614. doi:10.1016/j.cardfail.2008.02.011
29. Korda AP, Snoj B. Development, validity and reliability of perceived service quality in retail banking and its relationship with perceived value and customer satisfaction. Manag Glob Transit. 2010;8(2):187–205.
30. Horne R, Hankins M, Jenkins R. The Satisfaction with Information about Medicines Scale (SIMS): a new measurement tool for audit and research. Qual Health Care. 2001;10(3):135–140. doi:10.1136/qhc.0100135
31. Jha S, Panda M, Kumar S, et al. Psychological insulin resistance in patients with type 2 diabetes. J Assoc Physicians India. 2015;63(7):33–39.
32. Simon PRP, Said SM, Fattah AZ, Shah SA. Risk factors of insulin refusal among type 2 diabetes mellitus patients with poor glycaemic control at tanglin health clinic, Kuala Lumpur. Malaysian J Med Health Sci. 2019;15(2):84–92.
33. American Society on Aging and American Society of Consultant Pharmacists Foundation (ASCP). Adult medication: improving medication adherence in older adults. Alexandria: American Society on Aging and American Society of Consultant Pharmacists Foundation (ASCP); 2006. Available from: http://learning.rxassist.org/sites/default/files/Adult_Meducation%20All.pdf.
34. Berger BA, Krueger KP, Felkey BG. The pharmacist’s role in treatment adherence. Part 1: extent of the problem. US Pharm. 2014;11:50–54.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.