Back to Journals » Advances in Medical Education and Practice » Volume 14
Integration of Case-Based Dialogue to Enhance Medical Students’ Understanding of Using Health Communication to Address Social Determinants of Health
Received 19 November 2022
Accepted for publication 7 March 2023
Published 15 March 2023 Volume 2023:14 Pages 237—244
DOI https://doi.org/10.2147/AMEP.S397211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Jalysa King, Jennifer Taylor
Department of Family Medicine, Indiana University School of Medicine, Indianapolis, IN, USA
Correspondence: Jennifer Taylor, Email [email protected]
Background and Objectives: With the ever-growing diversity within our communities, it is imperative that we integrate social determinants of health (SDOH) such as racial disparity, economic instability, lack of transportation, intimate partner violence, and limited social supports, and the importance of health literacy into undergraduate medical education. By incorporating evidence-based curriculum on the disproportionality within healthcare faced by racial and ethnic minorities, we have the opportunity to develop more culturally sensitive providers. The purpose of this study was to assess the impact of a case-based debrief experience on medical students’ knowledge about how social determinants of health can impact health and healthcare within a family medicine clinical setting and their intent to practice in an underserved community.
Methods: We utilized a retrospective paired-sample t-test analysis of program data from 640 third-year medical students who engaged in a family medicine clerkship between July 2020, and April 2022. For inclusion in the study, students must have engaged in a case-based exercise and corresponding small group debrief around the impact of social determinants of health on patient care.
Results: We found a statistically significant improvement in students’ reported knowledge about SDOH, as well as the confidence and intent to work with and care for individuals of diverse cultural and socioeconomic backgrounds.
Conclusion: Medical students must have the knowledge and self-efficacy to understand how social determinants of health can impact health and healthcare within a family medicine clinical setting. As a result of integrating more active learning strategies such as the case-base and debrief experience, students may have a more robust medical education experience.
Keywords: social determinants of health, problem-based learning, vulnerable populations, education, medical, patient care
A Letter to the Editor has been published for this article.
Introduction
Despite advancements in healthcare, public health, and health education, health disparities still disproportionality effect groups that have been historically marginalized, especially African Americans and patients who live in low socioeconomic communities.1 According to the US Centers for Disease Control and Prevention, health disparities are preventable differences that impact historically marginalized individuals’ opportunities to receive optimal healthcare.2 Along with high mortality rates, health disparities result in higher instances of obesity, heart disease and cancer which are all chronic health conditions.3 The American Public Health Association has identified racism as a driving force of social determinants of health (SDOH) and as a barrier to health equity.4 SDOH are nonmedical factors that can influence healthcare and are not based on individual health behaviors or choices, but more so situations that are the result of where they live, work, and grow up.5 Examples of SDOH include access to transportation, food, employment, healthcare access and quality, economic stability, neighborhood safety, and other societal obstacles.
To improve population health, we must recognize the role of implicit bias in clinical decision and the indirect contribute to health-care disparities.6–9 Implicit bias describes associations or attitudes that unconsciously alter our perceptions, behaviors, interactions, and decision-making.9 When considering social factors that can impact patient care, students should also consider levels of health literacy for the patients they care for. Almost half of the adult population in the United States has low health literacy.10 According to the US Institute of Medicine, low health literacy occurs when a patient has a limited capacity to fully obtain and process health information needed to make informed health-care decisions.11 While, low health literacy can affect those across socioeconomic demographics, there are higher correlations among those from marginalized populations.12
In an effort to address health disparities, it is imperative that we include information and experiences in medical student education that exposes students to SDOH, the importance of health literacy, and plausible patient scenarios involving diverse patient populations. Students must understand the role of SDOH in patient care and develop the skills to use health communication strategies to address their patients’ unique health needs. Health communication is defined as the practice of applied communications to advance the health of people and populations.13 Accrediting bodies such as the Liaison Committee on Medical Education’ have incorporated standards addressing medical school diversity and the inclusion of health disparities into medical student education, although the standards do not include identified outcomes to define success.14 By incorporating evidence-based curriculum regarding the disproportionality within healthcare faced by racial and ethnic minorities, there is an opportunity to develop more culturally sensitive medical clinicians.8,15
Research shows that active learning strategies such as case-based experiences and small-group discussions or debriefs are valuable for improving student knowledge and understanding of population health disparities15,16 as well as the value of improving learner confidence to address challenges faced by patients in low-resourced underserved communities.17 Given the high value placed on medical students to understand how SDOH can impact patient care, we sought to assess the impact of a case-based experience and corresponding small group discussion on medical students’ knowledge about how social determinants of health can impact health and healthcare within a family medicine clinical setting and their intent to practice in an underserved community.
Methods
The study is a prospective pre-post cohort study assessing the association between a case-based experience and associated small group discussion designed to teach third-year medical students how to better communicate with patients impacted by SDOH. This study received exempt approval by the Indiana University institutional review board.
Students are first introduced to the concept of social determinants of health within first 2 years of their undergraduate medical education in Foundations of Clinical Practice course (two-year-long courses). During their third-year rotations, students can apply their knowledge about SDOH in real-life scenarios during multiple clinical rotations. At the start of their 160-hr family medicine clerkship experience, all third-year medical students complete online didactic modules involving health disparities and SDOH. At the conclusion of the modules, students are directed to participate in a simulated case experience designed to teach students to understand the role of social determinants of health on patient care. The case-based exercise is of a fictional 28-year-old black woman presenting with a chief concern of cough and shortness of breath. Students are given a history of present illness, laboratory results, medication list, social history, family history, and financial difficulties. The case outlines SDOH faced by the patient such as racial disparity, economic instability, lack of transportation, intimate partner violence, and lack of social supports. Students must identify three priority issues for the patient and develop a social needs action plan (using the American Academy of Family Physicians’ EveryONE Project Toolkit).18 The AAFP EveryONE Project Toolkit includes a social needs screening tool that allows students to screen their patients for five core health-related social needs, which include housing, food access, transportation, utilities, and personal safety, using validated screening questions, as well as the additional needs of employment, education, childcare, and financial strain.19 Students are tasked with identifying local community-based organizational resources (using the clinic’s zip code) as well as their local Area Health Education Center as they create a social needs plan for the patient’s short-term and long-term needs. The utilization of zip codes allows students to observe how some zip codes and parts of the state have more resources than others. Research shows that health disparities can often be more severe in communities (zip codes) with few resources.20,21
During the last week of their clerkships, students present their social needs plan along with a suggested follow-up care plan for the fictional patient to their preceptor for feedback. During the same week, students met for a 45 min facilitated virtual small group discussion with no more than six students per group. A facilitator trained in applied health and interpersonal communication led students through a series of questions designed to encourage learners to think critically about their experience, their role as future physicians, the importance of culturally competent care, health literacy, and the role race and ethnicity has on patient–clinician relationships and overall patient adherence. Throughout the small group discussion, students are encouraged to think critically about how SDOH can influence patients’ care and care decisions. Students are encouraged to share how they plan to use health communication strategies to identify a patient’s social determinants of health and work with the patient to identify feasible care options.
During the session, the facilitator uses two main communication theories, Muted Group Theory and Intersectionality Theory, to help lead the conversation, and tie scenarios together. Muted group theory is a communication theory that focuses on how marginalized groups are muted and excluded via the use of language and communication.22 Intersectionality Theory is an analytical framework for understanding how aspects of both a person’s social and political identity combine to create different modes of discrimination and privilege.23 Students are reminded that personal identities that can intersect include but are not limited to age, race, sexual orientation, physical ability, and education level. Within healthcare, it is important for students to understand how each part of a patients’ identity comes with its own set of obstacles and could potentially impact the care they receive, independently and collectively.
Following case-based experience and small group discussion, students complete an online survey evaluation. The survey includes retrospective pretest-posttest evaluation questions asking students to report their knowledge about social determinants of health, confidence to address social determinants of health in patient care, and plans for future practice in underserved communities. In the evaluation, students are asked to rank the following statements on a Likert scale where 1 is strongly disagree and 5 was strongly agree.
- I can recognize how social determinants (housing, income, work, food access) can affect patient care.
- I understand how a person’s culture and/or background (race, ethnicity, sexual orientation, religion, rural areas, etc.) may impact their overall health and health-care options.
- I feel prepared to work with individuals (both patients and professionals) from different cultures and/or backgrounds.
- I feel I have the skills to care for the unique needs of individuals in rural and medically underserved settings.
In addition to the evaluation questions, students were asked to self-report their demographic information such as identified race and ethnicity, whether they are from an underprivileged background (self-identified as the first generation in their family to attend college, received social assistance benefits, received free or reduced lunch as a child, etc.) and geographic background (urban or rural environment). Self-identified racial and ethnic backgrounds were recoded into a category identified as underrepresented in medicine. Underrepresented in medicine is defined as individuals from racial and ethnic backgrounds that are underrepresented in the medical profession relative to their numbers in the general population.24
The inclusion criteria for this study were that the participants must have been enrolled as a medical student with the Indiana University School of Medicine, participated in a 160-hr family medicine clerkship experience between July 2020, and April of 2022, and completed the program evaluation questions about their experience. The primary outcome of this study is to assess the impact of the case-based debrief experience on medical students’ knowledge about how social determinants of health can impact health and healthcare within a family medicine clinical setting and their intent to practice in an underserved community We conducted a paired t-test with the study data using SPSS version 28 A two-sided P value of less than 0.05 was statistical significance.
Results
Between July 2020 and April 2022, 640 third-year family medicine clerkship students completed the simulated case experiences and submitted the program evaluation. Most program participants self-reported their race as white or Caucasian (70.9%, 454), Asian (16.4%; 105), and Black or African American (5.0%, 32) with the remaining identifying as American Indian or Alaska Native (0.3%, 2), and other/more than one race (7.3%, 47). Approximately 11.1% (n=71) of the participants self-reported as Hispanic or Latino. Students reported growing up in an even mix of rural (39.5%, 253) versus urban (60.5%, 387) and approximately 31.4% (201) reported having an economically or educationally underprivileged background (Table 1).
 |
Table 1 Medical Students by Self-Reported Demographics |
The results of the program assessment are highlighted in Figure 1, depicting the pretest-posttest means for each evaluation question. The data analysis demonstrated a statistically significant positive change between the pre-test and post-test for students’ self-reported understanding how social determinants (housing, income, work, food access) can affect patient care [X² (4, N = 497) = −11.632, p<0.01] and how a person’s culture and/or background (race, ethnicity, sexual orientation, religion, rural areas, etc.) may impact their overall health and health-care options [X² (4, N = 497) = −11.632, p<0.01]. Furthermore, the data analysis demonstrated a statistically significant positive change between the pre-test and post-test for students’ self-reported confidence to work with other health professions (both in a clinic and community) in a rural or underserved setting [X² (4, N = 497) = −11.632, p<0.01]; work with individuals (both patients and professionals) from different cultures and/or backgrounds [X² (4, N = 497) = −11.632, p<0.01]; and care for the unique needs of individuals in urban and rural underserved settings [X² (4, N = 497) = −11.632, p<0.01].
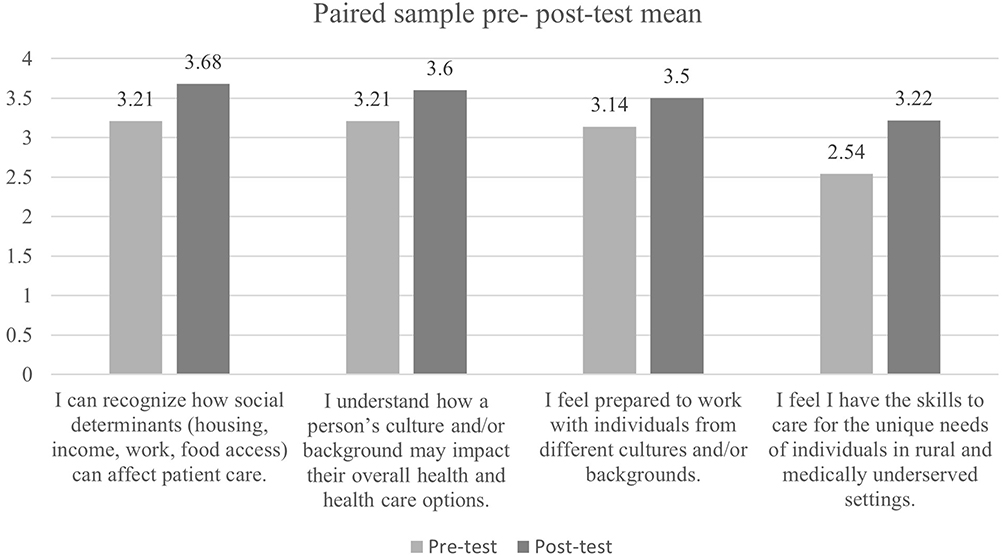 |
Figure 1 Paired sample mean (where 0 is strongly disagree and 4 is strongly agree) and standard deviation between the pretest and posttest. |
Discussion
If medical schools continue to integrate health disparity education into the curriculum, there is potential to improve the ability to further diversify medicine as a practice.6 As our population continues to diversify, it is crucial to increase access and exposure to curriculums that focus on healthcare disparities, diverse populations, and the impact on patient care. The focus of this study was to better understand the impact of a clinical case-based exercise and related small group discussion on student’s knowledge about how social determinants of health can impact health and healthcare within a family medicine clinical setting and their intent to practice in an underserved community. Our findings demonstrate a positive correlation between medical students engaging in the simulated case study and corresponding facilitated small group discussion and an improvement in knowledge and self-efficacy around the impact of social determinants on patient care.
Research shows that when students are given evidence about the ways in which race and lack of care for diverse patients can affect treatment and diagnosis, it can help increase their self-awareness as a physician.6 When this project was first created, the fictional patient was not assigned a race or ethnicity. During that time, Indiana had two high profile incidents where two Black female physicians passed away during medical visits/treatments. The decision was made to incorporate race to the scenario to better address the ways in which a patient’s race can impact the care they receive, particularly Black women.25–27 The goal is not to perpetuate existing stereotypes but to bring awareness to barriers or obstacles in care a Black patient could potentially face. Our hope is that by openly discussing the impact race can have on patients care, along with examples students have seen during their clinical rotations, we are not enhancing stereotypes but being observant of the ways implicit bias and microaggressions currently exist.
The small group discussion allows the students to share and reflect on their own experiences, but it also allows them the opportunity to connect with their peers and create community. The Indiana University School of Medicine is the largest allopathic medical school in the US with nine total campuses, thus students are spread across the state in both their didactic and clinical education experiences. Furthermore, the family medicine clerkship practice sites are often decentralized from the students’ academic campus. Conducting the discussions virtually gives students the opportunity to hear their peers’ experiences in other parts of the state.
A major component of the debrief experience is asking learners to identify any patients they have seen in a clinic that had a similar lived experience to the simulated patient case or any other social needs that needed to be addressed. During this discussion, students are asked to share how the experience made them feel, how they communicated with patients, and how to increase their patients’ interactions with clinicians, health literacy, and patient adherence. In sharing with each other, we believe that students are gaining the knowledge and skills necessary to be more culturally sensitive clinicians.
Our study faced several limitations. Case-based experience with a corresponding small group discussion is a new initiative designed to address SDOH within the curriculum during clinical training years. As a result, our findings are based on the initial 2 years of the project. Another limitation is due to the 4-week duration of the clerkship rotation, the current evaluation methodology does not include an observable assessment of behavioral changes or to determine if students are using health communication skills to address SDOH in a clinical setting. A third limitation is the self-reported/response shift bias nature of the program evaluation. We recognize that students may over-exaggerate their knowledge or self-efficacy. To limit the potential for response bias, we utilized a retrospective pre-post-test design known to limit pre-test over exaggeration and resulting bias.28 Additionally, given the large nature of the medical school, by default students are often placed in decentralized clinical practice sites throughout the state to complete their four-week rotation. With that, we recognize that students encountered different patient populations depending on where they were placed. Students who were placed in more affluent areas to complete this rotation did not have the same in-person encounters compared to their peers. However, the small group discussion provided students with the opportunity to share and learn about their experiences around SDOH and other observations they had in the clinical setting.
Health communication is a necessary skill for medical students. Research has shown that most medical schools incorporate health communications training during pre-clinical years when the clinical environment is an ideal setting for students to learn of and practice communication strategies.29,30 While case-based experience and discussion did not provide us with the opportunity to observe students utilizing their health communication skills, future initiatives should provide additional opportunities for students to further develop communication strategies in clinical situations with vulnerable patients faced with multiple SDOHs.
Conclusion
If we are to actively disrupt the trend of health disparities in our communities, we must ensure our students are comfortable and have the skills to care for vulnerable, diverse populations. To do so, medical students must have the knowledge and self-efficacy to understand how social determinants of health can impact health and healthcare within a family medicine clinical setting. As a result of integrating more active learning strategies such as the case-base and debrief experience, students may have a more robust medical education experience. Moving forward, we plan to incorporate more thought provoking and reflective questions for students to discuss in their small group discussions and exploring ways to determine if students implement any strategies learned during the base-based exercise. Our expectation is that by sharing these experiences, students learn about resources and other ways to provide care for their future patients.
Ethical Approval
This study was reviewed and received exempt approval (#16601) by the Indiana University Institutional Review Board due to the minimal risk to students participating in the program.
Informed Consent
Study participants voluntarily completed the form. A consent paragraph is provided at the start of the survey.
Funding
This project is supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) under the grant number U77HP23068 Area Health Education Centers Point of Service Maintenance and Enhancement for a total of $1,298,250. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the US Government.
Disclosure
The authors have no conflicts of interests to declare.
References
1. Thornton R, Glover C, Cene C, et al. Evaluating strategies for reducing health disparities by addressing the social determinants of health. Health Aff. 2016;35(8):1416–1423. doi:10.1377/hlthaff.2015.1357
2. Health Disparities. Centers for disease control and prevention; 2020. Available from: https://www.cdc.gov/healthyyouth/disparities/index.htm.
3. Ogden C, Carroll M. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA. 2014;311(8):806–814. doi:10.1001/jama.2014.732
4. Racism and Health. American public health association; 2022. Available from: https://www.apha.org/topics-and-issues/health-equity/racism-and-health.
5. Preda A, Voigt K. The social determinants of health: why should we care? Am J Bioeth. 2015;15(3):25–36. PMID: 25786009. doi:10.1080/15265161.2014.998374
6. Dehon E, Weiss N, Jones J, Faulconer W, Hinton E, Sterling S. A systematic review of the impact of physician implicit racial bias on clinical decision making. Acad Emerg Med. 2017;24(8):895–904. doi:10.1111/acem.13214
7. Chapman EN, Kaatz A, Carnes M. Physicians and implicit bias: how doctors may unwittingly perpetuate health care disparities. J Gen Intern Med. 2013;28(11):1504–1510. doi:10.1007/s11606-013-2441-1
8. Corsino L, Railey K, Brooks K, et al. The impact of racial bias in patient care and medical education: let’s focus on the educator. MedEdPORTAL. 2021;17:11183. doi:10.15766/mep_2374-8265.11183
9. Marcelin JR, Siraj DS, Victor R, Kotadia S, Maldonado YA. The impact of unconscious bias in healthcare: how to recognize and mitigate it. J Infect Dis. 2019;220(Suppl 2):S62–S73. doi:10.1093/infdis/jiz214
10. Schillinger D. The intersections between social determinants of health, health literacy, and health disparities. Stud Health Technol Inform. 2020;269:22–41. PMID: 32593981; PMCID: PMC7710382. doi:10.3233/SHTI200020
11. Paasche-Orlow M, Parker R, Gazmararian J, Nielsen-Bohlman L, Rudd RR. The prevalence of limited health literacy. J Gen Intern Med. 2005;20(2):175–184. doi:10.1111/j.1525-1497.2005.40245.x
12. Logan RA, Siegel ER. Health Literacy: A Prescription to End Confusion, Washington, DC: Institute of Medicine of the National Academies. Board on Neuroscience and Behavioral Health, Committee on Health Literacy; 2020; doi:10.1056/nejm200503033520926
13. About Health Communication. Society for health communication; 2016. Available from: https://www.societyforhealthcommunication.org/health-communication.
14. Barzansky B, Hash RB, Catanese V, Waechter D. What is the role of accreditation in achieving medical school diversity? AMA J Ethics. 2021;23(12):E946–E952. doi:10.1001/amajethics.2021.946
15. Kiles T, Jasmin H, Nichols B, Haddad R, Renfro CP. A scoping review of active-learning strategies for teaching social determinants of health in pharmacy. Am J Pharm Educ. 2020;84(11):8241. doi:10.5688/ajpe8241
16. Poirier TI. Is lecturing obsolete? Advocating for high value transformative lecturing. Am J Pharm Educ. 2017;81(5):83. doi:10.5688/ajpe81583
17. Longenecker RL, Wendling A, Hollander-Rodriguez J, Bowling J, Schmitz D. Competence revisited in a rural context. Fam Med. 2018;50(1):28–36. doi:10.22454/FamMed.2018.712527
18. The EveryONE Project. American academy of family physicians; 2023. Available from: https://www.aafp.org/family-physician/patient-care/the-everyone-project.html.
19. American Academy of Family Physicians. Address your patients’ social determinants of health; 2022. Available from: https://www.aafp.org/family-physician/patient-care/the-everyone-project/toolkit/assessment.html.
20. Khairat S, Haithcoat T, Liu S, et al. Advancing health equity and access using telemedicine: a geospatial assessment. J Am Med Inform Assoc. 2019;26(8–9):796–805. doi:10.1093/jamia/ocz108
21. Wilkins CH, Friedman EC, Churchwell AL, et al. A systems approach to addressing covid-19 health inequities. NEJM. 2021;2:1. doi:10.1056/CAT.20.0374
22. Barkman L. Muted group theory: a tool for hearing marginalized voices; 2018. Available from: https://www.cbeinternational.org/resource/muted-group-theory-tool-hearing-marginalized-voices/.
23. Ruiz AM, Luebke J, Klein K, et al. An integrative literature review and critical reflection of intersectionality theory. Nurs Inq. 2021;28(4):e12414. doi:10.1111/nin.12414
24. Association of American Medical Colleges. Underrepresented in medicine definition; 2004. Available from: https://www.aamc.org/what-we-do/equity-diversity-inclusion/underrepresented-in-medicine.
25. Crear-Perry J, Correa-de-Araujo R, Lewis Johnson T, McLemore MR, Neilson E, Wallace M. Social and structural determinants of health inequities in maternal health. J Womens Health. 2021;30(2):230–235. doi:10.1089/jwh.2020.8882
26. Saluja B, Bryant Z. How implicit bias contributes to racial disparities in maternal morbidity and mortality in the United States. J Womens Health. 2021;30(2):270–273. doi:10.1089/jwh.2020.8874
27. Smith NC. Black-White disparities in women’s physical health: the role of socioeconomic status and racism-related stressors. Soc Sci Res. 2021;99:102593. doi:10.1016/j.ssresearch.2021.102593
28. Little TD, Rong Chang BK, Gorrall LW, Eriko Fukuda PJ. The retrospective pretest–posttest design redux: on its validity as an alternative to traditional pretest–posttest measurement. Int J Behav Develop. 2019;44(2):175–183. doi:10.1177/0165025419877973
29. Junod Perron N, Sommer J, Louis-Simonet M, Nendaz M. Teaching communication skills: beyond wishful thinking. Swiss Med Wkly. 2015;145:w14064. doi:10.4414/smw.2015.14064
30. Grant C, Jopling H. Health coaching: a necessary role for medical students? Public Health. 2021;190:52–54. doi:10.1016/j.puhe.2020.11.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Commentary on Ultrasound Instruction in Undergraduate Medical Education: Perspective from Two Students
Allen AJ, White AB, Bacon DR, Beck Dallaghan GL, Jordan SG
Advances in Medical Education and Practice 2023, 14:1-7
Published Date: 4 January 2023
Patient’s Perceptions and Attitudes Towards Medical Student’s Involvement in Their Healthcare at a Teaching Hospital in Jordan: A Cross Sectional Study
Taha HA, Al Saqer JK, Al Harbi NR, Younis RN, Al Dawoud F, Nawaiseh MB, Berggren V
Patient Preference and Adherence 2023, 17:629-641
Published Date: 13 March 2023
Assessing the Proficiency in Basic and Advanced Life Support Among Physicians in Ecuador: A Cross-Sectional Study
Izquierdo-Condoy JS, Naranjo-Lara P, Arias Rodríguez FD, Puglla-Mendoza AG, Jima-Sanmartín J, Andrade Casanova D, Duque-Sánchez EP, Alegría N N, Rojas Cadena MG, Ortiz-Prado E
Advances in Medical Education and Practice 2024, 15:25-35
Published Date: 6 January 2024
Enhancing Surgical Nursing Student Performance: Comparative Study of Simulation-Based Learning and Problem-Based Learning
Ma L, Yan R, Wang X, Gao X, Fan N, Liu L, Kang H
Journal of Multidisciplinary Healthcare 2024, 17:991-1005
Published Date: 7 March 2024
The Tensegrity Curriculum: A Comprehensive Curricular Structure Supporting Cultural Humility in Undergraduate Medical Education

Jones AC, Bertsch KN, Williams D, Channell MK
Advances in Medical Education and Practice 2024, 15:381-392
Published Date: 3 May 2024