Back to Journals » Advances in Medical Education and Practice » Volume 14
Commentary on Ultrasound Instruction in Undergraduate Medical Education: Perspective from Two Students
Authors Allen AJ ![]() , White AB
, White AB ![]() , Bacon DR, Beck Dallaghan GL
, Bacon DR, Beck Dallaghan GL ![]() , Jordan SG
, Jordan SG ![]()
Received 30 August 2022
Accepted for publication 7 December 2022
Published 4 January 2023 Volume 2023:14 Pages 1—7
DOI https://doi.org/10.2147/AMEP.S388044
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Austin J Allen,1,* Alexander B White,1,* Daniel R Bacon,2 Gary L Beck Dallaghan,3 Sheryl G Jordan4
1University of North Carolina School of Medicine, Chapel Hill, NC, USA; 2Department of Surgery, The Ohio State University College of Medicine, Columbus, OH, USA; 3Department of Medical Education, University of Texas at Tyler School of Medicine, Tyler, TX, USA; 4Department of Radiology, University of North Carolina School of Medicine, Chapel Hill, NC, USA
*These authors contributed equally to this work
Correspondence: Sheryl G Jordan, University of North Carolina School of Medicine, 321 South Columbia Street, Chapel Hill, NC, 27514, USA, Tel +1 964 974 8123, Fax +1 919-966-9930, Email [email protected]
Background: Ultrasound integration in undergraduate medical education (UME) has been a focused endeavor in recent years. According to the American Institute of Ultrasound in Medicine, more than a third of all US medical schools have adopted a focused ultrasound training program for medical students. Medical student perspectives on best practices in ultrasound education are lacking in the literature.
Curricula Experiences: Two students’ reflections are presented regarding two different didactic approaches, flipped classroom and self-study learning models, to teaching ultrasound in the pre-clinical medical education curriculum. Students present reflections on these didactic approaches to facilitate further improvement in ultrasound education curricula.
Discussion: The self-directed learning model enabled students to learn foundational ultrasound exam techniques efficiently in a low-stress environment and subsequently optimized the efficiency of later faculty-led learning events. However, we noted that in both the flipped classroom and self-study learning models of education, the training on basic physical properties of ultrasound, tissue characteristics, and probe manipulation was limited.
Conclusion: A self-study learning model ultrasound curricula improves perceived learning efficiency and student confidence, especially when followed by faculty-guided didactics and scanning opportunities. We suggest a framework for ultrasound education curricula that includes components of both formats of ultrasound education alongside faculty-led sessions as an ideal model of ultrasound education. Further, we propose the added benefit of inanimate object scanning to optimize students’ knowledge of waveform physics (image acquisition and physical properties of materials) early in the ultrasound education process.
Keywords: ultrasound, ultrasonography, ultrasonography education, education, medical, undergraduate
Background
The incorporation of formal ultrasound (US) training in undergraduate medical education (UME) has gained popularity as accessibility and affordability of portable US probes has improved.1,2 According to the American Institute of Ultrasound in Medicine (AIUM), focused US training is defined as active learning where students are performing US rather than watching PowerPoints or interpreting images only on a rotation.3 The AIUM database reports that more than a third of all 214 medical schools in the United States have adopted a focused US training program, but only 35 of those medical schools have a focused US program for medical students throughout all four years of undergraduate medical education (UME).3 Integration of US into medical school curricula has historically been achieved through traditional didactics followed by large-group faculty-led scanning sessions. These traditional methods often require class-wide attendance with significant organizational efforts to coordinate post-lecture scanning opportunities.
The AIUM database as well as academic literature demonstrate that there is wide variability in how each institution structures its US training curriculum. Many curricular designs focus on incorporating US didactics and modules with gross anatomy, physical exam, and organ system blocks during preclinical years as part of a longitudinal curricula for all students.1,4–6 Other curricula options include selective ultrasound curricula for a small group of students interested in enriching their mandatory UME experience throughout all four years.7,8
Current published models for UME US curricula are predominantly built from established frameworks within emergency medicine residency programs.9–11 One inherent pitfall is that marked differences in clinical knowledge exist between learners/trainees within UME and GME; necessitating a role for the medical student perspective on identifying their educational needs. These differences can create blind spots when translating didactic approaches between the two groups, such as recognition that UME learners require more time gaining familiarity with normal anatomy and physiology. GME in US is often incorporated into bedside training with a diagnostic focus, which is often not the optimal method to introduce undergraduate learners to US principles. Chiem et al, along with the authors of the UMeCali Experience, report “the role of medical student involvement” as one of the five common themes integral to successful US education in UME.12 This involvement comes in the form of interest group leadership, peer scanning sessions, and collaboration with faculty on optimal training design. The medical student perspective on best practices in US education has yet to play a prominent role in the collegial discussion of curricular design within academic literature. The authors’ perspective is presented here to provide first-hand student commentary on US education models with a goal of optimizing student learning and efficiency of technical skill acquisition.
Curricula Experiences
Author Background
The primary authors of this paper (AA and AW) are current fourth-year medical students who were involved in the early stages of multiple US education initiatives throughout medical school. These educational experiences included US education sessions required of all students at the UNC School of Medicine (SOM), as well as involvement in the first cohort of a US scholarly concentration program (SCP), previously described by Bacon et al.8 Additionally, informal US educational training has been completed throughout third-year clerkships via resident- and attending-physician supervised point of care ultrasound (POCUS) scanning. The SCP has also allowed for monthly case presentations and longitudinal projects during clinical clerkships. The longitudinal projects did not begin until the self-study learning model curricula was complete. The structure of the preclinical curricular experiences is described in greater detail below, followed by the student-led discussion on the advantages and disadvantages of each teaching model. Ideas for future innovation, assessment strategies, and perspectives on the best practices in US education are also presented.
Flipped Classroom Model
The UNC School of Medicine curriculum, required of all students, features three semesters of preclinical studies. At the time of the primary authors’ (AA and AW) progression through the curriculum, US training sessions occurred approximately once every four to six weeks. There was a temporary pause in these sessions late in the second semester and early in the third semester due to the COVID-19 pandemic; thus, the authors experienced less than ten of these sessions each.
The initial teaching session, a large-group didactic, featured a brief review on US physics and image acquisition followed by details about the basic cardiac views (PSLA, PSSA, apical 4-chamber, and subxiphoid). Each subsequent teaching session focused on reviewing or learning a different US imaging technique, to include the Focused Assessment in the Setting of Trauma (FAST) scan, assessing the abdominal aorta and IVC, as well as other basic POCUS techniques. The teaching methodology for these sessions involved three components: review of background material at home on anatomy and the standard orientation for that type of US scan (flipped classroom component), a 10-to-15-minute faculty-led didactic lecture at the beginning of the session recapping the home study material, and approximately one hour in a small group with 3 to 5 other students practicing US scanning of a standardized patient under supervision from a physician or registered diagnostic medical sonographer (RDMS). Real-time feedback was provided on scanning technique by the instructor and students were surveyed to assess their confidence in learning; however, no formal assessment of US knowledge or scanning technique was completed at the time we progressed through this curriculum.
Self-Study Learning Model
As part of the US SCP, the primary authors (AA and AW) were two of twelve students to participate in the first iteration of a self-study learning model of US education during the summer between their first and second year of medical school. This enrichment curriculum was developed by physician authors of this paper (DB and SJ). Though the planned curriculum for the 2020 summer US experience was very similar to an accelerated version of that described in the flipped classroom education model above, restrictions due to the COVID-19 pandemic necessitated significant revision. Learners had completed approximately five flipped classroom sessions prior to the start of this curriculum. There was no simultaneous overlap of the two curricula; however, following the completion of the self-study model, learners did complete three additional flipped classroom sessions.
In the modified educational experience, students were each provided a personal portable US probe (Butterfly Probe; Butterfly Network, Inc. Guilford, CT) for use with their school-issued digital tablet and access to a virtual curriculum produced by EM Sono, LLC (Canton, OH). The virtual curriculum began with a detailed review of US physics including the impact on images, then progressed to detailed lessons on scanning techniques. Each lesson on a scanning technique featured video presentations on image acquisition and interpretation, followed by quiz questions accompanied by actual POCUS US images. Each module with quizzes required approximately 90 minutes to complete. Immediately practicing the technique covered in the modules was particularly helpful, though the time needed to gain a basic level of confidence varied based on difficulty of the specific view, and decreased as we gained more experience.
Anatomy and pathology interpretation skills were targeted throughout the program. Students were expected to practice obtaining correct images scanning themselves or a peer and submit best attempt samples of each image for review and grading. In our experience, revisiting and practicing the scan several times after the initial learning session was very helpful and easy to accommodate with access to the take-home probe. Following completion of the self-study portion of the curriculum, COVID restrictions were temporarily relaxed and several voluntary small group sessions were offered; students practiced real-time scanning with a ratio of 2 to 3 students per supervising physician.
Clinical Clerkships
In addition to the two formal preclinical education experiences described above, the primary authors (AA and AW) had additional informal POCUS learning opportunities during third-year clinical clerkships. Students were able to sign out portable ultrasound devices from the SOM for use with school-issued tablets when interesting scan opportunities arose in appropriate clinical settings. Students were also able to utilize POCUS devices already at clinical sites when available. Clerkships with the most frequent ultrasound utilization included surgery (FAST scan), OBGYN (assessing fetal position as well as multiple intra-operative obstetric and gynecologic indications), internal medicine (central venous access and arterial pressure monitoring line guidance), and emergency medicine (cardiac views, FAST scan, line placement guidance). There was also the opportunity to review formal ultrasound imaging studies on most clinical rotations. Monthly SCP student clinical case presentations enabled learners to reinforce scan interpretation and POCUS applications knowledge throughout their clinical clerkships. Lastly, the learners’ SCP fourth year culminated with a longitudinal ultrasound scholarly project.
Discussion
We present our experiences from the curricula described above, as well as our suggestions based on these experiences for improving future educational models. We have had significant discussion amongst the authors regarding advantages, disadvantages, and overall utility of each learning experience and have captured what we attribute to each learning experience in this discussion.
Flipped Classroom Model
Direct instruction from faculty and experienced sonographers was the highlight of the flipped classroom US education model. As content experts were well-versed in the subject material, faculty were frequently able to share pearls of wisdom and insight in obtaining ideal images. Faculty were also able to quiz students on what image findings showed in real-time, which helped students master the anatomy in a particular view and to consider clinical correlations to each scanning view. This insight was particularly valuable when students already had baseline scanning skills. Faculty lectures were helpful primers prior to the scanning as they synthesized background information from preparatory modules into the most relevant insights for obtaining images.
One notable limitation to this model was diminished “probe-in-hand” student scanning time. There was a limited amount of time for each student to practice acquiring images. It is the authors’ first-hand perspective that navigating the handheld US probe and directly observing changes in the optical window was the most valuable tool in learning POCUS. It has also been well documented that learners demonstrate improved higher-order information retrieval when they take charge of the educational process in a flipped classroom setting.13–15 Passive modes of information delivery, such as traditional didactics, allow for less active involvement in the information retrieval process. Other disadvantages to this model of education included a limited review of US physics and terminology prior to the first scanning session, limited assessment of pathology, no formal assessment of student scanning, and difficulty tailoring teaching to meet each student’s level.
Self-Study Learning Model
Advantages to the self-study US learning model included a detailed review on US physics and terminology, active assessment of any pathological image features on quizzes, grading and feedback on the technical quality of acquired images, and the ability to progress through modules and scanning practice at an ideal pace and schedule for each learner’s specific needs. Being able to rewind, slow, and pause modules helped ensure learning goals were met. The self-study learning model has gained notable popularity in recent educational practice.16–18 Access to a personal, portable POCUS device for practice at home during the self-study learning model allowed students more hands-on time practicing image acquisition than did faculty-led sessions, with the added benefit of initial practice occurring in a low-stress environment. In our experience, this helped to established confidence with basic image acquisition skills and ensured time in faculty-led scanning sessions was optimized.
Drawbacks to the self-study learning model are inherent to decreased faculty interface. During online modules and scanning practice at home, students are unable to ask faculty questions or receive feedback on scanning techniques, and faculty insights into clinical correlations are lacking. Student access to US probes is also costly if devices are purchased for every student. Furthermore, although a comprehensive virtual didactic module was presented on US physics and terminology, there was no way to apply and practice these foundational principles prior to peer scanning on human tissue.
Clinical Clerkships
Each clerkship during third year had inherently different opportunities and settings to utilize POCUS; however, several trends emerged across all clinical rotations. Most importantly, the completion of ultrasound preclinical curricula prepared students to acquire valuable POCUS images in clinical settings and in turn positively impact patient care. The opportunities to scan and directly acquire images were more helpful than passively observing others acquire images. Access to a personal portable POCUS device was valuable for creating additional scanning opportunities in settings which lacked dedicated ultrasound devices (eg, outpatient primary care offices and some inpatient medicine and surgery wards). Paradoxically, personal portable devices were not as helpful at sites that frequently utilize POCUS (OBGYN clinic, OB floor, and emergency trauma bay) as these high-use settings frequently had a designated portable ultrasound unit of superior quality.
Curricula Suggestions
Based on our experiences with two different models of structured US curriculums, as well as our experiences with informal POCUS training during clinical rotations (Figure 1), we propose the following tenets of UME US training curricula (Table 1).
 |
Table 1 Five Proposed Tenets of Undergraduate Medical Education Ultrasound Curriculum |
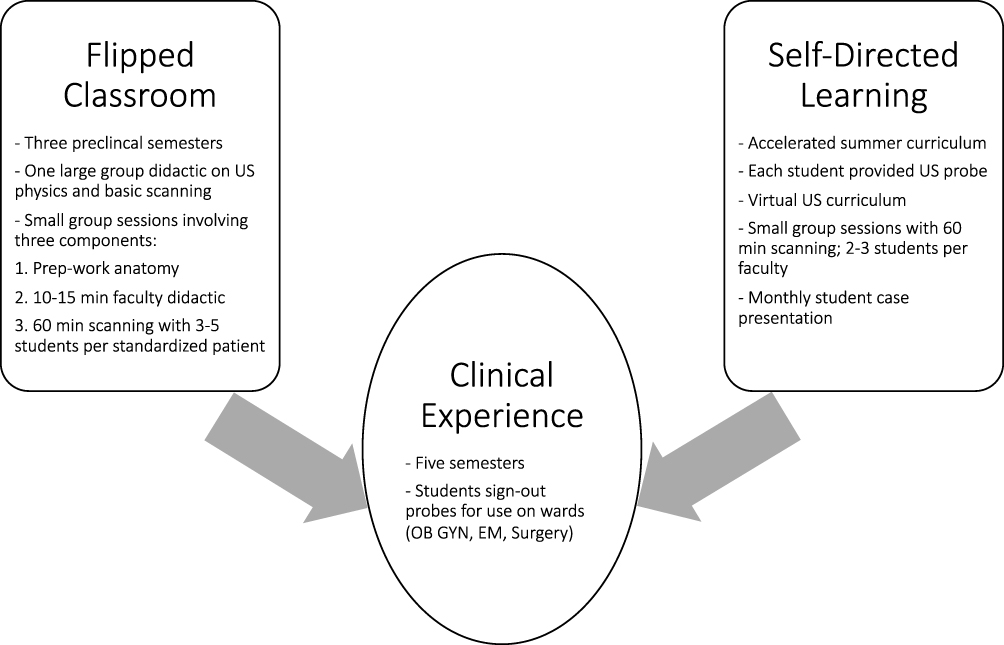 |
Figure 1 Schematic representation of ultrasound educational curricula experienced by the authors. Flipped classroom and self-study learning activities were incorporated into the training prior to having clinical experience applying US skills. |
Begin the Curriculum with a Review of Ultrasound Physics, Then Incorporate Inanimate Object Scanning in the First Training Session
One of the challenges we experienced early in the training program was visualizing how a physical object translated into an acquired US image. Though this skill set eventually became second nature, the learning process would have been expedited if this was recognized as an official learning objective. We feel that scanning inanimate objects (such as jello, chicken breasts, tofu, or other US model simulators) during the first training session would be more valuable than trying to dive directly into obtaining US images on living human models. This may be less of a concern when dealing with resident physician US education; however, we believe it should be a strong priority for preclinical medical students given they are less familiar with anatomy and medical imaging interpretation.
Incorporate Self-Study Learning Modules with Active Learning of Normal and Pathological Image Findings
Both curricula utilized some degree of self-study modules. We feel this is a critical component of US education in undergraduate medical education. The assessment of normal anatomy and pathological images in the modules is an important form of active learning.
Allow Access to Ultrasound Probes for Students to Practice Without Faculty Supervision
Access to portable US probes to practice obtaining images in a relaxed format with peers proved invaluable for learning probe repositioning and establishing confidence in basic image acquisition skills. Though hands-on assistance from faculty is appreciated and necessary in the confines of a short faculty-led session, the skill of image acquisition can ultimately only be obtained without hands-on assistance from others and may require more time than faculty appreciate during the early learning stages. We encourage faculty to supervise and direct students without directly assisting in probe manipulation as much as possible.
Integrate Both Voluntary and Mandatory Faculty-Led Sessions After Students Have Had Time to Practice Acquiring Images
Faculty-led scanning sessions and expertise are tremendously valuable for students because of the expertise that faculty have with the subject. We suggest these sessions be scheduled only after students have had time to practice scans independently thereby optimizing faculty time to fine-tune existing student skills.
Develop a Standardized and Comprehensive Method to Assess Student Competence in Obtaining Ultrasound Images
Though scans submitted as part of the self-study model were graded, and we completed modules assessing competence in identifying pathological image findings on sample ultrasound scans, we did not receive a comprehensive formal assessment of image acquisition skills in either curriculum. Indeed, such formal assessment of learner skills is an area that is lacking in the literature. The clinical utility of UME US curricula has proven difficult to uniformly assess with standard US guidelines or objective criteria, and often relies on post-instruction anatomy identification and survey data. Simulation-enhanced US curriculum has demonstrated 83% of students can adequately obtain parasternal long axis (PSLA) and hepatorenal images in an OSCE post-assessment.9 Efforts have been made to create validation tools for US competency. The Rapid Assessment of Competency in Echocardiography Scale (RACE) was one such attempt and demonstrated good inter-rater reliability with a significant ability to detect change in learner performance within the first 35 training sessions (P = 0.16).10,19
Developing a standardized assessment of UME learner US image acquisition and interpretation should be a high priority for the US community to facilitate feedback and allow students to demonstrate competency. We advocate for a comprehensive competency exam of a learner’s ability to acquire and interpret images in realtime. Specifically, this examination should include competency objectives in obtaining pre-specified images (ex: FAST, cardiac views, etc), optimization of image quality (modifying patient positioning and probe settings, gain, depth, scan mode, etc.), and real-time anatomy interpretation.
Conclusion
We recommend self-study learning modules combined with individual probes and peer scanning prior to faculty-led scanning as an ideal model for UME US education curricula. Our proposed framework also addresses gaps in training and features suggestions to increase student confidence with US image acquisition. Inanimate object scanning may be an underutilized aspect of US education.
Acknowledgments
The authors would like to acknowledge UNC School of Medicine for developing an US curriculum and proactively working to ensure continued improvement in this training program. We would also like to recognize the numerous clinicians and other educators who have served as mentors for medical students and made our educational experiences possible.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Feilchenfeld Z, Dornan T, Whitehead C, Kuper A. Ultrasound in undergraduate medical education: a systematic and critical review. Med Educ. 2017;51(4):366–378. doi:10.1111/medu.13211
2. Nelson BP, Sanghvi A. Out of hospital point of care ultrasound: current use models and future directions. Eur J Trauma Emerg Surg. 2016;42(2):139–150. doi:10.1007/s00068-015-0494-z
3. American Institute of Ultrasound in Medicine. AIUM ultrasound in medical education portal. American Institute of Ultrasound in Medicine website. Available from: http://meded.aium.org/medical-schools.
4. Bahner DP, Adkins EJ, Hughes D, Barrie M, Boulger CT, Royall NA. Integrated medical school ultrasound: development of an ultrasound vertical curriculum. Crit Ultrasound J. 2013;5(1):6. doi:10.1186/2036-7902-5-6
5. Miller GT, Scerbo MW, Zybak S, et al. Learner improvement from a simulation-enhanced ultrasonography curriculum for first-year medical students. J Ultrasound Med. 2017;36:609–619. doi:10.7863/ultra.15.12025
6. Rempell JS, Saldana F, DiSalvo D, et al. Pilot point-of-care ultrasound curriculum at Harvard medical school: early experience. West J Emerg Med. 2016;17(6):734–740. doi:10.5811/westjem.2016.8.31387
7. Wilson SP, Mefford JM, Lahham S, et al. Implementation of a 4-year point-of-care ultrasound curriculum in a liaison committee on medical education-accredited US medical school. J Ultrasound Med. 2017;36(2):321–325. doi:10.7863/ultra.16.03068
8. Bacon DR, Cowles K, Thapa D, et al. Creating an ultrasound scholarly concentration program for medical students. Adv Med Educ Pract. 2021;12:1103–1110. doi:10.2147/AMEP.S330771
9. Lewiss RE, Pearl M, Nomura JT, et al. CORD-AEUS: consensus document for the emergency ultrasound milestone project. Acad Emerg Med. 2013;20(7):740–745. doi:10.1111/acem.12164
10. Stolz LA, Stolz U, Fields JM, et al. Emergency medicine resident assessment of the emergency ultrasound milestones and current training recommendations. Acad Emerg Med. 2017;24(3):353–361. doi:10.1111/acem.13113
11. Amini R, Adhikari S, Fiorello A. Ultrasound competency assessment in emergency medicine residency programs. Acad Emerg Med. 2014;21(7):799–801. doi:10.1111/acem.12408
12. Chiem AT, Soucy Z, Dinh VA, et al. Integration of ultrasound in undergraduate medical education at the California medical schools: a discussion of common challenges and strategies from the UMeCali experience. J Ultrasound Med. 2016;35(2):221–233. doi:10.7863/ultra.15.05006
13. Chen KS, Monrouxe L, Lu YH, et al. Academic outcomes of flipped classroom learning: a meta-analysis. Med Educ. 2018;52(9):910–924. doi:10.1111/medu.13616
14. Hew KF, Lo CK. Flipped classroom improves student learning in health professions education: a meta-analysis. BMC Med Educ. 2018;18(1):38. doi:10.1186/s12909-018-1144-z
15. Belfi LM, Bartolotta RJ, Giambrone AE, Davi C, Min RJ. Flipping” the introductory clerkship in radiology: impact on medical student performance and perceptions. Acad Radiol. 2015;22(6):794–801. doi:10.1016/j.acra.2014.11.003
16. Sivarajah RT, Curci NE, Johnson EM, Lam DL, Lee JT, Richardson ML. A review of innovative teaching methods. Acad Radiol. 2019;26(1):101–113. doi:10.1016/j.acra.2018.03.025
17. Mazur E. Education. Farewell, lecture? Science. 2009;323(5910):50–51. doi:10.1126/science.1168927
18. Crouch CH, Mazur E. Peer instruction: ten years of experience and results. Am J Physics. 2001;69(9):970–977. doi:10.1119/1.1374249
19. Scott J, Millington M, Robert T, et al. The rapid assessment of competency in echocardiography scale: validation of a tool for point‐of‐care ultrasound. J Ultrasound Med. 2016;35:1457–1463. doi:10.7863/ultra.15.07083
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Improvement in Validity and Reliability of Airway Assessment Using Ultrasonography by Novice Personnel: A Learning Cohort Study

Prathep S, Sikarettrakul P, Nimmaanrat S, Juthasantikul W, Karnjanawanichkul O, Kovitwanawong N
Advances in Medical Education and Practice 2022, 13:1103-1111
Published Date: 22 September 2022
Patient’s Perceptions and Attitudes Towards Medical Student’s Involvement in Their Healthcare at a Teaching Hospital in Jordan: A Cross Sectional Study
Taha HA, Al Saqer JK, Al Harbi NR, Younis RN, Al Dawoud F, Nawaiseh MB, Berggren V
Patient Preference and Adherence 2023, 17:629-641
Published Date: 13 March 2023
Integration of Case-Based Dialogue to Enhance Medical Students’ Understanding of Using Health Communication to Address Social Determinants of Health
King J, Taylor J
Advances in Medical Education and Practice 2023, 14:237-244
Published Date: 15 March 2023
Assessing the Proficiency in Basic and Advanced Life Support Among Physicians in Ecuador: A Cross-Sectional Study
Izquierdo-Condoy JS, Naranjo-Lara P, Arias Rodríguez FD, Puglla-Mendoza AG, Jima-Sanmartín J, Andrade Casanova D, Duque-Sánchez EP, Alegría N N, Rojas Cadena MG, Ortiz-Prado E
Advances in Medical Education and Practice 2024, 15:25-35
Published Date: 6 January 2024
The Tensegrity Curriculum: A Comprehensive Curricular Structure Supporting Cultural Humility in Undergraduate Medical Education

Jones AC, Bertsch KN, Williams D, Channell MK
Advances in Medical Education and Practice 2024, 15:381-392
Published Date: 3 May 2024