Back to Journals » ImmunoTargets and Therapy » Volume 15
Induction Chemotherapy Followed by Immunotherapy Increases Pathological Complete Response Rate in dMMR/MSI-H Gastric Cancer: A Retrospective Cohort Study
Authors Zeng H, Wu Y, Zhang Z, Liu J, Sun J, Liu X ![]() , Gu Y, Tian M, Chen W, Shen Z, Shen K, Xu C, Wang X, Tang Z
, Gu Y, Tian M, Chen W, Shen Z, Shen K, Xu C, Wang X, Tang Z ![]() , Sun Y
, Sun Y
Received 31 August 2025
Accepted for publication 27 November 2025
Published 9 January 2026 Volume 2026:15 564230
DOI https://doi.org/10.2147/ITT.S564230
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Shurin
Hong Zeng,1,* Yingying Wu,1,* Ziwei Zhang,1 Jingdong Liu,1 Jie Sun,1 Xinyou Liu,1,2 Yuan Gu,1 Mengxin Tian,1 Weidong Chen,1 Zhenbin Shen,1 Kuntang Shen,1 Chen Xu,3 Xuefei Wang,1,2,4 Zhaoqing Tang,1,2,4 Yihong Sun1,4,5
1Department of Gastrointestinal Surgery, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China; 2Department of General Surgery, Zhongshan Hospital (Xiamen), Fudan University, Xiamen, People’s Republic of China; 3Department of Pathology, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China; 4Gastric Cancer Center, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China; 5Department of General Surgery, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yihong Sun, Department of Gastrointestinal Surgery, Department of General Surgery, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China, Email [email protected] Zhaoqing Tang, Department of Gastrointestinal Surgery, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China, Email [email protected]
Background: Immune checkpoint inhibitor (ICI)-based strategies have become a consensus in the preoperative treatment of mismatch repair-deficient (dMMR)/microsatellite instability-high (MSI-H) gastric cancer (GC). However, the necessity and optimal strategy of combining ICIs with chemotherapy remain uncertain.
Methods: This retrospective study aimed to evaluate the efficacy of different preoperative chemo-immunotherapy combinations in patients with dMMR/MSI-H GC. According to their therapeutic regimens, patients were divided into three cohorts: ICI-alone cohort; immunotherapy with induction chemotherapy (IC) cohort (ICI + IC): 1– 2 cycles of IC followed by ICI; concurrent chemo-immunotherapy cohort (ICI + chemo): ICI combined with chemotherapy throughout the entire preoperative treatment. The pathological complete response (pCR) rate and major pathological response (MPR) rate were analyzed. Peripheral blood parameters before and after preoperative treatment were analyzed.
Results: A total of 45 patients with locally advanced or oligometastatic dMMR/MSI-H GC were included. Baseline characteristics were well balanced among the three cohorts. The pCR rates were 18.2% (95% CI, 2.3– 51.8%) in the ICI-alone cohort, 85.7% (95% CI, 42.1– 99.6%) in the ICI + IC cohort, and 37.0% (95% CI, 19.4– 57.6%) in the ICI + chemo cohort. Notably, the ICI + IC cohort showed a significantly higher pCR rate than the other two cohorts (p=0.015). The MPR rates were 54.5%, 85.7%, and 48.1% in the three cohorts, respectively, with no statistical significance. After preoperative treatment, monocyte-to-lymphocyte ratio exhibited an upward trend in the ICI + IC (p=0.100) and ICI + chemo (p=0.058) cohorts, indicating enhanced antigen presentation activity and immune activation.
Conclusion: A preoperative strategy of IC followed by ICIs significantly increased pCR rate compared to ICI monotherapy or concurrent chemo-immunotherapy, suggesting a more effective strategy for patients with resectable dMMR/MSI-H GC. Given its retrospective design, small sample size, and lack of safety data, this study warrants validation in prospective clinical trials.
Keywords: dMMR/MSI-H gastric cancer, preoperative treatment, induction therapy, immunotherapy, chemotherapy, pathological complete response
Introduction
The mismatch repair-deficient (dMMR) or microsatellite instability-high (MSI-H) gastric cancer (GC) constitutes a distinct molecular subtype, accounting for 8–22% of all cases.1,2 This subtype is characterized by a unique therapeutic profile: it demonstrates a favorable response to immunotherapy while showing relative insensitivity to conventional fluorouracil-based chemotherapy.
The limited efficacy of perioperative chemotherapy for this group is well documented. Meta-analyses have confirmed that the addition of chemotherapy to surgery confers no significant survival benefit over surgery alone.3,4 This resistance is attributed to the inherent mechanism of dMMR, whereby impaired cell cycle checkpoint activation allows tumor cells to evade the cytotoxic DNA damage induced by chemotherapy, thereby promoting their survival and proliferation.5,6
In stark contrast, neoadjuvant strategies incorporating immune checkpoint inhibitors (ICIs) have yielded substantial pathological responses. The addition of ICIs to chemotherapy has demonstrated superior rates of pathological complete response (pCR) compared with chemotherapy alone in the dMMR/MSI-H subgroup, achieving rates of 28.0% in the MATTERHORN trial and 37.1% in the KEYNOTE-585 trial, respectively.7,8 The results of chemotherapy-free regimens are even more remarkable. Dual-ICIs achieved pCR rates of 58.6% in the GERCOR NEONIPIGA study (nivolumab plus ipilimumab) and 60% in the INFINITY study (tremelimumab plus durvalumab), respectively.9,10
However, this enhanced efficacy presents a clinical dilemma. Dual ICIs are associated with a considerable burden of treatment-related adverse events (TRAEs), with grade 3 or higher TRAEs occurring in 37.9% of patients in NO LIMIT trial.11 A logical approach to mitigate this toxicity is to use ICI monotherapy. This strategy is associated with a more favorable safety profile, with grade 3–5 TRAEs rates reported as low as 16.9%.12 Unfortunately, this reduction in toxicity appears to come at the cost of efficacy, as neoadjuvant ICI monotherapy trials have reported disappointing pCR rates of 14–19%.13,14
The role of chemotherapy as a component of neoadjuvant treatment also remains controversial. The addition of chemotherapy to ICIs has not demonstrated superior efficacy over ICI monotherapy for dMMR/MSI-H GC,15 and the potential for synergistic effects is complex and contingent upon the specific regimen, dosage, and sequence used.16
This leaves clinicians with a significant challenge: balancing the high efficacy of dual immunotherapy against its substantial toxicity, versus the lower toxicity but potentially compromised efficacy of monotherapy. An optimal, well-tolerated, and effective preoperative strategy for patients with dMMR/MSI-H GC has yet to be defined.
Therefore, the primary objective of this retrospective cohort study was to evaluate the pathological responses to different ICI-based preoperative therapies in patients with dMMR/MSI-H GC, to help elucidate a more effective therapeutic strategy for this population.
Methods
Study Design and Participants
This was a single-center, retrospective cohort study conducted at Zhongshan Hospital, Fudan University, Shanghai, China. We included consecutive adult patients with a diagnosis of dMMR/MSI-H gastric or gastroesophageal junction adenocarcinoma who received neoadjuvant or conversion therapy with ICIs followed by radical D2 gastrectomy with or without metastasectomy. The dMMR/MSI-H status was a mandatory inclusion criterion, confirmed by either immunohistochemistry (IHC) or molecular testing.
Participants were stratified into three cohorts based on the neoadjuvant regimen they received: ICI monotherapy (ICI-alone cohort): patients who received an ICI targeting PD-1, PD-L1, or CTLA-4 (as a single agent or dual ICI combination) without chemotherapy. Induction chemotherapy (IC) followed by ICI (ICI + IC cohort): patients who received one or two initial cycles of chemotherapy (with or without a concurrent ICI) followed by ICI monotherapy for all subsequent cycles. Concurrent chemo-immunotherapy (ICI + chemo cohort): patients who received an ICI combined with chemotherapy throughout their entire preoperative course.
The study protocol was approved by the ethics committee of Zhongshan Hospital, Fudan University on 4th January, 2025 (approval number B2025-541R), and was conducted in accordance with the Declaration of Helsinki. The requirement for individual patient consent was waived owing to the retrospective nature of the study. Patient data confidentiality was strictly maintained in accordance with institutional and national guidelines.
Procedures and Assessments
The dMMR status was determined by IHC for the mismatch repair proteins MLH1, PMS2, MSH2, and MSH6, with loss of expression in one or more proteins defining deficiency. MSI-H status was confirmed by polymerase chain reaction (PCR) or next generation sequencing (NGS), performed either concurrently with IHC or if IHC results were equivocal.17 A tumor was classified as dMMR/MSI-H if it met the criteria by either IHC or molecular testing.
Hematological and inflammatory markers were analyzed using peripheral venous blood samples collected before the start of perioperative therapy and before surgery. We calculated the monocyte-to-lymphocyte ratio (MLR), neutrophil-to-lymphocyte ratio (NLR), and platelet-to-lymphocyte ratio (PLR). The systemic immune-inflammation index (SII) was calculated as (platelet count × neutrophil count)/lymphocyte count.18
Outcomes
The primary outcome was the pCR. All surgical resection specimens were evaluated by a specialist gastrointestinal pathologist (Dr Xu). pCR was defined as the absence of any residual invasive tumor cells in the primary tumor bed and all resected regional lymph nodes (ypT0N0). For patients with oligometastatic disease at baseline, a clinical complete response of the metastatic lesion was also required for pCR. Furthermore, the rate of major pathological response (MPR), defined as ≤10% residual viable tumor in the primary tumor specimen, was also analyzed. Tumor regression was graded using the Becker tumor regression grade system.19
Statistical Analysis
Descriptive statistics were used to summarize patient characteristics. Categorical variables were presented as counts and percentages, and continuous variables as median and interquartile range (IQR). Rates of pCR and MPR were reported with 95% confidence intervals (CIs).
For comparisons between the three treatment cohorts, the χ2-test or Fisher’s exact test was used for unordered categorical variables, and the Kruskal–Wallis’s test for ordered categorical variables. For continuous variables, the Kruskal–Wallis’s test or one-way analysis of variance (ANOVA) was used as appropriate. To analyze changes in peripheral blood parameters before and after treatment, the paired t-test or Wilcoxon signed-rank test was used. Baseline and change values (Δ = post-pre) of inflammatory markers were compared between pCR and non-pCR groups using independent t-tests or Mann–Whitney U-tests as appropriate.
Univariate and multivariate logistic regression was performed to identify factors associated with pathological response, with results presented as odds ratios (ORs) and 95% CIs. All statistical tests were two sided, and a p value of less than 0.05 was considered statistically significant. All analyses were performed using SPSS Statistics (version 29, IBM). Plots were generated using Prism (version 10, GraphPad Software).
Results
Between January 2018 and January 2025, we screened 423 patients with GC who received ICI-based preoperative therapy followed by surgery. After excluding 378 patients who had proficient mismatch repair (pMMR) status or for whom mismatch repair status was unavailable, 45 patients with dMMR/MSI-H GC were included in the final analysis (Figure 1).
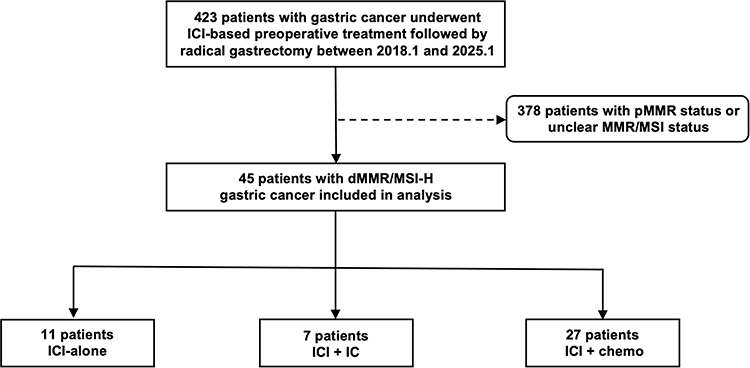 |
Figure 1 Study flowchart. Abbreviations: ICI, immune checkpoint inhibitor; pMMR, proficiency of mismatch repair; MMR, mismatch repair; MSI, microsatellite instability; dMMR, deficiency of mismatch repair; MSI-H, microsatellite instability high; IC, induction chemotherapy; chemo, chemotherapy. |
Characteristics of Cohort
The median age of the 45 included patients was 67.0 years (IQR 59.0–71.0), and 25 (55.6%) were female. The primary tumor was most commonly located in the lower third of the stomach (n=41, 91.1%). Most tumors were of the intestinal Lauren subtype (n=25, 55.6%), and 7 (15.6%) contained a signet-ring cell component. All patients had locally advanced disease (clinical stage cT3-4b) with clinical evidence of lymph node metastasis (cN+), and all were HER2 negative. 33 patients (73.3%) received neoadjuvant treatment, and 12 (26.7%) received conversion therapy for initially unresectable disease. Among the 12 patients who received conversion therapy, three underwent complete resection of metastatic lesions, while the remaining 9 patients showed marked regression of metastases after preoperative therapy and therefore did not undergo metastasectomy. For dMMR/MSI-H status, the loss of MLH1 and PMS2 expression were the most common mode of dMMR status (n=40, 89.0%). Two patients had tumors with equivocal MMR status: one showed loss of MLH1 and MSH6 expression, and the other did not undergo IHC staining; both were confirmed as MSI-H by molecular testing. Among all the included patients, 12 (26.7%) patients additionally underwent molecular testing and were confirmed as MSI-H status without discordance with IHC results. Baseline demographic and clinical characteristics were well balanced across the three cohorts (Table 1).
 |
Table 1 Baseline Clinicopathological Factors of Included Patients |
Preoperative Treatment
Of the 45 patients, 21 patients (46.7%) received four or fewer cycles of preoperative treatment, and 24 patients (53.3%) received more than four cycles. In the ICI-alone cohort (n=11), 9 patients received anti-PD-1 monotherapy, one received anti-PD-L1 monotherapy (Envafolimab) and one received anti-PD-1/CTLA-4 ICI (Cadonilimab). In the ICI + IC cohort (n=7), all patients received one or two cycles of IC before transitioning to anti-PD1 monotherapy: three patients received chemotherapy alone (S-1 or oxaliplatin plus S-1), and four patients received chemotherapy (S-1 or oxaliplatin plus S-1) combined with anti-PD-1 antibody. In the ICI + chemo cohort (n=27), all but one patient (who received a dual anti-PD-1/CTLA-4 antibody, Cadonilimab) were treated with an anti-PD-1 antibody plus chemotherapy. Full details of the chemotherapy regimens are provided in supplementary table 1.
Pathological Response
The rate of pCR (ypT0N0) was 18.2% (95% CI, 2.3–51.8%) in the ICI-alone cohort (2 of 11 patients) while one patient had a complete pathological response in the primary tumor but a positive lymph node (ypT0N1), 85.7% (95% CI, 42.1–99.6%) in the ICI + IC cohort (6 of 7 patients), and 37.0% (95% CI, 19.4–57.6%) in the ICI + chemo cohort (10 of 27 patients). The pCR rate in the ICI + IC cohort was significantly higher than in the other two cohorts (p=0.015; Table 2).
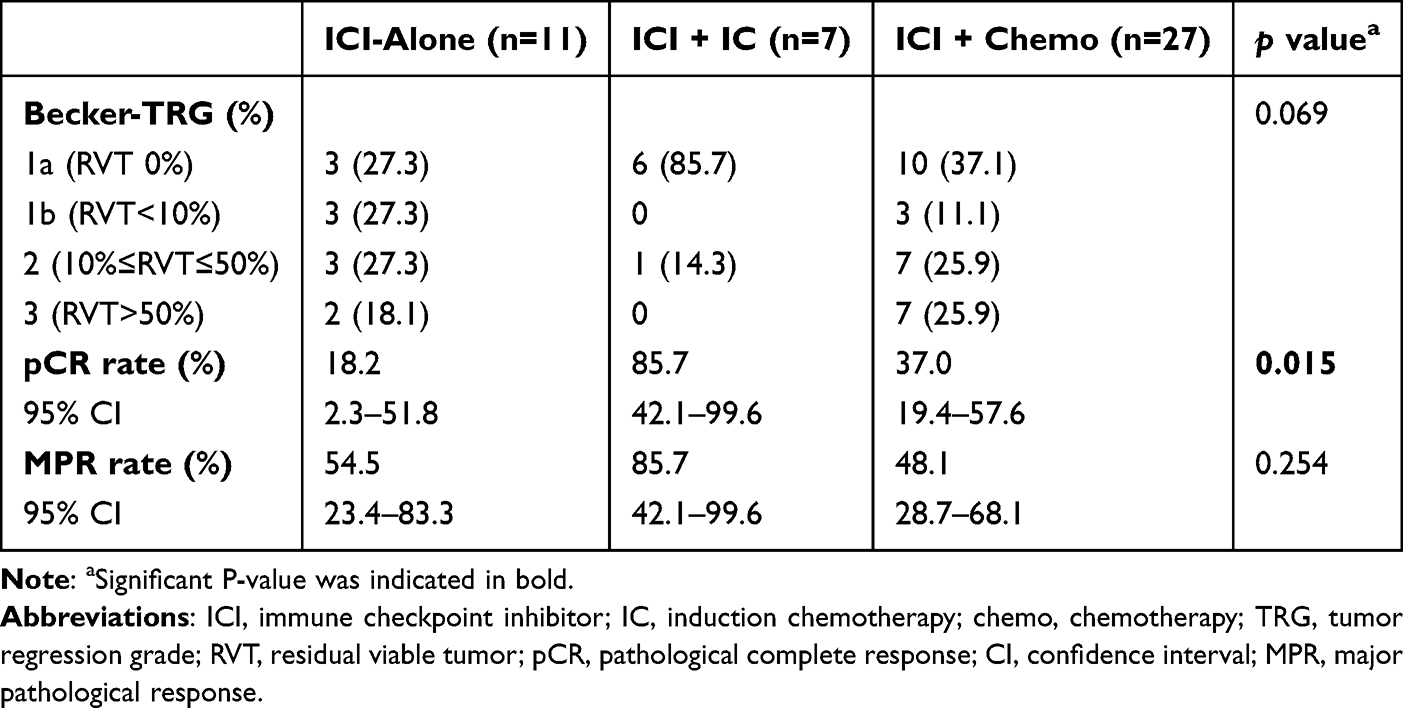 |
Table 2 Pathological Response Among the Three Cohorts |
The MPR rates were 54.5% (95% CI, 23.4–83.3%), 85.7% (95% CI, 42.1–99.6%), and 48.1% (95% CI, 28.7–68.1%) in the ICI-alone, ICI + IC, and ICI + chemo cohorts, respectively. The ICI + IC cohort showed the highest MPR rate, but differences among three cohorts were not statistically significant (Table 2). Tumor regression of the primary lesion in all patients is shown in Figure 2.
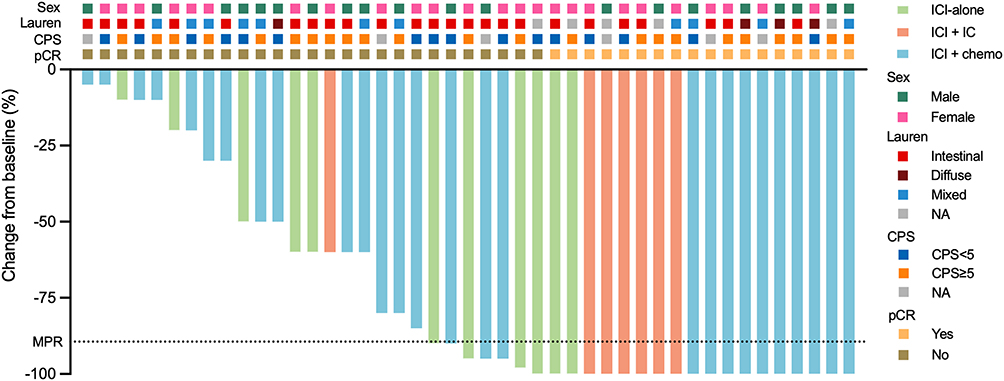 |
Figure 2 Waterfall plot illustrating pathological regression of the primary tumor. Each bar represents the percentage of primary tumor regression for an individual patient. Bars reaching the bottom indicate a pathological complete response of primary tumor (ypT0). The green, red and blue columns correspond to patients in the ICI-alone, ICI + IC, and ICI + chemo cohorts, respectively. Abbreviations: ICI, immune checkpoint inhibitor; IC, induction chemotherapy; chemo, chemotherapy; CPS, combined positive score; pCR, pathological complete response; NA, unavailable. |
A univariate analysis was performed to identify variables potentially associated with pCR (Supplementary Table 2), and the results were summarized in a forest plot (Supplementary Figure 1). Only treatment with ICI + IC regimen was significantly associated with a higher likelihood of achieving pCR (OR 27.00, 95% CI: 1.98–368.38, p=0.013). Lauren classification, tumor site, and cT stage were not associated with pCR. CPS and the total treatment duration were considered to be associated with treatment efficacy, but neither CPS ≥5 nor a total treatment duration >4 cycles was statistically associated with a higher pCR rate. Despite the known resistance of dMMR/MSI-H GC to platinum-based chemotherapy,3,20 the use of platinum-based regimens was not significantly associated with pCR in either the ICI + IC or ICI + chemo cohorts. Additionally, a multivariate logistic regression analysis was conducted to further validate these findings (Supplementary Table 3; Supplementary Figure 2). Consistent with the univariate analysis, only treatment with the ICI + IC regimen remained significantly associated with a higher likelihood of achieving pCR (OR 62.33, 95% CI: 2.08–1872.41, p=0.017).
Follow-Up and Recurrence
After a median follow-up of 14.9 months (IQR 9.3–21.3), one patient in each cohort had experienced disease recurrence. In the ICI-alone cohort, one patient developed distant metastases 6.9 months after surgery. In the ICI + IC cohort, one patient who had achieved a pCR developed distant metastases at 4.0 months after surgery. In the ICI + chemo cohort, one patient had developed distant metastases at 3.5 months after surgery and died one week later from acute liver failure and disseminated intravascular coagulation (Supplementary Figure 3).
Hematological and Inflammatory Markers
Patients in the ICI + IC cohort had a smaller reduction in lymphocyte counts than did patients in the ICI + chemo cohort. The lactate dehydrogenase (LDH) level after treatment was significantly higher in the ICI + chemo cohort compared with the ICI-alone and ICI + IC cohorts (p=0.006). After preoperative treatment, a downward trend was observed for the NLR, PLR, and SII across all three groups. In contrast, the MLR showed an upward trend in both the ICI + IC (p=0.100) and ICI + chemo (p=0.058) cohorts while remaining stable in the ICI-alone cohort (p=0.576; Table 3). Additionally, baseline and change values (Δ = post-pre) of inflammatory markers were compared between pCR and non-pCR groups. Patients achieving pCR showed a greater decrease in lymphocyte counts (p=0.023) and a greater increase in MLR (p=0.014) compared with those without pCR (Supplementary Table 4).
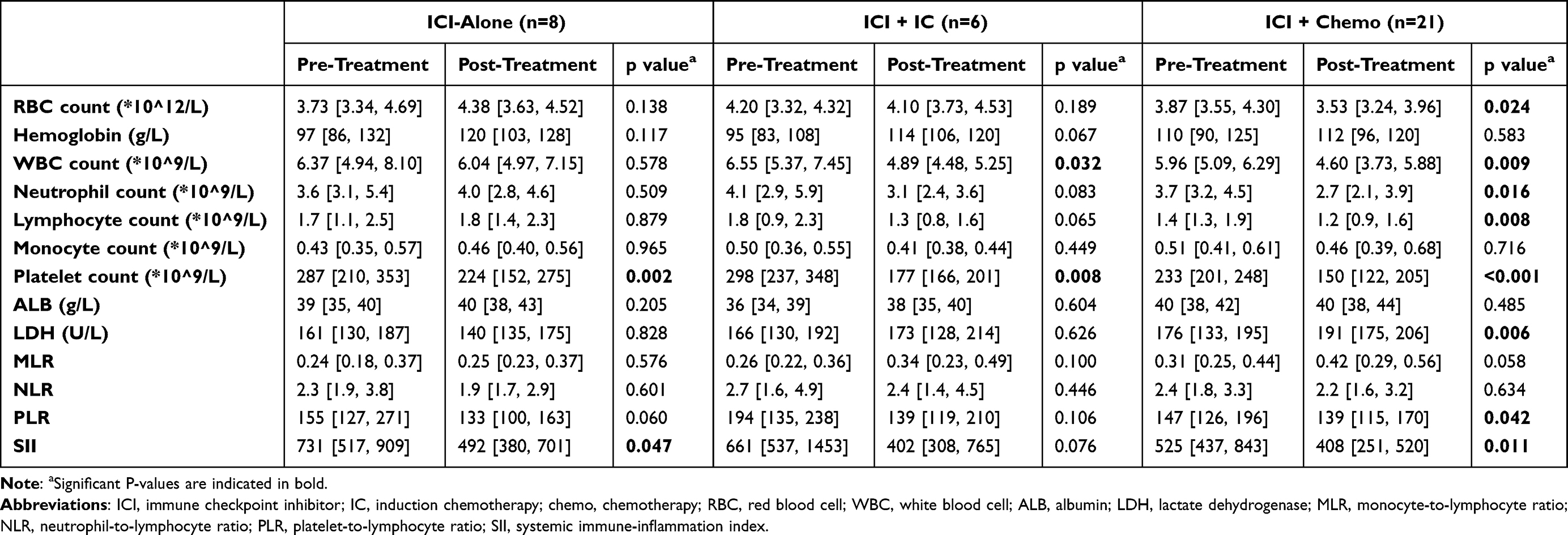 |
Table 3 Peripheral Blood Parameters of Included Patients |
Discussion
In recent years, neoadjuvant immunotherapy has become integral to the management of resectable dMMR/MSI-H GC, yet the optimal strategy for combining it with chemotherapy remains an open question.7–10 Our study addresses this gap, providing evidence that the sequence of administration is a critical determinant of efficacy. We found that a short course of IC followed by ICIs was associated with a notably high pCR rate of 85.7%, which was markedly superior to that achieved with either ICI monotherapy (18.2%) or concurrent chemo-immunotherapy (37.0%).
Our findings on systemic inflammatory markers provide further insight into these different outcomes. The principle that chemotherapy can synergize with immunotherapy is well established,16 and was supported by our observation that both combination regimens yielded higher response rates than ICI monotherapy. A potential mechanism for this is suggested by the upward trend in the MLR observed only in cohorts receiving chemotherapy, which may reflect enhanced monocyte-mediated antigen presentation.21,22 However, the striking difference in efficacy between the induction and concurrent chemotherapy cohorts suggests that the timing of this synergy is crucial. Patients receiving concurrent chemotherapy experienced a greater reduction in lymphocyte counts and had significantly higher post-treatment LDH levels, which may indicate greater treatment-related toxicity. In contrast, the induction strategy appeared to be lymphocyte sparing. This suggests that while both chemotherapy regimens may prime an immune response, a sequential induction strategy might optimally stimulate the immune system via mechanisms such as enhanced antigen presentation while mitigating the lymphocyte-depleting toxicity of prolonged chemotherapy, thus creating a more favorable microenvironment for subsequent ICI therapy.
This clinical observation is supported by preclinical models. Compared to concurrent administration, initial chemotherapy followed by ICIs increased the infiltration of CD8+ T cells and enhanced their cytotoxic function.23 In addition to CD8+ T cells, natural killer cells and neutrophils were also activated, while immunosuppressive cells were reduced.24,25 Furthermore, induction chemotherapy can trigger immunogenic cell death, leading to the release of tumor antigens and danger-associated molecular patterns, which promote dendritic cell maturation and enhance antigen presentation, thus activating tumor-specific T cell responses and creating a more favorable immune landscape for subsequent immunotherapy.26–28 More importantly, studies have shown that chemotherapy drugs, such as cisplatin combined with temozolomide, could induce mutations characteristic of dMMR. The subsequent loss of DNA damage repair function contributed to increased tumor-mutational burden (TMB) and expanded repertoire of clonal neoantigens, thereby provoking durable, CD8+ T cell-dominated anti-tumor immunity and sensitizing tumors to subsequent PD-1 blockade.29,30 In GCs with dMMR/MSI-H status at baseline, the addition of induction chemotherapy may therefore act synergistically to further increase TMB and amplify neoantigen-driven T cell responses. Taken together, these findings may explain the superior efficacy observed in the ICI + IC cohort compared to the other two cohorts.
From a clinical standpoint, our findings are important because they suggest a potential alternative to the current strategy of dual ICIs. Although highly effective, dual immunotherapy is associated with considerable toxicity and high healthcare costs.11 IC strategy followed by single-agent ICI could offer a highly effective, better tolerated, and more economically viable option. This may be particularly relevant in populations, such as those in many parts of Asia, where a low prevalence of Lynch syndrome might limit the benefit derived from dual ICIs.31
However, our study has several important limitations. The principal one is its retrospective, single-center design and small sample size, which can introduce selection bias and limit the generalizability of our findings. The low prevalence of dMMR/MSI-H GC makes large scale studies challenging, but our results should be considered hypothesis generating. Secondly, the retrospective data collection meant that detailed information on TRAEs was not uniformly available, which prevented a formal comparison of the safety profiles between cohorts. This may have obscured a potential advantage of the induction strategy in terms of reduced toxicity. Finally, some baseline data, including peripheral blood parameters, were missing for some patients.
Our findings require validation in prospective, multi-center randomized trials to confirm the efficacy and safety of the IC approach compared with concurrent chemo-immunotherapy and dual ICIs. Future studies should be powered to detect differences not only in pathological response but also in long-term outcomes such as disease-free and overall survival. Furthermore, translational research integrated into these trials is necessary to elucidate the precise immunological mechanisms underlying the superiority of the sequential strategy and to identify biomarkers that could predict which patients are most likely to benefit.
Conclusion
This retrospective study found that a neoadjuvant strategy of IC followed by ICIs was associated with a significantly higher pCR rate in patients with dMMR/MSI-H GC compared with either ICI monotherapy or concurrent chemo-immunotherapy. Given its retrospective design, small sample size, and lack of safety data, this study warrants validation in prospective clinical trials. However, this study should be considered hypothesis generating and represents a highly promising preoperative treatment strategy for dMMR/MSI-H GC.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to patient privacy and ethical restrictions, but are available from the corresponding author, Zhaoqing Tang, on reasonable request. Proposals will be reviewed and approved by the authors based on scientific merit.
Ethical Approval and Informed Consent
The study protocol was approved by the ethics committee of Zhongshan Hospital, Fudan University on 4th January, 2025 (approval number B2025-541R), and was conducted in accordance with the Declaration of Helsinki. The requirement for individual patient consent was waived owing to the retrospective nature of the study. Patient data confidentiality was strictly maintained in accordance with institutional and national guidelines.
Funding
This work was supported by the Science and Technology Commission of Shanghai Municipality (23ZR1410700 and 23Y11902100); the Natural Science Foundation of Fujian Province (2023J011692); the Natural Science Foundation of China (82273303); the Special Project for Clinical Research of Zhongshan Hospital (ZSLCYJ202335).
Disclosure
The authors report there are no competing interests to declare.
References
1. Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature. 2014;513(7517):202–11. doi:10.1038/nature13480
2. Strickland MR, Lander EM, Gibson MK, Ilson DH, Ajani JA, Klempner SJ. Gastroesophageal adenocarcinomas with defective mismatch repair: current knowledge and clinical management. J Natl Compr Canc Netw. 2024;22(3):e237103. doi:10.6004/jnccn.2023.7103
3. Pietrantonio F, Miceli R, Raimondi A, et al. Individual patient data meta-analysis of the value of microsatellite instability as a biomarker in gastric cancer. J Clin Oncol. 2019;37(35):3392–3400. doi:10.1200/JCO.19.01124
4. Liu B, Shen C, Yin X, et al. Perioperative chemotherapy for gastric cancer patients with microsatellite instability or deficient mismatch repair: a systematic review and meta-analysis. Cancer. 2025;131(7):e35831. doi:10.1002/cncr.35831
5. Ooki A, Osumi H, Yoshino K, Yamaguchi K. Potent therapeutic strategy in gastric cancer with microsatellite instability-high and/or deficient mismatch repair. Gastric Cancer. 2024;27(5):907–931. doi:10.1007/s10120-024-01523-4
6. de la Fouchardiere C, Cammarota A, Svrcek M, et al. How do I treat dMMR/MSI gastro-oesophageal adenocarcinoma in 2025? A position paper from the EORTC-GITCG gastro-esophageal task force. Cancer Treat Rev. 2025;134:102890. doi:10.1016/j.ctrv.2025.102890
7. Janjigian YY, Al-Batran SE, Wainberg ZA, et al. Perioperative durvalumab in gastric and gastroesophageal junction cancer. N Engl J Med. 2025;393(3):217–230. doi:10.1056/NEJMoa2503701
8. Shitara K, Rha SY, Wyrwicz LS, et al. Neoadjuvant and adjuvant pembrolizumab plus chemotherapy in locally advanced gastric or gastro-oesophageal cancer (KEYNOTE-585): an interim analysis of the multicentre, double-blind, randomised Phase 3 study. Lancet Oncol. 2024;25(2):212–224. doi:10.1016/S1470-2045(23)00541-7
9. Andre T, Tougeron D, Piessen G, et al. Neoadjuvant nivolumab plus ipilimumab and adjuvant nivolumab in localized deficient mismatch repair/microsatellite instability-high gastric or esophagogastric junction adenocarcinoma: the GERCOR NEONIPIGA Phase II study. J Clin Oncol. 2023;41(2):255–265. doi:10.1200/JCO.22.00686
10. Raimondi A, Lonardi S, Murgioni S, et al. Tremelimumab and durvalumab as neoadjuvant or non-operative management strategy of patients with microsatellite instability-high resectable gastric or gastroesophageal junction adenocarcinoma: the INFINITY study by GONO. Ann Oncol. 2025;36(3):285–296. doi:10.1016/j.annonc.2024.11.016
11. Kawakami H, Kadowaki S, Makiyama A, et al. Phase II study (NO LIMIT, WJOG13320G) of first-line nivolumab plus low-dose ipilimumab for microsatellite instability-high advanced gastric or esophagogastric junction cancer. J Clin Oncol. 2025;JCO2402463.
12. Shitara K, Van Cutsem E, Bang YJ, et al. Efficacy and safety of pembrolizumab or pembrolizumab plus chemotherapy vs chemotherapy alone for patients with first-line, advanced gastric cancer: the KEYNOTE-062 phase 3 randomized clinical trial. JAMA Oncol. 2020;6(10):1571–1580. doi:10.1001/jamaoncol.2020.3370
13. Fouchardiere CD, Zaanan A, Cohen R, et al. 1448P IMHOTEP phase II trial of neoadjuvant pembrolizumab in dMMR/MSI localized cancers: results of the digestive non-colorectal cancer cohorts. Ann Oncol. 2024;35:S899–S900. doi:10.1016/j.annonc.2024.08.1514
14. Hasegawa H, Shitara K, Takiguchi S, et al. A multicenter, open-label, single-arm Phase I trial of neoadjuvant nivolumab monotherapy for resectable gastric cancer. Gastric Cancer. 2022;25(3):619–628. doi:10.1007/s10120-022-01286-w
15. Chao J, Fuchs CS, Shitara K, et al. Assessment of pembrolizumab therapy for the treatment of microsatellite instability-high gastric or gastroesophageal junction cancer among patients in the KEYNOTE-059, KEYNOTE-061, and KEYNOTE-062 clinical trials. JAMA Oncol. 2021;7(6):895–902. doi:10.1001/jamaoncol.2021.0275
16. Zhu S, Zhang T, Zheng L, et al. Combination strategies to maximize the benefits of cancer immunotherapy. J Hematol Oncol. 2021;14(1):156. doi:10.1186/s13045-021-01164-5
17. Vikas P, Messersmith H, Compton C, et al. Mismatch repair and microsatellite instability testing for immune checkpoint inhibitor therapy: ASCO endorsement of college of American pathologists guideline. J Clin Oncol. 2023;41(10):1943–1948. doi:10.1200/JCO.22.02462
18. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
19. Becker K, Mueller JD, Schulmacher C, et al. Histomorphology and grading of regression in gastric carcinoma treated with neoadjuvant chemotherapy. Cancer. 2003;98(7):1521–1530. doi:10.1002/cncr.11660
20. Ambrosini M, Manca P, Nasca V, et al. Epidemiology, pathogenesis, biology and evolving management of MSI-H/dMMR cancers. Nat Rev Clin Oncol. 2025;22(6):385–407. doi:10.1038/s41571-025-01015-z
21. Li Z, Li S, Ying X, et al. The clinical value and usage of inflammatory and nutritional markers in survival prediction for gastric cancer patients with neoadjuvant chemotherapy and D2 lymphadenectomy. Gastric Cancer. 2020;23(3):540–549. doi:10.1007/s10120-019-01027-6
22. Larionova I, Iamshchikov P, Kazakova A, et al. Platinum-based chemotherapy promotes antigen presenting potential in monocytes of patients with high-grade serous ovarian carcinoma. Front Immunol. 2024;15:1414716. doi:10.3389/fimmu.2024.1414716
23. Mariniello A, Nasti TH, Chang DY, et al. Platinum-based chemotherapy attenuates the effector response of CD8 T cells to concomitant PD-1 blockade. Clin Cancer Res. 2024;30(9):1833–1845. doi:10.1158/1078-0432.CCR-23-1316
24. Li K, Gui S, Wang N, et al. Sequential pH/GSH-responsive stealth nanoparticles for co-delivery of anti-PD-1 antibody and paclitaxel to enhance chemoimmunotherapy of lung cancer. Eur J Med Chem. 2025;285:117273. doi:10.1016/j.ejmech.2025.117273
25. Zhu C, Shi Y, Li Q, et al. Rational administration sequencing of immunochemotherapy elicits powerful anti-tumor effect. J Control Release. 2022;341:769–781. doi:10.1016/j.jconrel.2021.12.022
26. Galluzzi L, Buque A, Kepp O, Zitvogel L, Kroemer G. Immunogenic cell death in cancer and infectious disease. Nat Rev Immunol. 2017;17(2):97–111. doi:10.1038/nri.2016.107
27. Kroemer G, Galassi C, Zitvogel L, Galluzzi L. Immunogenic cell stress and death. Nat Immunol. 2022;23(4):487–500. doi:10.1038/s41590-022-01132-2
28. Li C, Qi X, Yan M. Chemotherapy-induced immunogenic cell death in combination with ICIs: a brief review of mechanisms, clinical insights, and therapeutic implications. Front Pharmacol. 2025;16:1572195. doi:10.3389/fphar.2025.1572195
29. Vitiello PP, Rousseau B, Chila R, et al. Cisplatin and temozolomide combinatorial treatment triggers hypermutability and immune surveillance in experimental cancer models. Cancer Cell. 2025;43(7):1296–1312e7. doi:10.1016/j.ccell.2025.05.014
30. Rousseau B, Patel M, Artz O, et al. Induction of a mismatch repair deficient genotype by tailored chemical mutagenesis in experimental models of cancer. Cancer Cell. 2025;43(7):1313–1327e10. doi:10.1016/j.ccell.2025.05.010
31. Ito T, Suzuki O, Kamae N, et al. Comprehensive analysis of DNA mismatch repair-deficient gastric cancer in a Japanese hospital-based population. Jpn J Clin Oncol. 2021;51(6):886–894. doi:10.1093/jjco/hyab026
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pathologic Complete Response Prediction to Neoadjuvant Immunotherapy Combined with Chemotherapy in Resectable Locally Advanced Esophageal Squamous Cell Carcinoma: Real-World Evidence from Integrative Inflammatory and Nutritional Scores
Feng J, Wang L, Yang X, Chen Q, Cheng X
Journal of Inflammation Research 2022, 15:3783-3796
Published Date: 6 July 2022
Nanoparticles for Chemoimmunotherapy Against Triple-Negative Breast Cancer
Liu S, Li J, Gu L, Wu K, Xing H
International Journal of Nanomedicine 2022, 17:5209-5227
Published Date: 7 November 2022
A Case of Complete Remission in Proficient Mismatch Repair (pMMR) Advanced Colon Cancer Treated with Sintilimab and XELOX
Zhu J, Li G, Zhang Z, Wang Y
ImmunoTargets and Therapy 2023, 12:17-23
Published Date: 19 February 2023
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
Diagnosis, Prognosis, and Treatment of Triple-Negative Breast Cancer: A Review
Jie H, Ma W, Huang C
Breast Cancer: Targets and Therapy 2025, 17:265-274
Published Date: 17 March 2025