Back to Journals » International Medical Case Reports Journal » Volume 18
Hepatotoxicity Induced by Adalimumab in Chronic Plaque Psoriasis Patient: A Case Report
Authors Algarzae NK, Alotaibi HM, Alajlan AH ![]() , AlSaleh MR, Alsalman AA
, AlSaleh MR, Alsalman AA
Received 16 May 2025
Accepted for publication 5 July 2025
Published 9 July 2025 Volume 2025:18 Pages 877—881
DOI https://doi.org/10.2147/IMCRJ.S536412
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Norah K Algarzae,1 Hend M Alotaibi,2 Ahmed H Alajlan,2 Muneera R AlSaleh,3 Alanoud A Alsalman4
1Department of Physiology, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2Department of Dermatology, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 3Department of Dermatology, King Khalid University Hospital, Riyadh, Saudi Arabia; 4Department of Dermatology, King Fahad Medical City, Riyadh, Saudi Arabia
Correspondence: Ahmed H Alajlan, Email [email protected]
Introduction: Adalimumab is a TNF-α antagonist used to treat psoriasis and rheumatologic conditions; it can rarely cause hepatotoxicity manifesting as elevated liver enzymes.
Case Presentation: Here, we present a case of a 24-year-old female with chronic plaque psoriasis with no history of liver disease or any risk factor for liver disease who developed a drug-induced liver injury upon treatment initiation with Adalimumab. This case report highlights the importance of monitoring liver function tests in patients receiving Adalimumab, early recognition, and prompt medication dosage adjustment or discontinuation. Early diagnosis and treatment of chronic plaque psoriasis is critical for improving prognosis, especially in the case of increased risk factors of liver disease due to the administration of Adalimumab.
Conclusion: Our case presented a patient with no history of liver disease; however, she developed a drug-induced liver injury. Therefore, this case report is the first to emphasize the need for early recognition of LFTs upon Adalimumab administration, and prompt medication dosage adjustment or discontinuation is essential in patients receiving Adalimumab.
Keywords: Adalimumab, psoriasis, liver enzyme elevation, drug-induced liver injury, case report
Introduction
Adalimumab is a fully human recombinant immunoglobulin G (IgG) monoclonal antibody with specificity for tumor necrosis factor-alpha (TNF-α). Adalimumab binds to soluble and membrane-bound TNF-α, leading to a blockade of its activity, resulting in apoptosis of cells with membrane-bound TNF.1 The most common adverse reaction to Adalimumab is injection site reaction, occurring in more than 10% of treated patients; other adverse reactions include the reactivation of tuberculosis, which is the most serious.2 Drug-induced systemic lupus erythematosus, lymphoma, and demyelinating illness are other serious adverse effects, but these occur infrequently.3 Hepatotoxicity also affects less than 5% of patients on treatment, which commonly manifests as an asymptomatic increase in liver enzymes.4
There are a few case reports on hepatotoxicity and Adalimumab; however, these are primarily on patients diagnosed with other autoimmune diseases, such as rheumatoid arthritis and inflammatory bowel disease. Literature on hepatotoxicity associated with Adalimumab among patients with psoriasis is scarce.5 However, there is a case report of a patient with psoriasis who developed liver enzyme elevation. The liver failure prognosis was not attributed to Adalimumab because it was discounted, but the liver enzymes were elevated, possibly due to methotrexate.6 Currently, our case is the first to present a rare occurrence of liver enzyme elevation in a patient with psoriasis treated with Adalimumab. Our patient was a healthy young female who had never been treated previously with any medications aside from Adalimumab and topical treatments.
Case Presentation
A 24-year-old female with no known co-morbidities and no history of taking any medications was diagnosed with chronic plaque psoriasis in 2017. She first presented with erythematous plaques with silvery fine scaling over the knees as shown in Figure 1, which progressed to involve the elbows as shown in Figure 2, other areas of the lower limbs, and scalp. She has no family history of a similar disease.
 |
Figure 1 Erythematous plaques with silvery fine scaling over the knees consistent with chronic plaque psoriasis. |
 |
Figure 2 Progression of the erythematous plaques to involve the bilateral elbows. |
Prior to receiving therapy, the patient underwent viral hepatitis, viral load tests, and serologic testing for the hepatitis B and C viruses, all of which came out negative. She had never used drugs or alcohol, received blood transfusions, or had any other history of viral hepatitis risk factors. Initial treatment was done with calcipotriene-betamethasone 4% topical ointment twice a day and tacrolimus 0.1% topical twice daily without any noticeable improvement in the lesions. Adalimumab was subcutaneously administered in December 2020, and the dosage was 40 milligrams every 2 weeks. Clobetasol and calcipotriene solutions were simultaneously administered for the scalp lesions. At 5 months post-treatment, her symptoms resolved. However, her liver function tests (LFTs) revealed an alanine aminotransferase (ALT) level of 152 μ/L (2.3 times elevated the upper limit of normal [ULN]), aspartate aminotransferase (AST) level of 79 μ/L (2.5 times elevated the ULN) and total bilirubin level of 19.83 μmol/L (1.2 times elevated the ULN). Hepatology then assessed her to have developed a drug-induced liver injury.
Repeat viral hepatitis screening (including HBV, HCV, and HAV serologies and PCR when relevant) was required to rule out infectious reasons after liver enzyme increased in April 2021, but all results came back negative. Additionally unremarkable were signs of autoimmune liver disease and abdominal ultrasonography, which supported the diagnosis of drug-induced liver impairment. Following the test results, we discontinued Adalimumab immediately. The patient was then closely monitored with serial liver function tests over the following 4–6 weeks of Adalimumab discontinuation; her liver enzymes returned to baseline levels (LFTs returned to normal: ALT of 30 μ/L, AST of 20 μ/L, and total bilirubin of 10.45 μmol/L) without the need for hospitalization or further treatment. Upon involving the patient in the management plan, we decided to start her on subcutaneous Risankizumab at a dosage of 150mg. At a 6-month follow-up, there was no elevation in the liver enzymes.
Discussion
In the literature, Adalimumab has been linked to a low incidence of increased aminotransferases during treatment. However, such incidences are transient, mild, asymptomatic, and rarely necessitate dosage modification. The rise in levels resolved in 82% of patients upon follow-up.5 Liver enzyme abnormality was characterized as a twofold or more significant rise above the ULN in two or more of the following components: AST, ALT, total bilirubin, lactate dehydrogenase (LDH), or alkaline phosphatase (ALP).7 Our patient exhibited significantly increased AST and ALT levels. Although liver injury associated with TNF-α inhibitors such as Adalimumab is generally idiosyncratic, it presents a clinically relevant risk due to its potential cellular damage and variability.8 The precise mechanism remains unclear; however, the literature sheds some light on its possible involvement with immune-mediated harm or direct hepatocellular toxicity.9 In the literature, an example of the damage was shown in a case report that described a patient with rheumatoid arthritis treated with Adalimumab. Despite the patient having hepatitis C, their LFTs remained stable before commencing treatment. The patient’s gamma-glutamyl transpeptidase (GGT) level surged to 23 times the ULN three months post adalimumab administration, while the ALP level rose to 2.5 times the ULN. Interestingly, the patient did not display elevated AST and ALT levels; Adalimumab was discontinued six months after treatment.10 Similarly, in an analysis of thirty-four cases, hepatotoxicity linked to TNF-α antagonists varied from asymptomatic enzyme increases to severe liver damage, with most instances resolving upon discontinuation of the drug.11,12
The fundamental risk factors for liver disease, particularly in metabolic syndrome and fatty liver diseases in patients with psoriasis, enhance the chances of hepatotoxicity at the initial stages.13 Therefore, it is recommended that liver function tests be performed before the commencement of therapy and periodically during therapy. This predisposing risk is why routine monitoring must be employed to enable early detection. According to the recent literature, Madani and Almuhaideb described a case study of a patient with Down syndrome and psoriasis receiving Adalimumab whose liver enzymes flare up due to hepatitis B virus infection.14 Björnsson et al stated concern about drug-induced liver injury attributable to TNF-α antagonists.8 However, the stated overall risk remains relatively low as long as other predisposing factors are considered. In addition, Hagel et al9 noted that such injuries are highly unique and thus require monitoring to detect any subsequent similar injuries.
More specifically, the precise cause of liver injury related to Adalimumab is still unknown and appears to be quite random.9,12 Further research is, however, required to identify other factors that may predispose a patient to this side effect. In addition, more extensive research and surveys on a more significant population sample are needed to establish the injury patterns of hepatotoxicity. Our current case focuses on the importance of early identification and risk mitigation of drug-induced liver injury. LFTs should be performed before starting treatment and periodically throughout treatment.11 In this case, and indeed in managing most ADRs, withdrawal of the offending agent remains the strength of treatment, which we are the first to present. Active comparators like Risankizumab, which were proven to have a better hepatic safety profile in this patient, give hope for patients developing adverse reactions to Adalimumab.
In comparison with previous studies on the subject, our case report is the first to highlight the importance of routine testing of LFTs in patients receiving Adalimumab, early recognition, and prompt medication dosage adjustment or discontinuation (see Table 1). While Adalimumab has shown a favorable safety profile over 15 years of use,15 clinicians must remain vigilant for rare adverse events, such as hepatotoxicity, particularly in patients with additional risk factors.
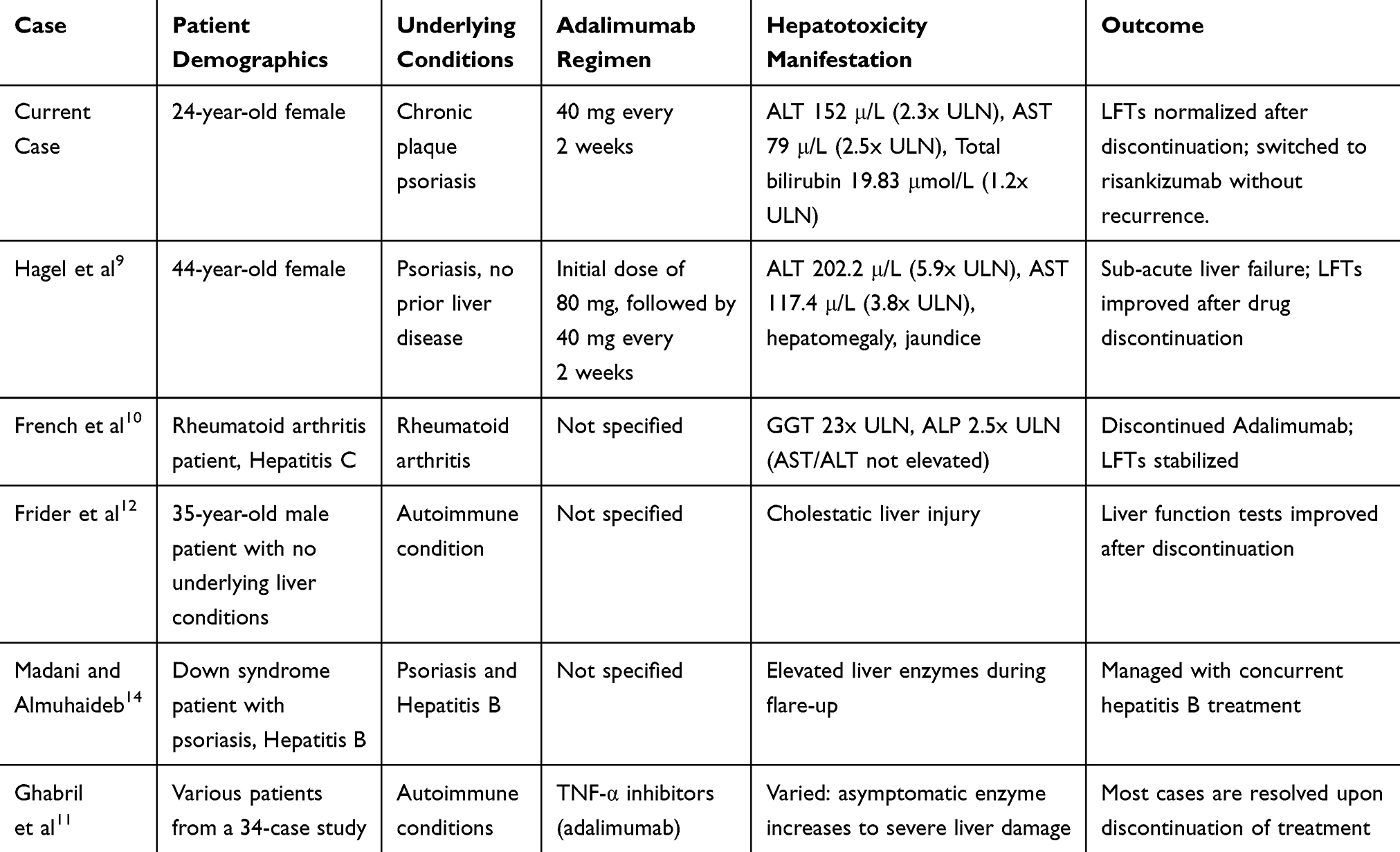 |
Table 1 Comparison of Current Cases with Previously Published Cases of Adalimumab-Induced Hepatotoxicity |
Conclusions
Early diagnosis and treatment of chronic plaque psoriasis is critical for improving prognosis, especially in the case of increased risk factors of liver disease due to the administration of Adalimumab. Our case presented a patient with no history of liver disease; however, she developed a drug-induced liver injury. Although the mechanism of liver injury could be idiosyncratic, liver injury is an uncommon, underreported adverse effect of this drug. Therefore, this case report emphasizes the need for early recognition of LFTs upon Adalimumab administration, and prompt medication dosage adjustment or discontinuation is essential in patients receiving Adalimumab.
Data Sharing Statement
All the data for this case report will be made available upon reasonable request. Further inquiries can be directed to the corresponding author.
Consent for Publication
All authors gave their consent for publication, and written informed consent was obtained from the patient to publish the details of their medical care and any accompanying images.
Study Approval Statement
Ethical approval is not required for case reports at our institution while not disclosing patient identity.
Acknowledgment
The authors are grateful to the team of physicians, nurses, and allied health professionals working at King Saud University Medical Complex who collaborated on this patient’s case. The authors would like to extend their gratitude to Researchers Supporting Project, King Saud University, Riyadh, Saudi Arabia, for funding this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not supported by any sponsor or funder.
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Jamieson T, Cook DN, Nibbs RJB, et al. The chemokine receptor D6 limits the inflammatory response in vivo. Nat Immunol. 2005;6(4):403–411. doi:10.1038/ni1182
2. Ramos-Casals M, Brito-Zerón P, Muñoz S, et al. Autoimmune diseases induced by TNF-targeted therapies: analysis of 233 cases. Medicine. 2007;86(4):242–251. doi:10.1097/MD.0b013e3181441a68
3. Su X, Yu H, Lei Q, et al. Systemic lupus erythematosus: pathogenesis and targeted therapy. Mol Biomed. 2024;5(1):54. doi:10.1186/s43556-024-00217-8
4. Trachana M, Pratsidou-Gertsi P, Pardalos G, Kozeis N, Badouraki M, Kanakoudi-Tsakalidou F. Safety and efficacy of Adalimumab treatment in Greek children with juvenile idiopathic arthritis. Scand J Rheumatol. 2011;40(2):101–107. doi:10.3109/03009742.2010.517546
5. Sokolove J, Strand V, Greenberg JD, et al. Risk of elevated liver enzymes associated with TNF inhibitor utilisation in patients with rheumatoid arthritis. Ann Rheum Dis. 2010;69(9):1612–1617. doi:10.1136/ard.2009.112136
6. Borman MA, Urbanski S, Swain MG. Anti-TNF-induced autoimmune hepatitis. J Hepatol. 2014;61(1):169–170. doi:10.1016/j.jhep.2014.01.032
7. Her M, Lee Y, Jung E, Kim T, Kim D. Liver enzyme abnormalities in systemic lupus erythematosus: a focus on toxic hepatitis. Rheumatol Int. 2011;31(1):79–84. doi:10.1007/s00296-009-1237-4
8. Björnsson ES, Gunnarsson BI, Gröndal G, et al. Risk of drug-induced liver injury from tumor necrosis factor antagonists. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. 2015;13(3):602–608. doi:10.1016/j.cgh.2014.07.062
9. Hagel S, Bruns T, Theis B, Herrmann A, Stallmach A. Subacute liver failure induced by Adalimumab. Int J Clin Pharmacol Ther. 2011;49(1):38–40. doi:10.5414/cpp49038
10. French JB, Bonacini M, Ghabril M, Foureau D, Bonkovsky HL. Hepatotoxicity Associated with the use of anti-TNF-α agents. Drug Saf. 2016;39(3):199–208. doi:10.1007/s40264-015-0366-9
11. Ghabril M, Bonkovsky HL, Kum C, et al. Liver injury from tumor necrosis factor-α antagonists: analysis of thirty-four cases. Clin Gastroenterol Hepatol Off Clin Pract J Am Gastroenterol Assoc. 2013;11(5):558–564.e3. doi:10.1016/j.cgh.2012.12.025
12. Frider B, Bruno A, Ponte M, Amante M. Drug-induced liver injury caused by Adalimumab: a case report and review of the bibliography. Case Rep Hepatol. 2013;2013:406901. doi:10.1155/2013/406901
13. Fiore M, Leone S, Maraolo AE, Berti E, Damiani G. Liver illness and psoriatic patients. BioMed Res Int. 2018;2018:3140983. doi:10.1155/2018/3140983
14. Madani A, Almuhaideb Q. Adalimumab therapy in a patient with psoriasis, down syndrome, and concomitant hepatitis B virus infection. Biol Targets Ther. 2021;15:375–378. doi:10.2147/BTT.S317888
15. Sator P. Safety and tolerability of Adalimumab for the treatment of psoriasis: a review summarizing 15 years of real-life experience. Ther Adv Chronic Dis. 2018;9(8):147–158. doi:10.1177/2040622318772705
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Anti-TNF Biosimilars for Psoriasis in Pediatric and Geriatric Populations: A 72-Week Real-Life Study
Megna M, Fornaro L, Potestio L, Luciano MA, Nocerino M, Delfino M, Guarino M, Fabbrocini G, Camela E
Psoriasis: Targets and Therapy 2022, 12:199-204
Published Date: 9 July 2022
Drug Survival Outcomes Associated with the Real-World Use of Ixekizumab, Secukinumab, Guselkumab, and Adalimumab for the Treatment of Plaque Psoriasis in China: A 52-Week Single-Center Retrospective Study
Li Y, Lu JJ, Zhong XY, Yu YY, Yu N, Wang Y, Yi XM, Ding YF, Shi YL
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2245-2252
Published Date: 20 October 2022
Psoriasis on Lesions of Vitiligo: A Case Report
Wang L, Zhang B
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2005-2007
Published Date: 4 August 2023
A Case Report of Adalimumab Successfully Treated a Severe Plaque Psoriasis Patient with Psoriatic End-Stage Renal Disease
Xu J, Chen A, Peng Y, Wen Z, Huang K, Wang P
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2841-2846
Published Date: 12 October 2023
Successful Treatment of Refractory Synovitis, Acne, Pustulosis, Hyperostosis, and Osteitis (SAPHO) Syndrome and Paradoxical Psoriasis with Secukinumab: A Case Report
Fan D, Li F, Liu Z, Tang Z, Lv S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:547-552
Published Date: 5 March 2024