Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
A Case Report of Adalimumab Successfully Treated a Severe Plaque Psoriasis Patient with Psoriatic End-Stage Renal Disease
Authors Xu J, Chen A, Peng Y, Wen Z, Huang K ![]() , Wang P
, Wang P
Received 11 May 2023
Accepted for publication 20 August 2023
Published 12 October 2023 Volume 2023:16 Pages 2841—2846
DOI https://doi.org/10.2147/CCID.S420900
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Jing Xu,1 Aijun Chen,1 Yuting Peng,1 Zhuyuan Wen,1,2 Kun Huang,1 Ping Wang1
1Department of Dermatology, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2College of Pediatric, Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Ping Wang, Department of Dermatology, The First Affiliated Hospital of Chongqing Medical University, No. 1, Youyi Road, Yuzhong District, Chongqing, People’s Republic of China, Email [email protected]
Abstract: Psoriasis is a common chronic inflammatory skin disease that manifests itself not only on the skin but also on various tissues and organs of the body. While some psoriasis co-morbidities have been investigated, little is known about its association with impairment of renal function. In 2005, the concept of psoriatic nephropathy was first introduced by Indian nephrologists, suggesting a potential relationship between psoriasis and kidney disease. Adalimumab, a fully human recombinant immunoglobulin G1 monoclonal antibody against tumor necrosis factor (TNF)-α, has been shown to be a safe and effective treatment for patients with moderate to severe psoriasis. Here, we present a case of severe plaque psoriasis accompanied with end-stage renal disease (ESRD) treated with adalimumab. Following the case presentation is a discussion of the relationship between psoriasis and chronic kidney disease (CKD) / ESRD and the possible role of biologics in psoriasis-related kidney damage. The aim of this report is to increase dermatologists’ awareness of psoriatic nephropathy as a complication of psoriasis and to raise awareness of the use of biologics in psoriasis.
Keywords: psoriasis, end-stage kidney disease, chronic kidney disease, adalimumab, biologics
Introduction
Psoriasis is a common chronic inflammatory skin disease that involves not only the skin but also several organs.1 A large body of literature confirms the association between psoriasis and a variety of diseases such as cardiometabolic disorders, stroke, and mood disorders in different populations and environments, which are referred to as psoriasis co-morbidities.2–4 In addition to this, cases of psoriasis related renal damage have also been reported.5–7 In the last decade, the treatment of psoriasis has seen the emergence of biologics targeting cytokines and receptors involved in pathogenesis, such as adalimumab, an TNF-α inhibitor.8 Here, we present a case of ESRD in a patient with psoriasis for more than 10 years. We suggest that patients with psoriasis are more likely to develop CKD and ESRD and that biologics may also play a role in therapy for psoriasis-related kidney damage.
Case Presentation
A 40-year-old male with a 10-year history of psoriasis was admitted to our nephrology department with a 1-year history of elevated blood pressure and 5-day edema in both lower extremities. A year ago, the patient developed dizziness with no apparent cause, and his blood pressure was found to be elevated to about 190/110 mmHg at the local hospital. He was treated with oral nifedipine, but without regular medication and blood pressure monitoring, and reported normal blood creatinine. Five days ago, the patient presented with bilateral lower extremity edema, scanty urine and increased foam in the urine, along with wheezing and fatigue after activity with a slight cough and a small amount of yellow sputum, followed by nausea and weakness, and fluid exudation from the broken skin of both lower extremities was seen. Local hospital test results suggested urine protein 3+, blood creatinine 976 umol/L, and elevated white blood cells. Then, he was transferred to our hospital, and symptomatic treatment was administered with ceftriaxone anti-infection, diuretic and calcium supplementation. 10 years ago, he was diagnosed with psoriasis vulgaris and had been treated intermittently and irregularly with acitretin capsules (Neotigason), xiaoyin tablets (Chinese patent drug, made from Rehmania, Tree Peony Bark, Red Peony and other herbs) and some topical medications for psoriasis, but his condition recurred without regular follow-up and management.
On admission, laboratory examination revealed severe renal dysfunction (creatinine 992 umol/L, urea 24.7mmol/L, uric acid 845 umol/L, urine protein 3+, and endogenous creatinine clearance [CCr] 9.3L/24h), renal anemia (hemoglobin 103.0 g/L), and elevated inflammatory markers (leukocyte 15.36*10^9/L, NEUT% 83.2%, and procalcitonin 0.58 ng/mL). Cardiac ultrasound showed increased left atrial volume, left ventricular hypertrophy, and mild tricuspid regurgitation. The patient was diagnosed with ESRD, and treated with anti-infective, diuretic, and antihypertensive therapy. On the second day of hospitalization, the patient received a dermatological consultation. Physical examination showed swollen skin of the lower extremities, and cracked and desquamated erythema on the scalp, trunk and extremities. There are many crusted pustules on top of patchy lesions involving more than 87% of the body surface area, with a tendency toward erythrodermic psoriasis (Figure 1a). There was no joint involvement. His PASI score was calculated as 62, and his Physician Global Assessment (PGA) score was 4. Based on dermatological consultation, the diagnosis of severe plaque psoriasis and pustular psoriasis was considered; therefore, the patient was given daily closure of the extremities and trunk with mometasone furoate cream (Eloson) + Vaseline. At the same time, considering the patient’s high severity of psoriasis, previous lack of significant improvement by traditional medications and the possible burden on the kidneys by traditional oral medications because of his comorbid ESRD, we concluded that biologic therapy was safe and effective, and the patient was advised to complete procalcitonin, interleukin assays and other related tests (Table 1).
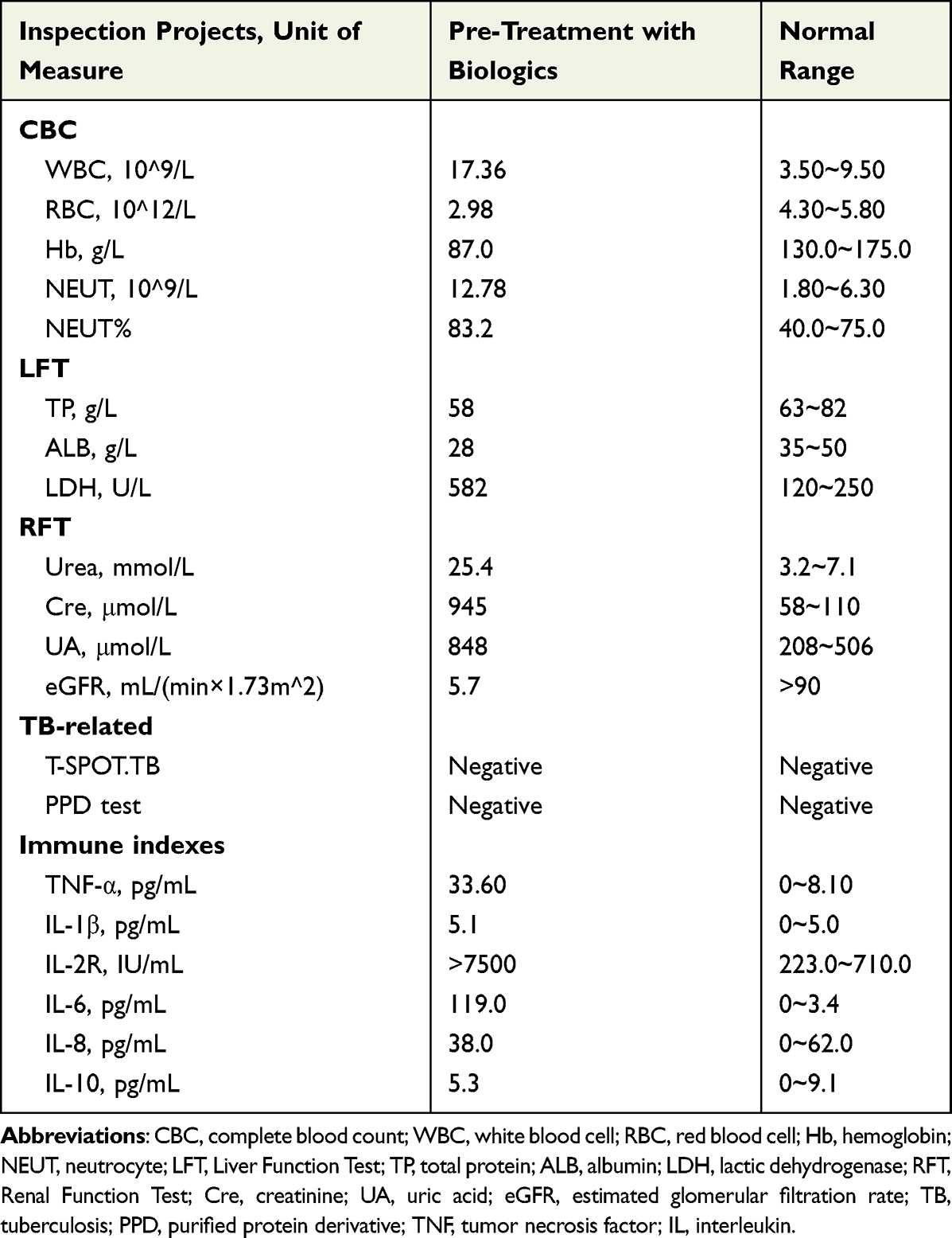 |
Table 1 Laboratory Examination Pre-Biologic Treatment |
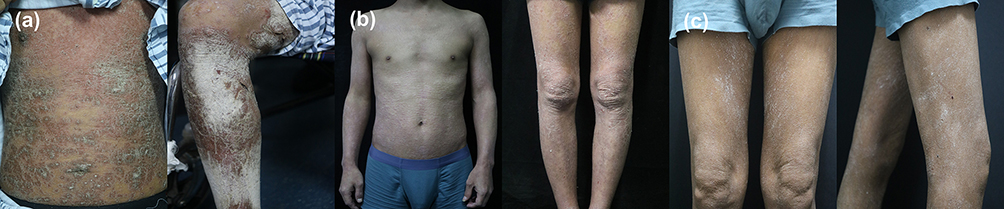 |
Figure 1 Clinical manifestation of Psoriasis. (a) Skin involvement of more than 80% of the body surface area on admission. The Psoriasis Area and Severity Index (PASI) score was 62. (b) Skin involvement after two sessions of Adalimumab treatment. The PASI score was 12. (c) Skin involvement at 12 weeks after Adalimumab initiation. The PASI score was 1. |
On the 7th day of hospitalization, adalimumab s.c. treatment at a dose of 80 mg was given to the patient after the appeal results showed no absolute contraindication to treatment with biological agents. At the introduction of adalimumab, laboratory examination also revealed renal dysfunction (creatinine 945 umol/L, urea 25.4 mmol/L, uric acid 848 umol/L, and estimate glomerular filtration rate [eGFR] 5.7 mL/min per 1.73 m2). The patient was advised to give adalimumab 40 mg injection after one week, and 40 mg every two weeks thereafter. During the second week of admission, he received a 40 mg adalimumab injection, and 8 days after the second adalimumab injection, the patient was discharged and received injections every other week thereafter. He reached PASI 75 (75% decrease in PASI) at discharge (Figure 1b). The affected skin area was reduced to 15% with a PASI of 12 and a PGA of 3.
After discharge from the hospital, the patient was on regular hemodialysis, and is now stable and awaiting a nephrogenic kidney transplant. The patient also adheres to regular adalimumab regimen, and is regularly followed up in the dermatology clinic for regular management. In a physical examination 2 months after he was discharged, only a few skin lesions were found on his lower limbs (Figure 1c). The surface area of lesions is only 1%, PASI was 2 and PGA was 1. Until now, he still follows up regularly, and maintains 90% improvement of the PASI score.
Discussion
Psoriasis is a chronic inflammatory proliferative skin disease that is prone to recurrence, which is clinically characterized by well-defined papules, plaques, and often covered with silvery scales.9 In addition to skin lesions, it also affects multiple organs such as the eyes, liver, cardiovascular system, kidney, and gastrointestinal tract.2,10 Renal involvement in the course of psoriasis is not an uncommon event. It is generally accepted that if renal lesions develop years after the onset of psoriasis, they are mostly related to the duration of the disease, the area of skin damage, the severity of the disease, and often improve as the skin damage improves. The manifestations of psoriasis-related renal damage are more diverse, such as back pain, microscopic hematuria, nephrotic syndrome, hypertension, and renal failure,11,12 but the link between the two diseases is still controversial. It is not totally clear if nephropathy is caused by psoriasis or it is simply coincidental.
The patient in this case developed ESRD 10 years after his diagnosis of psoriasis. There have been many discussions in recent years about the relationship between psoriasis and CKD and ESRD. Wan et al13 compared the incidence of CKD in 143,833 patients with psoriasis and 689,702 psoriasis-free controls. In their study, the severity of psoriasis was assessed according to the treatment modality taken by the patients, and the patients who had received phototherapy, methotrexate, azathioprine, cyclosporine, etanercept, adalimumab, infliximab, and ustekinumab were categorized as severe patients (7354 patients), and patients who had not been treated with phototherapy, systemic therapy, or biologics were classified as mild (136,529 patients). Their study found that severe psoriasis was an independent risk factor for CKD and ESRD after adjusting for sex, age, cardiovascular disease, diabetes, hypertension, hyperlipidemia, body mass index and use of non-steroidal anti-inflammatory drugs. In order to explore the risk of inflammatory skin disease and CKD, Schonmann et al14 matched each patient with CKD stages 3–5 with up to five patients without CKD to compare the prevalence of CKD stages 3–5 in individuals with and without inflammatory skin disease. Their study suggested that the CKD case group was more likely to have a combined history of atopic dermatitis, psoriasis, and hidradenitis suppurativa than the control group, and the results remained the same after correcting the analysis for confounding factors.
It has been found that psoriasis patients are not only more likely to develop CKD and ESRD, but the incidence is positively correlated with the disease severity of psoriasis. A cohort study in Taiwan found that the risk of CKD and ESRD in patients with severe psoriasis was nearly doubled and tripled, respectively.15 In a cohort study by Chiu et al16 in which patients with psoriasis were followed for 5 years to assess the incidence of CKD and glomerulonephritis (GN), it was found that both patients with mild and severe psoriasis had a significantly increased risk of developing CKD and GN compared to the controls without psoriasis, and that patients with severe psoriasis had higher risk ratios for CKD (HR 1.57 vs 1.52), and GN (HR 1.93 vs 1.46) were higher in patients with severe psoriasis than in those with mild psoriasis. We can see a definite correlation between psoriasis and CKD, but the underlying pathogenesis of the interaction between the two and the promotion of disease progression remains unclear.
In 2015, Japan reported the first successful treatment with adalimumab of a patient with psoriasis vulgaris who was on hemodialysis due to renal failure.17 The effective treatment of psoriasis with biological agents implies that the inflammatory factors such as TNF-α, IL-12, and IL-23 also have an important role in the inflammatory process of psoriasis.11,18 Interestingly, previous studies have found that these inflammatory factors are also involved in renal injury, such as TNF-α, which affects renal hemodynamics and renal unit transport, leading to NaCl retention and hypertension, and IL-23, which drives renal inflammation characterized by massive T-lymphocyte infiltration.19,20 Lavoz et al21 found that inhibition of IL-17 ameliorated renal injury and disease progression in mice with a diabetic nephropathy model. In addition, recent articles have reported that biologic treatment of psoriasis can simultaneously improve kidney damage in patients. Veronesi et al22 evaluated the renal function of 92 patients with moderate-to-severe plaque psoriasis treated with biologic agents, including 35 patients with anti-IL-17 biologics (28 with secukinumab and 7 with ixekizumab), 34 patients with anti-TNF-α biologics (25 with adalimumab and 9 with etanercept), and 23 patients with anti-IL-12/23 biologic (ustekinumab). Their study found a decrease in mean serum creatinine levels after 1 year of treatment (0.98 mL/min vs 0.90 mL/min), as well as a decrease in mean PASI from 17.55 to 1.20. As the use of biologics has become popular, their safety has also received attention. Maghfour et al23 found that biologics do not affect long-term renal function in patients with psoriasis combined with CKD. In addition, due to the extremely large molecular weight, biologics is difficult to excrete from the kidneys in its prototypical form and to metabolize by hepatic drug metabolizing enzymes, but is eliminated mainly by intracellular enzymatic degradation, making the use of biologics less burdensome to the kidneys.24 These studies showed that treatment targeting psoriasis-causing inflammatory factors may improve the underlying renal damage associated with psoriatic inflammation.
The risk of CKD and ESRD associated with moderate-to-severe psoriasis has been underestimated compared to that of psoriasis comorbidities such as cardiovascular disease and metabolic syndrome. As the prevention and care of CKD and ESRD has become an important public health policy, this case is also a reminder to all dermatologists that closer monitoring of renal insufficiency, such as routine screening for urinary microalbuminuria, serum creatinine and serum urea nitrogen tests, should be considered in patients with moderate to severe psoriasis, which can help with early detection and intervention to reduce the high morbidity and mortality of CKD and ESRD. Because host defenses are often compromised in patients with CKD/ESRD, careful monitoring and follow-up of infection is also required when administering biologic therapies. Further research into biologic therapies for patients with CKD/ESRD would provide useful treatment options for patients with psoriasis suffering from renal failure.
Conclusion
Our case report suggests that biologics are a reasonable treatment option for renal failure in patients with severe psoriasis. Further case reports and long-term studies are needed to elucidate the association between psoriasis and CKD/ESRD and to evaluate biologic therapies for the treatment of patients with severe psoriasis in combination with CKD/ESRD.
Consent Statement
Patients have given written informed consent for the publication of their clinical details and accompanying images. Institutional approval was not required for this case study.
Funding
This research was funded by national natural science foundation of China, grant number NSFC 82103733.
Disclosure
The authors have nothing to disclose.
References
1. Armstrong AW, Read C. Pathophysiology, Clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323(19):1945–1960.
2. Amin M, Lee EB, Tsai TF, Wu JJ. Psoriasis and co-morbidity. Acta Derm Venereol. 2020;100(3):adv00033. doi:10.2340/00015555-3387
3. Bu J, Ding R, Zhou L, Chen X, Shen E. Epidemiology of psoriasis and comorbid diseases: a narrative review. Front Immunol. 2022;13:2484.
4. Takeshita J, Grewal S, Langan SM, et al. Psoriasis and comorbid diseases: epidemiology. J Am Acad Dermatol. 2017;76(3):377–390.
5. Grewal SK, Wan J, Denburg MR, Shin DB, Takeshita J, Gelfand JM. The risk of IgA nephropathy and glomerular disease in patients with psoriasis: a population-based cohort study. Br J Dermatol. 2017;176(5):1366–1369. doi:10.1111/bjd.14961
6. Tokuyama M, Shimizu T, Yamada T, Kondoh A, Mabuchi T. Case of psoriasis vulgaris with atrial fibrillation, heart failure and chronic kidney disease which were found accidentally through blood examination during apremilast treatment. J Dermatol. 2019;46(7):e239–e240. doi:10.1111/1346-8138.14784
7. Sakemi T, Hayashida R, Ikeda Y, Baba N, Nishihara G, Kohda H. Membranous glomerulonephropathy associated with psoriasis vulgaris. Nephron. 1996;72(2):351–352.
8. Honma M, Hayashi K. Psoriasis: recent progress in molecular-targeted therapies. J Dermatol. 2021;48(6):761–777.
9. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. 2021;397(10281):1301–1315.
10. Takeshita J, Grewal S, Langan SM, et al. Psoriasis and comorbid diseases: implications for management. J Am Acad Dermatol. 2017;76(3):393–403. doi:10.1016/j.jaad.2016.07.065
11. Visconti L, Leonardi G, Buemi M, et al. Kidney disease and psoriasis: novel evidences beyond old concepts. Clin Rheumatol. 2016;35(2):297–302. doi:10.1007/s10067-015-3126-4
12. Conti A, Giovannini L, Mandel VD, et al. Chronic kidney disease in psoriasis: a cohort study. J Dtsch Dermatol Ges. 2020;18(5):438–445.
13. Wan J, Wang S, Haynes K, Denburg MR, Shin DB, Gelfand JM. Risk of moderate to advanced kidney disease in patients with psoriasis: population based cohort study. BMJ. 2013;347(oct15 7):f5961. doi:10.1136/bmj.f5961
14. Schonmann Y, Mansfield KE, Mulick A, et al. Inflammatory skin diseases and the risk of chronic kidney disease: population-based case-control and cohort analyses. Br J Dermatol. 2021;185(4):772–780. doi:10.1111/bjd.20067
15. Chi CC, Wang J, Chen YF, Wang SH, Chen FL, Tung TH. Risk of incident chronic kidney disease and end-stage renal disease in patients with psoriasis: a nationwide population-based cohort study. J Dermatol Sci. 2015;78(3):232–238. doi:10.1016/j.jdermsci.2015.03.012
16. Chiu HY, Huang HL, Li CH, et al. Increased risk of glomerulonephritis and chronic kidney disease in relation to the severity of psoriasis, concomitant medication, and comorbidity: a nationwide population-based cohort study. Br J Dermatol. 2015;173(1):146–154. doi:10.1111/bjd.13599
17. Kusakari Y, Yamasaki K, Takahashi T, et al. Successful adalimumab treatment of a psoriasis vulgaris patient with hemodialysis for renal failure: a case report and a review of the previous reports on biologic treatments for psoriasis patients with hemodialysis for renal failure. J Dermatol. 2015;42(7):727–730. doi:10.1111/1346-8138.12901
18. Skutnik-Radziszewska A, Maciejczyk M, Flisiak I, et al. Enhanced inflammation and nitrosative stress in the saliva and plasma of patients with plaque psoriasis. J Clin Med. 2020;9(3). doi:10.3390/jcm9030745
19. Li H, Tsokos MG, Bhargava R, et al. IL-23 reshapes kidney resident cell metabolism and promotes local kidney inflammation. J Clin Invest. 2021;131(12). doi:10.1172/JCI142428
20. Mehaffey E, Majid DSA. Tumor necrosis factor-alpha, kidney function, and hypertension. Am J Physiol Renal Physiol. 2017;313(4):F1005–F1008. doi:10.1152/ajprenal.00535.2016
21. Lavoz C, Matus YS, Orejudo M, et al. Interleukin-17A blockade reduces albuminuria and kidney injury in an accelerated model of diabetic nephropathy. Kidney Int. 2019;95(6):1418–1432. doi:10.1016/j.kint.2018.12.031
22. Veronesi G, Guglielmo A, Gardini A, et al. Biological therapy in patients with psoriasis: what we know about the effects on renal function. Dermatol Ther. 2022;35(1):e15202. doi:10.1111/dth.15202
23. Maghfour J, Elliott E, Gill F, Stumpf B, Murina A. Effect of biologic drugs on renal function in psoriasis patients with chronic kidney disease. J Am Acad Dermatol. 2020;82(5):1249–1251. doi:10.1016/j.jaad.2019.12.043
24. Posner J, Barrington P, Brier T, Datta-Mannan A. Monoclonal antibodies: past, present and future. Handb Exp Pharmacol. 2019;260:81–141.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Anti-TNF Biosimilars for Psoriasis in Pediatric and Geriatric Populations: A 72-Week Real-Life Study
Megna M, Fornaro L, Potestio L, Luciano MA, Nocerino M, Delfino M, Guarino M, Fabbrocini G, Camela E
Psoriasis: Targets and Therapy 2022, 12:199-204
Published Date: 9 July 2022
Drug Survival Outcomes Associated with the Real-World Use of Ixekizumab, Secukinumab, Guselkumab, and Adalimumab for the Treatment of Plaque Psoriasis in China: A 52-Week Single-Center Retrospective Study
Li Y, Lu JJ, Zhong XY, Yu YY, Yu N, Wang Y, Yi XM, Ding YF, Shi YL
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2245-2252
Published Date: 20 October 2022
Interleukin-17A Inhibitor Secukinumab Treatment in HIV-Positive Psoriasis Patient: A Case Report
Gong J, Wu W, Qiu L, Wang X, Bao J, Wang J, Cheng L, Fu Z, Hu F
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2949-2956
Published Date: 30 December 2022
Tildrakizumab for the Treatment of Moderate-to-Severe Psoriasis: Results from 52 Weeks Real-Life Retrospective Study
Ruggiero A, Fabbrocicni G, Cacciapuoti S, Potestio L, Gallo L, Megna M
Clinical, Cosmetic and Investigational Dermatology 2023, 16:529-536
Published Date: 27 February 2023
Efficacy and Safety of Secukinumab in Elderly Patients with Moderate to Severe Plaque-Type Psoriasis: Post-Hoc Analysis of the SUPREME Study
Talamonti M, Russo F, Malara G, Hansel K, Papini M, Cattaneo A, Parodi A, Chiricozzi A, Malagoli P, Bardazzi F, Brazzelli V, Dapavo P, Gisondi P, Zane C, Potenza C, Cantoresi F, Fargnoli MC, Trevisini S, Brianti P, Pescitelli L, Gigante G, Bartezaghi M, Caputo L, Aloisi E, Costanzo A
Clinical, Cosmetic and Investigational Dermatology 2023, 16:847-852
Published Date: 1 April 2023