Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Psoriasis on Lesions of Vitiligo: A Case Report
Received 14 April 2023
Accepted for publication 30 June 2023
Published 4 August 2023 Volume 2023:16 Pages 2005—2007
DOI https://doi.org/10.2147/CCID.S417290
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Lijuan Wang,1 Bin Zhang1,2
1Department of Dermatology, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, Beijing, 100045, People’s Republic of China; 2Department of Dermatology, Children’s Hospital Affiliated to Zhengzhou University, Henan Children’s Hospital, Zhengzhou Children’s Hospital, Zhengzhou, 450003, People’s Republic of China
Correspondence: Bin Zhang, Department of Dermatology, Beijing Children’s Hospital, Capital Medical University, National Center for Children’s Health, No. 56 Nanlishi Road, Xicheng District, Beijing, 100045, People’s Republic of China, Tel +861059616392, Fax +861059718700, Email [email protected]
Abstract: Vitiligo and psoriasis are common T cell-mediated autoimmune skin diseases, and the association of the two disorders has been well known. In most cases, vitiligo precedes the onset of psoriasis. In this study, we reported a case of vitiligo who developed psoriasis following an upper respiratory tract infection with a uniform shape of psoriatic lesions at the phototherapy site of vitiligo. After 2 months of discontinuation of phototherapy and concurrent treatment with topical corticosteroid and calcipotriol, the psoriasis lesions were significantly improved.
Keywords: vitiligo, psoriasis, phototherapy, Koebner phenomenon, case report
Introduction
The worldwide occurrence of psoriasis is 1–3%, and that of vitiligo in the general population is about 0.1–2%. Psoriasis and vitiligo are characterized by multifactorial, complex mechanisms, which include genetic predisposition and environmental factors that trigger immune pathways. As the common cutaneous disorders, there are numerous reports about the coexistence of psoriasis and vitiligo in the medical literature. Although the relationship between the two diseases is not well known, they do indeed have notable similarities: gene association, an activation of the Th1 and Th17 cellular immune system pathways, neuropeptides, and Koebner phenomenon.1,2 Recognition of this association can lead to a better understanding of the etiologies, pathogenesis, and treatment of these diseases.
Herein, we presented a case with vitiligo who developed psoriasis following an upper respiratory tract infection with a uniform shape of psoriatic lesions at the phototherapy site of vitiligo.
Case Report
A 5-year-old boy with vitiligo was treated with 308nm excimer laser for three months. One month ago, erythematous lesions appeared over whole body after an upper respiratory infection, which did not attract the attention of parents. Thus, phototherapy of vitiligo was not interrupted. After continuing the 308nm excimer laser at a dose of 400mJ/cm2 for one-week, red papules consistent with the shape of the laser machine spot appeared in the vitiligo phototherapy areas. Physical examination revealed multiple scaly papules and plaques scattered on the trunk and buttock (Figure 1A), particularly on the laser-treated vitiliginous areas (Figure 1B). The histological findings were consistent with psoriasis and vitiligo. Coexistence of vitiligo and guttate psoriasis with a Koebner phenomenon was made. After 2 months of discontinuation of phototherapy and concurrent treatment with topical corticosteroid and calcipotriol, the psoriasis lesions were significantly improved.
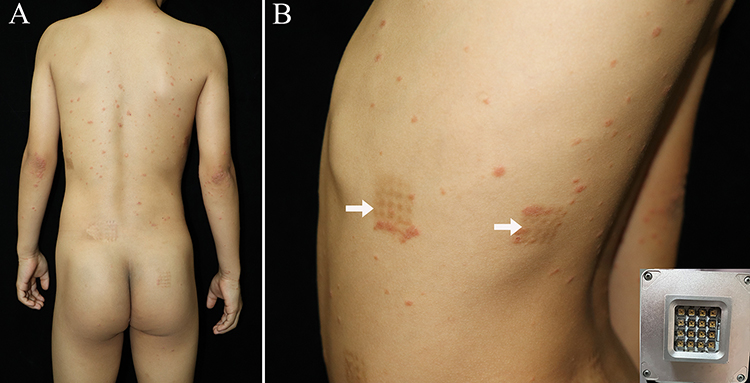 |
Figure 1 (A) Multiple scaly papules and plaques were scattered on the trunk. (B) Several scaly erythematosus papules were seen on the laser-treated hypopigmented areas (white arrows). Insert depicts the shape of laser machine. |
Discussion
Psoriasis and vitiligo are common cutaneous diseases, so the coexistence of each disease is not infrequent and surprising. The first case of psoriasis and vitiligo was reported by Selenyi in 1955.3 From then on, there have been several reports of the coexistence of these two diseases in the English medical literature. In most cases including the present one report, the initial vitiligo often precedes the development of psoriasis,4 although the cases of vitiligo following a longstanding history of psoriasis have been also reported.5 Although some authors thought the disease concomitance to be occasional based on the prevalence of psoriasis among vitiligo group similar to those in the general population,4 more evidence suggest the possibility for a relationship between psoriasis and vitiligo. On further review of the literature, 27 (6%) out of 436 Italian patients,1 12 (3.3%) out of 361 Iran patients2 and 6% of Iraq patients with vitiligo6 also had psoriasis, which were statistically significant when compared with the control.
Several theories have been proposed to explain the phenomenon. Both psoriasis and vitiligo are inflammatory autoimmune disorders, where Th1 and Th17 cells play an important role in their pathogenesis.7 IFN-γ is involved in the pathogenesis of vitiligo and psoriasis. Recently, the IL-23/IL-17 axis is considered fundamental in the pathogenesis of these two diseases. IL-17, the main immunological feature of the vitiligo, affects the melanocyte damage through different routes. Besides, psoriasis and vitiligo share a common genetic locus in the major histocompatibility complex. Rs. 9,468,925 in HLA-C/HLA-B was found associated with both psoriasis and vitiligo in China.8 Through a systematic evaluation, Arunachalam et al concluded that the presence of vitiligo and even mild psoriasis is significantly correlated with a family history of cardiovascular disease, which requires greater attention and follow-up.1 The Koebner phenomenon may be an alternative explanation for the coexistence and colocalization of these two diseases.1
It has previously been reported that psoriatic plaques and guttate lesions can be strictly localized or not colocalized to the vitiliginous patches, or both. The matter is further complicated lesions after treatment with PUVA9 and narrow-band UVB.10 The interesting colocalization of psoriatic guttate lesions over 308nm-excimer laser treated vitiliginous patches in our patient has raised speculation on the role of T-cell activation in the development of psoriasis. It has been demonstrated that 308nm is the most efficient wavelength for inducing T-lymphocyte apoptosis. In theory, our patient should not have developed psoriatic lesions on the 308nm-excimer laser treated vitiliginous areas. This paradox may be explained by the clinical heterogenicity and Koebner phenomenon. It is speculated that the phototherapy as a form of local trauma resulted in true koebnerization of psoriasis. Ultraviolet (UV) can trigger the occurrence and aggravation of psoriatic lesions. According to the literature, even suberythemal doses could induce psoriatic lesions or aggravate pre-existing psoriasis, which is named photosensitive psoriasis.11 It was speculated that the possible reason is the biphasic biologic response of UV, in which a low dose of UV radiation may suppress, whereas a higher dose may trigger psoriasis.12 However, more research is needed to clarify the exact mechanisms involved.
In our case, we could not identify the exact interrelationship of both diseases. However, because the psoriatic guttate lesions developed both UVB-treated vitiliginous areas and other areas, we suggest that the concurrence of psoriasis and vitiligo is not a coincidence. Further, more and extensive studies should be done to clarify the relationship and pathogenesis.
Conclusion
We presented an infrequent case of vitiligo coexisted with psoriasis, which was aggravated by phototherapy in the phototherapy vitiliginous patches. It is speculated that this curious cohabitation may be resulted from Koebner phenomenon. This requires further insight into their pathogenesis. Phototherapy is a double-edged sword for patients predisposed to psoriasis. We highlight the dermatologist’ awareness of this phenomenon and suggest that more caution should be exercised when adjusting the dose of phototherapy in patient with vitiligo and psoriasis.
Consent Statement
Informed consent for publication of the case details and associated images was obtained from the parents of the patient, and all procedures were performed in accordance with the Helsinki Declaration. Institutional approval was not required to publish the case details.
Funding
This study was supported by the National Natural Science Foundation of China (no. 82103698), the Natural Science Foundation of Beijing Municipality (no. 7222058), and Open Project of Henan Clinical Research Center of Childhood Diseases (no. YJZX202209).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Arunachalam M, Dragoni F, Colucci R, et al. Non-segmental vitiligo and psoriasis comorbidity - a case-control study in Italian patients. J Eur Acad Dermatol Venereol. 2014;28(4):433–437. doi:10.1111/jdv.12117
2. Yazdanpanah MJ, Banihashemi M, Pezeshkpoor F, Moradifar M, Feli S, Esmaeili H. Evaluation between Association of Psoriasis and Vitiligo. J Cutan Med Surg. 2015;19(2):140–143. doi:10.2310/7750.2014.14074
3. Selenyi A. Vitiligo and psoriasis on the same side with syringomyelia. Borgyogy Venerol Sz. 1955;9(3):94–96.
4. Sandhu K, Kaur I, Kumar B. Psoriasis and vitiligo. J Am Acad Dermatol. 2004;51:149–150. doi:10.1016/j.jaad.2003.12.014
5. Langley AR, Manley P, Asai Y. A case of colocalized vitiligo and psoriasis. J Cutaneous Med Surgery. 2016;20(2):150.
6. Sharquie KE, Salman HA, Yaseen AK. Psoriasis and vitiligo are close relatives. Clin Cosmet Invest Dermatol. 2017:341
7. Aghamajidi A, Raoufi E, Parsamanesh G. The attentive focus on T cell-mediated autoimmune pathogenesis of psoriasis, lichen planus and vitiligo. Scand J Immunol. 2021;93(4):e13000.
8. Zhu KJ, Lv YM, Yin XY, et al. Psoriasis regression analysis of MHC loci identifies shared genetic variants with vitiligo. PLoS One. 2011;6(11):e23089. doi:10.1371/journal.pone.0023089
9. Inamadar AC, Sampagavi VV, Athanikar SB, Patil MN, Deshmukh NS. Vitiligo and psoriasis: coexistence with colocalization. Indian J Dermatol Venereol Leprol. 2001;67:214.
10. Goodwin RG, Finlay AY, Anstey AV. Vitiligo following narrowband TL-01 phototherapy for psoriasis. Br J Dermatol. 2001;144:1264–1266. doi:10.1046/j.1365-2133.2001.04247.x
11. Rutter KJ, Watson RE, Cotterell LF, Brenn T, Griffiths CE, Rhodes LE. Severely photosensitive psoriasis: a phenotypically defined patient subset. J Invest Dermatol. 2009;129(12):2861–2867. doi:10.1038/jid.2009.156
12. Wolf P, Weger W, Patra V, Gruber-Wackernagel A, Byrne SN. Desired response to phototherapy vs photoaggravation in psoriasis: what makes the difference? Exp Dermatol. 2016;25(12):937–944. doi:10.1111/exd.13137
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Home Phototherapy Improves Access to Dermatologic Care: A Novel Stakeholder Alliance to Facilitate Its Implementation
Bawany F, Ryan Wolff J, Ritchlin CT, Tausk F
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1175-1180
Published Date: 2 May 2023
Hepatotoxicity Induced by Adalimumab in Chronic Plaque Psoriasis Patient: A Case Report
Algarzae NK, Alotaibi HM, Alajlan AH, AlSaleh MR, Alsalman AA
International Medical Case Reports Journal 2025, 18:877-881
Published Date: 9 July 2025
Knowledge, Attitude, and Behavior of Photoprotection in Thai Vitiligo Patients
Wongpraparut O, Wannawittayapa T, Wattanasillawat P, Yothachai P, Nuntawisuttiwong N, Silpa-archa N
Clinical, Cosmetic and Investigational Dermatology 2025, 18:3635-3644
Published Date: 28 December 2025
Case Report: Vitiligo and Alopecia Universalis Following Rituximab Therapy in a Patient with Myasthenia Gravis
Alzahrani D, Niaz G, Roblah TM, Al-Osaimi AK, Alsulaimani H
Clinical, Cosmetic and Investigational Dermatology 2026, 19:584164
Published Date: 16 March 2026
Development of Predictive Models for NB-UVB Treatment Efficacy and Safety in Psoriasis
Yu Y, Li B, Wang Y, Qu Z, Wang X, Jiang Y, Zhong X, Chen Y, Huang D, Bi X, Lu J, Ding Y, Gong Y, Gu J, Zhang X, Shi Y
Psoriasis: Targets and Therapy 2026, 16:609637
Published Date: 25 May 2026