Back to Journals » International Journal of Women's Health » Volume 18
Genetically Causal Associations Between Adenomyosis/Endometriosis and Adverse Pregnancy Outcomes - A Two-Sample Mendelian Randomization Study
Authors Wang J, Wang L, Wang X, Ai A, Qiao P
Received 22 September 2025
Accepted for publication 1 January 2026
Published 14 January 2026 Volume 2026:18 569458
DOI https://doi.org/10.2147/IJWH.S569458
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Jingyun Wang,1,* Lu Wang,1,* Xiaohui Wang,1 Ai Ai,1 Ping Qiao2
1Department of Reproductive Medicine, Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China; 2Department of Obstetrics, Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ping Qiao, Email [email protected] Ai Ai, Email [email protected]
Purpose: Observational studies have indicated a potential link between adenomyosis/endometriosis and adverse pregnancy outcomes (APOs), yet the potential relationship remains uncertain.
Patients and Methods: This study investigates whether genetically predicted adenomyosis/endometriosis influences APOs through a two-sample Mendelian randomization (MR) analysis, utilizing summary statistics from genome-wide association studies (GWAS). The primary analytical method employed was the inverse-variance weighted (IVW) approach, alongside supplementary techniques including weighted median, MR Egger regression, and weighted mode. Sensitivity analyses, such as Cochran’s Q test, the MR-Egger intercept test, the MR-PRESSO (Pleiotropy RESidual Sum and Outlier) test, and a leave-one-out analysis, were conducted to ensure result robustness.
Results: Results from the IVW method indicate that endometriosis may pose a risk factor for multiple consecutive miscarriage (OR = 1.07, 95% CI: 1.00– 1.14, P = 0.05). No significant associations were noted between adenomyosis and preterm birth (OR = 0.92, 95% CI: 0.75– 1.11, P = 0.38), birth weight (OR = 1.02, 95% CI: 0.96– 1.10, P = 0.50), or other APOs. The MR-Egger regression suggested no horizontal pleiotropy, while the MR-PRESSO test identified outliers concerning birth weight but did not reveal significant associations. Leave-one-out analysis corroborated the robustness of the findings.
Conclusion: This study provides evidence of a potential relationship between endometriosis and multiple consecutive miscarriage, emphasizing the importance of addressing comorbidities and making informed pregnancy decisions in the presence of endometriosis.
Keywords: endometriosis, adenomyosis, adverse pregnancy outcomes, pregnancy loss, genetic variant, mendelian randomization, causal association
Introduction
Adverse pregnancy outcomes (APOs) encompass a range of complications during pregnancy and childbirth, such as miscarriage, preterm birth, gestational hypertension, preeclampsia, fetal growth restriction, and placental issues like placenta previa or abruption, and stillbirth.1–3 Despite significant medical efforts, the global incidence of APOs remains troublingly high.4 For instance, preterm birth was a major contributor to child mortality in 2016, responsible for 16% of all child deaths and 35% of newborn deaths.5 Miscarriages are also alarmingly common, with an estimated 23 million occurring annually worldwide.6 Low birth weight (LBW), defined as a birth weight below 2500g, affects approximately 18 million newborns each year, often linked to the in-utero nutritional environment.7 Placental dysfunctions, including abruption or previa, are known to complicate pregnancies and childbirth significantly.1 The persistent and increasing prevalence of these APOs underscores the urgent need for deeper investigation into their causes, risk factors, and long-term health consequences for both mother and child.
Among potential risk factors, endometriosis, a chronic condition where endometrial-like tissue grows outside the uterus, has garnered attention.8 This benign proliferative disorder affects an estimated 6% to 10% of women of reproductive age.9,10 Closely related to endometriosis is adenomyosis, an estrogen-dependent uterine pathology characterized by the abnormal presence of endometrial tissue within the myometrium.11–13 Given their shared pathophysiological features, both endometriosis and adenomyosis are hypothesized to negatively impact pregnancy outcomes.3 Observational studies have explored this link with mixed results. For example, one retrospective study involving over 1300 pregnant women with endometriosis found a significantly higher incidence of placenta previa compared to controls, though no significant difference in preterm birth rates was observed.14 Another cohort study focusing on women with polycystic ovary syndrome (PCOS) and endometriosis reported a threefold increased risk of placental abruption in this group compared to PCOS women without endometriosis.15 These findings highlight potential associations, but observational research is inherently susceptible to confounding variables and reverse causality. Therefore, more robust evidence is crucial to definitively establish a causal link between adenomyosis/endometriosis and the risk of developing APOs.
To address this knowledge gap, Mendelian randomization (MR) offers a powerful analytical approach. MR utilizes genetic variants, randomly allocated during meiosis, as instrumental variables (IVs) to infer causality between an exposure and an outcome, analogous to a randomized controlled trial.16 This design minimizes biases from confounding factors and reverse causation that often plague traditional observational studies, thereby strengthening causal inference.17
In this study, we employ a two-sample MR analysis to investigate the potential causal relationships between genetically predicted adenomyosis and endometriosis (as exposures) and a spectrum of common APOs. These outcomes include preterm birth and its related factors, low birth weight, placental abruption, placenta previa, miscarriage (including sporadic and multiple consecutive miscarriages), and stillbirth. Elucidating these causal associations is critical not only for a better understanding of the pathogenesis of APOs in the context of these uterine conditions but also for guiding the development of targeted interventions and personalized management strategies to improve pregnancy outcomes for affected women.
Material and Methods
Study Design
In this study, two-sample MR analyses were employed to investigate the relationship between adenomyosis/endometriosis and APOs. This analysis was based on three key assumptions: 1) Genetic variants were associated with the exposures. 2) Genetic variants were independent of any confounding factors that could affect the exposure-outcome association. 3) Genetic variants were independent of the outcome and were only associated with the outcome through the gene expression of the exposures (Figure 1).18 This study utilized publicly available summary statistics from genome-wide association studies (GWAS) and did not involve the collection of new data from human subjects. According to Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (2023), this study is exempt from ethical review. All original studies included in this analysis obtained relevant ethical approval and participant informed consent. This study adhered to the strengthening the reporting of observational studies in epidemiology using Mendelian randomization (STROBE-MR) checklist.19
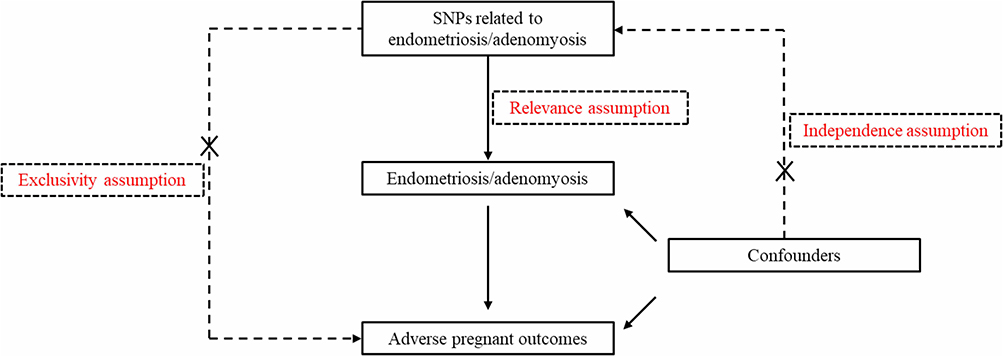 |
Figure 1 The flowchart of the MR analysis in this study. |
Data Source
Endometriosis and adenomyosis were identified as exposures in this study. Gestational duration, preterm birth, birth weight, placental abruption/placenta previa, and miscarriage/stillbirth were outcomes. GWAS data on endometriosis and adenomyosis were obtained from the FinnGen10 consortium (https://www.finngen.fi/en, Finnish ancestry). We obtained GWAS datasets on gestational duration, preterm birth and birthweight from the Early Growth Genetics (EGG) Consortium (http://egg-consortium.org/, European ancestry).20 Data on factors for preterm birth (maternal and child effects) was obtained from a GWAS study based on the MoBa cohort.21 Summary data on placental abruption/placenta previa, miscarriage/stillbirth were obtained from the UK Biobank (European ancestry).22 Datasets on multiple consecutive miscarriage and sporadic miscarriage was obtained from a previous GWAS study involving multi-ancestry populations.23 All databases were accessed between July and November 2024. Specific details on datasets were provided in Supplementary Table 1.
IVs Selection
In MR analysis, IVs serve as genetic proxies for the exposure, allowing for the assessment of genetically causal associations on the outcome. In this study, the included IVs needed to meet the following criteria: 1) single nucleotide polymorphisms (SNPs) that are significantly associated with adenomyosis/endometriosis were chosen at P < 5×10.−824 2) The minor allele frequency (MAF) of the included genetic variants had to be greater than 0.01.25 3) To avoid the impact of linkage disequilibrium (LD) among included genetic variants on the results, SNPs were excluded using the PLINK clumping method (r2 > 0.001 and clump window < 10,000 kb).26 4) The F statistic was used to identify if there is a weak IV bias, calculated using the formula: R2 × (N − 2) / (1 − R2), where R2 is the proportion of variance in the exposure explained by the IV (R2 =Σ [2 × (1 - MAF) ×MAF × β/ (SE2× N)], SE and β are the standard error and beta coefficient of the effect size), and N is the sample size. Each selected SNP’s F statistic must be greater than 10.27 5) For IVs absent from the outcome dataset, proxies with an R2 > 0.8 were used as substitute variables to maintain the robustness and efficiency of the MR study.28
Mendelian Randomization
All MR analyses were performed using the TwoSampleMR package in R software (version 4.0.5).29 The inverse variance-weighted (IVW) method, which calculates the weighted average of effect sizes using the inverse variance of each SNP as the weight, was used as the primary analytical approach to estimate the genetically predicted causal associations between adenomyosis/endometriosis and APOs.30 The results are represented by the odds ratio (OR) and 95% confidence interval (CI). Additional analytical methods included MR-Egger,31 weighted median model,32 and weighted mode methods.33 The MR-Egger accounts for the presence of an intercept term, allowing it to provide accurate estimates of potential causal effects even in the presence of pleiotropic bias.31 The weighted median method assumes that at least half of the instrumental variables are valid and uses this assumption to analyze the causal association between exposure and outcome.32 The weighted mode approach identifies the most common effect size estimate in scenarios where there is variability or differences among the IVs.33
Sensitivity Analysis
Sensitivity analyses were performed to verify the robustness of the MR estimates.34 In the IVW method, heterogeneity was assessed using Cochran’s Q test, a P < 0.05 indicated the presence of heterogeneity.35 Horizontal pleiotropy was assessed using the MR-Egger intercept test and the MR Pleiotropy Residual Sum and Outlier (MR-PRESSO) test, when the intercept term in MR-Egger regression is close to zero or statistically nonsignificant (P > 0.05), it suggests the absence of pleiotropy, similarly, a P > 0.05 in the MR-PRESSO test suggested the absence of pleiotropy.36,37 In addition, the MR-PRESSO method was used to identify and correct for the potential impact of outlier IVs that might indicate horizontal pleiotropy, by systematically excluding aberrant SNPs. The MR analyses were repeated to check whether the outliers influenced the estimated causal associations after eliminating the outliers. A leave-one-out analysis was done to assess the impact of each individual SNP on the overall outcomes.34 Similarly, all sensitivity analyses were performed using the TwoSampleMR package in R software (version 4.0.5).29
Results
IVs Selection
For the MR analysis with adenomyosis as the exposure, 28 IVs were selected with a mean F of 62.29, a min F of 29.98, and max F of 189.81. For the analysis with endometriosis as the exposure, 31 IVs were selected, the mean F value was 24.88, the min F was 20.86, and the max F was 40.63. All outcomes matched the summary data in this study when adenomyosis was exposure except for multiple consecutive miscarriage (1 unmatched IV), and gestational duration (5 unmatched IVs). The numbers of SNPs for outcomes including preterm birth, birth weight, placental abruption/placenta previa, miscarriage/stillbirth, multiple consecutive miscarriage, and gestational duration that did not match the summary data were 3, 3, 1, 1, 1, and 3 when endometriosis was identified as the exposure. Details on the dataset in this study were listed in Supplementary file 1.
Mendelian Randomization
Results of the IVW method showed that endometriosis may be a risk factor for multiple consecutive miscarriage (OR = 1.07, 95% CI: 1.00–1.14, P = 0.05) (Table 1). Non-significant results were yielded to the IVW estimator for endometriosis and preterm birth (OR = 0.92, 95% CI: 0.75–1.11, P = 0.38), birth weight (OR = 1.02, 95% CI: 0.96–1.10, P = 0.50), placental abruption/placenta previa (OR = 0.93, 95% CI: 0.66–1.30, P = 0.66), miscarriage/stillbirth (OR = 0.99, 95% CI: 0.83–1.18, P = 0.91), and gestational duration (OR = 1.00, 95% CI: 0.98–1.02, P = 0.99). Adenomyosis was not significantly related to any of the APOs. The scatter plot for effect sizes of SNPs for adenomyosis/endometriosis with APOs were shown in Figure 2A and Supplementary Figure 1. The forest plot did not demonstrate a potential effect adenomyosis/endometriosis of on APOs, as no statistically significant associations were observed except for endometriosis and multiple consecutive miscarriage (Figure 2B and Supplementary Figure 2). The results from the MR-Egger, weighted median, and weighted mode methods were consistent with those of the IVW method (Table 1).
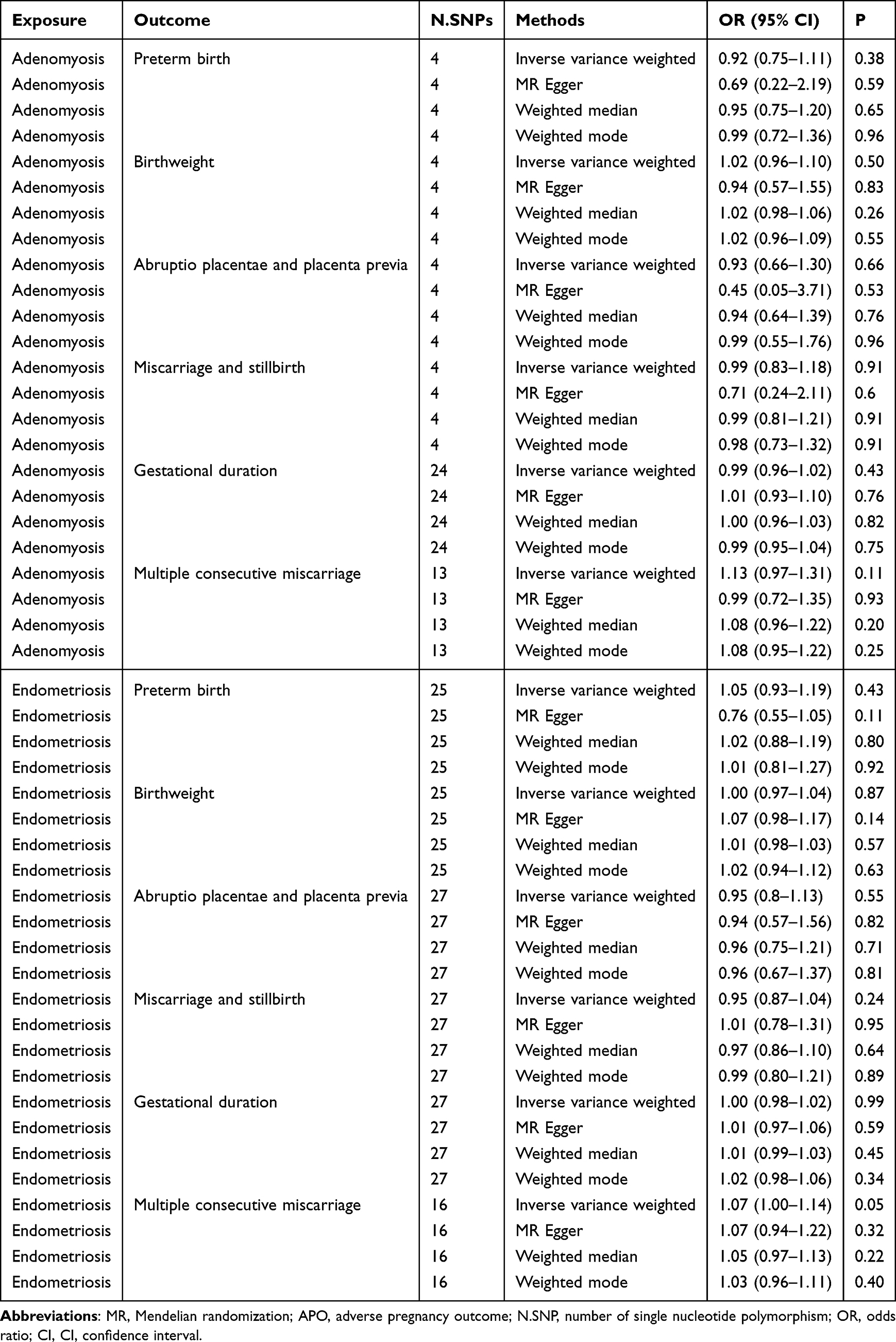 |
Table 1 MR Analysis Investigating the Causal Associations Between Adenomyosis/Endometriosis and APOs |
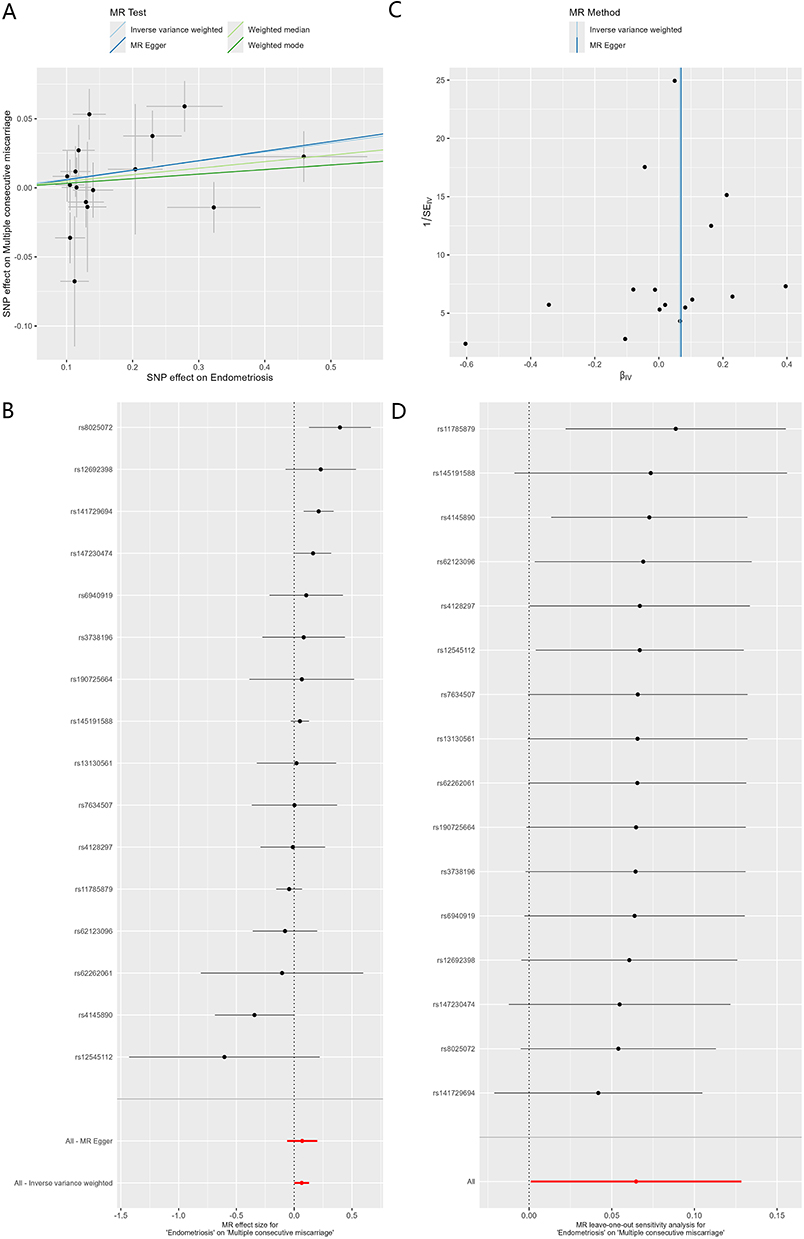 |
Figure 2 Causal association between endometriosis multiple consecutive miscarriage. (A) Scatter plot. (B) Forest plot. (C) Funnel plot. (D) Leave-one-out plot. |
Sensitivity Analysis
The MR-Egger regression analysis indicated the absence of horizontal pleiotropy (Figure 2C, Supplementary Figure 3 and Table 2). The MR-PRESSO results suggested that for birth weight as the outcome, there were 2 outliers in adenomyosis and 7 outliers in endometriosis; for gestational duration as the outcome, there were 3 outliers in adenomyosis and 2 outliers in endometriosis; for multiple consecutive miscarriage as the outcome, there were 15 outliers in adenomyosis and 14 outliers in endometriosis. After removing these outliers, there was still no statistically significant association except for the estimate of endometriosis and multiple consecutive miscarriage (Supplementary Table 2). In addition, leave-one-out analysis indicated relatively robust MR estimates (Figure 2D and Supplementary Figure 4).
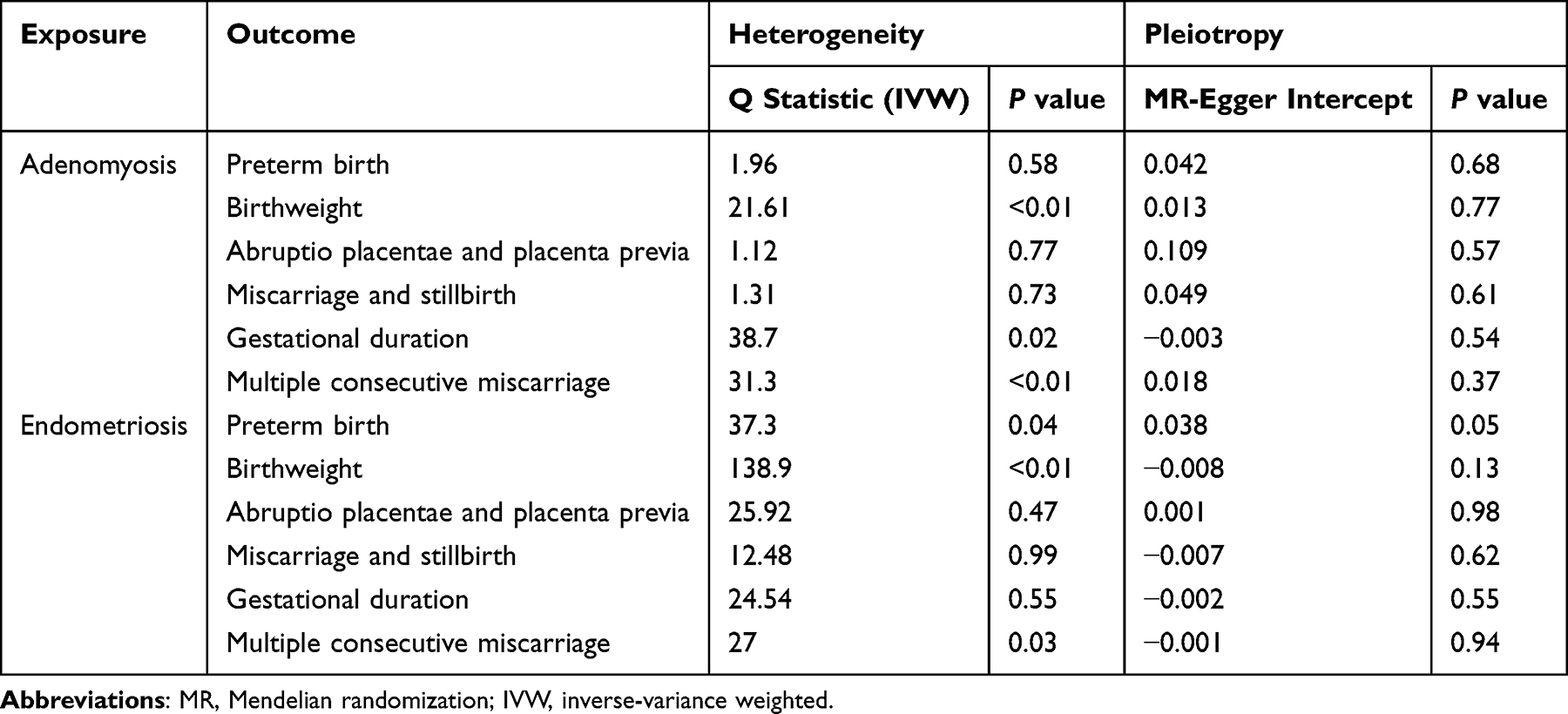 |
Table 2 Results on Sensitivity Analysis |
Discussion
This two-sample Mendelian randomization study found limited evidence for a potential causal relationship between genetic predisposition to adenomyosis or endometriosis and most common APOs investigated, including preterm birth, abnormal birth weight, placental issues, and gestational diabetes. However, a potential weak causal link between endometriosis and an increased risk of multiple consecutive miscarriages was suggested. Robustness was supported by sensitivity analyses (MR-PRESSO, MR-Egger intercept, Cochran’s Q), which indicated no significant heterogeneity or horizontal pleiotropy, suggesting IVs likely act through adenomyosis/endometriosis.
The observed association between endometriosis and multiple consecutive miscarriages aligns with some existing observational literature.38,39 A recent nationwide cohort study demonstrated a significant association between endometriosis and an increased risk of recurrent pregnancy loss.38 Similarly, Vercellini et al reported lower pregnancy and live birth rates, alongside an increased risk of miscarriage, in patients with endometriosis.39 Mechanistically, successful pregnancy maintenance relies on local immune tolerance and appropriate uterine vascular remodeling, partly regulated by decidual natural killer (NK) cells. Dysfunctional NK cells have been implicated in miscarriage.40,41 Notably, CD200S, a molecule linked to fetal rejection and expressed by endometrial NK cells, is found at increased frequencies in endometriosis, potentially impairing embryo survival.42 While our MR study provides some genetic support for a potential causal link between endometriosis and multiple consecutive miscarriages, further research is essential to elucidate the precise underlying mechanisms.
Our findings did not support a significant causal association between genetically predicted endometriosis or adenomyosis and most other APOs, such as placenta previa, preterm birth, and low birth weight, which contrast with some observational studies. For instance, retrospective and cohort studies have reported positive associations between endometriosis and placenta previa,14 or increased risks of preterm birth43 and low birth weight in women with adenomyosis.44 These discrepancies between MR findings and observational studies could arise from several factors. Observational studies are often susceptible to unmeasured or residual confounding factors (eg, educational level, socioeconomic status, lifestyle) and reverse causation, which MR analysis aims to mitigate.45 Furthermore, the broad categorization of endometriosis and adenomyosis without considering specific subtypes or disease severity in many studies, including our GWAS-based exposure, might obscure subtype-specific effects.
It is also crucial to consider the impact of comorbid gynecological conditions that frequently coexist with adenomyosis or endometriosis, such as uterine fibroids, PCOS, and uterine malformations, which can independently influence pregnancy outcomes.15,46 For example, uterine fibroids can enlarge during pregnancy, potentially leading to fetal growth restriction and preterm labor.47 The co-occurrence of PCOS and endometriosis may represent a distinct phenotype with specific implications for pregnancy,48 possibly linked through complex pathways like kisspeptin receptor signaling, although its role in endometriosis pathogenesis is less established than in PCOS.49 The GWAS datasets used in our study might also include individuals with unrecognized coexisting adenomyosis and endometriosis, potentially diluting specific effects, especially given that awareness and diagnostic accuracy for adenomyosis have improved more recently.39 Additionally, variations in diagnostic expertise could lead to underdiagnosis, further complicating the interpretation of broad population-based genetic associations.
The heterogeneity within endometriosis and adenomyosis likely plays a significant role. An observational study by Fernando et al indicated an increased risk of preterm birth specifically among women with ovarian endometrioma,50 while Benaglia et al reported no such increased risk in a similar subgroup undergoing assisted reproductive technology.51 These contrasting findings highlight the need for future MR studies to, where possible, utilize GWAS data for distinct clinical or pathological subtypes of endometriosis and adenomyosis to explore more nuanced causal relationships with APOs. Clinically, managing pregnancies in women with endometriosis or adenomyosis necessitates a personalized, multidisciplinary approach, involving obstetricians experienced in high-risk pregnancies, to optimize maternal and fetal well-being.
Regarding adenomyosis, our study did not observe significant causal associations with APOs. Several factors might contribute to this null finding. First, the genetic instruments for adenomyosis might have lower explanatory power compared to endometriosis due to smaller sample sizes in the original GWAS or greater phenotypic heterogeneity. Second, adenomyosis is often underdiagnosed or misdiagnosed as fibroids in general populations,52 which could introduce classification bias in the source data. Future studies with larger, more phenotypically refined cohorts are needed to validate these findings.
Our study possesses several strengths, including the use of an MR design to minimize confounding and reverse causality, rigorous IV selection criteria, and the utilization of large-scale, recent GWAS data, enhancing the reliability of our estimates. However, certain limitations must be acknowledged. MR analysis cannot account for all genetic or epigenetic mechanisms (eg, DNA methylation, RNA editing) that might influence disease. The reliance on GWAS data predominantly from European populations may limit the generalizability of our findings to other ethnicities, introducing potential racial bias. While a small number of SNPs did not directly match in the outcome datasets and were proxied, this is unlikely to have substantially affected the overall results.
Conclusion
In conclusion, our two-sample MR study revealed that endometriosis may be a risk factor for multiple consecutive miscarriage. However, no evidence of a causal association was observed for adenomyosis and the studied APOs. Clinical management should consider comorbidities with adenomyosis/endometriosis, and decisions related to pregnancy should be influenced by the existence of endometriosis. Further research is needed on the association of different subtypes of adenomyosis/endometriosis with APOs.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Acknowledgments
We thank all of the project participants for their contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Shanghai Pudong Science and Technology and Economic Commission Project PKJ2022-Y16. Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, Clinical research project 2023B02. Shanghai Municipal Health Commission General Project 202340111.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Tindal K, Cousins FL, Ellery SJ, et al. Investigating menstruation and adverse pregnancy outcomes: oxymoron or new frontier? A narrative review. J Clin Med. 2024;13(15):4430. doi:10.3390/jcm13154430
2. Li Q, Li Z, Li T, Wang Y, Feng J, Lu C. Efficacy and safety of soluble guanylate cyclase stimulators in patients with heart failure: a systematic review and meta-analysis. Pharmazie. 2021;76(10):488–10. doi:10.1691/ph.2021.1599
3. Lim HJ, Sun J, Min B, et al. Endometriosis and adverse pregnancy outcomes: a nationwide population-based study. J Clin Med. 2023;12(16):5392. doi:10.3390/jcm12165392
4. Li C, Liu C, Li N. Causal associations between gut microbiota and adverse pregnancy outcomes: a two-sample mendelian randomization study. Front Microbiol. 2022;13:1059281. doi:10.3389/fmicb.2022.1059281
5. Chadha A, Moore S, Kildea S, Gao Y. Health economic evaluations of programs reducing preterm birth: a scoping review. Int J Nurs Stud Adv. 2024;7:100228. doi:10.1016/j.ijnsa.2024.100228
6. Quenby S, Gallos ID, Dhillon-Smith RK, et al. Miscarriage matters: the epidemiological, physical, psychological, and economic costs of early pregnancy loss. Lancet. 2021;397(10285):1658–1667. doi:10.1016/S0140-6736(21)00682-6
7. Fang K, He Y, Mu M, Liu K. Maternal vitamin D deficiency during pregnancy and low birth weight: a systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2021;34(7):1167–1173. doi:10.1080/14767058.2019.1623780
8. Greene AD, Lang SA, Kendziorski JA, Sroga-Rios JM, Herzog TJ, Burns KA. Endometriosis: where are we and where are we going? Reproduction. 2016;152(3):R63–78. doi:10.1530/REP-16-0052
9. Giudice LC. Clinical practice. endometriosis. N Engl J Med. 2010;362(25):2389–2398. doi:10.1056/NEJMcp1000274
10. Hwang H, Chung YJ, Lee SR, et al. Clinical evaluation and management of endometriosis: guideline for Korean patients from Korean society of endometriosis. Obstet Gynecol Sci. 2018;61(5):553–564. doi:10.5468/ogs.2018.61.5.553
11. Bird CC, McElin TW, Manalo-Estrella P. The elusive adenomyosis of the uterus--revisited. Am J Obstet Gynecol. 1972;112(5):583–593. doi:10.1016/0002-9378(72)90781-8
12. García-Solares J, Donnez J, Donnez O, Dolmans MM. Pathogenesis of uterine adenomyosis: invagination or metaplasia? Fertil Steril. 2018;109(3):371–379. doi:10.1016/j.fertnstert.2017.12.030
13. Zhai J, Vannuccini S, Petraglia F, Giudice LC. Adenomyosis: mechanisms and pathogenesis. Semin Reprod Med. 2020;38(2–03):129–143. doi:10.1055/s-0040-1716687
14. Dai QH, Cai HR, Chen AE. Study on the correlation between endometriosis and adverse pregnancy outcomes. Eur J Obstet Gynecol Reprod Biol. 2024;299:208–212. doi:10.1016/j.ejogrb.2024.06.016
15. Ismail S, Majdell C, Badgheish A, Baghlaf H, Dahan MH. Pregnancy, delivery, and neonatal outcomes among women with PCOS and endometriosis: a population database cohort. Arch Gynecol Obstet. 2024;310(2):1235–1243. doi:10.1007/s00404-024-07589-w
16. Lawlor DA, Harbord RM, Sterne JAC, Timpson N, Davey Smith G. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med. 2008;27(8):1133–1163.
17. Burgess S, Dudbridge F, Thompson SG. Combining information on multiple instrumental variables in mendelian randomization: comparison of allele score and summarized data methods. Stat Med. 2016;35(11):1880–1906. doi:10.1002/sim.6835
18. Burgess S, Davey Smith G, Davies NM, et al. Guidelines for performing mendelian randomization investigations: update for summer 2023. Wellcome Open Res. 2019;4:186. doi:10.12688/wellcomeopenres.15555.1
19. Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the reporting of observational studies in epidemiology using mendelian randomization: the STROBE-MR statement. JAMA. 2021;326(16):1614–1621.
20. Liu X, Helenius D, Skotte L, et al. Variants in the fetal genome near pro-inflammatory cytokine genes on 2q13 associate with gestational duration. Nat Commun. 2019;10(1):3927.
21. Juodakis J, Ytterberg K, Flatley C, Sole-Navais P, Jacobsson B. Time-varying effects are common in genetic control of gestational duration. Hum Mol Genet. 2023;32(14):2399–2407. doi:10.1093/hmg/ddad086
22. Sudlow C, Gallacher J, Allen N, et al. UK biobank: an open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015;12(3):e1001779. doi:10.1371/journal.pmed.1001779
23. Laisk T, Soares ALG, Ferreira T, et al. The genetic architecture of sporadic and multiple consecutive miscarriage. Nat Commun. 2020;11(1):5980. doi:10.1038/s41467-020-19742-5
24. Zhu X, Cheng D, Ruan K, Shen M, Ye Y. Causal relationships between type 2 diabetes, glycemic traits and keratoconus. Front Med. 2023;10:1264061.
25. Long Y, Tang L, Zhou Y, Zhao S, Zhu H. Causal relationship between gut microbiota and cancers: a two-sample mendelian randomisation study. BMC Med. 2023;21(1):66. doi:10.1186/s12916-023-02761-6
26. Abecasis GR, Altshuler D, Auton A, et al. A map of human genome variation from population-scale sequencing. Nature. 2010;467(7319):1061–1073.
27. Burgess S, Thompson SG. Avoiding bias from weak instruments in mendelian randomization studies. Int J Epidemiol. 2011;40(3):755–764.
28. Deng MG, Liu F, Liang Y, Wang K, Nie JQ, Liu J. Association between frailty and depression: a bidirectional mendelian randomization study. Sci Adv. 2023;9(38):eadi3902.
29. Hemani G, Zheng J, Elsworth B, et al. The MR-Base platform supports systematic causal inference across the human phenome. Elife. 2018;7:e34408.
30. Burgess S, Butterworth A, Thompson SG. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol. 2013;37(7):658–665. doi:10.1002/gepi.21758
31. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
32. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
33. Hartwig FP, Davey Smith G, Bowden J. Robust inference in summary data mendelian randomization via the zero modal pleiotropy assumption. Int J Epidemiol. 2017;46(6):1985–1998. doi:10.1093/ije/dyx102
34. Burgess S, Bowden J, Fall T, Ingelsson E, Thompson SG. Sensitivity analyses for robust causal inference from mendelian randomization analyses with multiple genetic variants. Epidemiology. 2017;28(1):30–42. doi:10.1097/EDE.0000000000000559
35. Greco MF, Minelli C, Sheehan NA, Thompson JR. Detecting pleiotropy in mendelian randomisation studies with summary data and a continuous outcome. Stat Med. 2015;34(21):2926–2940. doi:10.1002/sim.6522
36. Burgess S, Thompson SG. Interpreting findings from mendelian randomization using the MR-Egger method. Eur J Epidemiol. 2017;32(5):377–389. doi:10.1007/s10654-017-0255-x
37. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
38. Boje AD, Egerup P, Westergaard D, et al. Endometriosis is associated with pregnancy loss: a nationwide historical cohort study. Fertil Steril. 2023;119(5):826–835. doi:10.1016/j.fertnstert.2022.12.042
39. Vercellini P, Viganò P, Bandini V, Buggio L, Berlanda N, Somigliana E. Association of endometriosis and adenomyosis with pregnancy and infertility. Fertil Steril. 2023;119(5):727–740. doi:10.1016/j.fertnstert.2023.03.018
40. Zhang X, Wei H. Role of decidual natural killer cells in human pregnancy and related pregnancy complications. Front Immunol. 2021;12:728291. doi:10.3389/fimmu.2021.728291
41. Yang S, Wang H, Li D, Li M. An estrogen-NK Cells regulatory axis in endometriosis, related infertility, and miscarriage. Int J Mol Sci. 2024;25(6):3362.
42. Clark DA, Reihani A, Arredondo JL, Ask K, Foster WG. CD200S-positive granulated lymphoid cells in endometrium appear to be CD56-positive uterine NK cells. J Reprod Immunol. 2022;150:103477. doi:10.1016/j.jri.2022.103477
43. Glavind MT, Forman A, Arendt LH, Nielsen K, Henriksen TB. Endometriosis and pregnancy complications: a Danish cohort study. Fertil Steril. 2017;107(1):160–166. doi:10.1016/j.fertnstert.2016.09.020
44. Nirgianakis K, Kalaitzopoulos DR, Schwartz ASK, et al. Fertility, pregnancy and neonatal outcomes of patients with adenomyosis: a systematic review and meta-analysis. Reprod Biomed Online. 2021;42(1):185–206. doi:10.1016/j.rbmo.2020.09.023
45. Davies NM, Holmes MV, Davey Smith G. Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ. 2018;362:k601.
46. Zhu T, Zhan G, Shang Z, Ying Z. Causal relationship between systemic lupus erythematosus and adverse pregnancy outcomes: a two-sample mendelian randomized study. Heliyon. 2024;10(15):e35401. doi:10.1016/j.heliyon.2024.e35401
47. Babunashvili EL, Son DY, Buyanova SN, et al. Outcomes of laparotomic myomectomy during pregnancy for symptomatic uterine fibroids: a prospective cohort study. J Clin Med. 2023;12(19):6406. doi:10.3390/jcm12196406
48. Crespi B. Variation among human populations in endometriosis and PCOS A test of the inverse comorbidity model. Evol Med Public Health. 2021;9(1):295–310. doi:10.1093/emph/eoab029
49. Salmeri N, Viganò P, Cavoretto P, Marci R, Candiani M. The kisspeptin system in and beyond reproduction: exploring intricate pathways and potential links between endometriosis and polycystic ovary syndrome. Rev Endocr Metab Disord. 2024;25(2):239–257. doi:10.1007/s11154-023-09826-0
50. Fernando S, Breheny S, Jaques AM, Halliday JL, Baker G, Healy D. Preterm birth, ovarian endometriomata, and assisted reproduction technologies. Fertil Steril. 2009;91(2):325–330. doi:10.1016/j.fertnstert.2008.01.096
51. Benaglia L, Bermejo A, Somigliana E, et al. Pregnancy outcome in women with endometriomas achieving pregnancy through IVF. Hum Reprod. 2012;27(6):1663–1667. doi:10.1093/humrep/des054
52. Santulli P, Vannuccini S, Bourdon M, Chapron C, Petraglia F. Adenomyosis: the missed disease. Reprod Biomed Online. 2025;50(4):104837. doi:10.1016/j.rbmo.2025.104837
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Associations Between Mean Platelet Volume and Risk of Deep Vein Thrombosis: A Mendelian Randomization Study and a Retrospective Study
Li J, Liang Y
International Journal of General Medicine 2023, 16:515-524
Published Date: 8 February 2023
IFN-γ, SCF, MIP1b and IL-16 Were Associated with Risk of Diabetic Nephropathy: A Mendelian Randomization Study
An L, Ren X, Pan Y, Gao W, Ren L, Wang J, Wang Y
Diabetes, Metabolic Syndrome and Obesity 2024, 17:851-856
Published Date: 22 February 2024
Causal Relationship Between Endometriosis and Pelvic Inflammatory Diseases: Mendelian Randomization Study
Liu K, Liu X, Cao T, Cui X, Sun P, Zhang L, Wu X
International Journal of Women's Health 2024, 16:727-735
Published Date: 24 April 2024
The Effect of Circulating Inflammatory Proteins on Endometriosis: A Mendelian Randomization Study
Wei Y, Zhao X, Li L
ImmunoTargets and Therapy 2024, 13:585-593
Published Date: 1 November 2024
Endometriosis Severity and Risk of Preeclampsia: A Combined Mendelian Randomization and Observational Study
Zu Y, Xie Y, Zhang H, Chen L, Yan S, Wang Z, Fang Z, Lin S, Yan J
International Journal of Women's Health 2025, 17:923-935
Published Date: 27 March 2025