")
Back to Journals » International Journal of General Medicine » Volume 16
Associations Between Mean Platelet Volume and Risk of Deep Vein Thrombosis: A Mendelian Randomization Study and a Retrospective Study
Received 11 December 2022
Accepted for publication 18 January 2023
Published 8 February 2023 Volume 2023:16 Pages 515—524
DOI https://doi.org/10.2147/IJGM.S401059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jianhong Li,1 Yingna Liang2
1Department of Radiology, Foshan Hospital of Traditional Chinese Medicine, Foshan, People’s Republic of China; 2Department of Gynaecology and Obstetrics, Guangzhou Baiyun First People’s Hospital (Baiyun District Maternal and Child Health Hospital), Guangzhou, Guangdong Province, People’s Republic of China
Correspondence: Yingna Liang, Department of Gynaecology and Obstetrics, Guangzhou Baiyun First People’s Hospital (Baiyun District Maternal and Child Health Hospital), Guangzhou, Guangdong Province, People’s Republic of China, Email [email protected]
Objective: In this study, it was intended to explore the causal association between mean platelet volume (MPV) and risk of deep vein thrombosis (DVT) using a two-sample Mendelian randomization (MR) analysis and a retrospective study.
Methods: This study applied two-sample MR analysis to estimate the causal association between MPV and risk of DVT. Twenty-one single nucleotide polymorphisms (SNPs) were selected as genetic variants from two independent consortiums cohorts (p-value < 5× 10− 8, linkage disequilibrium r2< 0.1). Inverse variance weighted (IVW), MR-egger method and weighted median were performed. A retrospective study was also conducted to verify the associations identified from the MR study.
Results: The MR analysis demonstrated that genetically predicted higher MPV was associated with significantly lower risk of DVT (OR 0.982, 95% CI = 0.967– 0.998, P = 0.023), with the consistent result in weighted median and MR-Egger. There was no directional horizontal pleiotropy in the method of MR-Egger regression (intercept=2.9e-04, P = 0.194). There was no single SNP was found to strongly drive the combined causal effect in the leave-one-out sensitivity analysis. Additionally, the similar result was observed in the retrospective study.
Conclusion: This study suggested that MPV was negatively associated with the risk of DVT. More basic researches are needed in the future to explore its specific mechanism.
Keywords: mean platelet volume, deep vein thrombosis, Mendelian randomization, causal association
Introduction
Deep venous thrombosis (DVT) is a substantial cause with severe complications in nearly all hospitalized patients, which increases the potential incidence both for morbidity and mortality. While a lot of efforts are performed in the DVT prevention, delay diagnosis of DVT still contributed to a high risk of pulmonary embolism and post-thrombotic syndrome, seriously affecting the quality of life of patients and bringing a heavy global health burden. As a result, timely and accurate prediction of DVT is of significant importance.1,2 D-dimer is the most common clinical indicator to diagnosis or rule out the DVT events in clinical practice.3 Due to the lack of specificity,4 the diagnostic value of D-dimer is not clinically recognized, thus to identify more effective diagnosis marker has become imperative.
Platelet plays an essential role in the process of thrombosis formation.5 As a common marker to measure the size of platelet in clinical practice, mean platelet volume (MPV) is expected to be a potential predictor of the diagnosis of DVT, while there is still controversy on the effect of MPV on DVT.6 Higher MPV was observed with increased risk of DVT in several retrospective studies. However, increasing researches reported different opinions on the effect of MPV towards the risk of DVT, indicating that the relationship has not been systematically examined and further studies are needed to explore the casual relationship between MPV and risk of DVT.7,8 Considering that most previous reports belonging to traditional observation research, the result was inevitably disturbed by confounding factors and reverse causation.11
As a new approach, Mendelian randomization (MR) has been widely performed to the casual inference, while it remained blank about MPV on the risk of DVT.
In the present study, we aimed to investigate a potentially causal association between MPV and risk of DVT by using MR as well as a retrospective study to verify the result.
Materials and Methods
Study Design
A two-sample MR analysis was performed to investigate the causal association between MPV and risk of DVT, in which the summary data of genetic variants associated with MPV and genetic variants associated with DVT were obtained from two independent consortiums cohorts.12 The analysis was based on three hypotheses.13 Firstly, to serve as instruments, genetic variants are robustly related to MPV. Secondly, genetic variants should be strictly independent of confounding factors between DVT and MPV. At last, genetic variants must affect the risk of DVT only through the way of MPV. The study complied with the Declaration of Helsinki.
Summary Statistics for MPV
As shown in Table 1, the publicly available summary data on MPV were extracted from the study conducted by Gieger et al in 2011.14 The study included 66,867 participants and all of them were Europeans. Single nucleotide polymorphism (SNP). To avoid the bias caused by strong linkage disequilibrium (LD), the selection threshold was set as p-value <5×10−8, linkage disequilibrium r2<0.1, as previous study.15 Twenty-eight SNPs (rs10076782, rs10512627, rs10813766, rs10876550, rs10914144, rs11601356, rs11734132, rs11789898, rs1354034, rs1558324, rs1668871, rs1790931, rs2015599, rs2227831, rs2950390, rs3000073, rs329003, rs342293, rs4305276, rs4521516, rs4812048, rs4814776, rs649729, rs7075195, rs7317038, rs7961894, rs8076739, rs997482) closely associated with MPV were identified from the dataset.
 |
Table 1 Details of Studies and Datasets Used for MR Analysis |
Summary Statistics for DVT
The summary data on DVT were obtained from MRC Integrative Epidemiology Unit Consortium (MRC-IEU) in 2018, which was included in UK Biobank (http://www.bristol.ac.uk/integrative-epidemiolog) with 462933 participants (18818 DVT patients and 444115 controls). Seven SNPs were not found in the MRC-IEU Consortium (rs10512627, rs11734132, rs1790931, rs342293, rs4305276, rs4521516, rs649729). Finally, the rest 21 SNPs were included, explaining 0.011% of the variations in the final analysis. The F statistic, an essential tool to assess the weak instrument bias, was 134 and well over 10.16 It was generally believed that the result was not affected from the bias caused by weak instruments. For the heterogeneity test among the 21 SNPs, there was no heterogeneity for causal inference of MPV on the risk of DVT (Q statistic, 29.95; P > 0.05). At last, 21 independent SNPs associated with DVT were included as instrumental variables for the final MR analysis. The detailed information, effect allele (EA), effect allele frequency (EAF), effect sizes (β), standard errors (SE) and P values were recorded and shown in Table 2.
 |
Table 2 Characteristics of the SNPs Associated with Mean Platelet Volume and Risk of Deep Vein Thrombosis |
Statistical Analyses
Three methods, inverse variance weighted (IVW), weighted median and MR-egger method were the classical method of MR analysis and performed to explore the causal association between MPV and risk of DVT.12,17 The result was presented as Results of MR of were expressed as odds ratios (OR) and confidence interval (CI) and visualized as forest plot and scatter plot. Sensitivity analysis was evaluated by pleiotropy test from the method of Egger regression and the leaving-one-out method. The MR analysis was performed by using the R (version 3.4.2) package “TwoSampleMR” (version 0.3.4).18 The P value less than 0.05 was considered as differences with statistically significant.
Retrospective Study
A retrospective cohort study was conducted at the adult patients with newly confirmed diagnosis of DVT from January 2020 to December 2021. The retrospective study was approved by the Ethics Committee of Foshan Hospital of Traditional Chinese Medicine and informed consent has been obtained from all the included participants. In the present study, the participants with the following were excluded: (1) acute infections; (2) already receiving anticoagulation or anti-platelet treatment; (3) Lacking of MPV value. The participants were divided into the DVT group and the non-DVT group. The diagnosis of DVT was based on the screening through color Doppler ultrasonography (iU 22, Philips, The Netherlands). The following variables were collected, such as age, sex, body mass index, related comorbidities, smoking status and laboratory examination. Continuous variables were represented as the mean ± standard deviation and categorical variables were expressed as counts (percentages). Comparison of quantitative variables was performed by using Student’s t-test or Mann–Whitney U-test while the Chi-squared Test was utilized in categorical variables. Threshold probability value of P < 0.05 was used in this study.
Results
Effect of MPV on the Risk of DVT
As shown in Table 3, the present two-sample MR analysis demonstrated that genetically predicted higher MPV was associated with significantly lower risk of DVT (OR 0.982, 95% CI = 0.967–0.998, P = 0.023). In term of orientation and magnitude, there was the consistent result observed in the method of the weighted median and MR-Egger. Each single causal estimate from each SNP and the 95% CI are demonstrated in Figure 1 while the combined causal effect of all the included 21 SNPs using three different methods was also presented. Three SNPs (rs1354034, rs8076739 and rs7075195) showed clear negative associations between MPV and the risk of DVT for the causal effect. Figure 2 illustrates the regression slops of causal effect between MPV and risk of DVT.
 |
Table 3 Mendelian Randomization Estimates of the Associations Between Mean Platelet Volume and Risk of Deep Vein Thrombosis |
 |
Figure 1 Forest plot of single nucleotide polymorphisms (SNPs) associated with MPV and risk of DVT. Each black point represented the MR estimates for treatment of MPV on risk of DVT. Red points showing the overall causal effect including all SNPs using three different methods (IVW method, weighted median method and MR‐Egger method). The horizontal lines represent 95% confidence intervals of the MR estimates. |
 |
Figure 2 Scatter plot of SNPs associated with MPV and the risk of DVT. The plot relating the effect sizes of the SNP-MPV association (x-axis, SD) and the SNP-DVT associations (y-axis, log (OR)) with 95% confidence intervals. The regression slopes of the lines correspond to causal estimates using three MR methods including the IVW approach, Weighted median and MR‐Egger method. |
Sensitivity Analysis
Little evidence was observed with directional horizontal pleiotropy in the method of MR-Egger regression, in which the P value was larger and suggested null effects (intercept=2.9e-04, P = 0.194). As shown in Figure 3, no single SNP was found to strongly drive the combined causal effect of MPV on the risk of DVT in the leave-one-out sensitivity analysis.
 |
Figure 3 Leave-one-out (LOO) sensitivity analysis of SNPs associated with MPV and risk of DVT. Each black point represents the effect size(β) excluding one SNP estimated by the IVW method. The red point presented the MR estimate including all resting SNPs. The line represents 95% confidence interval of MR estimates. The leave-one-out analysis shows no single SNP was strongly or reversely driving the overall effect of MPV on the risk of DVT. |
Replication Study
There were 343 participants in this study, among which the mean age was 77.2±9.0 years while about one-third of the patients are male. Forty-eight patients were diagnosed with DVT, and the incidence of was 14.0%. Compared with the non-DVT group, higher body mass index was observed in the DVT group (P < 0.05). There were no significant differences with regard to age, sex, smoking status, major comorbidities. For laboratory finding, the mean level of MPV was 12.0±2.6 fL while the lower level of MPV was significantly associated with patients with DVT. The other laboratory result failed to reach a significant association. The detailed information is presented in Table 4.
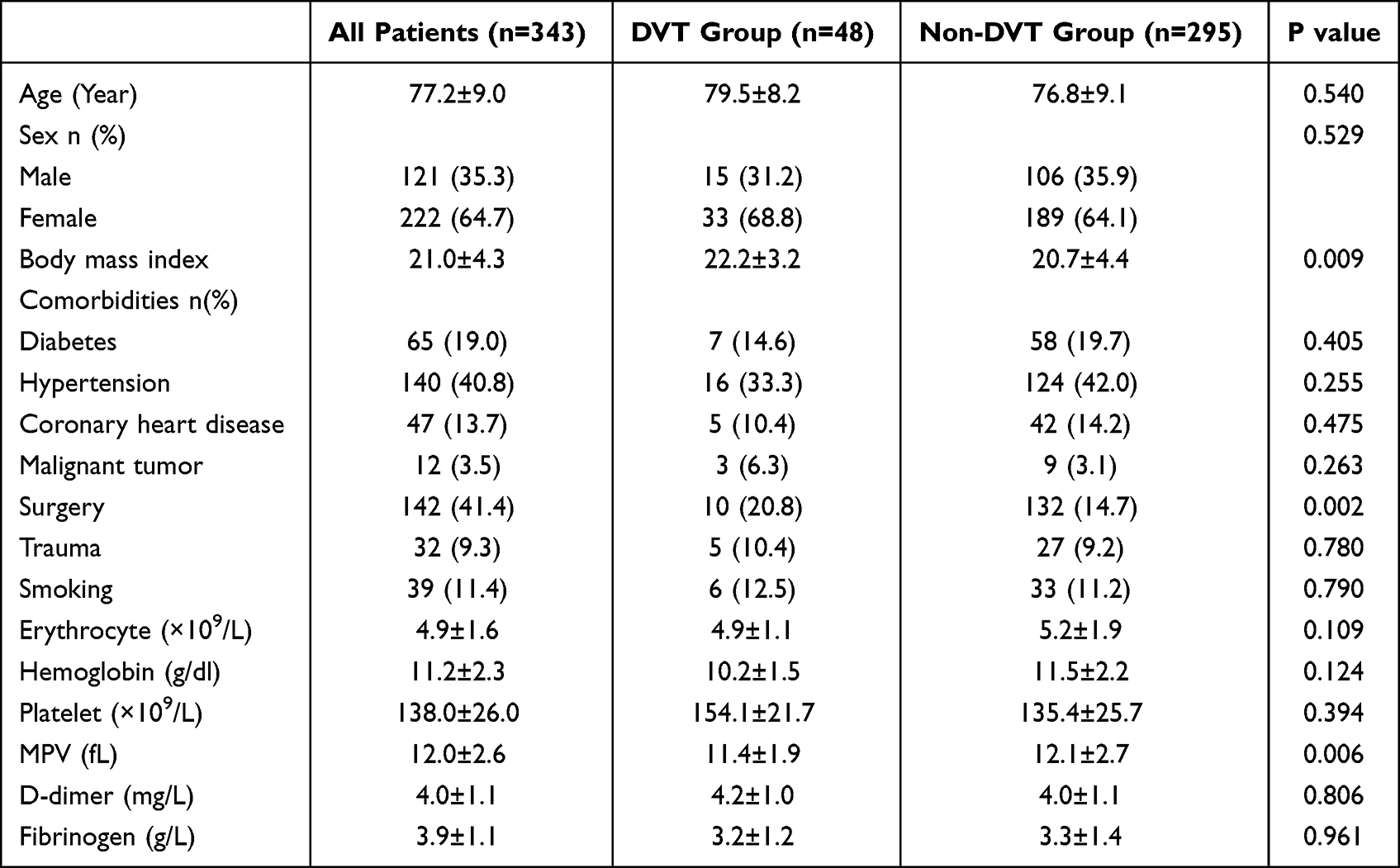 |
Table 4 Demographic Characteristics and Laboratory Data of the Included Patients with DVT and Without DVT |
Discussion
DVT is an important cause of cardiovascular disease, significantly associated morbidity, mortality and health cost worldwide.1 Accurate diagnosis and timely elimination of DVT is essential to reduce the risk of complications and improve the quality of life for patients. As a result, there is an urgent need to accurately assess the risk factor of DVT patients. Platelet plays an essential role in the complex process of thrombosis development in a complex process, while the specific causal between MPV and risk of DVT is still not clear. In the present study, the major finding demonstrated that MPV was negatively associated with the risk of DVT both in the two-sample MR analysis and retrospective study.
In this study, the incidence of DVT was 14% and negative association between MPV and the risk of DVT was reported, which was consistent with several previous studies. A research in China reported that the incidence was 15.1% and found that low MPV was associated with DVT in Older Patients with Hip Fracture.9 Ferroni et al19 demonstrated that low level of MPVs in cancer patients before chemotherapy was a predictor of increased risk venous thromboembolism risk while the similar result was confirmed in another researche in cancer patients from Australia.20 In the emergency department, a retrospective study conducted in Italy supported an inverse association between MPV and the risk of DVT.10 However, the role of MPV for the risk of DVT remained controversial while different results have been also reported.21,22 Considering that most previous studies were conventional retrospective studies, it is particularly important to adopt new research methods for these clinical issues. Two sample MR analysis has been widely performed in the exploration of risk factors for DVT.23,24 Recently, focus on the size of blood cells on the risk of DVT, there was a report through the method of MR analysis. He et al25 found that the distribution width and volume of red blood cells were associated with a higher risk of VTE. However, it has not yet been investigated exploring the size of the platelets on the risk of DVT through the MR analysis. In the present study, the causal estimates between MPV and risk of DVT were similar both in terms of direction and magnitude among IVW, weighted median and Egger regression, with great power to support the causal relationship.
The exact mechanisms of low MPV and increased risk of DVT have not been clarified. Compared with the larger platelets, the small platelets with lower MPV were observed with greater propensity to thrombosis formation. It should be noted that the result was observed in the cancer patients. Thus, the generalizability of the finding toward non-cancer participants needs to be confirmed. In vitro, platelets with a smaller size secreted more P-selectin, which played an important role in the surface adhesion in the thrombosis formation.26 Considering the few studies at present, more basic researches are needed in the future to explore its specific mechanism.
The study had several essential advantages. To the best of our knowledge, this was the first MR study to investigate the causality between MPV and risk of DVT. Depending on genetic instruments, MR analysis can effectively prevent the usual pitfalls of confounders and reverse causality, which are commonly present in traditional observational studies and an important cause of conflicting results. With the genetic instrument associated with MPV and DVT extracted from two different large consortiums, the study had included more than 450,000 participants and robustly instrumental variables (F statistics over lager than 10). Moreover, the result was further confirmed by the retrospective study, because of which the study had higher credibility for causal estimates. Early diagnosis is of great significance for improving the treatment effect of DVT and reducing complications. This study emphasizes the significance of the MPV. For patients with increased MPV, more attention should be paid the occurrence of DVT. Further, to well improve the diagnostic accuracy, more studies should be performed to combine MPV with the other clinical markers.
Inevitably, there were also some limitations to be desired. First, all the included participants in MR analysis were of European origin. Though the result was verified in our center, the retrospective study was a single-center study with the small sample size. As a result, it was still questionable whether our findings could generalizable to Asian populations. Further prospective studies with a larger sample in Asian population are needed to confirm the conclusion. Because of the limitation from the summary data, detailed information was not able to be obtained in the individual level, for which the MR analysis provided a linear relationship between MPV and risk of DVT. In a real-world study, the relationship between risk factor and outcome might be J- or U-shaped. More researches are needed to explore the MPV cut‐off points in DVT based on the clinical studies with large sample.
Conclusion
In this study, we found the negatively casual association between MPV and risk of DVT by using the two-sample Mendelian randomization method and retrospective study. But further researches are demanded to add to the findings and explore the potential mechanism of the size of platelets on the formation of DVT.
Ethics Approval and Consent to Participate
There were no patients involved in the MR analysis, so the ethical approval was waived by the ethic committee of Foshan Hospital of Traditional Chinese Medicine. The retrospective study was approved by the Ethics Committee of Foshan Hospital of Traditional Chinese Medicine.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Danwang C, Bigna JJ, Awana AP, et al. Global epidemiology of venous thromboembolism in people with active tuberculosis: a systematic review and meta-analysis. J Thromb Thrombolysis. 2021;51(2):502–512. doi:10.1007/s11239-020-02211-7
2. Jain N, Avanthika C, Singh A, et al. Deep vein thrombosis in intravenous drug users: an invisible global health burden. Cureus. 2021;13(10). doi:10.7759/cureus.18457
3. Kearon C, de Wit K, Parpia S, et al. Diagnosis of deep vein thrombosis with D-dimer adjusted to clinical probability: prospective diagnostic management study. BMJ. 2022;376. doi:10.1016/j.thromres
4. Bellesini M, Robert‐Ebadi H, Combescure C, et al. D‐dimer to rule out venous thromboembolism during pregnancy: a systematic review and meta‐analysis. J Thromb Haemost. 2021;19(10):2454–2467. doi:10.1111/jth.15432
5. Bye AP, Unsworth AJ, Gibbins JM. Platelet signaling: a complex interplay between inhibitory and activatory networks. J Thromb Haemost. 2016;14(5):918–930. doi:10.1111/jth.13302
6. Barrett TJ, Lee AH, Xia Y, et al. Platelet and vascular biomarkers associate with thrombosis and death in coronavirus disease. Circ Res. 2020;127(7):945–947. doi:10.1161/CIRCRESAHA.120.317803
7. Çil H, Yavuz C, Islamoğlu Y, et al. Platelet count and mean platelet volume in patients with in-hospital deep venous thrombosis. Clin Appl Thromb Hemost. 2012;18(6):650–653. doi:10.1177/1076029611435838
8. Braekkan SK, Mathiesen EB, Njølstad I, et al. Mean platelet volume is a risk factor for venous thromboembolism: the Tromsø study. J Thromb Haemost. 2010;8(1):157–162. doi:10.1111/j.1538-7836.2009.03498.x
9. Wang Z, Chen X, Wu J, et al. Low mean platelet volume is associated with deep vein thrombosis in older patients with hip fracture. Clin Appl Thromb Hemost. 2022;28:10760296221078837. doi:10.1177/10760296221078837
10. Lippi G, Buonocore R, Cervellin G. The mean platelet volume is decreased in patients diagnosed with venous thromboembolism in the emergency department. Semin Thromb Hemost. 2016;42(06):632–635. doi:10.1055/s-0036-1571335
11. Burgess S, Swanson SA, Labrecque JA. Are Mendelian randomization investigations immune from bias due to reverse causation? Eur J Epidemiol. 2021;36(3):253–257. doi:10.1007/s10654-021-00726-8
12. Bowden J, Del Greco MF, Minelli C, et al. A framework for the investigation of pleiotropy in two‐sample summary data Mendelian randomization. Stat Med. 2017;36(11):1783–1802. doi:10.1002/sim.7221
13. Hemani G, Zheng J, Elsworth B, et al. The MR-Base platform supports systematic causal inference across the human phenome. Elife. 2018;7:e34408. doi:10.7554/eLife.34408
14. Gieger C, Radhakrishnan A, Cvejic A, et al. New gene functions in megakaryopoiesis and platelet formation. Nature. 2011;480(7376):201–208. doi:10.1038/nature10659
15. Schaid DJ, Chen W, Larson NB. From genome-wide associations to candidate causal variants by statistical fine-mapping. Nat Rev Genet. 2018;19(8):491–504. doi:10.1038/s41576-018-0016-z
16. Burgess S, Thompson SG. Bias in causal estimates from Mendelian randomization studies with weak instruments. Stat Med. 2011;30(11):1312–1323. doi:10.1002/sim.4197
17. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet epidemiol. 2016;40:304–314. doi:10.1002/gepi.21965
18. Yavorska OO, Burgess S. Mendelian Randomization: an R package for performing Mendelian randomization analyses using summarized data. Int J Epidemiol. 2017;46:1734–1739. doi:10.1093/ije/dyx034
19. Ferroni P, Guadagni F, Riondino S, et al. Evaluation of mean platelet volume as a predictive marker for cancer-associated venous thromboembolism during chemotherapy. Haematologica. 2014;99(10):1638. doi:10.3324/haematol.2014.109470
20. Riedl J, Kaider A, Reitter EM, et al. Association of mean platelet volume with risk of venous thromboembolism and mortality in patients with cancer. Thromb Haemost. 2014;111(04):670–678. doi:10.1160/TH13-07-0603
21. Icli A, Aksoy F, Turker Y, et al. Relationship between mean platelet volume and pulmonary embolism in patients with deep vein thrombosis. Heart Lung Circ. 2015;24(11):1081–1086. doi:10.1016/j.hlc.2015.04.170
22. Han JS, Park TS, Cho SY, et al. Increased mean platelet volume and mean platelet volume/platelet count ratio in Korean patients with deep vein thrombosis. Platelets. 2013;24(8):590–593. doi:10.3109/09537104.2012.748187
23. Yuan S, Li X, Morange PE, et al. Plasma phospholipid fatty acids and risk of venous thromboembolism: Mendelian randomization investigation. Nutrients. 2022;14(16):3354. doi:10.3390/nu14163354
24. Larsson SC, Bäck M, Rees JMB, et al. Body mass index and body composition in relation to 14 cardiovascular conditions in UK Biobank: a Mendelian randomization study. Eur Heart J. 2020;41(2):221–226. doi:10.1093/eurheartj/ehz388
25. He J, Jiang Q, Yao Y, et al. Blood cells and venous thromboembolism risk: a two-sample Mendelian randomization study. Front Cardiovasc Med. 2022;9. doi:10.3389/fcvm.2022.919640
26. Handtke S, Steil L, Palankar R, et al. Role of platelet size revisited function and protein composition of large and small platelets. Thromb Haemost. 2019;119(3):
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.