Back to Journals » International Journal of Women's Health » Volume 18
Genetic Associations Between Premature Ovarian Insufficiency and Bone Health Traits: A Bidirectional Two-Sample Mendelian Randomization Study
Authors Zhou X, Quan C, Zhu M, Kang Z, Li D, Cao J, Liu W, You Z
Received 9 March 2026
Accepted for publication 22 May 2026
Published 30 June 2026 Volume 2026:18 607894
DOI https://doi.org/10.2147/IJWH.S607894
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Marta Barba
Xiayun Zhou1, Chunmei Quan2, Mohao Zhu1, Zhen Kang1, Duoduo Li1, Jianan Cao1, Weiai Liu1, Zhaoling You3
1Department of Acupuncture, The Second Affiliated Hospital of Hunan University of Chinese Medicine, Changsha, People’s Republic of China; 2Department of Gynecology, Hengyang City Traditional Chinese Medicine Hospital, Hengyang, People’s Republic of China; 3Department of Gynecology, The First Affiliated Hospital of Hunan University of Chinese Medicine, Changsha, People’s Republic of China
Correspondence: Weiai Liu, Email [email protected]; Zhaoling You, Email [email protected]
Background: Premature ovarian insufficiency (POI) is associated with reduced bone mineral density (BMD) and fracture risk, but the causal direction remains unclear. Clarifying this is crucial for individualized patient management and understanding shared biology between bone and ovary.
Objective: To investigate the bidirectional genetic causal relationships between POI and bone health using Mendelian randomization (MR).
Methods: We performed bidirectional two-sample MR using genome-wide association study summary statistics. Primary analyses used the inverse-variance weighted method, with MR-Egger and weighted median as supplements. Sensitivity analyses included tests for pleiotropy and heterogeneity. Multiple testing was controlled using the false discovery rate.
Results: Forward MR found no significant causal effect of genetically predicted POI on 29 bone health outcomes (all FDR P > 0.05). Reverse MR suggested nominally significant associations: higher genetically predicted heel BMD was associated with lower POI risk (OR = 0.792, 95% CI: 0.635– 0.988, P = 0.039), while genetic susceptibility to wrist fracture (OR = 1.44, 95% CI: 1.038– 1.986, P=0.025) and pelvic fracture (OR=1.177, 95% CI:1.056– 1.312, P=0.003) were associated with increased POI risk.
Conclusion: This study found no genetic evidence that POI causally influences bone health deterioration, suggesting that clinical bone loss in POI is likely a secondary consequence. Conversely, exploratory reverse MR analysis identified nominal associations suggesting that inherent bone traits may influence POI risk, offering a novel perspective for risk assessment and highlighting potential bone-ovary biological links; these findings require confirmation in future studies.
Keywords: premature ovarian insufficiency, bone mineral density, fracture, osteoporosis, mendelian randomization
Introduction
Premature ovarian insufficiency (POI) is a significant endocrine disorder affecting female reproductive health. Its primary characteristic is the premature decline of ovarian function, typically occurring before the age of 40. Clinical manifestations include oligomenorrhea, amenorrhea, and abnormal sex hormone levels, leading to decreased fertility.1,2 In recent years, the incidence of POI among young women has risen significantly. The global prevalence is 1%,3 while the prevalence in China has reached 2.8%.4 Due to long-term estrogen deficiency, POI is associated with various health risks, including infertility, decreased bone mineral density (BMD), increased risk of bone fractures, anxiety, and potential early cognitive decline. These risks have a serious impact on women’s health.5,6
Research has found a significant correlation between bone metabolic indices and ovarian reserve markers.7 BMD of women with POI is significantly lower than that of women with regular menstrual cycles. Early menopause and reduced estradiol levels accelerate the onset of osteoporosis.8 Therefore, POI is considered a hypogonadal state associated with low bone mineral density.9 The severity of osteoporosis can be assessed using clinical bone mineral density testing as an important indicator.10 Osteoporosis significantly increases the risk of bone fractures.11 Compared to women of the same age, patients with POI experience accelerated bone loss and deterioration of bone microstructure, thereby increasing the risk of changes in BMD, osteoporosis, and bone fractures.8,12–14 A related meta-analysis confirmed that the bone mineral density of the femoral neck and non-dominant forearm in POI patients is significantly lower than that of healthy women of the same age.15 Furthermore, their risk of bone fractures is higher.
However, although observational studies suggest that POI is significantly associated with an increased risk of low BMD, osteoporosis, and fractures, they cannot effectively determine whether this association is causal or due to confounding factors (eg., age, hormone therapy, lifestyle) or reverse causality.13,14 This uncertainty poses a challenge for clinical decision-making, such as determining the necessity and intensity of bone health interventions for all POI patients.
Mendelian Randomization (MR) is a powerful method that uses genetic variants as instrumental variables to infer causal relationships between exposures and outcomes. Since genotypes are randomly assigned at conception and are not influenced by postnatal environmental factors, this method is used to infer causal relationships between risk factors and disease outcomes, effectively avoiding the confounding biases present in traditional observational studies.16 Indeed, MR has been successfully applied to investigate the genetic causality between various endocrine factors (eg., sex hormone levels, vitamin D) and bone health outcomes, providing valuable insights into the biological pathways underlying bone metabolism. In recent years, the availability of large-scale GWAS data has made it possible to use two-sample MR to deeply explore causal relationships between complex diseases. Bidirectional two-sample MR analysis demonstrates unique advantages in disease mechanism research, as it can simultaneously test the bidirectional causal effects between exposure factors and outcome measures. This method supports multi-sample and cross-cohort joint analyses.17 However, a systematic bidirectional MR investigation specifically focusing on POI and a comprehensive range of bone health traits is still lacking. Recently, large-scale genome-wide association studies (GWAS) have identified various genetic variants associated with complex human traits and diseases, including POI.18–22 These studies, by using variants as instrumental variables (IVs) to implement two-sample MR, enhance statistical power, detect potential causal relationships between POI and other traits, and lay a solid theoretical foundation for disease prevention, control, and clinical intervention.
Although a clinical association exists between POI and abnormal bone metabolism, whether a bidirectional genetic causal relationship exists between the two remains unclear. Clarifying this is crucial for understanding the mechanisms of disease comorbidity and formulating precise prevention and management strategies. Furthermore, situating this genetic investigation within the broader landscape of bone health assessment is important. While methods like MR elucidate causal biology, the field of risk prediction is increasingly moving towards integrating multi-domain data (genetic, clinical, biochemical) to build more comprehensive models.Therefore, based on the latest GWAS summary statistics, this study employs bidirectional two-sample MR analysis for the first time to systematically evaluate the causal associations between POI and various bone health indicators (including BMD at different sites, bone fractures, and osteoporosis). We hypothesize that clarifying this bidirectional relationship will not only provide high-quality genetic-level evidence to inform the cross-system health management of women with POI but may also reveal shared biological pathways linking bone metabolism and ovarian function, offering new insights for both clinical practice and mechanistic research.
Materials and Methods
Study Design
This bidirectional two-sample MR study was conducted in accordance with the STROBE-MR reporting guidelines. The analysis comprised two components: forward MR, which assessed the causal effect of genetically predicted POI on various bone health outcomes (BMD at different sites, fractures, and osteoporosis); and reverse MR, which evaluated the potential causal effect of genetically predicted bone health traits on POI risk. This bidirectional design allows for a comprehensive investigation of the potential interplay between ovarian and skeletal health.
The validity of the MR analysis rests on three core assumptions for the genetic IVs: (i) strong association with the exposure; (ii) independence from confounders of the exposure-outcome relationship; and (iii) influence on the outcome exclusively through the exposure (ie., absence of horizontal pleiotropy). To minimize bias, all GWAS summary statistics for exposures and outcomes were sourced from independent, non-overlapping cohorts. The analysis utilized publicly available GWAS data published up to September 2025.
Data Sources
GWAS summary statistics were obtained from public databases. Data for POI (655 cases and 267,780 controls of European ancestry) were sourced from the FinnGen database (https://www.finngen.fi/en/), and the data used in this study were from the FinnGen R12 version.
Bone health trait data, including BMD at multiple sites (eg., total body, heel, forearm), fracture outcomes (eg., wrist, pelvis, femur), and osteoporosis, were obtained from large-scale consortia including the UK Biobank GWAS, the IEU Open GWAS project (https://gwas.mrcieu.ac.uk/), and the GWAS Catalog (https://www.ebi.ac.uk/gwas/).These datasets primarily comprise individuals of European ancestry. Detailed information for all datasets, including accession identifiers, sample sizes, case/control counts, and population characteristics, is provided in Table 1.
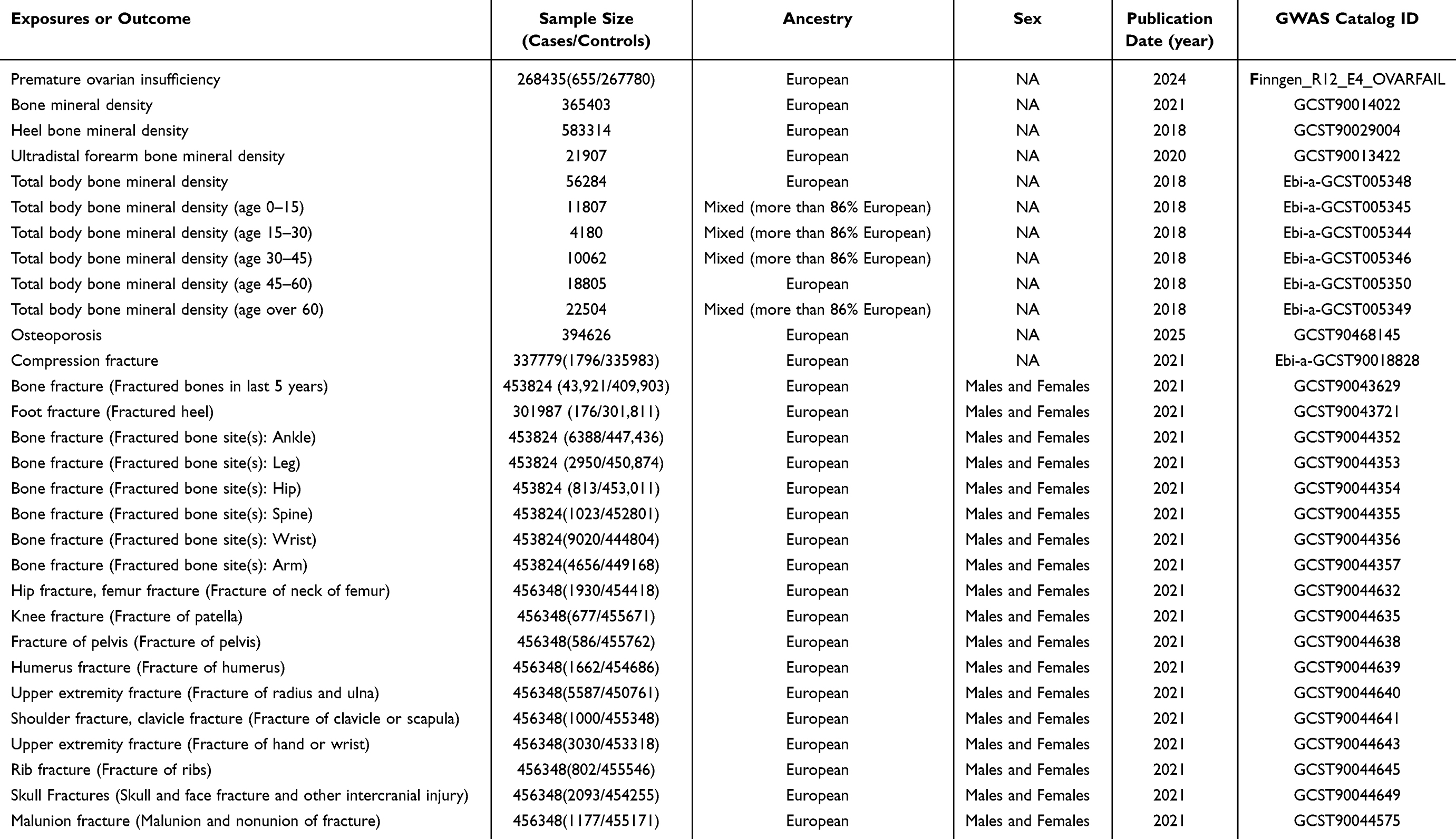 |
Table 1 Data Sources and Demographic Profiles in This Mendelian Randomization Study |
Instrumental Variable Selection
For each exposure, single-nucleotide polymorphisms (SNPs) significantly associated with the trait were selected as IVs. To ensure independence among IVs, we performed clumping with a linkage disequilibrium threshold of R2< 0.001 within a 10,000 kb window, retaining the SNP with the lowest P-value.
Considering the limited number of established genetic loci for POI, a significance threshold of P <1×10−5 was used to select POI-associated IVs, balancing statistical power with instrument validity, as done in prior studies.19,21,23 For bone health traits, a genome-wide significance threshold (P < 5×10−8) was applied for osteoporosis as an exposure. For BMD and fracture exposures, a threshold of P < 5×10−6 was used to obtain a sufficient number of IVs.
The strength of each IV was assessed using the F-statistic (F = R2(N-2)/(1-R2)), where R2 is the proportion of variance in the exposure explained by the SNP. All included SNPs had F-statistics > 10, indicating a low risk of weak instrument bias. The mean F-statistic for the POI instrument set was 21.69 (range: 19.47–28.99). Complete details for all exposures (number of SNPs, F-statistic range/mean, R2) are provided in Supplementary Table S1. The SNP screening and quality control workflow is summarized in Figure 1.
 |
Figure 1 (A) Overview of the research design. (B) MR analysis relies on three core assumptions. Assumption 1: Genetic tools are closely related to the exposure factor of interest; Assumption 2: Genetic tools are unrelated to confounding factors; Assumption 3: Genetic tools are unrelated to the outcome, and their influence on the outcome is achieved only through the exposure factor. “×” indicates that the assumption is not valid. The solid line represents a correlation, while the dotted line indicates no correlation. |
Statistical Analysis
This study primarily used the IVW method for causal effect estimation, which can be combined with causal estimates based on the Wald ratio for each SNP.24 Concurrently, MR-Egger regression and the weighted median method were used as supplementary analyses to verify the robustness of the results under different assumptions. The IVW method was chosen as the core analytical tool because, when all conditions are met, this method can select SNPs that provide the most accurate causal assessment results. These SNPs must be valid instrumental variables (IVs).25 To improve the reliability of the instrumental variable weight estimates, this study employed the MR-Egger test and the weighted median method. These methods can provide more reliable results for a broader range of cases.26 In the weighted median analysis, genetic variants must account for at least 50% of the total contribution to ensure the stability of the causal relationship estimate.27
Given that the forward MR involved testing one exposure (POI) against 29 independent bone health outcomes, the P-values from all forward IVW analyses were corrected for multiple testing using the false discovery rate (FDR) method. An FDR-adjusted P-value < 0.05 was considered statistically significant for the forward direction. In the reverse MR analysis, which explored the potential effects of 29 exposures on a single outcome (POI), results are primarily reported at a nominal significance level (P <0.05) and interpreted as exploratory and hypothesis-generating. We acknowledge this asymmetric statistical treatment.
Sensitivity Analysis
A series of sensitivity analyses were conducted to assess the robustness of the findings and the validity of the MR assumptions:
- Heterogeneity Test:Cochran’s Q statistic was used to assess heterogeneity among the IVs. In the presence of significant heterogeneity (P<0.05), the random-effects IVW model was applied.28,29
- Horizontal Pleiotropy Test:The MR-Egger intercept test was used to detect directional horizontal pleiotropy. A non-zero intercept with P<0.05 suggests the presence of pleiotropic bias.26 Additionally, the MR-PRESSO global test was employed to identify and correct for outliers.
- Leave-One-Out Analysis: To determine if the overall causal estimate was driven by any single influential SNP, we performed leave-one-out analysis by iteratively removing each SNP and recalculating the IVW estimate.
All analyses were performed using the “TwoSampleMR” and “MR-PRESSO” packages in R language (version 4.3.2).30,31
Results
Forward MR: Causal Effect of Genetically Predicted POI on Bone Health Outcomes
We selected 19 SNPs significantly associated with POI as instrumental variables for forward MR analysis (Supplementary Table S1). The primary IVW analysis was performed to assess the causal effect of genetically predicted POI on 29 bone health outcomes. Detailed results for all 29 forward MR IVW analyses, including beta coefficients, odds ratios (OR), 95% confidence intervals (CI), and p-values are provided in Supplementary Table S2a and visualized in Figures 2A–C.
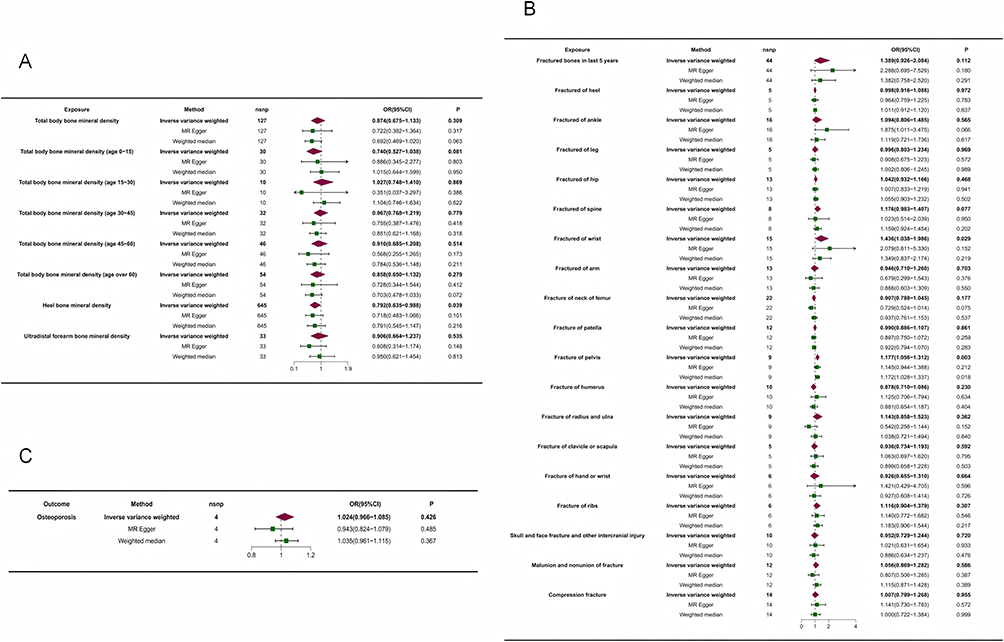 |
Figure 2 Forest map. (A) Forest map of POI on the risk of BMD. (B) Forest map of POI on the risk of fracture. (C) Forest map of POI on the risk of osteoporosis. |
Before multiple comparison correction, the IVW analysis suggested a nominal association between genetically predicted POI and a reduction in a specific bone mineral density phenotype (GCST90014022) (OR=0.995, 95% CI: 0.991–0.999, P=0.021). The MR-Egger intercept test (intercept =−0.003, P=0.291) and MR-PRESSO global test (P=0.337) did not indicate the presence of horizontal pleiotropy. Cochran’s Q test showed no significant heterogeneity among the instrumental SNPs (P=0.357). Leave-one-out analysis confirmed that the overall causal estimates were not driven by any single influential SNP (see Table 2 and Figures 3A–C, and Supplementary Table S2b and 2c).
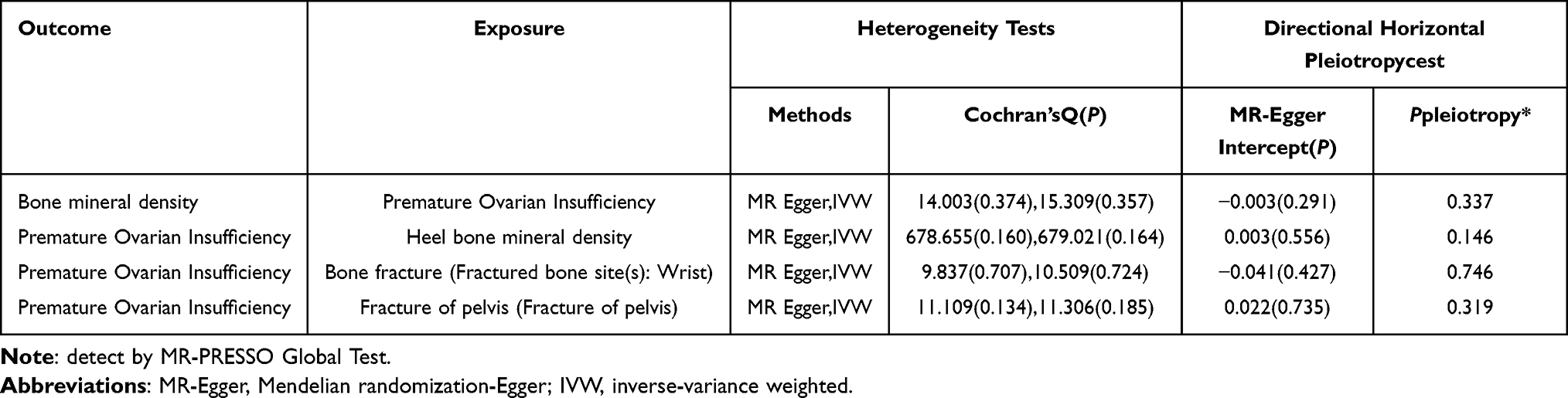 |
Table 2 MR Sensitivity Analyses of the Causal Relationship Between Bone Disorder and Premature Ovarian Insufficiency |
 |
Figure 3 The two-sample MR analysis of the genetically predicted casual associations between POI and BMD. (A) Scatter plot. (B) funnel plot. (C) leave-one-out sensitivity analysis. |
However, after applying false discovery rate (FDR) correction for all 29 tested outcomes, this association did not reach the statistical significance threshold (FDR-adjusted P> 0.05), nor did any other association. In summary, forward MR analysis did not find statistically significant causal effects of genetically predicted POI on any of the assessed bone health outcomes after rigorous multiple testing correction. Sensitivity analyses for the forward MR supported the robustness of the overall null findings.
Reverse MR: Causal Effect of Genetically Predicted Bone Health Outcomes on POI
Reverse MR analysis was conducted to explore the potential impact of genetically predicted bone health status on the risk of POI. Using the IVW method as the primary analysis, we identified nominal associations for three bone health indicators:
- Heel BMD (GCST90029004): Genetically predicted higher heel BMD was associated with a reduced risk of POI (IVW OR=0.792, 95% CI: 0.635–0.988, P=0.039).
- Wrist Fracture (GCST90044356): Genetic susceptibility to wrist fracture was associated with an increased risk of POI (IVW OR=1.436, 95% CI: 1.038–1.986, P=0.025).
- Pelvic Fracture (GCST90044638): Genetic susceptibility to pelvic fracture was associated with an increased risk of POI (IVW OR=1.177, 95% CI:1.056–1.312, P=0.003).
Importantly, these three associations were identified at a nominal significance threshold (P < 0.05) and did not survive FDR correction across the 29 exposures. Therefore, they should be interpreted as exploratory and hypothesis-generating, not as definitive causal inferences. Detailed results for all 29 reverse MR IVW analyses are provided in Supplementary Table S3a. All other tested bone health indicators (including BMD at other sites and other fracture types) showed no significant association with POI risk (see Table 2 and Figures 4A–C, and Supplementary Table S3b and 3c).
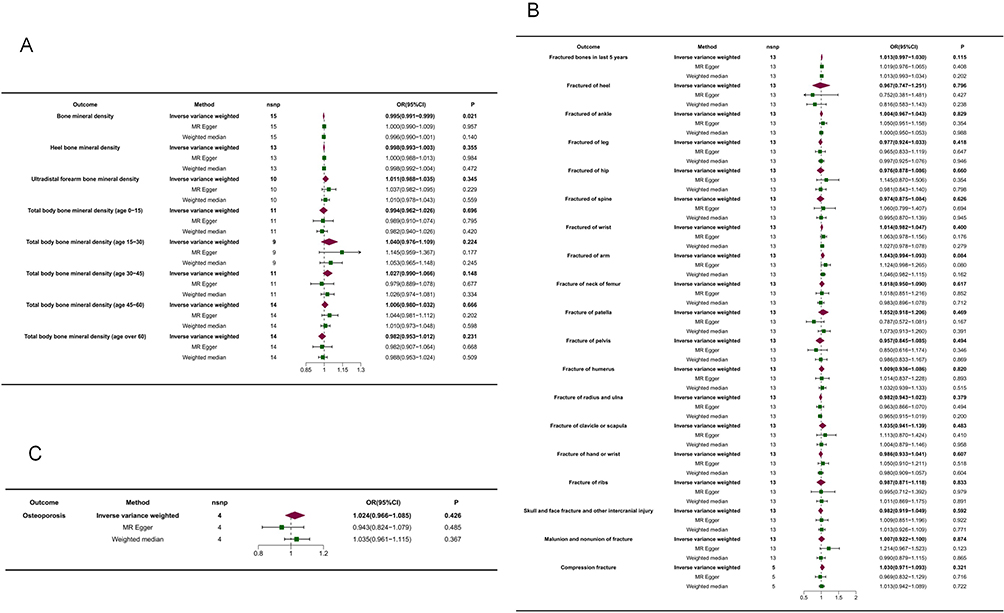 |
Figure 4 Forest map. (A) Forest map of BMD on the risk of POI. (B) Forest map of fracture on the risk of POI. (C) Forest map of osteoporosis on the risk of POI. |
Comprehensive sensitivity analyses were performed for the three significant associations to assess their reliability and the validity of the MR assumptions:
- Horizontal Pleiotropy: MR-Egger intercept tests provided no evidence of directional pleiotropy (Heel BMD: intercept=0.003, P=0.556; wrist fracture: intercept =−0.041, P=0.427; pelvic fracture: intercept=0.022, P=0.735). MR-PRESSO global tests yielded consistent results (see Table 2 and Figures 5A, 6A, 7A).

Figure 5 The two-sample MR analysis of the genetically predicted casual associations between calcaneal bone mineral density and POI. (A) Scatter plot. (B) funnel plot. (C) leave-one-out sensitivity analysis.

Figure 6 The two-sample MR analysis of the genetically predicted casual associations between fracture of the wrist and POI. (A) Scatter plot. (B) funnel plot. (C) leave-one-out sensitivity analysis.

Figure 7 The two-sample MR analysis of the genetically predicted casual associations between fracture of the pelvis and POI. (A) Scatter plot. (B) funnel plot. (C) leave-one-out sensitivity analysis.
- Heterogeneity: Cochran’s Q tests indicated no significant heterogeneity among the instrumental variables for these associations (all P>0.05) (see Table 2 and Figures 5B, 6B, 7B).
- Influence Analysis: Leave-one-out analyses demonstrated that the causal estimates for heel BMD, wrist fracture, and pelvic fracture were stable and not unduly influenced by any single SNP (see Table 2 and Figures 5C, 6C, 7C).



Collectively, these sensitivity analyses supported the robustness of the above-identified nominally significant associations, although they did not survive strict multiple testing correction.
Discussion
This study employed a systematic bidirectional two-sample MR analysis to investigate the genetic causal relationships between POI and a wide range of bone health phenotypes. Our primary finding is that, after rigorous multiple testing correction, we found no strong genetic evidence to support a causal effect of POI on decreased BMD or increased fracture risk. In the reverse direction, exploratory analyses suggested nominally significant associations whereby genetically predicted higher heel BMD was linked to a lower risk of POI, while genetic susceptibility to wrist and pelvic fractures was linked to a higher risk.These findings, particularly the robust null result from the forward analysis, provide a novel genetic perspective on the complex interplay between reproductive and skeletal health.The strength of this study lies in its adherence to MR core assumptions, the use of independent datasets to avoid sample overlap, and comprehensive sensitivity analyses. Notably, the application of FDR correction to the forward MR analysis enhances the robustness of our primary conclusion regarding the effect of POI on bone.
Interpretation of Main Findings in Context
Observational studies consistently suggest a close association between POI and impaired bone health, including lower BMD and higher fracture risk.32–37 For instance, a study involving over 350 POI patients reported that 58% had osteopenia or osteoporosis.38 Multiple studies have confirmed that BMD at key sites like the spine and femoral neck is significantly lower in POI patients compared to age-matched controls.39–41 Popat et al, using data from NHANES III, found spinal and femoral neck BMD in POI patients to be 2–3% lower.41 Risk factors for this bone loss include irregular menstruation before puberty, delayed POI diagnosis, poor adherence to estrogen therapy, and nutritional and lifestyle factors.42 In contrast, our MR analysis, which minimizes confounding, did not corroborate a genetic causal effect of POI on these bone health deficits. This suggests that the clinically observed osteopenia or osteoporosis in POI patients may be primarily a consequence of the condition (eg., post-onset estrogen deficiency) rather than sharing a strong common genetic cause with POI itself. This interpretation is supported by the time-dependent nature of the exposure: MR estimates reflect lifelong genetic predisposition, whereas significant bone loss in POI likely manifests after disease onset. This well-powered null finding represents a meaningful contribution, as it shifts the etiological focus from a strong shared genetic predisposition to modifiable post-diagnosis factors, underscoring that bone deterioration is not a pre-determined genetic fate for all POI patients. It reinforces the critical importance of timely post-diagnosis interventions (eg., hormone replacement therapy, lifestyle modifications) to mitigate this secondary risk.
Conversely, our reverse MR analysis provided exploratory insights into how inherent bone traits might influence POI risk. We found thatgenetically predicted higher heel BMD was nominally associated with a reduced risk of POI (OR=0.792, 95% CI: 0.635–0.988, P=0.039). This hypothesis-generating finding suggests that bone health status, potentially assessable via accessible sites like the heel, might reflect underlying biological processes relevant to ovarian reserve.
Regarding fractures, while observational studies indicate higher fracture risk in women with POI or early menopause,43,44 our forward MR did not support POI as a causal driver. Intriguingly, the reverse analysis suggested nominally significant associations where genetic susceptibility to pelvic (OR=1.177, 95% CI: 1.056–1.312; P=0.003) and wrist (OR=1.436, 95% CI: 1.038–1.986; P=0.025) fractures were linked to higher POI risk. These exploratory associations should be interpreted with caution. Speculatively, pelvic fractures could impact pelvic hemodynamics and ovarian perfusion,45 while a shared genetic propensity for factors like “accelerated aging” might underlie susceptibility to both fractures and follicular depletion. These preliminary findings invite future research into whether fracture history could be considered among multiple factors for assessing POI risk.
Potential Biological Mechanisms Linking Bone and Ovarian Function
The exploratory reverse MR findings invite speculation on potential shared biological pathways. The protective signal from heel BMD, influenced by mechanical loading, might implicate mechano-sensitive pathways (eg., Wnt/β-catenin) crucial for both bone formation and folliculogenesis.46,47 Alternatively, it could reflect a more active “bone endocrine” state, where osteoblast-derived factors like osteocalcin support ovarian function.48 The association with fracture susceptibility could point to a common substrate of genetically influenced cellular aging, DNA repair efficiency, or chronic inflammation,49,50 processes detrimental to both bone integrity and ovarian reserve.
Clinical and Translational Implications
The clinical implications of this study are nuanced and dual-focused. First, for POI management: While our genetic data do not support a strong innate causal link from POI to bone disease, the established observational association remains clinically paramount. Our findings emphasize that the bone health risk in POI is likely acquired and modifiable, strengthening the mandate for proactive, standardized bone health surveillance and intervention as a core component of POI care.Second, for POI risk assessment: The exploratory reverse associations propose that bone phenotype could be a mirror reflecting shared biological vulnerabilities relevant to POI. In practice, this might justify increased clinical attention to the ovarian function of young women with a history of fragility fractures, especially at the wrist or pelvis. Incorporating simple bone health metrics into broader health assessments could potentially aid in early risk stratification. Future research should aim to integrate genetic data with clinical and lifestyle factors to build predictive models for POI and its comorbidities.
Limitations
This study has several limitations. First, the primary data were derived from populations of European ancestry, and the generalizability of the conclusions needs to be validated in other populations. Second, although multiple sensitivity analyses were conducted, residual pleiotropy cannot be completely ruled out. Third, the GWAS sample sizes for some skeletal phenotypes (such as certain fractures) and for POI itself may have limited statistical power, which is common for rare outcomes. Fourth, we employed different multiple comparison correction strategies: FDR for the forward MR (testing multiple outcomes) and nominal thresholds for the exploratory reverse MR (testing multiple exposures on a single outcome). While this approach is methodologically justified by the differing hypothesis structures, it necessitates that the nominally significant reverse MR findings be interpreted as preliminary and requiring independent replication. Finally, MR reveals lifelong genetic risk and cannot be directly equated with the effects of interventions (eg., hormone therapy) at specific life stages.
Conclusion
In summary, this bidirectional MR study found no robust genetic evidence supporting a causal effect of POI on bone health outcomes. Exploratory reverse MR analyses suggested that genetically predicted higher heel bone mineral density may be associated with a lower risk of POI, while genetic susceptibility to wrist and pelvic fractures may be associated with a higher risk; these nominally significant associations require further validation. Collectively, the findings suggest that bone deterioration in POI is likely a critical but modifiable secondary complication rather than a genetically predetermined outcome. The potential link from certain bone traits to POI risk highlights a direction for future research into shared biological pathways. These insights offer a refined genetic perspective on the bone-ovary relationship, with potential implications for both the clinical management of POI and future risk assessment strategies.
Ethics Approval and Consent to Participate
All data utilized in this Mendelian randomization study were derived from publicly available, de-identified GWAS summary statistics on POI, BMD, fracture and osteoporosis. These original datasets had obtained prior ethical approvals and participant informed consent through their respective consortiums. This study is exempt from institutional ethics review under Article 32 of China’s Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (effective February 18, 2023), specifically meeting the following criteria: (1) Item 1: Research based on public databases that does not involve the identification or use of personal information., (2) Item 2: Analysis of collected data that does not involve the collection of new data or direct intervention in participants. As this work exclusively involved secondary analysis of aggregated genetic summary data without access to individual-level information, no additional ethical approval was required by our institutional review board.
Funding
This work was supported by the Key Research and Development Program of Hunan Province [Grant Number 2025JK2111] and the National Administration of Traditional Chinese Medicine’s You Zhaoling National Famous Doctor’s Legacy Workstation Construction Project [Grant Number (2022) No.5].
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Stuenkel CA, Gompel A, Solomon CG, Williams WW. Primary ovarian insufficiency. N Engl J Med. 2023;388(2):154–13. doi:10.1056/NEJMcp2116488
2. Brent S, Christakis M, Shirreff L. Primary ovarian insufficiency. CMAJ. 2023;195(28):E956. doi:10.1503/cmaj.221712
3. Verrilli L. Primary ovarian insufficiency and ovarian aging. Obstet Gynecol Clin North Am. 2023;50(4):653–661. doi:10.1016/j.ogc.2023.08.004
4. Golezar S, Ramezani Tehrani F, Khazaei S, et al. The global prevalence of primary ovarian insufficiency and early menopause: a meta-analysis. Climacteric. 2019;22(4):403–411. doi:10.1080/13697137.2019.1574738
5. De Vos M, Devroey P, Fauser BC. Primary ovarian insufficiency. Lancet. 2010;376(9744):911–921. doi:10.1016/S0140-6736(10)60355-8
6. Akande RO, Ibrahim Y. Genetics of primary ovarian insufficiency. Clin Obstet Gynecol. 2020;63(4):687–705. doi:10.1097/GRF.0000000000000575
7. Pal L, Bevilacqua K, Zeitlian G, et al. Implications of diminished ovarian reserve (DOR) extend well beyond reproductive concerns. Menopause. 2008;15(6):1086–1094. doi:10.1097/gme.0b013e3181728467
8. Anasti JN, Kalantaridou SN, Kimzey LM, et al. Bone loss in young women with karyotypically normal spontaneous premature ovarian failure. Obstet Gynecol. 1998;91(1):12–15. doi:10.1016/s0029-7844(97)00583-8
9. Marino R, Misra M. Bone health in primary ovarian insufficiency. Semin Reprod Med. 2011;29(4):317–327. doi:10.1055/s-0031-1280917
10. Billington EO, Feasel AL, Kline GA. At odds about the odds: women’s choices to accept osteoporosis medications do not closely agree with physician-set treatment thresholds. J Gen Intern Med. 2020;35(1):276–282. doi:10.1007/s11606-019-05384-x
11. Siris ES, Adler R, Bilezikian J, et al. The clinical diagnosis of osteoporosis: a position statement from the national bone health alliance working group. Osteoporos Int. 2014;25(5):1439–1443. doi:10.1007/s00198-014-2655-z
12. Rebar RW, Keator CS. Expanding our knowledge of premature ovarian insufficiency. Fertil Steril. 2021;115(2):328–329. doi:10.1016/j.fertnstert.2020.09.145
13. Cui X, Li H, Zhu X, et al. CCDC134 enhances ovarian reserve function and angiogenesis by directly interacting with INHA in a mouse model of premature ovarian insufficiency. Apoptosis. 2025;30(5–6):1311–1330. doi:10.1007/s10495-025-02092-2
14. Liu Z, Zhou Q, He L, et al. Identification of energy metabolism anomalies and serum biomarkers in the progression of premature ovarian failure via extracellular vesicles’ proteomic and metabolomic profiles. Reprod Biol Endocrinol. 2024;22(1):104. doi:10.1186/s12958-024-01277-9
15. Jiang M, Gao Y, Hou H, et al. Bone mineral density in patients with primary ovarian insufficiency: a systematic review and Meta-Analysis. Eur J Obstet Gynecol Reprod Biol. 2024;295:219–227. doi:10.1016/j.ejogrb.2024.02.013
16. Emdin CA, Khera AV, Kathiresan S. Mendelian Randomization. JAMA. 2017;318(19):1925–1926. doi:10.1001/jama.2017.17219
17. Wei L, Ma B, Wu D, et al. Sleep traits and risk of premature ovarian insufficiency - two-sample and multivariate mendelian randomisation analysis. Prz Menopauzalny. 2025;24(1):15–24. doi:10.5114/pm.2025.150594
18. Wang J, Luo R, Zhao X, et al. Association between gut microbiota and primary ovarian insufficiency: a bidirectional two-sample Mendelian randomization study. Front Endocrinol. 2023;14:1183219. doi:10.3389/fendo.2023.1183219
19. Wang J, Zhao X, Luo R, et al. The causal association between systemic inflammatory regulators and primary ovarian insufficiency: a bidirectional mendelian randomization study. J Ovarian Res. 2023;16(1):191. doi:10.1186/s13048-023-01272-5
20. Luo R, Wang J, Liu Y. Assessment of bidirectional relationships between autoimmune diseases and primary ovarian insufficiency: insights from a bidirectional two-sample Mendelian randomization analysis. Arch Gynecol Obstet. 2024. doi:10.1007/s00404-024-07482-6
21. Chen S, Zhou Z, Zhou Z, et al. Non-targeted metabolomics revealed novel links between serum metabolites and primary ovarian insufficiency: a Mendelian randomization study. Front Endocrinol. 2024;15:1307944. doi:10.3389/fendo.2024.1307944
22. Wang X, Mao R, Wang M, et al. The genetic relationship between systemic lupus erythematosus and risk of primary ovarian failure from a mendelian randomization study. Sci Rep. 2024;14(1):9413. doi:10.1038/s41598-024-59726-9
23. Peng K, Han X, Wu C, et al. The mitochondrial DNA copy number and ovary-related reproductive disorders: a bidirectional two-sample Mendelian randomization study. Int J Gynaecol Obstet. 2025;169(1):112–120. doi:10.1002/ijgo.16057
24. Burgess S, Butterworth A, Thompson SG. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol. 2013;37(7):658–665. doi:10.1002/gepi.21758
25. Bowden J, Holmes MV. Meta-analysis and Mendelian randomization: a review. Res Synth Methods. 2019;10(4):486–496. doi:10.1002/jrsm.1346
26. Burgess S, Thompson SG. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur J Epidemiol. 2017;32(5):377–389. doi:10.1007/s10654-017-0255-x
27. Bowden J, Davey Smith G. Haycock PC,et al.consistent estimation in mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.2196
28. Cohen JF, Chalumeau M, Cohen R, et al. Cochran’s Q test was useful to assess heterogeneity in likelihood ratios in studies of diagnostic accuracy. J Clin Epidemiol. 2015;68(3):299–306. doi:10.1016/j.jclinepi.2014.09.005
29. Azarzadeh M, Rahimi K. Heterogeneity between genetic variants as a proxy for pleiotropy in mendelian randomization-reply. JAMA Cardiol. 2020;5(1):108. doi:10.1001/jamacardio.20194284
30. Hemani G, Zheng J, Elsworth B, et al. The MR-Base platform supports systematic causal inference across the human phenome. Elife. 2018;7:e34408. doi:10.7554/eLife.34408
31. Verbanck M, Chen CY, Neale B, et al. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
32. Francucci CM, Romagni P, Camilletti A, et al. Effect of natural early menopause on bone mineral density. Maturitas. 2008;59(4):323–328. doi:10.1016/j.maturitas.2008.03.008
33. Gallagher JC. Effect of early menopause on bone mineral density and fractures. Menopause. 2007;14(3 Pt 2):567–571. doi:10.1097/gme.0b013e31804c793d
34. Patel R, Blake GM, Fogelman I. Peripheral and central measurements of bone mineral density are equally strongly associated with clinical risk factors for osteoporosis. Calcif Tissue Int. 2007;80(2):89–96. doi:10.1007/s00223-006-0217-x
35. Faubion SS, Kuhle CL, Shuster LT, et al. Long-term health consequences of premature or early menopause and considerations for management. Climacteric. 2015;18(4):483–491. doi:10.3109/13697137.2015.1020484
36. Shuster LT, Rhodes DJ, Gostout BS, et al. Premature menopause or early menopause: long-term health consequences. Maturitas. 2010;65(2):161–166. doi:10.1016/j.maturitas.2009.08.003
37. Dua M, Bhatia V, Malik S, et al. ART outcome in young women with premature ovarian aging. J Midlife Health. 2013;4(4):230–232. doi:10.4103/0976-7800.122257
38. Bachelot A, Rouxel A, Massin N, et al. Phenotyping and genetic studies of 357 consecutive patients presenting with premature ovarian failure. Eur J Endocrinol. 2009;161(1):179–187. doi:10.1530/EJE-09-0231
39. Uygur D, Sengül O, Bayar D, et al. Bone loss in young women with premature ovarian failure. Arch Gynecol Obstet. 2005;273(1):17–19. doi:10.1007/s00404-005-0029-7
40. Samad N, Nguyen HH, Hashimura H, et al. Abnormal trabecular bone score, lower bone mineral density and lean mass in young women with premature ovarian insufficiency are prevented by oestrogen replacement. Front Endocrinol. 2022;13:860853. doi:10.3389/fendo.2022.860853
41. Popat VB, Calis KA, Vanderhoof VH, et al. Bone mineral density in estrogen-deficient young women. J Clin Endocrinol Metab. 2009;94(7):2277–2283. doi:10.1210/jc.2008-1878
42. Soyka LA, Fairfield WP, Klibanski A. Clinical review 117: hormonal determinants and disorders of peak bone mass in children. J Clin Endocrinol Metab. 2000;85(11):3951–3963. doi:10.1210/jcem.85.11.6994
43. Hadji P, Colli E, Regidor PA. Bone health in estrogen-free contraception. Osteoporos Int. 2019;30(12):2391–2400. doi:10.1007/s00198-019-05103-6
44. Anagnostis P, Siolos P, Gkekas NK, et al. Association between age at menopause and fracture risk: a systematic review and meta-analysis. Endocrine. 2019;63(2):213–224. doi:10.1007/s12020-018-1746-6
45. Karakaya HC, Dirican Ozen B, Eskin P, et al. Efficacy of endovenous embolization for pelvic congestion syndrome and its impact on ovarian reserve. Reprod Biol Endocrinol. 2025;23(1):132. doi:10.1186/s12958-025-01470-4
46. Hao R, Li T, Zhou B, et al. Bushen Huoxue Formula alleviates lipid accumulation in premature ovarian insufficiency by activating the LRP6/β-catenin signaling pathway. Phytomedicine. 2026;150:157726. doi:10.1016/j.phymed.2025.157726
47. Rossetti R, Moleri S, Guizzardi F, et al. Targeted next-generation sequencing indicates a frequent oligogenic involvement in primary ovarian insufficiency onset. Front Endocrinol. 2021;12:664645. doi:10.3389/fendo.2021.664645
48. Li B, Boast S, de Los Santos K, et al. Mice deficient in Abl are osteoporotic and have defects in osteoblast maturation. Nat Genet. 2000;24(3):304–308. doi:10.1038/73542
49. Mattia L, Patel S, Webber K, et al. Growth differentiation factor 15 and the risk of Hip fracture in older adults. JBMR Plus. 2026;10(4):ziaf192. doi:10.1093/jbmrpl/ziaf192
50. Chang AJ, Go AS, Chandra M, et al. Heart Failure is an Independent risk factor for incident hip, proximal humerus, and wrist fractures in a high-risk older population. J Gen Intern Med. 2026. doi:10.1007/s11606-025-10092-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Hemoglobin Levels and Osteoporosis in Chinese Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study
Ye T, Lu L, Guo L, Liang M
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2803-2811
Published Date: 14 September 2022
Clinical Utility of Romosozumab in the Management of Osteoporosis: Focus on Patient Selection and Perspectives
Lim SY, Bolster MB
International Journal of Women's Health 2022, 14:1733-1747
Published Date: 15 December 2022
The Effects of Switching from Dipeptidyl Peptidase-4 Inhibitors to Glucagon-Like Peptide-1 Receptor Agonists on Bone Mineral Density in Diabetic Patients
Huang CF, Mao TY, Hwang SJ
Diabetes, Metabolic Syndrome and Obesity 2023, 16:31-36
Published Date: 11 January 2023
The Relationship Between Serum 25-Hydroxyvitamin D Levels and Osteoporosis in Postmenopausal Women
Wang D, Yang Y
Clinical Interventions in Aging 2023, 18:619-627
Published Date: 18 April 2023
Causal Effects of Female Reproductive and Hormonal Factors on Osteoporosis, Bone Mineral Density, and Osteoarthritis: A Two-Sample Mendelian Randomization Study
Li G, Shen W, Chen J, Dai Y, Mo G, Wang S, Wang X
International Journal of Women's Health 2026, 18:574318
Published Date: 7 May 2026