Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 14
Gender Differences in Oral Health Knowledge and Practices Among Adults in Jeddah, Saudi Arabia
Authors Rajeh MT ![]()
Received 19 June 2022
Accepted for publication 29 July 2022
Published 4 August 2022 Volume 2022:14 Pages 235—244
DOI https://doi.org/10.2147/CCIDE.S379171
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Mona T Rajeh
Department of Dental Public Health, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Mona T Rajeh, Department of Dental Public Health, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia, Tel +966 502500888, Email [email protected]
Aim: To determine the knowledge and practices of adults regarding oral health and to determine the associated gender differences.
Methods: A cross-sectional study design was used in Jeddah, Saudi Arabia, and a total of 1330 adults participated. Data were collected using self-administered validated questionnaire to gather information about sociodemographic data, oral health knowledge and practices. The scores of the oral health knowledge were calculated. Linear and logistic regressions were used to evaluate and compare the oral health knowledge and practices between males and females.
Results: Females had a significantly higher mean oral health knowledge score (8.5 ± 1.5) than males (8.1 ± 1.7). Regarding oral health practices, female participants reported a higher frequency of tooth brushing and mouthwash use than males (p = 0.001). The percentage of females who visited the dentist for check-ups and cleaning was significantly higher compared to males (41.5% and 35.2%, respectively). Participants with a university-level education showed a significantly higher knowledge score (coefficient = 0.27; 95% CI: − 0.46 to 0.46). Respondents who were less than 40 years old brushed their teeth more than twice a day compared to older individuals (OR = 1.51; 95% CI: 1.06 to 2.13). Nonsmokers had better knowledge, and brushing their teeth twice daily was more likely among them (OR = 0.76; 95% CI: 0.59 to 0.99).
Conclusion: Among the adult population, females were more knowledgeable about their oral health and exhibited better practices than males.
Keywords: adult, attitude, knowledge, oral health, Saudi Arabia
Introduction
Aside from being physically and mentally well, people should consider their oral health as part of their overall well-being. Oral health knowledge and good oral hygiene habits are essential for maintaining good health.1 Although knowledge about oral health practices can help individuals improve their behaviors and attitudes, it does not automatically translate into a change in their overall health. Poor oral health can significantly impact a person’s general health and lead to various chronic conditions, such as cancer and diabetes. The effects of poor oral health can also affect a person’s daily life. Apart from eating and smiling properly, people also experience pain and communication issues when they lose their teeth. People must therefore improve their oral health by taking the necessary steps.2
Despite the various initiatives aimed at improving oral health, the World Health Organization claimed that many people still have oral health problems. The Global Burden of Disease Organization revealed that around 3.5 billion people globally are affected by various oral diseases. Periodontal disease and caries are the most common oral conditions.3 Different studies have indicated that the prevalence of oral diseases is still very high in different countries.4–6 Low income, low level of education, high sugar intake, and a lack of fluoridated water are some factors that contribute to the development of oral diseases.7,8 High-cost dental treatment is another factor that can prevent people from taking good care of their oral health.2 Many studies have shown that individuals seek oral health care when experiencing pain and that regular oral hygiene habits are infrequent.2,9,10
As primary prevention professionals, dentists play a vital role in promoting positive behavioral changes in their patients and communities. Their social capacity to influence these changes has been shown to be extremely beneficial in improving oral health. The public perception of dentists as role models for oral hygiene is supported by evidence that they are more likely to provide effective and efficient care.11 A document titled “Global Goals for Oral Health 2020” which was created by the international dental research organization, aimed to set realistic goals for improving the oral health of people all around the world. This document sought to establish a comprehensive baseline of information about oral health, including the prevalence of diseases and the importance of healthy habits and procedures.4 This information will help health professionals and policymakers make informed decisions and implement effective measures.12
A person’s oral health knowledge is a combination of skills, experience, and judgment that can be used to acquire and preserve information. However, it is not enough to provide a person with oral health knowledge. Other factors, such as public knowledge and basic educational level can also contribute to the development of better oral care.13 In addition, maintaining good oral health knowledge is required to attain good oral health practices.14 Researchers have found that increased oral health knowledge leads to better oral health.9,15,16 It has been shown that people with this knowledge level are more likely to practice oral self-care procedures.17
There have been many studies examining the knowledge and practices of oral health of students across different countries at the national and international levels. Dental students receive and acquire the necessary knowledge of oral health and can spread it to their families and society.13,15 Unfortunately, previous studies have not been able to provide a clear picture of these students’ knowledge levels and attitudes.12,14–18 However, data on oral health knowledge and practice are limited in the adult population who are at least 20 years old. In 2005, Zhu et al conducted a study to examine the knowledge and practice of Chinese adults (35–74 years old) regarding their oral health. They found that knowledge about the causes of dental diseases and the prevention of these diseases was low.9 In the United Arab Emirates, a study found that a large number of adult participants had a high oral health knowledge, but less than half of them had a positive attitude toward it.19
In Saudi Arabia, a study investigated oral health knowledge among female primary school teachers.20 This study confirmed that teachers in private primary schools had better oral health knowledge than teachers in government primary schools.20 Other studies have shown that adults exhibit poor oral health knowledge.21,22 These previous studies focused only on oral health knowledge and not the practices of these populations. In addition, neither of these studies focused on how gender affects oral health knowledge, attitudes, or practices.
Given that the current adult population serves as a role model for younger generations and improves oral health outcomes for future generations, it is essential to identify behavior patterns among adults. Determining the current level of knowledge and practices helps policymakers provide programs designed to prevent high levels of disease and improve populations’ oral health. This study, therefore, examines the knowledge and practices regarding oral health among the adult population in Saudi Arabia and assess the associated gender differences.
Methods
Study Design
A cross-sectional survey was administered to adults 20 years old or older of any nationality living in Jeddah, Saudi Arabia. The study was conducted according to the Declaration of Helsinki and the ethical approval from the faculty of dentistry’s research ethics committee. All participants were informed about the study’s procedures and their confidentiality was assured. All participants provided informed consent.
Instrument
This study used a validated questionnaire developed by Buunk-Werkhoven.23 The questionnaire included 28 questions and three sections. The first one collected demographic information about the participants, such as their age, income, and nationality. The second section focused about the participants’ oral health knowledge. The third section asked about practices related to oral health such as the frequency of tooth brushing, mouth washing, dental visit and reasons of their last dental visits
The English questionnaire was translated into Arabic using a forward-backward method.
Three experts in questionnaire development assessed the questionnaire’s face validity. The experts were asked about the relevance and clarity of the questions. Then, a pilot study was conducted with 15 randomly selected adults living in Jeddah to assess the clarity of the questions. According to the responses, only a few words needed to be rephrased and clarified in the questionnaire. The Cronbach alpha coefficient indicated a good internal consistency, 0.97 for knowledge and 0.89 for practice.
Data Collection
Data were collected from August 2021 to December 2021 using SurveyMonkey (San Mateo, California, USA). The online questionnaire was then sent to the public through social media platforms such as WhatsApp and Twitter. A non-probability snowball sampling strategy was used, and participants were asked to share the survey with family and friends. The first question in the questionnaire was about whether or not you are 20 years old or older and live in the city of Jeddah. Responding to this question was a consent to participate in the study and helped exclude those who were ineligible. In addition, four dental interns distributed paper questionnaires in the largest shopping malls in each area of Jeddah. On average, it took around 5 min to complete the questionnaire. For the paper-based questionnaires, participants provided written informed consent. The participants did not receive compensation for completing the questionnaire. Permission to distribute the paper questionnaires was obtained from each local mall management office.
Statistical Analysis
Stata version 13.0 (StataCorp LP, College Station, TX, USA) was used to analyze the results of the study. The significance of the data was determined by the p-value <0.05. Different categorical variables were analyzed using Chi-square tests.
The knowledge score was calculated based on 11 knowledge questions: the score for a correct answer was 1, while the score for an incorrect answer was 0. The scores on all knowledge questions were added together to give each participant a total knowledge score from 0 to 11. Participants with higher scores demonstrated higher levels of knowledge.
The results of the study were analyzed using a linear regression analysis to determine the factors that influence the knowledge about oral health. The sociodemographic data were the independent variables. Logistic regression was additionally used to determine factors affecting oral health practice. The odds ratio and 95% confidence intervals for each variable were then calculated.
Results
In total, 1330 adults participated in the study (418 males and 912 females). Five questionnaires were dropped out because of missing data. Participants’ sociodemographic data are shown in Table 1. The majority of participants were between the ages of 20 and 40 (86%). Female participants had significantly higher education levels than males (p < 0.05). A significantly higher number of females worked in the private sector compared to males. The number of females with a monthly income lower than 10,000 SAR was significantly higher than that of male participants (70%). The smoking status of females and males differed significantly (68.9% of the females were nonsmokers, while 56.5% of the males were nonsmokers).
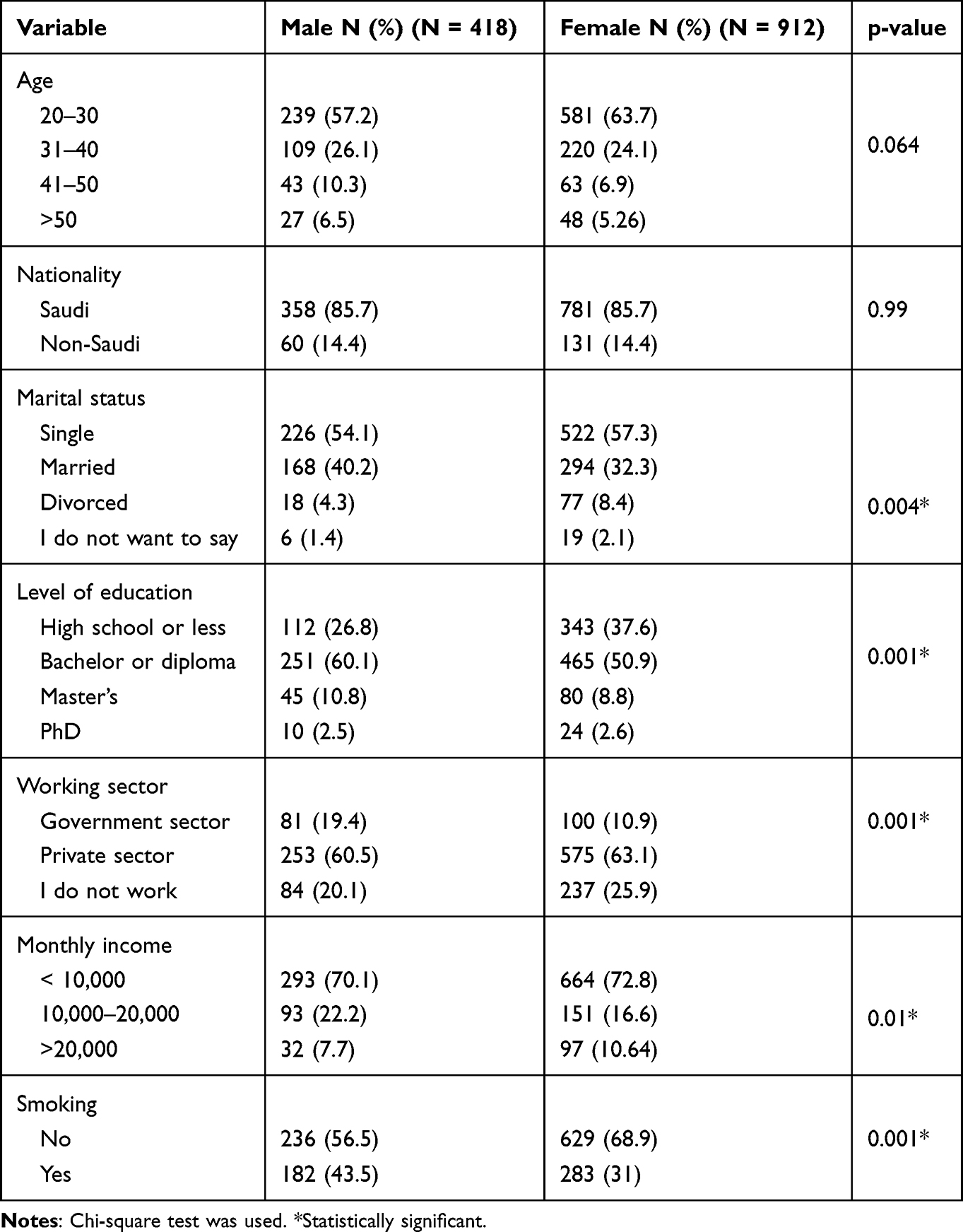 |
Table 1 Demographic Characteristics |
Overall, the females’ (8.5 ± 1.5) oral health knowledge mean ± SD score was significantly higher than that of the males (8.1 ± 1.7; p = 0.035). Table 2 illustrates the distribution of the participants’ oral health knowledge. However, a higher proportion of male participants (50.2%) than females (43.6%) knew that it was important to put gentle pressure on the toothbrush while brushing their teeth (p = 0.02). A significantly higher number of females indicated that it did matter if they used a toothbrush for a long time (77.5%) compared to males (72.5%; p = 0.04). In addition, a significantly greater number of females (75%) compared to males (64%) agreed that it is not true that gum inflammation can disappear by itself (p = 0.001). Females (89.3%) were more knowledgeable about gum disease causing bad breath than males (85.7%; p = 0.05).
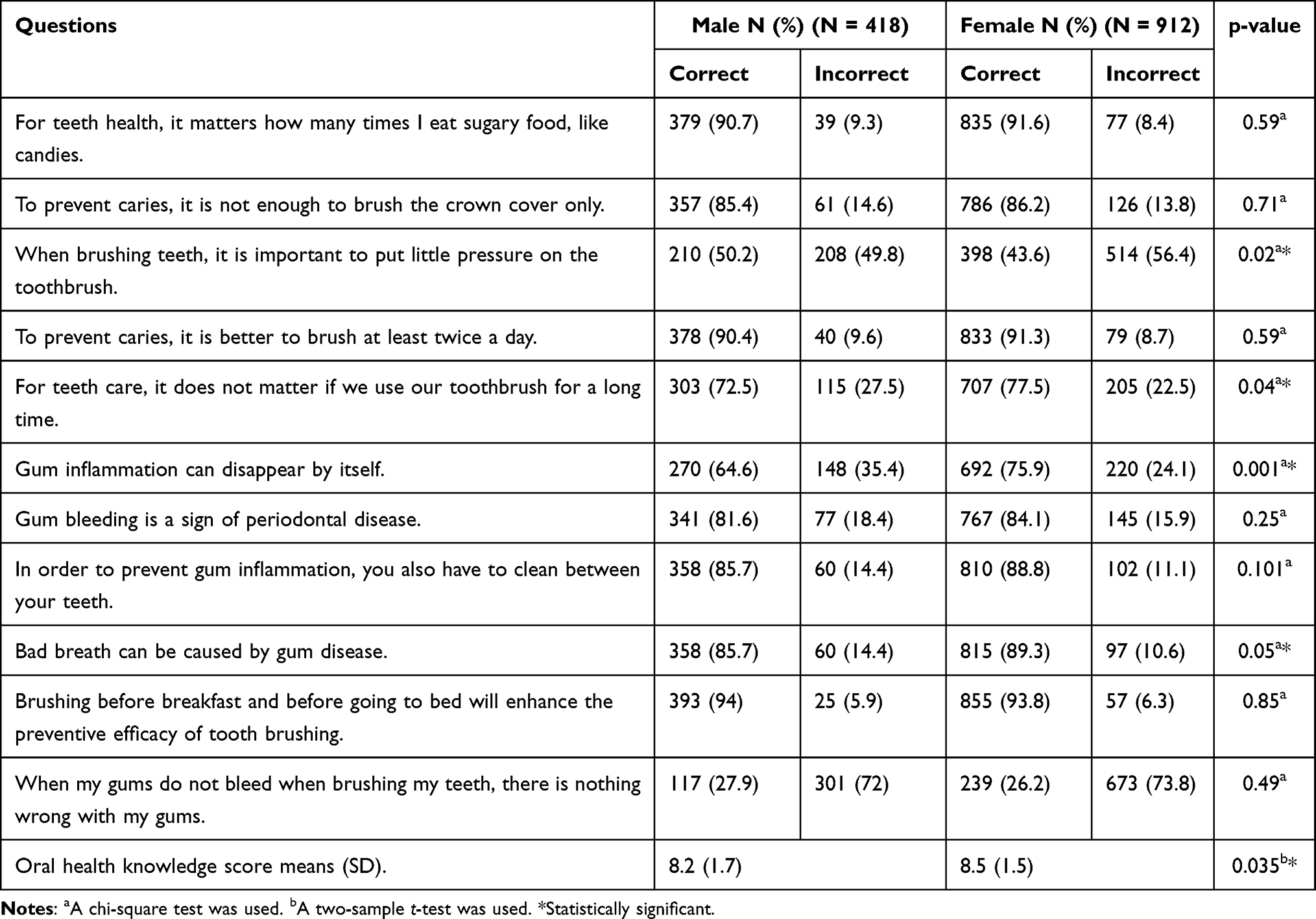 |
Table 2 Oral Health Knowledge Among Study Participants |
Oral health practices and attitudes are presented in Table 3. Female participants reported a higher frequency of tooth brushing (twice or more daily) than males (p = 0.001). Furthermore, the proportion of females who used mouthwash more frequently was higher than that of males (p = 0.001). The percentage of females who visited the dentist for check-ups and cleaning was significantly higher than that of males (41.5% and 35.2%, respectively).
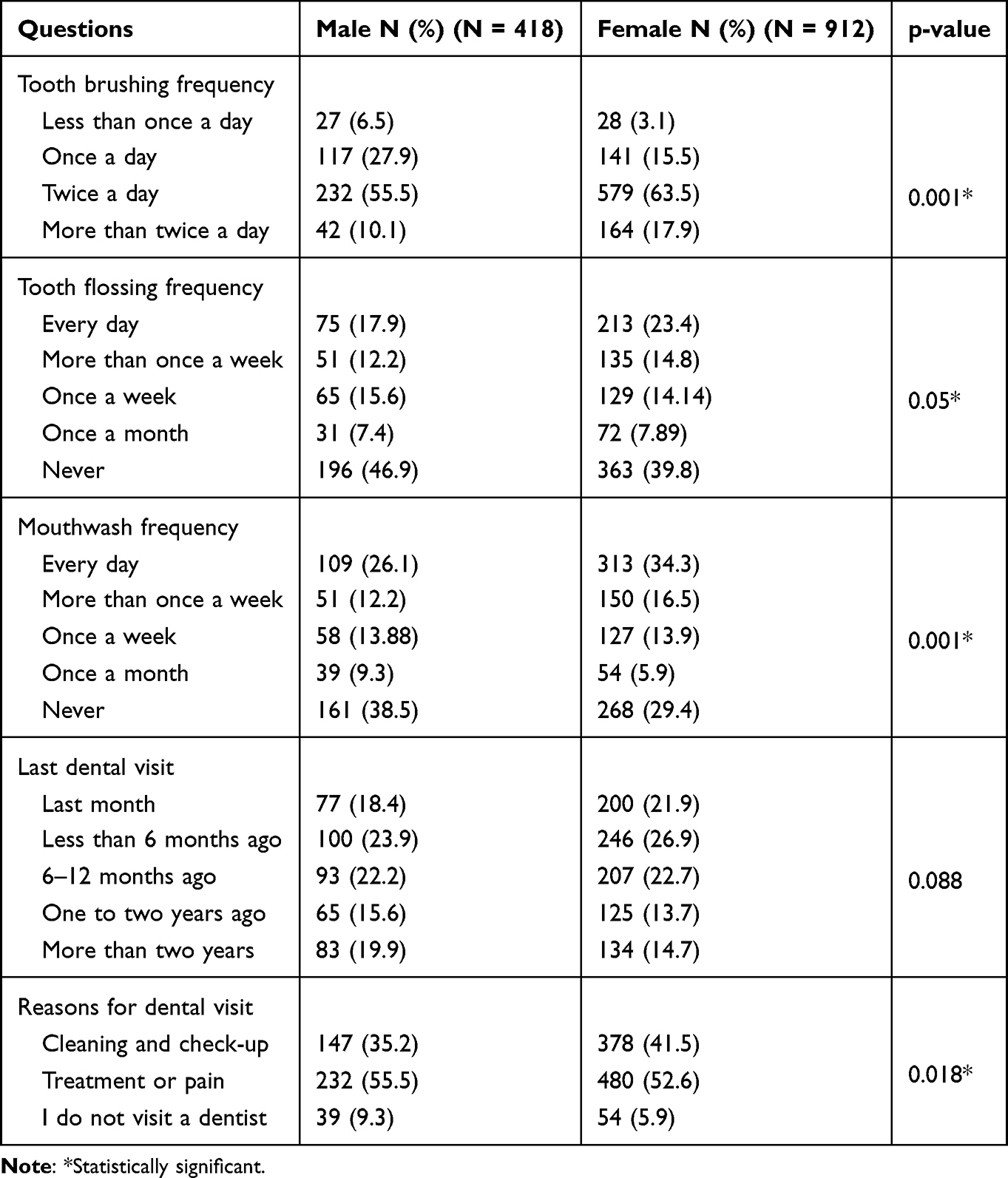 |
Table 3 Oral Health Practices and Attuites Among Study Participants |
Linear regression analysis was used to predict factors influencing oral health knowledge scores. There was a significant relationship between gender and knowledge score. Females demonstrated a significantly higher knowledge score than males (coefficient = 0.19; 95% CI: - 0.38 to −0.02). Furthermore, a statistically significant higher knowledge scores were found among participants having a university degree (coefficient = 0.27; 95% CI: −0.46 to 0.46). A lower knowledge score was associated with smoking (coefficient = −0.31; 95% CI: −0.48 to −0.13). An analysis of linear regression is shown in Table 4.
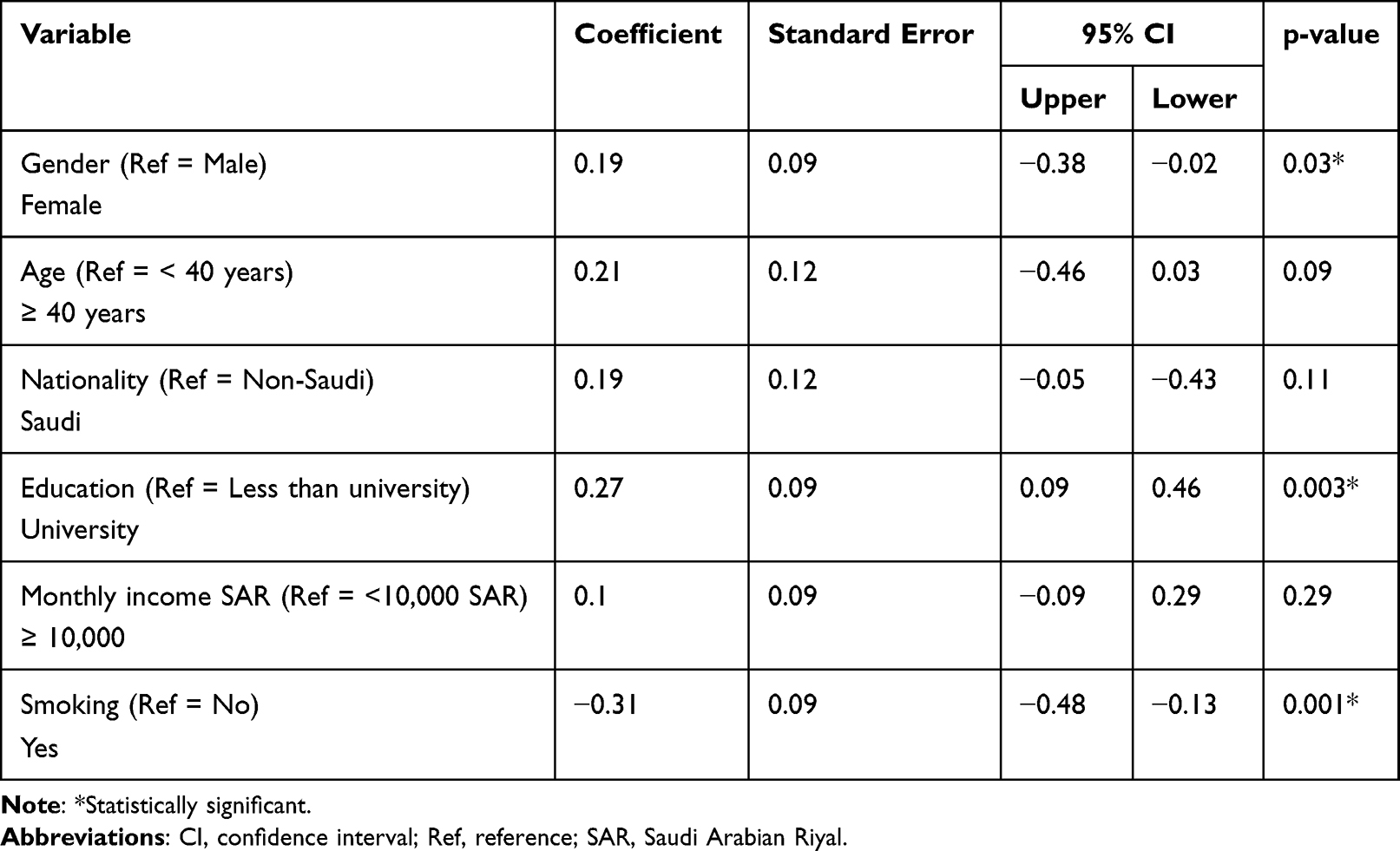 |
Table 4 Predictors of Oral Health Knowledge |
A logistic regression model was used to determine the factors that influence oral health practice (Table 5). According to the findings, a higher percentage of females brush twice a day or more (OR = 0.43; 95% CI: 0.33 to 0.56). The participants who were less than 40 years old were more likely to brush their teeth twice a day (OR = 1.51; 95% CI: 1.06 to 2.13). Non-smoking individuals were more likely to do so than those who smoke (OR = 0.76; 95% CI: 0.59 to 0.99).
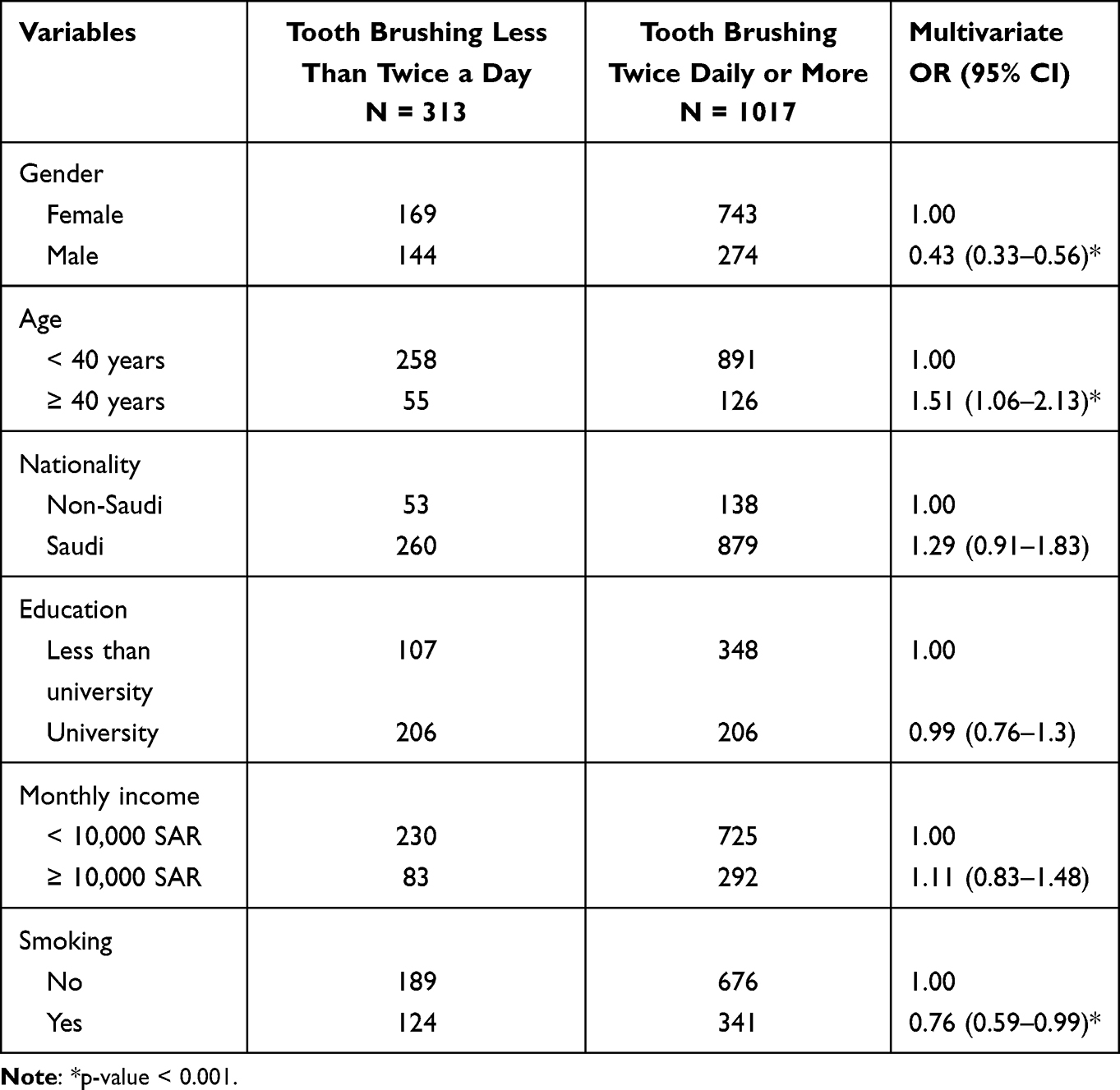 |
Table 5 Predictors of Oral Hygiene Behavior |
Discussion
Good oral health knowledge is considered a key factor in developing healthy and positive attitudes toward oral health. This study was conducted on 1330 randomly selected adults from Jeddah, Saudi Arabia. Our results demonstrated a significant difference between the knowledge and attitudes of females and males regarding oral health.
The results revealed that females had better knowledge than males regarding high sugar intake, which can lead to dental caries. This is consistent with previous studies’ results that showed that females have better knowledge about sugar consumption and its relationship with dental caries.21,22 This might be because females tend to care more about their health than males. Thus, females are more likely to follow a diet to control their weight and oral health, as they believe that healthy food choices are better for their general and oral health.24,25 In addition, the current study showed that females exhibited better knowledge regarding teeth brushing frequency and the proper use of a dental brush, similar to the results of previous studies.13,17,19 This result may be due to females caring more about aesthetics and appearances. Therefore, they visited the dentist more frequently. This could help them acquire more knowledge and proactive attitudes toward oral health.
Furthermore, the results indicated that socioeconomic level is associated with oral health knowledge. An individual’s knowledge of oral health is likely to be higher if they have a high level of education. This finding concurs with those obtained in other countries and populations.26–29 A study conducted in 2019 revealed that middle-aged Chinese adults’ level of education and oral health knowledge was significantly related.30 It has been known that people with low levels of education are more prone to experiencing issues with oral health.29,31 A complex web of factors has contributed to oral health disparities, such as healthcare utilization and access to dental care.32 The relation between oral health knowledge and level of education suggests that dentists should consider various factors beyond gender when assessing a patient’s oral health knowledge. In addition, it is suggested that oral health programs be targeted at groups with lower levels of education.
Additionally, oral health practices were associated with gender. Based on the study, the likelihood of females brushing their teeth, using mouthwash, and visiting the dentist for check-ups was higher than their male counterparts. The positive attitudes of females toward their oral health are in line with a US study comparing the oral health behaviors of females and males.28 The American Dental Association (ADA) recommends regular visits to check for signs of other conditions and to prevent dental disease. Previous studies have shown that males, people with low incomes, and people who fear dentists visit the dentists less often.29 The current study confirmed that males visit dentists less often than females and are more likely to seek dental care for acute conditions, such as pain, while females visit dentists more frequently for check-ups. This mirrors the findings of other studies that suggest men are less likely to visit dentists for preventive care.30,31 Several factors could explain such differences in oral health care utilization. One explanation could be that males’ stereotypical masculine attitudes could negatively affect their health-seeking behaviors. The importance of self-reliance, emotional control, and physical toughness in males are all factors that prevent them from seeking help from health professionals.31 Thus, it should not be surprising that men do not use dental services as often as females. On the contrary, females are more likely to believe that their oral health impacts their well-being, appearance, and quality of life than males.28 Consequently, females place a greater emphasis on preventive care and are more willing to visit dentists.
This study highlighted that older individual (40 years and above) are less likely to brush their teeth more frequently. This result is consistent with studies conducted in Mexico and Hong Kong that showed a low frequency of tooth brushing among the elderly population.33,34 Meanwhile, an analysis of 60-year-old participants in a study carried out in Nigeria estimated that 82% brush their teeth twice a day.35 The results of the studies may differ for various reasons, including methodology, population, and case definition. Regular tooth brushing is one of the most effective ways to maintain oral health. This is a public health action that various international and national organizations recommend. It is believed that tooth brushing helps support the oral health of older adults by stimulating the salivary flow rate, consequently improving oral equilibrium, preserving the tooth and periodontal health, and reducing tooth loss in older adults.36,37 Studies have shown that natural tooth loss causes a decline in tooth brushing frequency. A new survey of older adults revealed that those with functional dentition had a higher frequency of tooth brushing.34 As people get older, they lose interest in maintaining their oral health. This is because they start to not care about the potential consequences of a disease. Since oral diseases are associated with a low mortality rate, many never even consider such a possibility.34
Smoking was a significant determinant of oral health knowledge and practice. In the current study’s sample, individuals who smoked had lower knowledge scores and were less likely to brush their teeth more than twice a day. This agrees with a Swedish study that concluded regular dental care and anxiety were associated with smoking.38 Another study in South Korea found that tooth brushing frequency was lower in smokers than in nonsmokers.39 Smoking is associated with poor oral health and can also be considered a measure of health behavior.2 Oral health programs should focus on smoking cessation. Furthermore, through primary prevention, dentists can play a role in the fight against tobacco use by providing behavioral counseling and supporting legal reforms to prevent people from smoking.
Several limitations should be taken into consideration in this study. First, because the study is cross-sectional, it can only show associations, not cause-and-effect relationships. Second, the snowball sampling strategy and the use of a self-administered questionnaire are subject to recall bias. Third, most respondents were females (68%) compared to males (31%). This made the study prone to selection bias and could affect the gender comparison, limiting the ability to generalize the results to the entire population. However, this gender-based difference in responses to surveys is supported by Rübsamen et al’s findings.40 Finally, the use of social media can also affect the study’s results. For instance, it is likely that individuals who use social media know more about oral health compared to those who do not.
This study serves as a basis for obtaining new information regarding the knowledge and practices among adults concerning oral care and identifying predictors related to their oral health knowledge and practice. Therefore, the results helped identify risk groups and improve adult oral health promotion strategies. Both policymakers and government agencies need to coordinate their efforts to enhance the participation and awareness of the public about the importance of oral health. Moreover, the government should continue providing financial assistance to the adult population and monitor their oral health. It is also recommended that policymakers encourage health professionals to establish educational programs promoting healthy oral habits. These community-based programs could help decrease the prevalence of oral diseases. In addition, adults should be taught about the importance of maintaining their oral hygiene and seeking preventive dental care. Future studies should be conducted on a wider Saudi Arabian population, especially among individuals with lower socioeconomic status.
Conclusion
The study of adult population revealed that the knowledge and practices of females regarding oral health are better than those of males in Saudi Arabia. We believe that there is a need to implement effective campaigns to increase the awareness of males about the importance of oral health.
Acknowledgments
The author would like to thank all the participants for their valuable contributions. Special thanks for the dental interns, Alya Balbuid, Dalia Zarzar, Rahaf Mandoura and Israa Saleem for their efforts in data collection.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Alshahrani S, Alshuaibi A, Alkhaldi M, Koppolu P. Perception and knowledge of patients from different regions in the kingdom of Saudi Arabia towards oral hygiene and oral hygiene aids. Healthcare. 2021;9(5):592. doi:10.3390/healthcare9050592
2. Petersen P, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bull World Health Organ. 2005;83(9):661–669.
3. Global burden of disease collaborative network. Global burden of disease study 2019 (GBD 2019). Seattle: Institute of Health Metrics and Evaluation (IHME); 2020. Available from: http://ghdx.healthdata.org/gbd-results-tool.
4. Hobdell M, Petersen P, Clarkson J, Johnson N. Global goals for oral health 2020. Int Dent J. 2020;53(5):285–288. doi:10.1111/j.1875-595x.2003.tb00761.x
5. Varghese C, Jesija J, Prasad J, Pricilla R. Prevalence of oral diseases and risks to oral health in an urban community aged above 14 years. Indian J Dent Res. 2019;30(6):844–850. doi:10.4103/ijdr.IJDR_42_18
6. Peres M, Macpherson L, Weyant R, et al. Oral diseases: a global public health challenge. Lancet. 2019;394(10194):249–260. doi:10.1016/S0140-6736(19)31146-8
7. Elani H, Harper S, Allison P, Bedos C, Kaufman J. Socio-economic inequalities and oral health in Canada and the United States. J Dent Res. 2012;91(9):865–870. doi:10.1177/0022034512455062
8. Almutlaqah M, Baseer M, Ingle N, Assery M, Al Khadhari M. Factors affecting access to oral health care among adults in Abha city, Saudi Arabia. J Int Soc Prev Community Dent. 2018;8(5):431–438. doi:10.4103/jispcd.JISPCD_205_18
9. Zhu L, Petersen P, Wang H, Bian J, Zhang B. Oral health knowledge, attitudes and behaviour of adults in China. Int Dent J. 2005;55(4):231–241. doi:10.1111/j.1875-595x.2005.tb00321.x
10. Abbas Ali S, Sadatullah S, Ali A, Elmahdi A, Ibrahim W. Determinants of dental health care seeking behaviour in Aseer Province, Kingdom of Saudi Arabia. Ann Med Health Sci Res. 2020;10:1034–1039.
11. Wagle M, Trovik T, Basnet P, Acharya G. Do dentists have better oral health compared to general population: a study on oral health status and oral health behavior in Kathmandu, Nepal. BMC Oral Health. 2014;14:1–8. doi:10.1186/1472-6831-14-23
12. Farsi N, Merdad Y, Mirdad M, et al. Oral health knowledge, attitudes, and behaviors among university students in Jeddah, Saudi Arabia. Clin Cosmet Investig Dent. 2020;12:515–523. doi:10.2147/CCIDE.S272986
13. Halboub E, Dhaifullah E, Yasin R. Determinants of dental health status and dental health behavior among Sana’a University students, Yemen. J Investig Clin Dent. 2013;4(4):257–264. doi:10.1111/j.2041-1626.2012.00156.x
14. Peltzer K, Pengpid S. Oral health behaviour and social and health factors in university students from 26 low, middle and high income countries. Int J Environ Res Public Health. 2014;11(12):12247–12260. doi:10.3390/ijerph111212247
15. Peltzer K, Pengpid S. Dental health status and oral health behavior among university students from five ASEAN countries. Nagoya J Med Sci. 2017;79(2):123–133. doi:10.18999/nagjms.79.2.123
16. Togoo R, Yaseen S, Al Zamzami M. Oral hygiene knowledge and practices among school children in a rural area of southern Saudi Arabia. Int J Contemp Dent. 2012;3(1):57–62.
17. Al-Omari Q, Hamasha A. Gender-specific oral health attitudes and behavior among dental students in Jordan. J Contemp Dent Pract. 2005;6(1):107–114. doi:10.5005/jcdp-6-1-107
18. Riad A, Buchbender M, Howaldt HP, Klugar M, Krsek M, Attia S. Oral health knowledge, attitudes, and behaviors (KAB) of German dental students: descriptive cross-sectional study. Front Med. 2022;9:852660. doi:10.3389/fmed.2022.852660
19. Gharbieh E, Saddik B, Faramawi M, Hamidi S, Basheti M, Basheti M. Oral health knowledge and behavior among adults in the United Arab Emirates. BioMed Res Int. 2019;2019:7568679. doi:10.1155/2019/7568679
20. Al Rasheed N, Shetty A. Oral health knowledge among female primary school teachers in Riyadh city, Kingdom of Saudi Arabia. Int J Appl Dent Sci. 2017;3(4):164–170.
21. Elrashid A, Al-Kadi R, Baseer M, Rahman G, Alsaffan A, Uppin R. Correlation of sociodemographic factors and oral health knowledge among residents in Riyadh city, Kingdom of Saudi Arabia. J Oral Health Community Dent. 2018;12(1):8–13. doi:10.5005/jp-journals-10062-0018
22. Ahmad M, Bhayat A, Al-Samadani K, Abuong Z. Oral health knowledge and practice among administrative staff at Taibah university, Madina, KSA. Eur J Gen Dent. 2016;2(3):308–311.
23. Buunk-Werkhoven Y, Dijkstra A, Van Der Schans C. Determinants of oral hygiene behavior: a study based on the theory of planned behavior. Community Dent Oral Epidemiol. 2011;39(3):250. doi:10.1111/j.1600-0528.2010.00589.x
24. Zumbo G, Costacurta M, Zara F, et al. Diet implications and oral health status of women in central Italy. Eur J Dent. 2021;(1). doi:10.1055/s-0041-1735906
25. Mazur M, Bietolini S, Bellardini D, et al. Oral health in a cohort of individuals on a plant-based diet: a pilot study. Clin Ter. 2020;171(2):e142–e148. doi:10.7417/CT.2020.2204
26. Marquez-Arrico C, Almerich-Silla J, Montiel-Company J. Oral health knowledge in relation to educational level in an adult population in Spain. J Clin Exp Dent. 2019;11(12):e1143–e1150. doi:10.4317/jced.56411
27. Batista M, Lawrence H, Sousa M. Oral health literacy and oral health outcomes in an adult population in Brazil. BMC Public Health. 2018;18(1):60. doi:10.1186/s12889-017-4443-0
28. Mohammadi T, Malekmohammadi M, Hajizamani H, Mahani R. Oral health literacy and its determinants among adults in Southeast Iran. Eur J Dent Educ. 2018;12(3):439–442. doi:10.4103/ejd.ejd_429_17
29. Jones M, Lee J, Rozier R. Oral health literacy among adult patients seeking dental care. J Am Dent Assoc. 2007;138:1199–1208. doi:10.14219/jada.archive.2007.0344
30. Ho M, Liu M, Chang C. A preliminary study on the oral health literacy and related factors of community mid-aged and older adults. J Nurs. 2019;66(1):38–47. doi:10.6224/JN.201902_66(1).06
31. Guo Y, Logan H, Dodd V, Muller K, Marks J, Riley J. Health literacy: a pathway to better oral health. Am J Public Health. 2014;104(7):85–91. doi:10.2105/AJPH.2014.301930
32. Sabbah W, Tsakos G, Sheiham A, Watt R. The role of health-related behaviors in the socioeconomic disparities in oral health. Soc Sci Med. 2009;68(2):298–303. doi:10.1016/j.socscimed.2008.10.030
33. Chu C, Ng A, Chau A, Lo E. Oral health status of elderly Chinese with dementia in Hong Kong. Oral Health Prev Dent. 2015;13(1):51–57. doi:10.3290/j.ohpd.a32343
34. Islas-Granillo H, Casanova-Rosado J, De La Rosa-Santillana R, et al. Self-reported oral hygiene practices with emphasis on frequency of tooth brushing: a cross-sectional study of Mexican older adults aged 60 years or above. Medicine. 2020;99(36):e21622. doi:10.1097/MD.0000000000021622
35. Olusile A, Adeniyi A, Orebanjo O. Self-rated oral health status, oral health service utilization, and oral hygiene practices among adult Nigerians. BMC Oral Health. 2014;14:140. doi:10.1186/1472-6831-14-140
36. Affoo R, Trottier K, Garrick R, Mascarenhas T, Jang Y, Martin R. The effects of tooth brushing on whole salivary flow rate in older adults. Biomed Res Int. 2018;2018:3904139. doi:10.1155/2018/3904139
37. Bando S, Tomata Y, Aida J, Sugiyama K, Sugawara Y, Tsuji I. Impact of oral self-care on incident functional disability in elderly Japanese: the Ohsaki Cohort 2006 study. BMJ Open. 2017;7(9):e017946. doi:10.1136/bmjopen-2017-017946
38. Carlsson V, Hakeberg M, Wide Boman U. Associations between dental anxiety, sense of coherence, oral health-related quality of life and health behavior–a national Swedish cross-sectional survey. BMC Oral Health. 2015;15:100. doi:10.1186/s12903-015-0088-5
39. Park J, Han K, Park Y, Ko Y. Association between socioeconomic status and oral health behaviors: the 2008–2010 Korea national health and nutrition examination survey. Exp Ther Med. 2016;12(4):2657–2664. doi:10.3892/etm.2016.3679
40. Rubsamen N, Akmatov M, Castell S, Karch A, Mikolajczyk R. Comparison of response patterns in different survey designs: a longitudinal panel with mixed-mode and online-only design. Emerg Themes Epidemiol. 2017;14:4. doi:10.1186/s12982-017-0058-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Physicians’ Knowledge and Practices Regarding Asthma: A Cross-Sectional Study in Saudi Arabia
Dairi MS
International Journal of General Medicine 2022, 15:6671-6680
Published Date: 19 August 2022
The Effect of an Education Program on School Children Oral Health in Khartoum, Sudan
Albani GFAA, Abdelgadir WI, Mohamed AAA, Yousif M, Mustafa AMA, Almkiy EAA, Mohammed KZM, Mohamed EAS, Alghamdi FAA, Ahmed RG, Hakami MSA, Dinar NA, Alsulami A, Mudawi AIA, Ahmed WAM
Journal of Multidisciplinary Healthcare 2024, 17:1065-1077
Published Date: 12 March 2024
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024
Knowledge, Attitude and Practice Towards Hepatitis B Infection and HBV Vaccine Among the Healthy Population in Makkah, Saudi Arabia
Almalki F, Alraffah YM, Alasiri RA, Dhafar MW, Albogami FM, Alhazmi MN, Alyazidi AM, Alharbi LA, Alotaibi ME
Infection and Drug Resistance 2025, 18:2153-2164
Published Date: 28 April 2025
The Knowledge-Attitude-Behavior Paradox in E-Cigarette Adoption Among University Students at Northern Border University, Saudi Arabia
Alenezi IN, Mersal FA, Osman Mohamed HA, El Said FG, Alanazi FJ, Abu-Negm LM, Aboelola TH, Alrwili AG
Journal of Multidisciplinary Healthcare 2026, 19:578360
Published Date: 18 February 2026