Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Gastrointestinal Adverse Effects of GLP-1 and Dual GLP-1/GIP Receptor Agonists: A Comprehensive Update in Diabetic and Obese Populations
Authors Yılmaz N ![]() , Bastemir M
, Bastemir M ![]()
Received 27 November 2025
Accepted for publication 13 January 2026
Published 30 January 2026 Volume 2026:19 584175
DOI https://doi.org/10.2147/DMSO.S584175
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Halis Akturk
Nimet Yılmaz,1 Mehmet Bastemir2
1Department of Gastroenterology, SANKO University Faculty of Medicine, Gaziantep, Turkey; 2Department of Endocrinology, SANKO University Faculty of Medicine, Gaziantep, Turkey
Correspondence: Nimet Yılmaz, Department of Gastroenterology, SANKO University Faculty of Medicine, Gaziantep, Turkey, Email [email protected]
Background: Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) and dual GLP-1/GIP receptor agonists are highly effective agents for the treatment of type 2 diabetes and obesity. However, gastrointestinal (GI) adverse events remain the most common limitations to long-term therapy.
Methods: A narrative review with a structured literature search was conducted using PubMed, Embase, and Cochrane Library databases from inception to March 2025. Randomized controlled trials, observational studies, meta-analyses, and pharmacovigilance reports evaluating GI adverse effects of GLP-1–based therapies were included.
Results: Nausea, vomiting, diarrhea, and constipation were the most frequently reported GI adverse events, generally dose-dependent and transient. Delayed gastric emptying, gastroparesis-like symptoms, intestinal obstruction, biliary disease, and pancreatic safety concerns were variably reported, with heterogeneous and sometimes conflicting evidence across studies.
Conclusion: GLP-1–based therapies are associated with predictable GI adverse effects, most of which are mild to moderate and manageable. Serious complications appear rare, but evidence remains inconsistent. Individualized risk assessment, patient education, and careful dose titration are essential for optimizing long-term tolerability.
Keywords: glucagon-like peptide-1 receptor agonist, obesity, type 2 diabetes, gastrointestinal adverse events
Introduction
Diabetes and obesity are increasing at an alarming rate worldwide and placing a significant burden on global healthcare systems. When lifestyle interventions such as diet and exercise prove insufficient, pharmacological treatments play a crucial role. Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have transformed the treatment of obesity and type 2 diabetes mellitus (T2DM) by mimicking endogenous GLP-1 activity, increasing glucose-dependent insulin secretion and suppressing glucagon release.1 These agents also delay gastric emptying and reduce appetite via central mechanisms, thereby contributing to their metabolic effects.1,2 Initially developed as antidiabetic treatments, GLP-1 RAs and, more recently, dual glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 receptor agonists have demonstrated favourable metabolic outcomes with significant and sustainable weight loss in large randomised controlled trials (RCTs) and real-world studies.3,4 Consequently, their use has rapidly become widespread in clinical practice. Despite their efficacy, the safety profiles of GLP-1-based therapies continue to be actively investigated.5 Gastrointestinal (GI) adverse events are the most commonly reported side effects in both clinical trials and real-world cohorts and typically occur at the start of treatment or during dose escalation. Common symptoms include nausea, vomiting, abdominal pain, diarrhoea, and constipation, which are generally mild to moderate in severity and tend to improve over time. However, these symptoms can negatively affect treatment adherence, quality of life, and discontinuation rates, thereby impacting long-term treatment success.6–8 Furthermore, the potential association between GLP-1 RA use and more serious GI complications such as acute pancreatitis, cholelithiasis, and bowel obstruction remains controversial due to inconsistent findings in observational studies and meta-analyses.9–12 As these treatments are often prescribed for long-term use and are increasingly used for off-label indications, a clear understanding of their GI safety profiles is crucial for informed clinical decision-making.
In this narrative review, we summarise the current evidence on approved GLP-1 RAs and GIP/GLP-1 RAs for T2DM and obesity, focusing on GI adverse events, their frequencies, underlying mechanisms, and clinical significance. Furthermore, to provide clinicians with an up-to-date and clinically useful resource to support their daily practice, we discuss practical strategies for the prevention and management of GI adverse events.
Methods
Literature Search Strategy
This narrative review was conducted using a structured literature search strategy. PubMed, Embase, and the Cochrane Library were searched using keyword combinations related to GLP-1 receptor agonists, dual GLP-1/GIP agonists, and GI adverse events, from the inception of the database up to March 2025.
Data Sources and Eligibility Criteria
Eligible studies included RCTs, observational cohort studies, meta-analyses, and large pharmacovigilance analyses published in English. The literature search and data extraction were performed by the authors. Given the narrative nature of this review, a double-blind screening process was not applied, which is acknowledged as a limitation.
Study Selection and Quality Assessment
The search was limited to human studies in adults (≥18 years) and articles published in English or Turkish. Case reports, very small case series (<10 patients), conference abstracts without full texts, non-systematic narrative reviews, editorials, and letters were excluded. GLP-1 RAs approved by the US Food and Drug Administration (FDA) for T2DM and obesity (semaglutide, exenatide, liraglutide, tirzepatide, dulaglutide) were included in the analysis.
Studies examining GLP-1 RAs that were withdrawn from the market due to safety concerns related to GI adverse effects were also excluded. Reference lists of key articles and major clinical practice guidelines were manually screened to identify any additional relevant studies. When multiple publications originated from the same clinical research program, the most recent or most comprehensive report was used as the primary source.
Physiology of Incretins
GLP-1 and GIP are incretin hormones secreted from the intestine in response to food intake and stimulate glucose-dependent insulin release, β-cell proliferation, and cellular survival. Unlike GLP-1, GIP suppresses glucagon secretion under hyperglycemic conditions; however, it enhances glucagon release during normoglycemia or hypoglycemia. GLP-1 is one of the key hormonal components of the intestinal traffic control mechanism known as the “ileal brake,” which regulates the rate of nutrient transit and absorption. These effects help prevent the rapid rise in insulin secretion associated with hyperglycemia by allowing nutrients to enter the circulation more slowly and consistently. GLP-1, secreted by the intestine, brainstem, and pancreas, also exerts appetite-suppressing and gastric emptying-delaying effects on the hypothalamus.
All these properties make GLP-1 a potent anti-diabetic agent; however, the very short half-life of endogenous GLP-1 (1–2 minutes) has limited its therapeutic use. Nonetheless, the same mechanisms—particularly delayed gastric emptying and central satiety signals—also underlie a wide spectrum of GI side effects, ranging from mild and transient symptoms to clinically significant complications such as gastroparesis and acute pancreatitis.2
In 1980, Jean-Pierre Raufman identified an animal venom capable of stimulating increased digestive enzyme secretion from the pancreas and exhibiting properties similar to GLP-1. This molecule, termed “exendin-4,” was found in the saliva of a lizard species known as the Heloderma suspectum. The ability of this desert-dwelling animal to consume half its body weight in food in a single sitting while maintaining stable blood sugar levels and proper metabolic function caught the attention of researchers and ultimately led to a series of studies that resulted in the development of GLP-1 receptor agonists.1
Clinical Use of GLP-1 and GLP-1/GIP RAs
Approved Agents and Dosing
GLP-1 RAs have a relatively long half-life of approximately one week. They increase glucose-dependent insulin secretion, suppress glucagon release, and slow gastric emptying by activating specific receptors in the gut and hypothalamus, thereby suppressing appetite and contributing to weight loss. Figure 1 summarizes a conceptual overview rather than a single experimental model, developed on the basis of published evidence, with the aim of facilitating the understanding of central and peripheral pathways involved in the GI effects associated with GLP-1 receptor agonists.
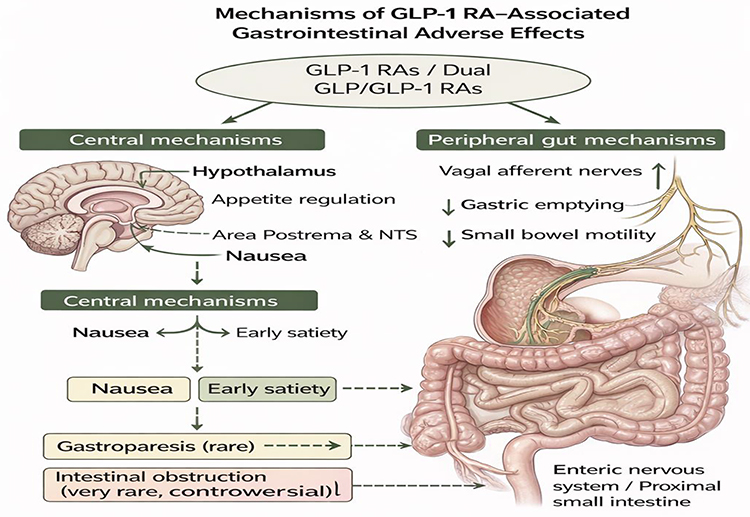 |
Figure 1 Mechanisms underlying gastrointestinal adverse effects of GLP-1 receptor agonists. This figure presents a conceptual overview of the central and peripheral pathways involved in gastrointestinal effects associated with GLP-1 receptor agonists, based on established physiological evidence. Central mechanisms include hypothalamic and brainstem pathways regulating appetite and nausea, while peripheral mechanisms involve vagal afferent signaling, delayed gastric emptying, and reduced intestinal motility. These pathways contribute to commonly reported symptoms such as nausea, reduced appetite, early satiety, and constipation, as well as less frequent outcomes including gastroparesis and intestinal obstruction. |
Dual agonists that activate both GLP-1 and GIP receptors have been shown to provide more pronounced weight loss, better glycemic control, and better metabolic outcomes compared to GLP-1 RAs alone.3
GLP-1 RAs are typically administered using prefilled single-use injection pens, with injections given in the abdomen, thigh, or upper arm. Titration schedules are generally planned to minimize early GI side effects. Treatment typically begins with a low dose and is gradually increased at weekly or biweekly intervals.
In recent years, long-acting GLP-1 RAs such as liraglutide, dulaglutide, semaglutide, and the dual GIP/GLP-1 receptor agonist tirzepatide have become widely used. In contrast, short-acting formulations such as exenatide and the older-generation agent lixisenatide are now prescribed far less frequently, and several formulations have been withdrawn from the market in certain countries, largely due to limited clinical uptake, the availability of more effective long-acting alternatives, and commercial considerations rather than confirmed safety concerns.1
Following FDA approval of liraglutide, semaglutide, and tirzepatide for chronic weight management, prescription rates have increased rapidly. FDA-approved GLP-1 and dual GIP/GLP-1 receptor agonists, their indications, formulations and dosing regimens are summarized in Table 1.
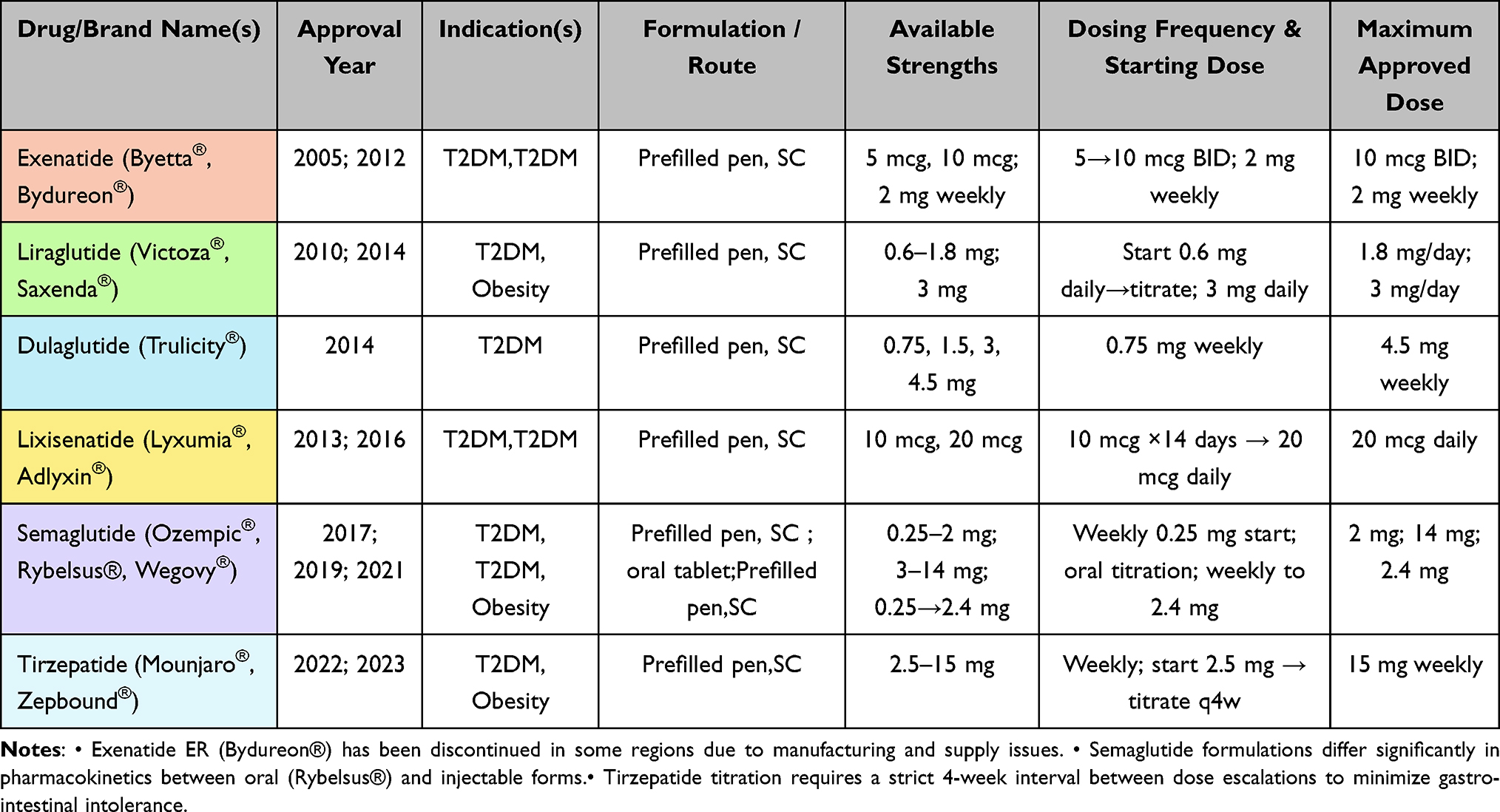 |
Table 1 Characteristics of GLP-1 and GIP/GLP-1 Receptor Agonists |
Antidiabetic Efficacy and Outcomes
GLP-1 RAs bind to GLP-1 receptors located on pancreatic β-cells, increasing glucose-dependent insulin secretion and thereby improving both postprandial and overall glycemic control without significantly increasing the risk of hypoglycemia. Because this effect is entirely glucose-dependent, insulin secretion decreases as plasma glucose approaches normal levels, providing a significant safety advantage over traditional secretagogues.
A systematic review and meta-analysis by Yao et al demonstrated that GLP-1 RAs were superior to placebo in reducing hemoglobin A1c (HbA1c) and fasting plasma glucose levels in patients with T2DM. Notably, tirzepatide showed greater HbA1c reductions compared with other GLP-1 RAs, supported by high-certainty evidence.13 These findings are consistent with results from the SURPASS-1 trial, in which tirzepatide at all studied doses significantly improved HbA1c over 40 weeks without increasing hypoglycemia risk.14 Further evidence from Phase 3 RCTs supports these findings. In a large RCT involving obese and prediabetic individuals, tirzepatide significantly delayed the onset of T2DM compared with placebo across multiple doses, with sustained benefits observed during long-term follow-up.15 Additionally, head-to-head comparisons with semaglutide demonstrated superior HbA1c reductions with tirzepatide at 40 weeks,16 findings that were later confirmed in subsequent phase 3 trials and meta-analyses.17 Similarly, in a meta-analysis of 14 RCTs in T2DM patients conducted by Liu et al, tirzepatide was shown to provide superior HbA1c reduction and improved metabolic outcomes compared to placebo, insulin, and all other GLP-1 RAs at all doses examined.18
Despite the overall consistency in demonstrating the glycemic efficacy of GLP-1 RAs and dual GIP/GLP-1 receptor agonists, substantial heterogeneity exists across studies. This heterogeneity may be attributed to differences in baseline HbA1c levels, obesity prevalence, trial duration, comparator treatments, dosing strategies, and outcome definitions. Moreover, variability in study populations and healthcare settings limits the direct comparability of results and may influence the magnitude of observed treatment effects.
In addition to heterogeneity, potential sources of bias must be considered, particularly in observational studies assessing treatment persistence and real-world effectiveness. Such studies are inherently susceptible to confounding by socioeconomic status, access to healthcare, reimbursement policies, and patient adherence, all of which may significantly impact treatment continuation and metabolic outcomes. Importantly, while RCTs consistently demonstrate robust short-term glycemic improvements, real-world data suggest that long-term treatment continuity remains a major challenge. A large observational cohort study reported that nearly half of patients discontinued GLP-1 RA therapy within one year, with lower income significantly associated with discontinuation.19 This discrepancy highlights the gap between efficacy observed in controlled trial settings and effectiveness in routine clinical practice.
Finally, the increasing off-label use of GLP-1 RAs for weight loss in non-diabetic individuals may further exacerbate access limitations and drug shortages, potentially disadvantaging patients with T2DM. The lack of reimbursement in some healthcare systems represents an additional structural barrier to equitable access. Addressing these economic and systemic challenges is essential to maximize the long-term benefits of GLP-1 RA therapy and improve outcomes in diabetes management.
Weight Reduction Mechanisms and Outcomes
The weight-reducing effects of GLP-1 RAs are primarily attributed to reduced food intake rather than increased energy expenditure. These agents are known to decrease food intake and promote weight loss through delayed gastric emptying, enhanced satiety, and appetite suppression. Additionally, evidence suggests that they may facilitate fat-based weight reduction by influencing adipose tissue metabolism and inflammatory processes.20 From the outset, the primary objective has been for GLP-1 RA–induced weight loss to originate predominantly from fat mass while preserving lean body mass. Consistent with this expectation, Argyrakopoulou et al reported that in a cohort of obese individuals treated with liraglutide, the dominant change was a reduction in fat mass, accompanied by only a minimal decline in lean mass.21 Similarly, Wilding et al demonstrated that in overweight or obese participants receiving 2.4 mg semaglutide, both total and regional visceral fat mass decreased, whereas lean body mass increased.22 More recent research indicates that tirzepatide induces greater reductions in total and visceral fat mass compared with other GLP-1 RAs.23,24 In a network meta-analysis, Karakasis et al found that 15 mg tirzepatide and 2.4 mg semaglutide were the most effective agents for reducing body weight and fat mass; however, they were among the least effective in preserving lean mass, with lean mass loss contributing to approximately 25% of total weight reduction.25 Given concerns that skeletal muscle loss may predispose patients to long-term metabolic complications, including sarcopenia, it is recommended that individuals undergoing treatment with GLP-1 RAs receive adequate protein intake and appropriate micronutrient supplementation to preserve muscle mass and function, thereby maximizing the clinical benefits of therapy.26
The weight-loss effects of GLP-1 RAs have been attributed not only to appetite-suppressing mechanisms but also to increased energy expenditure through activation of hindbrain pathways and stimulation of thermogenesis in brown adipose tissue.27 However, contrary to preclinical findings, human studies indicate that weight loss induced by GLP-1 RAs is primarily due to reduced energy intake rather than increased energy expenditure. In a 26-week study of obese and T2DM patients treated with 1.8 mg liraglutide once daily, van Eyk et al demonstrated an average weight loss of 4.3 kg. This weight reduction was primarily explained by decreased caloric intake rather than an increase in resting energy expenditure.28 The efficacy of semaglutide in obesity treatment has been demonstrated in the STEP program.29 In a study involving 1,306 overweight or obese individuals receiving 2.4 mg of semaglutide, approximately 6% and 12% weight loss was observed at 12 and 28 weeks, respectively, and total fat mass decreased by approximately 20% after 56 weeks of treatment.4 The weight-loss efficacy of tirzepatide in both diabetic and non-diabetic individuals has been shown in the SURMOUNT trials.30,31 In the SURMOUNT-1 study, among obese participants, the mean weight loss at week 72 with tirzepatide monotherapy was 15.0%, 19.5%, and 20.9% for the 5, 10, and 15 mg groups, respectively, compared with 3.1% with placebo (all comparisons P<0.001).32 In the extension phase, changes in body weight from baseline to week 176 were –12.3%, –18.7%, and –19.7% in the 5, 10, and 15 mg tirzepatide groups, respectively, compared with –1.3% with placebo (all P<0.001), demonstrating that tirzepatide produces clinically meaningful and sustained weight loss over three years in overweight or obese individuals.15
In the SURPASS-1 study, tirzepatide monotherapy at increasing doses of 5, 10, and 15 mg resulted in significant weight loss of 7, 7.8, and 9.5 kg, respectively, at week 40 in patients with T2DM, compared with a 0.7 kg decrease with placebo.14 However, in two studies that included participants not enrolled in the SURPASS and SURMOUNT studies, ie, a large number of individuals who switched from other GLP-1 RAs to tirzepatide, those who transitioned from semaglutide experienced greater weight loss with tirzepatide treatment.33,34 Head-to-head data directly comparing GLP-1 RAs in obesity remain limited. In a large cohort study from the United States involving more than 18,000 overweight or obese individuals, Rodriguez et al reported that the average weight loss after one year was 8.3% with semaglutide and 15.3% with tirzepatide.35 Similarly, in a recent study of obese individuals without diabetes, Louis et al demonstrated that tirzepatide (10 or 15 mg) resulted in significantly greater weight loss than semaglutide (1.7 or 2.4 mg) over a 72-week period. The mean body weight changes were –20.2% (95% CI –21.4 to –19.1) and –13.7% (95% CI –14.9 to –12.6), respectively (P<0.001).36 Several other recent studies also confirmed that tirzepatide treatment is superior to other GLP-1 RAs and placebo in promoting meaningful weight loss.37–39
While it is encouraging that the weight loss achieved with GLP-1/GIP–GLP-1 receptor agonists approaches levels typically seen after bariatric procedures such as gastric bypass or sleeve gastrectomy, the rapid regain of a significant portion of the lost weight after treatment discontinuation, accompanied by a reduction in lean body mass, raises new clinical concerns.40 In one study, patients who discontinued semaglutide regained approximately 68% of their initial weight loss within one year, resulting in a net weight loss of only 5.6%.41 Similarly, Aronne et al reported that in overweight or obese individuals, most of the weight lost during tirzepatide therapy was regained after treatment discontinuation; however, continuation of treatment preserved weight loss and further increased total weight reduction.42 In the STEP 1 study, participants who achieved a mean weight loss of 10.6% after 20 weeks of semaglutide were rerandomized in STEP 4 to either continue semaglutide or switch to placebo for an additional 48 weeks. Those who switched to placebo regained approximately 7% of their body weight, whereas those continuing semaglutide treatment lost an additional 3%.43 Therefore, discontinuation of treatment—primarily due to cost and access limitations—remains the major barrier to the widespread and sustainable use of these agents.
Gastrointestinal Side Effects
Although studies on GLP-1 RAs clearly demonstrate substantial clinical benefits, their short- and long-term safety profiles have not yet been fully elucidated. In particular, RCTs conducted for weight loss indications are often of limited duration and therefore may be insufficient to reliably detect rare or delayed adverse events. As a result, the long-term GI safety of these agents continues to be actively investigated. Although proven effective, GLP-1 RAs have been associated with numerous GI adverse events. These events have been seen as important factors affecting patient satisfaction, treatment compliance and continuation of treatment. Importantly, the declining use or market withdrawal of earlier GLP-1 RAs does not necessarily reflect an unfavorable GI safety profile. Nevertheless, understanding GI adverse events across both earlier and newer GLP-1–based therapies remains highly relevant, particularly as these agents are increasingly prescribed for long-term and off-label indications.
Upper/Lower Gastrointestinal Symptoms
Adverse event reporting databases, RCTs, and real-world data consistently show that GLP-1 RAs are commonly associated with GI symptoms such as nausea, vomiting, diarrhea, constipation, abdominal pain, and dyspeptic complaints. These symptoms typically appear shortly after treatment initiation or following a dose increase; they generally improve within a relatively short timeframe once the maintenance dose is reached.44,45 In a meta-analysis of 48 RCTs including 27,729 participants, the overall incidence of GI adverse events was reported to be 11.6%, with nausea identified as the most common symptom (21.4%).46 In studies evaluating the efficacy and safety of GLP-1 RAs, nausea emerged as the most frequently reported GI symptom, generally following a dose-dependent pattern, appearing during the first weeks of therapy, and decreasing as tolerance developed. Diarrhea is also common but tends to be intermittent and typically resolves spontaneously, representing a short-term symptom. Conversely, constipation has been shown to persist longer than other GI side effects and is more frequently observed in obesity-focused studies. Abdominal pain and nonspecific dyspeptic complaints (bloating, gas, belching) are reported less frequently.22,32 In a large-scale real-world cohort study of more than 10,000 patients using a GLP-1 RA, abdominal pain was the most common symptom (57.6%), followed by constipation (30.4%), diarrhea (32.7%), and nausea/vomiting (23.4%). Importantly, these adverse events were generally mild to moderate in severity and rarely resulted in complications or permanent treatment discontinuation.7
In a survey involving 443 physicians, the reasons for discontinuing GLP-1 RAs were investigated in patients who had stopped treatment within the previous six months. Physicians most frequently cited GI side effects—particularly persistent nausea and vomiting—as the primary reasons for discontinuation.47 Another analysis reported that semaglutide use in individuals with T2DM increased the risk of developing GI adverse events by 2.14 times compared with control groups, although it was emphasized that the vast majority of these side effects were mild.48 Similarly, among obese individuals without diabetes, semaglutide use was shown to increase the risk of developing GI adverse events by 1.59 times compared with the control group.49 A recent systematic review and meta-analysis involving obese individuals without diabetes demonstrated that tirzepatide, semaglutide, liraglutide, and exenatide significantly increased the risk of GI adverse events compared with placebo. In this analysis, nausea, vomiting, diarrhea, and constipation were identified as the most frequently observed side effects. It was noted that belching complaints were more common among patients receiving liraglutide or semaglutide, whereas such an increase was not observed with exenatide or tirzepatide. Furthermore, the review showed that both semaglutide and tirzepatide significantly increased the risk of flatulence.50
A recent meta-analysis including thirteen RCTs has shown that semaglutide and tirzepatide treatment significantly increases GI side effects such as nausea, vomiting, diarrhea, and constipation in obese individuals without diabetes compared to control groups. It has been suggested that the higher risk observed with tirzepatide relative to semaglutide may be attributed to the use of higher doses of tirzepatide.51 Similarly, another meta-analysis demonstrated that patients with T2DM receiving higher doses of tirzepatide exhibited a greater risk of GI adverse events compared to those receiving lower doses, consistent with a clear dose–response relationship.52 In a large meta-analysis by Chiang et al involving 106,395 participants and 55 RCTs, GLP-1 RA therapy was associated with an increased risk of gastroesophageal reflux disease (GERD) compared to placebo, with a reported relative risk of 2.19 (95% CI: 1.48–3.25). Subgroup analyses indicated that this risk was particularly elevated in individuals receiving high-dose treatment, in studies of long-acting agents, and in overweight/obese populations.12 Consistent with these findings, Liu et al also reported that GLP-1 RA use was associated with an increased risk of erosive reflux disease (RR 1.15; 95% CI: 1.09–1.22) and Barrett’s esophagus. The authors attributed this increased risk to delayed gastric emptying, resulting in greater gastric volume and intra-gastric pressure and thereby contributing to acid reflux.53
Pancreatic and Hepatobiliary Events
Pancreatitis and Pancreatic Disorders
It has been suggested that GLP-1 RAs may influence pancreatic physiology through multiple mechanisms, including effects related to rapid weight loss and gallstone formation, which have been hypothesized to contribute indirectly to pancreatitis risk.54 Early observational studies raised concerns regarding a potential association between GLP-1 RA therapy and pancreatitis. For example, a population-based observational study reported a higher incidence of pancreatitis among obese individuals treated with semaglutide or liraglutide compared with those receiving naltrexone–bupropion.10 Additional observational analyses in patients with T2DM also suggested increased rates of pancreatitis and pancreatic cancer in GLP-1 RA users compared with other antidiabetic therapies.55,56 These findings prompted regulatory safety communications and heightened surveillance regarding pancreatic safety.57
However, subsequent evidence from large RCTs and real-world studies has not consistently confirmed a causal association between GLP-1 RA use and pancreatitis. Several large-scale RCTs and meta-analyses have reported no statistically significant increase in pancreatitis risk associated with GLP-1 RAs.12,58,59
In a comprehensive systematic review and meta-analysis including more than 34,000 patients with T2DM, semaglutide therapy was not associated with an increased risk of pancreatitis.60 These findings are supported by additional observational and real-world cohort studies demonstrating similar pancreatitis rates among patients treated with GLP-1 RAs and those receiving other glucose-lowering therapies.45,61–63
Notably, some recent population-based retrospective studies have even suggested a neutral or potentially lower risk of pancreatitis-related complications during follow-up among GLP-1 RA users after an initial episode of acute pancreatitis.64 Taken together, the current body of evidence suggests that while early observational signals raised concern, more robust and contemporary data do not demonstrate a consistent or clinically meaningful increase in pancreatitis risk associated with GLP-1 RA therapy.
Nonetheless, given the heterogeneity of available data and the presence of residual uncertainty, a cautious and individualized clinical approach remains warranted. A history of pancreatitis should prompt careful risk–benefit assessment and close monitoring rather than being considered an absolute contraindication to GLP-1 RA therapy. Ongoing large-scale prospective studies and post-marketing surveillance are needed to further refine risk estimates and inform evidence-based clinical guidance for patients at higher baseline risk.
Gallbladder and Biliary Tract Diseases
In addition to obesity, rapid and excessive weight loss is known to reduce gallbladder motility, alter bile composition, and thereby predispose individuals to gallstone formation.65 In a meta-analysis by He et al, which included 76 RCTs covering more than 100,000 overweight or obese individuals, GLP-1 RA use was reported to increase the risk of gallbladder stones or biliary tract disease by 37% (RR 1.37 [95% CI 1.23–1.52]). The study also indicated that GLP-1 RA treatment was associated with a moderately increased risk of gallstones (RR: 1.27, 95% CI 1.10–1.47), cholecystitis (RR: 1.36, 95% CI 1.14–1.62), and overall gallbladder disease risk (RR: 1.55, 95% CI 1.08–2.22) compared to placebo.9 Another study supporting these findings also associated GLP-1 RA treatments with a 46% higher risk of gallstones compared to placebo.12 A recent meta-analysis of 26,894 obese participants without diabetes showed that semaglutide use increased the risk of gallbladder stones by 2.6 times, while this risk was not evident for tirzepatide.51
In these studies, it has been reported that gallbladder stones and biliary tract diseases are more common in patients using GLP-1 RAs compared with placebo; furthermore, the risk increases with longer treatment durations, higher doses, and when these agents are used for weight loss. However, no significant increase in the risk of serious biliary tract disease has been observed. On the other hand, a nationwide cohort study showed that GLP-1 RA use in T2DM patients did not increase the risk of gallbladder or biliary tract diseases.66 In a randomized, controlled phase 3 study by Jastreboff et al, no difference in gallbladder stone rates was observed between 5, 10, and 15 mg tirzepatide treatment and placebo in obese individuals over 72 weeks.32 A recent systematic review and meta-analysis supporting these findings also showed that GLP-1 RA use was not associated with cholecystitis or gallstones in overweight/obese individuals without diabetes.50
Gastrointestinal Motility Disorders: Gastric and Intestinal Manifestations
GLP-1 RAs reduce GI motility and prolong intestinal transit time, effects that have raised concerns regarding an increased risk of gastroparesis, intestinal obstruction, or ileus. Several observational and real-world studies have reported associations between GLP-1 RA use and these motility-related complications.63,67 However, interpretation of these findings requires caution, as diagnostic confirmation of gastroparesis is challenging, and gastric emptying scintigraphy—the diagnostic gold standard—is not consistently performed in routine clinical practice. Some cohort studies have suggested an increased risk of intestinal obstruction among GLP-1 RA users. For example, a population-based cohort study in obese individuals without diabetes reported a fourfold increase in intestinal obstruction risk associated with GLP-1 RA use.10 Similarly, real-world analyses in patients with T2DM have demonstrated that the use of GLP-1 RAs is associated with a higher risk of gastroparesis (HR 1.591, P<0.001) and intestinal obstruction (HR 1.383, P=0.025) compared to oral antidiabetic therapy.63 In a large-scale real-world study, the use of GLP-1 receptor agonists in patients with T2DM was also shown to increase the risk of intestinal obstruction compared to sodium–glucose cotransporter-2 (SGLT-2) inhibitors. Furthermore, it was reported that this risk increases with the duration of exposure to GLP-1 receptor agonists, with the highest risk observed after 1.6 years.68 In contrast, other large-scale population-based studies have failed to demonstrate a significant increase in intestinal obstruction risk when GLP-1 RAs were compared with SGLT-2 inhibitors.69,70 Notably, findings from pharmacovigilance databases and real-world cohorts have been inconsistent, with some reports suggesting an association with specific agents, such as semaglutide, while others have not observed such relationships.71,72 From a clinical perspective, these conflicting data suggest that motility-related adverse events are uncommon but may occur in susceptible individuals, particularly with prolonged exposure or in the presence of pre-existing GI motility disorders. Differences in pharmacokinetic profiles among GLP-1 RAs may also contribute to variability in GI tolerability, with longer-acting agents generally associated with more persistent, though often less intense, symptoms compared with short-acting formulations. Beyond objective clinical outcomes, GI motility disturbances can substantially affect patient-reported outcomes, including daily functioning, dietary intake, and overall quality of life. Persistent nausea, early satiety, bloating, or constipation may lead to reduced treatment satisfaction and contribute to therapy interruption or discontinuation. These consequences may, in turn, increase healthcare utilization and associated costs through additional diagnostic testing, clinic visits, or hospitalizations. Taken together, current evidence indicates that while a definitive causal relationship between GLP-1 RA therapy and severe motility disorders has not been established, clinicians should remain vigilant for GI symptoms suggestive of delayed gastric emptying or obstruction. Individualized risk assessment, patient education, and prompt evaluation of persistent symptoms are essential to optimize treatment adherence and minimize potential clinical and economic consequences.
Clinical Management of Gastrointestinal Side Effects
GI side effects associated with GLP-1 RAs can be effectively managed with patient-centred strategies. Before initiating treatment, clinicians should provide patients with comprehensive counselling regarding the effects of the medication, possible GI symptoms, typical time course, and current management approaches. Ongoing communication between patients and healthcare providers is essential to monitor symptom severity, weight changes, glycemic control, and treatment tolerability. Collaboration with a registered dietitian may further support adherence, particularly in patients with maladaptive eating behaviors or unrealistic expectations regarding weight loss. For patients experiencing mild to moderate GI symptoms, initial management should focus on non-pharmacological interventions, including smaller and more frequent meals, avoidance of high-fat or spicy foods, cessation of eating upon early satiety, and adequate hydration and fiber intake. If symptoms persist beyond the early titration period, temporary dose stabilization or dose reduction should be considered. Once symptoms resolve, re-titration using a slower dose-escalation schedule may improve long-term tolerability. Nausea is the most commonly reported side effect, and antiemetic or prokinetic agents may be recommended for short-term use when it is severe or persistent. At this point, domperidone should be preferred over metoclopramide due to the risk of extrapyramidal side effects.73 In patients with reflux-predominant symptoms unresponsive to lifestyle modification, proton pump inhibitors or histamine-2 receptor antagonists may be used. Abdominal pain warrants careful clinical evaluation to exclude alternative etiologies, irrespective of GLP-1 RA use. If acute pancreatitis is confirmed, GLP-1 RA therapy should be discontinued immediately and not restarted. For constipation, osmotic or stimulant laxatives may be used when dietary measures are insufficient, whereas loperamide or probiotic supplementation may be considered for persistent diarrhea. Prolonged reliance on symptom-directed pharmacotherapy should be avoided whenever possible, as dose adjustment remains the most effective strategy for improving tolerability. When GI adverse effects remain severe or refractory despite these measures, temporary discontinuation of GLP-1 RA therapy or a structured “drug holiday” may be appropriate. Given inter-individual variability in tolerability profiles, switching to an alternative GLP-1 RA may also represent a reasonable strategy. Overall, management decisions should be individualized to balance therapeutic benefit with patient comfort and adherence.45,74 In summary, expanding practical guidance for the management of GI adverse effects is critical to ensuring treatment continuity and maximizing clinical benefit. A multidisciplinary approach involving physicians, dietitians, and, when necessary, other specialists can substantially improve symptom control, treatment persistence, and patient-reported quality of life.
Conclusion
GLP-1 RAs and dual GIP/GLP-1 RAs are highly effective treatment options for T2DM and obesity. The most common GI side effects of these agents include nausea, vomiting, diarrhoea, abdominal pain, and constipation. These symptoms, which generally occur at the start of treatment and during dose escalation, are mostly mild to moderate in severity and tend to diminish over time. They can be effectively managed through patient education, dietary changes, gradual dose titration, and short-term pharmacological support when necessary. Discontinuation of treatment or switching between agents should be reserved for patients with persistent or severe symptoms despite optimised management strategies. Current evidence consistently supports associations with common symptoms such as nausea, vomiting, diarrhea, and constipation, whereas links to more serious complications including pancreatitis, gastroparesis, or intestinal obstruction remain weak or inconsistent. Current evidence from randomised controlled trials, meta-analyses, and real-world studies indicates no consistent or causal relationship between these agents and serious GI side effects; however, uncertainty persists due to heterogeneity in study design, outcome definitions, and follow-up duration. Individualised risk-benefit assessment and close clinical monitoring are particularly important in patients with a history of GI disorders or pancreatitis. A multidisciplinary approach involving physicians, dietitians, and other healthcare professionals plays a critical role in maintaining treatment adherence and improving patients’ reported quality of life. There are still significant knowledge gaps regarding the long-term GI safety of GLP-1-based therapies and the optimal management of persistent or delayed-onset symptoms. To address these limitations and improve evidence-based guidelines for clinical practice, large-scale prospective studies and standardised real-world analyses are required in the future.
AI Statement
This manuscript was supported by the use of a large language model (ChatGPT, OpenAI) for language editing and formatting assistance. All scientific content, interpretation, and conclusions were developed by the authors.
Data Sharing Statement
No new data were generated or analyzed in this study.
Ethical Statement
This article is a narrative review of previously published studies and does not involve new data collection involving human or animal subjects; therefore, ethical approval was not required.
Author Contributions
N.Y. and M.B.: Conceptualization, Methodology, Data curation, Formal analysis, Writing – original draft, Writing – review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No external funding was received for this work.
Disclosure
The authors declare no conflicts of interest.
References
1. Zheng Z, Zong Y, Ma Y. et al. Glucagon-like peptide-1 receptor: mechanisms and advances in therapy. Signal Transduct Target Ther. 2024;9(1):234. doi:10.1038/s41392-024-01931-z
2. Drucker DJ. GLP-1 physiology informs the pharmacotherapy of obesity. Mol Metab. 2022;57:101351. doi:10.1016/j.molmet.2021.101351
3. Müller TD, Adriaenssens A, Ahrén B, et al. Glucose-dependent insulinotropic polypeptide (GIP). Mol Metab. 2025;95:102118. doi:10.1016/j.molmet.2025.102118
4. Wilding JP, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989–13. doi:10.1056/NEJMoa2032183
5. Kaplan JM, Zaman A, Abushamat LA. Curbing the Obesity Epidemic: should GLP-1 Receptor Agonists Be the Standard of Care for Obesity? Curr Cardiol Rep. 2024;26(9):1011–1019. doi:10.1007/s11886-024-02097-4
6. Moiz A, Filion KB, Toutounchi H, et al. Efficacy and safety of glucagon‐like peptide‐1 receptor agonists for weight loss among adults without diabetes: a systematic review of randomized controlled trials. Ann Intern Med. 2025;178(2):
7. Aldhaleei WA, Abegaz TM, Bhagavathula AS. Glucagon-like Peptide-1 Receptor Agonists Associated Gastrointestinal Adverse Events: a Cross-Sectional Analysis of the National Institutes of Health All of Us Cohort. Pharmaceuticals. 2024;17(2):199. doi:10.3390/ph17020199
8. Drucker DJ. Efficacy and safety of GLP-1 medicines for type 2 diabetes and obesity. Diabetes Care. 2024;47:1873–1888. doi:10.2337/dci24-0003
9. He L, Wang J, Ping F, et al. Association of Glucagon-Like Peptide-1 Receptor Agonist Use With Risk of Gallbladder and Biliary Diseases: a Systematic Review and Meta-analysis of Randomized Clinical Trials. JAMA Intern Med. 2022;182(5):513–519. doi:10.1001/jamainternmed.2022.0338
10. Sodhi M, Rezaeianzadeh R, Kezouh A, Etminan M. Risk of Gastrointestinal Adverse Events Associated With Glucagon-Like Peptide-1 Receptor Agonists for Weight Loss. JAMA. 2023;330(18):1795–1797. doi:10.1001/jama.2023.19574
11. Cao C, Yang S, Zhou Z. GLP-1 receptor agonists and pancreatic safety concerns in type 2 diabetic patients: data from cardiovascular outcome trials. Endocrine. 2020;68(3):518–525. doi:10.1007/s12020-020-02223-6
12. Chiang CH, Jaroenlapnopparat A, Colak SC, et al. Glucagon-Like Peptide-1 Receptor Agonists and Gastrointestinal Adverse Events: a Systematic Review and Meta-Analysis. Gastroenterology. 2025;169(6):1268–1281. doi:10.1053/j.gastro.2025.06.003
13. Yao H, Zhang A, Li D, et al. Comparative effectiveness of GLP-1 receptor agonists on glycaemic control, body weight, and lipid profile for type 2 diabetes: systematic review and network meta-analysis. BMJ. 2024;384:e076410. doi:10.1136/bmj-2023-076410
14. Rosenstock J, Wysham C, Frías JP, et al. Efficacy and safety of a novel dual GIP and GLP-1 receptor agonist tirzepatide in patients with type 2 diabetes (SURPASS-1): a double-blind, randomised, phase 3 trial. Lancet. 2021;398(10295):143–155. doi:10.1016/S0140-6736(21)01324-6
15. Jastreboff AM, le Roux CW, Stefanski A, Aronne LJ, Halpern B, Wharton S. Tirzepatide for Obesity Treatment and Diabetes Prevention. N Engl J Med. 2025;392(10):958–971. doi:10.1056/NEJMoa2410819
16. Frías JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus semaglutide once weekly in patients with type 2 diabetes. N Engl J Med. 2021;385(6):503–515. doi:10.1056/NEJMoa2107519
17. Karagiannis T, Malandris K, Avgerinos I, et al. Subcutaneously administered tirzepatide vs semaglutide for adults with type 2 diabetes: a systematic review and network meta‐analysis of randomised controlled trials. Diabetologia. 2024;67(7):
18. Liu L, Shi H, Xie M, Sun Y, Nahata MC. The efficacy and safety of tirzepatide in patients with diabetes and/or obesity: systematic review and meta-analysis of randomized clinical trials. Pharmaceuticals. 2025;18(5):668. doi:10.3390/ph18050668
19. Rodriguez PJ, Zhang V, Gratzl S, et al. Discontinuation and reinitiation of dual-labeled GLP-1 receptor agonists among US adults with overweight or obesity. JAMA Network Open. 2025;8(1):e2457349. doi:10.1001/jamanetworkopen.2024.57349
20. Samms RJ, Kusminski CM. A mechanistic rationale for incretin-based therapeutics in the management of obesity. Annu Rev Physiol. 2025;87:279–299. doi:10.1146/annurev-physiol-022724-105443
21. Argyrakopoulou G, Gitsi E, Konstantinidou SK, Kokkinos A. The effect of obesity pharmacotherapy on body composition, including muscle mass. Int J Obes Lond. 2025;49(3):381–387. doi:10.1038/s41366-024-01533-3
22. Wilding JPH, Batterham RL, Calanna S, et al. Impact of semaglutide on body composition in adults with overweight or obesity: exploratory analysis of the STEP 1 study. J Endocr Soc. 2021;5:A16–7. doi:10.1210/jendso/bvab048.030
23. Rochira V, Greco C, Boni S, et al. The effect of Tirzepatide on body composition in people with overweight and obesity: a systematic review of randomized, controlled studies. Diseases. 2024;12(9):204. doi:10.3390/diseases12090204
24. Cariou B, Linge J, Neeland IJ, et al. Effect of tirzepatide on body fat distribution pattern in people with type 2 diabetes. Diabetes Obes Metab. 2024;26(6):2446–2455. doi:10.1111/dom.15566
25. Karakasis P, Patoulias D, Fragakis N, Mantzoros CS. Effect of glucagon-like peptide-1 receptor agonists and co-agonists on body composition: systematic review and network meta-analysis. Metabolism. 2025;164:156113. doi:10.1016/j.metabol.2024.156113
26. Mechanick JI, Butsch WS, Christensen SM, et al. Strategies for minimizing muscle loss during use of incretin-mimetic drugs for treatment of obesity. Obes Rev. 2025;26(1):e13841. doi:10.1111/obr.13841
27. Jacobsen JM, Petersen N, Torz L, et al. Housing mice near vs. below thermoneutrality affects drug-induced weight loss but does not improve prediction of efficacy in humans. Cell Rep. 2024;43(8):114501. doi:10.1016/j.celrep.2024.114501
28. van.Eyk HJ, Paiman EHM, Bizino MB, et al. Liraglutide decreases energy expenditure and does not affect the fat fraction of supraclavicular brown adipose tissue in patients with type 2 diabetes. Nutr Metab and Cardiovasc Dis. 2020;30(4):616–624. doi:10.1016/j.numecd.2019.12.005
29. Kushner RF, Calanna S, Davies M, et al. Semaglutide 2.4 mg for the treatment of obesity: key elements of the STEP trials 1 to 5. Obesity. 2020;28(6):1050–1061. doi:10.1002/oby.22794
30. Kadowaki T, Kiyosue A, Shingaki T, Oura T, Yokote K. Efficacy and safety of once-weekly tirzepatide in Japanese patients with obesity disease (SURMOUNT-J): a multicentre, randomised, double-blind, placebo-controlled phase 3 trial. Lancet Diabetes Endocrinol. 2025;13(5):384–396. doi:10.1016/S2213-8587(24)00377-2
31. Zhao L, Cheng Z, Lu Y, et al. Tirzepatide for weight reduction in Chinese adults with obesity: the SURMOUNT-CN randomized clinical trial. JAMA. 2024;332(7):551–560. doi:10.1001/jama.2024.9217
32. Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387(3):
33. Buckley A, Suliman S, Allum M, et al. Real world use of tirzepatide in the treatment of type 2 diabetes in an Arab population. Diabetes Obes Metab. 2024;26(8):
34. Kelly MS, Scopelliti EM, Goodson KE, Cma L, Nguyen HX, Simon B. Real‐world evaluation of the effects of tirzepatide in patients with type 2 diabetes mellitus. Diabetes Obes Metab. 2024;26(12):
35. Rodriguez PJ, Goodwin Cartwright BM, Gratzl S, et al. Semaglutide vs tirzepatide for weight loss in adults with overweight or obesity. JAMA Intern Med. 2024;184(9):1056–1064. doi:10.1001/jamainternmed.2024.2525
36. Aronne LJ, Horn DB, le Roux CW, et al. Tirzepatide as Compared with Semaglutide for the Treatment of Obesity. N Engl J Med. 2025;393(1):26–36. doi:10.1056/NEJMoa2416394
37. Chuang MH, Chen JY, Wang HY, Jiang ZH, Wu VC. Clinical outcomes of tirzepatide or GLP‐1 receptor agonists in individuals with type 2 diabetes. JAMA Network Open. 2024;7(8):e2427258. doi:10.1001/jamanetworkopen.2024.27258
38. Khawaji A, Jaly A, Bakri H, et al. Weight Loss Efficacy of Tirzepatide Compared to Placebo or GLP-1 Receptor Agonists in Adults With Obesity or Overweight: a Meta-Analysis of Randomized Controlled Trials With ≥ 20 Weeks Treatment Duration. J Obes. 2025;2025:3442754. doi:10.1155/jobe/3442754
39. Kasagga A, Assefa A, Amin MN, et al. Dose-Dependent Efficacy and Safety of Tirzepatide for Weight Loss in Non-diabetic Adults With Obesity: a Systematic Review and M eta-analysis of Randomized Controlled Trials. Cureus. 2025;17(6):e85531. doi:10.7759/cureus.85531
40. Hall KD. Physiology of the weight-loss plateau in response to diet restriction, GLP-1 receptor agonism, and bariatric surgery. Obesity. 2024;32(6):1163–1168. doi:10.1002/oby.24027
41. Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: the STEP 1 trial extension. Diabetes Obes Metab. 2022;24:1553–1564. doi:10.1111/dom.14725
42. Aronne LJS, Horn N, He DBB, et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity: the SURMOUNT-4 randomized clinical trial. JAMA. 2024;331(1):38–48. doi:10.1001/jama.2023.24945
43. Rubino D, Abrahamsson N, Davies M, et al. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: the STEP 4 randomized clinical trial. JAMA. 2021;325(14):1414–1425. doi:10.1001/jama.2021.3224
44. Osei SP, Akomaning E, Florut TF, et al. Gastrointestinal safety assessment of GLP-1 receptor agonists in the US: a real-world adverse events analysis from the FAERS database. Diagnostics. 2024;14(24):2829. doi:10.3390/diagnostics14242829
45. Zhang Z, Zhang Q, Tan Y, et al. GLP-1RAs caused gastrointestinal adverse reactions of drug withdrawal: a system review and network meta-analysis. Front Endocrinol. 2023;14:1149328. doi:10.3389/fendo.2023.1149328
46. Xie X, Yang S, Deng S, et al. Comparative Gastrointestinal Adverse Effects of GLP-1 Receptor Agonists and Multi-Target Analogs in Type 2 Diabetes: a Bayesian Network Meta-Analysis in Type 2 Diabetes: a Bayesian Network Meta-Analysis. Front Pharmacol. 2025;16:1613610. doi:10.3389/fphar.2025.1613610
47. Sikirica MV, Martin AA, Wood R, et al. Reasons for discontinuation of GLP1 receptor agonists: data from a real‐world cross‐sectional survey of physicians and their patients with type 2 diabetes. Diabetes Metab Syndr Obes. 2017;10:
48. Huang X, Wu M, Lin J, Mou L, Zhang Y, Jiang J. Gastrointestinal safety evaluation of semaglutide for the treatment of type 2 diabetes mellitus: a meta-analysis. Medicine. 2024;103(21):e38236. doi:10.1097/MD.0000000000038236
49. Tan HC, Dampil OA, Marquez MM. Efficacy and Safety of Semaglutide for Weight Loss in Obesity Without Diabetes: a Systematic Review and Meta-Analysis. J ASEAN Fed Endocr Soc. 2022;37(2):65–72. doi:10.15605/jafes.037.02.14
50. Ismaiel A, Scarlata GGM, Boitos I, et al. Gastrointestinal adverse events associated with GLP-1 RA in non-diabetic patients with overweight or obesity: a systematic review and network meta-analysis. Int J Obes. 2025;49(10):1946–1957. doi:10.1038/s41366-025-01859-6
51. Safwan M, Bourgleh MS, Alotaibi SA, Alotaibi E, Al-Ruqi A, El Raeya F. Gastrointestinal safety of semaglutide and tirzepatide vs. placebo in obese individuals without diabetes: a systematic review and meta analysis. Ann Saudi Med. 2025;45(2):129–143. doi:10.5144/0256-4947.2025.129
52. Tong K, Yin S, Yu Y, et al. Gastrointestinal adverse events of tirzepatide in the treatment of type 2 diabetes mellitus: a meta-analysis and trials sequential analysis. Medicine. 2023;102(43):e35488. doi:10.1097/MD.0000000000035488
53. Liu BD, Udemba SC, Liang K, et al. Shorter-acting glucagon-like peptide-1 receptor agonists are associated with increased development of gastro-oesophageal reflux disease and its complications in patients with type 2 diabetes mellitus: a population-level retrospective matched cohort study. Gut. 2024;73(2):246–254. doi:10.1136/gutjnl-2023-329651
54. Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of type 2 diabetes - state-of-the-art. Mol Metab. 2021;46:101102. doi:10.1016/j.molmet.2020.101102
55. Elashoff M, Matveyenko AV, Gier B, et al. Pancreatitis, pancreatic, and thyroid cancer with glucagon-like peptide-1-based therapies. Gastroenterology. 2011;141(1):150–156. doi:10.1053/j.gastro.2011.02.018
56. Singh S, Chang HY, Richards TM, et al. Glucagonlike peptide 1-based therapies and risk of hospitalization for acute pancreatitis in type 2 diabetes mellitus: a population-based matched case-control study. JAMA Intern Med. 2013;173(7):534–539. doi:10.1001/jamainternmed.2013.2720
57. FDA Drug Safety Communication. FDA investigating reports of possible increased risk of pancreatitis and pre-cancerous findings of the pancreas from incretin mimetic drugs for type 2 diabetes. 2013. Available from: https://www.fda.gov/Drugs/DrugSafety/ucm343187.htm.
58. Wilhite K, Reid JM, Lane M. Risk of pancreatitis with incretin therapies versus thiazolidinediones in the Veterans Health Administration. Ann Pharmacother. 2024;58:685–689. doi:10.1177/10600280231205490
59. Kim JA, Yoo HJ. Exploring the Side Effects of GLP-1 Receptor Agonist: to Ensure Its Optimal Positioning Diabetes &. Metabolism J. 2025;49(4):525–541. doi:10.4093/dmj.2025.0242
60. Masson W, Lobo M, Barbagelata L, Lavalle-Cobo A, Nogueira JP. Acute pancreatitis due to different semaglutide regimens: an updated meta-analysis. Endocrinol Diabetes Nutr. 2024;71(3):124–132. doi:10.1016/j.endien.2024.03.012
61. Rayner CK, Wu T, Aroda VR, et al. Gastrointestinal adverse events with insulin glargine/lixisenatide fixed-ratio combination versus glucagon-like peptide-1 receptor agonists in people with type 2 diabetes mellitus: a network meta-analysis. Diabetes Obes Metab. 2021;23:136–146. doi:10.1111/dom.14202
62. Zeng Q, Xu J, Mu X, Shi Y, Fan H, Li S. Corrigendum: safety issues of tirzepatide (pancreatitis and gallbladder or biliary disease) in type 2 diabetes and obesity: a systematic review and meta-analysis. Front Endocrinol. 2024;15:1342543. doi:10.3389/fendo.2023.1214334
63. Niu C, Kefang S, Jing Z, et al. Gastrointestinal and Hepatobiliary Safety of Glucagon-Like Peptide-1 Receptor Agonists in Patients With Type 2 Diabetes. Am J Gastroenterol. 2025. doi:10.14309/ajg.0000000000003760
64. Nieto LM, Martinez J, Narvaez SI, et al. Glucagon-Like Peptide-1 Receptor Agonists Use Does Not Increase the Risk for Acute Pancreatitis and Is Associated With Lower Complications in Patients With Type 2 Diabetes Who Develop Acute Pancreatitis: a Multicenter Analysis. Am J Gastroenterol. 2025. doi:10.14309/ajg.00000000000003525
65. Kim HJ, Kang TU, Kim MJ, Swan H, Park SM. Long-term weight patterns and physical activity in gallstones. Sci Rep. 2024;14(1):25817. doi:10.1038/s41598-024-77218-8
66. Dong YH, Wu JH, Chang CH, Lin JW, Wu LC, Toh S. Association between glucagon- like peptide-1 receptor agonists and biliary-related diseases in patients with type 2 diabetes: a nationwide cohort study. Pharmacotherapy. 2022;42(6):483–494. doi:10.1002/phar.2688
67. Jalleh RJ, Plummer MP, Marathe CS, et al. Clinical Consequences of Delayed Gastric Emptying With GLP-1 Receptor Agonists and Tirzepatide. Clin Endocrinol Metab. 2024;110(1):1–15. doi:10.1210/clinem/dgae719
68. Faillie JL, Yin H, Ohy Y, et al. Incretin-Based Drugs and Risk of Intestinal Obstruction Among Patients With Type 2 Diabetes. Clin Pharmacol Ther. 2022;111(1):272–282. doi:10.1002/cpt.2430
69. Ueda P, Wintzell V, Melbye M, et al. Use of DPP4 Inhibitors and GLP-1 Receptor Agonists and Risk of Intestinal Obstruction: scandinavian Cohort Study. Clin Gastroenterol Hepatol. 2024;22(6):1226–1237. doi:10.1016/j.cgh.2023.08.034
70. Gao Z, Tabernacki T, Dorney I, et al. Association of GLP-1 receptor agonists with risk of intestinal obstruction in patients with type 2 diabetes mellitus: a retrospective cohort study. Acta Diabetol. 2025;62(11):1941–1951. doi:10.1007/s00592-025-02525
71. Wu T, Zhang Y, Shi Y, et al. Safety of glucagon-like peptide-1 receptor agonists: a real-world study based on the US FDA adverse event reporting system database. Clin Drug Investig. 2022;42(11):
72. Liu L, Chen J, Wang C, Chen L, Chen L. Association between different GLP-1 receptor agonists and gastrointestinal adverse reactions: a real-world disproportionality study based on FDA adverse event reporting system database. Front Endocrinol. 2022;13:1043789. doi:10.3389/fendo.2022.1043789
73. Gorgojo‐Martínez JJ, Mezquita‐Raya P, Carretero‐Gómez J, et al. Clinical recommendations to manage gastrointestinal adverse events in patients treated with Glp‐1 receptor agonists: a multidisciplinary expert consensus. J Clin Med. 2022;12(1):145. doi:10.3390/jcm12010145
74. Wharton S, Davies M, Dicker D, et al. Managing the gastrointestinal side effects of GLP-1 receptor agonists in obesity: recommendations for clinical practice. Postgrad Med. 2022;134(1):14–19. doi:10.1080/00325481.2021.2002616
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Health Technology Assessment Based on Chinese Guidelines: Glucagon-Like Peptide-1 Receptor Agonist in the Treatment of Type 2 Diabetes Complicated with Cardiovascular Disease
Xie Z, Li J, Yang S, Deng W, Chen J
Therapeutics and Clinical Risk Management 2022, 18:889-900
Published Date: 30 August 2022
Evaluation of miRNA-143 and miRNA-145 Expression and Their Association with Vitamin-D Status Among Obese and Non-Obese Type-2 Diabetic Patients
Aladel A, Khatoon F, Khan MI, Alsheweir A, Almutairi MG, Almutairi SO, Almutairi FK, Osmonaliev K, Beg MMA
Journal of Multidisciplinary Healthcare 2022, 15:2979-2990
Published Date: 28 December 2022
Association of Serum Leptin and Adiponectin Concentrations with Type 2 Diabetes Biomarkers and Complications Among Saudi Women
Mohammed Saeed W, Nasser Binjawhar D
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2129-2140
Published Date: 13 July 2023
DR10627, a Novel Dual Glucagon‑like Peptide‑1 and Gastric Inhibitory Polypeptide Receptor Agonist for the Treatment of Obesity and Type 2 Diabetes Mellitus
Shao Y, Chen Y, Zhu M, Liu Y, Fang C, Wang M, Sun P, Fu W, Huang J, Sheng S, Huang Y
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1563-1573
Published Date: 6 April 2024
Relative Effectiveness and Safety of the GLP-1 (Glucagon-Like Peptide 1) Receptor Agonists, Semaglutide and Liraglutide in the Treatment of Obese Type 2 Diabetics: A Prospective Observational Cohort Study in Poland
Hoffmann K, Michalak M, Paczkowska A
Diabetes, Metabolic Syndrome and Obesity 2025, 18:2723-2738
Published Date: 7 August 2025