Back to Journals » Drug Design, Development and Therapy » Volume 20
From Methotrexate Resistance to Biologic and Targeted Pharmacotherapy: A Decade of Phase 4 Clinical Trials Evidence in Rheumatoid Arthritis
Authors Alsharif ST ![]()
Received 15 November 2025
Accepted for publication 1 January 2026
Published 8 January 2026 Volume 2026:20 581822
DOI https://doi.org/10.2147/DDDT.S581822
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Shaker T Alsharif
Pharmaceutical Science Department, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Shaker T Alsharif, Pharmaceutical Science Department, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia, Email [email protected]
Background: Methotrexate (MTX) remains the cornerstone of rheumatoid arthritis (RA) management; however, up to 30– 40% of patients experience inadequate response or intolerance, necessitating escalation to advanced therapeutic strategies. Tumor necrosis factor (TNF) inhibitors were the first biologic agents introduced for RA and continue to play an important role in MTX-resistant disease, alongside newer biologic and targeted synthetic disease modifying antirheumatic drugs (DMARDs).
Objective: To synthesize Phase 4 clinical trial evidence published between 2014 and 2024 evaluating therapeutic strategies for MTX-resistant RA, including TNF inhibitor optimization, newer biologic and targeted synthetic DMARDs, adjunctive therapies, and emerging precision medicine approaches.
Methods: A systematic review of Phase 4 interventional trials registered on ClinicalTrials.gov was conducted using the keyword “rheumatoid arthritis”, with predefined eligibility restrictions applied. Trials enrolling adults with MTX-resistant RA and reporting clinical, safety, biomarker, imaging, or patient reported outcomes were included. Extracted data encompassed study design, intervention type, trial classification (exploratory/mechanistic, optimization/treat to target, or effectiveness/safety), outcomes, and enrolment.
Results: Eighteen Phase 4 trials were identified, encompassing a heterogeneous range of study designs and therapeutic strategies. Optimization and treat-to-target studies demonstrated continued clinical relevance of TNF inhibitors, particularly in combination with MTX. Newer biologic and targeted synthetic DMARDs showed comparable efficacy, while exploratory trials provided mechanistic insights through biomarker and imaging assessments. Safety profiles across trials were generally consistent with established class effects, with infections and laboratory abnormalities most frequently reported and no unexpected safety signals observed.
Conclusion: Phase 4 evidence highlights the continued role of TNF inhibitors alongside newer biologic and targeted synthetic therapies in MTX-resistant RA. Trial heterogeneity reflects real world clinical complexity, underscoring the importance of treatment optimization, safety monitoring, and emerging precision strategies in contemporary RA management.
Keywords: rheumatoid arthritis, methotrexate resistance, biologic DMARDs, abatacept, tofacitinib, sarilumab, biomarkers
Introduction
Rheumatoid arthritis (RA) is a systemic autoimmune disease affecting approximately 0.5–1% of the population worldwide and is characterized by chronic synovitis, progressive joint destruction, and extra-articular manifestations.1 Over the past decades, methotrexate (MTX) has remained the main therapy due to its efficacy, safety, and affordability.2 However, up to 30–40% of patients show inadequate response or intolerance, leading to ongoing inflammation, radiographic progression, disability, and higher mortality risk.3 Tumor necrosis factor (TNF) inhibitors represented the first major biologic advance in the management of rheumatoid arthritis and remain a foundational component of treatment algorithms for patients with inadequate response to MTX. Agents such as infliximab, etanercept, adalimumab, golimumab, and certolizumab pegol have consistently demonstrated efficacy in reducing disease activity, preventing radiographic progression, and improving functional outcomes in randomized controlled trials and long-term observational studies.4,5 Despite the introduction of newer biologic and targeted synthetic DMARDs, TNF inhibitors continue to be widely used owing to their extensive long term safety data, clinician familiarity, and increasing availability of biosimilars.6 Importantly, loss or absence of response in MTX-resistant patients may reflect treatment sequencing or optimization issues rather than true class failure, underscoring the continued relevance of TNF inhibitors within contemporary treatment paradigms.7
The introduction of biologic and targeted synthetic disease-modifying antirheumatic drugs (DMARDs) has revolutionized the treatment landscape. Abatacept, a selective T-cell co-stimulation modulator, has demonstrated clinical efficacy and a favorable safety profile.8 Janus kinase (JAK) inhibitors such as tofacitinib offer effective oral options with rapid onset of action.9 In addition, interleukin-6 (IL-6) inhibitors including sarilumab and tocilizumab provide alternative pathways for disease control.5,10 Beyond these agents, glucocorticoids remain widely used for their anti-inflammatory effects, as highlighted by the GLORIA study of low-dose prednisolone.11 Novel agents such as Acthar Gel and repurposed therapies like ticagrelor have also been investigated, alongside biomarker-driven and imaging-based studies that signal the emergence of precision medicine approaches.12,13 According to the most recent ACR (2023) and EULAR (2024) treatment recommendations, therapeutic decision-making in RA should be guided by disease activity, comorbidity profile, and biomarker data rather than a stepwise escalation alone.6,14 In parallel with clinical trial development, emerging biomaterials-based strategies, including multifunctional nanoparticle platforms, have demonstrated promising therapeutic potential in preclinical RA models, highlighting future translational directions for targeted and precision-based interventions.15
Despite these advances, there remains a critical gap in understanding how biologic and targeted synthetic DMARDs perform in MTX resistant patients. This review addresses that gap by systematically evaluating Phase 4 clinical trials registered between 2014 and 2024 to clarify therapeutic outcomes, safety, and innovation trends.
Phase 4 clinical trials are particularly relevant in RA as they assess safety, efficacy, and applicability in broader patient populations, including older adults and those with comorbidities.16 They also provide opportunities to explore biomarker stratification, withdrawal strategies, and treatment optimization. This review evaluates 18 Phase 4 clinical trials in MTX-resistant RA conducted between 2014 and 2024, summarizing their findings and implications for clinical practice.
Methods
This review was conducted in accordance with the PRISMA 2020 statement, and the search was last updated on October 22, 2025. The ClinicalTrials.gov database was searched using the keyword “rheumatoid arthritis”. Predefined eligibility screening restrictions were then applied to limit results to completed Phase 4 clinical trials conducted within the past 10 years and enrolling adult populations. This approach yielded 3586 RA related clinical trial records.
Following screening based on study phase, completion status, and population characteristics, 52 completed Phase 4 clinical trials were assessed for eligibility. In total, 34 studies were excluded due to non-interventional design, lack of available protocols or results, or insufficient relevance to therapeutic management in RA. A total of 18 Phase 4 clinical trials met the inclusion criteria and were included in the final qualitative synthesis. The study selection process is summarized in Figure 1 in accordance with PRISMA 2020 guidelines.
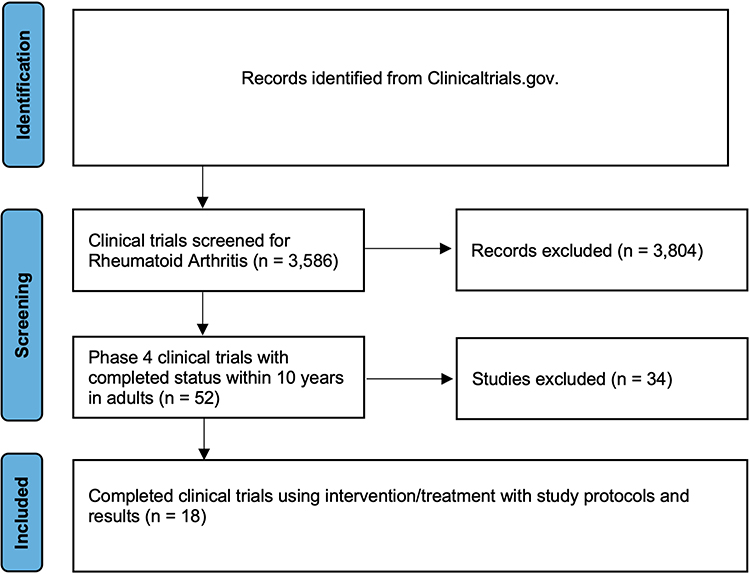 |
Figure 1 PRISMA flow diagram illustrating the identification, screening, eligibility assessment, and inclusion of phase 4 clinical trials in rheumatoid arthritis, updated from ClinicalTrials.gov as of 22/10/2025. |
Inclusion Criteria
Studies were eligible for inclusion if they were registered as completed Phase 4 clinical trials on ClinicalTrials.gov, conducted within the past 10 years, and enrolled adult or older adult participants aged 18 years or above with a diagnosis of RA. Trials were required to involve an interventional treatment and to provide accessible study protocols or results. Following identification, studies were reviewed for relevance to therapeutic management in RA based on trial descriptions, intervention characteristics, and reported outcomes, with only those addressing clinical treatment strategies retained for qualitative synthesis.
Exclusion Criteria
Studies were excluded if they were non-interventional or observational in design, classified as Phase 1–3 trials, conducted exclusively in pediatric populations, or ongoing, withdrawn, or terminated without available results. Trials lacking defined treatment interventions or insufficiently relevant to clinical management of RA were also excluded.
Data Extraction
Data extraction was performed directly from ClinicalTrials.gov records. The following information was collected: study title, interventions, primary and secondary outcome measures, sample size, design, and patient age categories. Where available, registry entries were cross checked with published articles to ensure accuracy and to provide supporting evidence. In total, 18 studies fulfilled the inclusion criteria and were analyzed for this review.
Results
Eighteen Phase 4 clinical trials met the inclusion criteria and were analyzed for this review. These studies evaluated a range of biologic, targeted synthetic, and adjunctive therapies addressing MTX-resistant rheumatoid arthritis, with outcomes focusing on disease activity indices, biomarker profiles, imaging findings, and patient-reported measures. The study selection process is summarized in Figure 1, and detailed characteristics of each trial are presented in Table 1.5,17–33
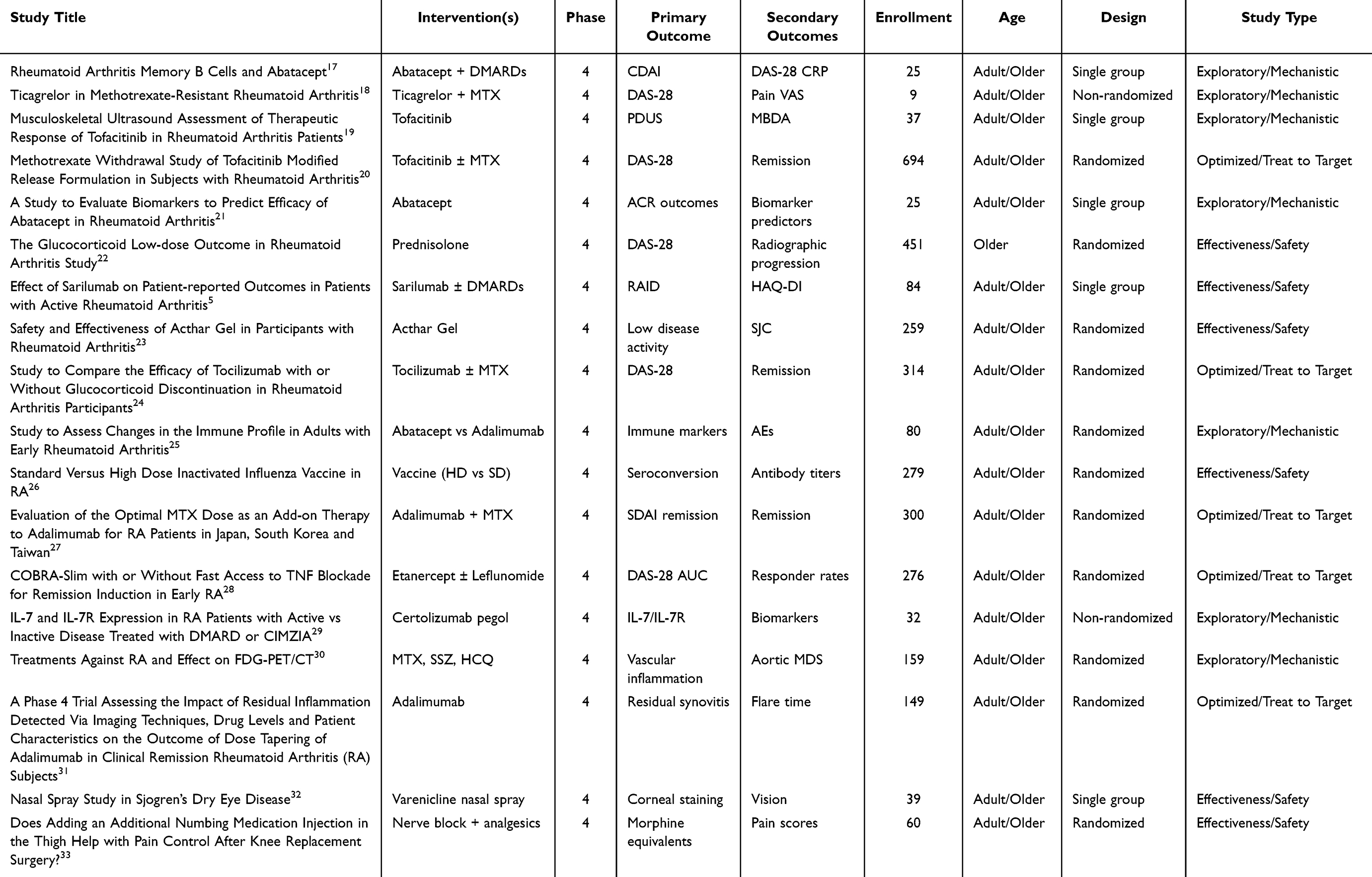 |
Table 1 Full Table of Clinical Trials on Rheumatoid Arthritis in Adults (2014–2024) |
Across the 18 included Phase 4 studies, interventions were categorized into four major therapeutic classes: T-cell co-stimulation modulators (abatacept, n = 3), JAK inhibitors (tofacitinib, n = 2), cytokine inhibitors (sarilumab and tocilizumab, n = 2), and adjunctive or exploratory agents including glucocorticoids, Acthar Gel, TNF inhibitor optimization, and novel pathway modulators such as ticagrelor and IL-7/IL-7R targeting (n = 11). Among biologic and targeted DMARD trials, mean reductions in DAS-28 ranged from 1.6 to –2.8 points, with remission rates of 35–55% at 24 weeks. Adjunctive corticosteroid and Acthar Gel studies demonstrated more modest DAS-28 improvements of approximately 1.2 points, though variability in adverse-event profiles was greater. Collectively, these data underscore consistent efficacy across mechanistically distinct therapies while highlighting the ongoing need to balance disease control with safety in real-world Phase 4 settings.
Abatacept was evaluated in multiple trials addressing disease activity, biomarker signatures, and immune modulation. Consistent reductions in CDAI and DAS-28 were reported, and biomarker-based approaches identified predictors of therapeutic response.
Tofacitinib was tested in mechanistic and pivotal contexts, with ultrasound and biomarker studies demonstrating reductions in synovitis, while the ORAL Shift trial confirmed that tofacitinib monotherapy following MTX withdrawal-maintained remission rates comparable to combination therapy.
IL-6 inhibitors, including sarilumab and tocilizumab, showed robust efficacy in both clinical and patient-reported outcomes. The GLORIA trial highlighted the effectiveness of low-dose prednisolone in reducing DAS-28 and slowing radiographic progression, although safety concerns particularly infection risk and metabolic complications were noted.
Acthar Gel proved beneficial in refractory RA cases unresponsive to multiple biologic classes. TNF inhibitor optimization studies, including adalimumab-based combination and structured treat to target protocols, reinforced the importance of continued MTX co-therapy for achieving and maintaining remission in MTX-resistant disease.
Several Phase 4 trials evaluated optimization strategies for TNF inhibitors in patients with MTX resistant rheumatoid arthritis. Rather than assessing novel biologic efficacy, these studies focused on treatment sequencing, combination strategies, and remission maintenance. Trials involving adalimumab and structured treatment protocols, including treat to target and COBRA Slim based approaches, demonstrated that continuation of MTX alongside TNF inhibition resulted in superior disease control and more durable remission compared with TNF inhibitor monotherapy. These findings reinforce the role of TNF inhibitors as effective therapeutic options in MTX-resistant disease when appropriately optimized and combined with conventional DMARD therapy. Exploratory interventions such as ticagrelor and IL-7/IL-7R modulation provided mechanistic insights into immune regulation and cardiovascular risk.
Imaging-based studies employing FDG-PET/CT and ultrasound revealed that persistent subclinical inflammation correlated with delayed remission and increased vascular inflammation. Adjunctive investigations into influenza vaccination, ocular therapy in Sjögren’s-associated rheumatoid arthritis, and pain management broadened the evidence base for comprehensive care strategies.
Safety and Adverse Events
Safety outcomes were reported across the included Phase 4 clinical trials, with adverse events generally consistent with the known safety profiles of the evaluated therapies. Biologic and targeted synthetic DMARD trials most commonly reported infections, gastrointestinal symptoms, and laboratory abnormalities as adverse events. IL-6 inhibitors and JAK inhibitors were associated with higher rates of infections and laboratory related adverse events, including lipid and liver enzyme elevations, while serious adverse events were infrequent. Low dose glucocorticoid therapy demonstrated an increased incidence of infections and metabolic complications, particularly in older adult populations, as observed in the GLORIA trial. Acthar Gel studies reported acceptable tolerability in refractory patients, although data were limited by small sample sizes. Overall, no unexpected safety signals were identified, but variability in adverse event reporting across trials limited direct comparison.
Considerable heterogeneity was observed across trials, with sample sizes ranging from 9 to 694 participants. This variability largely reflects differences in study objectives, ranging from mechanistic biomarker focused investigations to large pragmatic effectiveness trials, and affects both statistical power and result interpretation.
Discussion
The collective evidence from these 18 Phase 4 clinical trials highlights the continued evolution of RA management beyond MTX centered strategies toward biologic and targeted synthetic DMARD optimization. Abatacept consistently demonstrated improvements in disease activity and functional outcomes, and biomarker based studies suggested potential predictors of therapeutic response, supporting its role in personalized treatment approaches.34 Tofacitinib further confirmed its efficacy as an oral targeted therapy, with the ORAL Shift study showing that remission could be maintained following MTX withdrawal in selected patients, reinforcing its flexibility in long-term disease control strategies.35 IL-6 inhibitors, including sarilumab and tocilizumab, also showed robust clinical and patient-reported outcome improvements in MTX inadequate responders, underscoring the importance of cytokine blockade as an alternative mechanism of action.36,37
Low dose glucocorticoids remain an important adjunctive therapy, particularly in older patients and those with high inflammatory burden. The GLORIA trial demonstrated meaningful reductions in disease activity and slowed radiographic progression with low dose prednisolone, although long term use was limited by safety concerns, including infections and metabolic complications.11 Acthar Gel also showed clinical benefit in highly refractory RA populations who had failed multiple biologic therapies, supporting its role as a potential adjunctive option in selected cases.38 In parallel, Phase 4 TNF inhibitor optimization studies provided important real evidence that therapeutic failure in MTX resistant patients often reflects suboptimal treatment strategies rather than true biologic inefficacy. Adalimumab based combination and treat to target protocols demonstrated improved remission durability when TNF inhibitors were used alongside MTX, reinforcing their continued relevance as cost effective and mechanistically established options when appropriately optimized.39 Exploratory and mechanistic studies further expanded the therapeutic landscape by providing insight into inflammatory pathways and comorbidity risk. Investigations involving ticagrelor highlighted the intersection between RA inflammation and cardiovascular risk, while IL-7 and IL-7 receptor modulation studies offered early evidence supporting immune-pathway stratification and future precision immunology approaches.13,40 Imaging based trials using FDG-PET/CT and power Doppler ultrasound demonstrated that persistent subclinical inflammation may contribute to delayed remission and increased vascular inflammation, emphasizing the need for sensitive disease monitoring strategies beyond conventional clinical indices.41 Beyond clinical and biomarker driven strategies, advances in biomaterials research have introduced injectable hydrogel based therapeutic platforms for RA. Preclinical studies have demonstrated that locally administered injectable hydrogels can enable sustained drug release, targeted modulation of synovial inflammation, and reduced systemic exposure in experimental models of RA, thereby improving anti-inflammatory efficacy while minimizing off target toxicity.42 Although these approaches remain investigational, they represent promising translational strategies that may complement future precision and targeted treatment paradigms in RA.
Biomarker driven and imaging based approaches featured prominently in several Phase 4 trials and provide important insight into emerging precision medicine strategies in RA. Elevated baseline inflammatory markers, including CRP, were associated with greater clinical improvement following biologic and targeted synthetic DMARD therapy in multiple trials, suggesting potential predictive value for treatment response.34,36 Imaging biomarkers, particularly power Doppler ultrasound and FDG-PET/CT, demonstrated that persistent subclinical synovitis and vascular inflammation were associated with delayed remission and increased cardiometabolic risk, highlighting their utility for monitoring disease activity beyond conventional clinical indices.41 In addition, exploratory immune biomarkers involving the IL-7 and IL-7 receptor pathway provided mechanistic insight into T-cell driven disease activity and may inform future patient stratification strategies.40 Although these biomarker approaches are not yet fully integrated into routine clinical practice, Phase 4 evidence supports their potential role in refining therapeutic selection, monitoring response, and advancing individualized treatment paradigms in MTX -resistant RA.
Vaccination and adjunctive treatment studies broadened the clinical context of RA management, emphasizing infection prevention, symptom-directed supportive care, and management of extra articular manifestations. These investigations highlight the importance of comprehensive treatment frameworks that extend beyond disease activity control alone and address long-term patient well-being.
Safety considerations remain central to treatment selection in MTX-resistant RA, particularly in Phase 4 settings. Across the included trials, adverse event profiles were largely consistent with known class-specific risks, allowing for comparative assessment across therapeutic categories. JAK inhibitors and IL-6 inhibitors were most frequently associated with infections and laboratory abnormalities, including lipid and hepatic enzyme elevations, whereas TNF inhibitors and abatacept demonstrated comparatively stable long term safety profiles when used in combination with MTX. Importantly, recent post marketing and randomized safety evaluations have raised concerns regarding increased cardiovascular and malignancy risk associated with JAK inhibitors in selected high-risk populations, emphasizing the need for careful patient selection and risk stratification.16 Low dose glucocorticoid therapy was also associated with increased infection and metabolic risk in older adults, as demonstrated in the GLORIA trial.11 Although serious adverse events were uncommon across most Phase 4 studies, heterogeneity in reporting practices and limited follow-up durations underscore the importance of continued pharmacovigilance and individualized risk benefit assessment when selecting advanced therapies.
Recent meta analyses and comparative evaluations reinforce these findings, demonstrating pooled DAS-28 reductions ranging from approximately 1.8 to 2.5 points and remission rates of 40–55% among MTX inadequate responders treated with biologic or targeted synthetic DMARDs.6,43 However, cost effectiveness studies highlight important distinctions between biologic and targeted synthetic DMARDs. Analyses from European and North American healthcare models suggest that JAK and IL-6 inhibitors achieve comparable efficacy to TNF or T-cell targeted agents but at substantially higher annual treatment costs. Conversely, abatacept and optimized TNF inhibitor regimens demonstrate greater cost-utility, particularly in long term disease control. These findings emphasize the necessity of integrating pharmacoeconomic and accessibility considerations into future RA management guidelines and policy frameworks. Variations in healthcare infrastructure, reimbursement policies, and drug availability play a critical role in shaping real-world treatment strategies for MTX-resistant RA. Although the included Phase 4 clinical trials did not provide region-specific cost or access data, existing economic evidence highlights substantial differences in drug affordability and utilization patterns across healthcare systems, particularly for advanced therapies where direct treatment costs continue to rise.44 Analyses of utilization and healthcare expenditures associated with JAK inhibitors further demonstrate how access to targeted therapies may be influenced by payer policies, regulatory restrictions, and regional prescribing practices.45 In contrast, treatment sequences involving TNF inhibitors and abatacept, especially with the increasing availability of biosimilars have been associated with more favorable cost effectiveness profiles in multiple healthcare settings.46 These considerations underscore the importance of integrating economic and regional factors into treatment decision making and highlight the need for future studies to incorporate region specific effectiveness and cost analyses.
Overall, the findings from these Phase 4 clinical trials underscore a paradigm shift toward precision guided immunomodulation in RA. Integration of clinical characteristics, biomarkers, imaging findings, safety profiles, and economic considerations is essential to optimize treatment outcomes while minimizing adverse events. Future research should prioritize long-term comparative effectiveness studies, robust safety surveillance, and biomarker driven treatment algorithms to support individualized, value based care across diverse patient populations.
Limitations
This review was limited to registered Phase 4 trials, which may exclude unpublished data. Some exploratory studies were small and non-randomized, limiting generalizability. Safety, cost effectiveness, and comparative biologic studies remain insufficiently addressed, emphasizing the need for further large-scale research.
Conclusion
Phase 4 clinical evidence confirms that biologic and targeted synthetic DMARDs, including TNF inhibitors, abatacept, JAK inhibitors, and IL-6 inhibitors, provide meaningful improvements in disease activity and remission rates among MTX-resistant RA patients. In addition to newer targeted therapies, Phase 4 trials evaluating TNF inhibitor optimization strategies highlight the continued clinical relevance of established biologics, particularly when used in combination with MTX and within structured treat to target frameworks.
Adjunctive approaches, including low dose glucocorticoids and Acthar Gel, may offer additional benefit in selected refractory populations but require careful safety monitoring. Evidence from biomarker driven and imaging-based studies support the evolving role of precision medicine in refining therapeutic selection and disease monitoring. Safety considerations remain central to treatment decision-making, particularly in light of class specific risks associated with advanced therapies.
Collectively, these findings support a transition from a purely MTX-centered approach toward a more individualized, evidence driven treatment paradigm that integrates established biologics, novel targeted agents, safety profiling, and patient-specific factors. Future research should prioritize long-term comparative effectiveness studies, pharmacoeconomic evaluations, and biomarker guided strategies to optimize outcomes and support sustainable, value-based care in RA.
Abbreviations
AEs, Adverse Events; CDAI, Clinical Disease Activity Index; CRP, C-Reactive Protein; DAS-28, Disease Activity Score-28 Joints; DMARDs, Disease-Modifying Antirheumatic Drugs; FDG-PET/CT, Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography; HAQ-DI, Health Assessment Questionnaire-Disability Index; HCQ, Hydroxychloroquine; HD vs SD, High-Dose versus Standard-Dose; IL-7/IL-7R, Interleukin-7/Interleukin-7 Receptor; MBDA, Multi-Biomarker Disease Activity Score; MDS, Mean Density Score; MTX, Methotrexate; PDUS, Power Doppler Ultrasound; RAID, Rheumatoid Arthritis Impact of Disease Score; SDAI, Simple Disease Activity Index; SJC, Swollen Joint Count; SSZ, Sulfasalazine; VAS, Visual Analog Scale.
Funding
No funding was received for this work.
Disclosure
The author declares no conflicts of interest in this work.
References
1. Aletaha D, Smolen JS. Diagnosis and management of rheumatoid arthritis: a review. JAMA. 2018;320(13):1360–9. doi:10.1001/jama.2018.13103
2. Singh JA, Saag KG, Bridges SL, et al. 2015 American college of rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016;68(1):1–26. doi:10.1002/art.39480
3. Burmester GR, Pope JE. Novel treatment strategies in rheumatoid arthritis. Lancet. 2017;389(10086):2338–2348. doi:10.1016/S0140-6736(17)31491-5
4. Lipsky PE, van der Heijde DM, St Clair EW, et al. Infliximab and methotrexate in the treatment of rheumatoid arthritis. anti-tumor necrosis factor trial in rheumatoid arthritis with concomitant therapy study group. N Engl J Med. 2000;343(22):1594–1602. doi:10.1056/NEJM200011303432202
5. Effect of sarilumab on patient-reported outcomes in patients with moderately to severely active rheumatoid arthritis and with inadequate response or intolerance to current conventional synthetic DMARDs or tumor necrosis factor inhibitors [Internet]. 2018. Available from: https://clinicaltrials.gov/study/NCT03449758.
6. Smolen JS, Landewé RBM, Bergstra SA, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis. 2023;82(1):3–18. doi:10.1136/ard-2022-223356
7. Taylor PC, Matucci Cerinic M, Alten R, Avouac J, Westhovens R. Managing inadequate response to initial anti-TNF therapy in rheumatoid arthritis: optimising treatment outcomes. Ther Adv Musculoskelet Dis. 2022;14:1759720x221114101. doi:10.1177/1759720X221114101
8. Kremer J. Methotrexate pharmacogenomics. Ann Rheumatic Dis. 2006;65(9):1121–1123. doi:10.1136/ard.2006.051789
9. Taylor PC, Keystone EC, Van Der Heijde D, et al. Baricitinib versus placebo or Adalimumab in rheumatoid arthritis. N Engl J Med. 2017;376(7):652–662. doi:10.1056/NEJMoa1608345
10. Smolen JS, Beaulieu A, Rubbert-Roth A, et al. Effect of interleukin-6 receptor inhibition with tocilizumab in patients with rheumatoid arthritis (OPTION study): a double-blind, placebo-controlled, randomised trial. Lancet. 2008;371(9617):987–997. doi:10.1016/S0140-6736(08)60453-5
11. Boers M, Hartman L, Opris-Belinski D, et al. Low dose, add-on prednisolone in patients with rheumatoid arthritis aged 65+: the pragmatic randomised, double-blind placebo-controlled GLORIA trial. Ann Rheum Dis. 2022;81(7):925–936. doi:10.1136/annrheumdis-2021-221957
12. Gillis T, Crane M, Hinkle C, Wei N. AB0502 HP Acthar® Gel (repository corticotropin injection) as adjunctive therapy in patients with rheumatoid arthritis who have failed at least three biologic therapies with different modes of action. Ann Rheumatic Dis. 2015;74:1066. doi:10.1136/annrheumdis-2015-eular.2092
13. Garshick MS, Rosenthal PB, Luttrell-Williams E, Cronstein BN, Berger JS. Ticagrelor added to methotrexate improves rheumatoid arthritis disease severity. Rheumatology. 2021;60(11):5473–5475. doi:10.1093/rheumatology/keab481
14. Fraenkel L, Bathon JM, England BR, et al. 2021 American college of rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2021;73(7):1108–1123. doi:10.1002/art.41752
15. Huang R, Zhang C, Bu Y, et al. A multifunctional nano-therapeutic platform based on octahedral yolk-shell Au NR@CuS: photothermal/photodynamic and targeted drug delivery tri-combined therapy for rheumatoid arthritis. Biomaterials. 2021;277:121088. doi:10.1016/j.biomaterials.2021.121088
16. Ytterberg SR, Bhatt DL, Mikuls TR, et al. Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med. 2022;386(4):316–326. doi:10.1056/NEJMoa2109927
17. Rheumatoid arthritis memory B cells and abatacept (RAMBA) [Internet]. 2018. Available from: https://clinicaltrials.gov/study/NCT03652961.
18. Ticagrelor in methotrexate-resistant rheumatoid arthritis [Internet]. 2016. Available from: https://clinicaltrials.gov/study/NCT02874092.
19. Musculoskeletal ultrasound assessment of therapeutic response of tofacitinib in rheumatoid arthritis patients [Internet]. 2014. Available from: https://clinicaltrials.gov/study/NCT02321930.
20. A Phase 3B/4 randomized double blind placebo controlled study of methotrexate (MTX) withdrawal in subjects with rheumatoid arthritis (RA) treated with tofacitinib 11MG modified release (MR) formulation [Internet]. 2016. Available from: https://clinicaltrials.gov/study/NCT02831855.
21. Phase IV open-label study to evaluate biomarkers to predict the efficacy of abatacept in subjects with rheumatoid arthritis [Internet]. 2018. Available from: https://clinicaltrials.gov/study/NCT03882008.
22. The glucocorticoid low-dose outcome in rheumatoid arthritis study comparing the cost-effectiveness and safety of additional low-dose glucocorticoid in treatment strategies for elderly patients with rheumatoid arthritis [Internet]. 2015. Available from: https://clinicaltrials.gov/study/NCT02585258.
23. A multicenter, 2 part study to assess the efficacy and safety of acthar gel in subjects with rheumatoid arthritis with persistently active disease despite dual-DMARD treatment [Internet]. 2016. Available from: https://clinicaltrials.gov/study/NCT02919761.
24. Prospective, multicentre, placebo-controlled, double-blind interventional study to compare the efficacy of maintenance treatment with tocilizumab with or without glucocorticoid discontinuation in rheumatoid arthritis patients [Internet]. 2015. Available from: https://clinicaltrials.gov/study/NCT02573012.
25. A randomized, head-to-head, single-blinded study to assess changes in the immune profile in response to treatment with subcutaneous abatacept in combination with methotrexate versus subcutaneous adalimumab in combination with methotrexate in adults with early rheumatoid arthritis who are naive to biologic disease-modifying antirheumatic drugs [Internet]. 2015. Available from: https://clinicaltrials.gov/study/NCT02557100.
26. Improving influenza immunization responses in rheumatoid arthritis: a strategy to enhance protection against a preventable cause of death in an at risk population? [Internet]. 2016. Available from: https://clinicaltrials.gov/study/NCT02936180.
27. MIRACLE (Methotrexate inadequate response patient with rheumatoid arthritis treated by adalimumab in combination with low-dose methotrexate) study [Internet]. 2018. Available from: https://clinicaltrials.gov/study/NCT03505008.
28. Effectiveness of a combination of methotrexate and a step down glucocorticoid regimen (COBRA-Slim) for remission induction in patients with early rheumatoid arthritis (RA), with or without fast access to 24 weeks of tumor necrosis factor (TNF) blockade in insufficient responders, a randomized, multicenter, pragmatic trial [Internet]. 2018. Available from: https://clinicaltrials.gov/study/NCT03649061.
29. IL-7 and IL-7R expression in peripheral blood mononuclear cells, peripheral blood monocytes or differentiated macrophages of rheumatoid arthritis patients with active vs. inactive disease treated with DMARD and/or CIMZIA [Internet]. 2015. Available from: https://clinicaltrials.gov/study/NCT02451748.
30. Treatments against RA and effect on FDG-PET/CT (The TARGET trial) [Internet]. 2015. Available from: https://clinicaltrials.gov/study/NCT02374021.
31. A Phase 4 trial assessing the impact of residual inflammation detected via imaging techniques, drug levels and patient characteristics on the outcome of dose tapering of adalimumab in clinical remission rheumatoid ArThritis (RA) subjects (PREDICTRA) [Internet]. 2014. Available from: https://clinicaltrials.gov/study/NCT02198651.
32. A single-arm investigator initiated study to evaluate the efficacy of OC-01 (Varenicline solution) nasal spray on signs and symptoms of dry eye disease in subjects with Sjogren’s syndrome [Internet]. 2023. Available from: https://clinicaltrials.gov/study/NCT05700422.
33. Evaluating the addition of obturator nerve block to adductor canal block for total knee arthroplasty [Internet]. 2017. Available from: https://clinicaltrials.gov/study/NCT03326999.
34. Kremer JM, Genant HK, Moreland LW, et al. Effects of Abatacept in patients with methotrexate-resistant active rheumatoid arthritis: a randomized trial. Ann Intern Med. 2006;144(12):865–876. doi:10.7326/0003-4819-144-12-200606200-00003
35. Cohen SB, Pope J, Haraoui B, et al. Efficacy and safety of tofacitinib modified-release 11 mg once daily plus methotrexate in adult patients with rheumatoid arthritis: 24-week open-label phase results from a phase 3b/4 methotrexate withdrawal non-inferiority study (ORAL Shift). RMD Open. 2021;7(2):e001673. doi:10.1136/rmdopen-2021-001673
36. Burmester GR, Lin Y, Patel R, et al. Efficacy and safety of sarilumab monotherapy versus Adalimumab monotherapy for the treatment of patients with active rheumatoid arthritis (MONARCH): a randomised, double-blind, parallel-group Phase III trial. Ann Rheum Dis. 2017;76(5):840–847. doi:10.1136/annrheumdis-2016-210310
37. Yokota S, Imagawa T, Mori M, et al. Efficacy and safety of tocilizumab in patients with systemic-onset juvenile idiopathic arthritis: a randomised, double-blind, placebo-controlled, withdrawal phase III trial. Lancet. 2008;371(9617):998–1006. doi:10.1016/S0140-6736(08)60454-7
38. Fleischmann R, Furst DE. Safety of repository corticotropin injection as an adjunctive therapy for the treatment of rheumatoid arthritis. Expert Opin Drug Saf. 2020;19(8):935–944. doi:10.1080/14740338.2020.1779219
39. A multicenter, randomized, double-period, double - blind study to determine the optimal protocol for treatment initiation with methotrexate and adalimumab combination therapy in patients with early rheumatoid arthritis (OPTIMA) [Internet]. 2007. Available from: https://clinicaltrials.gov/study/NCT00420927.
40. Pickens SR, Chamberlain ND, Volin MV, et al. Characterization of interleukin-7 and interleukin-7 receptor in the pathogenesis of rheumatoid arthritis. Arthritis Rheum. 2011;63(10):2884–2893. doi:10.1002/art.30493
41. Pean De Ponfilly – Sotier M, Seror R, Nocturne G, Besson FL. 18F-FDG PET molecular imaging: a relevant tool to investigate chronic inflammatory rheumatisms in clinical practice? Front Med. 2022;9:1070445. doi:10.3389/fmed.2022.1070445
42. Pan W, Dai C, Li Y, et al. PRP-chitosan thermoresponsive hydrogel combined with black phosphorus nanosheets as injectable biomaterial for biotherapy and phototherapy treatment of rheumatoid arthritis. Biomaterials. 2020;239:119851. doi:10.1016/j.biomaterials.2020.119851
43. Singh JA. The emerging safety profile of JAK inhibitors in rheumatic diseases. BioDrugs. 2023;37(5):625–635. doi:10.1007/s40259-023-00612-7
44. Westhovens R, Annemans L. Costs of drugs for treatment of rheumatic diseases. RMD Open. 2016;2(2):e000259. doi:10.1136/rmdopen-2016-000259
45. Convertino I, Lorenzoni V, Gini R, et al. Drug-utilization, healthcare facilities accesses and costs of the first generation of JAK inhibitors in rheumatoid arthritis. Pharmaceuticals. 2023;16(3):465. doi:10.3390/ph16030465
46. Jansen JP, Incerti D, Mutebi A, et al. Cost-effectiveness of sequenced treatment of rheumatoid arthritis with targeted immune modulators. J Med Econ. 2017;20(7):703–714. doi:10.1080/13696998.2017.1307205
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Is Tofacitinib Effectiveness in Patients with Rheumatoid Arthritis Better After Conventional Than After Biological Therapy? – A Cohort Study in a Colombian Population
Santos-Moreno P, Martinez S, Ibata L, Villarreal L, Rodríguez-Florido F, Rivero M, Rojas-Villarraga A, Galarza-Maldonado C
Biologics: Targets and Therapy 2022, 16:107-117
Published Date: 13 July 2022
APOE and CCR2: Potential Macrophage-Specific Biomarkers in the Rheumatoid Arthritis Synovial Microenvironment Identified by Bioinformatics and Experimental Verification in Murine Models
Wang D, Lu L, Zhang Y, Shang W
Journal of Inflammation Research 2026, 19:587712
Published Date: 25 March 2026
Mitochondrial Hub Genes in Rheumatoid Arthritis Identified by Machine Learning and Mendelian Randomization with Experimental Validation
Luo X, Dong Z, Song Y, Hu J, Liao S, Ding X
Journal of Inflammation Research 2026, 19:576901
Published Date: 27 March 2026
Hypoxia-Inducible Factors in Rheumatoid Arthritis: Central Pathogenic Roles and Therapeutic Opportunities
Luo TT, He LX, Yin Q, Wang ZF, Zuo J
Journal of Inflammation Research 2026, 19:600186
Published Date: 23 May 2026