Back to Journals » Journal of Pain Research » Volume 19
Family Functioning and Kinesiophobia in Patients After Pacemaker Implantation: A Cross-Sectional Serial Mediation Study of Pain and Pain Catastrophizing
Authors Xu M, Zhang T, Ma J, Li Y, Jia W, Yao L
Received 14 March 2026
Accepted for publication 4 June 2026
Published 11 June 2026 Volume 2026:19 608536
DOI https://doi.org/10.2147/JPR.S608536
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rocío de la Vega
Min Xu,1 Tao Zhang,2 Jing Ma,1 Yanran Li,1 Wei Jia,1 Li Yao3
1School of Nursing, Ningxia Medical University, Yinchuan, Ningxia, People’s Republic of China; 2Medical Imaging Center, People’s Hospital of Ningxia Hui Autonomous Region, Yinchuan, Ningxia, People’s Republic of China; 3Department of Cardiology, The General Hospital of Ningxia Medical University, Yinchuan, Ningxia, People’s Republic of China
Correspondence: Li Yao, Department of cardiology, The General Hospital of Ningxia Medical University, Yinchuan, Ningxia, People’s Republic of China, Email [email protected]
Aim: This cross-sectional study aimed to explore the relationships among family functioning, pain, pain catastrophizing, and kinesiophobia in patients after permanent pacemaker implantation, and to examine the serial indirect effects of pain and pain catastrophizing.
Background: Kinesiophobia is common among patients after pacemaker implantation and may hinder participation in cardiac rehabilitation. Although previous studies have reported associations between family functioning, pain, pain catastrophizing, and kinesiophobia, how these factors are interrelated remains unclear.
Methods: This was a cross-sectional study. A convenience sample of 211 patients who underwent permanent pacemaker implantation was recruited from October 2025 to January 2026 in a tertiary hospital in Yinchuan, Ningxia, China. Data were collected using questionnaires including the Family APGAR Index, Numeric Rating Scale (NRS), Pain Catastrophizing Scale (PCS), and Tampa Scale for Kinesiophobia Heart (TSK-SV Heart). Data were analysed using descriptive statistics, Pearson correlation analysis, and serial mediation analysis with Model 6 of the PROCESS macro version 4.0.
Reporting Method: This study followed the STROBE reporting guideline.
Results: A total of 211 patients were included (mean age 66.08 years, SD = 12.67). The prevalence of kinesiophobia was 59.7%. Pearson correlation analysis showed that family functioning was negatively correlated with kinesiophobia (r = − 0.39, p < 0.001), pain (r = − 0.30, p < 0.001), and pain catastrophizing (r = − 0.34, p < 0.001). Pain was positively correlated with kinesiophobia (r = 0.39, p < 0.001) and pain catastrophizing (r = 0.33, p < 0.001). Pain catastrophizing was positively correlated with kinesiophobia (r = 0.49, p < 0.001). Serial mediation analysis revealed significant indirect effects. The serial indirect effect of family functioning on kinesiophobia through pain and pain catastrophizing was significant (effect = − 0.06, 95% CI: − 0.14 to − 0.01). The total indirect effect was − 0.58 (95% CI: − 0.88 to − 0.32).
Conclusion and Relevance to Clinical Practice: In this cross-sectional study, family functioning was associated with kinesiophobia, and pain and pain catastrophizing showed significant serial indirect effects in this relationship. These findings suggest that family support, pain management, and pain catastrophizing may be important areas for future intervention research aimed at reducing kinesiophobia and promoting cardiac rehabilitation participation. However, causal conclusions cannot be drawn because of the cross-sectional design, and longitudinal studies are needed to confirm these findings.
Keywords: kinesiophobia, family functioning, pain catastrophizing, pain, pacemaker implantation, serial indirect effects
Introduction
Permanent pacemaker implantation is a primary therapeutic intervention for patients with bradyarrhythmia and cardiac conduction disorders.1 With the accelerating ageing population and the increasing prevalence of cardiovascular diseases, the clinical use of pacemakers has expanded substantially worldwide.2 Currently, more than 3.25 million individuals globally are living with permanent pacemakers, with annual implantation rates increasing by 10%–30%.3 In China alone, approximately 166,000 devices are implanted each year.4 Although advancements in pacing technology have markedly improved survival rates and quality of life, postoperative rehabilitation challenges have received growing attention. Postoperative pain and activity restriction are among the most frequently reported complications following pacemaker implantation.5,6 Kinesiophobia, defined as an excessive and irrational fear of movement due to concerns about pain or reinjury, has emerged as a prevalent psychological response in this population.7 Evidence indicates that the incidence of kinesiophobia among patients after pacemaker implantation may reach as high as 81.4%.8 Kinesiophobia can lead patients to deliberately limit physical activity, thereby delaying cardiopulmonary and muscular recovery and increasing the risk of complications such as thrombosis and muscle atrophy.9 In addition, concerns about device-related complications, such as lead dislodgement or Twiddler syndrome, may further increase patients’ fear of movement after pacemaker implantation.10 Therefore, identifying factors associated with kinesiophobia in patients following pacemaker implantation is essential for optimising postoperative rehabilitation management.
Family functioning, which represents a crucial source of social support in chronic disease management and postoperative rehabilitation, refers to the emotional, informational and practical support perceived and received by patients from family members during the disease recovery process.11 In patients with cardiovascular diseases, family functioning has been recognised as an important external resource influencing psychological adjustment and behavioural recovery. Previous studies have demonstrated that adequate family support can alleviate negative emotions, enhance patients’ confidence in rehabilitation and promote the maintenance of health-related behaviours. Conversely, insufficient family support may intensify anxiety and avoidance tendencies, thereby reducing patients’ willingness to actively engage in rehabilitation activities.12 Compared with patients reporting lower levels of family functioning, those with stronger family support tend to achieve significantly higher postoperative quality-of-life scores.13 Persistent postoperative pain is relatively common after cardiac surgery, with approximately 37% of patients experiencing pain at 6 months postoperatively and about 17% still reporting pain more than 2 years after the procedure.14 Previous studies have shown that persistent or high-intensity pain may delay functional recovery and induce avoidance of physical activity.15 Although the present study focused on the early postoperative stage, acute postoperative pain may similarly contribute to patients’ concerns about movement and participation in rehabilitation activities. Evidence suggests that higher levels of family support are significantly associated with lower pain intensity and greater participation in rehabilitation activities, indicating that family functioning may also be related to patients’ pain experience.16
Beyond pain itself, patients’ cognitive appraisal of pain also plays an important role in the development of kinesiophobia. Pain catastrophizing refers to an exaggerated negative cognitive response to actual or anticipated pain, characterised by persistent rumination about pain, excessive concern about its consequences and feelings of helplessness.17 Previous research has demonstrated that pain catastrophizing is associated with greater pain perception, increased anxiety, and stronger avoidance behaviours, and is regarded as an important psychological correlate of kinesiophobia.18 In addition, social support has been shown to buffer individuals’ catastrophic cognitive responses to pain. A study involving patients with chronic pain reported that supportive and positive interactions with family members were significantly associated with lower levels of pain catastrophizing.19 According to the biopsychosocial model, individuals’ health outcomes are shaped by the dynamic interaction of biological, psychological and social factors.20 In the context of postoperative recovery, this model provides a theoretical rationale for examining how social factors (family functioning), biological factors (pain), and psychological factors (pain catastrophizing) jointly influence kinesiophobia.
The fear-avoidance model provides a theoretical framework suggesting that pain may be associated with negative cognitive appraisals such as pain catastrophizing, which may in turn relate to fear of movement and avoidance behaviours.21 However, no study has yet tested whether pain and pain catastrophizing sequentially mediate the association between family functioning and kinesiophobia in patients after pacemaker implantation. Therefore, guided by the biopsychosocial model and fear-avoidance framework, the present cross-sectional study aimed to investigate the associations among family functioning, pain, pain catastrophizing and kinesiophobia, and to test the serial indirect effects of pain and pain catastrophizing in the association between family functioning and kinesiophobia. Based on this framework, the following hypotheses were proposed: H1: Family functioning is associated with kinesiophobia. H2: Pain has an indirect effect in the association between family functioning and kinesiophobia. H3: Pain catastrophizing has an indirect effect in the association between family functioning and kinesiophobia. H4: Pain and pain catastrophizing have a serial indirect effect in the association between family functioning and kinesiophobia.
Materials and Methods
Participants
This study employed a cross-sectional design. From October 2025 to January 2026, using convenience sampling, all eligible patients admitted to the cardiology department, general medical wards, and geriatric wards of a tertiary hospital in Yinchuan, Ningxia, China were consecutively invited to participate. Questionnaires were administered on postoperative days 2–3, once patients’ vital signs were stable and pacemaker function (pacing and sensing) was verified as normal. This timeframe allowed patients to complete the assessments cooperatively and reflected the early postoperative rehabilitation stage following pacemaker implantation. The inclusion criteria were: (1) age ≥ 18 years; (2) first-time implantation of a single- or dual-chamber pacemaker; (3) New York Heart Association (NYHA) functional class ≤ III; (4) ability to communicate effectively and cooperate with the assessment; and (5) provision of written informed consent. The exclusion criteria were: (1) presence of malignant tumors or severe diseases affecting major systems such as the brain or kidneys; (2) occurrence of serious intraoperative or postoperative complications (eg, persistent fresh bleeding from the surgical wound); (3) impaired consciousness; and (4) pre-existing chronic pain conditions or diagnosed mental health disorders.
The required sample size was estimated using the Cochran formula:  , where α was set at 0.05 and Zα/2 = 1.96, corresponding to a 95% confidence interval (CI). The allowable margin of error (δ) was set at 0.06, and the estimated prevalence (π) of kinesiophobia (78%) was derived from Xu Yulin (2025).22 Based on these parameters, the minimum required sample size was calculated to be 184. Considering a potential non-response rate of 10%, the final required sample size was increased to 205 participants. A total of 211 patients were ultimately included. For mediation analysis, Fritz and MacKinnon (2007) recommend a minimum of 148 participants to detect a medium‑sized indirect effect with 80% power, a threshold met by the present sample.23
, where α was set at 0.05 and Zα/2 = 1.96, corresponding to a 95% confidence interval (CI). The allowable margin of error (δ) was set at 0.06, and the estimated prevalence (π) of kinesiophobia (78%) was derived from Xu Yulin (2025).22 Based on these parameters, the minimum required sample size was calculated to be 184. Considering a potential non-response rate of 10%, the final required sample size was increased to 205 participants. A total of 211 patients were ultimately included. For mediation analysis, Fritz and MacKinnon (2007) recommend a minimum of 148 participants to detect a medium‑sized indirect effect with 80% power, a threshold met by the present sample.23
Data Collection
This study was approved by the Ethics Committee of a tertiary hospital in Yinchuan, China. Prior to the survey, all researchers received standardized training on data collection procedures. During the survey, the purpose and procedures of the study were explained to all participants, and written informed consent was obtained. Data were collected through face-to-face interviews using structured questionnaires. After collection, two trained researchers independently reviewed the questionnaires to ensure completeness and consistency. A total of 220 questionnaires were distributed. Nine were excluded due to invalid responses: two had >20% missing data, three had missing key variables, and four showed patterned responses. No imputation methods were applied. Ultimately, 211 valid questionnaires were included (effective response rate: 95.9%). The final sample size met the minimum sample size requirement estimated for this study.
Measures
Demographic Characteristics
A self-designed questionnaire was used to collect participants’ demographic and clinical information, including sex, age, marital status, educational level, personal financial status, medical payment method, and New York Heart Association (NYHA) functional classification.
Family APGAR Index
Family functioning was assessed using the Family Adaptation, Partnership, Growth, Affection, and Resolve (APGAR) Index, developed by Smilkstein in 1982.24 The scale measures individuals’ satisfaction with family functioning and consists of five items covering adaptation, partnership, growth, affection, and resolve. Each item is rated on a three-point Likert scale (0–2). Total scores range from 0 to 10, with scores of 0–3 indicating severe family dysfunction, 4–6 moderate dysfunction, and 7–10 good family functioning. The Chinese version has shown good reliability, with a Cronbach’s α of 0.830.25
Numeric Rating Scale for Pain (NRS)
Pain intensity was assessed using the Numeric Rating Scale (NRS), a widely used unidimensional measure of pain. Participants were asked to rate their pain on a scale ranging from 0 to 10, where 0 indicates no pain and 10 represents the worst possible pain. Scores of 1–3 indicate mild pain, 4–6 moderate pain, and 7–10 severe pain.26 The NRS has demonstrated good reliability and validity in clinical populations. Previous research reported a Cronbach’s α greater than 0.88, indicating good internal consistency and stability.27
Pain Catastrophizing Scale (PCS)
Pain catastrophizing was measured using the Pain Catastrophizing Scale (PCS).17 The Chinese version includes 13 items across three dimensions: rumination (4 items), magnification (3 items), and helplessness (6 items). Each item is rated on a five-point Likert scale ranging from 0 (“not at all”) to 4 (“all the time”), with total scores ranging from 0 to 52. Higher scores indicate greater pain catastrophizing. The scale demonstrated excellent internal consistency, with a reported Cronbach’s α of 0.927.28
Tampa Scale for Kinesiophobia Heart (TSK-SV Heart)
Kinesiophobia was assessed using the short version of the Tampa Scale for Kinesiophobia Heart (TSK-SV Heart), developed by Bäck et al in 2012.29 The scale consists of 17 items across four dimensions, including fear of injury, fear of physical activity, avoidance of exercise, and dysfunctional beliefs. Each item is rated on a four-point Likert scale ranging from 1 (“completely disagree”) to 4 (“completely agree”). Items 4, 8, 12, and 16 are reverse-scored. Total scores range from 17 to 68, with higher scores indicating greater levels of kinesiophobia. A score greater than 37 suggests the presence of kinesiophobia. The scale demonstrated acceptable reliability, with a reported Cronbach’s α of 0.859.30
Statistical Analyses
All statistical analyses were performed using IBM SPSS Statistics version 27.0. The mediation analysis was conducted using the PROCESS macro for SPSS, version 4.0 (written by Andrew F. Hayes). Harman’s single-factor test was performed to assess common method bias.31 All measurement items from the core instruments were entered into an unrotated exploratory factor analysis.
Continuous variables were expressed as mean and standard deviation (SD), while skewed data were presented as median and interquartile range (IQR). Group differences in continuous variables were analyzed using independent-samples t-tests, and categorical variables were presented as frequencies and compared using the chi-square (χ²) test. Pearson’s bivariate correlation analysis was conducted to examine the relationships between variables. Before conducting the correlation and mediation analyses, assumptions including normality, linearity, multicollinearity, and influential outliers were examined. Multicollinearity was assessed using variance inflation factor (VIF) values. Serial mediation analysis was conducted using Model 6 of the PROCESS macro. The significance of regression coefficients and indirect effects was evaluated using a bootstrap method with 5000 resamples to generate 95% confidence intervals (CI). An indirect effect was considered statistically significant if the 95% CI did not include zero.
Ethical Considerations
This study was approved by the Ethics Committee of the General Hospital of Ningxia Medical University and was conducted in accordance with the Declaration of Helsinki (Approval No. KYLL-2023-0259). All participants were fully informed of the study purpose, procedures, potential risks, and benefits, and provided written informed consent prior to participation.
Results
Common Method Bias Test
Harman’s single-factor test was conducted to examine common method bias. All 37 items from the core instruments—the Numeric Rating Scale (NRS), Family APGAR Index, Pain Catastrophizing Scale (PCS), and Tampa Scale for Kinesiophobia Heart (TSK-SV Heart)—were entered simultaneously into an unrotated exploratory factor analysis. The results showed that six factors with eigenvalues greater than 1 were extracted. The first factor accounted for 28.36% of the total variance, which was below the critical threshold of 40%, indicating that common method bias was unlikely to be a serious issue.
Socio-Demographic Characteristics
Among the 211 participants, 59.7% (n = 126) exhibited kinesiophobia. The participants’ ages ranged from 25 to 89 years, with a mean age of 66.08 (12.67) years, and 46.9% were male. As shown in Table 1, significant differences were observed between the kinesiophobia group and the non-kinesiophobia group in age, educational level, medical payment method, and New York Heart Association (NYHA) classification after permanent pacemaker implantation (p < 0.05).
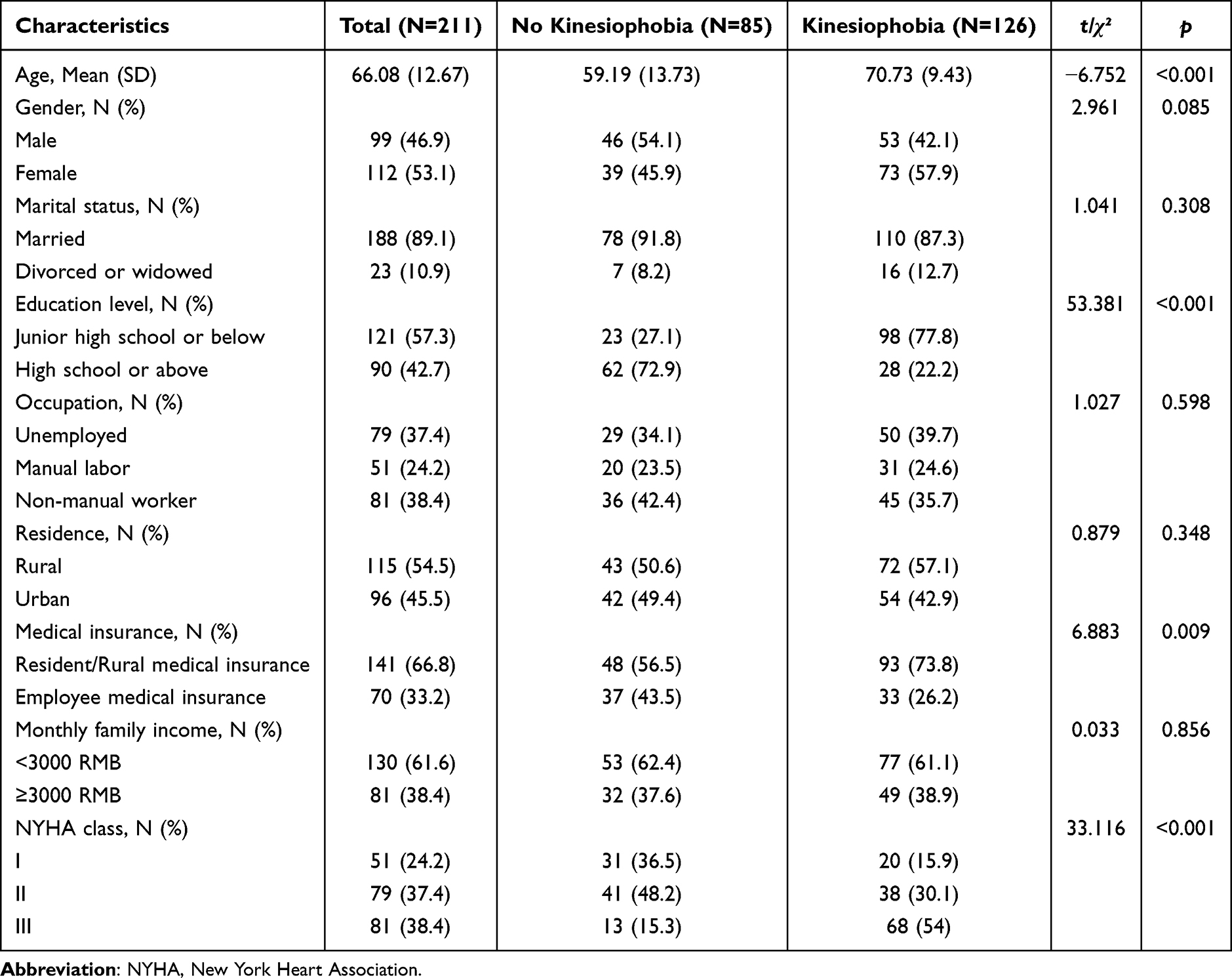 |
Table 1 Participant Characteristics Stratified by Kinesiophobia Status (N=211) |
Scale Scores
As shown in Table 2, the distributions of the Family APGAR Index, pain intensity, pain catastrophizing, and kinesiophobia scores were skewed. The median scores were 7.00 (IQR: 5–9) for family functioning, 2.00 (IQR: 1–3) for pain intensity, 21 (IQR: 13–31) for pain catastrophizing, and 44 (IQR: 31–48) for kinesiophobia.
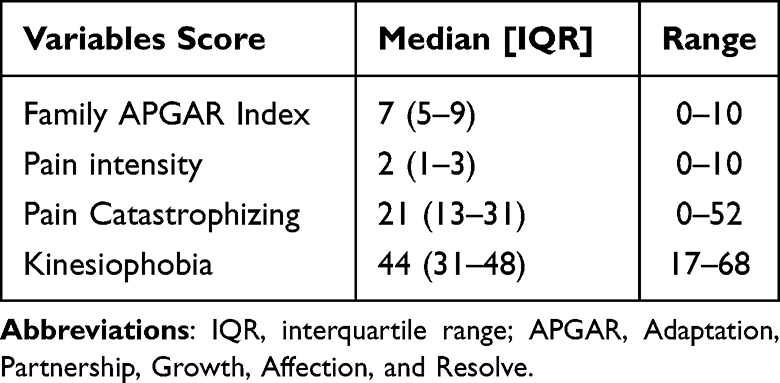 |
Table 2 Descriptive Statistics of Study Variables (N = 211) |
Correlation Analysis of Family Functioning, Pain, Pain Catastrophizing, and Kinesiophobia
Pearson’s correlation analysis showed that family functioning had weak to moderate negative correlations with pain (r = −0.30, p < 0.001), pain catastrophizing (r = −0.34, p < 0.001), and kinesiophobia (r = −0.39, p < 0.001). Pain showed a weak positive correlation with pain catastrophizing (r = 0.33, p < 0.001) and a moderate positive correlation with kinesiophobia (r = 0.39, p < 0.001). Pain catastrophizing showed a moderate positive correlation with kinesiophobia (r = 0.49, p < 0.001). The detailed results are presented in Table 3.
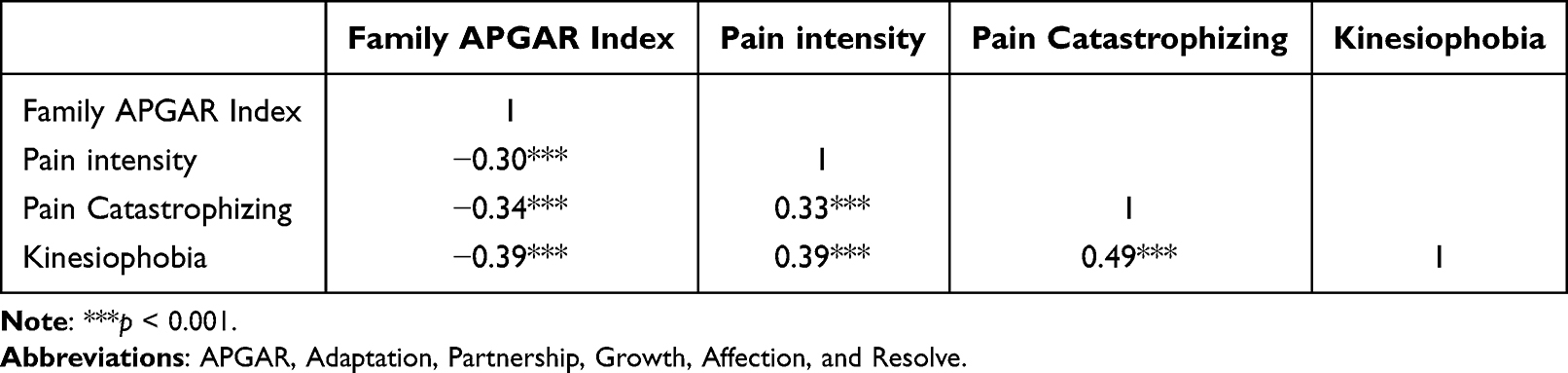 |
Table 3 Correlation Analysis of Variables (N=211) |
Path Analysis and Mediation Effects
Based on the univariate analyses (Table 1), age, educational level, method of medical payment, and NYHA class were included as covariates in the mediation model. Prior to the mediation analysis, multicollinearity diagnostics were examined. Variance inflation factor (VIF) values ranged from 1.17 to 1.21, indicating no evidence of significant multicollinearity among the study variables. The regression results indicated that family functioning was negatively associated with pain (B = −0.14, p < 0.001) and pain catastrophizing (B = −1.23, p < 0.001), while pain was positively associated with pain catastrophizing (B = 1.74, p < 0.01). In the model predicting kinesiophobia, both pain (B = 1.49, p < 0.01) and pain catastrophizing (B = 0.25, p < 0.001) showed significant positive associations, whereas family functioning showed a significant negative association (B = −0.70, p < 0.05). All reported coefficients are unstandardized coefficients (B). The serial mediation model is shown in Figure 1, and the regression results are presented in Table 4.
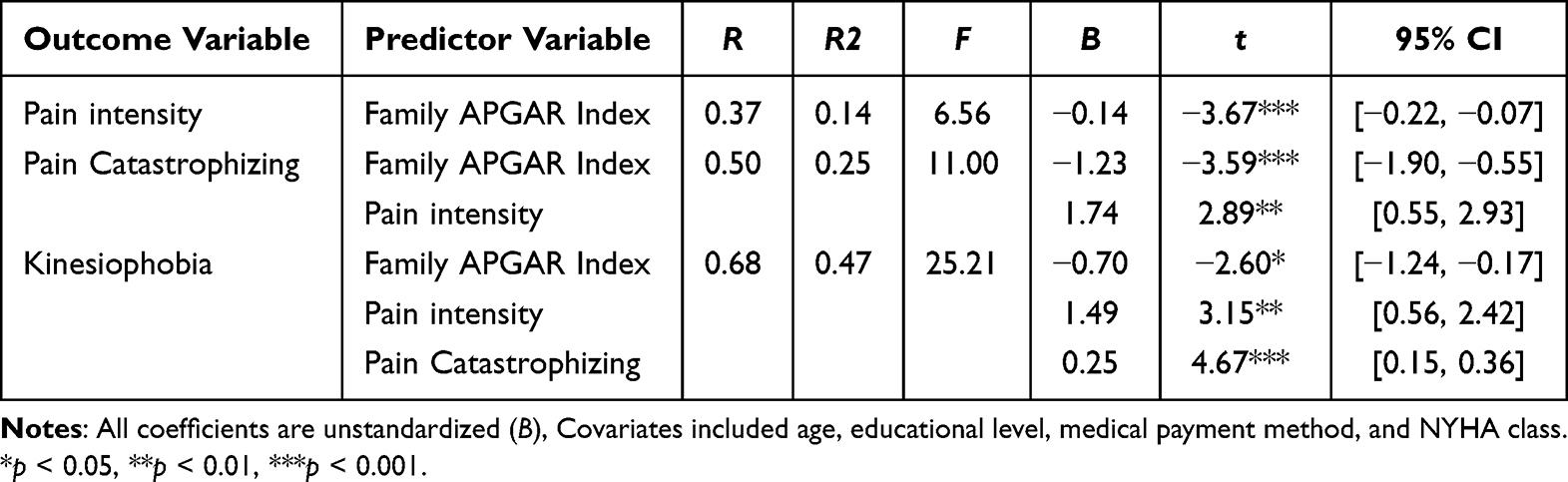 |
Table 4 Regression Analysis for the Serial Mediation Model |
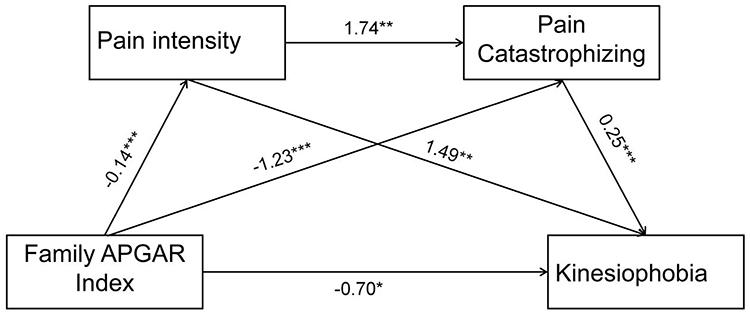 |
Figure 1 The serial mediation model of family functioning, pain intensity, pain catastrophizing, and kinesiophobia in patients after permanent pacemaker implantation. Values are unstandardized coefficients. The model was adjusted for age, educational level, medical payment method, and NYHA class. *p < 0.05, **p < 0.01,***p < 0.001. |
Bias-corrected bootstrap analysis with 5000 resamples was performed to estimate the confidence intervals of the direct and indirect effects. The total effect of family functioning on kinesiophobia was −1.28, of which the direct effect was −0.70, accounting for 54.79% of the total effect. Pain and pain catastrophizing showed significant serial indirect effects in the association between family functioning and kinesiophobia, with a total indirect effect of −0.58, accounting for 45.21% of the total effect. Three significant mediation pathways were identified: (1) family functioning → pain → kinesiophobia (effect = −0.21, 16.32% of the total effect); (2) family functioning → pain catastrophizing → kinesiophobia (effect = −0.31, 24.08% of the total effect); (3) family functioning → pain → pain catastrophizing → kinesiophobia (effect = −0.06, 4.81% of the total effect). Detailed mediation results are presented in Table 5.
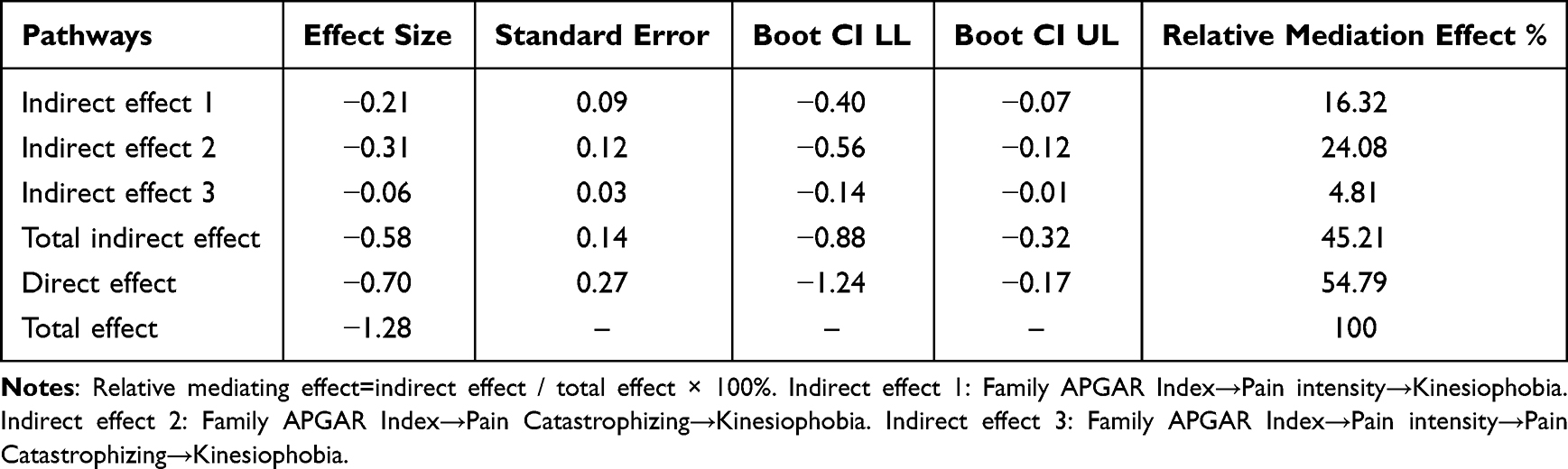 |
Table 5 Analysis of the Mediating Role of Pain Intensity and Pain Catastrophizing |
Discussion
This study explored the relationships among family functioning, pain, pain catastrophizing, and kinesiophobia in patients after permanent pacemaker implantation and tested a serial mediation model. The findings showed that family functioning was associated with kinesiophobia both directly and indirectly through its associations with pain and pain catastrophizing, as well as through their sequential indirect pathway. These findings provide additional insight into biopsychosocial factors associated with postoperative kinesiophobia and may help inform future nursing intervention research.
In this study, family functioning was significantly negatively associated with kinesiophobia, suggesting that lower family functioning was related to higher levels of kinesiophobia, which is consistent with previous studies.32 One possible explanation is that some family members may underestimate the importance of postoperative rehabilitation after pacemaker implantation and lack sufficient health knowledge to provide adequate support during recovery. As a result, patients may receive less assistance and encouragement in daily activities and rehabilitation exercises, which may increase concerns about potential discomfort or device-related risks during movement and lead to avoidance of physical activity.33,34 In some cases, concerns about device-related complications, such as lead dislodgement, Twiddler syndrome, or upper-limb neurovascular symptoms, may further increase patients’ fear of movement after pacemaker implantation.35,36 In addition, insufficient family support may increase negative emotional experiences, such as loneliness or helplessness, which may further contribute to fear of movement.37
Previous systematic reviews have reported that the prevalence of kinesiophobia among patients with cardiovascular disease is approximately 61%, which is consistent with the present findings and suggests that kinesiophobia is common in this population.38 Further analysis showed that kinesiophobia was significantly associated with age, medical payment method, educational level, and New York Heart Association (NYHA) functional class. With increasing age, declining physiological reserve may heighten concerns about cardiac workload and adverse events, which may be associated with stronger avoidance tendencies. Patients with a higher out-of-pocket medical burden may experience greater anxiety about disease recurrence or rehospitalization.39 In addition, individuals with lower educational levels may have limited ability to interpret health information and recognize risks, making them more likely to perceive exercise-related discomfort as a potential danger. Patients with more severe NYHA functional class often have lower confidence in their tolerance for physical activity, which may further increase the likelihood of kinesiophobia.40 Therefore, healthcare professionals should pay attention to these factors and consider interventions aimed at improving rehabilitation participation and reducing movement-related concerns.
The results of this study showed that pain partially accounted for the association between family functioning and kinesiophobia, representing 36.21% of the total indirect effect. Pain, defined as an unpleasant sensory and emotional experience associated with tissue damage, is one of the common symptoms experienced by patients after permanent pacemaker implantation.41 During this early postoperative stage, patients require both careful nursing care and emotional support. Family members may not always have sufficient knowledge or confidence to provide appropriate support for early mobilization and pain management after pacemaker implantation.42 Insufficient family support may limit patients’ access to emotional and caregiving resources, which may make patients more attentive to postoperative discomfort and contribute to a more negative pain experience. In turn, patients with higher pain levels may be more cautious about movement because of concerns about discomfort, which may be reflected in lower willingness to engage in activity and higher kinesiophobia scores.37,43 Therefore, early postoperative management should include pain assessment, appropriate analgesic treatment, and family involvement in rehabilitation care.
This study also found that pain catastrophizing partially accounted for the association between family functioning and kinesiophobia, representing 53.45% of the total indirect effect. Family functioning was negatively correlated with pain catastrophizing, which is consistent with previous findings.44 Patients after pacemaker implantation may experience postoperative pain, restricted upper-limb movement, and concerns about device-related complications, which may increase negative cognitive evaluations of pain.6 Previous studies have shown that adequate family support can alleviate pain experiences and reduce catastrophic thinking, whereas insufficient support may lead patients to focus excessively on pain and its potential consequences.32,45 Pain catastrophizing, in turn, has been identified as an important psychological factor associated with kinesiophobia. Consistent with previous findings, this study also found a positive association between pain catastrophizing and kinesiophobia.18,46 Therefore, adequate family support may be associated with lower kinesiophobia by alleviating catastrophic pain-related cognition. Clinically, healthcare professionals should identify patients with pain catastrophizing tendencies and provide health education and emotional support to promote participation in cardiac rehabilitation.
The results demonstrated a significant serial indirect effect of family functioning on kinesiophobia through pain and pain catastrophizing. Specifically, lower family functioning was associated with higher acute postoperative pain, while higher pain levels were also associated with stronger pain catastrophizing and higher kinesiophobia. This pattern is consistent with the fear-avoidance model, in which pain-related cognitive appraisal is considered an important link between pain experience and fear of movement. Previous studies have often examined the factors of kinesiophobia from single domains, such as pain intensity or psychological cognition, whereas relatively few studies have explored the combined effects of social support, pain experience, and cognitive appraisal.15,18 From a biopsychosocial perspective, the present findings highlight a potential pathway through which family functioning is associated with kinesiophobia through both pain and pain catastrophizing. According to the biopsychosocial model, social support may buffer negative emotional responses to pain and influence individuals’ cognitive appraisal processes, thereby reducing catastrophic thinking and improving perceptions of exercise-related discomfort.47 Previous studies have also shown that patients with higher levels of pain catastrophizing are more likely to interpret exercise-related discomfort as a potential threat, which may reduce participation in physical activity and increase kinesiophobia.16 Therefore, in addition to strengthening postoperative pain management, healthcare professionals should also pay attention to patients’ pain catastrophizing tendencies and encourage family members to actively participate in rehabilitation care to reduce excessive concerns about pain and promote engagement in cardiac rehabilitation.
Limitations
This study has several limitations. First, the cross-sectional design limits the ability to establish causal relationships among family functioning, pain, pain catastrophizing, and kinesiophobia. Therefore, the mediation findings should be interpreted as cross-sectional statistical indirect effects rather than evidence of causal mediation, and future longitudinal studies are needed to further confirm these associations. Second, questionnaires were administered on postoperative days 2–3; therefore, pain scores mainly reflected acute postoperative pain, and kinesiophobia may have represented early concerns about movement and device-related safety rather than a stable long-term rehabilitation-related pattern. Third, kinesiophobia was assessed using a self-reported scale and was not combined with objective measures of physical activity, shoulder range of motion, or rehabilitation participation. Future research may incorporate objective indicators to provide a more comprehensive assessment. In addition, all variables were assessed using self-reported questionnaires at a single time point, which may have increased the risk of common method bias. Fourth, convenience sampling was used, and participants were recruited from a single tertiary hospital, which may have introduced selection bias and limited the representativeness and generalisability of the findings. Finally, some potentially relevant factors, such as anxiety, depression, preoperative pain, previous physical activity, comorbidities, and postoperative complications, were not included in the analysis. These unmeasured variables may have influenced the observed associations and should be considered in future studies.
Conclusion
The present study showed that family functioning was associated with kinesiophobia in patients after permanent pacemaker implantation, and pain and pain catastrophizing showed significant separate and serial indirect effects in this cross-sectional model. These findings suggest that postoperative kinesiophobia may be understood from a biopsychosocial perspective involving family support, acute postoperative pain, and pain-related catastrophic cognition. Given the cross-sectional design, these associations should be confirmed in future longitudinal studies. Clinically, the findings may help nurses identify patients at risk of kinesiophobia during the early postoperative period and inform future intervention research aimed at improving rehabilitation participation after pacemaker implantation.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Ningxia Nursing Association (Grant No. NXHL22-22).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Glikson M, Nielsen JC, Kronborg MB, et al. 2021 ESC guide-lines on cardiac pacing and cardiac resynchronization therapy. Europace. 2022;24(1):71–11. doi:10.1093/europace/euab232
2. Chinese Society of Pacing and Electrophysiology, Chinese Medical Association; Arrhythmia Committee, Chinese Medical Doctor Association. Chinese expert consensus on the evaluation and management of patients with bradycardia and conduction disorders (2020). Chin J Cardiac Arrhyth. 2021;25(3):185–211.
3. Liu S, Zuo J. Research progress on rehabilitation exercise after permanent cardiac pacemaker implantation. Guangxi Med J. 2022;44(18):2163–2166.
4. The Writing Committee of the Report on Cardiovascular Health and Diseases in China. Report on cardiovascular health and diseases in China 2024: an updated summary. Chin Circ J. 2025;40(6):521–559.
5. Daniels JD, Sun S, Zafereo J, et al. Preventing shoulder pain after cardiac rhythm management device implantation: a randomized, controlled study. Pacing Clin Electrophysiol. 2011;34(6):672–678. doi:10.1111/j.1540-8159.2010.03026.x
6. Yu J, Chen F, Ren Y, Zeng J. Kinesiophobia, exercise self-efficacy, and physical activity in patients with permanent pacemaker implantation: a latent profile and mediation analysis. Geriatr Nurs. 2026;68:103828. doi:10.1016/j.gerinurse.2026.103828
7. Wang Z, Zhang Y, Wang Y, Liu L, Zhang J. Kinesiophobia and its associated factors in patients with coronary heart disease: a cross-sectional study based on latent feature analysis. BMJ Open. 2023;13(7):e072170. doi:10.1136/bmjopen-2023-072170
8. Wang L, Lv L, Li L, et al. Kinesiophobia and influencing factors among 172 patients after permanent pacemaker implantation. J Nurs. 2024;31(23):18–22.
9. Taylor RS, Dalal HM, McDonagh STJ. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat Rev Cardiol. 2022;19(3):180–194. doi:10.1038/s41569-021-00611-7
10. Navarro-Gonzalez J, Durán Caamaño M, Lara Pedreros C, Sepulveda K. A case of twiddler’s syndrome: a rare complication of pacemakers. Cureus. 2024;16(10):e71923. doi:10.7759/cureus.71923
11. Wang Y, Masingboon K, Wacharasin C. Mediating role of self-efficacy in the relationship between family functioning and self-management behaviors in patients with coronary heart disease: a cross-sectional study in Jiangsu, China. Belitung Nurs J. 2025;11(1):59–66. doi:10.33546/bnj.3638
12. Shi Y, Liang Z, Zhang Y, Zhu L, Gao G, Li J. The relationships among family function, psychological resilience, and social network of patients with chronic disease in the community. Geriatr Nurs. 2024;60:52–58. doi:10.1016/j.gerinurse.2024.08.038
13. Wang MM, Chen DM, Zhang O, et al. Effect of family support on quality of postoperative life in patients with digestive cancer. Ann Palliat Med. 2020;9(4):2072–2078. doi:10.21037/apm-20-1129
14. Guimarães-Pereira L, Reis P, Abelha F, Azevedo LF, Castro-Lopes JM. Persistent postoperative pain after cardiac surgery: a systematic review with meta-analysis regarding incidence and pain intensity. Pain. 2017;158(10):1869–1885. doi:10.1097/j.pain.0000000000000997
15. Sharif-Nia H, Nazari R, Hajihosseini F, et al. The relationship of fear of pain, pain anxiety, and fear-avoidance beliefs with perceived stress in surgical patients with postoperative kinesiophobia. BMC Psychol. 2025;13(1):420. doi:10.1186/s40359-025-02743-8
16. Zhang X, Zhang R, Lin X, Zeng L, Zhang J. The impact of social support on pain intensity in older adults with chronic pain: the serial mediating roles of positive and negative affect and pain catastrophizing. BMC Geriatr. 2026;26(1):289. doi:10.1186/s12877-026-07081-x
17. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychological Assessment. 1995;7(4):524–532. doi:10.1037/1040-3590.7.4.524
18. Wang J, Chen Y. Pain catastrophizing, kinesiophobia, and exercise adherence in postoperative cardiovascular surgery patients: the mediating role of exercise self-efficacy. J Rehabil Med. 2025;57:jrm43853. doi:10.2340/jrm.v57.43853
19. Mohammadi S, Alinajimi F, Esmaeilian N, Dehghani M, Khatibi A. Pain catastrophizing thoughts explain the link between perceived caregiver responses and pain behaviors of patients with chronic musculoskeletal pain. Front Psychol. 2020;11:1386. doi:10.3389/fpsyg.2020.01386
20. Borrell-Carrió F, Suchman AL, Epstein RM. The biopsychosocial model 25 years later: principles, practice, and scientific inquiry. Ann Fam Med. 2004;2(6):576–582. doi:10.1370/afm.245
21. Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317–332. doi:10.1016/S0304-3959(99)00242-0
22. Xu Y, Li H, Wang X, et al. Social participation and influencing factors among young and middle-aged patients after pacemaker implantation. J Nurs Sci. 2025;40(19):21–25.
23. Fritz MS, Mackinnon DP. Required sample size to detect the mediated effect. Psychol Sci. 2007;18(3):233–239. doi:10.1111/j.1467-9280.2007.01882.x
24. Smilkstein G. The physician and family function assessment[J]. Family Syst Ems Med. 1984;2(3):263–278. doi:10.1037/h0091661
25. Lv F, Gu Y. Family APGAR questionnaire and its clinical application. Foreign Med Sci. 1995;11(2):56–59.
26. Li CR, Zhang W, Fan BF. Comparison of the Numerical Rating Scale (NRS) and Verbal Rating Scale (VRS) in elderly patients with chronic pain. Chin J Pain Med. 2016;22(9):683–686.
27. Wang YJ, Zhou HJ, Yuan Y, et al. Reliability of the numerical rating scale in evaluating dysesthesia at key points in patients with spinal cord injury. Chin J Rehabil Theory Pract. 2019;25(10):1117–1119.
28. Yap JC, Lau J, Chen PP, et al. Validation of the Chinese Pain Catastrophizing Scale (HK-PCS) in patients with chronic pain. Pain Med. 2008;9(2):186–195. doi:10.1111/j.1526-4637.2007.00307.x
29. Bäck M, Jansson B, Cider Å, Herlitz J, Lundberg M. Validation of a questionnaire to detect kinesiophobia (fear of movement) in patients with coronary artery disease. J Rehab Med. 2012;44(4):363–369. doi:10.2340/16501977-0942
30. Lei MJ, Liu TT, Xiong SQ, et al. Chinese translation and validation of the Tampa Scale for Kinesiophobia in patients with heart disease. Chin Nurs Manage. 2019;19(11):1637–1642.
31. Harman HH. Modern Factor Analysis. Chicago, IL: University of Chicago Press; 1976.
32. You M, Mou Q, Cao X, et al. Kinesiophobia and associated factors among patients after cardiac surgery under cardiopulmonary bypass: a cross-sectional study. Front Psychiatry. 2025;16:1584789. doi:10.3389/fpsyt.2025.1584789
33. Yang Z, Zheng X, Hu N, Zhang F, Wang A. “Challenges to Normalcy”- perceived barriers to adherence to home-based cardiac rehabilitation exercise in patients with chronic heart failure. Patient Prefer Adherence. 2023;17:3515–3524. doi:10.2147/PPA.S440984
34. Gao X, Yang J, Cao W, Liu Y, Zhao T. Knowledge, attitudes, and practices regarding cardiac rehabilitation among patients with chronic heart failure and their families: a cross-sectional study. J Multidiscip Healthc. 2025;18:7073–7087. doi:10.2147/JMDH.S553152
35. Yalçınkaya B, Çolak AF, Abacıoğlu HB, Özçakar L. Sonographic follow up for brachial plexopathy after a pacemaker implantation. Neurol Sci. 2025;46(8):4077–4079. doi:10.1007/s10072-025-08117-7
36. Hsu PC, Chang KV, Mezian K, et al. Sonographic pearls for imaging the brachial plexus and its pathologies. Diagnostics. 2020;10(5):324. doi:10.3390/diagnostics10050324
37. Franqueiro AR, Yoon J, Crago MA, Curiel M, Wilson JM. The interconnection between social support and emotional distress among individuals with chronic pain: a narrative review. Psychol Res Behav Manag. 2023;16:4389–4399. doi:10.2147/PRBM.S410606
38. Liu L, Yang Q, Li T, et al. Prevalence and influencing factors of kinesiophobia in patients with heart disease: a meta-analysis and systematic review. Sci Rep. 2024;14(1):18956. doi:10.1038/s41598-024-69929-9
39. Xiang Q, Xiong XY, Zhang MJ, et al. Incidence and influencing factors of kinesiophobia in patients with chronic heart failure: a scoping review. Front Psychol. 2024;15:1395199. doi:10.3389/fpsyg.2024.1395199
40. Shen Z, Geng D, Huang C, et al. Kinesiophobia and its associated factors among patients after transcatheter aortic valve replacement: a cross-sectional study based on latent profile analysis. BMC Cardiovasc Disord. 2025;25(1):477. doi:10.1186/s12872-025-04934-y
41. Goldthorpe SB. Pain after pacemaker/ICD implants. Br J Cardiol. 2022;29(3):24. doi:10.5837/bjc.2022.024
42. Beheshtaeen F, Molazem Z, Kalyani MN, Mohebbi Z. Caregiver burden reduction program among family caregivers of patients undergoing coronary artery bypass graft surgery: designing and evaluating. BMC Nurs. 2025;24(1):1258. doi:10.1186/s12912-025-03918-9
43. Mekonnen Y, Gashaw M, Abich Y, et al. Kinesiophobia and associated factors among people with musculoskeletal disorders in Ethiopia: a multicenter cross-sectional study. BMC Musculoskelet Disord. 2025;26(1):55. doi:10.1186/s12891-025-08306-7
44. Ai S, Wang Y, Niu P, Xiao W, Xu G, Zhu C. Pain catastrophizing and acute post-surgical pain in knee arthroplasty patients: the moderating role of social support. J Pain Res. 2024;17:3127–3136. doi:10.2147/JPR.S474652
45. Zeng Z, Wan L, Zheng J, Shen Y, Luo H, He M. Summary of the best evidence for the management of kinesiophobia in patients after cardiac surgery. BMC Cardiovasc Disord. 2025;25(1):127. doi:10.1186/s12872-025-04570-6
46. Zhou Y, Gao W, Cao Z, et al. Network analysis of pain catastrophizing, self-efficacy, and kinesiophobia among patients after total knee arthroplasty: a cross-sectional study. Patient Prefer Adherence. 2024;18:1897–1906. doi:10.2147/PPA.S452773
47. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–136. doi:10.1126/science.847460
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sex Differences in the Mediating Effect of Kinesiophobia on Chronic Pain, Dysesthesia, and Health-Related Quality of Life in Japanese Individuals Aged 65 Years Old and Older Treated with Surgery for Lumbar Spinal Stenosis
Higuchi D, Kondo Y, Watanabe Y, Miki T
Journal of Pain Research 2022, 15:1845-1854
Published Date: 30 June 2022
Pain Empathy and Its Association with the Clinical Pain in Knee Osteoarthritis Patients
Zhao R, Ji Y, Li J, Li X, Wu T, Wu H, Liu C
Journal of Pain Research 2022, 15:4017-4027
Published Date: 19 December 2022
Pain Catastrophizing, Kinesiophobia and Exercise Adherence in Patients After Total Knee Arthroplasty: The Mediating Role of Exercise Self-Efficacy
Zhou Y, Gao W, Gao S, Guo X, Liu M, Cao C
Journal of Pain Research 2023, 16:3993-4004
Published Date: 21 November 2023
Network Analysis of Pain Catastrophizing, Self-Efficacy, and Kinesiophobia Among Patients After Total Knee Arthroplasty: A Cross-Sectional Study
Zhou Y, Gao W, Cao Z, Gao S, Guo X, Liu M, Cao C
Patient Preference and Adherence 2024, 18:1897-1906
Published Date: 16 September 2024
Depression and Anxiety as Mediators Between Family Functioning and Academic Burnout in First-Year Traditional Chinese Medicine Students
Zhang Y, Liu J, Wang X, Cheng J, Wang X, Zheng C, Liu Q, Li W
Psychology Research and Behavior Management 2025, 18:1717-1727
Published Date: 12 August 2025