Back to Journals » Journal of Pain Research » Volume 16
Pain Catastrophizing, Kinesiophobia and Exercise Adherence in Patients After Total Knee Arthroplasty: The Mediating Role of Exercise Self-Efficacy
Authors Zhou Y ![]() , Gao W, Gao S, Guo X, Liu M, Cao C
, Gao W, Gao S, Guo X, Liu M, Cao C
Received 18 August 2023
Accepted for publication 31 October 2023
Published 21 November 2023 Volume 2023:16 Pages 3993—4004
DOI https://doi.org/10.2147/JPR.S432106
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Yi Zhou,1 Weina Gao,2 Shumin Gao,2 Xutong Guo,2 Meng Liu,2 Congjie Cao1
1School of Nursing, Langfang Health Vocational College, Langfang, Hebei, People’s Republic of China; 2Department of Orthopedics, Baoding No.1 Central Hospital, Baoding, Hebei, People’s Republic of China
Correspondence: Weina Gao, Department of Orthopedics, Baoding No.1 Central Hospital, No. 320, Changcheng North Street, Lianchi District, Baoding, Hebei, 071000, People’s Republic of China, Tel/Fax +86 312-5975023, Email [email protected]
Purpose: To examine whether exercise self-efficacy mediates the contributions of pain catastrophizing and kinesiophobia to exercise adherence in patients after total knee arthroplasty.
Patients and Methods: A cross-sectional study design was conducted. A total 211 post-total knee arthroplasty patients were recruited from three orthopedics units of a tertiary hospital in China. Participants were invited to complete questionnaires on pain catastrophizing, kinesiophobia, exercise self-efficacy, and exercise adherence. Mplus 8.3 software was used to construct mediation models.
Results: Pain catastrophizing and kinesiophobia were negatively correlated with exercise adherence (r = − 0.509, r = − 0.605, p < 0.001 respectively), while exercise self-efficacy were positively associated with exercise adherence (r = 0.799, p < 0.001). The results found exercise self-efficacy mediated the correlations of pain catastrophizing and kinesiophobia with exercise adherence after adjusting for demographic and clinical covariates. Pain catastrophizing indirectly affected patients’ exercise adherence through its effect on exercise efficacy (indirect effect: − 0.412), while Kinesiophobia is directly associated with exercise adherence and also indirectly through exercise self-efficacy (direct effect: − 0.184, indirect effect: − 0.415).
Conclusion: Patients after total knee arthroplasty who have high levels of psychological distress (pain catastrophizing and kinesiophobia) are vulnerable to be non-adherent to exercise behaviors. Exercise self-efficacy explains the effects of pain catastrophizing and kinesiophobia on exercise adherence and may be a key target for measures to improve exercise behaviors in patients after total knee arthroplasty.
Keywords: pain catastrophizing, kinesiophobia, self-efficacy, exercise, adherence, total knee arthroplasty
Introduction
Osteoarthritis (OA) is one of the leading causes of disability worldwide, affecting approximately 10% of individuals over 65 years.1,2 Over 130 million individuals are affected by OA in China3 and the incidence of OA has been increasing gradually due to the aging population and the exposure to risk factors (e.g., obesity, osteoporosis).4 Globally, the knee was the leading OA site,5 and the prevalence of symptomatic Knee OA is reported to be 10.3% (women) and 5.7 (men) in old Chinese.6 For individuals with primary, end-stage, knee OA, total knee arthroplasty (TKA) is most commonly recommended and considered optimal and effective,7 which could significantly decrease self-reported pain and increase functional capability, mobility, and quality of life.8,9 Almost 400,000 individuals underwent TKA each year in China, and the number still showed an increasing trend.10 Functional exercise after TKA is considered an essential part of achieving optimal patient outcomes.11,12 Early functional exercise can effectively reduce the incidence of post-surgery complications, promote joint recovery and strength gains, and shorten the length of hospital stay.12–14
Despite the substantial impact of exercise on post-TKA recovery, evidence revealed that poor adherence to exercise is common in patients after TKA,15–17 limiting the effectiveness of their recovery and potentially leading to further complications such as increased pain and muscle weakness.13,18 Understanding the factors of adherence to exercise after TKA, will allow healthcare professionals (HCPs) to provide more effective measures to increase exercise adherence and further improve recovery outcomes.19 Notably, sociodemographic and clinical factors, such as education level, income, marital status, postoperative complications, and comorbidities are associated with exercise adherence.19,20 Socioeconomic factor, patients with more support from family/ friends would have more time to devote to exercise, and motivation to continue exercise.19 In addition, a growing body of evidence implicated some psychological factors, such as high levels of pain catastrophizing and kinesiophobia, low self-efficacy correlated with poor exercise adherence and negatively affect prognostic post-TKA.21–23
Pain catastrophizing is a psychological distress regarded as a negative cognitive and emotional coping strategy towards pain. It is characterized by three main components, including an excessive focus on pain sensations (rumination), an exaggerated perception of the threat value of pain symptoms (magnification), and beliefs that the control of pain is beyond one’s ability (helplessness).24,25 Catastrophizing in a pain context, patients tend to avoid engaging in pain-inducing activities due to their excessive focus on pain, which may lead to a reduction in exercise adherence and have a negative effect on post-TKA joint function recovery and outcomes.23 Evidence has indicated that patients with high levels of pain catastrophizing are more prone to be non-adherent to exercise.26
Kinesiophobia, or fear of movement, is referred as an irrational and debilitating fear of physical movement and activity.27 According to the theoretical framework of Fear of Movement, patients can respond to fear of movement in one of two ways: by confronting fear or avoiding fear. Confrontation leads to decrease fear, active exercise, and faster recovery. In contrast, avoidance can result in kinesiophobia, which may cause negative health outcomes, such as physical inactivity and disability.28,29 Kinesiophobia patients believe that painful activity will result in damage and that will increase suffering and/ or functional loss, leading to activity avoidance or escape and further causing low levels of physical activity and exercise.30 Evidence found that kinesiophobia is negatively associated with physical activity and exercise in post-TKA patients,31 knee OA patients,21 and other populations.32,33
Self-efficacy is a critical predictor of exercise adherence for patients after TKA,34 and exercise self-efficacy can be described as the individual’s ability to self-manage when faced with exercise task.35 According to the Theory of Self-efficacy proposed by psychologist Bandura,34 high levels of exercise self-efficacy increase patients’ confidence and beliefs in their capacity to carry out post-TKA exercise tasks. When they encounter setbacks or challenges during exercise, they possibly make more effort and generate satisfying exercise performance.36 A systematic review has shown that postoperative self-efficacy was more consistently related to recovery outcomes such as longer distance ambulation, exercise repetition and frequency, walking speed, and disability.37 And previous evidence revealed that exercise self-efficacy is positively correlated with exercise behaviors20 and self-efficacy enhancement intervention is demonstrated useful to increase patients’ exercise adherence.38,39
The existing literature review demonstrated pain catastrophizing, Kinesiophobia, and exercise self-efficacy are associated with exercise adherence. While, to our best knowledge, none have examined the relationships between all three constructs together in post-TKA patients. Clarifying and understanding the mechanisms behind the strong correlations between these psychosocial variables and health-promoting behaviors may assist in tailoring effective measures and interventions that are targeted at promoting exercise adherence in post-TKA patients. To summarize, the study aims to clarify the direct/ indirect association and possible causal pathways of these variables by using the mediation model.
Based on the Fear-Avoidance Model and the Theory of Self-Efficacy and the literatures mentioned above, we hypothesized that 1) pain catastrophizing is negatively correlated with exercise adherence; 2) exercise self-efficacy would mediate the relationship between pain catastrophizing and exercise adherence; 3) kinesiophobia is negatively correlated with exercise adherence; 4) exercise self-efficacy would mediate the relationship between kinesiophobia and exercise adherence. The hypothesized mediation model is shown in Figure 1.
 |
Figure 1 The hypothesized mediation models. (A) The mediation model for the effect of exercise self-efficacy on the relationships between pain catastrophizing and exercise adherence; (B) The mediation model for the effect of exercise self-efficacy on the relationships between kinesiophobia and exercise adherence. |
Materials and Methods
Participants
A cross-sectional survey was conducted on participants recruited by convenience sampling in three orthopedics units of a tertiary hospital in Baoding, a city in northern China, from September 2022 to June 2023. This study conformed with the principles outlined in the Declaration of Helsinki and was approved by the Medical Institutional Review Board of Baoding No.1 Central Hospital (Approval Number: [2022]068). Each participant signed an informed consent form before participating in this study. The participants met the following inclusion criteria: 1) a definite diagnosis of osteoarthritis by an orthopedic physician; 2) underwent primary total knee arthroplasty; 3) age ≥ 18 years. Participants were excluded if they had 1) cancer or other severe diseases, and 2) a mental disorder that prevented them from understanding the questionnaires.
Patients in the hospital followed the traditional (non-enhanced recovery after surgery, NRAS) pathway. Prior to the surgery, patients received ankle pump training as well as deep breathing and effective cough exercises. Upon returning to the ward, patients were provided in-person guidance (about 15–20 minutes) on knee joint exercises and encouraged patients to get out of bed the next day. Furthermore, they also were provided a paper-based functional exercise guidance program. Patients were encouraged to gradually perform exercises such as straight leg raises, knee joint bends, and walking with the assistance of auxiliary tools in the following days. Finally, nurses provided health education to patients who would be discharged from the hospital about how to continue joint exercises after discharge.
Following study enrollment, each patient completed questionnaires under the guidance of trained research assistants before they discharge. Research assistants received uniform training sessions to ensure consistency in data collection. The survey and the brief interview took about 20 minutes to complete.
The required sample size was calculated using G*Power version 3.1 based on a Priori Power Analyses.40 It is based on a medium effect size of 0.02, α of 0.05, and a power of 0.95. Considering a dropout rate of 10%, the required minimum sample size was 202 participants. Two hundred and eleven participants met the sample size requirement for the study.
Measures
Sample Characteristic
The socio-demographic and clinical data include age, gender, marital status, education attainment, monthly income per person, living condition, insurance type, joint pain duration (years), replacement site, length of stay and post-TKA complications. Data were reviewed from hospital medical records by research assistants.
Pain Catastrophizing
Pain catastrophizing was measured using the Chinese Version of the Pain Catastrophizing Scale (PCS-CV).41 This scale includes 13 items that assess negative perceptions related to pain. The scale has three dimensions: rumination (4 items), magnification (3 items), and helplessness (6 items). Each item is rated from “not at all” (score = 0) to “all the time” (score = 4). The total score is the sum of the items, ranging from 0 (no catastrophizing) to 52 (severe catastrophizing), and a higher score indicates higher levels of pain catastrophizing. In the current study, the Cronbach’s α for the PCS-CV was 0.90.
Kinesiophobia
The Chinese Version of the Tampa Scale for Kinesiophobia (TSK-CV) was used to measure kinesiophobia.42 It has shown good reliability and validity in the Chinese population with orthopedics diseases.43,44 The TSK-CV contains 17 items that assess the subjective rating of kinesiophobia, answered by a 4 - point Likert scale ranging from “strongly disagree” (score = 1) to “strongly agree” (score = 4). A total sum is calculated after the reversion of items 4, 8, 12, and 16. The total score varies between 17 and 68, with a higher score indicating a stronger perceived level of kinesiophobia. The Cronbach’s α for the TSK-CV was 0.84 in this study.
Exercise Self-Efficacy
The Self-efficacy for rehabilitation outcome scale (SER) was developed by Waldrop,35 followings Bandura’s guidelines to assess participants’ beliefs about their ability to perform behaviors typical in physical rehabilitation for hip and knee surgery. Items are rated on an 11-point Likert scale ranging from 0 (I cannot do it) to 10 (certain I can do it). The original English language scale can be considered reliable with a Cronbach’s α of 0.94. The Chinese Version of SER was translated by Wang,45 and has good reliability and validity.46 It contains two dimensions (twelve items): self-efficacy for rehabilitation therapy exercises (six items) and self-efficacy in overcoming barriers (six items). Higher total scores indicate better self-efficacy for physical rehabilitation for knee and hip surgery. In the present study, Cronbach’s α for SER was 0.88.
Exercise Adherence
Exercise adherence was measured by the functional exercise adherence scale for orthopedics patients, developed by Tan based on the World Health Organization (WHO) adherence concept framework, literature review, interview, and expert consultation.47 This scale consists of three dimensions (psychological, active learning, and physical) and fifteen items. Each item is rated from 1 to 5 points (“I cannot do it at all” = 1, “I can do it” = 5). The total scores range from 15 to 75, with higher scores indicating better adherence to function exercise. Adherence rate = (actual adherence score/ theoretical maximum adherence score) × 100%. It was categorized as high (> 75.0%), medium (50.0–75.0%), and low (< 50.0%). The scale has good validity and reliability (with Cronbach’s α of 0.930),48 which can be used as a valid tool to assess adherence to functional exercise for orthopedics patients. In the current study, the Cronbach’s α was 0.92.
Statistical Analyses
Data analyses for this study were performed using SPSS 22.0 (SPSS; IBM, Armonk, NY, USA) and Mplus 8.3. First, a descriptive analysis was conducted to report the sample characteristics (continuous variables: means and standard deviations (SD); categorical variables: frequencies and percentages). Second, a Pearson correlation coefficient was computed to examine the relationship between the four variables (pain catastrophizing, kinesiophobia, exercise self-efficacy, and exercise adherence). Next, mediation analysis was conducted using Mplus 8.3. All the demographic and clinical variables (such as age, gender, marital status, education, income, and insurance) were controlled as covariates in this mediation analysis. The goodness-of-fit indices, including the Comparative Fit Index (CFI > 0.90), Tucker Lewis index (TLI > 0.90) and Root Mean Square Error of Approximation (RMSEA < 0.05), were used to evaluate the model goodness of fit. 5000 bootstraps were used and a 95% Confidence Interval (CI) was estimated for the mediation effects, with CI not containing 0, indicating the mediation effects being significant. Harman’s single-factor test was used to examine the common method bias (CMB).49 The variance explained by the first factor was lower than 40%, indicating that no CMB exists in the research data.
Results
Demographic and Clinical Characteristics of the Samples
The sample consisted of 211 patients after TKA, 44 males and 167 females, aged between 51 and 81 years old (mean = 66.75, SD = 6.15). Most patients were married (n = 176, 83.4%), and lived with family members (n = 195, 92.4%). The average length of hospital stay was 12.56 days (SD = 3.42), ranging from 7 to 29 days. Socio-demographic and clinical characteristics are shown in Table 1.
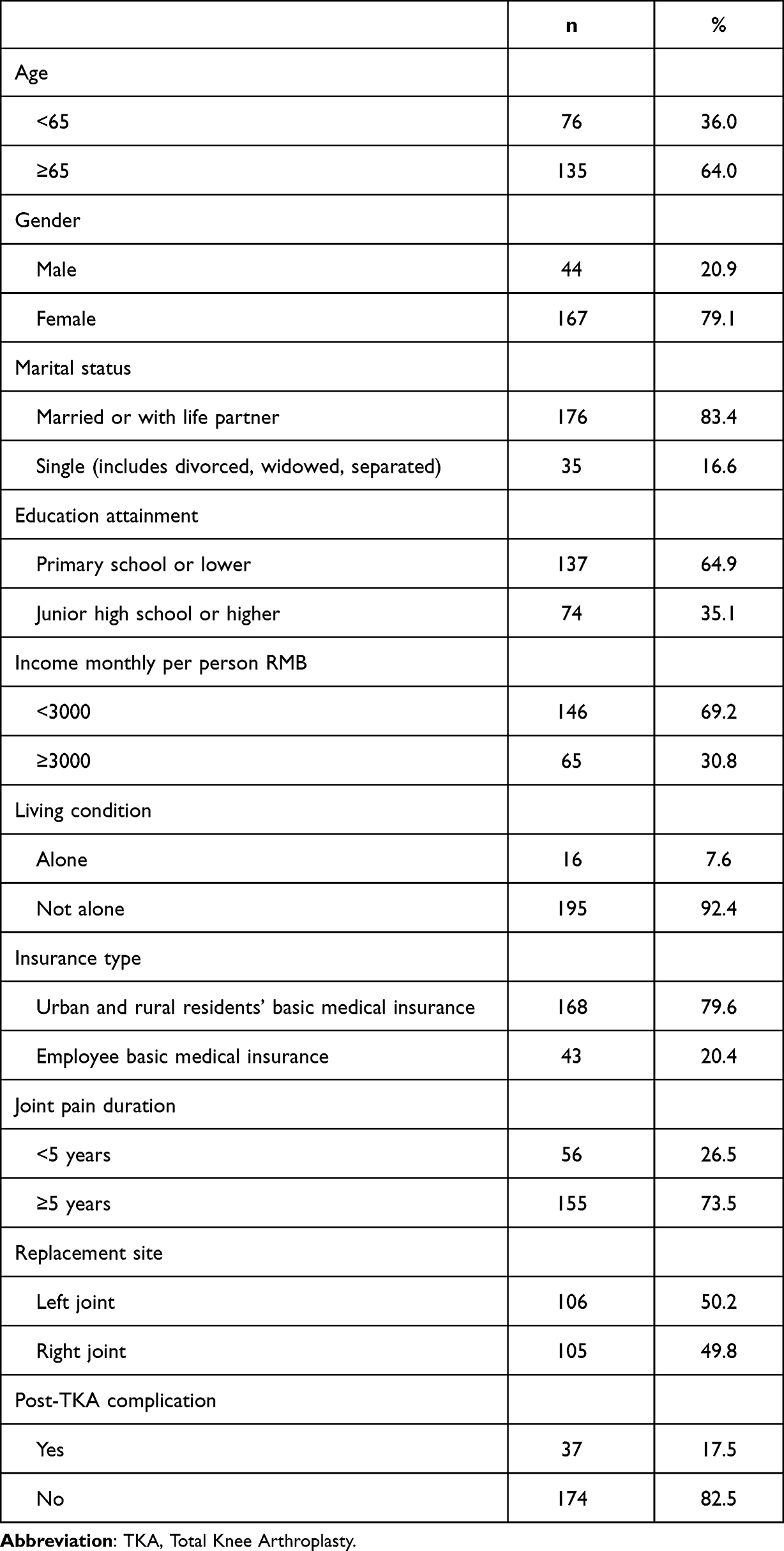 |
Table 1 Socio-Demographic and Clinical Characteristics (N = 211) |
Descriptive Statistics and Correlation Among Pain Catastrophizing, Kinesiophobia, Exercise Self-Efficacy and Exercise Adherence
The mean score for exercise adherence 56.10 ± 11.32, and the adherence rate were high (n = 121, 57.4%), medium (n = 72, 34.1%), and low (n = 18, 8.5%). The high adherence rate of psychological dimension was highest (n = 154, 73.0%) and the active learning dimension was lowest (n = 29, 13.7%). Descriptive characteristics of the four variables are presented in Table 2.
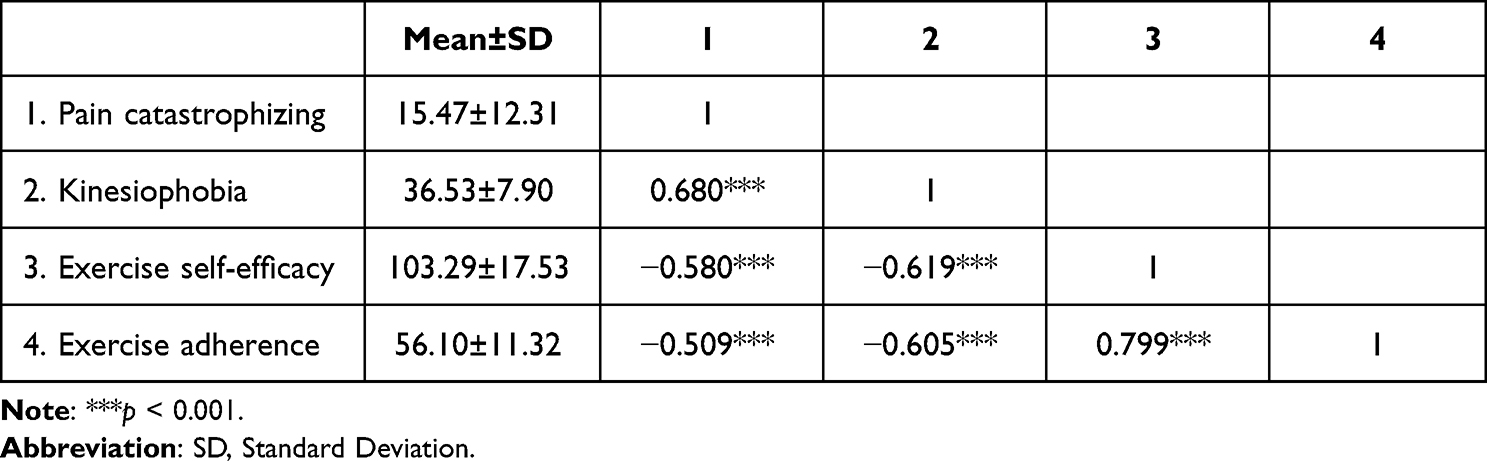 |
Table 2 Descriptive Statistics and Correlations Among Pain Catastrophizing, Kinesiophobia, Exercise Self-Efficacy and Exercise Adherence (N = 211) |
Pain catastrophizing and kinesiophobia were negatively associated with exercise self-efficacy (r = −0.580, r = −0.619, all P < 0.001) and exercise adherence (r = −0.509, r = −0.605, all P < 0.001) and exercise self-efficacy was positively related to exercise adherence (r = 0.799, P < 0.001) (Table 2).
Common Method Bias
The Herman single-factor analysis was carried out to examine Common Method Bias,49 and items of the four variables, ie, pain catastrophizing, kinesiophobia, exercise self-efficacy, and exercise adherence were examined by non-rotation principal component factor analysis. The first factor resulted in 33.59% of variance lower than 40%, indicating that there was no CMB in this study.
Pain Catastrophizing, Exercise Self-Efficacy and Exercise Adherence
The mediation model has a good overall fit (CFI = 1.000, TLI = 1.000 and RMSEA = 0.000). Figure 2A displays that the standardize coefficient of pain catastrophizing on exercise adherence decreased from −0.466 (95% CI (−0.557, −0.359)) to −0.054 (95% CI (−0.154, 0.047)), which was not statistically significant, after introducing the mediator of exercise self-efficacy into the model with controlling covariates. This result suggested a full mediation, and the relationship between pain catastrophizing and exercise adherence was totally mediated by exercise self-efficacy. Pain catastrophizing could indirectly influence TKA patients’ exercise adherence via exercise self-efficacy. The mediation effect was −0.412 (95% CI (−0.513, −0.314)), with an effect size of 88.4%. The more detailed information is shown in Table 3.
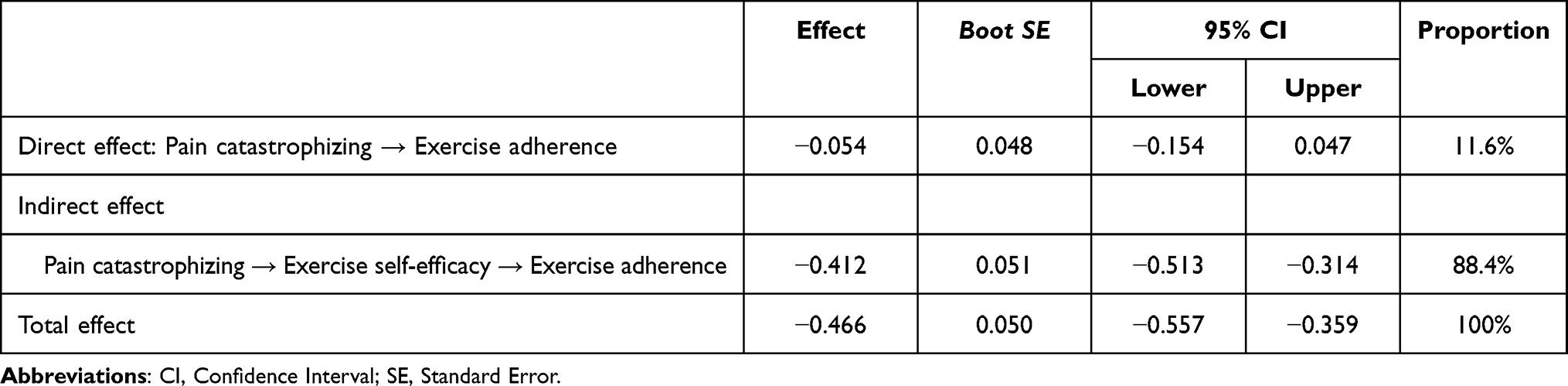 |
Table 3 Mediation Analysis of Pain Catastrophizing and Exercise Adherence (N = 211) |
 |
Figure 2 Standardized path coefficients for the mediation models. (A) The mediation model linking pain catastrophizing and exercise adherence; (B) The mediation model linking kinesiophobia and exercise adherence. The lower coefficient in parentheses represents the path before exercise self-efficacy was introduced into the model, and the upper coefficient represents the path after exercise self-efficacy was introduced into the model. All models were adjusted for following covariates: age, gender, marital status, education, income, living condition, insurance, joint pain duration, replacement site, length of stay, post-TKA complications. ***p < 0.001. |
Kinesiophobia, Exercise Self-Efficacy and Exercise Adherence
The data has met a good of fit of model (CFI = 1.000, TLI = 1.000 and RMSEA = 0.000) (Figure 2B). The direct effect from kinesiophobia to exercise adherence was significant (β = −0.184; 95% CI (−0.280, −0.094)), after controlling covariates and introducing the mediator of exercise self-efficacy. This result indicated a partial mediation, and the relationship between kinesiophobia and exercise adherence was partially mediated by exercise self-efficacy. Kinesiophobia could directly influence exercise adherence and also indirectly via exercise self-efficacy. The mediation effect was −0.415 (95% CI (−0.494, −0.340)), with an effect size of 69.3%. More details are presented in Table 4.
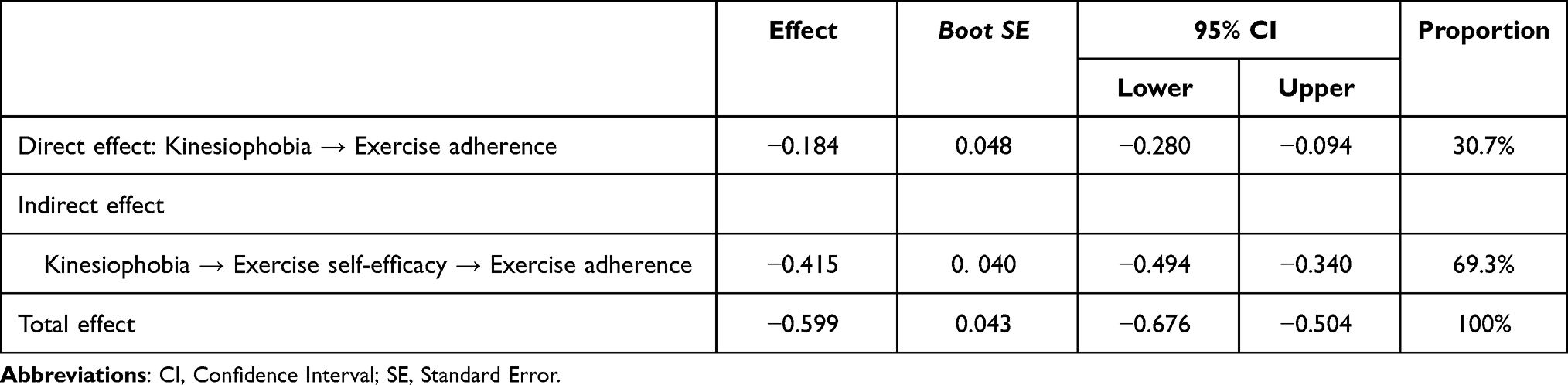 |
Table 4 Mediation Analysis of Kinesiophobia and Exercise Adherence (N = 211) |
Discussion
To our best knowledge, this is the first study to consider the correlation among pain catastrophizing, kinesiophobia, exercise self-efficacy, and exercise adherence in patients after TKA. It is also the first study to explore whether exercise self-efficacy mediates the relationship between pain catastrophizing, kinesiophobia, and exercise adherence. This study provides a new insight towards understanding how pain catastrophizing and kinesiophobia affect exercise adherence in patients after TKA.
In the current study, exercise adherence among post-TKA patients was 56.10, which was similar to the previous study.15 Our results showed the medium- and low-adherence rate was 42.6%, and the rate of adherence in the active learning dimension was the lowest, which is in line with the results in the early study.50 This result may be explained by the fact that 64% of the patients were old and generally obtained a low level of education in this study, and they had limited ability to actively learn and accept new things.15 Accordingly, HCPs should provide more detailed functional exercise protocols for old patients with low education levels, and increase patients’ awareness of actively seeking help from multiple sources, such as HCPs, the Internet, or other patients.
The present study found a significant negative correlation between pain catastrophizing and exercise adherence, which is consistent with the previous study.26 This suggests that post-TKA patients who have a higher level of pain catastrophizing are more likely to be nonadherent with rehabilitation exercise. A possible explanation for this might be that pain catastrophizing probably contributes to escape and avoidance behaviors.29 Growing evidence indicated that pre- and post-operative pain catastrophizing has a negative effect on patients undergoing TKA, often leading to persistent pain and poor function.51,52 Post-TKA patients who catastrophize pain may perceive more persistent pain during rehabilitation exercise and concern that worsen their keen condition. Thus, patients are more likely to avoid or reduce their participation in post-TKA exercise, resulting in decreased exercise adherence.53 In addition, our results also showed exercise self-efficacy as a mediator of correlation between pain catastrophizing and exercise adherence, indicating patients with high pain catastrophizing would have a lower confidence to attend and insist on post-TKA exercise, further leading to poor exercise adherence. Early mobilization and exercise may cause pain and discomfort in patients due to knee joint swelling following TKA. It may boost catastrophizing thoughts and avoid pain-induced activities and behaviors in pain-catastrophizing patients, which reduce their confidence to engage in exercise and ultimately lead to poor exercise adherence.
Our finding that kinesiophobia was associated with exercise adherence conforms to previous studies in post-TKA patients.30,31 Kinesiophobia patients are less to adhere to exercise after TKA. One qualitative study conducted in China to explore the real experience of post-TKA patients with kinesiophobia in early rehabilitation exercise,54 found that fear of pain, uncertainty about the effects of early rehabilitation exercise, high economic and psychological pressure, and lack of families, professionals, and social support might be the explanations for low enthusiasm for early exercise. Our study further demonstrated that kinesiophobia not only directly and negatively affected exercise adherence in post-TKA patients, but also indirectly influenced the level of exercise adherence through diminishing exercise self-efficacy. This result is similar to earlier studies55,56 on the relationship among kinesiophobia, physical self-efficacy, and physical activity in kidney transplant recipients. Liu et al55 and Zelle et al56 study reported self-efficacy mediated the relationship between kinesiophobia and physical activity. Based on Bandura’s self-efficacy theory, physical and emotional states as major contributors to the promotion of self-efficacy.34 Positive emotion may enhance self-efficacy, while negative emotion diminishes them. Kinesiophobia as an emotional response to perceived health threats associated with physical movement and activity, is likely to reduce individuals’ self-efficacy and thereby decrease exercise adherence.56
These findings suggest that exercise self-efficacy is a crucial cognitive mechanism by which pain catastrophizing and kinesiophobia may affect exercise adherence behaviors in patients after TKA. Self-efficacy, a modifiable psychological factor, could be enhanced and increased through four major approaches proposed by Bandura, including performance accomplishments, verbal persuasion, vicarious learning and physiological, and emotional states or physiological feedback.34 For example, HCPs help patients to develop more detailed planning of early exercise, which contributes to attaining exercise goals, thereby increasing mastery experience. And focusing on small successes that have been achieved enhances self-efficacy.57,58 Patients with good self-efficacy and exercise adherence behaviors are encouraged and invited to share the successful experience of persistently participating in early exercise. And to improve verbal persuasion about the capacity, HCPs could provide more encouragement and persuasion to patients to perform early mobilization and exercise task, so that patients feel more confident to perform these tasks.58
This study adds to existing knowledge by showing that pain catastrophizing and kinesiophobia have strong contributions to exercise adherence in post-TKA patients and that exercise self-efficacy may serve as a key mechanism for these correlations. The evidence from this study provides a direction for healthcare professionals to tailor targeted and effective interventions and measures to improve exercise adherence in post-TKA patients. Our findings suggest that exercise adherence in post-TKA patients with pain catastrophizing or kinesiophobia could be promoted by enhancing their exercise self-efficacy. HCPs are expected to pay closer attention to post-TKA patients who experience pain catastrophizing and kinesiophobia and to apply effective measures and interventions strategies aimed at improving exercise self-efficacy. In this study, we focused on pain-related catastrophizing and kinesiophobia among post-TKA patients, while previous evidence also indicated that pre-TKA pain-related fear and anxiety were common, which are harmful for patients’ recovery.59 Therefore, pre-TKA pain-related catastrophizing and kinesiophobia should be paid more attention in future studies. Furthermore, post-TAK patients need to continue functional exercise. However, the adherence to exercise was poor. Earlier evidence revealed that frequent physiotherapist’s instruction helps the patients improve knee exercises and recovery outcomes.60 Thus, HCPs should explore establishing a post-discharge joint exercise guidance program based on physiotherapist.
Limitation
This study has two limitations. First, this study used a convenience sampling method to recruit post-TKA patients from one hospital, which limited the representativeness of the results to some extent. Second, the cross-sectional study design limits the ability to infer causal relationships between variables. In the future, longitudinal research design and experimental design could be used to verify the findings of our study and further examine the causality between these variables.
Conclusion
This study examines the connections among pain catastrophizing, kinesiophobia, exercise self-efficacy, and exercise adherence in post-TKA patients using mediation models. The findings of this study demonstrated that pain catastrophizing and kinesiophobia were significantly correlated with exercise adherence. Moreover, pain catastrophizing and kinesiophobia could indirectly influence exercise adherence through exercise self-efficacy. Therefore, it seems necessary to reduce pain catastrophizing and kinesiophobia in post-TKA patients at an early stage through targeted and effective measures to enhance exercise self-efficacy in order to promote exercise adherence and obtain better rehabilitation outcomes.
Abbreviations
OA, Osteoarthritis; TKA, Total Knee Arthroplasty; HCPs, Healthcare Professionals; PCS-CV, The Chinese Version of the Pain Catastrophizing Scale; WHO, World Health Organization; TSK-CV, The Chinese version of the Tampa Scale for Kinesiophobia; SER, The Self-efficacy for Rehabilitation Outcome Scale; SD, Standard Deviation; CFI, Comparative Fit Index; TLI, Tucker Lewis index; RMSEA, Root Mean Square Error of Approximation; CI, Confidence Interval; CMB, Common Method Bias.
Data Sharing Statement
The data used to support the conclusions in this study can be obtained from the corresponding authors upon reasonable request.
Ethics Statement
The study was approved by the Medical Institutional Review Board of Baoding No.1 Central Hospital (Approval Number: [2022]068). All procedures performed in studies involving human participants were in accordance with the ethical standards and with the Helsinki Declaration. Informed consent was obtained from all individual participants included in the study.
Informed Consent
Informed consent was obtained from all individual adult participants included in the study.
Acknowledgments
We acknowledge the contributions of the patients who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Program of Baoding (grant number: 2341ZF092).
Disclosure
The authors declare that there is no conflict of interest in this work.
References
1. Safiri S, Kolahi -A-A, Smith E, et al. Global, regional and national burden of osteoarthritis 1990–2017: a systematic analysis of the Global Burden of Disease Study 2017. Ann Rheum Dis. 2020;79(6):819–828. doi:10.1136/annrheumdis-2019-216515
2. Fu M, Zhou H, Li Y, Jin H, Liu X. Global, regional, and national burdens of hip osteoarthritis from 1990 to 2019: estimates from the 2019 Global Burden of Disease Study. Arthritis Res Ther. 2022;24(1):1–11. doi:10.1186/s13075-021-02705-6
3. Long H, Liu Q, Yin H, et al. Prevalence trends of site-specific osteoarthritis from 1990 to 2019: findings from the Global Burden of Disease Study 2019. Arthritis Rheumatol. 2022;74(7):1172–1183. doi:10.1002/art.42089
4. Long H, Zeng X, Liu Q, et al. Burden of osteoarthritis in China, 1990–2017: findings from the Global Burden of Disease Study 2017. Lancet Rheumatol. 2020;2(3):e164–e172. doi:10.1016/S2665-9913(19)30145-6
5. Sun X, Zhen X, Hu X, et al. Osteoarthritis in the middle-aged and elderly in China: prevalence and influencing factors. Int J Environ Res Public Health. 2019;16(23):4701. doi:10.3390/ijerph16234701
6. Tang X, Wang S, Zhan S, et al. The prevalence of symptomatic knee osteoarthritis in China: results from the China health and retirement longitudinal study. Arthritis Rheumatol. 2016;68(3):648–653. doi:10.1002/art.39465
7. Ritter MA, Albohm MJ, Keating EM, Faris PM, Meding JB. Comparative outcomes of total joint arthroplasty. J Arthroplasty. 1995;10(6):737–741. doi:10.1016/S0883-5403(05)80068-3
8. Chang J, Fu M, Cao P, Ding C, Wang D. Patient-reported quality of life before and after total knee arthroplasty: a multicenter observational study. Patient Prefer Adherence. 2022;16:737–748. doi:10.2147/PPA.S357632
9. Cram P, Lu X, Kates SL, Singh JA, Li Y, Wolf BR. Total knee arthroplasty volume, utilization, and outcomes among medicare beneficiaries, 1991–2010. JAMA. 2012;308(12):1227–1236. doi:10.1001/2012.jama.11153
10. Bian YY, Cheng KY, Chang X, Weng XS. Reports and analysis of amount of hip and knee arthroplasty in China from 2011 to 2019. Chin J Orthop. 2020;40(21):1453–1460.
11. Bakaa N. Exercise Adherence Post Total Knee Arthroplasty. McMaster University; 2020.
12. Chen H, Li S, Ruan T, Liu L, Fang L. Is it necessary to perform prehabilitation exercise for patients undergoing total knee arthroplasty: meta-analysis of randomized controlled trials. Phys Sportsmed. 2018;46(1):36–43. doi:10.1080/00913847.2018.1403274
13. Alrawashdeh W, Eschweiler J, Migliorini F, El Mansy Y, Tingart M, Björn R. Effectiveness of total knee arthroplasty rehabilitation programmes: a systematic review and meta-analysis. J Rehabil Med. 2021;53(6):jrm00200. doi:10.2340/16501977-2827
14. Jakobsen TL, Kehlet H, Husted H, Petersen J, Bandholm T. Early progressive strength training to enhance recovery after fast-track total knee arthroplasty: a randomized controlled trial. Arthritis Care Res. 2014;66(12):1856–1866. doi:10.1002/acr.22405
15. Qu QQ. The relationship between family resilience, activation and exercise compliance in patients with artificial joint replacement. Dalian Med Univ; 2022.
16. Zhao GY. Home-based rehabilitation adherence and its influencing factors among patients who underwent total knee arthroplasty. Shanghai Jiaotong Univ; 2019.
17. Li F. Study on compliance and influencing factors of home rehabilitation training for patients after total knee arthroplasty in Hainan Province. Hainan Med Univ; 2021.
18. Pozzi F, Snyder-Mackler L, Zeni J. Physical exercise after knee arthroplasty: a systematic review of controlled trials. Eur J Phys Rehabil Med. 2013;49(6):877–892.
19. Bakaa N, Chen LH, Carlesso L, Richardson J, Shanthanna H, Macedo L. Understanding barriers and facilitators of exercise adherence after total-knee arthroplasty. Disabil Rehabil. 2022;44(21):6348–6355. doi:10.1080/09638288.2021.1965232
20. Zhao GY, Xu YL. Rehabilitation adherence and its influencing factors among patients after artificial joint replacement surgery. Nurs J Chin PLA. 2018;35(16):41–45.
21. Aydemir B, Huang CH, Foucher KC. Strength and physical activity in osteoarthritis: the mediating role of kinesiophobia. J Orthop Res. 2022;40(5):1135–1142. doi:10.1002/jor.25151
22. Chester R, Daniell H, Belderson P, et al. Behaviour change techniques to promote self-management and home exercise adherence for people attending physiotherapy with musculoskeletal conditions: a scoping review and mapping exercise. Musculoskelet Sci Pract. 2023;66:102776. doi:10.1016/j.msksp.2023.102776
23. Yakobov E, Stanish W, Tanzer M, Dunbar M, Richardson G, Sullivan MJ. The prognostic value of pain catastrophizing in health-related quality of life judgments after total knee arthroplasty. Health Qual Life Outcomes. 2018;16(1):1–8. doi:10.1186/s12955-018-0955-2
24. Sullivan MJ, Thorn B, Haythornthwaite JA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain. 2001;17(1):52–64. doi:10.1097/00002508-200103000-00008
25. Sullivan M, Tanzer M, Stanish W, et al. Psychological determinants of problematic outcomes following total knee arthroplasty. Pain. 2009;143(1–2):123–129. doi:10.1016/j.pain.2009.02.011
26. De Lira MR, De Oliveira AS, França RA, Pereira AC, Godfrey EL, Chaves TC. The Brazilian Portuguese version of the Exercise Adherence Rating Scale (EARS-Br) showed acceptable reliability, validity and responsiveness in chronic low back pain. BMC Musculoskelet Disord. 2020;21(1):1–13. doi:10.1186/s12891-020-03308-z
27. Kori S. Kinesiophobia: a new view of chronic pain behaviour. Pain Manag. 1990;3:35–43.
28. Vlaeyen JW, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317–332. doi:10.1016/S0304-3959(99)00242-0
29. Crombez G, Eccleston C, Van Damme S, Vlaeyen JW, Karoly P. Fear-avoidance model of chronic pain: the next generation. Clin J Pain. 2012;28(6):475–483. doi:10.1097/AJP.0b013e3182385392
30. Bunzli S, Smith A, Watkins R, Schütze R, O’Sullivan P. What do people who score highly on the Tampa Scale of kinesiophobia really believe? Clin J Pain. 2015;31(7):621–632. doi:10.1097/AJP.0000000000000143
31. Zia S, Atta S, Ahmad MS, Murtaza F, Ahmad MZ, Hassan SZ. Relationship between kinesiophobia, fall risk and activity level among elderly females after total knee arthroplasty. J Riphah Coll Rehabili Sci. 2022;10(02):70–74. doi:10.53389/JRCRS.2022100203
32. Bäck M, Cider Å, Herlitz J, Lundberg M, Jansson B. Kinesiophobia mediates the influences on attendance at exercise-based cardiac rehabilitation in patients with coronary artery disease. Physiother Theory Pract. 2016;32(8):571–580. doi:10.1080/09593985.2016.1229828
33. Wang J, Bai C, Zhang Z, Chen O. The relationship between dyspnea-related kinesiophobia and physical activity in people with COPD: cross-sectional survey and mediated moderation analysis. Heart Lung. 2023;59:95–101. doi:10.1016/j.hrtlng.2023.02.007
34. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037/0033-295X.84.2.191
35. Waldrop D, Lightsey OR Jr, Ethington CA, Woemmel CA, Coke AL. Self-efficacy, optimism, health competence, and recovery from orthopedic surgery. J Couns Psychol. 2001;48(2):233–238. doi:10.1037/0022-0167.48.2.233
36. Dohnke B, Knäuper B, Müller-Fahrnow W. Perceived self-efficacy gained from, and health effects of, a rehabilitation program after hip joint replacement. Arthritis Rheum. 2005;53(4):585–592. doi:10.1002/art.21324
37. Magklara E, Burton CR, Morrison V. Does self-efficacy influence recovery and well-being in osteoarthritis patients undergoing joint replacement? A systematic review. Clin Rehabil. 2014;28(9):835–846. doi:10.1177/0269215514527843
38. Caetano LC, Pacheco BD, Samora GA, Teixeira-Salmela LF, Scianni AA. Self-efficacy to engage in physical exercise and walking ability best predicted exercise adherence after stroke. Stroke Res Treat. 2020;2020:2957623. doi:10.1155/2020/2957623
39. Chen W, Li XH, Xu ZZ, Huang YZ, Gu JW, Chen XY. The effects of rehabilitation self-efficacy on home-based rehabilitation exercises adherence in patients after total knee arthroplasty. J Clin Nurs Pract. 2020;6(09):140–143.
40. Faul F, Erdfelder E, Buchner A, Lang A-G. Statistical power analyses using G* Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
41. Yap JC, Lau J, Chen PP, et al. Validation of the Chinese Pain Catastrophizing Scale (HK-PCS) in patients with chronic pain. Pain Med. 2007;9(2):186–195. doi:10.1111/j.1526-4637.2007.00307.x
42. Hu W. Cross-cultural adaptation of simplified Chinese version of TSK/FABQ, and its clinical application in the assessment of fear avoidance for patients with low back pain. Nav Med Univ; 2012.
43. Cai L, Liu Y, Xu H, Xu Q, Wang Y, Lyu P. Incidence and risk factors of kinesiophobia after total knee arthroplasty in Zhengzhou, China: a cross-sectional study. J Arthroplasty. 2018;33(9):2858–2862. doi:10.1016/j.arth.2018.04.028
44. Tan M, Liu Y, Li J, et al. Factors associated with kinesiophobia in Chinese older adults patients with osteoarthritis of the knee: a cross-sectional survey. Geriatr Nurs. 2022;48:8–13. doi:10.1016/j.gerinurse.2022.08.013
45. Wang HY, Xu YL, Hu SL, Zhou L, Qian Y, Qian HJ. Evaluation of the reliability and validity of Chinese version self-efficacy for rehabilitation outcome scale. Chin J Mod Nurs. 2014;20(3):268–270. doi:10.3760/cma.j.issn.1674-2907.2014.03.007
46. Xiang N, Ma YF, Gao N, et al. The clinical study of early ambulation in patients with total knee arthroplasty under the guidance of fast track surgery. Chin Nurs Manage. 2018;18(11):1544–1549. doi:10.3969/j.issn.1672-1756.2018.11.024
47. Tan YY, He H, Yang XX, Li XS, Mi JX. Development and reliability and validity test of the compliance scale of functional exercise for orthopedic patients. Chin Nurs Manage. 2019;19(11):1626–1631.
48. Pan WY, Zhang JJ, Li WL, Dong YH, Liu SY, Zheng J. Study on effect of innovative Teach- back tool kit on improving functional exercise compliance and rehabilitation for patients undergoing total knee arthroplasty. Chin Nurs Res. 2022;36(23):4243–4247.
49. Zhou H, Long LR. Statistical remedies for common method biases. Adv Psychol Sci. 2004;12(06):942–950.
50. Xx L, Qy L, Jz L, Mf Z. Influence of exercise self-efficacy on exercise compliance after discharge of patients receiving Hip arthroplasty. Chin Nurs Manage. 2019;19(09):1371–1375.
51. Burns LC, Ritvo SE, Ferguson MK, Clarke H, Seltzer Z, Katz J. Pain catastrophizing as a risk factor for chronic pain after total knee arthroplasty: a systematic review. J Pain Res. 2015;8:21–32. doi:10.2147/JPR.S64730
52. Riddle DL, Wade JB, Jiranek WA, Kong X. Preoperative pain catastrophizing predicts pain outcome after knee arthroplasty. Clin Orthop Relat Res. 2010;468(3):798–806. doi:10.1007/s11999-009-0963-y
53. Elfving B, Andersson T, Grooten WJ. Low levels of physical activity in back pain patients are associated with high levels of fear-avoidance beliefs and pain catastrophizing. Physiother Res Int. 2007;12(1):14–24. doi:10.1002/pri.355
54. Cai LB, Liu YJ, Cui MR, Guo YR, Zheng SS, Wang YY. Early rehabilitation exercise in total knee arthroplasty patients with kinesiophobia: a qualitative study. Chin J Nurs. 2019;54(11):1663–1668.
55. Liu M, Sun Q, Cui L, et al. Fear of movement and physical self-efficacy partially mediate the association between fatigue and physical activity among kidney transplant recipients. Clin Nurs Res. 2021;30(7):950–959. doi:10.1177/1054773821990263
56. Zelle DM, Corpeleijn E, Klaassen G, Schutte E, Navis G, Bakker SJ. Fear of movement and low self-efficacy are important barriers in physical activity after renal transplantation. PLoS One. 2016;11(2):e0147609. doi:10.1371/journal.pone.0147609
57. Olander EK, Fletcher H, Williams S, Atkinson L, Turner A, French DP. What are the most effective techniques in changing obese individuals’ physical activity self-efficacy and behaviour: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2013;10(1):29. doi:10.1186/1479-5868-10-29
58. Williams SL, French DP. What are the most effective intervention techniques for changing physical activity self-efficacy and physical activity behaviour—and are they the same? Health Educ Res. 2011;26(2):308–322. doi:10.1093/her/cyr005
59. Londhe SB, Shah RV, Patwardhan M, et al. Understanding the apprehension and concern haunting patients before a total knee arthroplasty. Arthroplasty. 2021;3(14):1–5. doi:10.1186/s42836-021-00069-5
60. Londhe SB, Shah RV, Doshi AP, et al. Home physiotherapy with vs. without supervision of physiotherapist for assessing manipulation under anaesthesia after total knee arthroplasty. Arthroplasty. 2021;3(10):1–5. doi:10.1186/s42836-020-00063-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Adherence to an mHealth Tool for Self-Management of COPD Exacerbations
Bischoff EW, Ariens N, Boer L, Vercoulen J, Akkermans RP, van den Bemt L, Schermer TR
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2381-2389
Published Date: 1 November 2023
MICROS: Asthma Control App for School Adolescents in a Low Resource Setting - A Cluster Randomized Controlled Trial Protocol
Katumba JD, Kirenga B, Muwagga Mugagga A, Kalyango JN, Nantanda R, Karamagi C
Patient Preference and Adherence 2023, 17:3125-3133
Published Date: 30 November 2023
Network Analysis of Pain Catastrophizing, Self-Efficacy, and Kinesiophobia Among Patients After Total Knee Arthroplasty: A Cross-Sectional Study
Zhou Y, Gao W, Cao Z, Gao S, Guo X, Liu M, Cao C
Patient Preference and Adherence 2024, 18:1897-1906
Published Date: 16 September 2024
Pain Intensity and Pain Catastrophizing Among Patients with Chronic Pain: The Mediating Effect of Self-Efficacy
Li J, Cui Y, Jia Q, Ouyang A, Hua Y
Journal of Pain Research 2025, 18:1361-1373
Published Date: 19 March 2025
Revolution or Empty Promise? A 6- and 12-Month Follow-Up to an RCT of the Online Exercise Program PERMANENTO in Older Adults
Machacova K, Polanska H, Steffl M, Bartova A, Novotna B, Holmerova I
Clinical Interventions in Aging 2025, 20:1519-1535
Published Date: 9 September 2025